Back to Journals » Risk Management and Healthcare Policy » Volume 15
A Population-Based Study on the Prognostic factors and Efficacy of Adjuvant Chemotherapy in the Postoperative Stage for Patients with Stage IIA Non-Small Cell Lung Cancer
Authors Wang W, Teng F, Bu S, Xu W, Cai QC, Jiang YQ, Wang ZQ
Received 10 May 2022
Accepted for publication 17 August 2022
Published 25 August 2022 Volume 2022:15 Pages 1581—1592
DOI https://doi.org/10.2147/RMHP.S373510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Wei Wang,* Fei Teng,* Shi Bu, Wei Xu, Qing-Chun Cai, Yue-Quan Jiang, Zhi-Qiang Wang
Key Laboratory for Biorheological Science and Technology of Ministry of Education (Chongqing University), Chongqing University Cancer Hospital, Chongqing, 400030, China
*These authors contributed equally to this work
Correspondence: Yue-Quan Jiang; Zhi-Qiang Wang, Key Laboratory for Biorheological Science and Technology of Ministry of Education (Chongqing University), Chongqing University Cancer Hospital, No. 181 of Hanyu Road, Shapingba District, Chongqing, 400030, China, Tel +86 13708335256 ; +86 15215023098, Email [email protected]; [email protected]
Objective: This study aimed to design a nomogram survival prediction by means of the figures retrieved from the Surveillance, Epidemiology, and End Results (SEER) source bank, and to predict the overall survival (OS) of patients with stage IIA non-small cell lung cancer (NSCLC) after surgery.
Methods: Data for 4511 patients who had been diagnosed with postoperative stage IIA NSCLC were collected from the SEER databank, while information on 528 patients was acquired from the Chongqing University Cancer Hospital for the external validation cohort. The independent risk factors that affected the prognosis were identified using a multivariate Cox proportional hazards regression model (also used to conduct a nomogram). A survival analysis between the low- and the high-risk groups was performed using the Kaplan–Meier method. Furthermore, a subgroup analysis was conducted of the two groups using the Kaplan–Meier method to determine whether the patients had received adjuvant chemotherapy.
Results: The following five variables were integrated into the nomogram: sex (female: HR 1.73, 95% CI 0.64– 0.83), age (≥ 60: HR 1.61, 95% CI 1.39– 1.87), differentiation grade (grade II: HR 2.19, 95% CI 1.66– 2.88; grade III: HR 2.65, 95% CI 2.00– 3.51; grade IV: HR 3.17, 95% CI 1.99– 5.03), surgery (lobectomy: HR 0.72, 95% CI 0.59– 0.86), and lymph node resection (> 12: HR 0.82, 95% CI 0.70– 0.96). Furthermore, the patients selected were categorized into high- and low-risk groups. The OS rate was significantly lower in the high-risk group than in the low-risk group (P < 0.001). Finally, adjuvant chemotherapy was highly correlated with OS in the high-risk set (P = 0.035); however, adjuvant chemotherapy was not related to OS in the low-risk set.
Conclusion: A nomogram was created as a reliable, convenient scheme that could predict OS, and it was determined that the high-risk feature patients identified by the nomogram gained benefits from adjuvant chemotherapy.
Keywords: nomogram, stage IIA non-small cell lung cancer, adjuvant chemotherapy, OS prediction
Introduction
Lung carcinoma is a malicious tumor, affecting people globally, of which the incidence and mortality rate rank first among cancers.1,2 Over 80% of pulmonary cancer cases are non-small cell lung cancer (NSCLC).3 The overall five-year survival rate of NSCLC is only about 15%,4 posing a significant public health threat. Therefore, appropriate adjuvant treatment for lung cancer after surgery is important for the prognosis.5,6 Stage I lung cancer usually does not require postoperative adjuvant therapy due to its good prognosis. Adjuvant chemotherapy or even combined with radiotherapy is routinely recommended for patients with intermediate stage and above lung cancer. However, stage IIA lung cancer is at the junction of early-stage lung cancer and intermediate-stage lung cancer, and whether it can benefit from postoperative adjuvant chemotherapy is still controversial.7 According to the 8th edition of NCCN guidelines, conventional adjuvant chemotherapy is not recommended after surgery for stage IIA lung cancer, and adjuvant chemotherapy is only suitable for patients with high risk factors, such as pleural invasion, tumors larger than 4 cm, perineural invasion, and vascular invasion.
The single risk factor method may not be sufficiently reliable to screen patients with postoperative stage IIA NSCLC who need adjuvant chemotherapy, resulting in possible overtreatment or undertreatment. Therefore, it is important to develop a prognostic model that incorporates more risk factors to accurately identify high-risk groups after surgery for stage IIA lung cancer, and to assess whether patients can benefit from adjuvant chemotherapy based on this model. Currently, the nomogram is considered an effective instrument to evaluate risks by considering vital clinical and pathological features in cancer diagnoses.8,9 By creating a simple and efficient evaluation structure, these well-used graphs could help practitioners and patients implement an appropriate and personalized therapeutic regimen. Additionally, the nomogram outweighs the traditional Classification of Malignant Tumors (TNM) in forecasting cancer categories.9 Moreover, the nomogram could guide postoperative chemotherapy for patients with stage IIA NSCLC.
Accordingly, this study’s aim was to create a nomogram to accurately project the overall survival (OS) of patients with mature stage IIA NSCLC and provide evidence of the adjuvant chemotherapy benefits based on existing pathological factors and data obtained from the Surveillance, Epidemiology, and End Results (SEER) records.
Methods
Patient Assortment and Data Processing
Patient data were obtained from the SEER source bank, including 18 registries via the SEER*Stat version 8.3.8 software (https://seer.cancer.gov/). The post-surgery information on all individuals was collected. Extraction criteria included the following conditions: a disease location in the lung and bronchus, a positive histology diagnosis, and a diagnosis year between 2007 and 2016. The following variables were evaluated: patient identification, age, race, sex, marital status (an unmarried status composed of widowed, single, divorced, and separated), insurance code, microanatomy grade, tumor magnitude, surgery, American Joint Committee on Cancer (AJCC) stage, transmutative sites, visceral pleural invasion (VPI), irradiation, chemotherapy, tumor-specific mortality, all-cause fatality, and survival time. These patients were treated as the training cohort.
Inclusion criteria included the following: (1) a pathological stage IIA defined as the 8th-version-AJCC/T2bN0M0; (2) historical surgical care; (3) valid OS follow-up figures. Exclusion criteria included the following: (1) an extra malignant tumor; (2) an upfront surgery record; (3) a survival time within one month after surgery. Finally, 4511 eligible patients were enrolled for this study, but seventeen percent (767 of 4511) of the total was missing; it was presumed to be missing randomly and therefore imputed with the manifold imputation of the chained equations model according to the datum characteristics. Ten imputed data sets were created, and the results were pooled using the “mice” function of the mice R package.
The external validation cohort data originated from 528 patients with stage IIA NSCLC who had undergone surgical treatment between April 2008 and February 2020 at the Chongqing University Cancer Hospital. The inclusion and exclusion criteria are the same as those of the training cohort to ensure that there is no selection bias between the two groups of data.
This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics committee of Chongqing University Cancer Hospital (Chongqing, China). Informed consent obtained from the study participants prior to study commencement.
Construction of the Nomogram
In regard to the training cohort, a univariate Cox regression inquiry was used, and multivariate analysis was implemented based on major consequences (P < 0.1) from the univariate analysis. According to the results of the multivariate analysis, the hazard ratio (HR) and related 95% confidence interval (CI) that were identified and influencing factors in the chart were included to predict the possibility of one-, three-, and five-year survival rates after surgical treatment in patients with stage IIA NSCLC.
Discrimination and Standardization of the Nomogram
The graph was evaluated internally for the training group and externally for the validation group. The discriminative ability of this nomogram was measured by means of a concordance curve (C-index), which has the same area under the curve (AUC).10,11 The C-index was set with a range of 0.5 to 1, with a C-index of 1 suggesting a perfect anticipation and a C-index of 0.5 considered a random assignment. Moreover, time-based receiver operating characteristic (ROC) curves and consistent AUCs were established at one-, three-, and five-year points to determine its prediction accuracy.
A standardization curve was constructed to present the link between the tangible consequences and the projection analysis.12 We used 1000 bootstrap samples to assess both the discrimination and calibration. A commonly used curve is a line with a slope of 1 across the original point of the reference axis. The closer the standard curve to the predicted calibration curve, the greater the predictive power.
Diverse Risk Groups Graded According to the Revised Nomogram
The linear predictor of each individual was created according to the model’s risk factors, which was regarded as a covariate in the Cox model. The cut-off point for the hazard level grading was calculated via the “surv_cutpoint” of the survminer R package. The survival analysis was performed using the Kaplan–Meier method, and dissimilarities between low- and high-risk survival were measured using the Log rank test.
The Predictive Value of the Adjuvant Regimen Among High-Risk Groups
Independent risk elements were identified through multivariate analysis and were included in the subgroup study. The analysis was stratified according to whether the patients had received adjuvant chemotherapy in the high-risk groups and was evaluated to determine the survival differences between the two experimental groups in line with the Kaplan–Meier survival curve.
Sensitivity Analyses
Two sensitivity analyses were conducted as follows: (1) all analyses were repeated using the raw data, of which missing data were not imputed by multiple imputation (4511 patients); (2) the Fine and Gray competing risk model for fatality risk analysis was applied.11 All analyses were performed using the R software (version 4.0.1; https://www.r-project.org/). A two-sided P value of <0.05 was regarded as statistically substantial.
Results
Patient Features
After reviewing data collected from the SEER database, 4511 patients who were diagnosed with stage IIA NSCLC after surgery between 2007 and 2016 were enrolled in this study; these patients constituted the training cohort. In addition, 528 patients with stage IIA NSCLC after surgery between April 2008 and February 2020 at the Chongqing University Cancer Hospital were enrolled as the external validation cohort. Table 1 shows the clinicopathological characteristics and demographic data of the two groups. In the training cohort, the median age of the population was 68 (61–75) years old, and the stage IIA NSCLC cases displayed the following characteristics: female (53.2%), married (57.8%), white (82.6%), upper lobe (62.4%), right (59.6%), grade II (12.6%), and adenocarcinoma (57%). Patient features were similar between the training set and the validation set.
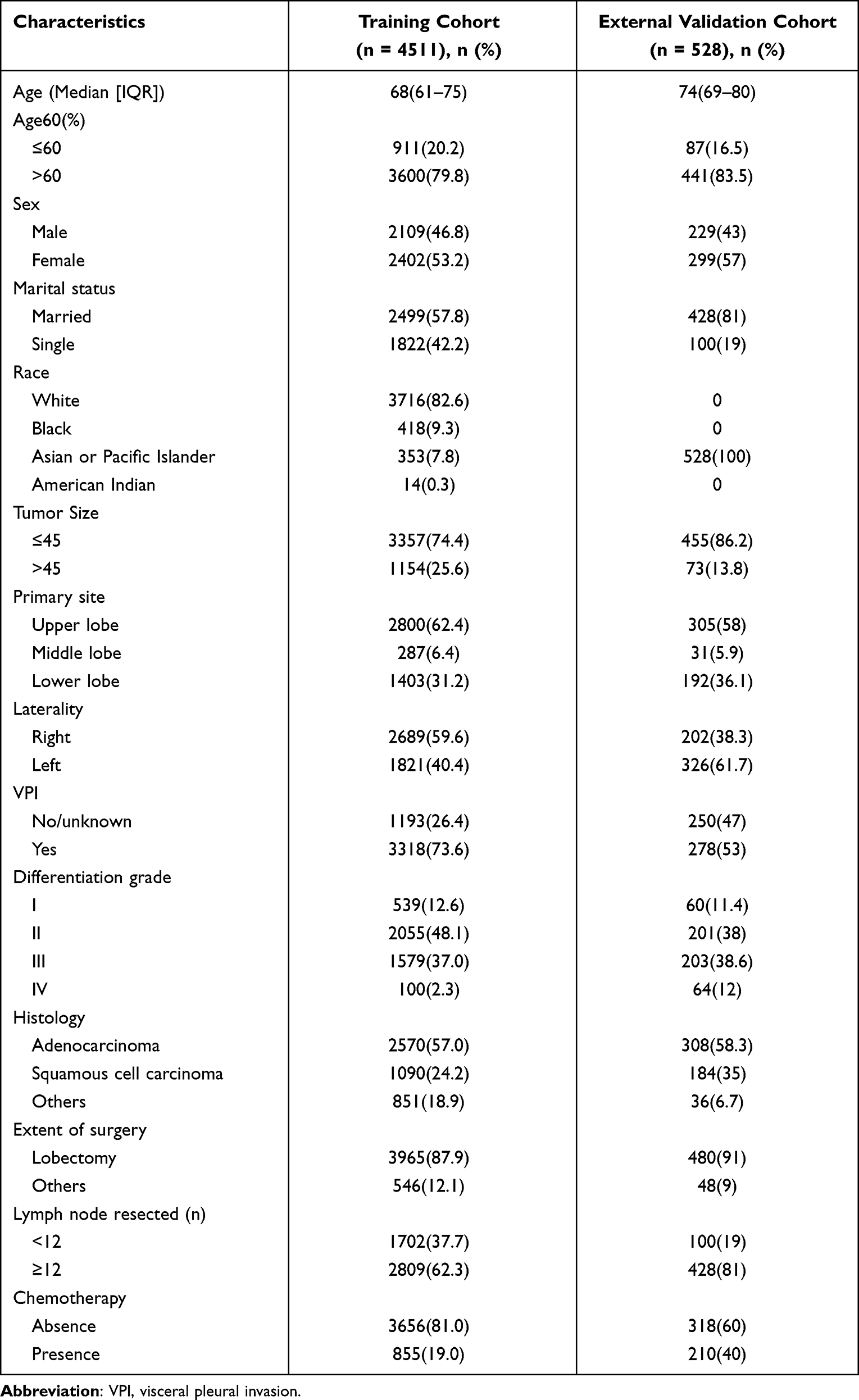 |
Table 1 Demographics and Clinicopathologic Characteristics of the Training and External Validation Cohort |
Prognostic Predictors in the Training Set
The univariate analysis determined that age, gender, race, VPI, differentiation grade, histology, extent of surgery, lymph node resection, and chemotherapy were potentially associated with the OS (P≤0.1). Conversely, marital status, tumor size, primary site, and laterality were insignificant (P > 0.1). According to the result of the univariate evaluation, the following eight risk factors were entered into the multivariate Cox regression analysis: age (≥60: HR 1.61, 95% CI 1.39–1.87, P < 0.001), gender (female: HR 1.73, 95% CI 0.64–0.83, P < 0.001), differentiation grade (grade II: HR 2.19, 95% CI 1.66–2.88, P < 0.001; grade III: HR 2.65, 95% CI 2.00–3.51, P < 0.001; grade IV: HR 3.17, 95% CI 1.99–5.03, P < 0.001), histology (squamous cell carcinoma: HR 1.13, 95% CI 0.97–1.32, P = 0.127; others: HR 1.07, 95% CI 0.89–1.29, P = 0.457), extent of surgery (lobectomy: HR 0.72, 95% CI 0.59–0.86, P < 0.001), lymph node resection (>12: HR 0.82, 95% CI 0.70–0.96, P = 0.01), and chemotherapy (presence: HR 0.84, 95% CI 0.70–1.01, P = 0.08). Table 2 displays more details related to the univariate and multivariate analysis.
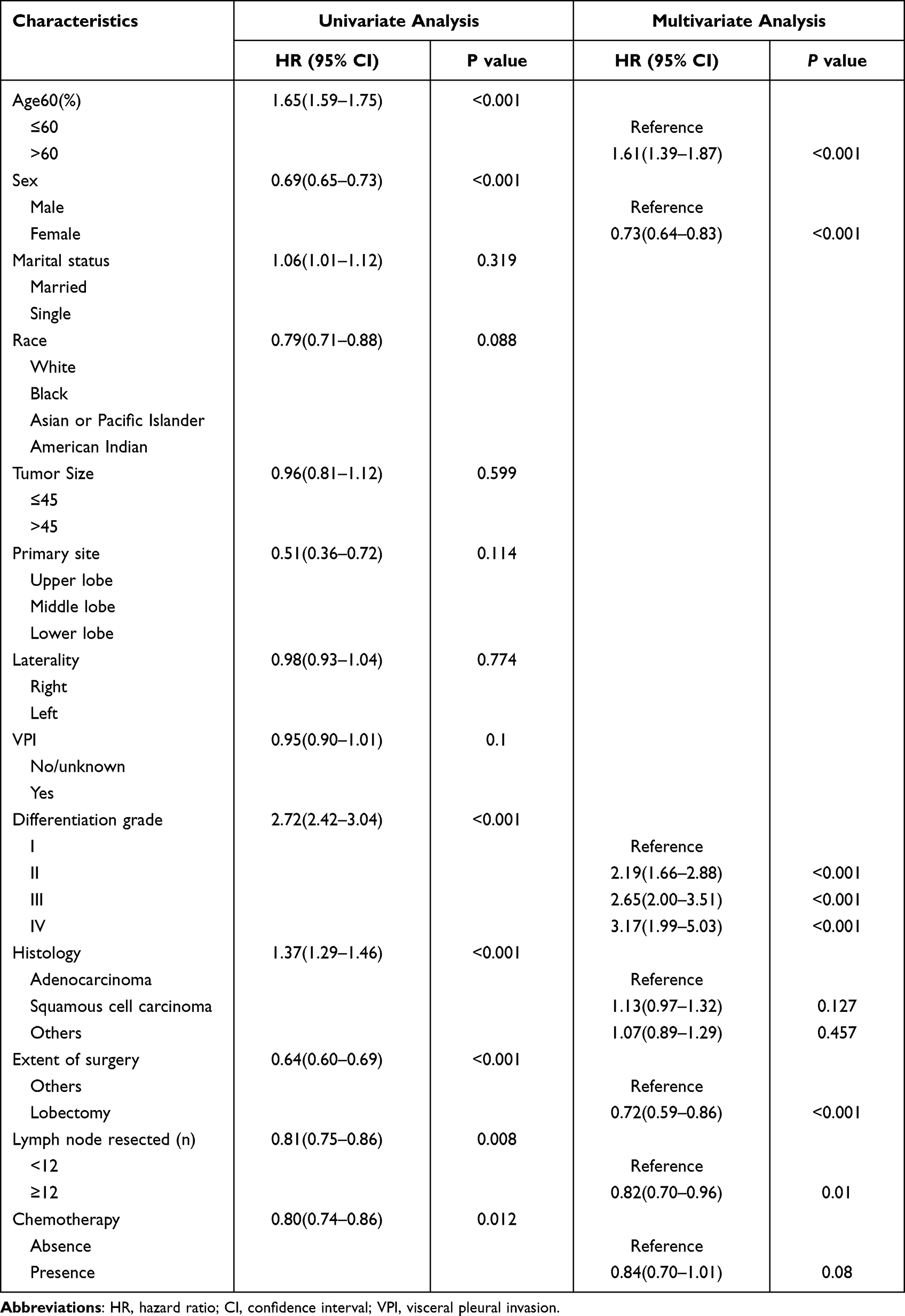 |
Table 2 Selected Factors in the Training Cohort for Building the Model by Univariate and Multivariate Cox Regression Analysis |
The OS Prognostic Nomogram
A nomogram model was developed based on five selected prognostic predictors for predicting the one-, three-, and five-year OS rates (Figure 1). The nomogram illustrated the points for each independent risk factor ranging from 0 to 100. The total score was estimated and placed on the total point scale, which corresponded to the prediction probability. Then, the one-, three-, and five-year OS for each patient were estimated.
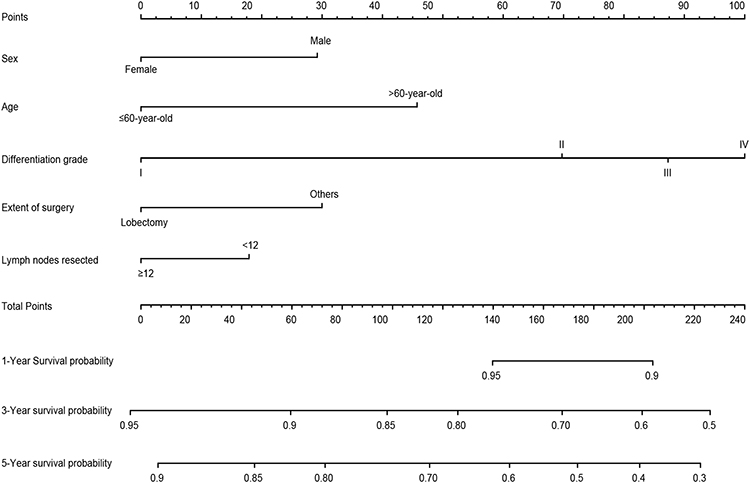 |
Figure 1 Nomogram of 1-, 3-, 5-year OS. |
The Nomogram’s Calibration and Discrimination
Calibration splines illustrated great consistency between the predicted and detected results for the one-, three-, and five-year OS in the two cohorts (Figure 2). This study’s nomogram featured favorable prognostic accuracy and medical applicability with C-index values of 0.638 in the training cohort and 0.645 in the external validation cohort. The stated index data were equivalent to the AUC values aligned with the ROC curve analysis (0.69, 0.64, 0.62 in the training cohort and 0.66, 0.63, 0.65 at one, three, and five years in the external validation cohort, respectively) (Figure 3).
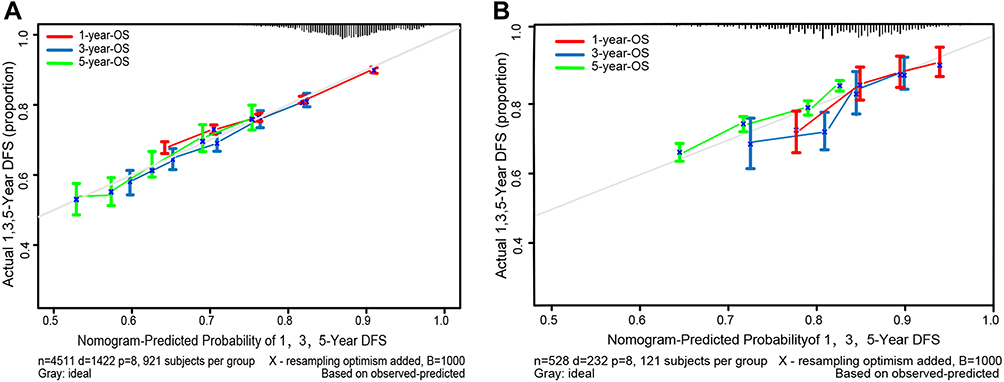 |
Figure 2 Calibration curves for predicting OS at 1-, 3-, 5-year in the training cohort (A) and the external validation cohort (B). |
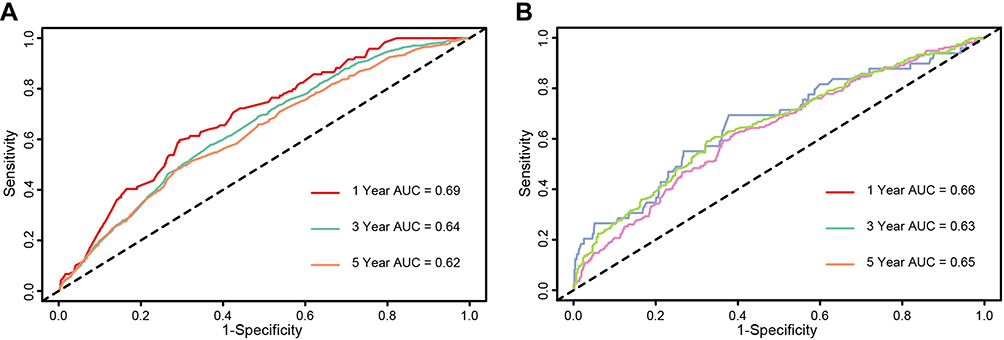 |
Figure 3 ROC curves and AUCs at 1-, 3-, 5-year in the training set (A) and the external validation cohort (B) were adopted to evaluate the prognostic accuracy. |
Low- and High-Risk Group Survival Analysis
The cut-off value of the linear predictors was 0.23, according to the coefficients of the model (Figure 4), which was regarded as a covariate in the Cox matrix. All samples in the training set were categorized into high- and low-risk units based on a cut-off value of 0.23.
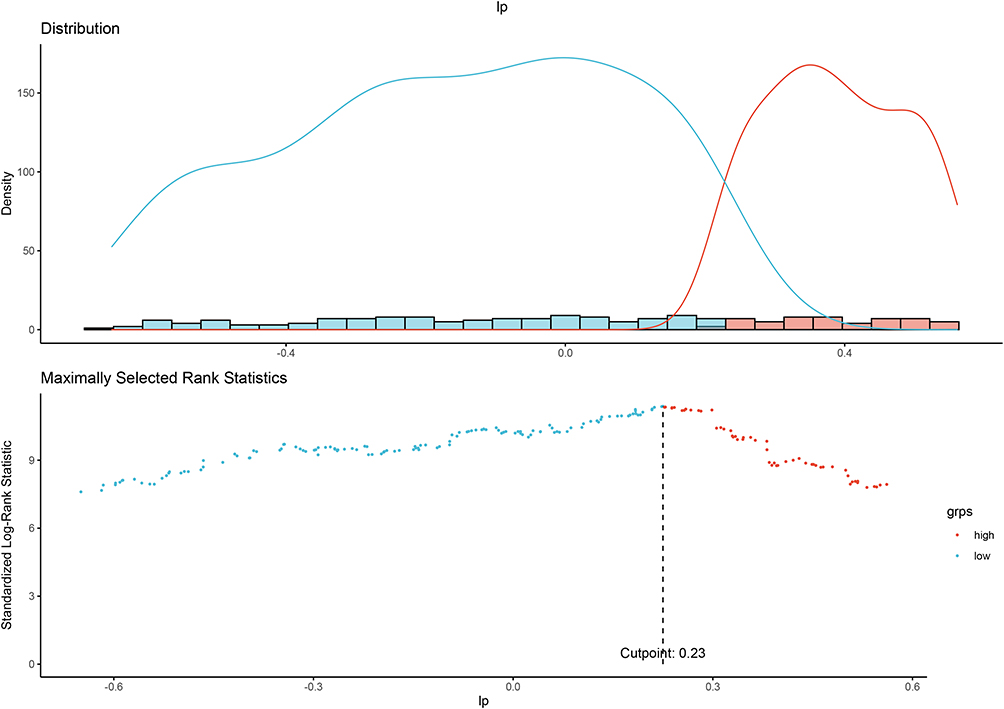 |
Figure 4 The entire samples in the training set and the validation set were categorized separately into a high- and a low-risk unit based on the cut-off value of 0.23. |
The survival rate was higher in the low-risk set than in the high-risk set (P < 0.001) (Figure 5A). Furthermore, we retrieved data on major survival differences between the two experimental groups in the external validation set (P < 0.001) using the identical cut-off value (Figure 5B).
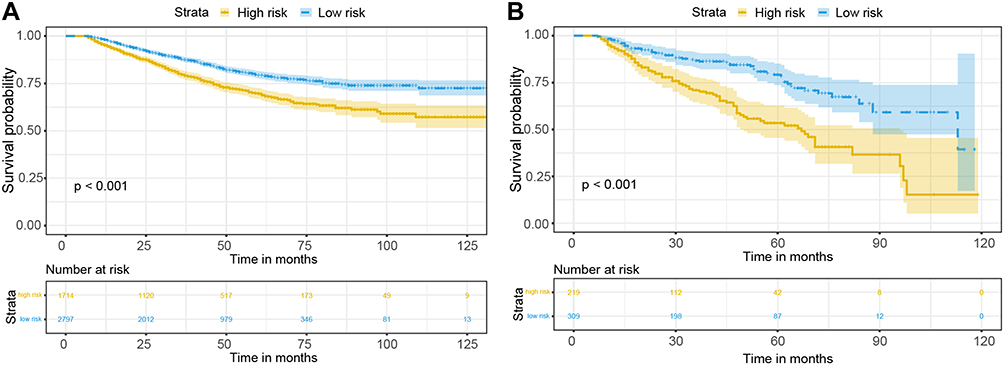 |
Figure 5 K-M plots of survival for risk stration in the training cohort (A) and the external validation cohort (B). |
In addition, there were considerable OS differences between the two risk-rated groups in the training cohort (P < 0.001) (Figure 6A) and the external validation cohort (P < 0.001) (Figure 6B); the Fine and Gray matrix (with censoring) was used as the competing risk item.
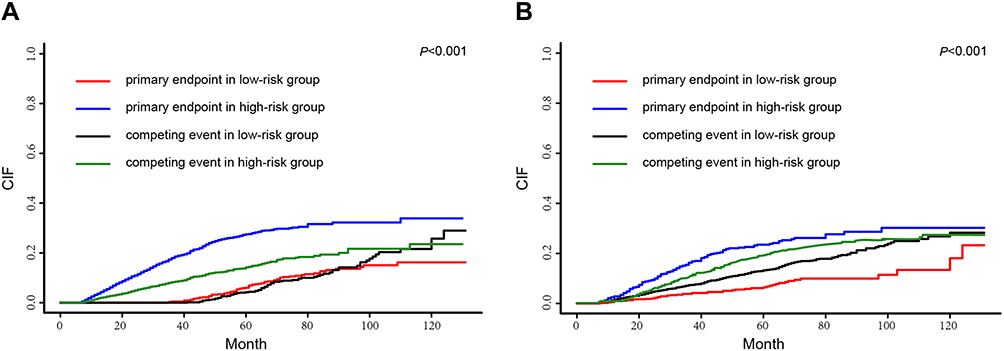 |
Figure 6 Using the Fine (A) and Grey matrix (B) to explain competing risks owing to mortality. |
The Predictive Effect of Adjuvant Chemotherapy Determined in the Subgroup Analysis
The low- and high-risk groups also supported a subgroup analysis for the training set based on whether they had received adjuvant chemotherapy. The analysis showed that adjuvant chemotherapy proved beneficial within the high-risk groups in the training cohort (P = 0.035) (Figure 7A) and in the external validation cohort (P = 0.02) (Figure 7B), as it resulted in a better OS rate; however, the patients in the low-risk group benefitted little from the adjuvant chemotherapy in the training set (P = 0.57) (Figure S1A). So does it among external validation set (P = 0.88) (Figure S1B).
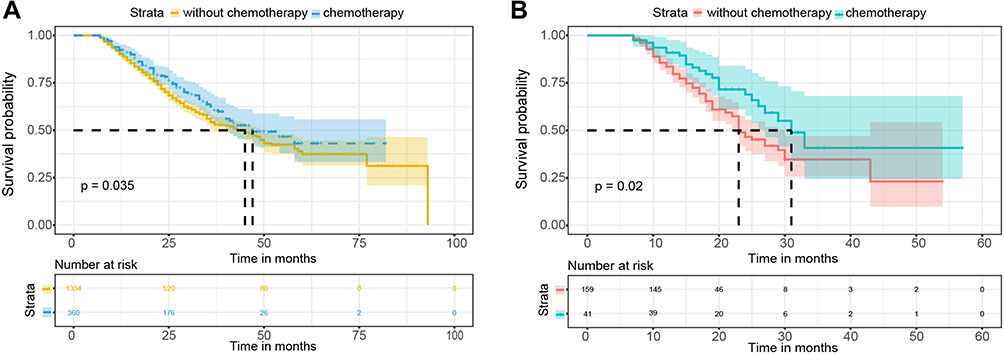 |
Figure 7 K-M plots of survival for high-risk subgroup in the training cohort (A) and the external validation cohort (B). |
Discussion
The majority of postoperative patients diagnosed with stage IIA NSCLC had received a favorable prognosis, however, some of them did not reach the expected OS. It is impractical to expect clinicians’ prediction of OS by solely using TNM staging to identify multiple potential prognostic factors. The NCCN guidelines13 state that only the post-surgery patients at high-risk with stage IIA should receive adjuvant chemotherapy, but it remains difficult for physicians to identify personalized risk factors and make prognostic stratifications. A more accurate prognosis prediction for stage IIA NSCLC is highly necessary; therefore, we have established a nomogram for long-term survival calculation for patients with stage IIA NSCLC after surgery based on selected independent risk factors. In this study, patients were divided into high- and low-risk groups based on risk scores, and in a subgroup analysis, they were further stratified into two groups according to whether they had been treated with an adjuvant regimen. The results verified that high-risk patients saw an obvious benefit from adjuvant chemotherapy.
The training set was obtained from the SEER database, and the external validation set was obtained from Chongqing University Cancer Hospital, renowned for having the largest cancer treatment scale in the southwestern part of China. The cases selected in the set were typically and universally applicable, which represented the broader Chinese population diagnosed with stage II NSCLC. With respect to nomogram calibration, our study resulted in a reasonable concordance between the training and the external validation set. The C-indexes displayed in the abovementioned two cohorts of 0.638 and 0.645, respectively, seemed to show a likeness to the figures stated in previous findings,14–16 even though they were not very high. The main reasons were analyzed. (1) Stage IIA lung cancer belongs to a relatively low-risk population, and the impact of risk factors in this population is not very prominent; (2) This study starts from the clinical question of whether patients with stage IIA lung cancer need adjuvant chemotherapy after surgery. Looking for the most easily collected risk factors in clinical work to guide patients with postoperative adjuvant chemotherapy, and due to the limitations of clinical information in the SEER database, current research hotspots such as gene mutation and epigenetics have not been included for model construction. Risk factors The limited selection is the main reason for the unsatisfactory C index; (3) The principle behind the most commonly used TNM staging in clinical practice is the prognostic model, and its predictive ability C index is usually only about 60%.17 However, its simplicity, practicality and universality do not affect its wide clinical application. The prognostic model constructed in this study has higher prognostic value than the traditional TNM staging. More importantly, it can effectively distinguish whether patients with stage IIA lung cancer can benefit from adjuvant chemotherapy, so it has high clinical application value.
In this study, univariate and multivariate evaluation were used to pinpoint five neutral forecast elements, including sex, age, differentiation grade, extent of surgery, and lymph node resection. The effectiveness of these five independent risk factors matched the outcomes in previous studies, further stating that an older age was considered as an independent risk factor that can affect the OS for patients with NSCLC.16–19 Additionally, the lung cancer mortality rate was significantly higher in males than in females.20,21 This is related to the genetic mutation between men and women. It is well known that the genetic mutation of non-smoking women is significantly higher than that of smoking men. With the rapid development of molecular targeted drugs, patients with genetic mutations can benefit more. Pathological grading was discovered to be a crucial independent predictor for OS, which was also similar to previous reports. The higher the pathological grade, the greater the malignancy of the tumor and the worse the prognosis. Therefore, the pathological grade is an independent risk factor in the prognosis of most malignant tumors. Although a sublobectomy is not inferior to a lobectomy regarding OS among patients with lung cancer in the early stage, at present, a lobectomy combined with an organized mediastinal lymphadenectomy is regarded as the procedure of choice.22,23 In our study, a lobectomy was related to a more obvious OS than other procedures, including a triangle-shaped resection, pneumonectomy, and segmentectomy. Moreover, a significant difference was observed in the OS contingent upon the number of lymphocytes resected. If the number was over 12, the OS varied greatly; this is in line with a previous analysis reporting that people with lung cancer would have a better chance of survival once there were as many as 11 lymph nodes harvested.16,24 Our study states that lymph node assessment was essential for precise staging and prognosis.
Although the influence of the NCCN staging system on prediction is quite important, it may not comprehensively predict the prognosis. Therefore, in this study, we developed a nomogram according to the five independent prognostic factors and separated the patients into high- and low-risk groups using linear predictors. In the low-risk category, the survival rate of the patients was higher than in the high-risk category. Furthermore, we verified the significant survival difference between the two groups by using the Fine and Gray model, with death as the competing risk item. Our study revealed that adjuvant chemotherapy was not an obvious independent risk factor for stage IIA NSCLC. A certain number of records proved that an adjuvant regimen was not associated with a better chance of survival for NSCLC in the early stage.25 Conversely, some studies indicated that early-stage NSCLC could benefit from postoperative adjuvant chemotherapy. These findings may differ due to the high-risk factors for cancer-related death in patients with early-stage NSCLS, such as vascular invasion, visceral pleural infiltration, and poor differentiation.26 Currently, a postoperative adjuvant regimen is only recommended for people suffering from stage IIA lung cancer with high-risk factors.13 Thus, we calculated the linear predictor of each patient and selected the high-risk patients using the “surv_cutpoint” function of the survminer R package. The results proved that adjuvant chemotherapy was correlated with a better OS in the high-risk group, while it played a less important role in the low-risk group. Therefore, the patients categorized in the high-risk group by our nomogram were supposed to receive adjuvant chemotherapy.
It has been verified that VPI is a prognostic risk element for patients with lung cancer.27,28 Based on the eighth version of the TNM classification, VPI was regarded as a T2 influencing element irrespective of tumor size. Regarding VPI, some tumors less than 3 cm in diameter were upstaged to T2. However, in our study, we did not find that VPI correlated with the prognosis in either cohort. An explanation for this result may be that VPI is more common in advanced lung cancer, and the VPI-related diagnosis in NSCLC varied depending on the size of the lumps. A report showed that the existence of VPI was not obviously correlated with the prognosis for a tumor that is smaller than 5 cm.29
To our knowledge, the nomogram was the first tool designed for the OS prediction in people who suffer from stage IIA pulmonary carcinoma based on the SEER database and, with long-lasting tracking, we verified it with an external validation set. The calibration curves exhibited great consistency between the practical observations and the predictive outcomes. To a great extent, the conventional TNM system considers stage IIA lung cancers as a whole and cannot stratify cases into various risk subgroups. Thus, the nomogram could assist clinicians in predicting the individualized OS of patients with postoperative stage IIA lung cancer by means of a highly cost-efficient risk score system. Moreover, the scoring system could help in selecting high-risk patients who should receive chemotherapy to achieve a better chance of survival and protect low-risk patients from physical injuries due to unnecessary chemotherapy.
Similar to other reports based on the SEER database, there were some limitations to our study. First, this was a retrospective study, which could have caused an inevitable bias. Second, some important prognostic factors, such as the surgical margin status, genotype characteristics, smoking status, family history of lung cancer, vascular invasion, and nerve invasion, as well as a history of medicine use, were not available in the SEER source bank. In addition, the SEER database lacked sufficient information on disease-free survival, which correlates with adjuvant regimens for stage IIA NSCLC with high-risk elements.30 In the years to come, we expect that an increasing number of potential prognostic factors will be entered into the nomogram to acquire a more accurate prediction power. Additionally, in this study, the C-index in the nomogram was not convincing, because a high predictive ability does not ensure suitability for medical treatment. It is convenient to make a personal survival forecast by using the nomogram, considering that all the information that is required in the nomogram is easy to get in clinical data.
Conclusions
In this study, we created a nomogram as a reliable, convenient scheme that could predict the OS and select individual treatments for patients with stage IIA NSCLC after surgery. The high-risk feature patients identified by the nomogram did gain benefits from adjuvant chemotherapy. In the future, we hope that further research on this topic will corroborate our findings.
Abbreviations
OS, overall survival; NSCLC, non-small-cell lung cancer; SEER, Surveillance, Epidemiology & End Results; NCCN, National Comprehensive Cancer Network; TNM, tumor node metabolism; AJCC, American joint Committee on Cancer; VPI, Visceral pleural invasion; HR, hazard ratio; CI, confidence interval; AUC, the area under the curve; rROC, receiver operating characteristic; NCCN, National Comprehensive Cancer Network; DFS, disease-free survival.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics committee of Chongqing University Cancer Hospital (Chongqing, China).
Funding
This work was supported by Chongqing Research Institute Performance Incentiveand Guidance SpecialKey Project (No.cstc2019jxjl130005) and Key Technology Project for Prevention and Control of Major Diseases in Chongqing (No. 2019ZX002).
Disclosure
The authors declare no competing interests.
References
1. Hu B, Deng T, Ma H., et al. Deubiquitinase DUB3 Regulates Cell Cycle Progression via Stabilizing Cyclin A for Proliferation of Non-Small Cell Lung Cancer Cells. Cells. 2019;8(4):297. doi:10.3390/cells8040297
2. Yang Q, Zhang P, Wu R, Lu K, Zhou H. Identifying the Best Marker Combination in CEA, CA125, CY211, NSE, and SCC for Lung Cancer Screening by Combining ROC Curve and Logistic Regression Analyses: is It Feasible? Dis Markers. 2018;2018:2082840. doi:10.1155/2018/2082840
3. Zhou X, Xu X, Gao C, Cui Y. XIST promote the proliferation and migration of non-small cell lung cancer cells via sponging miR-16 and regulating CDK8 expression. Am J Transl Res. 2019;11(9):6196–6206.
4. Jiang Q, Xing W, Cheng J, Yu Y. Knockdown of lncRNA XIST Suppresses Cell Tumorigenicity in Human Non-Small Cell Lung Cancer by Regulating miR-142-5p/PAX6 Axis. Onco Targets Ther. 2020;13:4919–4929. doi:10.2147/OTT.S238808
5. Arriagada R, Bergman B, Dunant A, Le Chevalier T, Pignon J, Vansteenkiste J. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med. 2004;350(4):351–360.
6. Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer. N Eng j Med. 2005;352(25):2589–2597. doi:10.1056/NEJMoa043623
7. Douillard J, Rosell R, De lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): a randomised controlled trial. Lancet Oncol. 2006;7(9):719–727. doi:10.1016/S1470-2045(06)70804-X
8. Han DS, Suh YS, Kong SH, et al. Nomogram predicting long-term survival after d2 gastrectomy for gastric cancer. J Clin Oncol. 2012;30(31):3834–3840. doi:10.1200/JCO.2012.41.8343
9. Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J clin oncol. 2013;31(9):1188–1195. doi:10.1200/JCO.2012.41.5984
10. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;14(143):29–36. doi:10.1148/radiology.143.1.7063747
11. Mori S. Comment on: a review of the use of time-varying covariates in the Fine-Gray subdistribution hazard competing risk regression model by Peter C. Austin Aurelien Latouche Jason P Fine Stat Med. 2020;39(20):2689–2691.
12. Liu A, Hou F, Qin Y, et al. Predictive value of a prognostic model based on pathologic features in lung invasive adenocarcinoma. Lung Cancer. 2019;131:14–22. doi:10.1016/j.lungcan.2019.03.002
13. Ettinger D, Aisner D, Wood D, et al. NCCN Guidelines Insights: non-Small Cell Lung Cancer, Version 5.2018. J National Comprehensive Cancer Network. 2018;16(7):807–821. doi:10.6004/jnccn.2018.0062
14. Zeng Y, Mayne N, Yang CJ, et al. A Nomogram for Predicting Cancer-Specific Survival of TNM 8th Edition Stage I Non-small-cell Lung Cancer. Ann Surg Oncol. 2019;26(7):2053–2062. doi:10.1245/s10434-019-07318-7
15. Liang W, Zhang L, Jiang G, et al. Development and validation of a nomogram for predicting survival in patients with resected non-small-cell lung cancer. J Clin Oncol. 2015;33(8):861–869. doi:10.1200/JCO.2014.56.6661
16. Zuo Z, Zhang G, Song P, et al. Survival Nomogram for Stage IB Non-Small-Cell Lung Cancer Patients, Based on the SEER Database and an External Validation Cohort. Ann Surg Oncol. 2021;28(7):3941–3950. doi:10.1245/s10434-020-09362-0
17. Sun H, Liu M, Yang X, Ren Y, Dai H, Wang C. Construction and validation of prognostic nomograms for elderly patients with metastatic non-small cell lung cancer. Clin Respir J. 2022;16(5):380–393. doi:10.1111/crj.13491
18. Sozzi G, Boeri M, Rossi M, et al. Clinical utility of a plasma-based miRNA signature classifier within computed tomography lung cancer screening: a correlative MILD trial study. J Clin Oncol. 2014;32(8):768–773.
19. Sozzi G, Boeri M, Rossi M, et al. Clinical utility of a plasma-based miRNA signature classifier within computed tomography lung cancer screening: a correlative MILD trial study. J Clin Oncol. 2014;32:768–773.
20. Naliganti C, Valupadas C, Akkinepally RR, Eesam S. Evaluation of drug utilization in cardiovascular disease at a teaching and referral hospital in Northern Telangana. Indian J Pharmacol. 2019;51(5):323–329. doi:10.4103/ijp.IJP_743_17
21. Polak M, Genowska A, Szafraniec K, Fryc J, Jamiołkowski J. Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases. Int J Environ Res Public Health. 2019;16(10):1791. doi:10.3390/ijerph16101791
22. Nakamura K, Saji H, Nakajima R, et al. A Phase III randomized trial of lobectomy versus limited resection for small-sized peripheral non-small cell lung cancer (JCOG0802/WJOG4607L). Jpn J Clin Oncol. 2010;40(3):271–274. doi:10.1093/jjco/hyp156
23. Suzuki K, Saji H, Aokage K, et al. Comparison of pulmonary segmentectomy and lobectomy: safety results of a randomized trial. J Thorac Cardiovasc Surg. 2019;158(3):895–907. doi:10.1016/j.jtcvs.2019.03.090
24. Dai J, Liu M, Yang Y. Optimal Lymph Node Examination and Adjuvant Chemotherapy for Stage I Lung Cancer. J Thorac Oncol. 2019;14(14):1277–1285. doi:10.1016/j.jtho.2019.03.027
25. Heon S, Johnson BE. Adjuvant chemotherapy for surgically resected non-small cell lung cancer. J Thorac Cardiovasc Surg. 2012;144(3):S39–42. doi:10.1016/j.jtcvs.2012.03.039
26. Jang HJ, Cho S, Kim K, Jheon S, Yang HC, Kim DK. Effect of Adjuvant Chemotherapy after Complete Resection for Pathologic Stage IB Lung Adenocarcinoma in High-Risk Patients as Defined by a New Recurrence Risk Scoring Model. Cancer Res Treat. 2017;49(4):898–905. doi:10.4143/crt.2016.312
27. Jiang L, Liang W, Shen J, et al. The impact of visceral pleural invasion in node-negative non-small cell lung cancer: a systematic review and meta-analysis. Chest. 2015;148(4):903–911. doi:10.1378/chest.14-2765
28. Wo Y, Zhao Y, Qiu T, et al. Impact of visceral pleural invasion on the association of extent of lymphadenectomy and survival in stage I non-small cell lung cancer. Cancer Med. 2019;8(2):669–678. doi:10.1002/cam4.1990
29. David E, Thall PF, Kalhor N, et al. Visceral Pleural Invasion Is Not Predictive of Survival in Patients With Lung Cancer and Smaller Tumor Size. Ann Thorac Surg. 2013;95(6):1872–1877. doi:10.1016/j.athoracsur.2013.03.085
30. Hung J, Wu Y, Chou T, Jeng W, Yeh Y, Hsu W. Adjuvant Chemotherapy Improves the Probability of Freedom From Recurrence in Patients With Resected Stage IB Lung Adenocarcinoma. Ann Thorac Surg. 2016;101(4):1346–1353. doi:10.1016/j.athoracsur.2015.10.075
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.