Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
A Pilot Study to Evaluate a Reading Pen-Based, Audio-Assisted Health Education Tool for Postoperative Percutaneous Coronary Intervention Care in Older Adults
Authors Sun T, Liu L, Ye R, Wei Y, Zhai G
Received 2 April 2026
Accepted for publication 29 June 2026
Published 10 July 2026 Volume 2026:19 614062
DOI https://doi.org/10.2147/JMDH.S614062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 1
Editor who approved publication: Professor Tilakavati Karupaiah
Tingting Sun,1 Lili Liu,1 Rui Ye,2 Yaqi Wei,1 Guangyao Zhai1
1Department of Cardiology, Beijing Luhe Hospital, Capital Medical University, Beijing, 101100, People’s Republic of China; 2Department of Geriatrics, Beijing Luhe Hospital, Capital Medical University, Beijing, 101100, People’s Republic of China
Correspondence: Guangyao Zhai, Department of Cardiology, Beijing Luhe Hospital, Capital Medical University, No. 82 of Xinhua South Road, Tongzhou District, Beijing, 101100, People’s Republic of China, Tel +86010-69543901, Email [email protected]
Objective: This study aimed to develop a pen-based, audio-assisted health education tool and evaluate its feasibility in a pilot study.
Methods: In this single-arm pilot study, a literature review and guideline analysis were conducted to identify the health education needs of older adults following percutaneous coronary intervention (PCI). Guided by geragogy principles, a health education tool comprising three modules was developed: (1) a manual integrating text, images, audio, and video for educational delivery; (2) a poster placed in visible locations to reinforce instructions related to emergency management and follow-up care; and (3) a medication box providing pen-activated audio instructions for medication administration. Following prototype development, a 4-week pilot study was conducted using convenience sampling in 20 patients after PCI. Usability, satisfaction, perceived usefulness, engagement, and applicability were assessed using questionnaires and interviews. Descriptive statistics were used for quantitative data.
Results: A pen-based, audio-assisted health education tool characterized by operational simplicity and alignment with the cognitive and physiological characteristics of older adults was developed. The 20 participants had a mean age of 71.30± 5.03 years. The overall mean item score on the 5-point questionnaire was 4.82± 0.26, with dimension scores ranging from 4.53± 0.23 (applicability) to 4.96± 0.17 (satisfaction). All patients (100%) demonstrated high applicability. Interview data indicated that audiovisual components reduced anxiety associated with memory impairment, and the medication box with audio-enabled instructions was reported to improve medication adherence.
Conclusion: The pen-based, audio-assisted health education tool demonstrated preliminary feasibility and good acceptability among patients. It has the potential to address limitations of conventional education approaches and to enhance the learning experience of older adults, providing a basis for further evaluation of clinical effectiveness. Limitations include the absence of a control group and the small sample size, which preclude definitive conclusions on efficacy and needs to be further tested in a RCT format.
Keywords: audio-assisted, health education, older adults, percutaneous coronary intervention, pen-based
Introduction
Percutaneous coronary intervention (PCI) is a primary treatment modality for coronary heart disease. It facilitates rapid restoration of coronary blood flow and improves myocardial ischemia and hypoxia, thereby contributing to disease management and enhancing quality of life.1 Generally, patients with a higher level of disease knowledge tend to have better self-management competence.2–4 Therefore, improving patients’ knowledge through effective health education is an important approach to optimize their self-management behaviors.
Current digital health education tools feature complicated interfaces, tedious login and registration procedures, frequent operational steps and network synchronization requirements, as well as small font sizes and poor color contrast. In addition, the lack of relevant training and technical support often discourages elderly patients, especially those with impaired vision, hearing, fine motor skills or cognitive function, leading them to stop using such tools.5,6 Based on the physiological characteristics and clinical needs of the elderly, this study developed a health education tool that is easy to understand, simple to operate and well accepted by users, aiming to enhance elderly patients’ knowledge of coronary heart disease and optimize their self-management behaviors.
Subjects and Methods
Subjects
Using convenience sampling, a total of 20 elderly patients who underwent percutaneous coronary intervention (PCI) in the Department of Cardiology of Beijing Luhe Hospital, Capital Medical University were enrolled as research subjects in this single-arm pilot study. Sample screening was performed in strict accordance with pre-established inclusion and exclusion criteria, and the study design and implementation complied with ethical requirements for clinical research.
Inclusion Criteria
① Aged 60 years or older; ② Normal eyesight and hearing, no history of mental illness, clear consciousness and intact cognitive function, capable of full cooperation with questionnaires and intervention throughout the research; ③ Patients and their family members were fully informed of the study content, volunteered to participate, and signed written informed consent forms.
Exclusion Criteria
① Previous PCI surgery within the past 12 months; ② Patients unable to complete the 6-month postoperative follow-up due to unstable physical conditions or non-local residence.
Sample Screening and Enrollment
Full-time cardiology ward nurses preliminarily screened hospitalized elderly PCI patients per the inclusion and exclusion criteria to identify potential candidates. Researchers communicated one-on-one with eligible patients and their family members at bedside to elaborate on research objectives, intervention protocols, required cooperation, study duration, safety guarantees and data confidentiality regulations. Subjects were formally enrolled only after full informed consent and signature of written consent forms. The sample size of 20 was selected based on the exploratory pilot nature of this study. This sample size is considered adequate to provide reliable estimates of variance for continuous outcome measures, thereby informing sample size calculations for future definitive randomized controlled trials. Furthermore, given that the study population consisted of older adults with multiple comorbidities following PCI, which presents challenges in intervention implementation and data collection, a smaller sample size allowed for rigorous quality control and minimized missing data.
Research Methods
Intervention Protocol
The intervention was delivered via a customized audio reading pen-based health education tool, consisting of commercially available off-the-shelf reading pens paired with self-developed supporting reading-enabled educational materials; the educational content was not the original factory configuration of the purchased pens. The intervention content was divided into four core modules: basic knowledge of coronary heart disease and PCI, typical clinical manifestations of coronary heart disease, specialized perioperative nursing for PCI, and continuous home-based rehabilitation guidance covering four weeks post-discharge. The 4-week intervention period was chosen as the primary focus of this pilot study to assess the short-term feasibility, user experience, and data collection feasibility of the tool. Longer-term follow-up was not within the scope of this initial pilot; however, future definitive studies will extend the follow-up duration to evaluate medium- and long-term effects.
Development Process of the Health Education Tool
All educational manuals and posters were independently compiled by the research team. Tool fabrication was completed through standardized audio recording by specialized cardiac nurses, sticker placement of invisible identification codes and audio-code binding, with detailed procedures as follows: First, guided by clinical guidelines on perioperative management and home rehabilitation for patients with coronary heart disease receiving PCI, researchers compiled standardized health education content and formatted it into printed manuals and wall-mounted educational posters. Second, senior cardiac nurses uniformly recorded all audio narrations in standard Mandarin with consistent speaking pace and tone to avoid inconsistent explanation quality, ensuring professional, standardized and easy-to-understand content matching the auditory and cognitive characteristics of elderly adults. Finally, exclusive invisible reading codes matching each knowledge point were pasted onto corresponding positions of self-made manuals and posters; pre-recorded standardized audio files were bound to respective codes and imported into the reading pen system (Figure 1).
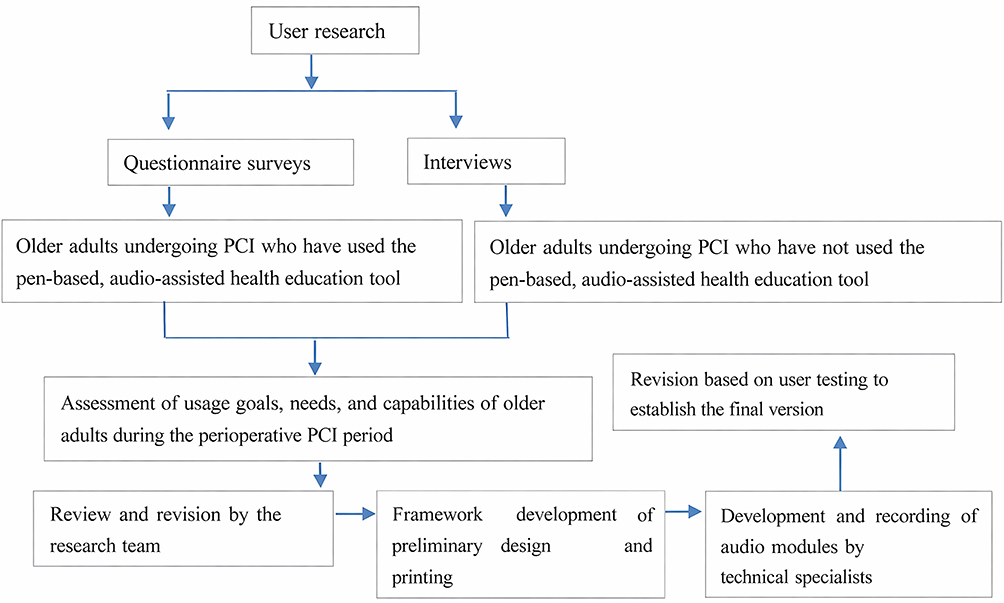 |
Figure 1 Development process of the pen-based, audio-assisted health education tool for perioperative PCI care. |
Main Components and Application of the Pen-Based, Audio-Assisted Education Tool
The pen-based, audio-assisted health education tool for perioperative PCI comprises three components: a health education manual, a self-management poster, and a medication box. Each component is equipped with pen-activated audio functionality, enabling patients to access audio instructions using a dedicated reading pen. Upon discharge, patients are provided with the complete set of educational materials for home use. The research team delivers weekly text message reminders to encourage engagement with the materials and to facilitate the application of acquired knowledge in daily practice.
Health Education Manual
The manual provides a systematic overview of coronary heart disease, including disease-related information, clinical manifestations, preoperative preparation, postoperative guidance, and discharge instructions. It includes detailed explanations of risk factors, pathogenesis, treatment approaches, medication effects, and related precautions. Each section of text and accompanying images is supported by audio explanations, which can be accessed via QR codes using a smartphone or through a dedicated reading pen. The pen-based audio function is particularly suitable for older adults with limited proficiency in smartphone use.
Self-Management Poster
The poster presents key self-management behaviors required after discharge using a combination of text and images. It incorporates embedded codes that provide detailed explanations and reminders for each behavior, including medication use, dietary management, and physical activity. Audio guidance can be accessed by activating the codes with a dedicated reading pen.
Medication Box
All discharge medications are integrated with audio-enabled codes. Prior to discharge, nurses record audio instructions covering medication dosage, timing, administration methods, and precautions, which are stored within the corresponding codes. Patients can access these instructions using the reading pen, facilitating accurate medication administration and enhancing understanding of medication effects and precautions.
Standardized Intervention Implementation and Quality Control
Admission phase: Full-time health education nurses delivered systematic bedside health education combining the customized reading materials with face-to-face verbal instruction to unify teaching standards across all enrolled patients.
Discharge day: Each patient and accompanying caregiver received one commercial reading pen plus complete self-developed supporting reading materials. Nurses provided hands-on bedside training covering power on/off, volume adjustment and point-to-read operation to ensure independent home use. Patients were instructed to repeatedly access audio content concerning medication, diet, physical activity, rehabilitation and outpatient follow-up as needed. Devices were limited to research use only, and participants were guided to translate acquired health knowledge into daily self-management behaviours.
Post-discharge phase: The whole intervention period lasted from hospital admission to four weeks after discharge. The research team sent weekly SMS reminders to encourage regular autonomous learning with the reading tool and standardize rehabilitation behaviours, so as to improve participant adherence and guarantee homogeneous intervention implementation.
Baseline Assessment and Questionnaire Administration
Survey Timing and Questionnaire Collection
Questionnaire surveys were conducted on the first admission day and one day before discharge respectively. Demographic and clinical data questionnaires were distributed on admission for self-completion by patients. All finished questionnaires were collected on-site, checked item by item for completeness, and supplemented for missing entries immediately to guarantee authentic, intact and valid research data.
Standard for Questionnaire Completion
All questionnaires were distributed face-to-face and filled out independently by participants. For patients with low literacy unable to finish questionnaires by themselves, trained investigators completed forms objectively through non-suggestive standardized verbal inquiry after ensuring full understanding of each item, so as to obtain reliable research data.
Patients’ Evaluation of the Health Education Tool
Guided by the Technology Acceptance Model proposed by Fred Davis, and considering the characteristics of the health education tool developed in this study, a questionnaire was designed to assess patient acceptance and utilization.7 The questionnaire was developed through iterative revisions by three clinical experts and one nursing research expert from the research team.
The instrument comprised five dimensions—usefulness, ease of use, applicability, engagement, and satisfaction—encompassing a total of 20 items. Each item was rated on a 5-point Likert scale, with scores ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Five experts (holding intermediate or higher professional titles and with more than 10 years of experience in cardiovascular care) were invited to evaluate the content validity of the questionnaire, yielding a content validity index of 0.880. The Cronbach’s α coefficient of the scale was 0.788, indicating satisfactory reliability of the scale.
Statistical Analysis
All the data collected in this study were analyzed using SPSS 22.0 software. The measurement data were expressed as mean±standard deviation (SD). The categorical data were expressed as n (%).
Ethical Approval
This study was conducted with approval from the Ethics Committee of Beijing Luhe Hospital, Capital Medical University (No. 2020-LHKY-049-03) and in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Results
Participant Baseline Characteristics
A total of 20 older adults who underwent first-time PCI were enrolled. The mean age was 71.30 ± 5.03 years. Among them, 11 (55.0%) were male and 9 (45.0%) female. Regarding marital status, 18 (90.0%) were married and 2 (10.0%) were widowed. Educational level distribution was as follows: primary school or below in 5 (25.0%), junior high school in 13 (65.0%), and secondary/high school in 2 (10.0%). Two participants (10.0%) lived alone, 15 (75.0%) lived with a spouse, and 3 (15.0%) lived with children. Payment methods included urban employee medical insurance (n=9, 45.0%), urban resident medical insurance (n=9, 45.0%), new rural cooperative medical scheme (n=1, 5.0%), and self-pay (n=1, 5.0%).
Regarding medical history, 14 patients (70.0%) had no prior diagnosis of coronary heart disease, 2 (10.0%) had a diagnosis for 1–5 years, and 4 (20.0%) had a diagnosis for >5 years. Four patients (20.0%) had previously received coronary stenting. Comorbidities included hypertension in 15 (75.0%), hyperlipidemia in 12 (60.0%), diabetes in 5 (25.0%), and cerebrovascular disease in 5 (25.0%). Two patients (10.0%) were current smokers, and 18 (90.0%) were non-smokers (Table 1).
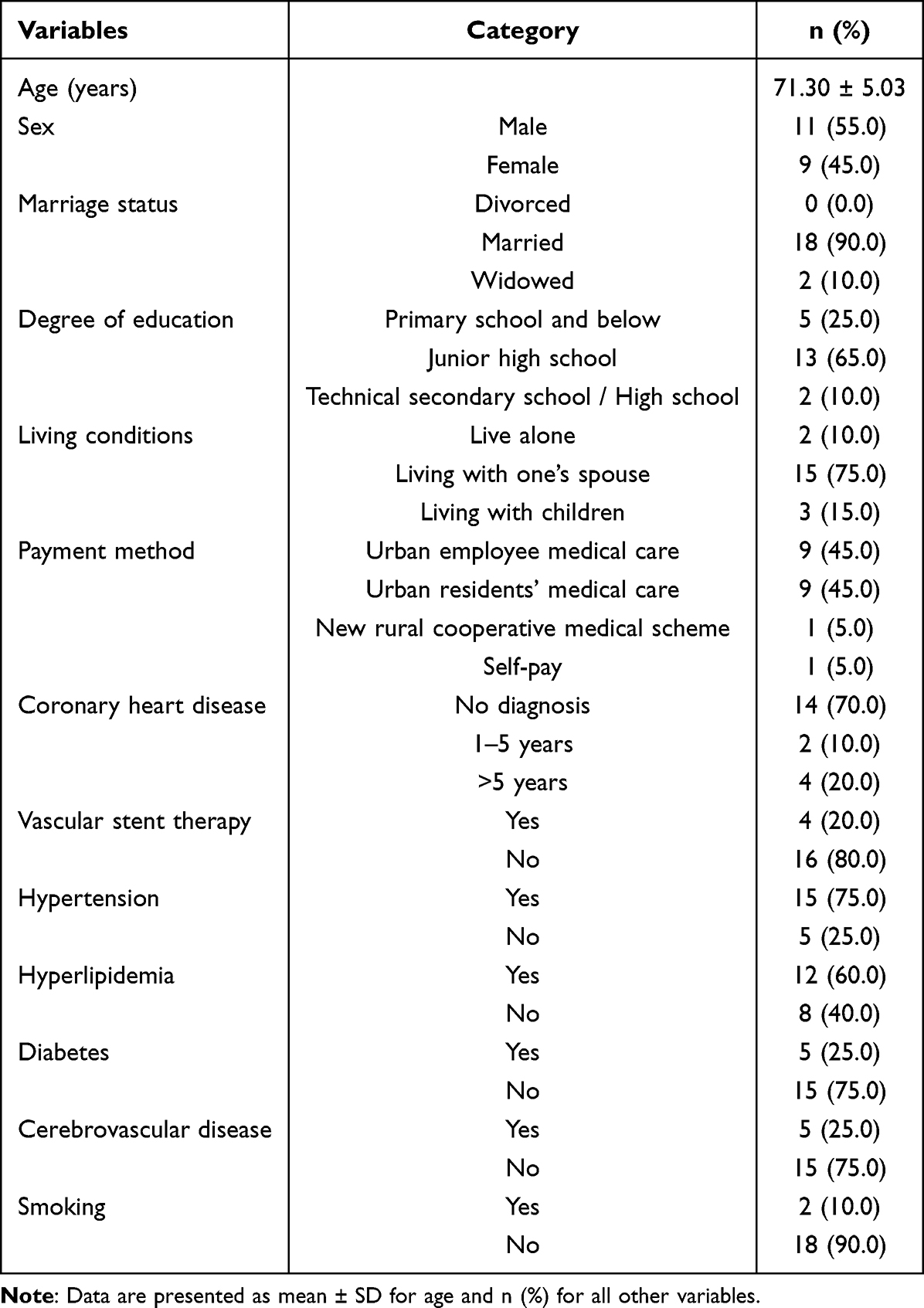 |
Table 1 Baseline Demographic and Clinical Characteristics (n = 20) |
Quantitative Evaluation of the Health Education Tool
All 20 participants completed the 20-item questionnaire (response rate: 100%). The overall mean item score was 4.82 ± 0.26 (out of a maximum of 5), indicating a very high level of acceptance. All participants demonstrated high applicability, with no cases classified as low or moderate applicability. The dimension scores, ranked from highest to lowest, were: satisfaction (4.96 ± 0.17), ease of use (4.95 ± 0.10), usefulness (4.95 ± 0.10), engagement (4.69 ± 0.29), and applicability (4.53 ± 0.23). The total score across all dimensions was 96.50 ± 2.33 (possible range: 20–100). Detailed dimension scores are presented in Table 2.
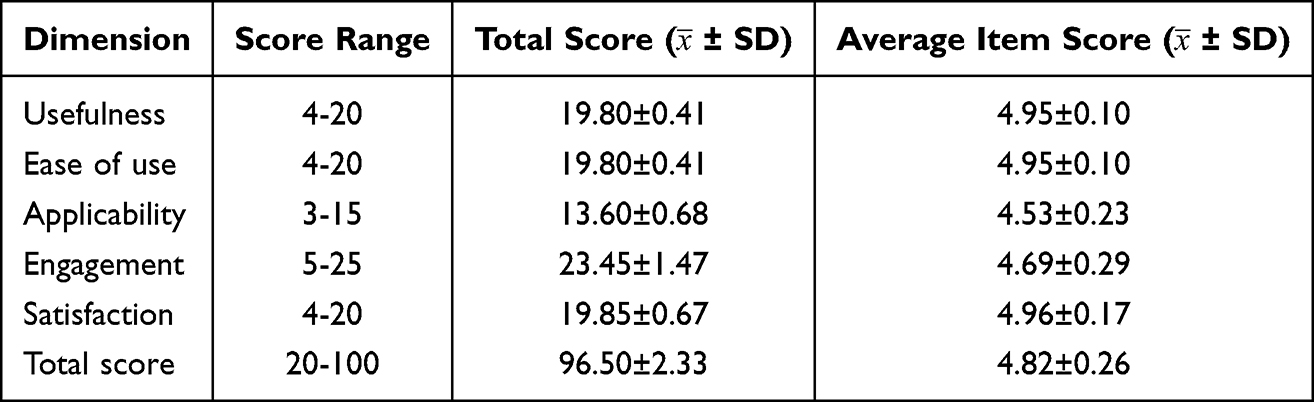 |
Table 2 Scores Across Questionnaire Dimensions |
Qualitative Findings from Interviews
Semi-structured interviews were conducted with all 20 participants following the 4-week intervention. Two independent researchers coded the transcripts; discrepancies were resolved through discussion. Four major themes emerged.
Theme 1: Reduced Anxiety Related to Memory Decline
18 participants (90%) explicitly stated that the audio-assisted feature alleviated their fear of forgetting critical health information. A representative quote: “I can’t remember everything the doctor says, but with this pen, I just tap and listen again. It makes me feel safe”. Another participant noted: “My memory is not what it used to be. Having the voice repeat the instructions takes away the worry”.
Theme 2: Enhanced Medication Adherence via the Audio-Enabled Medication Box
17 participants (85%) reported that the medication box with audio instructions improved their correct use of medications. One patient stated: “I used to mix up my pills. Now I tap the box and it tells me which one to take and when. I haven’t missed a dose since”. Another commented: “My wife also listens with me, so we both know the schedule”.
Theme 3: Audible Poster Clarifies Daily Rehabilitation Routines, Providing Psychological Reassurance
16 participants (80%) indicated that the pen-activated education poster (specific to post-PCI care) placed in the ward provided standardized, step-by-step guidance on daily home rehabilitation, including rest, activity, and contraindications. The clear visual layout combined with repeatable audio explanations alleviated their sense of uncertainty regarding post-discharge recovery. One patient remarked:
After discharge, I didn’t know whether I should rest or move around, I felt anxious all the time. Now the first thing I do each morning is tap the poster with the pen and listen. I know exactly what to do every day, and it makes me feel secure.
Another participant added:
The poster content is very practical, wound care, post-meal activities, foods to avoid, I can tap and listen without repeatedly bothering my children or consulting doctors.
Theme 4: Reduced Caregiver Burden and Facilitation of Independent Self-Rehabilitation
18 participants (90%) reported that the complete set of pen-based educational materials could be operated independently, eliminating the need to rely on their children for repeated explanations of post-discharge knowledge or medication reminders, thereby reducing feelings of being a burden to family members. One participant stated:
My children are very busy with work. I don’t like to keep calling them to ask about post-discharge issues. With this pen-based tool, I can understand everything on my own without constantly troubling the younger generation.
Another patient said:
My children no longer have to watch over me constantly to remind me to take my medication or exercise. I can manage myself, and my family can feel reassured.
Discussion
This study preliminarily evaluated the application effect of a self-developed pen-based, audio-assisted health education tool among elderly patients after percutaneous coronary intervention (PCI). According to questionnaire results, the overall average item score of the tool was 4.82±0.26 (full score = 5 points), with all dimension scores at a high level. The satisfaction dimension yielded the highest average item score of 4.96±0.17, followed by usefulness and ease of use, both at 4.95±0.10. The applicability dimension had the relatively lowest average item score of 4.53±0.23. These findings indicate that elderly patients showed a very high subjective acceptance of the tool, with particularly high overall satisfaction. Nevertheless, there is still room for improvement in its applicability across diverse clinical scenarios and patient subgroups.
Highest Score in Patient Satisfaction
Elderly people commonly suffer from diminished eyesight and impaired fine motor control in their hands. As audio-output devices, talking reading tools greatly reduce reliance on screen reading, which caters to the perceptual needs of older adults with poor vision.8 Featuring instant voice feedback upon simple taps, these tools minimize operational errors and frustration caused by unsteady hands or slow response.9 Users can freely select content to play or replay at will. This on-demand learning mode gives them a strong sense of control, leading to positive perceptions that the tool is user-friendly and satisfactory.
People aged over 70 are generally reluctant to use smartphones, as deteriorated eyesight and motor coordination hinder touchscreen operations.6 Systematic reviews indicate that mobile health education tools are prone to technical malfunctions, insufficient storage, high power consumption, synchronization failures, connection and network errors, unstable Wi-Fi and login difficulties among the elderly. These issues cause frustration and discourage usage. Additionally, many older adults do not have access to smartphones, computers, dedicated applications or internet services, creating substantial practical barriers.5
Excellent Perceived Utility and Usability
The tap-to-read audio-assisted health education tool achieved extremely high scores in perceived utility (4.95±0.10) and usability (4.95±0.10), nearly reaching full marks. This indicates that elderly patients after PCI generally find the tool easy to operate, and highly recognize its practical value in improving disease awareness and self-management capabilities.
The superior utility of the tool stems primarily from its ultra-simplified interaction design. It adopts a tap-to-play operation mode, with no need for multi-level menus, text input or page scrolling. Most elderly people are familiar with tap-to-read pens and similar daily products. Since the operation logic aligns with their existing cognitive patterns, the learning cost is nearly negligible.
Its high utility is also reflected in barrier-free information access and memory reinforcement via repeated playback. Traditional printed health education materials have obvious limitations for the elderly: they are easy to lose and inconvenient for repeated reference; small fonts and dense layouts create reading difficulties for those with impaired vision; such materials lack interaction and real-time feedback, are hard to update, and show limited effects on long-term behavioral changes and treatment adherence.10,11 Systematic reviews have confirmed that presenting key information via repeatable audio can effectively prevent memory loss caused by one-time information delivery.12 Patients can replay content as needed to compensate for age-related memory decline, which further enhances the practical effectiveness of the tool.
Reasons for the Relatively Lower Score in Applicability
The applicability dimension of the tap-to-read audio-assisted health education tool evaluates its adaptability among elderly patients with varying educational backgrounds, disease severity and family support levels. Although the score of 4.53 remains at a relatively high level, it is markedly lower than the satisfaction score of 4.96.
Despite the promising findings of this pilot study, several limitations must be acknowledged. First, the small sample size (n=20) and single-center design limit the statistical power and generalizability of the results. Findings may not be representative of older PCI patients in other regions, healthcare systems, or with different demographic characteristics. Second, convenience sampling was employed without a control group, which introduces selection bias and precludes causal inferences regarding the tool’s effectiveness. Third, the inclusion criteria required normal eyesight and hearing; therefore, the tool’s applicability to older adults with hearing impairment, a common comorbidity in this population, was not evaluated. This is a notable gap, as the audio-assisted feature is central to the intervention. Fourth, although family/caregiver involvement was mentioned during the intervention (eg, caregivers received training alongside patients), the role of caregivers was not systematically analyzed or quantified. Future studies should formally assess caregiver engagement and its impact on patient outcomes. Finally, the 4-week follow-up period was relatively short; longer-term durability of the observed high acceptability and usability remains unknown. These limitations are inherent to the pilot nature of this study, and our conclusions should be interpreted as preliminary. Future large-scale, multicenter randomized controlled trials are warranted to validate and extend these findings.
Conclusion
In this pilot study, the pen-based, audio-assisted health education tool demonstrated preliminary feasibility and acceptable usability among older adults undergoing their first PCI procedure. The tool’s design, integrating text, images, audio, and video with pen-activated functionality, was well received by participants, as reflected in high questionnaire scores and positive qualitative feedback. However, these findings should be interpreted as hypothesis-generating rather than definitive evidence of effectiveness, given the small sample size, single-center design, short follow-up (4 weeks), and lack of a control group. Future research should employ large-scale, multicenter randomized controlled trials (RCTs) with longer follow-up periods to rigorously evaluate the tool’s impact on clinical outcomes, self-management behaviors, and long-term adherence. Additionally, adaptations for older adults with hearing impairment and more comprehensive content covering quantified rehabilitation guidance are warranted before broader implementation.
Abbreviations
PCI, Percutaneous Coronary Intervention; TAM, Technology Acceptance Model.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
This study was conducted with approval from the Ethics Committee of Beijing Luhe Hospital, Capital Medical University (No. 2020-LHKY-049-03), and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
The authors thank all individuals and institutions that supported this work. Financial support is gratefully acknowledged.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Figulla HR, Lauten A, Maier LS, Sechtem U, Silber S, Thiele H. Percutaneous coronary intervention in stable coronary heart disease -is less more? Dtsch Arztebl Int. 2020;117(9):137–9. doi:10.3238/arztebl.2020.0137
2. Lei H, Zhu L, Zhang X. Knowledge, attitude, and practice toward postoperative self-management among patients after percutaneous coronary intervention: a structural equation modeling analysis. Clin Cardiol. 2024;47(3):e24232. doi:10.1002/clc.24232
3. Cao Z, Yan P, Hou F, et al. The mediating role of self-efficacy in the relationship between self-management and health-promoting behaviors in post-PCI patients. PLoS One. 2026;21(1):e0341826. doi:10.1371/journal.pone.0341826
4. Xi G, Yang F, Xu J, Liu J, Chen D. Using secondary prevention strategies in patients after PCI: a narrative review. Front Public Health. 2025;13:1562201. doi:10.3389/fpubh.2025.1562201
5. Jacob C, Sezgin E, Sanchez-Vazquez A, Ivory C. Sociotechnical factors affecting patients’ adoption of mobile health tools: systematic literature review and narrative synthesis. JMIR Mhealth Uhealth. 2022;10(5):e36284. doi:10.2196/36284
6. Schorr EN, Gepner AD, Dolansky MA, et al. Harnessing mobile health technology for secondary cardiovascular disease prevention in older adults: a scientific statement from the American heart association. Circ Cardiovasc Qual Outcomes. 2021;14(5):e000103. doi:10.1161/HCQ.0000000000000103
7. Lee JWY, Tan JY, Bello F. Technology acceptance model in medical education: systematic review. JMIR Med Educ. 2025;11:e67873. doi:10.2196/67873
8. Damluji AA, Nanna MG, Mason P, et al. Coronary artery revascularization in the older adult population: a scientific statement from the American heart association. Circulation. 2025;152(25):e494–e525. doi:10.1161/CIR.0000000000001387
9. Liu N, Yin J, Tan SS, Ngiam KY, Teo HH. Mobile health applications for older adults: a systematic review of interface and persuasive feature design. J Am Med Inform Assoc. 2021;28(11):2483–2501. doi:10.1093/jamia/ocab151
10. Ferraz LT, Santos AJT, Lorenzi LJ, Frohlich DM, Barley E, Castro PC. Design considerations for the migration from paper to screen-based media in current health education for older adults: a scoping review. BMJ Open. 2024;14(4):e078647. doi:10.1136/bmjopen-2023-078647
11. Simon ST, Kini V, Levy AE, Ho PM. Medication adherence in cardiovascular medicine. BMJ. 2021;374:n1493. doi:10.1136/bmj.n1493
12. Jones WE, Benge JF, Scullin MK. Preserving prospective memory in daily life: a systematic review and meta-analysis of mnemonic strategy, cognitive training, external memory aid, and combination interventions. Neuropsychology. 2021;35(1):123–140. doi:10.1037/neu0000704
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.