Back to Journals » International Journal of Women's Health » Volume 18
A Preoperative Nomogram Integrating Clinical and Ultrasonic Features to Predict Extra-Pelvic Metastasis in Ovarian Cancer: A Multicenter Retrospective Study
Authors Wang Y, Lin W, He Y, Wang D, Wu X, He S, Gong M, Li L, Lyu G ![]()
Received 15 October 2025
Accepted for publication 18 January 2026
Published 24 January 2026 Volume 2026:18 574550
DOI https://doi.org/10.2147/IJWH.S574550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Yanli Wang,1,* Weihong Lin,2,* Yifang He,1 Dandan Wang,1 Xiuming Wu,3 Shaozheng He,1 Min Gong,4 Luhong Li,2 Guorong Lyu1,5
1Department of Ultrasound, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, People’s Republic of China; 2Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, People’s Republic of China; 3Department of Ultrasound, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, People’s Republic of China; 4Department of Ultrasound, Chengdu Third People’s Hospital, Chengdu, People’s Republic of China; 5Department of Clinical Medicine, Quanzhou Medical College, Quanzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guorong Lyu, Department of Ultrasound, The Second Affiliated Hospital of Fujian Medical University, No. 34 North Zhongshan Road, Quanzhou, Fujian Province, 362000, People’s Republic of China, Email [email protected] Luhong Li Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Fujian Medical University, No. 34 North Zhongshan Road, Quanzhou, Fujian Province, 362000, People’s Republic of China, Email [email protected]
Purpose: Ovarian cancer (OC) is a prevalent gynecological malignancy, often diagnosed at an advanced stage with extra-pelvic metastases. The accurate identification of advanced OC is essential for guiding appropriate treatment plans and influencing outcomes. The purpose of this research was to establish a preoperative nomogram integrating clinical and ultrasonic features to predict extra-pelvic metastasis, which may facilitate precise diagnosis and personalized treatment for OC patients.
Patients and Methods: This retrospective study included 347 women with OC from three medical centers who had clear pathology and ultrasonic examination before surgery from March 2016 to July 2025. They were divided into two groups according to whether extra-pelvic metastasis occurred: group A without extra-pelvic metastasis (n=164) and group B with extra-pelvic metastasis (n=183). The total patient population was randomly split between a training set (70%) and a validation set (30%). Predictors were selected using LASSO, followed by univariate and multivariate logistic regression analyses. A predictive nomogram was established to predict the risk of extra-pelvic metastasis of OC.
Results: Four independent risk factors ascites (OR 7.07, 95% CI 3.54– 14.11, p< 0.001), maximum tumor diameter (OR 1.08, 95% CI 1.01– 1.15, p=0.029), ill-defined boundary (OR 4.20, 95% CI 2.18– 8.12, p< 0.001), and blood flow score level 4 (OR 4.69, 95% CI 1.70– 12.97, p=0.003) were screened using LASSO and logistic regression, and a nomogram was established. The model demonstrated high discriminatory power, with an AUC of 0.860 (95% CI: 0.812– 0.908) in the training set and 0.865 (95% CI: 0.798– 0.932) in the validation set. The calibration curve and decision curve analysis curve show great performance.
Conclusion: The developed nomogram, incorporating readily available clinical and ultrasonic features, provides a valuable tool for individualized prediction of extrapelvic metastasis in OC patients. It serves as a practical tool for preoperative risk stratification to guide clinical decision-making.
Keywords: ovarian cancer, extra-pelvic metastasis, ultrasound, nomogram
Introduction
Ovarian cancer (OC) is the ninth most prevalent cancer among women globally, representing roughly 3.4% of all cancer diagnoses and contributing to 4.8% of cancer-related deaths.1,2 Approximately 324,398 women worldwide receive a diagnosis of OC each year, with 206,839 succumbing to the disease.3 The global incidence and fatalities of OC are projected to escalate by 47% and 58%, respectively, by 2045, according to the report of the World Health Organization.4 Furthermore, at the time of initial diagnosis, as many as 70% of OC cases present with advanced-stage disease and distant metastasis.5 A substantial number of OC patients persist in encountering disease relapse and demonstrate resistance to chemotherapy, leading to a mere 49% global 5-year survival rate.6,7 Among these instances, high-grade serous ovarian cancer (HGSOC) emerges as the most frequently diagnosed histological subtype.8 In advanced HGSOC cases, a striking 80% of patients already exhibit metastasis.9 Importantly, the occurrence of extra-pelvic metastases in particular anatomical sites, such as the liver, lungs, and brain, serves as a predictor of unfavorable clinical outcomes.10,11
The prognosis of OC patients is greatly influenced by their initial course of treatment. OC patients with fertility needs in the International Federation of Gynecology and Obstetrics (FIGO) stage I can undergo fertility-sparing surgery.12 Furthermore, an optimal clinical approach involves resecting the tumor and maximizing the reduction of tumor cells at metastatic sites, complemented by chemotherapy or radiation therapy for OC patients.7 However, surgical intervention often becomes challenging or ineffective when patients are accompanied by extra-pelvic metastases. As a result, chemotherapy and targeted medication therapy have emerged as the primary treatment modalities.13 It is worth noting that patients diagnosed with stage III–IV OC who have extra-pelvic metastasis show a much worse prognosis than those with stage I or II disease without extra-pelvic spread.14 Therefore, for all kinds of OC patients, it is crucial to accurately assess their metastases and determine their stage prior to surgery.
Ultrasound (US) is currently the most popular imaging technique used for OC screening and diagnostic assessment.15 Compared with computed tomography (CT) and magnetic resonance imaging (MRI), US offers the benefits of low costs, high repeatability, and no radiation risk. However, the US poses challenges in identifying the characteristic signs of FIGO stage III and IV disease, such as small extra-pelvic peritoneal implants, metastases to retroperitoneal lymph nodes, and small metastatic deposits on the hepatic or splenic surface. Research indicates that thirty percent of patients who received an initial diagnosis of early-stage OC via imaging are ultimately found to have occult metastatic lesions upon pathological examination of retroperitoneal lymph nodes and omental tissue.1 Currently, guidelines from the American College of Radiology for the Ovarian Adnexal Reporting and Data System have gained widespread adoption in clinical practice for risk stratification of ovarian tumors.16 Nevertheless, the system is limited to assessing the malignancy of the ovarian tumors. Currently, there are no definitive clinical or ultrasonic indicators that can indicate or reliably predict the presence of extra-pelvic metastasis of OC. The aim of this study was to delineate the clinical and ultrasonic profiles of OC patients and to elucidate risk factors associated with advanced disease manifesting extra-pelvic metastasis. This can prompt ultrasound physicians and clinicians to conduct more comprehensive examinations, so as to more accurately determine the FIGO stage of patients, which is conducive to individualized treatment and ultimately improves their prognosis.17
Materials and Methods
Study Design
Patients with pathologically confirmed OC who had undergone surgery and US were recruited in this study across three hospitals (The Second Affiliated Hospital of Fujian Medical University, Quanzhou First Hospital, and Chengdu Third People’s Hospital) from March 2016 to July 2025. Preoperative US images and relevant clinical information were obtained in the diagnostic system. Exclusionary criteria included: (1) patients with unclear pathology; (2) cases lacking complete imaging or clinical information; (3) cases with unclear ultrasonic images. Finally, 347 cases were enrolled in our study. They were dichotomized by the status of extra-pelvic metastasis: group A without extra-pelvic metastasis (n=164) and group B with extra-pelvic metastasis (n=183). The ultrasonic parameters were measured. Age, pausimenia, preoperative CA125, and ascites were recorded through the clinical system. Clinical gynecologic oncologists with 20 years of clinical experience determine whether extra-pelvic metastasis has occurred and the final FIGO staging based on medical history, intraoperative conditions, and various auxiliary examinations.
Parameters of Ultrasound
All patients underwent standardized ultrasonography. Ultrasonic testing equipment includes GE-Voluson E10 (GE Medical Systems, Zipf, Austria), GE-Voluson E8 (GE Medical Systems, Zipf, Austria), Mindray Resona I9 (Mindray, Shenzhen, China), Philips IU22 (Philips, Bothell, WA, USA), Philips CX-50 (Philips, Bothell, WA, USA), and Philips A70 (Philips, Bothell, WA, USA). The frequency of the abdominal probe is 3.5 to 6.5 MHZ, and the frequency of the transvaginal probe is 3 to 10 MHZ. All US image features were evaluated by two US experts with over 10 years of diagnostic experience. According to the ultrasonic images, bilateral (Yes/No), multifocal (Yes/No), maximum tumor diameter, the maximum diameter of the largest solid components, the proportion of solid components, ill-defined boundary (Yes/No), Irregular shape (Yes/No), calcification (Yes/No), and separation (Yes/No) were recorded. Moreover, the number of nipples (recorded as “4” when there are more than 3), enhanced echo behind the tumors (Yes/No), acoustic shadow (Yes/No), blood flow score (1= no blood flow; 2= small blood flow; 3= moderate blood flow; 4= very strong blood flow),18 peak systolic velocity (PSV), end-diastolic velocity (EDV) and resistance index (RI) were recorded too.
Statistical Analysis
This study employed R (version 4.2.2) for statistical analysis. Continuous variables were described as mean ± standard deviation if normally distributed, or as median (interquartile range) otherwise. Categorical variables are presented as frequencies (n). Intergroup comparisons for these variables were performed using the Chi-square test or Fisher’s exact test. Multivariate analysis utilizing LASSO logistic regression was applied to the training set to select independent risk factors and to build a nomogram predicting pelvic metastasis. The assessment of model performance was carried out utilizing receiver operating characteristic (ROC) and calibration curves. Furthermore, a decision curve analysis (DCA) was undertaken to establish the clinical utility and net benefit of the predictive model. A two-sided p-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
This study initially identified 383 patients with OC. Following the exclusion of 9 cases with unclear pathology, 19 with incomplete imaging or clinical data, and 8 with poor-quality ultrasonic images, a final cohort of 347 patients was included for analysis. And they were divided into two groups according to whether extra-pelvic metastasis occurred: group A without extra-pelvic metastasis (n=164) and group B with extra-pelvic metastasis (n=183) (Figure 1). The total patient population was randomly split between a training set (70%) and a validation set (30%).
 |
Figure 1 Flowchart of patient screening in this study. Abbreviation: OC, ovarian cancer. |
The baseline feature table presents information on various characteristics in the training cohort and the test cohort (Table 1). The median age was comparable between the two cohorts, with values of 53.0 (IQR 45.0–61.0) years in the training set and 52.0 (IQR 45.0–62.5) years in the internal test set. There were no significant differences in age, FIGO, pausimenia, ascites, CA125, bilateral, multifocal, maximum tumor diameter, maximal diameter of the largest solid part, proportion of solid components, ill-defined boundary, irregular shape, calcification, separation, number of papillations, enhanced echo behind the tumors, acoustic shadow, Blood flow score, PSV, EDV and RI between training set and internal test set (P = 0.909, 0.616, 0.626, 0.642, 0.812, 0.406, 0.620, 0.823, 0.744, 0.470, 0.681, 0.566,0.319, 0.733, 0.750, 0.217, 0.499, 0.669, 0.385, 0.151, 0.640, respectively). Overall, these results indicate that the baseline characteristics were homogeneous between the training and internal test sets, supporting the validity of the set split for subsequent predictive modeling.
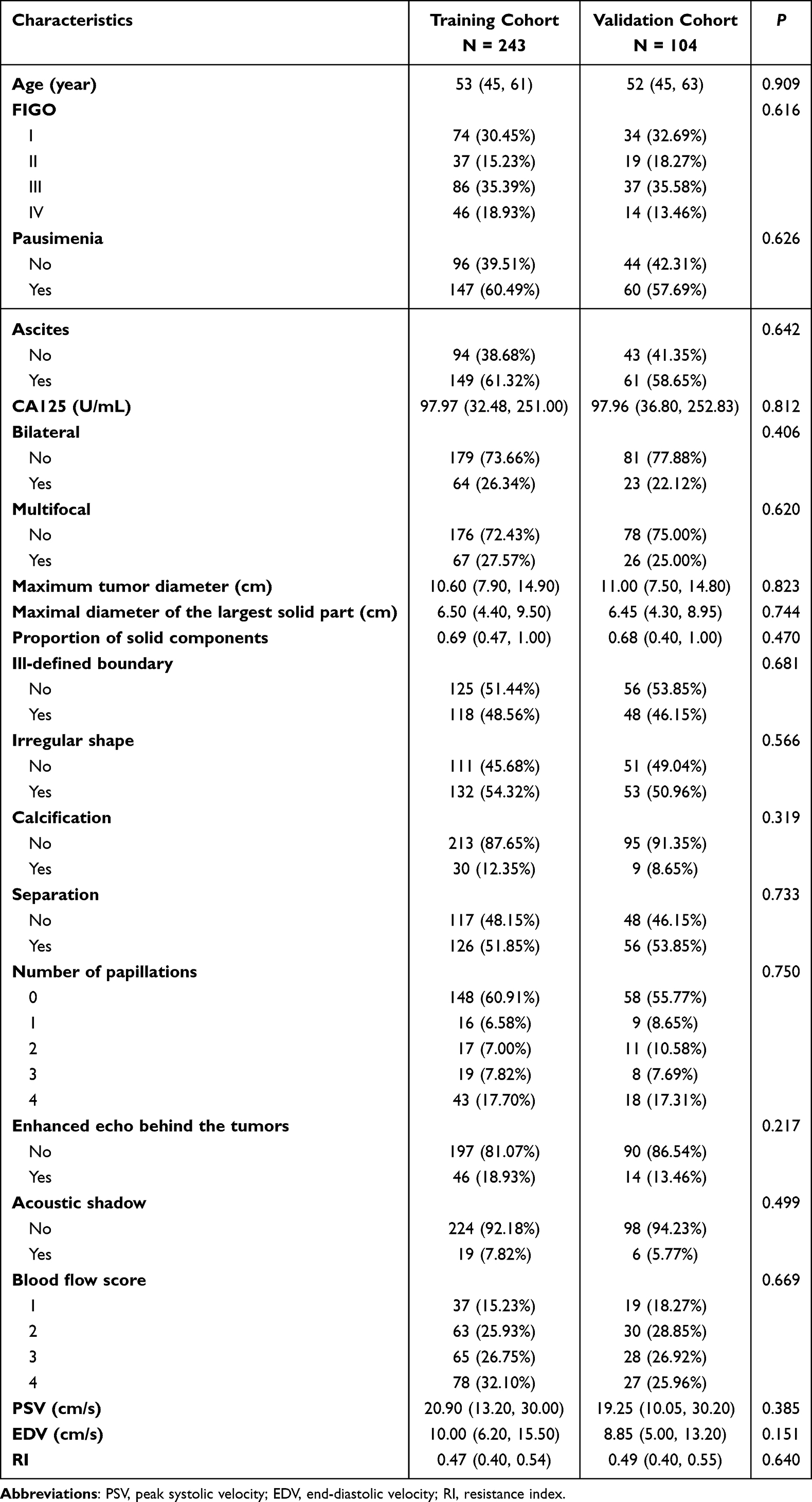 |
Table 1 Clinical and Ultrasonic Characteristics of Patients |
Screening of Indicators for Extra-Pelvic Metastasis
The patient cohort was randomly partitioned into training and validation sets at a ratio of 7:3. Four independent risk factors, ascites, maximum tumor diameter, ill-defined boundary, and blood flow score (P<0.05), were screened using LASSO in the training set. A coefficient profile is plotted in Figure 2A. The respective plot of the cross-validated errors from the LASSO regression is depicted in Figure 2B. The most penalized and simplest model, which had a cross-validated error within one standard error of the best, comprised 4 variables. The coefficients of the Lasso regression analysis are shown in Table S1. The corresponding risk factors were subjected to univariate and multivariate analysis, the results of which are summarized in Table 2.
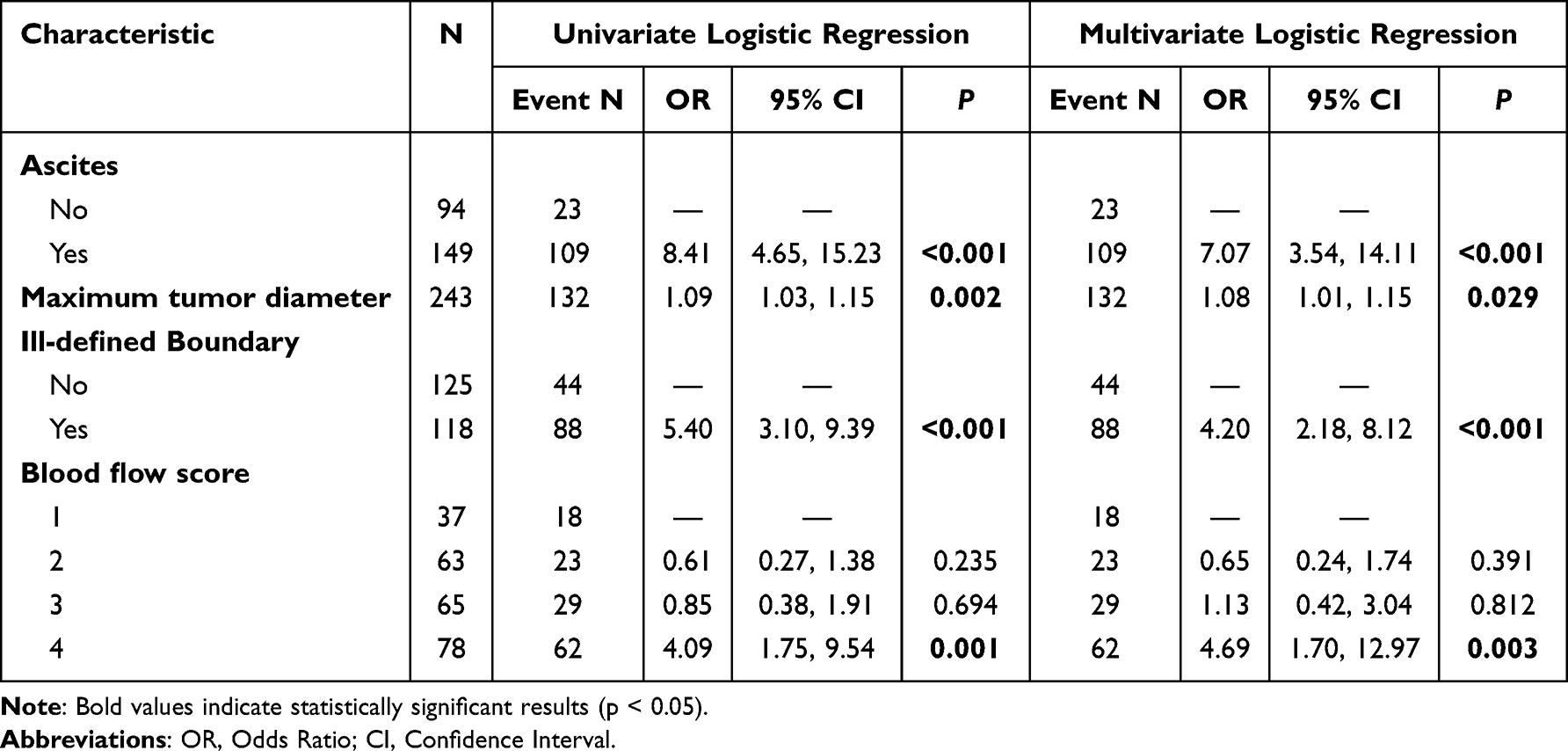 |
Table 2 Results of Multivariate Logistic Regression of Risk Factors in the Training Set |
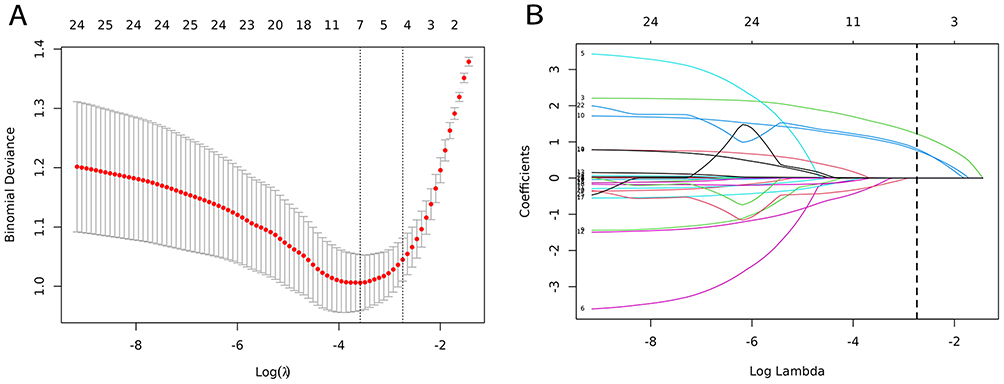 |
Figure 2 LASSO regression and tenfold cross-validation were used to select the features. (A) Optimal feature selection of cross-validation. (B) LASSO coefficient profiles of the features. Abbreviation: LASSO, least absolute shrinkage and selection operator. |
ROC Curve Analysis of Individual Predictors
ROC curves demonstrated robust predictive performance of the model across both the training and validation sets for pelvic metastasis. The result of the ROC curve showed that the area under the curve (AUC) for ascites was 0.733 (95% CI: 0.677 ~ 0.788), for maximum tumor diameter was 0.626 (95% CI: 0.555–0.697), for ill-defined boundary was 0.698 (95% CI: 0.640–0.756), and for blood flow score level 4 was 0.687 (95% CI: 0.623–0.751) (Figure 3 and Table 3).
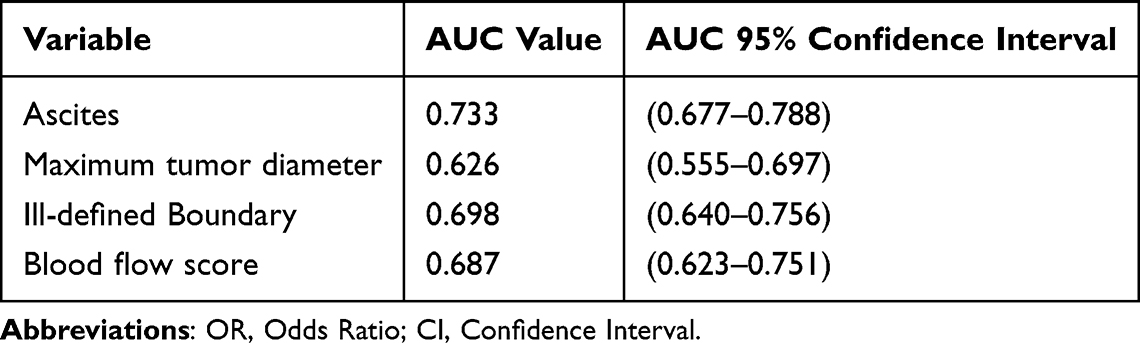 |
Table 3 AUC Values and 95% Confidence Intervals for Variables |
 |
Figure 3 ROC curves of selected predictors. Abbreviation: AUC, area under the curve. |
Construction and Validation of a Predictive Nomogram
In the nomogram, each parameter predictive of extra-pelvic metastasis in OC patients is allocated a specific score. The summative score of all indices contributes to estimating the probability of extra-pelvic metastasis (Figure 4). Figure 5 shows two examples of evaluation by the nomogram in OC patients. The model achieved AUC values of 0.860 and 0.865 in the training set and validation set, respectively (Figure 6). The calibration plots of the nomogram across the various cohorts are presented in Figure 7, illustrating a strong correlation between the observed and predicted extra-pelvic metastasis. The results indicate that the original nomogram remains valid for application in the validation sets, and the calibration curve of this model closely approximates the ideal curve, suggesting that the predicted outcomes align well with the actual observations. The classification accuracy across various risk thresholds in the training set is summarized in Table 4. Furthermore, the model demonstrated good calibration, with its curve aligning closely to the ideal 45° line, and its DCA curve yielding a positive net benefit across a range of thresholds, as depicted in Figure 8.
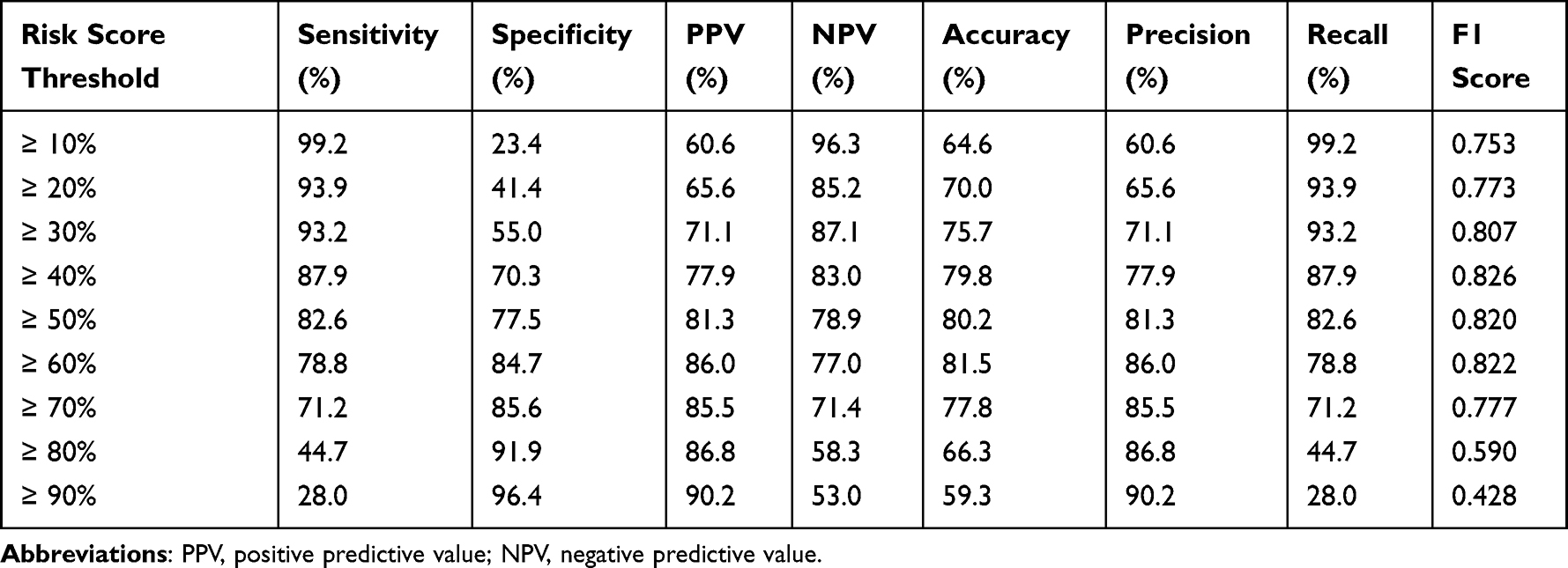 |
Table 4 Classification Accuracy for Prediction at Different Risk Cutoff Points for the Model in the Training Set |
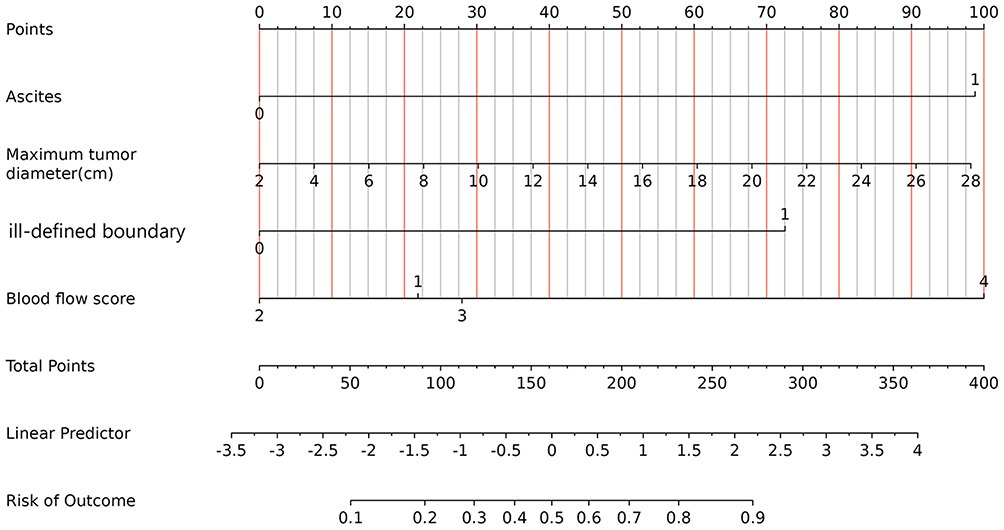 |
Figure 4 Nomogram for predicting extra-pelvic metastasis in patients with OC. |
 |
Figure 5 The evaluation of the model in patients with OC. (A and B): a 47-year-old patient with OC. The tumor was located on the right ovary. It was 83mm, with a defined boundary, irregular shape, visible solid component and separation, no blood flow signal (blood flow score grade 1), and no ascites. According to the nomogram, the risk of extra-pelvic metastasis in this patient was < 10%. The patient was eventually diagnosed with HGSOC, which was not accompanied by extra-pelvic metastasis; (C and D) a 49-year-old patient with OC. The tumor was located on the right ovary. It was 88mm, with an ill-defined boundary, irregular shape, mostly solid components, abundant blood flow signal (blood flow score grade 4), and no ascites. According to the nomogram, the risk of extra-pelvic metastasis in this patient was 80%-90%. The patient was eventually diagnosed with HGSOC, which was accompanied by extra-pelvic metastasis. The green and white boxes in (B and D), respectively, mark the regions of interest for color Doppler flow signal measurement. |
 |
Figure 6 ROC curves of the training set and validation set. |
 |
Figure 7 Calibration curves of a nomogram for predicting extra-pelvic metastasis in patients with OC. (A) Training set. (B) Validation set. The Ideal line represents the reference line. The Apparent curve represents the fit of the predicted value to the actual value. The Bias-corrected curve represents the fit after correction. There are only small deviations between the Apparent curve and the Ideal line, and the model shows great predictive performance. |
 |
Figure 8 DCA of the nomogram for screening for extra-pelvic metastasis in patients with OC in the training set (A) and validation set (B). The DCA curve is above None and All, which means that the model is acceptable. |
Discussion
In this study, we performed a comprehensive analysis of patients with OC at three distinct centers to develop a predictive model utilizing clinical and US features. The model aims to forecast the occurrence of extra-pelvic metastasis in patients with OC. Our analysis revealed four independent risk factors: ascites, maximum tumor diameter, ill-defined boundary, and blood flow score level 4, and established a nomogram based on the four factors. Both the training and validation sets demonstrated high AUC values, and the calibration curves, as well as the DCA curves, demonstrate robust model performance.
OC, a prevalent gynecologic malignancy, poses a serious threat to women’s health. 70% of patients with OC are already at an advanced stage at initial diagnosis and are accompanied by extra-pelvic metastases, which results in a lower 5-year survival rate for OC.19 The typical modes of metastasis for OC encompass peritoneal dissemination, hematogenous spread, lymphatic metastasis, and neural-associated metastasis. Among these, peritoneal and lymphatic metastases are the most frequently observed.10 Clinically, different surgical methods are often adopted for OC patients according to different FIGO stages. Gynecologists usually decide whether to use full-stage surgery or cytoreductive surgery (CRS) combined with chemotherapy based on the status and location of the metastasis.13,20 Furthermore, studies have shown that one of the most critical prognostic factors in OC patients undergoing cytoreductive surgery is whether all visible tumors are removed during cytoreductive surgery (complete CRS).21 The tumor can be deemed to have achieved satisfactory reduction if there is no residual tumor or the diameter of the residual tumor is less than 1cm, resulting in improved progression-free survival and overall survival for these patients compared to those with larger residual tumors.22 Therefore, it is crucial to determine the presence and size of extra-pelvic metastasis before surgery. Secondly, the feasibility of conducting a complete CRS hinges on both the degree of peritoneal involvement and the engagement of vital structures outside the pelvis.23 Pre-surgical confirmation of the metastasis status and location can potentially minimize the duration and trauma associated with surgical exploration. In conclusion, a precise diagnosis of tumor extent and metastatic sites in OC patients before surgery is pivotal for devising an effective preoperative surgical plan and enhancing patient prognosis.
At present, the US is the preferred OC imaging method in physical screening and clinical diagnosis, which can evaluate tumor size, proportion of cystic solid components, boundaries, margins, blood perfusion, and metastasis.15 CT and MRI are often used as further evaluation methods after US. The specificity of CT in the diagnosis of neoplastic abdominal lymph nodes is 89%, but the sensitivity is only 41%, which is a serious underestimate.24,25 Secondly, the presence of peritoneal metastases is also consistently underreported by CT.26 In conclusion, assessing the nature of soft tissue using CT poses challenges, and there are inherent radiation risks associated with its use. Likewise, MRI encounters difficulties in diagnosing malignant abdominal lymph nodes, with a sensitivity of 77% and a specificity of 91%.27 Compared with CT and MRI, US has the advantages of non-radiation, economy, and convenience. Furthermore, previous studies have demonstrated that US demonstrates superiority over MRI and CT in the evaluation of global peritoneal cancer (0.87, 0.86, and 0.77, respectively). In evaluating deep wall infiltration of rectosigmoid, the accuracy and sensitivity of US (93% and 100%) were superior to MRI (83% and 75%) and CT (84% and 88%).28 However, the US is prone to missed diagnosis when identifying smaller extrascites in FIGO stage III–IV, such as small retroperitoneal lymph node metastases. Therefore, in this study, we explored clinical and ultrasonic characteristics to determine whether they can predict extra-pelvic metastasis in patients with OC, which may prompt the sonographer to more thoroughly examine the extra-pelvic sites.
In our study, ascites emerged as one of the independent factors screened to forecast the occurrence of extrapelvic metastasis in OC. Among patients with advanced OC, ascites frequently manifests, potentially resulting from the transfer of fluid to the peritoneum, thereby stimulating excessive serous fluid production. Concurrently, the presence of ascites facilitates the dissemination of cancer cells to other organs.29,30 The maximum tumor diameter in patients with extra-pelvic metastasis was significantly larger than that in patients without extra-pelvic metastasis (125 ± 50mm vs 104 ± 50mm, P=0.001) in the training set in this study, which was in accordance with the findings of Yang et al.31 In their study, the maximum tumor diameter in OC patients with lymph node metastasis was larger than that in the group without lymph node metastasis (81.67±49.22 vs 110.31±49.02, P<0.001), and was an independent predictor of lymph node metastasis in OC patients. Furthermore, research has indicated that the maximum tumor diameter independently predicts the efficacy of neoadjuvant chemotherapy in advanced OC patients (P<0.05),32 as well as the risk of platinum resistance in OC patients (P<0.05).33
Ill-defined boundary coupled with abundant blood flow constitutes a prominent US feature in the diagnosis of OC. In our study, both ill-defined boundary and blood flow score level 4 served as predictors within our model. The unclear tumor boundaries may indicate high aggressiveness towards surrounding tissues. Additionally, blood transfer represents a significant mode of OC metastasis. Numerous studies have revealed the presence of circulating tumor cells in the bloodstream in OC patients, which may contribute to the dissemination and correlate with an unfavorable prognosis.34 When masses were detected with copious blood flow in OC patients by US, particularly when reaching a score of 4, it prompts a more comprehensive examination by doctors to identify any extra-pelvic metastases. Such thorough assessments can greatly benefit the treatment and prognosis of patients. When US observation shows that the blood flow of the mass in OC patients is abundant and reaches a score of 4, it suggests that doctors should more comprehensively check whether the patient is accompanied by extra-pelvic metastasis, which will benefit the treatment and prognosis.
In addition to the above risk factors, we should note that the median age of onset in this set was relatively young (53 years in the training set and 52 years in the internal test set), which is consistent with the demographic profile of the Chinese population. Studies indicate that the median age of diagnosis for OC patients in China is 53 years,35 notably younger than the median age of approximately 63 years in Western populations.36 This discrepancy is largely attributed to a higher proportion of younger-onset cases and a distinct distribution of pathological subtypes in China. We also developed a nomogram to predict the risk of extra-pelvic metastasis of OC based on the independent predictors: ascites, maximum tumor diameter, ill-defined boundary, and blood flow score level 4. The model achieved AUC values of 0.860 and 0.865 in the training and validation sets, respectively. The model developed from clinical and ultrasonic characteristic parameters can predict the status of OC patients with extra-pelvic metastasis accurately. These indicators can be obtained during the preoperative examination of the patient and can prompt the doctor to conduct a careful examination of other organs outside the pelvis, which will facilitate the confirmation of FIGO staging and the customization of personalized treatment plans for OC patients, thereby improving the prognosis of patients.
Several limitations of this study should be considered. Firstly, the research employs a retrospective design, and there may be inherent biases within the included population. Prospective studies are necessary to validate our findings. Secondly, this study only analyzed the relatively common US image characteristics of OC patients. Radiomics could be employed to explore deeper image features and identify new US-based predictors for extra-pelvic metastasis in OC patients in future research. Lastly, further research and validation are required to establish the external validity and its broader applicability in clinical practice.
Conclusion
The model developed by clinical and ultrasonic characteristic parameters empowers doctors to more accurately identify the III–IV stage OC patients with extra-pelvic metastases, thereby facilitating the formulation of tailored surgical plans, optimizing preoperative decision-making regarding neoadjuvant therapy, and ultimately aiming to improve patient prognosis.
Data Sharing Statement
The data from the current study are available from the corresponding author, Guorong Lyu, on reasonable request.
Ethical Approval and Informed Consent
This study was performed in accordance with the Declaration of Helsinki, and approved by the ethics committee of the Second Affiliated Hospital of Fujian Medical University (IRB No. 2024323). The requirement for written informed consent was waived due to the retrospective nature of the study. All patient data were anonymized and handled with strict confidentiality to protect participant privacy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or n all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Special Fund for Doctoral Supervisors of The Second Affiliated Hospital of Fujian Medical University (no. 2022BD1005).
Disclosure
Yanli Wang and Weihong Lin are co-first authors for this study. The authors declare that they have no conflicts of interest in this work.
References
1. Caruso G, Weroha SJ, Cliby W. Ovarian Cancer: a Review. JAMA. 2025;334(14):1278. doi:10.1001/jama.2025.9495
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
3. Yang Y, Huang Q, Xiao Z, et al. Nanomaterial-based biosensor developing as a route toward in vitro diagnosis of early ovarian cancer. Mater Today Bio. 2022;13:100218. doi:10.1016/j.mtbio.2022.100218
4. Lliberos C, Richardson G, Papa A. Oncogenic Pathways and Targeted Therapies in Ovarian Cancer. Biomolecules. 2024;14(5):585. doi:10.3390/biom14050585
5. Zhao C, Xiong K, Zhao F, Adam A, Li X. Glycosylation-related genes predict the prognosis and immune fraction of ovarian cancer patients based on weighted gene coexpression network analysis (WGCNA) and machine learning. Oxid Med Cell Longev. 2022;2022(1):3665617. doi:10.1155/2022/3665617
6. Terp SK, Stoico MP, Dybkær K, Pedersen IS. Early diagnosis of ovarian cancer based on methylation profiles in peripheral blood cell-free DNA: a systematic review. Clin Clin Epigenet. 2023;15(1):24. doi:10.1186/s13148-023-01440-w
7. Gaillard S, Lacchetti C, Armstrong DK, et al. Neoadjuvant chemotherapy for newly diagnosed, advanced ovarian cancer: ASCO guideline update. J Clin Oncol. 2025;43(7):868–891. doi:10.1200/JCO-24-02589
8. Kordowitzki P, Lange B, Elias KM, et al. Transforming treatment paradigms: focus on personalized medicine for high-grade serous ovarian cancer. CA Cancer J Clin. 2025;75(5):436–460. doi:10.3322/caac.70008
9. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
10. Bayraktar E, Chen S, Corvigno S, Liu J, Sood AK. Ovarian cancer metastasis: looking beyond the surface. Cancer Cell. 2024;42(10):1631–1636. doi:10.1016/j.ccell.2024.08.016
11. Tadić V, Zhang W, Brozovic A. The high-grade serous ovarian cancer metastasis and chemoresistance in 3D models. Biochim Biophys Acta Rev Cancer. 2024;1879(1):189052. doi:10.1016/j.bbcan.2023.189052
12. González-Martín A, Harter P, Leary A, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(10):833–848. doi:10.1016/j.annonc.2023.07.011
13. Konstantinopoulos PA, Matulonis UA. Clinical and translational advances in ovarian cancer therapy. Nat Cancer. 2023;4(9):1239–1257. doi:10.1038/s43018-023-00617-9
14. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
15. Strachowski LM, Jha P, Chawla TP, et al. O-RADS for ultrasound: a user’s guide, from the AJR special series on radiology reporting and data systems. AJR Am J Roentgenol. 2021;216(5):1150–1165. doi:10.2214/AJR.20.25064
16. Andreotti RF, Timmerman D, Strachowski LM, et al. O-RADS US risk stratification and management system: a consensus guideline from the ACR ovarian-adnexal reporting and data system committee. Radiology. 2020;294(1):168–185. doi:10.1148/radiol.2019191150
17. Wentzensen N, Ring K, Erickson BK, et al. Ovarian cancer risk prediction: a clinical epidemiology perspective. Am J Epidemiol. 2025;194(5):1182–1191. doi:10.1093/aje/kwae293
18. Chen H, Yang BW, Qian L, et al. Deep learning prediction of ovarian malignancy at US compared with O-RADS and expert assessment. Radiology. 2022;304(1):106–113. doi:10.1148/radiol.211367
19. Eisenhauer EA. Real-world evidence in the treatment of ovarian cancer. Ann Oncol. 2017;28(suppl_8):viii61–viii65. doi:10.1093/annonc/mdx443
20. Kumar KP, Madhusoodanan M, Pangath M, Menon D. Innovative landscapes in intraperitoneal therapy of ovarian cancer. Drug Deliv Transl Res. 2025;15(6):1877–1906. doi:10.1007/s13346-024-01765-w
21. Shan Y, Jin Y, Pan L. Hepatic metastases in ovarian cancer. Hepatobiliary Surg Nutr. 2022;11(6):924–926. doi:10.21037/hbsn-22-484
22. Shi Y, Dai M, Zhang Y, Qi Y, Li Z, Cai H. Residual tumor diameter predicts progression after primary debulking surgery of ovarian clear cell carcinoma (OCCC): clinicopathologic study of stage II-IV OCCC patients from a single institution. Cancer Manag Res. 2021;13:2215–2222. doi:10.2147/CMAR.S293677
23. El Asmar A, Pop F, Helou EE, et al. Prognostic value of peritoneal scar-like tissue in patients with peritoneal metastases of ovarian origin presenting for curative-intent cytoreductive surgery. World J Surg Oncol. 2023;21(1):269. doi:10.1186/s12957-023-03153-z
24. Kim TH, Lim MC, Kim SI, Seo SS, Kim SH, Park SY. Preoperative prediction of cardiophrenic lymph node metastasis in advanced ovarian cancer using computed tomography. Ann Surg Oncol. 2016;23(4):1302–1308. doi:10.1245/s10434-015-5015-0
25. Widschwendter P, Blersch A, Friedl TWP, et al. CT scan in the prediction of lymph node involvement in ovarian cancer - a retrospective analysis of a tertiary gyneco-oncological unit. Geburtshilfe Frauenheilkd. 2020;80(5):518–525. doi:10.1055/a-1079-5158
26. van ‘t Sant I, Engbersen MP, Bhairosing PA, et al. Diagnostic performance of imaging for the detection of peritoneal metastases: a meta-analysis. Eur Radiol. 2020;30(6):3101–3112. doi:10.1007/s00330-019-06524-x
27. Engbersen MP, Van Driel W, Lambregts D, Lahaye M. The role of CT, PET-CT, and MRI in ovarian cancer. Br J Radiol. 2021;94(1125):20210117. doi:10.1259/bjr.20210117
28. Fischerova D, Pinto P, Burgetova A, et al. Preoperative staging of ovarian cancer: comparison between ultrasound, CT and whole-body diffusion-weighted MRI (ISAAC study). Ultrasound Obstet Gynecol. 2022;59(2):248–262. doi:10.1002/uog.23654
29. Zheng X, Wang X, Cheng X, et al. Single-cell analyses implicate ascites in remodeling the ecosystems of primary and metastatic tumors in ovarian cancer. Nat Cancer. 2023;4(8):1138–1156. doi:10.1038/s43018-023-00599-8
30. Qu Q, Liu L, Cui Y, Chen Y, Wang Y, Wang Y. Exosomes from human omental adipose-derived mesenchymal stem cells secreted into ascites promote peritoneal metastasis of epithelial ovarian cancer. Cells. 2022;11(21):3392. doi:10.3390/cells11213392
31. Yang Y, Ye X, Zhou B, et al. Nomogram for predicting lymph node metastasis in patients with ovarian cancer using ultrasonography: a multicenter retrospective study. BMC Cancer. 2023;23(1):1121. doi:10.1186/s12885-023-11624-5
32. Huang J, Du D, Chen H, et al. Clinical value of serum tumor markers in assessing the efficacy of neoadjuvant chemotherapy in advanced ovarian cancer: single-center prospective clinical study. Front Oncol. 2024;14:1399502. doi:10.3389/fonc.2024.1399502
33. Li R, Xiong Z, Ma Y, et al. Enhancing precision medicine: a nomogram for predicting platinum resistance in epithelial ovarian cancer. World J Surg Oncol. 2024;22(1):81. doi:10.1186/s12957-024-03359-9
34. Yousefi M, Dehghani S, Nosrati R, et al. Current insights into the metastasis of epithelial ovarian cancer - hopes and hurdles. Cell Oncol Dordr. 2020;43(4):515–538. doi:10.1007/s13402-020-00513-9
35. Shen F, Chen S, Gao Y, Dai X, Chen Q. The prevalence of malignant and borderline ovarian cancer in pre- and post-menopausal Chinese women. Oncotarget. 2017;8(46):80589–80594. doi:10.18632/oncotarget.20384
36. Kotsopoulos J, Gronwald J, Karlan B, et al. Age-specific ovarian cancer risks among women with a BRCA1 or BRCA2 mutation. Gynecol Oncol. 2018;150(1):85–91. doi:10.1016/j.ygyno.2018.05.011
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Risk Factors for Urinary Tract Infection in Ovarian Cancer Patients After Cytoreductive Surgery and Construction of a Nomogram Model
He M, Li J, Huang L, Liang F
International Journal of Women's Health 2025, 17:5035-5044
Published Date: 2 December 2025