Back to Journals » Risk Management and Healthcare Policy » Volume 15
A Pre-Generation of Emergency Reference Plan Model of Public Health Emergencies with Case-Based Reasoning
Received 21 August 2022
Accepted for publication 2 December 2022
Published 15 December 2022 Volume 2022:15 Pages 2371—2388
DOI https://doi.org/10.2147/RMHP.S385967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Danyang Ru, Haoyu Wen, Yuntao Zhang
School of Economics and Management, Xidian University, Xi’an, Shaanxi, People’s Republic of China
Correspondence: Haoyu Wen, Email [email protected]
Background and Purpose: In the early 21st century, the coronavirus alone has ravaged the world three times. Public health emergencies have caused a tremendous negative impact on public health, daily life, and global economic development, for having the characteristics of complexity and great harm. To tackle these problems, a pre-generation of emergency reference plan model of public health emergencies is proposed to better deal with the outbreak and spread of public health events.
Methods: The method is divided into three stages. First, the modified SEIR model is used to predict the attribute values of the target case. Then, the similar case sets are extracted and filtered by calculating the similarity through the cross-efficiency evaluation method with the parallel system. Finally, the multi-stage emergency effect evaluation model is conducted so that the emergency plan with the best response effect at this stage can be made for reference.
Results: We collected 25 typical events of COVID-19 that occurred in 11 cities in China as historical case bases and target cases, respectively. The result of the experiment verified the feasibility and effectiveness of the proposed method.
Conclusion: This paper presents a new perspective on making a public health emergency plan, which could improve the decision-making accuracy and efficiency, maximize the emergency effect and save precious time for emergency response. This model can provide rapid decision supports for decision-making for public services such as government departments, centers for disease control, medical emergency centers and transport authorities, etc.
Keywords: public health emergencies, case-based reasoning, data envelopment analysis, modified SEIR model, life cycle model
Introduction
Public health emergencies refer to major infectious diseases, unexplained diseases, major food poisoning, and occupational poisoning that occurs suddenly and causes severe damage to the physical and mental health of the public, as well as those caused by natural disasters, accident disasters or social security events. These seriously affect the physical and psychological health of people. In recent years, there have been frequent public health events around the world, such as Severe Acute Respiratory Syndrome (SARS), Avian Influenza, Middle East Respiratory Syndrome (MERS), Influenza A (H1NI), and Coronavirus Disease 2019 (COVID-19) that has been raging since the end of 2019.1 These public health emergencies have had a significant negative impact on people’s health and everyday life. COVID-19 is the most severe infectious disease pandemic in the world in a century. It is also a major public health emergency with the fastest spread, the widest infection range, and the most challenging prevention and control.2 At the same time, the epidemic has also profoundly exposed many shortcomings in the decision-making methods and emergency plans for responding to public health emergencies.3
Whether major public health emergencies are handled appropriately, emergency decision support is critical.4 Untimely access to information, limited knowledge and case reserves, difficulty in judging the development trend, and increasing complexity and difficulty of evidence-based decision-making5 are also tricky problems that are difficult to solve in the face of major public health emergencies around the world. At the same time, a common problem faced in the decision-making process of public health emergencies is that decision-makers cannot collect all relevant information within a limited time.6 If an ideal decision-making result were to be obtained by collecting all relevant decision information, the implementation effect of the emergency plan would be greatly reduced, for the best implementation time has been missed. The occurrence of public health emergencies is uncertain, so it is necessary to prepare in advance, strengthen strategic planning, and ensure sufficient material reserves. Conversely, if an emergency occurs, it will be difficult for decision-makers to ensure the scientificity, rationality, and efficiency of decisions made in a short time. To sum up, how to pre-generate effective emergency plans and measures for the next period based on available information in a short time is an essential issue with great practical significance and research value.
The methods that have been used to deal with emergency decision-making include group decision-making (GDM),7 D-S evidence theory,8 multi-objective decision,9 model based on decision-tree,10 Prospect theory,11 evolutionary game,12 the fault tree analysis (FTA) based method,13,14 and case-based reasoning (CBR),15 etc. CBR has the widest application and significant advantages among the numerous emergency decision-making methods. CBR is a problem-solving paradigm derived from artificial intelligence, which includes the following four steps: retrieve, reuse, revise and retain.16 CBR solves problems by imitating the thinking process of human reasoning, which can effectively apply previous experience to provide decision-making reference for current incident cases. Moreover, CBR is an incremental learning model, that is, throughout successive learning processes, the knowledge domain that the system can handle is expanding, and the generated emergency decision-making scheme is gradually improving.
The application of CBR in the field of emergency decision-making is very multitudinous. A large number of examples show that CBR is suitable for solving related problems in this field. For instance, Raskob et al16 applied CBR to the analytical platform to support the management of nuclear events in different accident phases. Zhang et al17 designed a system framework for the traffic monitoring and management system according to its characteristics and provided a traffic emergency aid decision-making method by integrating the CBR specific to the traffic emergencies. Wang et al18 analyzed the scenario evolution mechanism of environmental emergencies and constructed an emergency decision-making model for environmental emergencies based on CBR. Liao et al15 designed the CBR-Oil Spill Response and Preparedness System as an emergency reference for environmental emergencies. Shao et al19 proposed a demand prediction method called intuitionistic fuzzy case-based reasoning (IFCBR) for the characteristics of relief supply demand prediction of the environment. Yao et al20 proposed a dynamic geological disaster emergency plan selection scheme based on CBR. Based on the theory of geographical CBR, Li et al21 presented an expression framework of urban emergency planning cases based on integrating subjective humanistic factors and objective geographical environment factors. Wang et al22 introduced risk source identification and emergency classification and developed an emergency decision model based on scenario retrieval and case-based reasoning. By fully mining the spatial features, Zhao et al23 proposed a novel spatial case-based reasoning method for landslide risk assessment.
Most of the current research on CBR in the field of emergency decision-making focuses on improving the retrieval efficiency of similar cases,24–28 optimizing the case base,29–32 and combining with various intelligent algorithms.33–37 Although the above methods have advanced and refined the application of CBR in emergency decision-making, there are many problems such as low retrieval accuracy, complex retrieval steps, and long response time. And emergencies such as earthquake disasters and fires have the characteristics that once these occur, the negative impact will reach a peak immediately. Therefore, their emergency response focuses on the follow-up disaster relief work and the resettlement of victims. Yet the public health emergency has different peculiarities. When the authorities respond to the event, it is often still in an early stage of development,38 so the follow-up emergency response measures are critical to put the brakes on the deterioration of the epidemic. At the same time, researchers often ignore the characteristics such as rapid evolution39 and the difficulty of judging the development trend by personal experience. So, the situation changed dramatically when decision-makers developed emergency plans for the current phase. This will inevitably lead to a lag in emergency decision-making, so the selected emergency scheme will not be reasonable and effective. In the end, the critical prevention and control timing will be delayed, and the situation will further deteriorate. Therefore, formulating scientific and accurate prevention and control plan40 in advance by predicting the development trend of public health emergencies is imperative for further control of the development of the epidemic. The development of public health emergencies is phased with different characteristics in different phases. Hence, its decision-making problems and goals will also change with the evolution of the situation. Consequently, the emergency effect can be significantly improved by judging the stage of the current epidemic, giving priority to solving the critical problems in this stage, and taking corresponding means and emergency measures.
To address these problems, we propose a method to pre-generate an emergency plan for public health emergencies based on CBR, combined with the modified susceptible-exposed-infected-removed (SEIR) model and life cycle theory. First, the modified SEIR model is used to predict the attribute values of the target case. Then, the DEA model for parallel system cross-efficiency evaluation model is used to retrieve similar case sets. Finally, we build the multi-stage emergency effect evaluation model to calculate the implementation effect score of similar cases. The emergency plan of the effective similar historical case with the highest score is extracted as an emergency reference plan for the target case. The flow chart is shown in Figure 1.
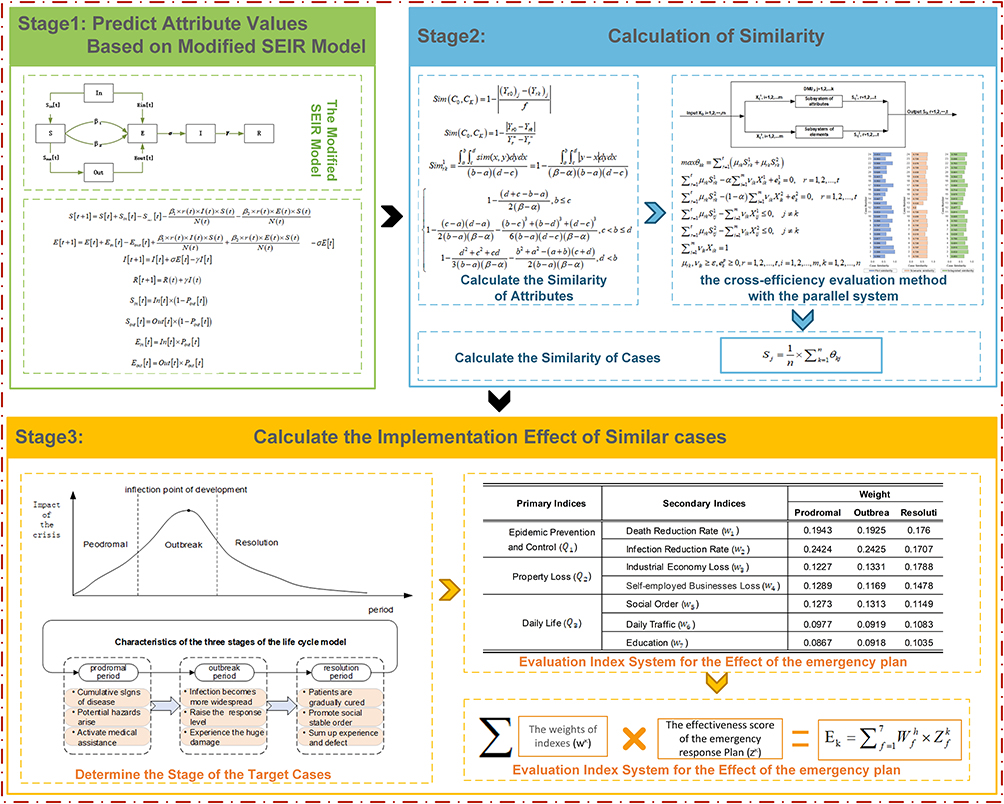 |
Figure 1 Decision-making Framework Model of Public Health Emergencies. |
The Problem Description
In the study on making public health emergency references, a case usually consists of three parts: scenario description, emergency plans, and the results of plan implementation. Since the high complexity and individual differences of public health emergencies, it is difficult to retrieve cases with high similarity and validity for application. Recent studies have shown that emergency decision support should be based on the scenario, and the key to solving the difficulty of case retrieval is to transform case-based reasoning into scenario-based reasoning. At the scenario level, there are similar scenarios even between two different types of public health emergencies. For example, major infectious disease outbreaks and unexplained mass diseases involve a scenario in which there is an urgent need to isolate the incidence population from this scenario.
Therefore, the representation of emergency cases in this paper uses the multi-dimensional situation space representation model,41 and the scenario description is divided into two parts: plot and situation. A plot, consisting of attributes, refers to a segment that describes a real case. It presents detailed information about the time and space of a case. The situation, the core of a case, can show the development process of emergency events composed of elements.
To sum up, the basic symbols for emergency cases are stipulated as follows:
 represents the historical case set of public health emergencies in the emergency case database, and
represents the historical case set of public health emergencies in the emergency case database, and  is the target emergency case.
is the target emergency case.  denotes the set of the attributes, in which
denotes the set of the attributes, in which  represents the value of the rth attribute with regard to emergency case
represents the value of the rth attribute with regard to emergency case  . Let
. Let  be a set of elements, in which
be a set of elements, in which  represents the value of the rth element with regard to emergency case
represents the value of the rth element with regard to emergency case  .
.  denotes the set of the attribute similarity, in which
denotes the set of the attribute similarity, in which  represents the value of the kth attribute similarity with regard to emergency case
represents the value of the kth attribute similarity with regard to emergency case  .
.  represents the set of elements similarity, in which
represents the set of elements similarity, in which  represents the value of the rth element similarity with regard to emergency case
represents the value of the rth element similarity with regard to emergency case  .
.  is the weight vector of the attributes or elements, where
is the weight vector of the attributes or elements, where  denotes the weight of the rth attribute or element with regard to emergency case
denotes the weight of the rth attribute or element with regard to emergency case  .
.  represents the set of evaluation indicators, in which
represents the set of evaluation indicators, in which  denotes the value of the fth indicator with regard to emergency case
denotes the value of the fth indicator with regard to emergency case  . Let
. Let  represents the weight vector of evaluation indicators, where
represents the weight vector of evaluation indicators, where  is the value of the fth indicator in the hth stage.
is the value of the fth indicator in the hth stage.
Methods
Stage 1: Predict Attribute Values Based on Modified SEIR Model
Unlike other disaster events, public health emergencies have the characteristics of long duration, fast evolution and severe impact. Preparedness ensures success and unpreparedness spells failure. If key attributes of public health emergencies are not predicted timely, the resulting emergency reference plans may not apply to the current scenario, thereby delaying critical decision-making opportunities. Therefore, forecasting the development trend of the epidemic is crucial for making practical prevention and control measures, controlling the development of the epidemic, and curbing the expansion of its adverse effects. The modified SEIR model42 is a relatively recognized method for predicting the development trend of the epidemic, so this method will be used to predict the values of related attributes.
The original SEIR model assumes that the number of susceptible populations is constant, but in practice, this number changes dynamically due to the flow of people. So we modified it to account for a dynamic Susceptible  and Exposed
and Exposed  population state by introducing the move-in, I
population state by introducing the move-in, I and move-out,
and move-out,  parameters.42 This model is presented in Figure 2.
parameters.42 This model is presented in Figure 2.
 |
Figure 2 The Modified SEIR Model. |
The modified SEIR model is given by:








We assume that latent  population is asymptomatic but infectious, and
population is asymptomatic but infectious, and  refers to the symptomatic and infectious population. Here,
refers to the symptomatic and infectious population. Here,  is the number of susceptible people in a city.
is the number of susceptible people in a city.  refers to the number of exposed people.
refers to the number of exposed people.  is the number of infected people in a city.
is the number of infected people in a city.  is the number of the recovery or death.
is the number of the recovery or death.  is inflow or outflow of susceptible people based on the publicly available daily Migration.
is inflow or outflow of susceptible people based on the publicly available daily Migration.  is the number of inflowing/outflowing exposed people.
is the number of inflowing/outflowing exposed people.  is the probability of the outflowing exposed people.
is the probability of the outflowing exposed people.  is population inflow to a city, and
is population inflow to a city, and  is population outflow from a city.
is population outflow from a city.
 refers to the transmission rate for the susceptible to infection.
refers to the transmission rate for the susceptible to infection.  denotes the rate of transmission for the susceptible to exposure. The incubation rate, σ is described as the rate by which the exposed individual develops symptoms.
denotes the rate of transmission for the susceptible to exposure. The incubation rate, σ is described as the rate by which the exposed individual develops symptoms.  is the probability of recovery or death.
is the probability of recovery or death.
Stage 2: Calculation of Similarity
Calculate the Similarity of Attributes
To calculate the similarity between historical cases and the target case of public health emergencies, it is mainly to calculate the similarity of scenario descriptions. The similarity between target case  and historical case
and historical case  with respect to attribute r is defined as the following formula.
with respect to attribute r is defined as the following formula.
Ordered Enumerator
When the attribute value has a fixed value range with a certain order, it belongs to an ordered enumeration type. The values of an ordered enumeration type are sorted in a certain order within a fixed range of values. It is obvious that the closer the distance is, the higher the similarity becomes:

Here,  represents the number of enumerations.
represents the number of enumerations.  and
and  are the order of attribute
are the order of attribute  of the target case
of the target case  and the historical case
and the historical case  .
.
Crisp Number
When attributes  and
and  are crisp numbers, their similarity is given as follows:
are crisp numbers, their similarity is given as follows:

Here,  is the maximum value of attribute r, and
is the maximum value of attribute r, and  is the minimum value of attribute r in all cases.
is the minimum value of attribute r in all cases.
Interval Number
When attributes are interval numbers, the attribute similarity is given as follows:

Considering the values of a, b, c, and d, a simplified formula can be written as follows:

Here,  and
and  are two interval values of attribute
are two interval values of attribute  . And
. And  and
and  are the maximum and minimum values of attribute r in all cases, respectively.
are the maximum and minimum values of attribute r in all cases, respectively.
Calculate the Similarity of Cases
DEA is a nonparametric evaluation method based on the relative comparison between the evaluated objects. The comparative effectiveness of the decision-making unit can be evaluated by input data and output data without the intermediate process and data from input to output. Therefore, it has the advantages of simplicity and convenience.
In calculating the similarity between the target case and the historical case, the determination of attribute weights is the key point. The expression of emergency cases in this paper is based on the multi-dimensional situation space representation model, and the situation description is divided into two parts: plot and scenario. The plot and the situation are independent of each other, so they are regarded as two parallel subsystems with parallel structure.43 In cross-efficiency evaluation, each decision-making-unit (DMU) gets a self-appraised score obtained by its own most favorable weights and  peer scores obtained using the other DMUs’ most favorable weights. Then, all these efficiencies are aggregated into a final efficiency for the DMU under evaluation.44 Compared with the traditional DEA calculation method, the cross-efficiency evaluation method has fewer constraints and the assessment is more objective.
peer scores obtained using the other DMUs’ most favorable weights. Then, all these efficiencies are aggregated into a final efficiency for the DMU under evaluation.44 Compared with the traditional DEA calculation method, the cross-efficiency evaluation method has fewer constraints and the assessment is more objective.
To sum up, we propose a new case retrieval method based on the cross-efficiency evaluation method with the parallel system to calculate the similarity between the historical case  and the target case
and the target case  , as shown in Figure 3.
, as shown in Figure 3.
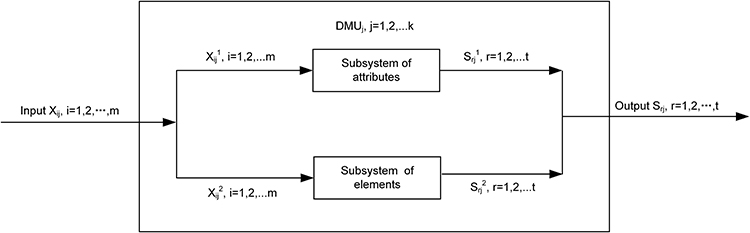 |
Figure 3 Calculate the Case Similarities with the Structure of the Parallel System. |
The similarity of attributes and elements can be derived from Equations (9–12). Then, we determine the similarity of attribute as  , where subscript denotes the attribute r of the historical case
, where subscript denotes the attribute r of the historical case  . Similarly,
. Similarly,  is the similarity of element. Thus an attribute similarity matrix of size
is the similarity of element. Thus an attribute similarity matrix of size  will have
will have  DMUs and
DMUs and  outputs, and it is shown in Equation (13).
outputs, and it is shown in Equation (13).
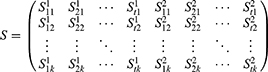
Each row of the attribute similarity matrix is viewed as a DMU, and each column of the attribute similarity matrix is viewed as an output. In the meantime, we employ a dummy input with a value of 1 for all the DMUs.45 Thus, a DMU will have one constant input and  outputs. Equation (14) is applied for the similarity of self-evaluation.
outputs. Equation (14) is applied for the similarity of self-evaluation.
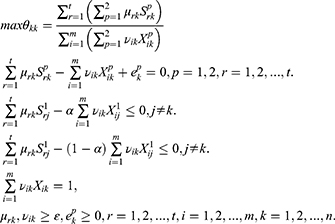
When  are introduced in Equation (14), the objective function can be rewritten as
are introduced in Equation (14), the objective function can be rewritten as 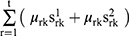 . Let the self-appraised similarity between the historical case
. Let the self-appraised similarity between the historical case  and the target case
and the target case  be given by:
be given by:
We define α as the importance of the plot, and thus (1–α) be the importance of the scenario. The  and
and  are the weights of the rth output and the ith input, respectively. The
are the weights of the rth output and the ith input, respectively. The  ,
,  ,
,  and
and  calculated by Equation (15), where asterisk indicates optimal solution. Hence, the plot similarity of Ck occurs when p = 1, and the scenario similarity of Ck occurs when p = 2.
calculated by Equation (15), where asterisk indicates optimal solution. Hence, the plot similarity of Ck occurs when p = 1, and the scenario similarity of Ck occurs when p = 2.

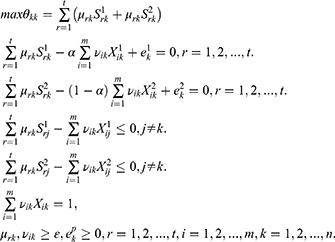
The self-appraised score  , as shown in Equation (15), that is, the self-appraised similarity between the historical case
, as shown in Equation (15), that is, the self-appraised similarity between the historical case  and the target case
and the target case  . Thus, we calculate the efficiency scores of each DMU n times, obtaining n weights of output by Equation (15). Then, the unit’s peer scores can be obtained by Equation (17). In this way, (n-1) peer scores and one self-appraised score are obtained for each DMU.
. Thus, we calculate the efficiency scores of each DMU n times, obtaining n weights of output by Equation (15). Then, the unit’s peer scores can be obtained by Equation (17). In this way, (n-1) peer scores and one self-appraised score are obtained for each DMU.
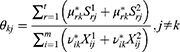
Here, is the average cross-efficiency of Cj calculated by Equation (18), and Sj represents the value of integrated similarity of the J–th case to the target case. Clearly, the greater the value of Sj, the more similar the historical case Cj is to the target case C0, and the corresponding solution is considered to be a better alternative, where
is the average cross-efficiency of Cj calculated by Equation (18), and Sj represents the value of integrated similarity of the J–th case to the target case. Clearly, the greater the value of Sj, the more similar the historical case Cj is to the target case C0, and the corresponding solution is considered to be a better alternative, where  satisfies
satisfies  .
.

Stage 3: Calculate the Implementation Effect of Similar Cases
Life Cycle Model of Public Health Emergencies
In 1986, Steven Fink, an American management scholar, first proposed the crisis life cycle model. He divided the development process of crisis into four stages: prodromal, outbreak, chronic and resolution.46 Public health emergencies often demonstrate periodic changes. Its development is also a dynamic and continuous process, which will experience the life cycle from occurrence to recession. The whole life cycle is also divided into several stages, and each stage has different performance, impact and characteristics. Therefore, as it has illuminated in Figure 4, the life cycle model of public health emergencies can be obtained by applying the crisis life cycle model to public health emergencies.
 |
Figure 4 The Life Cycle Model of Public Health Emergencies. |
The first stage is the prodromal period. It refers to when factors and dangers triggering public health emergencies have emerged in some areas, or individual cases have occurred. During this phase, the event evolves rapidly. If not dealt with immediately, the crisis may further increase, and the scope and intensity of its impact may further expand. At this time, if policymakers have a strong sense of crisis and actively adopt effective prevention measures, potential crises will be nipped in the bud. At this point, the effect of resolving the crisis is the best, with the lowest cost and the least harm.
The second stage is the outbreak period. It refers to a period when the negative impact of a public health emergency is expanding, and an inflection point is imminent. At this time, the impact and loss of emergency events reach the highest point, and the number of occurrences also shows a gradually decreasing trend, which seriously affects the stability of society. Although this stage usually does not last for a long time, it is the stage that produces the greatest harm. Because of its dramatic effect, some scholars equate this stage with the whole process of crisis events. At the same time, this stage is also the most arduous one in the emergency process, and the follow-up work is arranged and launched from this.
The third phase is the resolution period. During this period, the epidemic is effectively managed and contained, so the epidemic is effectively controlled, and the situation tends to be stable In the meantime, the secondary hazards caused by the epidemic should be minimized with the premise of ensuring the orderly progress of the prevention and control work. It is necessary to remain vigilant to avoid the recurrence of the crisis, although the impact of the crisis events during this period gradually subsided, and the production and life of people gradually returned to normal. At this stage, except for decision-makers doing the relevant aftermath work, they should also summarize the experience in the process of responding to this public health emergency, analyze the reasons for the outbreak of the crisis, and think about how to avoid the recurrence of the crisis. This is a long-lasting phase.
Therefore, the characteristics of the three stages of the life cycle model are illustrated in Figure 5.
 |
Figure 5 The Characteristics of Evolution of Public Health Emergencies. |
Evaluation Index System for the Effect of the Emergency Plan
The evaluation of the implementation effect of an emergency plan involves a large number of influencing factors, so the process is complicated. To ensure the accuracy and objectivity of the evaluation results, it is necessary to establish a scientific evaluation index system. We consult the relevant literature47–49 and refer to the practical experience to construct an evaluation index system for the implementation effect of the emergency reference plan. Therefore, H = {Prevention and control of the epidemic ( ), Reduction of property losses (
), Reduction of property losses ( ) and Reduction of the impact on daily life (
) and Reduction of the impact on daily life ( ) make up the first-level indicators}. The secondary indicators are defined as W = {Control the mortality rate (
) make up the first-level indicators}. The secondary indicators are defined as W = {Control the mortality rate ( ), Control the infection rate (
), Control the infection rate ( ), Reduce the impact on the industry economy (
), Reduce the impact on the industry economy ( ), Reduce the impact on the public economy (
), Reduce the impact on the public economy ( ), Reduce the impact on the social order (
), Reduce the impact on the social order ( ), Reduce the impact on daily traffic (
), Reduce the impact on daily traffic ( ), Reduce the impact on education (
), Reduce the impact on education ( )}. As can be seen in Table 1, we utilize D-AHP to calculate the weights of indexes based on five experts.
)}. As can be seen in Table 1, we utilize D-AHP to calculate the weights of indexes based on five experts.
 |
Table 1 The Weights of Evaluation Index System |
The implementation effect of the emergency reference plan of the historical case Ck is shown in Equation (19).

Clearly, the higher the value of Ek, the more the implementation effect of the emergency plan of the historical case Ck can be considered the best.
Illustrative Example
In this section, an illustrative example of an application is proposed to demonstrate the effectiveness and efficiency of the method for generating emergency solutions. We collected 24 historical cases that occurred in 11 cities in China. A typical COVID-19 epidemic in Dalian City of Liaoning Province, China, on November 6, 2021, is considered the target case.
Collection of Case Index and Data
Selection and Collection of Case Index
Referring to relevant literature, 60% of the confirmed COVID-19 cases were found in places where the air temperature ranged from 5°C to 15°C, and the number of confirmed cases was significantly related to relative humidity.50 The nitrogen dioxide (NO2) concentration can be used as an environmental lockdown indicator to evaluate the effectiveness of lockdown measures,51 that is to help policymakers effectively monitor and manage non-pharmaceutical interventions in outbreaks. At the same time, the number of new confirmed cases and the number of existing confirmed cases reflect the development of the epidemic and the treatment of patients. Since the number of close contacts is less affected by changes in statistical caliber, it can more objectively reflect the evolvement trend of the epidemic. Asymptomatic coronavirus carriers as “invisible” infected persons have important epidemiological significance.
As discussed earlier, we have four attributes for calculating the similarity of plots, including the temperature ( ), relative humidity (
), relative humidity ( ), NO2 concentration (
), NO2 concentration ( ), and weather (
), and weather ( ). We regard indicators reflecting the development of the epidemic as elements for calculating the similarity of scenarios, containing the number of new confirmed cases (
). We regard indicators reflecting the development of the epidemic as elements for calculating the similarity of scenarios, containing the number of new confirmed cases ( ), number of existing confirmed cases (
), number of existing confirmed cases ( ), number of existing close contacts (
), number of existing close contacts ( ), and number of existing asymptomatic coronavirus carriers (
), and number of existing asymptomatic coronavirus carriers ( ).
).
Collection of Case Data
Corresponding observational data of air temperature and relative humidity were obtained from the Weather Underground website,52 and the data on NO2 concentration came from the World’s Air Pollution website.53 The relevant data on COVID-19 was acquired from the latest reports of the National Health Commission of the People’s Republic of China and the Health Commission of the Province.54–56 The total population of Dalian came from the communique of the seventh time national census in Liaoning Province.57 The solutions and specific measures for each historical case came from the policies issued by the National Health Commission and relevant local governments. To sum up, we have constructed a historical case database containing 24 cases, whose specific information is shown in Table 2.
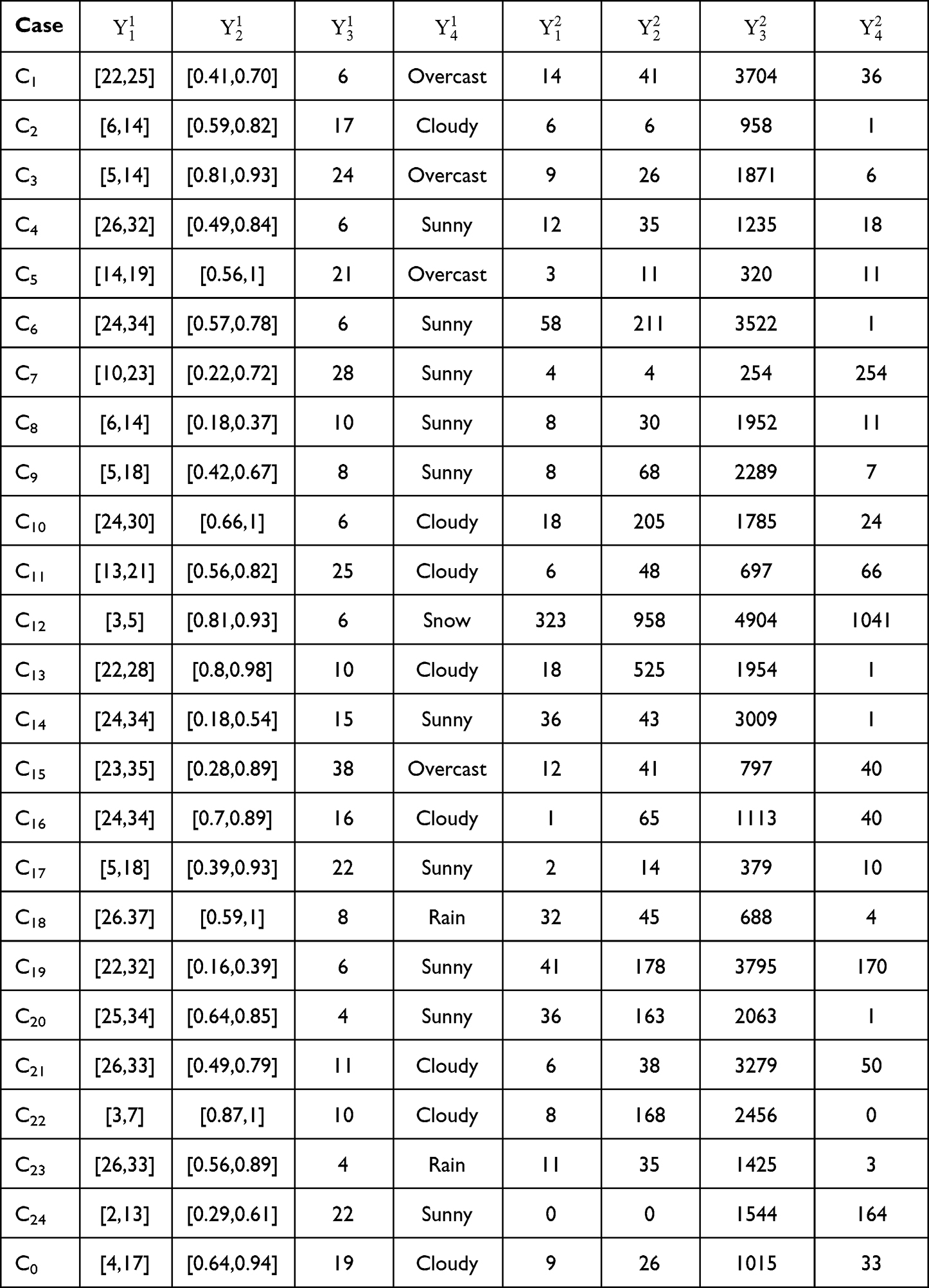 |
Table 2 Problem Attributes and Elements for the Historical Cases and the Target Case |
Predict Attribute Values Based on Modified SEIR Model
As has been shown in Table 3, the values of the parameters can be obtained by referring to relevant literature research42,58–60 and measures of plague prevention and control in Dalian.
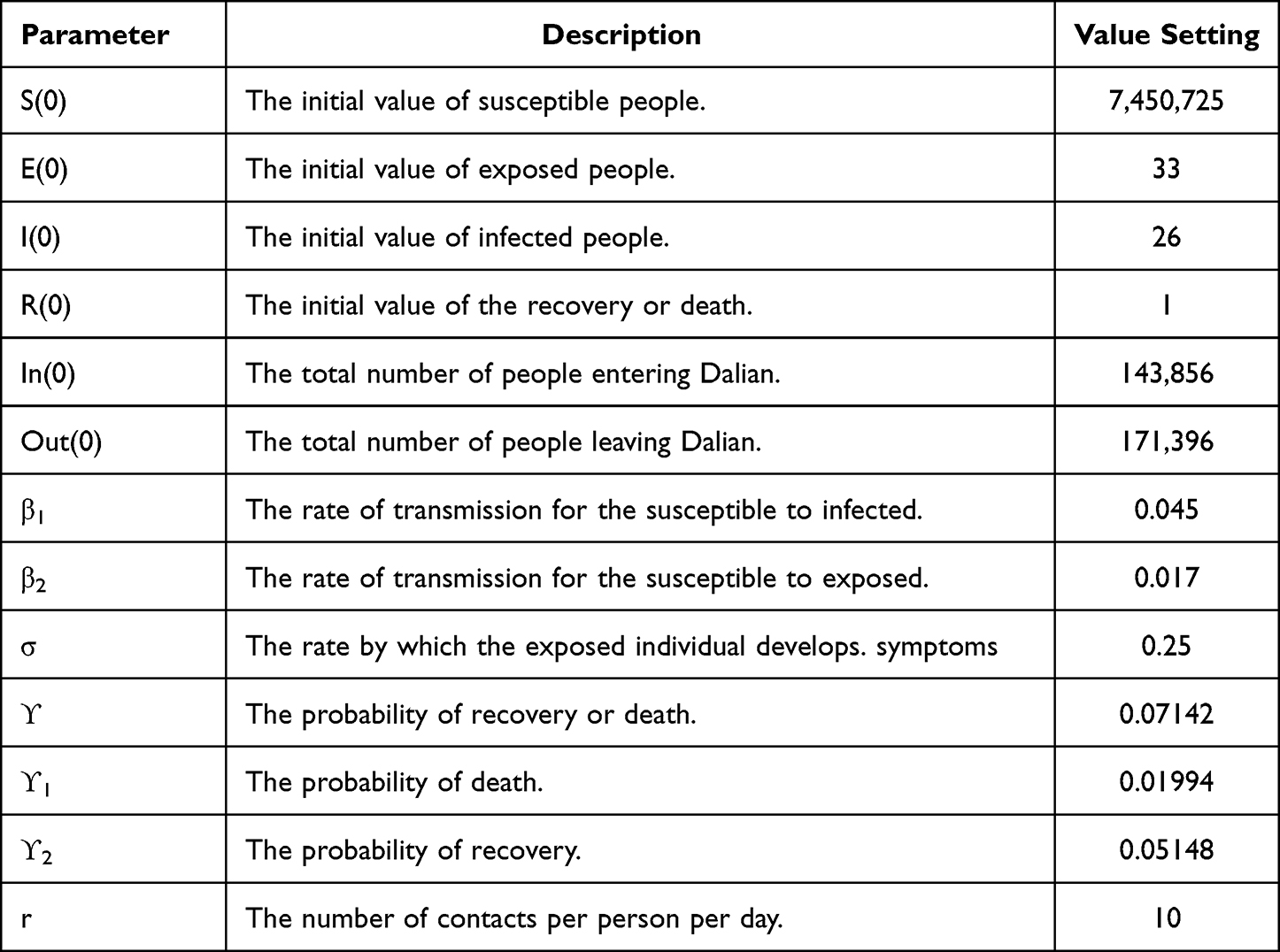 |
Table 3 Parameter Values of the Modified SEIR Model |
We use the modified SEIR model to re-evaluate the value of elements through the data and parameter values in Tables 2 and 3. Using Equation (3), we can determine  , that is, the number of existing confirmed cases (
, that is, the number of existing confirmed cases ( ) is 33. The
) is 33. The  is given as 26 in Table 3, so the difference between
is given as 26 in Table 3, so the difference between  and
and  is 7, that is, the containing the number of new confirmed cases (
is 7, that is, the containing the number of new confirmed cases ( ) is 7. According to Equations 2, 7, and 8, the
) is 7. According to Equations 2, 7, and 8, the  is obtained as
is obtained as  , that is, the number of existing asymptomatic coronavirus carriers (
, that is, the number of existing asymptomatic coronavirus carriers ( ) is 42. The number of existing close contacts (
) is 42. The number of existing close contacts ( ) is 1385, calculated by Equations 4–6.
) is 1385, calculated by Equations 4–6.
To sum up, we can predict the value of elements in the target case, that is, Y2={7,33,1385,42} and the actual value is Y2={20,45,1582,43}. By comparing two sets of data, it can be seen that the predicted number is slightly lower than the actual number. However, the accuracy of the results is relatively excellent.
Calculate the Similarity of Cases
Among all attributes and elements,  and
and  are interval numbers,
are interval numbers,  ,
,  ,
,  ,
,  are crisp numbers, and
are crisp numbers, and  is an ordered enumerator, whose enumerator set is
is an ordered enumerator, whose enumerator set is  . Using Equation (12), we can determine the similarity of interval number attributes, including temperature
. Using Equation (12), we can determine the similarity of interval number attributes, including temperature and relative humidity
and relative humidity . The similarity of crisp attributes is calculated by Equation (10), which includes NO2 concentration
. The similarity of crisp attributes is calculated by Equation (10), which includes NO2 concentration  , the number of new confirmed cases
, the number of new confirmed cases , the number of existing confirmed cases
, the number of existing confirmed cases , the number of existing close contacts
, the number of existing close contacts , and the number of existing asymptomatic coronavirus carriers
, and the number of existing asymptomatic coronavirus carriers  . For the ordered enumerators, the similarity of weather
. For the ordered enumerators, the similarity of weather is calculated by Equation (9). We list the similarity of attributes or elements in Table 4.
is calculated by Equation (9). We list the similarity of attributes or elements in Table 4.
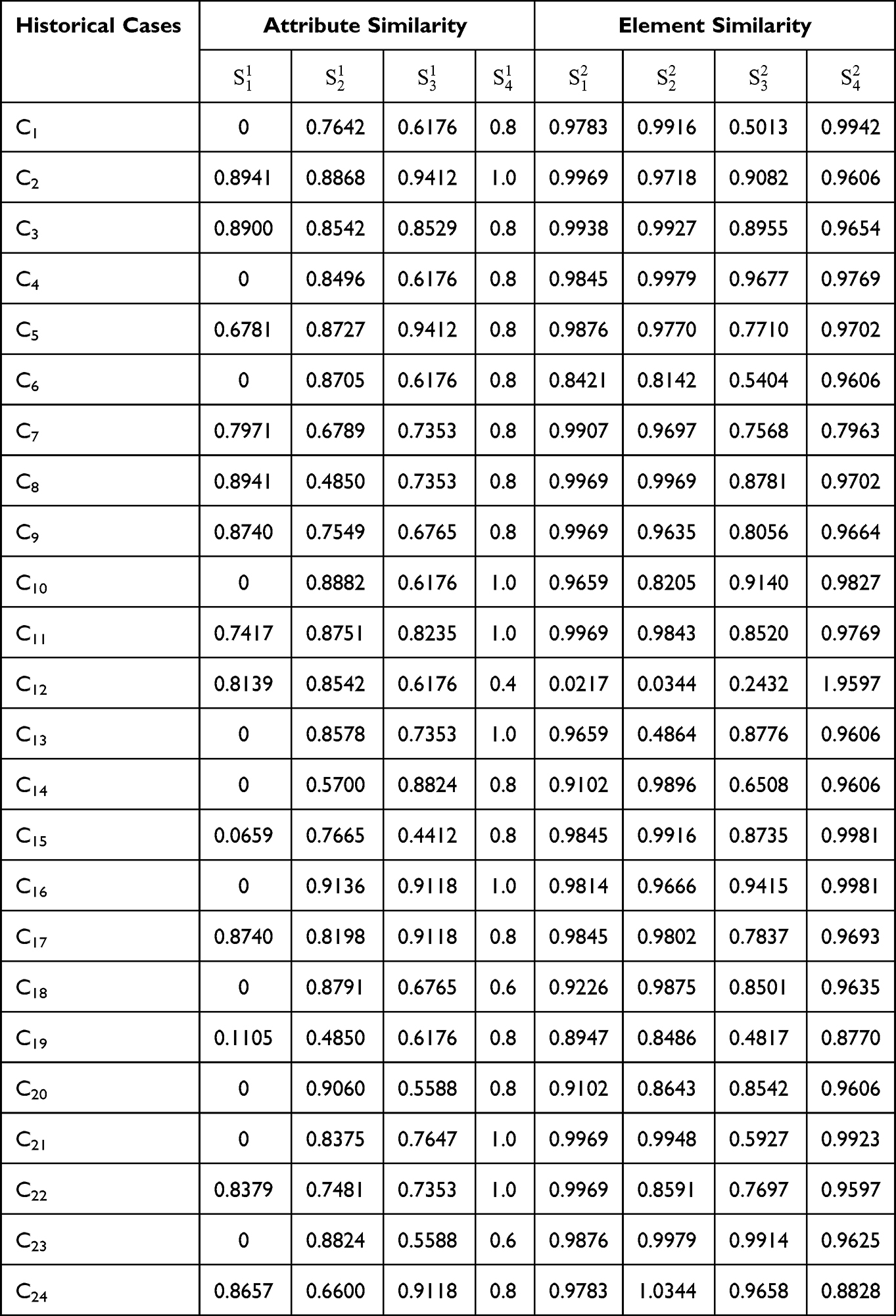 |
Table 4 The Computation Results of Attribute Similarity Between Historical Cases and the Target Case |
Using Equations (15–17), we can determine the efficiency scores of plot similarity ( ) and scenario similarity (
) and scenario similarity ( ). According to Equation (18), the average cross-efficiency scores of case similarity (Sj) are obtained. The decision-makers determined the value of α as 0.4. The computation results can be found in Figure 6.
). According to Equation (18), the average cross-efficiency scores of case similarity (Sj) are obtained. The decision-makers determined the value of α as 0.4. The computation results can be found in Figure 6.
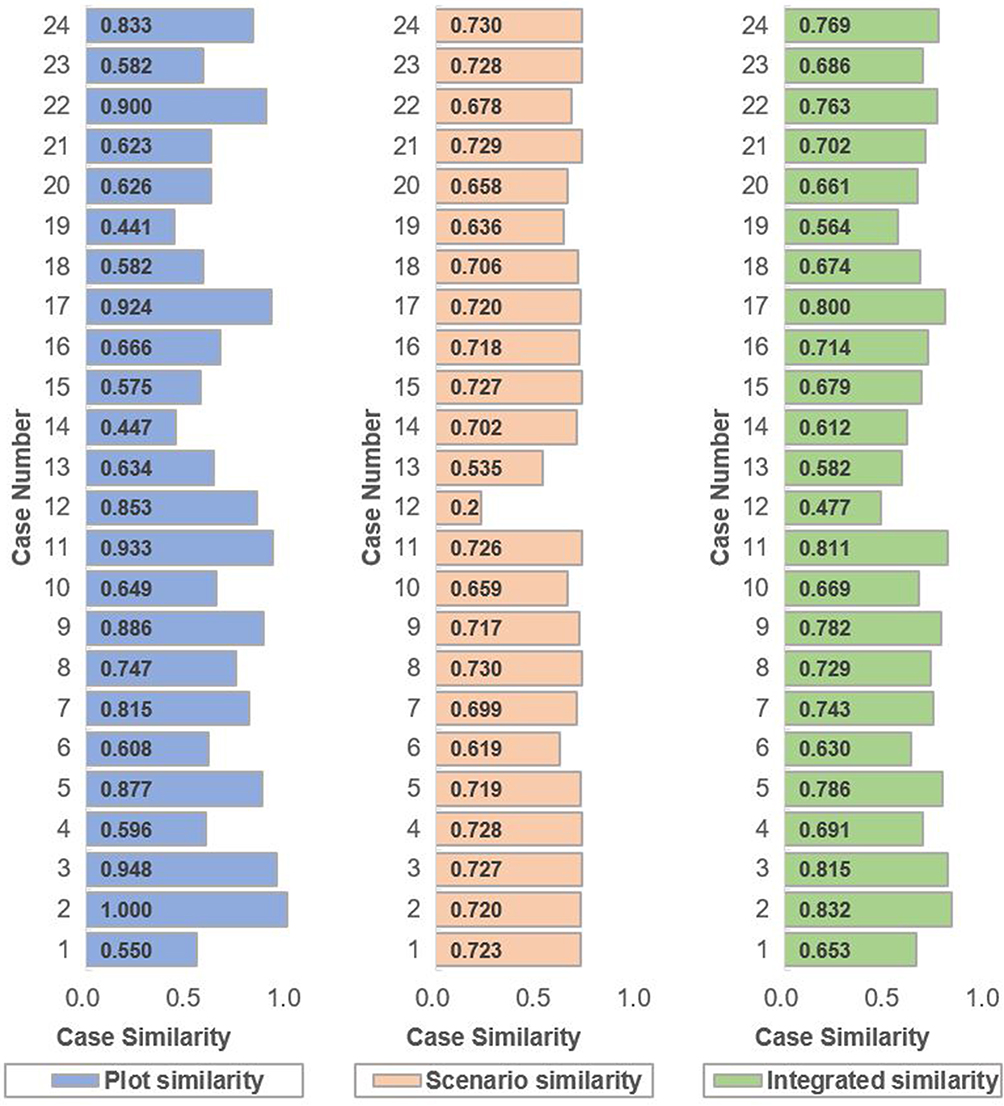 |
Figure 6 Case Similarity Calculated from the Cross-evaluation Methods for 24 Historical Cases. |
The case similarity threshold given as 0.7 by the decision-makers. It is indicated from the computation results that the retrieved historical cases C2, C3, and C11 have the most resemblance to the target case.
Calculate the Implementation Effect of Similar Cases
Combined with the actual situation, we can judge that the target case is in the prodromal period, so the weight vector of practical effect is  . The score vector of similar emergency plans for historical cases C2, C3, and C11 provided by the experts of decision-making are Z2={10,8,8,9,6,7},
. The score vector of similar emergency plans for historical cases C2, C3, and C11 provided by the experts of decision-making are Z2={10,8,8,9,6,7},  , and
, and  .
.
Using Equation (19), we can determine the final score of three similar emergency solutions, that is,  ,
,  , E11=7.7239. It is obvious that C3 is the best one. Therefore, it can be used as an emergency reference plan for the next epidemic period. After the end of this epidemic, the emergency measures will be optimized and modified according to the experience and stored in the historical cases library as a reference plan. Figure 7 lists the specific emergency reference measures.
, E11=7.7239. It is obvious that C3 is the best one. Therefore, it can be used as an emergency reference plan for the next epidemic period. After the end of this epidemic, the emergency measures will be optimized and modified according to the experience and stored in the historical cases library as a reference plan. Figure 7 lists the specific emergency reference measures.
 |
Figure 7 Emergency Reference Measures of the Target Case. |
Discussion
Implications
It is well known that one of the challenges in generating emergency reference plans for public health emergencies is how to quickly and accurately generate an effective reference plan for the development of an outbreak so that government departments, health systems, and hospitals can respond in advance to contain the deterioration of the outbreak. As discussed earlier, most existing methods for generating emergency reference plans using CBR do not consider the forecast of target cases or the phase of public health emergencies. The majority of researchers base their reasoning on a complete case, which does not facilitate case retrieval and reuse.
This paper developed a new approach to pre-generate emergency plans for public health emergency events to better cope with the epidemic. The proposed method has three contributions compared with existing methods for generating emergency plans. Firstly, a method for predicting some attribute values based on the modified SEIR model is proposed according to the characteristics of public health emergencies, such as fast changing speed and long development period. This method solves the problem that existing methods for generating emergency plans have a lag compared with the development of actual events, thereby realizing intelligent prediction and making the generated solution more forward-looking and pertinent. Secondly, through the cross-efficiency evaluation model of the parallel system, the similarity calculation based on case reasoning is transformed into the calculation based on the scenario and plot. In this way, the scale of case information retrieval is reduced, and a more scientific similarity calculation fusion method is constructed, so that the retrieval results are more objective, detailed and accurate. Finally, considering the multi-stage evolution of public health emergencies and the differences in decision-making objectives at each stage, we established a multi-stage emergency effect evaluation model combined with the public health emergency life cycle model to make the most effective alternative for reference.
Limitations
There are still some limitations that should be noted for future research. First, we determine the stage of the target case in the life cycle model of public health emergency by the judgment of experts. So, the following issue needs to be addressed: build a function to fit the life cycle curve of public health emergencies to accurately divide each stage, define key decision points, and scientifically judge the stage of the target case, thereby generating more accurate and effective emergency reference plans. Second, as the COVID-19 epidemic evolves, medical decision-making departments have proposed prevention and control measures such as “dynamic zero-Covid policy” and “zero community transmission policy”. In future work, these policies will integrate with predictive models to make the final decision more accurate. Third, it has to be discussed the influence of psychological factors on the generation of emergency reference plans, such as the mood of the population, their psychological state and the expectations of decision-makers regarding the effectiveness of the response. This would be a significant research problem for future research.
Conclusion
In the outbreak of a major public health emergency, this research can provide rapid decision support and corresponding management recommendations for public services such as government departments, centers for disease control (CDC), medical emergency centers and transport authorities, etc. During a pandemic, government departments can achieve relevant measures by applying the pre-generation of emergency reference plan model, which provides suggestions to managers on deploying remedies in the medical, economic and livelihood areas in advance, reducing public panic and avoiding secondary harm to the population due to lagging emergency plans. For medical institutions, it is possible to allocate and dispatch medical staff and resources more quickly and accurately according to the scale of the current epidemic, so that they can better respond to the development of the epidemic and reduce the risk of physical and mental health of the population. As for some areas with a relatively low level of emergency management, this method can be used to quickly integrate emergency resources, conduct emergency command and dispatch, rationally allocate emergency supplies, and minimize the consequences of disasters.
This article provides a new idea and perspective to deal with public health emergency events. The method proposed in this paper improves the level of intelligence and precision of decision-making in public health emergencies while considering the speed and quality of decision-making. This provides a reliable basis for generating emergency plans for public health emergencies in real situations and offers a corresponding reference for decision-making in other similar public health emergencies, thereby reducing or avoiding the negative influence of public health emergencies. The numerical example proves that this methodology with practical application value can support emergency decision-making of relevant departments.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Ethics and Exemption Statement
In the overall process, this research used non-interventional studies methods such as literature research, and all data were collected from the daily report published on the official website of the National Health Commission of the People’s Republic of China. Therefore, all data used in the research were publicly available by local government departments. Ethical approval is not required according to the local regulations “Ethical Guidelines on Biomedical Research Involving Human Subjects” for the use of epidemic data already published by the government on the Internet for relevant research. Therefore, this article does not require ethical approval.
Funding
This study is supported by the Science and Technology Department of Shaanxi Province, China (grant number 2021JM-144).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Janssen M, van der Voort H. Agile and adaptive governance in crisis response: lessons from the COVID-19 pandemic. Int J Inform Manage. 2020;55:102180. doi:10.1016/j.ijinfomgt.2020.102180
2. Mohammad A, Reza T. A new methodology for COVID-19 preparedness centers based on a location-allocation platform. JISE. 2020;13(1):35–41.
3. Mohammad A, Reza T, Mina S. Scheduling the COVID-19 vaccine distribution based on data-driven decision-making methods. JIEMS. 2022;8(2):196–206. doi:10.22116/jiems.2022.138130
4. Abdulkareem KH, Mohammed MA, Salim A, et al. Realizing an effective COVID-19 diagnosis system based on machine learning and IoT in smart hospital environment. IEEE Internet Things. 2021;8(21):15919–15928. doi:10.1109/JIOT.2021.3050775
5. Prachand VN, Milner R, Angelos P, et al. Medically necessary, time-sensitive procedures: scoring system to ethically and efficiently manage resource scarcity and provider risk during the COVID-19 pandemic. J Am Coll Surgeons. 2020;231(2):281–288. doi:10.1016/j.jamcollsurg.2020.04.011
6. Mohammad A, Amir A, Fariborz J. Prioritizing and queueing the emergency departments’ patients using a novel data-driven decision-making methodology, a real case study. Expert Syst Appl. 2022;195:116568. doi:10.1016/j.eswa.2022.116568
7. Yu L, Lai KK. A distance-based group decision-making methodology for multi-person multi-criteria emergency decision support. Decis Support Syst. 2011;51(2):307–315. doi:10.1016/j.dss.2010.11.024
8. Li P, Wei CP. An emergency decision-making method based on D-S evidence theory for probabilistic linguistic term sets. Int J Disast Risk Re. 2019;37. doi:10.1016/j.ijdrr.2019.101178
9. Zhao M, Liu X. Development of decision support tool for optimizing urban emergency rescue facility locations to improve humanitarian logistics management. Safety Sci. 2018;102:110–117. doi:10.1016/j.ssci.2017.10.007
10. Losada J, Sanchez SR, Garcia MC, et al. Rapid response to large-scale emergencies: a neural network model and a decision-tree algorithm. Emergencias. 2012;24(3):175–180.
11. Wang L, Zhang Z, Wang Y. A prospect theory-based interval dynamic reference point method for emergency decision making. Expert Syst Appl. 2015;42(23):9379–9388. doi:10.1016/j.eswa.2015.07.056
12. Wq S, Wang HZ, Chen C, Kong ZJ. Evolutionary game analysis of decision-making dynamics of local governments and residents during wildfires. Int J Disast Risk Re. 2021;53. doi:10.1016/j.ijdrr.2020.101991
13. Shi B, Jiang JP, Liu RT, Khan AU, Wang P. Engineering risk assessment for emergency disposal projects of sudden water pollution incidents. Environ Sci Pollut R. 2017;24(17):14819–14833. doi:10.1007/s11356-017-9078-2
14. Liu Y, Fan ZP, Yuan Y, Hy L. A FTA-based method for risk decision-making in emergency response. Comput Oper Res. 2014;42:49–57. doi:10.1016/j.cor.2012.08.015
15. Liao ZL, Mao XW, Liu YH, Xu ZX, Hannam PM. CBR respond and preparedness system development for environmental emergency. Civ Eng Environ Syst. 2011;28(4):301–323. doi:10.1080/10286608.2011.604416
16. Raskob W, Mohrle S, Bai S. Knowledge database and case-based reasoning. Radioprotection. 2016;51(HS2):S185–S186. doi:10.1051/radiopro/2016069
17. Zhang H, Dai GL. Research on traffic decision making method based on image analysis case based reasoning. Optik. 2018;158:908–914. doi:10.1016/j.ijleo.2018.01.007
18. Wang DL, Wan KD, Ma WX. Emergency decision-making model of environmental emergencies based on case-based reasoning method. J Environ Manage. 2020;262:110382. doi:10.1016/j.jenvman.2020.110382
19. Shao JF, Liang CY, Liu YJ, Xu J, Zhao SP. Relief demand forecasting based on intuitionistic fuzzy case-based reasoning. Socio-Econ Plan Sci. 2021;74:100932. doi:10.1016/j.seps.2020.100932
20. Yao X, Guo HX, Zhu J, Shi Y. Dynamic selection of emergency plans of geological disaster based on case-based reasoning and prospect theory. Nat Hazards. 2021. doi:10.1007/s11069-021-05036-6
21. Li R, Wang JQ, Wang SL, Wu HY. Prediction of network public opinion features in urban planning based on geographical case-based reasoning. Int J Digit Earth. 2022;15(1):890–910. doi:10.1080/17538947.2022.2078437
22. Wang QE, Su MM, Zeng L, Chen HH, New A. Method to assist decision-making of water environmental emergency in expressway region. Int J Env Res Pub He. 2022;19:16. doi:10.3390/ijerph191610043
23. Zhao Z, Chen JH, Xu KH, Xie HW, Gan XX, Xu H. A spatial case-based reasoning method for regional landslide risk assessment. Int J Appl Earth Obs. 2021;102. doi:10.1016/j.jag.2021.102381
24. Zheng J, Wang Y, Chen S. Dynamic case retrieval method with subjective preferences and objective information for emergency decision making. IEEE/CAA J Autom Sin. 2018;5(3):749–757. doi:10.1109/JAS.2016.7510232
25. Jl D, Jiao F. Novel case-based reasoning system for public health emergencies. Risk Manag Healthc P. 2021;14:541–553. doi:10.2147/RMHP.S291441
26. Gu DX, Liang CY, Zhao HM. A case-based reasoning system based on weighted heterogeneous value distance metric for breast cancer diagnosis. Artif Intell Med. 2017;77:31–47. doi:10.1016/j.artmed.2017.02.003
27. Fan ZP, Li YH, Wang XH, Liu Y. Hybrid similarity measure for case retrieval in CBR and its application to emergency response towards gas explosion. Expert Syst Appl. 2014;41(5):2526–2534. doi:10.1016/j.eswa.2013.09.051
28. Chen WL, Wang XL, Wang W, Zhu YS, Cai ZJ, Yang S. A heterogeneous GRA-CBR-based multi-attribute emergency decision-making model considering weight optimization with dual information correlation. Expert Syst Appl. 2021;182. doi:10.1016/j.eswa.2021.115208
29. Zhang XH, Deng ZH, Liu W, Cao H. Combining rough set and case based reasoning for process conditions selection in camshaft grinding. J Intell Manuf. 2013;24(2):211–224. doi:10.1007/s10845-011-0557-x
30. Li H, Andina D, Sun J. Multiple proportion case-basing driven CBRE and its application in the evaluation of possible failure of firms. Int J Syst Sci. 2013;44(8):1409–1425. doi:10.1080/00207721.2012.659686
31. Park Y. Improving real-time efficiency of case retrieving process for case-based reasoning. Asia Pac J Inf Syst. 2015;25(4):626–641. doi:10.14329/apjis.2015.25.4.626
32. He W, Xu LD. Integrating both Wikis and XML with case bases to facilitate case base development and maintenance. Expert Syst Appl. 2011;38(7):8632–8638. doi:10.1016/j.eswa.2011.01.067
33. Yan AJ, Zhang KH, Yu YH, Wang P. An attribute difference revision method in case-based reasoning and its application. Eng Appl Artif Intel. 2017;65:212–219. doi:10.1016/j.engappai.2017.07.015
34. Yu XB, Li CL, Zhao WX, Chen H. A novel case adaptation method based on differential evolution algorithm for disaster emergency. Appl Soft Comput. 2020;92:106306. doi:10.1016/j.asoc.2020.106306
35. Yu XB, Yu XR, Zhang XY. Case-based reasoning adaptation based on fuzzy gravitational search algorithm for disaster emergency plan. J Intell Fuzzy Syst. 2021;40(6):11007–11022. doi:10.3233/JIFS-202132
36. Liang YR, Wang HB, Xu AJ, Tian NY. A two-step case-based reasoning method based on attributes reduction for predicting the endpoint phosphorus content. Isij Int. 2015;55(5):1035–1043. doi:10.2355/isijinternational.55.1035
37. Guo Y, Zhang B, Sun Y, Jiang K, Wu K. Machine learning based feature selection and knowledge reasoning for CBR system under big data. Pattern Recogn. 2021;112:107805. doi:10.1016/j.patcog.2020.107805
38. Awel S, Ahmed I, Tilahun D, Tegenu K. Impact of COVID-19 on health seeking behavior of patients with chronic disease at public hospitals in Jimma Zone, South West Ethiopia. Risk Manag Healthc P. 2022;15:1491–1500. doi:10.2147/RMHP.S367730
39. Zhao DH, Lin HJ, Zhang ZR. Evidence-based framework and implementation of China’s strategy in combating COVID-19. Risk Manag Healthc P. 2020;13:1989–1998. doi:10.2147/RMHP.S269573
40. Alsaqqa HH. Building the culture of public health as a positive reflection from the COVID-19 crisis. Risk Manag Healthc P. 2022;15:1683–1693. doi:10.2147/RMHP.S365233
41. Qian J, Liu Y, Liu C, Jiao Y. Research on two-layer case retrieval algorithm based on multidimensional scenario space representation. Manage Rev. 2016;28:8. doi:10.14120/j.cnki.cn11-5057/f.2016.08.005
42. Yang Z, Zeng Z, Wang K, et al. Modified SEIR and AI prediction of the epidemics trend of COVID-19 in China under public health interventions. J Thorac Dis. 2020;12:165–174. doi:10.21037/jtd.2020.02.64
43. Kao C. Efficiency measurement for parallel production systems. Eur J Oper Res. 2009;196(3):1107–1112. doi:10.1016/j.ejor.2008.04.020
44. Sexton T, Silkman R, Hogan A. Data envelopment analysis: critique and extensions. New Dir Eval. 1986;1986:73–105. doi:10.1002/ev.1441
45. Ramanathan R. Data envelopment analysis for weight derivation and aggregation in the analytic hierarchy process. Comput Oper Res. 2006;33:1289–1307. doi:10.1016/j.cor.2004.09.020
46. Fink S, American MA. Crisis Management: Planning for the Inevitable. Amacom; 1986.
47. Wang YS, Sun HJ, Zou JC, Ning J, Du Y. Evaluation model for hospital response capability for public health emergency. Disaster Med Public. 2021;15(4):403–408. doi:10.1017/dmp.2020.31
48. Ma GF, Tan S, Shang SS. The evaluation of building fire emergency response capability based on the CMM. Int J Env Res Pub He. 2019;16:11. doi:10.3390/ijerph16111962
49. Zheng J, Wang YM, Zhang K, Liang J. A dynamic emergency decision-making method based on group decision making with uncertainty information. Int J Disast Risk Sc. 2020;11(5):667–679. doi:10.1007/s13753-020-00308-4
50. Huang Z, Huang J, Gu Q, Du P, Liang H, Dong Q. Optimal temperature zone for the dispersal of COVID-19. Sci Total Environ. 2020;736:139487. doi:10.1016/j.scitotenv.2020.139487
51. Lian X, Huang J, Zhang L, Liu C, Liu X, Wang L. Environmental Indicator for COVID-19 non-pharmaceutical interventions. Geophys Res Lett. 2020;48. doi:10.1029/2020GL090344
52. Local Weather Forecast, News and Conditions. Weather underground. Available from: https://www.wunderground.com/.
53. World’s air pollution: real-time air quality index. Available from: http://waqi.info/.
54. National Health Commission of the People’s Republic of China. Notify the COVID-19 outbreak. Available from: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml.
55. Health Commission of Hubei Province. Notify the COVID-19 outbreak of Hubei Province. Available from: http://wjw.hubei.gov.cn/bmdt/dtyw/.
56. Health Commission of Shaanxi Province. Important health news of Shaanxi Province. Available from: http://sxwjw.shaanxi.gov.cn/sy/wjyw/.
57. The People’s Government of Liaoning Province. The communique of seventh time national census in Liaoning Province. Available from: http://tjj.ln.gov.cn/tjsj/tjgb/rkpcgb/202105/t20210530_4139310.html.
58. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA-J Am Med Assoc. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
59. Read JMLJ. Social mixing patterns in rural and urban areas of southern China. Biol Sci. 2014. doi:10.1098/rspb.2014.0268
60. The platform of Baidu Qianxi. Available from: https://qianxi.baidu.com/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.