Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Practical Guide to Hair Graft Placement Using the Sharp Implanter Method
Authors Park JH ![]() , Ho YH, Manonukul K
, Ho YH, Manonukul K ![]()
Received 7 March 2023
Accepted for publication 8 July 2023
Published 11 July 2023 Volume 2023:16 Pages 1777—1785
DOI https://doi.org/10.2147/CCID.S411488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Supplementary video 1 of “Hair graft placement using the sharp implanter method” [ID 411488].
Views: 547
Jae Hyun Park,1 Yeh Hong Ho,2 Kotchamol Manonukul3
1Dana Plastic Surgery Clinic, Seoul, Korea; 2Dana Taipei Hair Transplantation Clinic, Taipei City, 106, Taiwan, People’s Republic of China; 3V Design Hair by Dana International, Vibhavadi Hospital, Bangkok, 10900, Thailand
Correspondence: Jae Hyun Park, Dana Plastic Surgery Clinic, 10F Samju Building, Gangnamdaero 606, Gangnamgu, Seoul, Korea, Tel +82-2-512-0922, Fax +82-2-512-0942, Email [email protected]
Purpose: Hair transplantation using the sharp implanter method is increasing in popularity. However, there has been little discussion pertaining to surgical know-how or specific techniques that increase efficiency and precision. We describe surgical techniques that enable dense packing in a swift and efficient fashion with the sharp implanter method using photos and videos.
Patients and Methods: Grafts were placed using the sharp implanter method while adhering to several important principles. Eleven principles regarding the following aspects of hair transplant surgery were explained: gripping the implanter, graft placing technique that minimizes graft popping and tissue trauma when using the implanter, efficient team surgery system with assistant staff, direction and sequence of graft insertion, effective regimen for using epinephrine to control bleeding, selection of appropriately sized implanter tip, selection and usage of wide and narrow channel implanter tips, importance and methods of depth control, and staff training.
Results: High graft survival and dense and natural hair density can be obtained with the sharp implanter method when performed in compliance with the principles described here.
Conclusion: Appropriate use of the sharp implanter technique allows efficient and rapid graft insertion and achieves natural outcomes.
Keywords: hair follicle, hair transplant, implanter, sharp implanter, alopecia
Introduction
Graft insertion for hair transplantation can be performed using the one-step stick and place method or the two-step pre-made site method.1 With the slit method, the first step is incision, which is followed by graft placement after bleeding ceases. This method is useful in patients with rigid skin including scar. This method can be performed using various graft placement devices including the KEEP (Koray Erdogan Embedding Placer), Dull Needle Implanter, Devroye’s multi-implanter, Mohebi’s implanter, and others.2–4 With the sharp implanter method, hair follicles are first loaded into a needle. Then, the skin is punctured and the graft is left within the incision. Finally, the needle is withdrawn. Incision and graft insertion simultaneously take place.5–7
The sharp implanter method has advantages and disadvantages compared to the slit method.8,9 Advantages include simplicity and ease of technique, shorter operation time, and less propensity for crushing injury compared to the method using forceps to grab hair follicles. The incision angle can be delicately adjusted according to the hair curl and thickness because incision and insertion simultaneously take place.10 In addition, the physician directly performs the entire procedure. Disadvantages are that the technique can be burdensome in patients with a propensity for bleeding and that it is labor intensive. Furthermore, repeated graft popping in inexperienced hands may result in a low graft survival rate and disappointing outcome. Although the sharp implanter method can be easily mastered, it still requires cumulative experience to skillfully perform the procedure. However, to the best of our knowledge, little is known regarding proper handling of sharp implanters, avoiding graft insertion complications, and achieving high density and natural surgical outcomes. Therefore, this article aimed to review the sharp implanter technique based on our experience and to summarize the relevant literature.
Materials and Methods
Here, we describe principles and surgical techniques that enable dense packing in a swift and efficient fashion with the sharp implanter method.
Three-Finger Technique
The importance of proper grip of the implanter shaft cannot be overemphasized in hair transplant surgery, as the skin is punctured thousands of times. The implanter should be gripped using only the thumb, index finger, and middle finger because they are the most freely moving fingers (Figure 1) (Supplementary Video 1). Such a grip allows accurate and free control of the insertion angle and direction and enables rapid implantation. In addition, when an acute angle of insertion is required, such as in the area of the temple or sideburns, this grip is much more advantageous. If the ring finger is used to grip the implanter, it is caught below the implanter shaft, which prevents insertion at an acute angle and causes unnatural movements. Once the three-finger technique becomes familiar, it enables the most comfortable, fast, and agile implantation.
 |
Figure 1 3 Finger grip. |
When gripping, the thickest part of the volar side of the distal phalanx should be used. The implanter should be held with little force, as if you were holding a raw egg (Supplementary Video 2). If the grip is too forceful, scalp soft tissue trauma may result. Gripping with the fingertips causes interphalangeal joint flexion, which causes tension and prevents smooth motion (Supplementary Video 3). Grafts should also be inserted with minimal movement and with the surgeon in a position that he or she is most comfortable.
Vertical Rectilinear Movement of the Implanter
Vertical rectilinear movement of the implanter is extremely important and a fundamental concept. In the process of penetrating the skin with the implanter needle and coming back out, failure to move in a straight distance but rather making a curved motion causes more tissue damage and exerts pressure to the adjacent tissue leading to graft popping. A vertical rectilinear movement generates minimal pressure on the scalp tissue, resulting in less graft popping, less trauma, and ultimately better graft survival. (Supplementary Video 4) However, it is difficult to follow if not mastered. When placing grafts, arm movement should occur mainly at the shoulder, elbow, and wrist; movement at the finger and metacarpal joints should be limited. This not only reduces the pressure transferred to the hair follicle itself, but also reduces the incidence of pitting scars, which enables faster wound healing. Grafts must be transferred with the least trauma possible.11
Implanter Circulating System
Graft placement using implanters consists of three steps: loading, passing, and implantation. First, the nurse carefully loads the grafts into the implanters without causing any trauma to them. With a traditional circulating system, the nurse places a loaded implanter in the communication zone for the surgeon to pick up and use. However, this system is slow and inefficient because it requires the surgeon to remove his or her focus from the implantation site. Moreover, it requires a large degree of surgeon hand motion.
I use the 2-1-1 or 3-1-1 implanter circulating system in which one assistant and two or three loaders, respectively, pass and circulate implanters between the loaders and the surgeon.12 (Figure 2) With these systems, the surgeon’s eyes are fixed on the surgical field and hand movement is less than 5 cm. This reduces surgeon fatigue and enables fast and accurate graft placement. Accurate and fast movement and control prevent graft popping and bleeding during surgery. Here, hand–eye coordination is important. Accurate, fast, and delicate movements are possible only when the hands are within the line of vision. The passer stands right next to the surgeon. Depending on surgical team preference, the passer may be situated facing the surgeon. However, I prefer the passer stand beside the operator to read the angle and direction of graft insertion as well as the direction of the bevel. This allows the passer to adjust accordingly in real time. The passer removes the used implanter with the right hand while the left hand simultaneously passes a newly loaded implanter into the surgeon’s hand. Then, the left hand is immediately prepared with another newly loaded implanter (Supplementary Video 5). Assistants should check proper loading of the graft into the implanter tip and lightly push in any grafts that are protruding outside the bevel. Any improperly loaded implanters should not be handed to the surgeon. Instead, they should be exchanged for the next one.
 |
Figure 2 2(3)-1-1 system. Two or three loaders, passer and operator. |
Sequence of Graft Insertion
Order of implantation must be posterior to anterior and left to right (for right-handed surgeons). In general, the hair exit angle ranges from 30 to 40 degrees in the mid-scalp and 10 to 20 degrees along the anterior hairline.13 Therefore, push-out pressure that contributes to popping-out is much greater anteriorly. Grafts placed posteriorly are less affected by push-out pressure due to offset of the force vector. Furthermore, working from posterior to anterior prevents any bleeding from obscuring the immediate site of implantation. For right-handed surgeons, working from left to right is natural as it is also the direction most languages are written. In addition, progressing from right to left will cause the palm of the right hand to rub the grafts that have just been transplanted. With the left hand, the surgeon may hold gauze to wipe off blood or hold microforcep to press down on follicles to prevent graft popping, pick up dislodged grafts, or push in grafts that were not fully inserted in to the incision site.
Segmental Transplantation Timing Control Based on Duration of Epinephrine-Induced Vasoconstriction
Graft placement using sharp implanters is susceptible to bleeding because incision and insertion take place simultaneously. Therefore, hemostasis is important. The vasoconstriction effect of epinephrine lasts for approximately 30 to 40 minutes in tissue undergoing hair transplant surgery.14 Use of high-dose epinephrine mixed with lidocaine is not associated with shedding of the transplanted hair follicles.14,15 The vasoconstriction effect is dose-dependent and varies by scalp region. For example, the effect tends to quickly disappear from the midfrontal hairline because of the supraorbital artery.
The above factors must be considered during the process of graft insertion. Bleeding gradually increases after the vasoconstriction effect wears off. Moreover, the vasoconstriction response to epinephrine can decrease after repeated injections. Therefore, local anesthesia injections should be performed in a step-by-step fashion to cover only a region that can be implanted within 30 to 40 minutes. Of course, this depends on the number of prepared grafts and the size of the recipient area, which must be kept in mind when devising the surgical plan.
Gradual Angle and Direction Control
Abrupt changes in angle or direction can cause graft popping, injury to adjacent or previously placed grafts, and a see-through appearance of the scalp.16
Implanter Tip Size and Sharpness
The sharpest implanter tip possible should be used. As soon as the tip feels blunt or worn out, it should be replaced. Generally, a 0.6 mm diameter implanter tip is used for eyebrow and eyelash hair restoration. For 1-hair follicular unit (FU) transplantation, 0.6, 0.7, and 0.8 mm diameters may be used. For 2-hair FU transplantation, 0.9 or 1.0 mm may be used. Three- and 4-hair FU transplantation may be performed with 1.0 to 1.2 mm tips (Figure 3).
 |
Figure 3 Various size implanters. |
Choosing the right implanter size is very important.17,18 When the tip is too large for the graft, a “snug fit” will not occur and the grafts are more prone to graft popping, which can cause a suboptimal outcome. However, when the tip is too small for the graft, crushing or bending of hair follicles may occur during graft loading. The surgical staff must be educated to use standard sizes designated for 1-, 2-, 3-, and 4-hair FU transplantations and to flexibly select among them when loading grafts. It is beneficial to use implanter tips of various sizes.
Another consideration is that hair follicle thickness may vary in the same patient. For example, both 0.7 mm and 0.8 mm implanter tips are used for 1-hair FU grafts in men. In other words, the assistant selects a 0.7 mm implanter tip when loading a thinner single-hair follicle and a 0.8 mm tip for a thicker one.
Place the Bevel of Implanter Tip Anteriorly
Pointing the bevel forward reduces tip damage. The Rainbow implanterTM (Seson Medical company, Seoul, Korea) which I use, has a protruding structure on the body that is always positioned in the same direction as the bevel. In addition, the main body has two lines at the end, black on one side and red, orange, yellow, green, blue, or purple on the other. The color indicates implanter size. The black line is always positioned in the same direction as the bevel (Supplementary Video 6). Pointing the bevel forward also places the colored line in the surgeon’s line of vision, which enables the surgeon to check both the position of the bevel face and the implanter size (Supplementary Video 7).
Wide and Narrow Channel
Channel size is classified as narrow or wide. (Figure 4) FUT grafts are tear-drop shaped, while FUE grafts have reverse triangular shapes. (Figure 5) FUT grafts are dissected into follicular units after removing a strip, resulting in their resemblance to a cylinder or a water drop. In case of FUE, the skin is dissected around the hair follicle using a cylindrical punch, and the grafts are extracted by pulling out with forceps, thus taking on a triangular shape with less perifollicular fat tissue. So, wide channel implanters are used for FUE grafts and narrow channel implanters for FUT grafts. For narrow channel implanters, grafts are loaded to be completely enclosed in the lumen. For wide channel ones, they are loaded with the epidermis protruding through the lumen. Length of epidermis protruding out of wide channel is almost similar to the length of bevel. (Figure 6) Protruding epidermal caps act like a stopper to automatically control the incision depth (Supplementary Video 8).
 |
Figure 4 Wide channel and narrow channel implanters. |
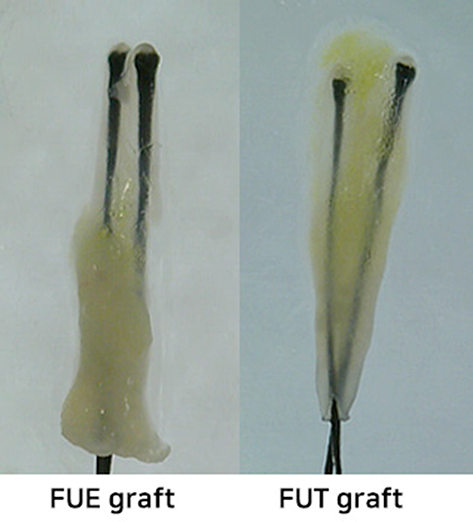 |
Figure 5 FUE graft and FUT grafts have different shape. |
 |
Figure 6 Length of epidermis protruding out of wide channel is almost similar to the length of bevel. |
Depth Control
The importance of proper depth control when transplanting hair follicles cannot be overemphasized.19 Grafts implanted at a shallow depth may fail to survive. An incision that is too deep causes soft tissue damage that is associated with scarring, delayed wound healing, and slower recovery of microcirculation. In addition, deeper incisions may result in severely curly hairs and pitting scars. Ultimately, proper depth control is the key factor for graft survival. The incision made to insert a hair graft should be just as long as the length of a hair follicle. Proper depth control is necessary to avoid full-depth incisions.
When performing FU transplantation with a narrow channel implanter, the surgeon must hold the implanter very lightly to make incisions that are approximately 50% to 70% of the total length of the needle. This is because the hair follicles must be loaded to be completely enclosed in the lumen. When penetrating the skin during graft insertion, hair follicles exposed in the bevel area may not be placed within the incision but bent outward and ultimately fail to survive. The bevel length is about 20–50% of the total needle length with some variations by manufacturer, size of the needle, and the average length of the hair follicles. Inserting the needle as deep as the full needle length causes unnecessary damage to the scalp tissue. Also, deeply placed grafts may develop into folliculitis or result in excessive scarring. Thus, one should avoid tightly gripping or making forceful insertions with the implanter. It is important to hold and insert gently by adjusting the force. A loose grip enables delicate motions using only three fingers: the thumb, index and middle fingers. For FUE grafts, wide channel sharp implanters are used. Grafts are loaded with the epidermis protruding to automatically help control incision depth (Figure 7).
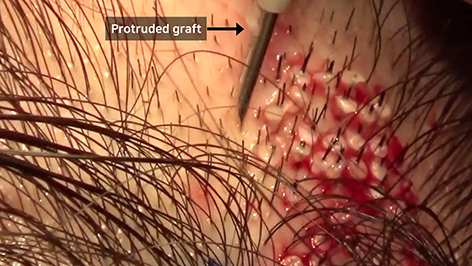 |
Figure 7 Epidermis protruding out of wide channel automatically controls the incision depth. |
Staff Training
Hair transplantation is a team effort. Satisfactory outcomes rely on performance of the surgeon and the assistants. The surgeon’s skill cannot compensate for sub-standard performance of the assistant team. Careful attention is required to ensure successful dissection of the harvested hair follicles and prevent dehydration or trauma to the grafts during graft loading. This requires continuous education and monitoring. With my team, senior and junior staff are grouped into pairs to form sub-teams to enable mentoring and monitoring of graft dissection and loading. In addition, the sub-teams cross-monitor each other.
Implantation Method Flexibility
As with any surgery, there is no single absolute way to perform hair transplant surgery. Grafts can be inserted using the forceps, implanter, and Dull Needle Implanter methods as well as others.20–22 (Table 1) A single patient may require application of more than one method based on regional scalp and individual hair characteristics. For example, if graft popping is occurring because of hard and rubbery skin or excessive bleeding is causing delay, slit incisions are made and grafts are placed after the bleeding stops. Either forceps or implanters may be used for insertion.
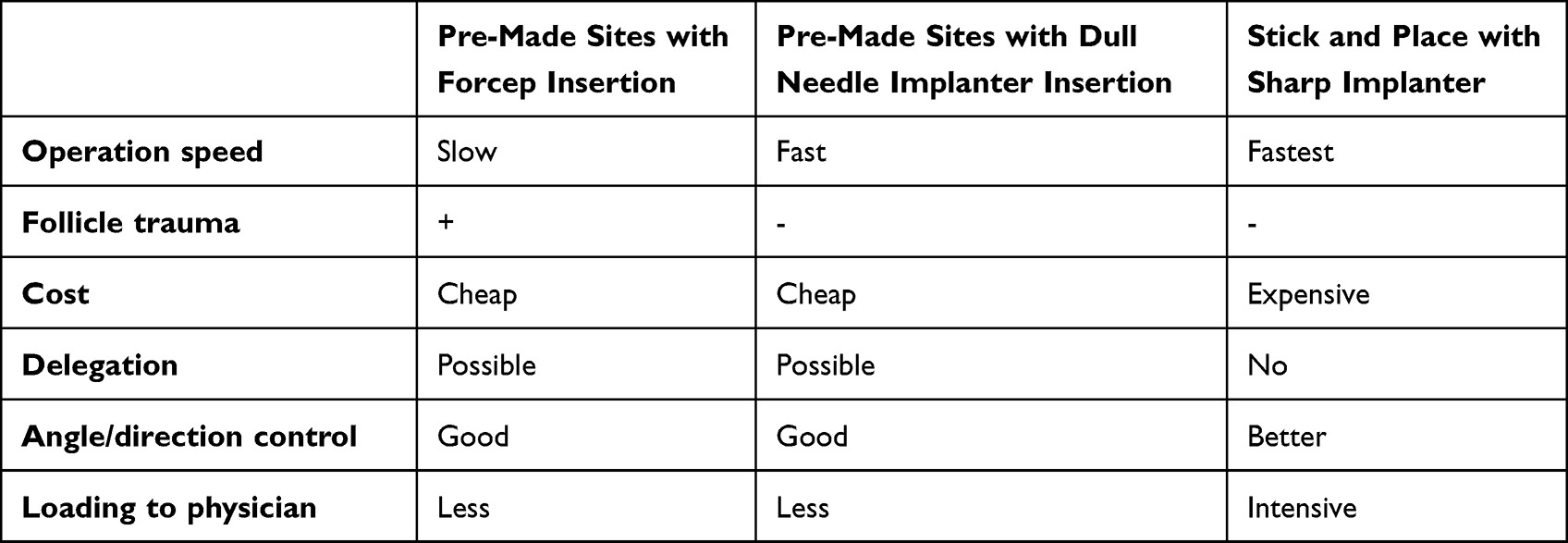 |
Table 1 Comparison by Graft Placing Method |
When the above rules are followed while using the sharp implanter method, graft popping is rather rare. Graft insertion of more than 50 to 60 grafts per square centimeter is possible without causing graft popping or impairing graft survival.
Conclusion
Natural results can be rapidly and efficiently achieved when using the sharp implanter method as described above.
Data Sharing Statement
In addition to photographic evidence showing interval changes that appear in the manuscript, complete medical records of the presented cases are stored in the treating clinic, in line with the standard of care.
Ethics and Consent
All procedures performed in studies involving human participants were in accordance with the Declaration of Helsinki (as was revised in 2013). Institutional Review Board approval was not required as this report was not a prospective or systematic investigation of hair transplantation procedure treatment but described general principles for routine hair transplantation practice. All patients provided informed consent for the case details and images to be published in this report.
Funding
No funding was received for this article.
Disclosure
JH Park owns patents and ownership interest of Rainbow implanter of Seson medical company. The remaining two authors have no conflicts of interest to declare.
References
1. Knudsen R. Controversies: forceps vs. implanters. Hair Transplant Forum Intl. 2014;24:57. doi:10.33589/24.2.0057
2. Devroye JM. A new multi-graft implanter system. Hair Transplant Forum Intl. 2018;28(3):100–101. doi:10.33589/28.3.0100
3. Speranzini M. Graft placement using the dull needle implanter (DNI) technique. Hair Transplant Forum Intl. 2017;27:52–56. doi:10.33589/27.2.0045
4. Mohebi P. A novel device to insert FU grafts into premade sites. Hair Transplant Forum Intl. 2018;28(4):146–148. doi:10.33589/28.4.0146
5. Kim JC. Graft implanters. In: Unger W, Shapiro R, editors. Hair Transplantation.
6. Lee SJ, Lee HJ, Hwang S, et al. Evaluation of survival rate after follicular unit transplantation using the KNU implanter. Dermatol Surg. 2001;27:716–720. doi:10.1046/j.1524-4725.2001.01029.x
7. Lee W, Lee S, Na G, Kim D, Kim M, Kim J. Survival rate according to grafted density of Korean one-hair follicular units with a hair transplant implanter: experience with four patients. Dermatol Surg. 2006;32(6):815–818. doi:10.1111/j.1524-4725.2006.32166.x
8. Lorenzo J, Vila X. Introduction to the use of implanters. Part I. Hair Transplant Forum Intl. 2011;4:121–122. doi:10.33589/21.4.0121
9. Lorenzo J, Vila X. Introduction to the use of implanters. Part II. Hair Transplant Forum Intl. 2011;5:170–171. doi:10.33589/21.5.0170
10. Park JH. A novel concept for determining the direction of implanted hair in hairline correction surgery in East Asian women. Arch Plast Surg. 2018;45(3):292–294. PMID: 29788691; PMCID: PMC5968325. doi:10.5999/aps.2017.01767
11. Park JH. Sharp implanter. In: True RH, Grag AK, Garg S, editors. Practical Guide to Hair Transplantation.
12. Park JH. Novel Implanter Technique That Enables More Than 1600 Grafts in 1 Hour with Dense Packing. ISHRS Video Library; 2013.
13. Unger WP. Recipient area hair direction and angle in hair transplanting. Dermatol Surg. 2004;30:829–836. doi:10.1111/j.1524-4725.2004.30250.x
14. Na YC, Park R, Jeong HS, Park JH. Epinephrine vasoconstriction effect time in the scalp differs according to injection site and concentration. Dermatol Surg. 2016;42(9):1054–1060. doi:10.1097/DSS.0000000000000845
15. Panchaprateep R. Does epinephrine influence post-surgical effluvium? In: Pathomvanich D, Imagawa K, editors. Practical Aspects of Hair Transplantation in Asians.
16. Park JH. See-through scalp appearance. Int J Dermatol. 2022;61(9):1165–1167. doi:10.1111/ijd.16118
17. Wolf BR. The art and craft of recipient site creation and graft placement. Hair Transplant Forum Intl. 2014;24:41,46–49. doi:10.33589/24.2.0041
18. Wolf BR. Cyberspace chat: post-operative inflammation: an interesting discussion about possible causes (incision and graft size, J hairs, placing techniques, implanters). Hair Transplant Forum Intl. 2016;26:106–109. doi:10.33589/26.3.0106
19. Hwang ST, Cotterill PC. Intra-patient graft length differenced influencing depth controlled incisions. Hair Transplant Forum Intl. 2012;22(117):122–123. doi:10.33589/22.4.0117
20. Bansal A, Sethi P, Kumar A, Sahoo AK, Das P. Use of implanters in premade recipient sites for hair transplantation. J Cutan Aesthet Surg. 2019;12(4):250–254. doi:10.4103/JCAS.JCAS_33_19
21. Speranzini M. FUE graft placement with dull needle implanters into premade sites. Hair Transplant Forum Intl. 2016;26(49):54–56. doi:10.33589/26.2.0049a
22. von Albertini C, von Albertini M. Does the use of implanters affect the quality of FUE grafts? Hair Transplant Forum Intl. 2016;27(3):96–98. doi:10.33589/27.3.0096
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Novel Follicular Unit Excision Device That Reduces Graft Injury and Improves Ergonomics in Hair Transplantation Surgery

Park JH
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2009-2019
Published Date: 3 August 2023