Back to Journals » Clinical Ophthalmology » Volume 16
A Pooled Assessment of Ocular Surface Disease After Switching from Preserved Prostaglandins to Tafluprost Across Six Countries in Asia
Authors Tumbocon JA ![]() , Wong TT, Sangapillai T, Yen YC
, Wong TT, Sangapillai T, Yen YC ![]() , Park SW, Lim HH, Ruangvaravate N
, Park SW, Lim HH, Ruangvaravate N ![]()
Received 6 May 2022
Accepted for publication 1 August 2022
Published 17 August 2022 Volume 2022:16 Pages 2669—2676
DOI https://doi.org/10.2147/OPTH.S372312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Joseph Anthony Tumbocon,1,2 Tina T Wong,3– 5 Thanendthire Sangapillai,6 Yung-Chang Yen,7 Sang-Woo Park,8 Hsien Han Lim,9 Ngamkae Ruangvaravate10
1Eye Institute, St. Luke’s Medical Center, Quezon City, Philippines; 2Department of Ophthalmology, St. Luke’s Medical Center College of Medicine, Quezon City, Philippines; 3Glaucoma Department, Singapore National Eye Centre, Singapore, Singapore; 4Cataract & Comprehensive Ophthalmology Department, Singapore Eye Research Institute, Singapore, Singapore; 5Ophthalmology & Visual Sciences, Duke-NUS Graduate Medical School, Singapore, Singapore; 6Tun Hussein Onn National Eye Hospital, Petaling Jaya, Selangor, Malaysia; 7Department of Ophthalmology, Chi Mei Medical Center, Tainan City, Taiwan; 8Department of Ophthalmology, Chonnam National University Medical School and Hospital, Gwangju, South Korea; 9Eye Centre, Sunway Medical Centre, Petaling Jaya, Selangor, Malaysia; 10Department of Ophthalmology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Joseph Anthony Tumbocon, Eye Institute, St. Luke’s Medical Center, 279 E Rodriguez Sr. Ave, Quezon City, Metro Manila, 1112, Philippines, Email [email protected]
Background: Preserved prostaglandin analogs (PGAs) have been linked to ocular surface disease (OSD). While the benefits of preservative-low (PL) or -free (PF) Tafluprost (Santen Inc., Japan) were reported in real-world studies in Western countries, this is the first study in Asia to assess the effectiveness and safety of switching from preserved PGA to PL or PF-Tafluprost.
Methods: We conducted a meta-analysis on studies that included adults (> 18 years of age) with a Corneal Fluorescein Staining Score (CFS) > 1. These individuals had switched to PL or PF-tafluprost after using a preserved PGA therapy for at least 3 months for glaucoma and were identified from Santen’s tafluprost study database. A total of six studies from South Korea, Philippines, Malaysia, Singapore, Thailand, Taiwan were pooled for analysis.
Results: An intraocular pressure (IOP) reduction of 5.9% (0.91 mmHg) was seen in 265 patients. However, this result was not statistically significant (95% CI: − 3.64, 1.81; Figure 1). Among 132 patients, a 47.9% reduction in the CFS (95% CI: − 3.65, − 1.91) was seen. Tear film break-up (n=183) significantly increased by 1.06 seconds (95% CI: 0.65, 1.47). In 88 patients, the bulbar conjunctiva score decreased by − 0.46 (95% CI: − 0.81, − 0.10) and palpebral conjunctiva score decreased by − 0.42 (95% CI: − 0.67– 0.17). One or more new adverse reactions were reported in 3% of the individuals after switching.
Conclusion: Tafluprost IOP reduction is comparable to other PGAs, with significant improvements in the ocular surface and minimal adverse reactions which were already previously reported.
Keywords: ocular surface disease, glaucoma, preserved prostaglandins, tafluprost, PGA, preservative-free, preservative-low, Asian population, meta analysis
Introduction
Glaucoma is the leading cause of irreversible blindness, and its prevalence in Asia is on the rise.1 The two main types of glaucoma are primary open-angle glaucoma (POAG) and primary angle-closure glaucoma (PACG).2 Glaucoma is a progressive disease that is exacerbated by increased intraocular pressure (IOP), which leads to retinal ganglion loss, thinning and loss of neuroretinal rim and retinal nerve fiber layer. Reducing IOP to delay progression and maintain quality of life are key interventions in the clinical management of glaucoma.3 These have been the mainstay of treatment since 1875 when pilocarpine was first discovered, followed by epinephrine in the early 1900s.2,4 Prostaglandin analogs (PGAs) were developed in the mid-1990s as a more effective and safer topical option, leading them to become the first line of treatment in POAG, PACG and ocular hypertension (OHT).3
PGAs facilitate a hypotensive effect via the prostaglandin FP receptors, located in the ciliary muscle and in the trabecular meshwork that provide increased uveoscleral and trabecular meshwork outflow.3 Prior to 2009, as infections have been long associated with eye drops, PGAs were preserved with benzalkonium chloride (BAC), which is a quaternary ammonium compound with effective bactericide and fungicide actions. Clinicians in Asia routinely prescribe preserved PGAs, such as latanoprost (0.02% BAC), bimatoprost 0.03% containing 0.005% BAC or bimatoprost 0.01% containing 0.02% BAC), and travoprost [containing 0.015% BAC or polyquaternium-1 (Polyquad)].
As treatments for glaucoma are typically long-term, continued use of the above-mentioned preserved PGAs is associated with ocular surface disease (OSD) that manifests into signs and symptoms, such as irritation (burning sensations), itchiness, foreign body sensations, conjunctival hyperemia, redness, dry eye and tearing.5–7 Consequently, this can lead to patient’s lack of compliance, glaucoma progression and eventually result in decreased quality of life.5
Tafluprost (Santen Inc., Osaka, Japan) was the fourth-generation and first preservative-free PGA to be introduced in Europe and Japan for more than 12 years (2009). Tafluprost is offered as low-preservative (0.001% BAC) and preservative-free options.8 Randomized control trials and isolated real-life studies have confirmed the effectiveness and safety of tafluprost. While there have been a few large-scale, real-life studies assessing the potential, added benefits of using a preservative-free or low-preservative PGA, such studies are concentrated in Western countries.9–11 In fact, there is a lack of large, real-life studies of pharmaco-efficacy and safety of switching to tafluprost after continued use of preserved PGAs in Asian populations. Therefore, our study aimed to assess the clinical efficacy and safety of switching from preserved PGA to preservative-low (PL) or preservative-free (PF)-tafluprost in Asia.
Methods
Real-life studies from Asia that assessed the clinical efficacy (via measurement of IOP) and/or safety (via assessment of OSD) of switching from preserved PGA to tafluprost were identified via Santen’s tafluprost study database, which, as a common funder, provided expedited access to the data and study groups. Eligibility criteria for this pooled study were as follows: data collection in the years 2014–2020, studies that included patients who were ≥18 years of age, Corneal Fluorescein Staining Score (CFS) score >1, switched to tafluprost after using a preserved PGA therapy for at least 3 months for glaucoma and similarity in outcomes assessment. Two independent reviewers confirmed the eligibility of the studies for the pooled analysis by reviewing protocols, manuscripts and/or study reports. This study was conducted according to the 2020 edition of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA).12
A total of six studies were compiled from six Asian countries including South Korea, Philippines, Malaysia, Singapore, Thailand, Taiwan (Table 1). Data from all countries were published (Philippines,13 Singapore,14 Thailand,15 Malaysia,16 Korea,17 Taiwan18) at the time of this analysis (it is stated in the references section that the Taiwan study was just presented as poster in a scientific meeting and not published). Assessment of study outcomes for all studies was performed using a similar method: IOP and OSD [CFS, tear film break-up time (TBUT), hyperemia]. Outcomes were operationalized (Table 2) across all studies as follows:
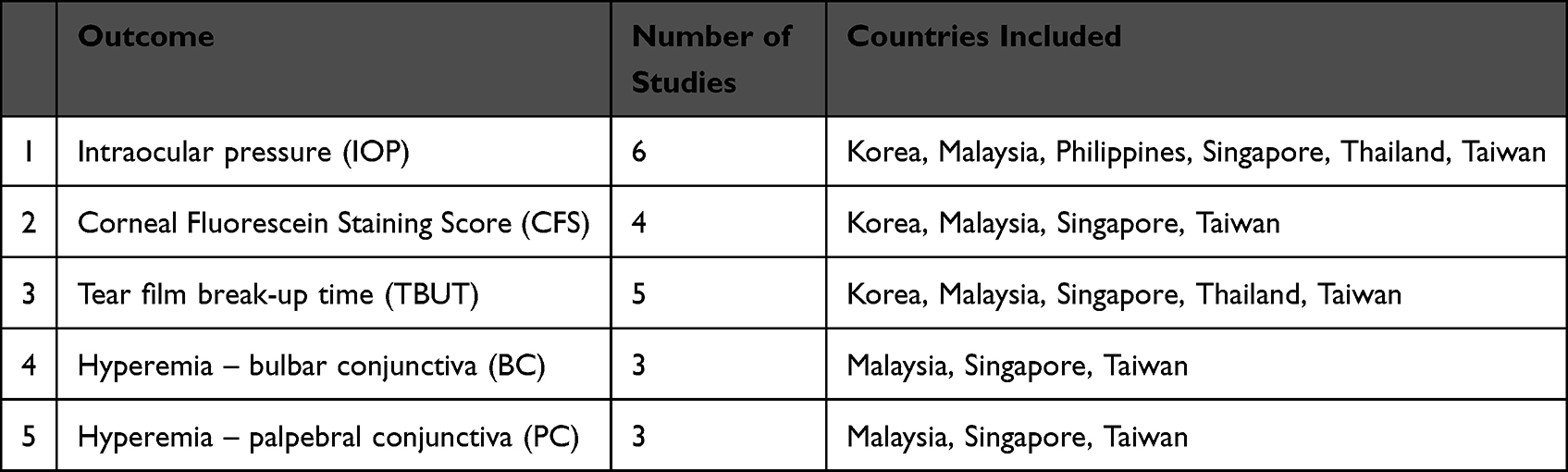 |
Table 1 Outcomes and Studies Included |
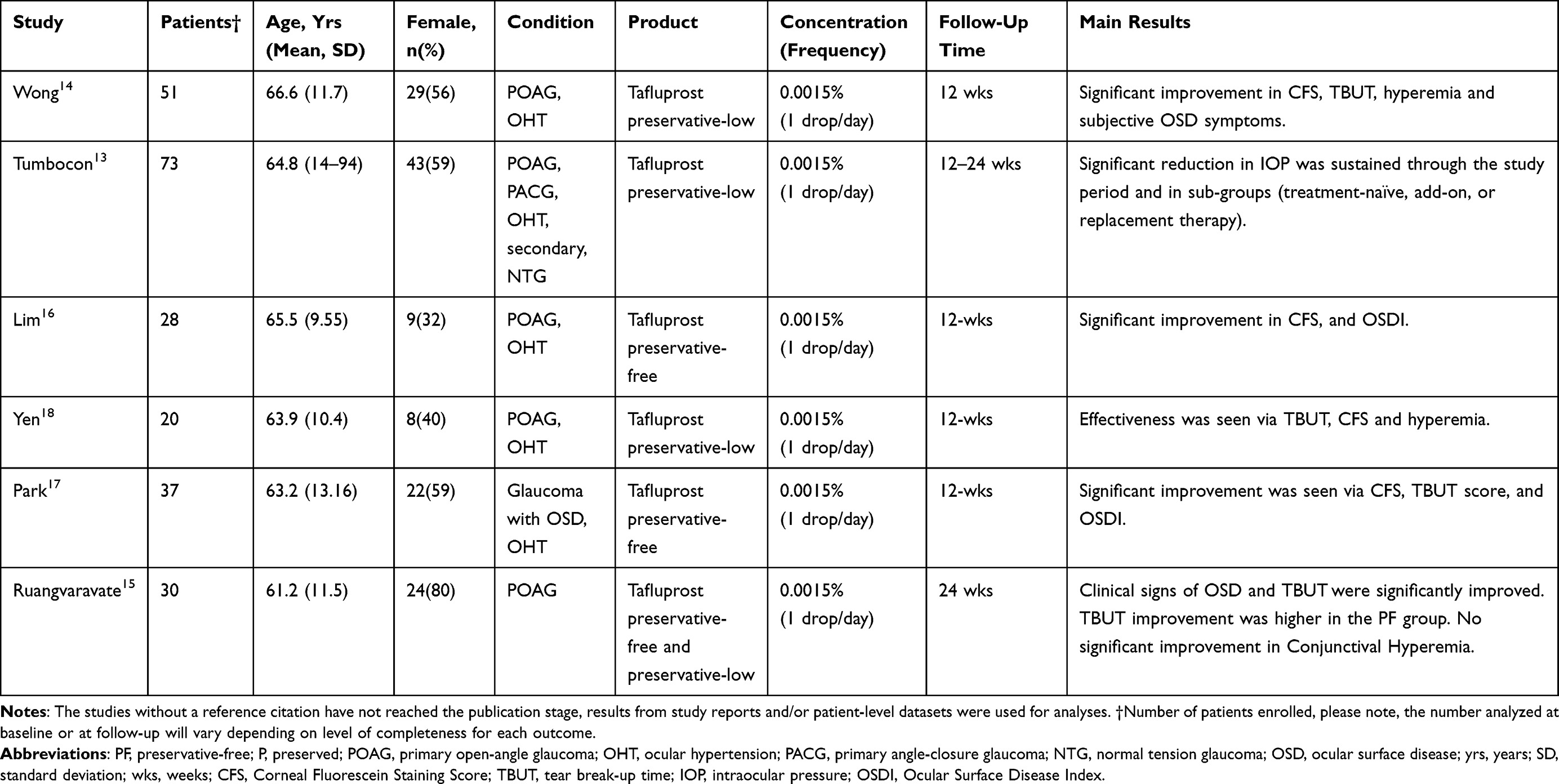 |
Table 2 Characteristics and Main Results from the Observational Studies That Switched from Preserved PGAs to Tafluprost |
IOP: intraocular pressure was assessed via a Goldmann applanation tonometer.
CFS: Corneal Fluorescein Staining Score was collected on five areas of the cornea (central; superior; temporal; nasal and inferior) using the National Eye Institute Industry (NEI) grade method). This assesses the viability of the corneal epithelium.
TBUT: tear film break-up time was observed using the slit-lamp microscope, which helps to evaluate the stability of the tear film and for evaporative dry eye.
Conjunctival hyperemia was assessed via reference photographs as per the criteria of the Japanese Guideline for Allergic Conjunctival Diseases (0 = none; 1 = mild; 2 = moderate; 3 = severe).19
Patient-level, de-identified datasets or summary results were used to compile data from all studies. The results of continuous (IOP, TBUT) and ordinary-scaled (CFS, hyperemia scores) outcomes were extracted via mean differences (standard deviations). The results of each study and the pooled results were shared with each investigator for review and confirmation. One study from Thailand15 assessed both PL- and PF-tafluprost; data for these two groups were extracted and entered into analysis as separate studies. Patient-reported new adverse events (AE) after the intervention, such as irritation, itching, redness, burning sensation, and foreign body sensation, were extracted (AEs by country can be found in Table S1). Thailand was not included in the AE analysis as diagnosis of OSD was part of the inclusion criteria. In Singapore, Malaysia, and Taiwan 3–5 enrolled patients were excluded from the study due to adverse events under the principal investigator’s discretion.
The heterogeneity and percentage of variation across studies due to heterogeneity (I2) were assessed during all pooled analyses. Although the studies were similar in design and analysis, significant heterogeneity was noted (I2 >50%) for all outcomes, and random effects models were adopted for all analyses. As the study populations were derived from different countries, using random effects models offered the most conservative approach while allowing for differences, such as demographic or clinical characteristics, that may confound the results.
The internal validity of all studies was assessed using the “Quality Assessment Tool for Before–After (pre-post) Studies with No Control Group” provided by the National Institutes of Health.20 Review Manager (RevMan) [Computer program, Version 5.4, The Cochrane Collaboration, 2020] was used for analysis and construction of forest plots. R version 4.1.0 was used to rerun all outcome assessments to replicate results from RevMan and ensure that the results were reliable as a quality control measure, specifically regarding the precise calculation of standard error and 95% Confidence Intervals (CI). Statistical significance was assessed with a 0.05 margin of error. All RevMan results (Tables/Figures) were annotated by the study’s first author and the year of publication.
Results
All six studies were similar in study design, methods of data collection, outcome assessment, and study population parameters that were reported. After confirming congruency between studies, those that assessed the same outcomes were pooled (see Table 2 for breakdown of outcomes and studies included). For all studies, the primary outcome of interest was the change in IOP or CFS after switching from a preserved PGA (latanoprost, travoprost, or bimatoprost) to PL- or PF-tafluprost (0.0015%) for at least 12 weeks.
A total of 239 unique patients from Singapore, Taiwan, Philippines, Korea, Malaysia, and Thailand were eligible for the study. The average age among the pooled population was 64.2 years, and 57% of the total population was female. The patient sample had one or more of the following diagnoses: POAG and/or OHT and/or PACG. Individual study characteristics are summarized in Table 2. To clarify, Table 2 shows the eligible, unique patient sample of each study (n=239) that was used for reporting demographic characteristics. The sample size shown in all figures or forest plots denotes the final sample size of contributing studies. For CFS and IOP assessments, Thailand’s study15 sample size (30) was treated as two individual samples and entered twice as each patient received PL-tafluprost in one eye and PF-tafluprost in the other eye.
With a pooled sample of 265 patients that switched to tafluprost, an IOP reduction of 5.9% (0.91 mmHg) was seen, yet this result was not statistically significant (95% CI: −3.64, 1.81; Figure 1). Among 132 patients, switching to PL- or PF-tafluprost was associated with a significant improvement in the CFS. To clarify, after 12 weeks of PL-or PF-tafluprost, there was a 47.9% reduction in the CFS (95% CI: −3.65, −1.91; Figure 2). Similarly, TBUT (n=183) significantly increased by 1.06 seconds (95% CI: 0.65, 1.47; Figure 3) after 12 weeks of receiving PL-or PF-tafluprost. In 88 patients, the reduction in hyperemia that was observed in individual studies was sustained in the pooled effect for both bulbar (BC) and palpebral conjunctiva (PC). The BC score decreased by −0.46 (95% CI: −0.81, −0.10; Figure 4) and PC score decreased by −0.42 (95% CI: −0.67–0.17; Figure 5). As for AEs, 3% of the study cohort reported one or more new adverse reaction after switching, such as itching, burning, tearing, dizziness, blurred vision. The most frequently reported complaint was eye redness (n=4, 0.01%; see Table S1).
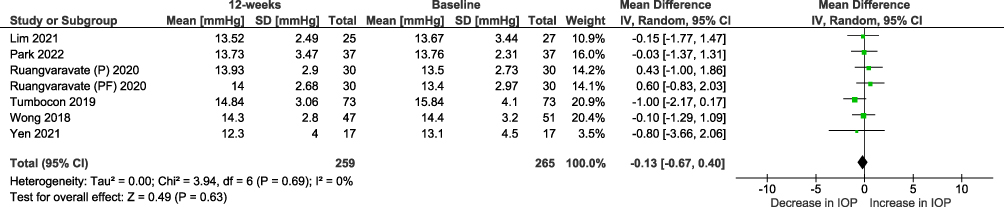 |
Figure 1 Change in IOP when switched from other PGAs to Tatfluprost, 0–12 weeks. Abbreviations: IV, interval variable; SD, standard deviation; CI, confidence interval; IOP, intraocular pressure. Notes: The study from Thailand (Ruangvaravate) assessed both P- and PF-tafluprost; therefore, respective groups are included in the analysis as separate cohorts. |
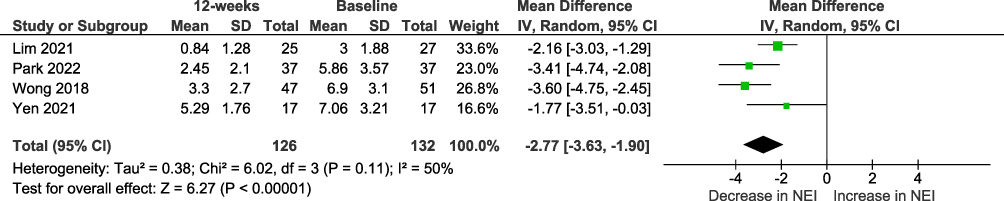 |
Figure 2 Change in fluorescein staining score when switched from other PGAs to tafluprost 0–12 weeks. Abbreviations: IV, interval variable; SD, standard deviation; CI, confidence interval; NEI, National Eye Institute/Industry grading system. |
 |
Figure 3 Change in tear film break-up time when switched from other PGAs to tafluprost, 0–12 weeks. Abbreviations: IV, interval variable; SD, standard deviation; CI, confidence interval; TBUT, tear break-up time. Notes: The study from Thailand (Ruangvaravate) assessed both P- and PF-tafluprost, therefore, respective groups are included in the analysis as separate cohorts. |
 |
Figure 4 Change in bulbar conjunctiva when switched from other PGAs to tafluprost. Abbreviations: IV, interval variable; SD, standard deviation; CI, confidence interval; BC, bulbar conjunctiva. |
 |
Figure 5 Change in palpebral conjunctiva when switched from other PGAs to tafluprost. Abbreviations: IV, interval variable; SD, standard deviation; CI, confidence interval; PC, palpebral conjunctiva. |
A majority (4 out of 6) of the studies received a “good” grade and two received a “fair” grade for level of risk of bias. According to the GRADE21,22 approach (https://gdt.gradepro.org/app/handbook/handbook.html), a high certainty of evidence was evident in this meta-analysis as the results of the individual studies were consistent, had a low risk of bias, used direct outcomes that were established clinically, and had precise results (small CI bands for all outcomes assessed). Three studies had zero patients lost to follow-up and in the remaining three studies all others had less than 18% lost to follow-up with results from all outcomes reported. Therefore, the potential for reporting bias was low.
Discussion
After pooling six similar studies with comparable study populations from Asia, tafluprost maintained the reduction of IOP when switched from other PGAs and effectively lowered OSD. The switch to tafluprost was shown to maintain the IOP level from baseline to at least 12 weeks as the reduction in IOP was not significant. This may be due to receiving tafluprost as a second line of therapy after having received the initial PGA for 3 months where a clinically meaningful reduction had already been achieved. In PGA-naïve and switch patients, there has been continued empirical evidence showing that the IOP lowering effect of tafluprost is similar to other PGAs in both controlled and in real-life settings.7,10,11,23,24
Our findings are supported by multiple previous studies in Europe that also revealed that a switch from preserved prostaglandin to PL- or PF-tafluprost reduces IOP while conserving the ocular surface morphology.25–27 Uusitalo et al27 investigated the tolerability and IOP after switching from latanoprost to tafluprost. They also demonstrated that after receiving tafluprost for 12 weeks, baseline IOP was maintained, and a significant reduction in the proportion of patients reporting subjective OSD symptoms (eg, itching, irritation/burning, foreign body sensation) and showing abnormal clinical signs of OSD (eg, CFS, Schirmer’s test, hyperemia) was achieved. Hommer et al26 assessed the effect of changing from preserved prostaglandin to PF-tafluprost on tear film thickness and detected a significant increase in TBUT and tear film thickness after the switch.
Additionally, a large regional study of 577 patients in Europe found improvements in corneal staining score, hyperemia and OSD subjective symptoms when patients receiving a preserved PGA (including PL-tafluprost), or beta-blockers switched to a fixed-dose combination of PF-tafluprost/timolol.10
As prostaglandin therapy is long-term and lifelong for some, an easy-to-use (one drop per day), effective treatment with minimum side effects is a sustainable treatment option. However, in overall PGA therapy, the average adherence rate was reported to be 76%, suggesting a need to improve therapy persistence.28 Additionally, there is speculation that hyperemia may be related to low adherence as patients complain of a visible red-eye appearance.29 We can expect an improvement in therapy persistence with tafluprost as patients recover ocular surface quality with significant decrease in clinical indications and complaints of ocular disease, such as hyperemia, as we have noted in this study. Although our patients were not followed-up for a long duration, a multicenter, real-world evidence study in Japan that monitored 4502 patients for 2 years showed that 84.6% of the patients continued taking tafluprost for 1 year and 76.1% for 2 years.24
This is the first large, real-world study of tafluprost effectiveness and safety in Asian patients.
The pooling of data was warranted due to the high level of congruence in methodology and patient population between the included studies, as described in the methods section. The results of this study are reliable as supported by the high level of evidence and internal validity of the studies included.
There were innate limitations to this analysis. As studies were conveniently identified via a study group under Santen Pharmaceutical Asia Pte. Ltd, other relevant studies were not included. As not all studies had the same outcomes, sample sizes were smaller in outcomes such as CFS, hyperemia and TBUT when compared to IOP. There was a mixture of PL- and PF-tafluprost in the pooled analysis as different studies used one product or both. Moreover, a subgroup analysis of PL-tafluprost and PF-tafluprost could not be conducted due to the current study being underpowered since not all studies evaluated both tafluprost products. Although this study was conducted in accordance with the PRISMA 2020 guidelines where and when feasible, the study protocol was not constructed nor was it registered as a review analysis.
Conclusion
Preservative-low or preservative-free PGA can help to maintain ocular surfaces. Compared to preservative-high PGAs, tafluprost was similar in IOP reduction but relatively superior in restoring the ocular surface quality with minimal AEs. Tafluprost may be a better treatment option for those experiencing OSD signs or symptoms and prefer to avoid further worsening of the condition or for treatment-naïve patients who wish to avoid OSD.
Acknowledgment
Medical writing support and analysis were provided by Medical Writers’ Asia, 483 Yio Chu Kang Road, Singapore 787057. The authors thank Tin Aung, Ho Ching Lin, Jiwoong Lee, Michael S. Kook, and Anne Marie Macasaet for their contributions.
Funding
This study was funded by Santen Pharmaceutical Asia Pvt Ltd alongside the decision to submit the article for publication. The analysis and writing of the article were independent of the sponsor.
Disclosure
Professor Joseph Anthony Tumbocon reports non-financial support from Santen, during the conduct of the study; personal fees from Santen, personal fees from Allergan, personal fees from Novartis, personal fees from Stada, outside the submitted work. Professor Ngamkae Ruangvaravate reports non-financial support from drugs in the study was provided by a pharmaceutical company, outside the submitted work. No other conflict of interest were reported by the authors.
References
1. Chan EW, Li X, Tham YC, et al. Glaucoma in Asia: regional prevalence variations and future projections. Br J Ophthalmol. 2016;100(1):78–85. doi:10.1136/bjophthalmol-2014-306102
2. European Glaucoma Society. Terminology and guidelines for glaucoma 4th edition - Chapter 3: treatment principles and options supported by the egs foundation: part 1: foreword; introduction; glossary; chapter 3 treatment principles and options. Br J Ophthalmol. 2017;101(6):130–195. doi:10.1136/bjophthalmol-2016-EGSguideline.003
3. Harasymowycz P, Birt C, Gooi P, et al. Medical management of glaucoma in the 21st century from a Canadian perspective. J Ophthalmol. 2016;2016:6509809. doi:10.1155/2016/6509809
4. Realini T. A history of glaucoma pharmacology. Optom Vis Sci. 2011;88(1):36–38. doi:10.1097/OPX.0b013e3182058ead
5. Baudouin C, Renard JP, Nordmann JP, et al. Prevalence and risk factors for ocular surface disease among patients treated over the long term for glaucoma or ocular hypertension [published online ahead of print, 2012 Jun 11]. Eur J Ophthalmol. 2012. doi:10.5301/ejo.5000181
6. Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341–349. doi:10.1177/112067210701700311
7. Liu Y, Mao W. Tafluprost once daily for treatment of elevated intraocular pressure in patients with open-angle glaucoma. Clin Ophthalmol. 2013;7:7–14. doi:10.2147/OPTH.S30951
8. Swymer C, Neville MW. Tafluprost: the first preservative-free prostaglandin to treat open-angle glaucoma and ocular hypertension. Ann Pharmacother. 2012;46(11):1506–1510. doi:10.1345/aph.1R229
9. Lanzl I, Hamacher T, Rosbach K, et al. Preservative-free tafluprost in the treatment of naive patients with glaucoma and ocular hypertension. Clin Ophthalmol. 2013;7:901–910. doi:10.2147/OPTH.S41640
10. Ansari E, Pavicic-Astalos J, Ayan F, et al. Treatment of open-angle glaucoma and ocular hypertension with preservative-free tafluprost/timolol fixed-dose combination therapy: UK and Ireland results from the VISIONARY Study [published correction appears in Adv Ther. 2022 Jan;39(1):831]. Adv Ther. 2021;38(6):2990–3002. doi:10.1007/s12325-021-01725-7
11. Ranno S, Sacchi M, Brancato C, Gilardi D, Lembo A, Nucci P. A prospective study evaluating IOP changes after switching from a therapy with prostaglandin eye drops containing preservatives to nonpreserved tafluprost in glaucoma patients. ScientificWorldJournal. 2012;2012:804730. doi:10.1100/2012/804730
12. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
13. Tumbocon JA, Macasaet AM. Efficacy and safety of tafluprost 0.0015% - retrospective analysis of real-world data from the Philippines. Clin Ophthalmol. 2019;13:1627–1634. doi:10.2147/OPTH.S209942
14. Wong TT, Aung T, Ho CL. Ocular surface status in glaucoma and ocular hypertension patients with existing corneal disorders switched from latanoprost 0.005% to tafluprost 0.0015%: comparison of two prostaglandin analogues with different concentrations of benzalkonium chloride. Clin Exp Ophthalmol. 2018;46(9):1028–1034. doi:10.1111/ceo.13329
15. Ruangvaravate N, Choojun K, Srikulsasitorn B, Chokboonpiem J, Asanatong D, Trakanwitthayarak S. Ocular surface changes after switching from other prostaglandins to tafluprost and preservative-free tafluprost in glaucoma patients. Clin Ophthalmol. 2020;14:3109–3119. doi:10.2147/OPTH.S264984
16. Lim HH, Sangapillai T. Ocular surface conditions in Asian glaucoma patients with existing corneal disorders switching from preserved prostaglandin analogue monotherapy to preservative-free tafluprost. Malays J Ophthalmol. 2021;3(3):109–122. doi:10.35119/myjo.v3i3.185
17. Park SW, Lee J, Kook MS. Efficacy, safety and patient-reported outcomes with preservative-Free (PF) tafluprost or PF-dorzolamide/timolol compared with preserved latanoprost: a prospective multicenter study in Korean glaucoma patients with ocular surface disease. Pharmaceuticals. 2022;15(2):201. doi:10.3390/ph15020201
18. Yen YC. Prospective, single center switching study of 0.0015% tafluprost ophthalmic solution in primary open-angle glaucoma and ocular hypertension patients with corneal disorders (Switching from 0.005% latanoprost ophthalmic solution).
19. Takamura E, Uchio E, Ebihara N, et al. Japanese guideline for allergic conjunctival diseases. Allergol Int. 2011;60(2):191–203. doi:10.2332/allergolint.11-RAI-0335
20. Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. 2020;7(1):7. doi:10.1186/s40779-020-00238-8
21. Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. Gdt.guidelinedevelopment.org. Available from: http://gdt.guidelinedevelopment.org/app/handbook/handbook.html.
22. GRADEpro GDT. GRADEpro guideline development tool [software]. McMaster University, (developed by Evidence Prime, Inc.); 2020. Available from: gradepro.org.
23. Hamacher T, Airaksinen J, Saarela V, Liinamaa MJ, Richter U, Ropo A. Efficacy and safety levels of preserved and preservative-free tafluprost are equivalent in patients with glaucoma or ocular hypertension: results from a pharmacodynamics analysis. Acta Ophthalmol Suppl. 2008;242:14–19. doi:10.1111/j.1755-3768.2008.01381.x
24. Kuwayama Y, Hashimoto M, Kakegawa R, Nomura A, Shimada F. Prospective observational post-marketing study of tafluprost for glaucoma and ocular hypertension: effectiveness and treatment persistence. Adv Ther. 2017;34(6):1411–1425. doi:10.1007/s12325-017-0549-0
25. Erb C, Lanzl I, Seidova SF, Kimmich F. Preservative-free tafluprost 0.0015% in the treatment of patients with glaucoma and ocular hypertension. Adv Ther. 2011;28(7):575–585. doi:10.1007/s12325-011-0038-9
26. Hommer A, Schmidl D, Kromus M, et al. Effect of changing from preserved prostaglandins to preservative-free tafluprost in patients with glaucoma on tear film thickness. Eur J Ophthalmol. 2018;28(4):385–392. doi:10.1177/1120672117753703
27. Uusitalo H, Chen E, Pfeiffer N, et al. Switching from a preserved to a preservative-free prostaglandin preparation in topical glaucoma medication. Acta Ophthalmol. 2010;88(3):329–336. doi:10.1111/j.1755-3768.2010.01907.x
28. Wilensky J, Fiscella RG, Carlson AM, Morris LS, Walt J. Measurement of persistence and adherence to regimens of IOP-lowering glaucoma medications using pharmacy claims data. Am J Ophthalmol. 2006;141(1 Suppl):S28–S33. doi:10.1016/j.ajo.2005.09.011
29. Feldman RM. Conjunctival hyperemia and the use of topical prostaglandins in glaucoma and ocular hypertension. J Ocul Pharmacol Ther. 2003;19(1):23–35. doi:10.1089/108076803762718088
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ocular Surface Disease and Dry Eye Severity in Glaucoma Patients at Urban Private Eye Care Centres in Malaysia
Gan EH, Woo WW, Seng KF, Singh P, Lee MY, Kong VY, Khoo SP, Lee MW, Liang LK
Clinical Ophthalmology 2024, 18:3249-3262
Published Date: 14 November 2024