Back to Journals » International Journal of Women's Health » Volume 9
A pilot randomized controlled clinical trial of second uterine curettage versus usual care to determine the effect of re-curettage on patients’ need for chemotherapy among women with low risk, nonmetastatic gestational trophoblastic neoplasm in Urmia, Iran
Authors Ayatollahi H, Yekta Z, Afsari E
Received 8 April 2017
Accepted for publication 21 July 2017
Published 21 September 2017 Volume 2017:9 Pages 665—671
DOI https://doi.org/10.2147/IJWH.S139226
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Haleh Ayatollahi,1 Zahra Yekta,2 Elnaz Afsari1
1Department of Gynecology and Obstetrics, Reproductive Health Research Center, 2Department of Community and Preventive Medicine, Urmia University of Medical Sciences, Urmia, Iran
Objective: The objective of this study was to determine if second curettage was associated with a decreased need for the number of chemotherapy treatments compared to usual care.
Methods: A pilot randomized controlled clinical trial was designed at Motahhari Referral Hospital in 2014. Fifty-two patients with low risk, nonmetastatic gestational trophoblastic neoplasm were assigned randomly to two arms. The interventional arm included a repeat uterine curettage, and the control group received standard care (chemotherapy). All participants were followed periodically over 6 months. Primary outcome was defined as the number of chemotherapy courses in each arm. Student’s t-test and receiver operator characteristics (ROC) curve were applied for statistical analysis as appropriate.
Results: Fifty percent of participants who underwent re-curettage did respond to intervention with no further chemotherapy after 6 months of follow-up. The intervention arm had higher number of remissions without chemotherapy compared to those who received usual care. In the subgroup analysis, the ROC curve could predict the re-curettage treatment response by beta human chorionic gonadotropin (BhCG) level significantly. No complications were reported in the intervention arm.
Conclusion: Second curettage is an alternative effective procedure to decrease the need for chemotherapy among patients with low risk, nonmetastatic gestational trophoblastic neoplasm. Further clinical trials with larger sample size may be needed to determine the effective role of second curettage among patients.
Keywords: gestational trophoblastic neoplasm, uterine curettage, chemotherapy
Introduction
Gestational trophoblastic diseases (GTDs) represent a wide spectrum of disorders from hydatidiform mole (complete and partial) to choriocarcinoma with various nonsignificant clinical presentations.1
The epidemiology of GTDs is not well defined due to rarity of the disease and challenges in data collection. However, its incidence appears to be influenced by age, geographic region, ethnicity, reproductive history, socioeconomic conditions, and dietary deficiencies.2–8
Post-molar GTN, defined as plateauing of beta human chorionic gonadotropin (BhCG) for three consecutive weekly measurements or rising BhCG in the serum for two consecutive weekly measurements, is highly curable, and nonlife threatening.9–11 There are various pathologic types for GTN; however, the reported prevalence of post-molar GTN is 20% in complete hydatidiform mole and 0.5%–9.9% in partial hydatidiform mole.12,13 While chemotherapy is considered the standard of care for patients with low risk, nonmetastatic GTN, according to recent studies, repeat uterine evacuation has been explored as an alternative approach for nonmetastatic low risk GTN.1,14 Currently, existing evidence is inconsistent regarding the curative effect of second curettage in post-molar trophoblastic disease.15 In a retrospective cohort study, a significantly lower number of patients who had uterine re-evacuation required chemotherapy compared to controls. In addition, having a uterine re-evacuation was also associated with a lower number of chemotherapy courses among those who did require medical treatment later.15 However, only a limited number of patients appear to benefit from re-evacuation (9.4%).15 A randomized clinical trial conducted by Osborne et al evaluated the efficacy and safety of second curettage regarding the number of remissions among patients.16 They suggested re-curettage as an initial treatment for post-molar GTN patients with 40% positive response rate without significant morbidity.16 Another observational study reported that 60% of patients with second curettage were cured completely with no need for additional chemotherapy.1 On the contrary, there is evidence that considers second evacuation as an unnecessary procedure with unknown benefit and adverse complications including uterus perforation. Therefore, they emphasized prioritizing immediate medical treatment in post-molar GTN management.17,18
Differences in participant characteristics, varying definitions of post-molar GTN, and limitations related to observational study design have been suggested as potential explanation for observed contradictions in the literature.1,10,14,15
Motahhari Teaching Hospital in West Azerbaijan province is a referral center for managing gestational trophoblastic disease. The prevalence of post-molar GTN among patients referred with hydatidiform mole is 20% which is relatively the same as other studies.12,13 The social impact of the recent economic sanctions in Iran has included a rapid decline in the household income for many families, resulting in limited access to previously available chemotherapy medication. In addition, many patients in this population are reluctant to receive chemotherapy medication for social reasons. Therefore, although the results of chemotherapy for persistent GTD are generally excellent, the benefits were not observed among our patients due to the limited drug adherence. We therefore sought to provide evidence-based data for the effectiveness of alternative treatments as existing data are primarily based on observational studies and prone to potential biases. In this pilot randomized controlled trial (RCT), we aimed to compare the effect of second uterine curettage versus usual care based on the required courses of chemotherapy among women with low risk, nonmetastatic gestational trophoblastic neoplasm.
Materials and methods
This is a pilot RCT study which was conducted at Motahhari Teaching Hospital in the province of West Azerbaijan, Iran between 2014 and 2015.
Persistent low risk GTD according to International Federation of Gynecology and Obstetrics (FIGO)/World Health Organization (WHO) staging and risk score is defined by one of the following criteria:19
- <10% decline in BhCG levels in four consecutive measurements over a 3-week period;
- >20% rise in BhCG levels in three consecutive measurements over a 2-week period;
- elevated BhCG level for >6 months, and risk score less than six according to WHO.
We excluded patients with evidence of metastasis and recurrent GTN who had previously been treated with chemotherapy. Patients whose disease had transformed into choriocarcinoma, placental site trophoblastic tumor, or epithelioid tumor (histologically diagnosed at curettage procedure) were excluded from the study. The study population included complete and partial mole.
Patients presenting with post-molar GTN were recruited as eligible population and assigned to each arm by using a concealed envelope. A trained nurse was responsible for randomization. Once a patient consented to participate in the trial, a sealed opaque envelope containing the random number was opened and the patient was then offered the allocated treatment approach. While due to the nature of the intervention, placebo was not possible, the gynecology residence was blinded to record data over the follow-up period.
Nine out of 62 recruited patients did not meet the study inclusion criteria during the study. Reasons for exclusion were choriocarcinoma (two patients in the control arm and one in the intervention arm), and developing high risk post-molar GTN (three patients in each group). There was one loss to follow-up in the intervention arm. Consort flow design is represented in Figure 1.
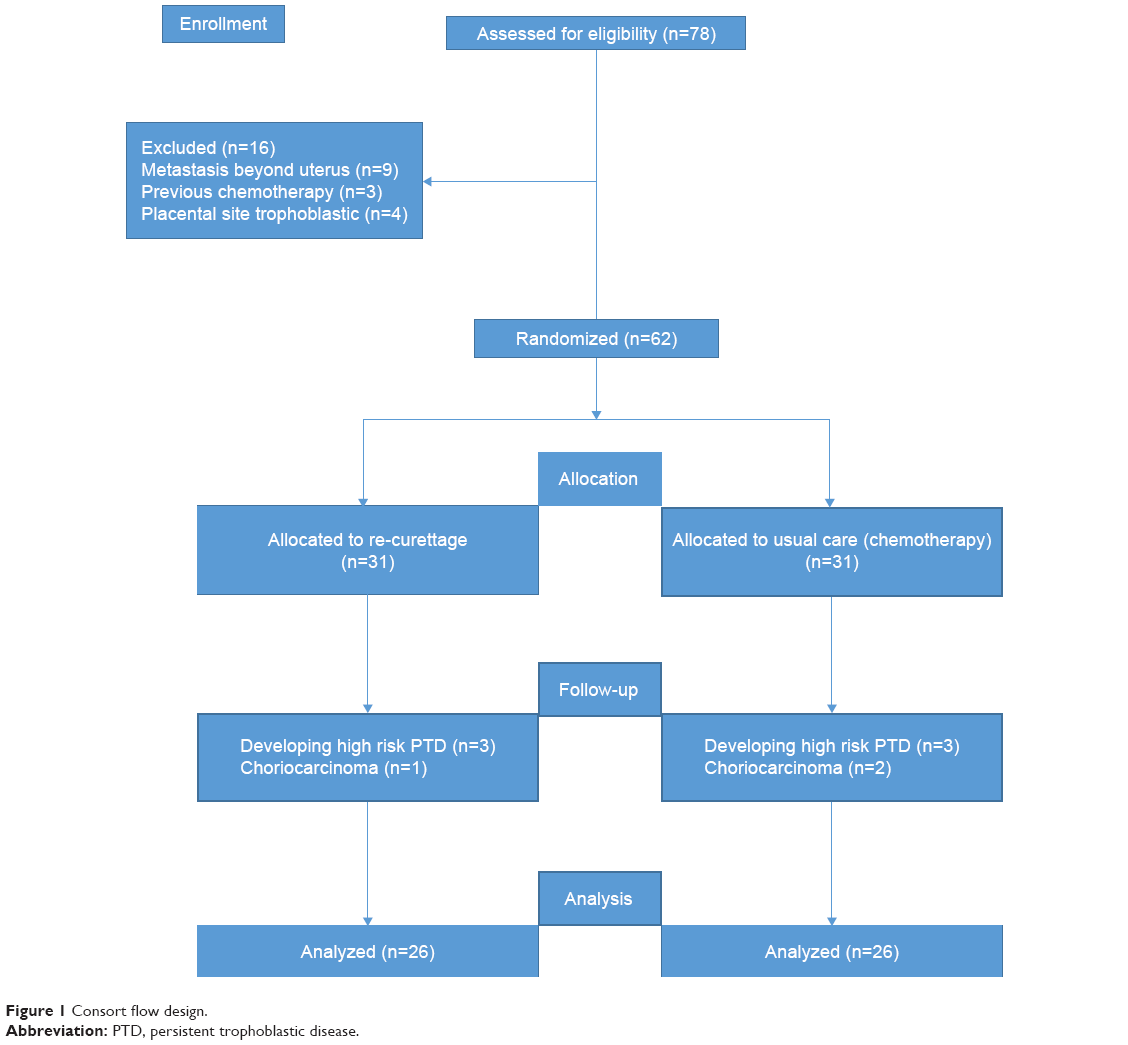 | Figure 1 Consort flow design. |
The aim of the study and possible harm and benefits of the intervention versus usual care were explained to each participant. Patients and their husbands signed the consent form to participate. Urmia University of Medical Sciences Ethic Committee approved the protocol based on the Declaration of Helsinki (Ethics Committee identifier Ir.umsu.rec.1392.73). The protocol was reviewed and approved by Urmia University of Medical Sciences Institutional Board (clinical trial registration number 1363). The Solid Tumor Research Center of Urmia Medical Sciences University also approved the design of this study.
Cervical preparation with prostaglandin was performed in order to reach cervical ripening before second curettage. The method for quantitative determination of BhCG is a sandwich chemiluminescence immunoassay. The test was performed on a LIAISON Analyzer (LIAISON hCG, Ref 312311; DiaSorin, Saluggia, Italy). The median of the reference range among women was 0.6 (95th percentile =2.4).
The intervention was defined as second uterine evacuation. Re-curettage was performed by one gynecologist and one pathologist examined all samples to report the type of tumor.
Follow-up sessions for the intervention arm were scheduled 24 hours and 1 week after re-curettage; it was continued until the beta level became normal for three consecutive weeks. After that, patients were followed monthly over 6 months to make certain of normalizing BhCG level. For patients with increasing BhCG after 1 week, chemotherapy was initiated.
In the control group, patients received chemo medications as usual care. Weekly low dose methotrexate (50 mg/m2, intramuscular) was used to treat control participants as the first line treatment in this study. BhCG levels were measured weekly until BhCG became normal for three consecutive weeks, then monthly follow-up for at least 1 year was continued by BhCG measurement.
Primary outcome was defined as the number of chemotherapy courses. Secondary outcome was defined as the number of weeks of therapy required to obtain complete response in each arm.
We also recorded curettage complications such as uterus perforation, bleeding, and chemo side effects. Some covariates like age, parity, blood group, hemoglobin, and pathologic type of tumor were also recorded in dataset.
SPSS (SPSS Inc, Chicago, IL, USA) was used for statistical analysis. Normality of distribution was explored by Kolmogrov–Smirnov test. Descriptive statistics were reported as mean (standard deviation) or median (interquartile range) for continuous variables and frequency (percentage) for categorical variables. We also reported 95% confidence intervals for percentages. Student’s t-test and Wilcoxon rank sum test were used to compare continuous variables, as appropriate. Differences in categorical variables between groups were tested by using chi-square test.
In the subgroup analysis, receiver operator characteristics (ROC) curve was used to determine the cutoff point for BhCG level to distinguish patients who required chemotherapy after second curettage. The overall performance was assessed by the area under the ROC curve, in which the area closer to one represents the optimum capability for discrimination. All tests were considered statistically significant at P<0.05.
Results
A total of 62 patients were recruited and randomized to each arm. During the study, nine patients were excluded, with exclusion reasons detailed in the consort flow design in Figure 1.
Table 1 shows the distribution of basic characteristics among participants. The mean age of participants in the intervention arm was 31.37±10.11 versus 27.80±7.58 in the control group (P=0.15). There was a similar distribution in each arm for nulliparity and blood groups. Pathologic types were reported as complete mole and partial mole hydatidiform. We found equally distributed pathologic types across either arm.
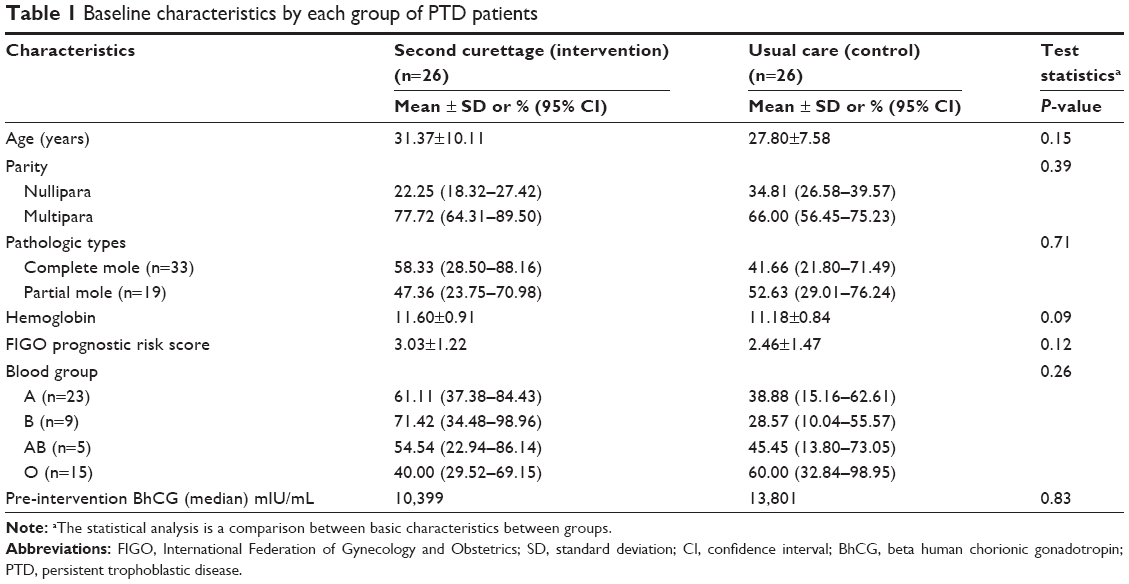 | Table 1 Baseline characteristics by each group of PTD patients |
Since BhCG was highly skewed in both groups, the median was used for comparison which showed no significant statistical difference between groups. Patients’ baseline characteristics in each group are shown in Table 1.
Fifty percent (13/26) of participants were cured after second curettage with no need for chemotherapy. The number of chemotherapy courses in re-curettage participants compared to the control group was not statistically significant after complete follow-up (6.69±3.17 vs 3.07±2.55). The mean of the number of weeks to obtain optimal result based on the negative level of BhCG after chemotherapy was significantly lower in patients with re-curettage evacuation. Table 2 compares the clinical manifestations at the end of follow-up in each group.
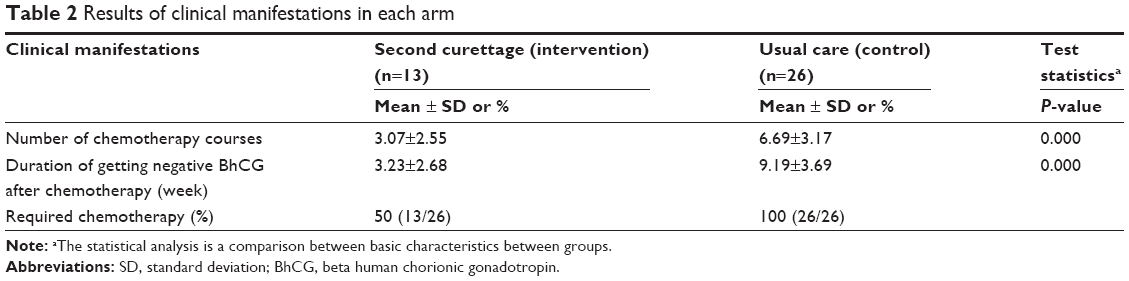 | Table 2 Results of clinical manifestations in each arm |
In the subgroup analysis of the intervention arm, the percentage of decline in BhCG level for patients who responded to second curettage after 24 hours was 65% versus 38% in BhCG level among those who failed the re-curettage procedure and then needed further chemotherapy.
ROC curve was also used to determine the level of BhCG to predict a positive response to second curettage with no further chemotherapy in the subgroup analysis. The curve indicated the 0.8 area under the curve which was statistically significant (Figure 2). BhCG 1,983 mIU/mL was set as the cutoff which perfectly distinguish the required chemo after re-curettage with 93% sensitivity and 75% specificity. No complications due to first and second curettage were reported during the study follow-up.
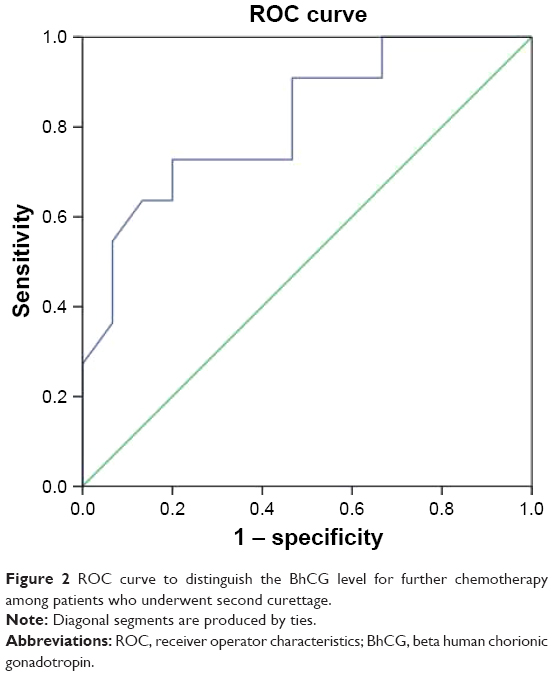 | Figure 2 ROC curve to distinguish the BhCG level for further chemotherapy among patients who underwent second curettage. |
Discussion
In post-molar GTN, tumor activity continues despite uterine evacuation of a hydatidiform mole as measured by subsequent unaltered high or even surging BhCG concentrations in the blood.15 While the current standard of care includes the use of chemotherapy medication as first line therapy for post-molar GTN patients, second curettage has been suggested as an alternative surgical procedure based on the results of observational data in different settings. Our study found a significant association between second curettage and a reduced number of patients who needed chemotherapy among post-molar GTN patients. In addition, among patients who required chemotherapy after second curettage, there was a significant decrease in the number of chemotherapy courses. BhCG before second curettage could significantly distinguish patients’ response to second curettage versus those needing chemotherapy. These results suggested that second curettage could be an important effective approach in the treatment of post-molar GTN patients, although additional clinical trial studies may be needed to confirm these results.
Our study revealed that second curettage had a significant curative effect in post-molar GTN low risk patients who met FIGO/WHO criteria.20 Almost half of the patients were cured completely without receiving chemotherapy in our study. There is contradictory evidence regarding second curettage response rate.1,15,17,18,21 One retrospective study demonstrated that 16% of participants experienced remission without chemotherapy after second curettage. Since 8% of these patients had uterine perforation after the second curettage, investigators in this study were reluctant to recommend re-curettage as the primary approach for post-molar GTN.17 Likewise, van Trommel et al found a small clinical impact of second curettage on patients’ outcome (9.4%).15 On the contrary, Pezeshki et al reported that 60% of patients undergoing re-curettage did not require chemotherapy.1 A Phase II clinical trial indicated a second curettage curable rate of 40% with no significant adverse effects.16 There are some explanations for this contradictory evidence. First of all, they used different systems for disease definition and classifications. One study recommended second curettage for those with less than three consecutive BhCG weekly measurements which is not consistent with post-molar GTN definitions.1 Meanwhile, the observational design introduced some potential biases that can impact interpretation of results. Patients’ drug adherence, ethnicity, and insurance policy were also some factors which may directly influence the treatment approach in different medical centers.
In our study, the number of courses of chemotherapy was significantly lower after second curettage as compared to the control group. We also revealed that the duration of obtaining an effective response after chemotherapy based on BhCG negative result was significantly lower in patients with second curettage with no reported medication resistance versus the control group. Taylor et al demonstrated that patients with a FIGO/WHO score of 6 may develop treatment resistance compared to those with a score <5.22 However, all participants included in our study had a risk score <6. The result of our study was also consistent with several other studies which reported significant lower course of chemotherapy after re-curettage.1,15,23 A debulking effect has been suggested to explain the potential reason of reduction in chemotherapy courses among patients receiving second curettage.
Second curettage complications like perforation which were reported in some studies make investigators reluctant to recommend second curettage.1,15 No complications after re-curettage were observed in our study. There might be some reasons that explain the lack of complications in our study. Curettage and re-curettage were performed with sonography guidance which reduced the risk of uterine perforation. Patients also received serum misoprostol after curettage to prevent the risk of uterine bleeding.
One limitation of this study was small sample size. It was a pilot clinical trial, with time and budget restrictions. In addition, patients were not followed up over the long-term, limiting our ability to assess long-term curettage complications such as Asherman’s syndrome.
In conclusion, in this pilot controlled clinical trial, second curettage was associated with lower number of patients who required chemotherapy. Subgroup analysis indicated that the BhCG level before second curettage was a significant predictor for effective outcome with no further chemotherapy. We recommend conducting additional clinical trials with larger sample size to confirm the effectiveness of second curettage among women with persistent, low risk, nonmetastatic gestational trophoblastic neoplasm.
Disclosure
The authors report no conflicts of interest in this work.
References
Pezeshki M, Hancock BW, Silcocks P, et al. The role of repeat uterine evacuation in the management of persistent gestational trophoblastic disease. Gynecol Oncol. 2004;95(3):423–429. | ||
Gockley AA, Joseph NT, Melamed A, et al. Effect of race/ethnicity on clinical presentation and risk of gestational trophoblastic neoplasia in patients with complete and partial molar pregnancy at a tertiary care referral center. Am J Obstet Gynecol. 2016;215(3):334. | ||
Gockley AA, Melamed A, Joseph NT, et al. The effect of adolescence and advanced maternal age on the incidence of complete and partial molar pregnancy. Gynecol Oncol. 2016;140(3):470–473. | ||
Bakhtiyari M, Mirzamoradi M, Kimyaiee P, et al. Postmolar gestational trophoblastic neoplasia: beyond the traditional risk factors. Fertil Steril. 2015;104(3):649–654. | ||
Steigrad SJ. Epidemiology of gestational trophoblastic diseases. Best Pract Res Clin Obstet Gynaecol. 2003;17(6):837–847. | ||
Stafford L, Judd F. What do women with gestational trophoblastic disease understand about the condition? Int J Gynecol Cancer. 2011;21(1):161–166. | ||
Ozalp SS. Regional perspectives on gestational trophoblastic disease in Turkey. J Reprod Med. 2008;53(8):639–642. | ||
Maesta I, Berkowitz RS, Goldstein DP, Bernstein MR, Ramirez LA, Horowitz NS. Relationship between race and clinical characteristics, extent of disease, and response to chemotherapy in patients with low-risk gestational trophoblastic neoplasia. Gynecol Oncol. 2015;138(1):50–54. | ||
Sun SY, Goldstein DP, Bernstein MR, et al. Maternal near miss according to World Health Organization classification among women with a hydatidiform mole: experience at the New England Trophoblastic Disease Center, 1994–2013. J Reprod Med. 2016;61(5–6):210–214. | ||
Goldstein DP, Garner EI, Feltmate CM, Berkowitz RS. The role of repeat uterine evacuation in the management of persistent gestational trophoblastic disease. Gynecol Oncol. 2004;95(3):421–422. | ||
Stevens FT, Katzorke N, Tempfer C, et al. Gestational trophoblastic disorders: an update in 2015. Geburtshilfe Frauenheilkd. 2015;75(10):1043–1050. | ||
Berkowitz RS, Goldstein DP. Gestational trophoblastic disease. Cancer. 1995;76(10 Suppl):2079–2085. | ||
Goto S, Yamada A, Ishizuka T, Tomoda Y. Development of postmolar trophoblastic disease after partial molar pregnancy. Gynecol Oncol. 1993;48(2):165–170. | ||
Garner EI, Feltmate CM, Goldstein DP, Berkowitz RS. The curative effect of a second curettage in persistent trophoblastic disease: a retrospective cohort survey. Gynecol Oncol. 2005;99(1):3–5. | ||
van Trommel NE, Massuger LF, Verheijen RH, Sweep FC, Thomas CM. The curative effect of a second curettage in persistent trophoblastic disease: a retrospective cohort survey. Gynecol Oncol. 2005;99(1):6–13. | ||
Osborne RJ, Filiaci VL, Schink JC, et al. Second curettage for low-risk nonmetastatic gestational trophoblastic neoplasia. Obstet Gynecol. 2016;128(3):535–542. | ||
Schlaerth JB, Morrow CP, Rodriguez M. Diagnostic and therapeutic curettage in gestational trophoblastic disease. Am J Obstet Gynecol. 1990;162(6):1465–1470. | ||
Berkowitz RS, Goldstein DP. Chorionic tumors. N Engl J Med. 1996;335(23):1740–1748. | ||
FIGO Oncology Committee. FIGO staging for gestational trophoblastic neoplasia 2000. Int J Gynaecol Obstet. 2002;77(3):285–287. | ||
Ngan HY, Kohorn EI, Cole LA, et al. Trophoblastic disease. Int J Gynaecol Obstet. 2012;119(Suppl 2):S130–S136. | ||
Soper JT. Role of surgery and radiation therapy in the management of gestational trophoblastic disease. Best Pract Res Clin Obstet Gynaecol. 2003;17(6):943–957. | ||
Taylor F, Grew T, Everard J, et al. The outcome of patients with low risk gestational trophoblastic neoplasia treated with single agent intramuscular methotrexate and oral folinic acid. Eur J Cancer. 2013;49(15):3184–3190. | ||
Hemida RA, Toson E, Van Doorn HC. The impact of uterine re-curettage, pre-evacuation and week-one level of hCG on the number of chemotherapy courses in treatment of post molar GTN. J Exp Ther Oncol. 2011;9(3):217–220. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.