Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 15
A Phase 1, Multicenter, Open-Label Study to Evaluate the Pharmacokinetics of Iberdomide in Subjects with Mild, Moderate, or Severe Hepatic Impairment Compared with Healthy Subjects
Authors Cheng Y ![]() , Ye Y, Gaudy A, Ghosh A, Xue Y, Wang A, Zhou S, Li Y
, Ye Y, Gaudy A, Ghosh A, Xue Y, Wang A, Zhou S, Li Y
Received 8 December 2022
Accepted for publication 17 February 2023
Published 28 February 2023 Volume 2023:15 Pages 9—19
DOI https://doi.org/10.2147/CPAA.S397826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Yiming Cheng,1 Ying Ye,1 Allison Gaudy,1 Atalanta Ghosh,2 Yongjun Xue,3 Alice Wang,1 Simon Zhou,1 Yan Li1
1Clinical Pharmacology & Pharmacometrics, Bristol Myers Squibb, Princeton, NJ, USA; 2Global Biometrics and Data Sciences, Bristol Myers Squibb, Princeton, NJ, USA; 3Nonclinical Research & Development, Bristol Myers Squibb, Princeton, NJ, USA
Correspondence: Yan Li, Clinical Pharmacology & Pharmacometrics, Bristol Myers Squibb, 556 Morris Ave, Summit, Princeton, NJ, 07901, USA, Tel +1 908-481-6203, Email [email protected]
Introduction: Iberdomide, a novel cereblon modulator (CELMoD®), is currently under clinical investigation for hematology indications. To evaluate the influence of hepatic impairment on the pharmacokinetics (PK) of iberdomide and its major active metabolite M12, a phase 1, multicenter, open-label study was conducted in healthy subjects and subjects with mild, moderate, and severe hepatic impairment.
Methods: Forty subjects were enrolled in the study and divided into five groups based on hepatic function. 1 mg iberdomide was administered and plasma samples were collected to evaluate the pharmacokinetics of iberdomide and M12.
Results: After a single dose of iberdomide (1 mg), mean iberdomide Cmax (maximum observed concentration) and AUC (area under the concentration-time curve) exposure were generally comparable between hepatic impairment (HI) subjects (severe, moderate and mild) and their respective matched normal controls. Mean Cmax and AUC exposure of the metabolite M12 were generally comparable between mild HI and matched normal subjects. However, mean Cmax of the M12 was 30% and 65% lower and AUC was 57% and 63% lower in moderate and severe HI subjects as compared to their respective matched normal controls. However, given the relatively low M12 exposure as compared to its parent drug, the observed differences were not considered clinically meaningful.
Conclusion: In summary, 1 mg single oral dose of iberdomide was generally well-tolerated. HI (mild, moderate or severe) had no clinically relevant impact on iberdomide PK and therefore, no dose adjustment is warranted.
Keywords: hepatic impairment, iberdomide, pharmacokinetics
Introduction
Iberdomide, a novel cereblon modulator, is under clinical development for hematological malignancies and inflammatory and autoimmune-mediated diseases.1–13
Iberdomide plasma exposure increased proportionally with dose (0.1 to 6 mg) in human. Iberdomide was quickly absorbed with a median Tmax (time to Cmax) between 2.5 and 4 hours. The terminal half-life (t1/2) of iberdomide was around 9 to 13 hours.14 No significant food effect was identified.14
Iberdomide was primarily metabolized by CYP3A enzymes. Based on a clinical drug–drug interaction study, a strong CYP3A inhibitor (itraconazole) augmented the iberdomide AUC by 136%; while a strong CYP3A inducer (rifampin) significantly lowered iberdomide exposure by 82% for AUC and 70% for Cmax, respectively.15 At clinically relevant concentrations, iberdomide showed no notable inhibition effects on human efflux and uptake transporters, including MRP2, OAT1, OAT3, OATP1B1, OATP1B3, OCT2, MATE1, MATE2k, P-gp and BCRP.15
Human absorption, distribution, metabolism, and excretion (ADME) study on iberdomide (data on file) showed that based on total radioactivity (TRA) in systemic circulation, the major component in plasma was iberdomide (59%) and its major and pharmacologically active metabolite M12 (14%). In the excreta, the recovery of TRA was 88.5% and iberdomide was approximately 16% in urine and 11% in feces, suggesting extensively metabolism. In vitro human plasma protein binding of iberdomide and M12 is approximately 78% and 67%, respectively.16 The pharmacokinetics (PK) of M12 was characterized in an integrated population PK analysis, which showed that M12 PK tracked the PK of iberdomide and the metabolite to parent ratio was consistent across doses and time.16
Acute and chronic liver diseases are leading causes of morbidity and mortality worldwide.17,18 Alterations of excretory and metabolic activities by hepatic impairment can lead to drug accumulation or, less often, failure to form an active metabolite, which may trigger efficacy and/or safety concerns for certain drugs. Therefore, clinical studies in patients with hepatic impairment, usually performed during drug development, can provide information that may help guide initial dosing in patients.19 Like other similar class of compounds, iberdomide is intended for elder patient population and thus is often associated with a high prevalence of chronic liver disease.20 Since hepatic metabolism constitutes a relatively major clearance pathway for iberdomide, hepatic impairment could potentially impact the PK of iberdomide and its metabolites by altering hepatic clearance. As such, a clinical study (CC-220-CP-007; clinicalTrials.gov identifier: NCT03824678) was carried out with the objective to evaluate the impact of HI (mild, moderate, and severe) on iberdomide PK and its major active metabolite M12.
Method
Ethical Conduct of the Study
All subjects confirmed their informed consent in writing prior to screening. This study complies with the ethical principles of the International Council for Harmonisation (ICH) harmonised tripartite guideline E6(R2): Good Clinical Practice (GCP): integrated addendum to E6(R1) and with the Declaration of Helsinki, Title 21 of the US Code of Federal Regulations, Parts 50 and 56 concerning informed consent and institutional review board regulations, and applicable national, state, and local laws or regulations. The study was performed by PPD, Inc. (Austin, TX, USA) and approved by the institutional review boards of IntegReview institutional review boards (Austin, TX, USA) and Advarra institutional review boards (Columbia, MD, USA). This study was conducted from February 13, 2019 to June 18, 2019.
Study Design
This was an open-label study to compare the PK of iberdomide between HI subjects (mild, moderate, and severe) and their respective sex, age (± 10 years), and weight (± 13.6 kg [30 pounds]) matched normal controls. The study had screening (Day −29 through Day-2), treatment period (Day −1 to Day 5), and follow-up telephone call on Day 10 (± 1 day) periods.
Child-Pugh Classification Criteria was used to determine HI degree during screening. Subjects were divided into following groups with approximately 8 subjects in each group.
- Group 1: Child Pugh score of ≥ 5 to ≤ 6 (Mild HI)
- Group 2: Child Pugh score of ≥ 7 to ≤ 9 (Moderate HI)
- Group 3: Child Pugh score of ≥ 10 to ≤ 13 (Severe HI)
- Group 4: Normal subjects matched to Group 2
- Group 5: Normal subjects matched to Group 3
Blood Collection for Pharmacokinetic Analysis
Serial blood sampling for the determination of iberdomide and metabolite M12 concentrations in plasma was performed at the following time points:
- predose, 1, 2, 3, 4, 6, 8, 12, 24 36, 48, 72, and 96 hours postdose.
Bioanalytical Methodology
Briefly, following blood collection, plasma was harvested, and liquid chromatography-tandem mass spectrometry assays (LC-MS/MS) were used to measure iberdomide and M12 in plasma. Detail descriptions regarding bioanalytical methods were referred to previous publications.8,14,15
Pharmacokinetic Analyses
The plasma PK parameters of iberdomide and metabolite M12, including but not limited to Cmax, Tmax and AUC, were determined using noncompartmental methods in Phoenix WinNonlin Version 6.3 (St. Louis, Missouri).
Statistical Analyses
Plasma concentrations and PK parameters were summarized using descriptive statistics.
Analysis of variance (ANOVA) was used to calculate geometric means ratio (GMR) and associated 90% confidence interval between HI group and respective matched controls. Group was included in the ANOVA model as a fixed effect. Nonparametric method was used for Tmax.
In addition, graphical display and regression analysis were performed to assess the correlation between PK parameters (ie, Cmax and AUC) with each of the following covariates, as deemed appropriate: Child-Pugh scores, baseline serum albumin, serum bilirubin, and prothrombin time.
Safety Assessment
Current version of the Medical Dictionary for Drug Regulatory Activities (MedDRA) classification system was used to record and code adverse events (AEs). AEs, treatment-emergent AEs (TEAEs), serious adverse events (SAEs), vital sign measurements, concomitant medications, physical examinations (PEs), 12-lead ECG data and clinical laboratory test results were summarized, as appropriate.
Results
Demographic and Other Characteristics at Baseline
The study enrolled 40 subjects and all subjects completed the study (no discontinuation).
Overall, similar demographic and baseline characteristics across groups were noted, as shown in Table 1. There were 26 male subjects (65.0%) and 14 female subjects (35.0%). Subjects were mostly white (82.5%) and Hispanic or Latino (55.0%), with a mean body weight of 81.74 kg (range 52.1 to 122.3 kg), a mean BMI (body mass index) of 29.08 kg/m2 (range 21.8 to 39.5 kg/m2), and a mean age of 58.2 years (range 42 to 70 years).
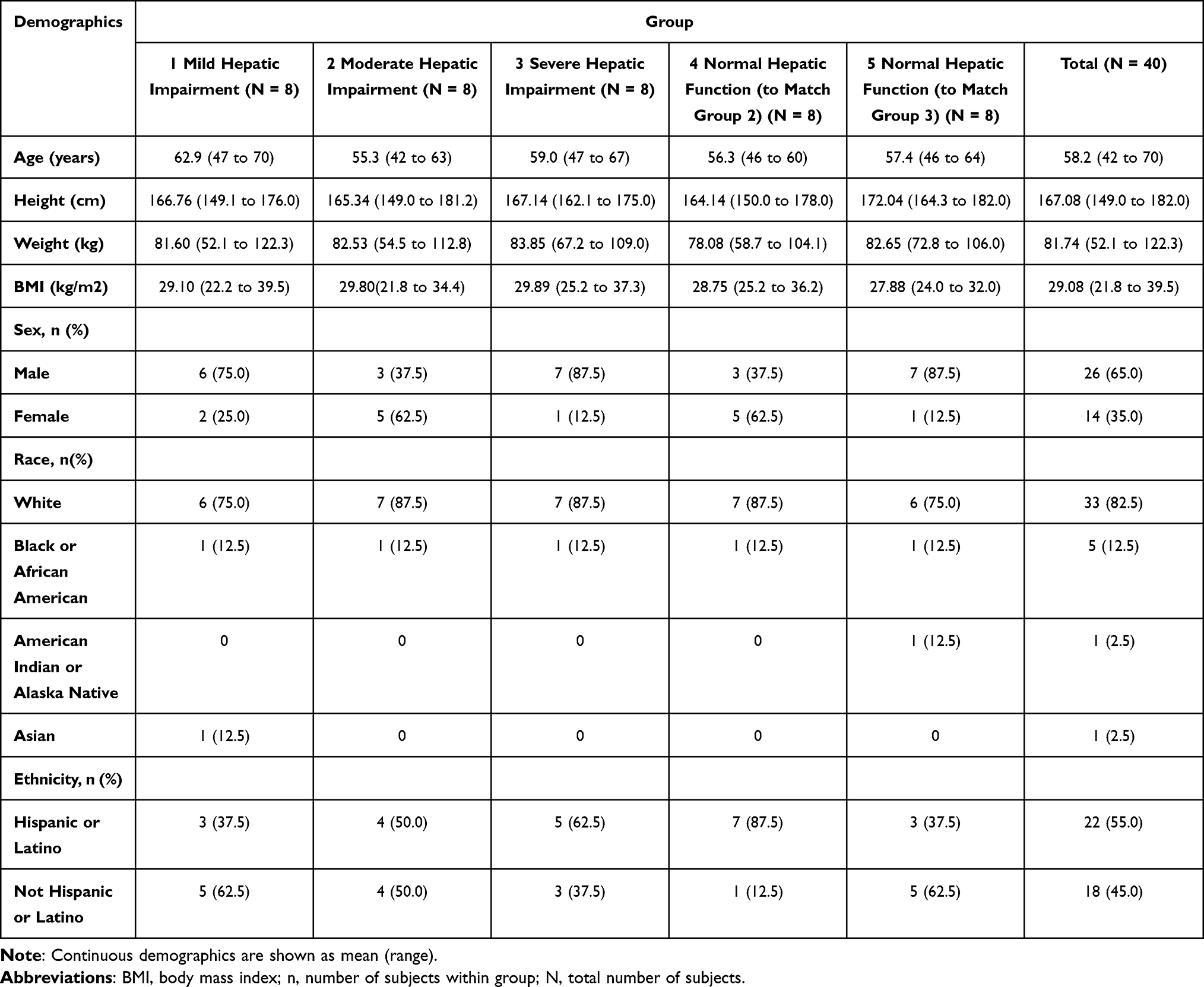 |
Table 1 Demographic and Baseline Characteristics |
Plasma Pharmacokinetics of Iberdomide and M12
Mean (±SD) plasma iberdomide and M12 concentration versus time profiles by treatment groups are presented in Figures 1 and 2, respectively. Plasma PK parameters of iberdomide and of the metabolite M12 are summarized in Table 2.
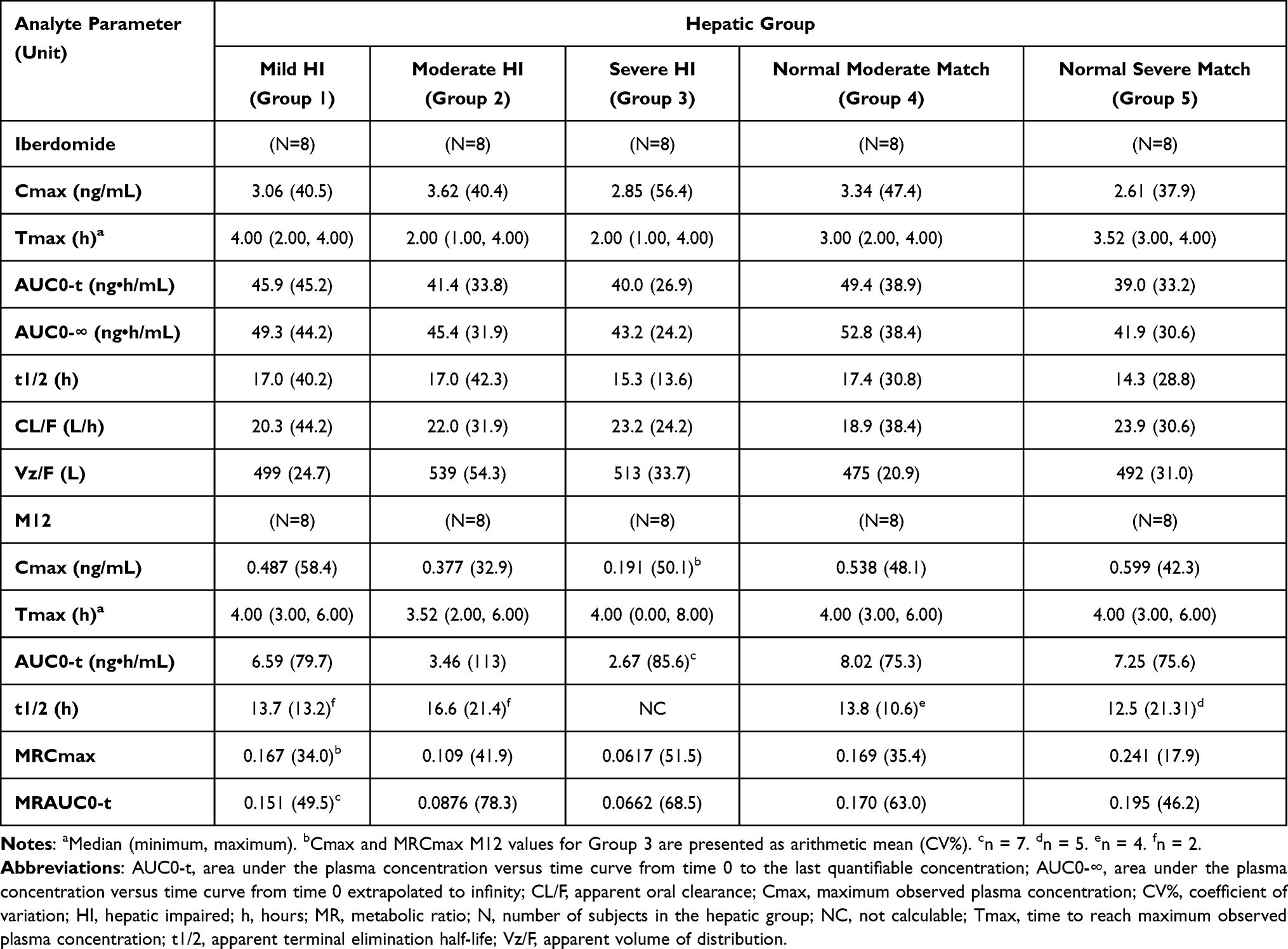 |
Table 2 Geometric Mean (Geometric CV%) of Iberdomide and M12 Plasma Pharmacokinetic Parameters |
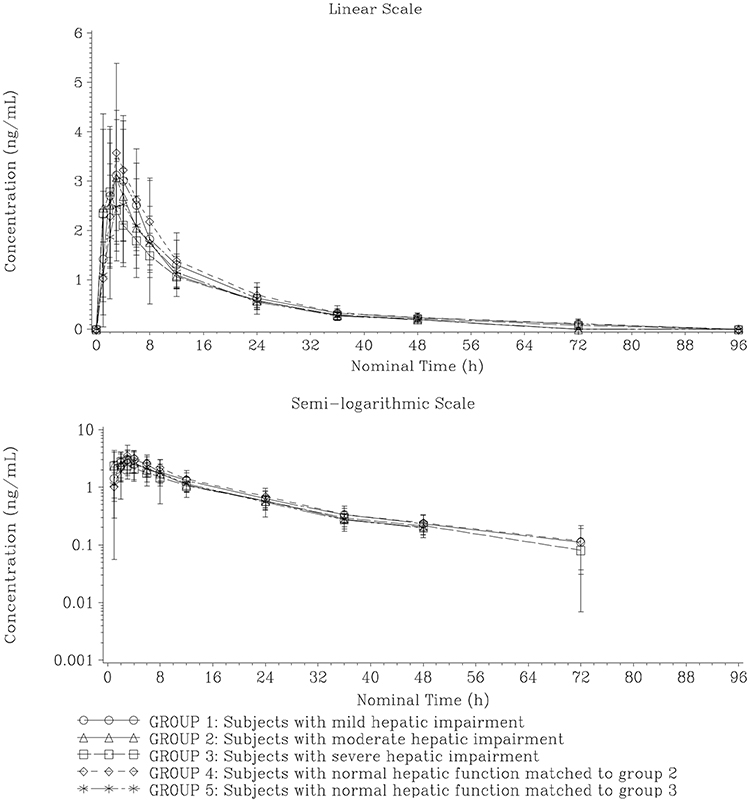 |
Figure 1 Mean (±SD) plasma concentration versus time profiles for iberdomide. |
 |
Figure 2 Mean (±SD) plasma concentration versus time profiles for M12. |
Following a single dose of 1 mg iberdomide, iberdomide Cmax was comparable among all subjects regardless of hepatic function (range: 2.61 to 3.62 ng/mL). Similar to Cmax, overall exposure (AUC0-∞) was comparable across all groups, ranging from approximately 41.9 ng•h/mL to 52.8 ng•h/mL, with moderate variability (CV% range of approximately 24% to 44%).
Iberdomide was quickly absorbed with a median Tmax occurring 2 to 4 hours post-dose across all groups. The geometric mean t1/2 of iberdomide was estimated from approximately 14.3 to 17.4 hours across all groups. Iberdomide apparent clearance (CL/F) was generally comparable among groups.
For the metabolite M12, Tmax was observed between 3.52 and 4.00 hours postdose across all groups. Thereafter, M12 PK decreased with geometric mean t1/2 values ranging from approximately 12.5 to 16.6 hours across all groups, except for Group 3 where it was not possible to estimate the geometric mean t1/2 due to the inadequate data (BLQ (below limit of quantification)) at terminal phase. The overall PK profiles of M12 were parallel with the PK profile of parent drug (iberdomide), which was in line with the recent parent-metabolite population pharmacokinetic (popPK) analysis.8
The geometric mean metabolite-to-parent ratios of the exposure parameters (MRCmax and MRAUC0-t) ranged from approximately 17–24% in normal controls. Similar results were observed in mild HI group (MRCmax and MRAUC0-t of 15–17%). The MRCmax and MRAUC0-t in moderate and severe HI groups were 9–11% and 6–7%, respectively, showing a trend of decreased metabolite-to-parent exposure ratios.
Statistical Assessment of Hepatic Impairment on the PK of Iberdomide
Table 3 summarized the statistical analyses results. After 1 mg oral dose of iberdomide, Cmax and AUC0-∞ were comparable between normal matched controls and mild HI, with geometric means ratio (90% CI) of 91.5% (63.1%, 132.7%) and 93.3% (65.8%, 132.4%) for Cmax and AUC0-∞, respectively. The Cmax geometric means ratio (90% CI) for the moderate and severe HI groups compared to normal matched controls were 108.2% (74.7%, 156.7%) and 109.1% (73%, 163.2%), respectively. The geometric means ratio (90% CI) for iberdomide AUC0-∞ were 86.0% (63.6%, 116.4%) and 103.0% (81.1%, 130.8%) in moderate and severe HI groups compared to normal matched controls, demonstrating similar exposure between HI groups and normal matched controls.
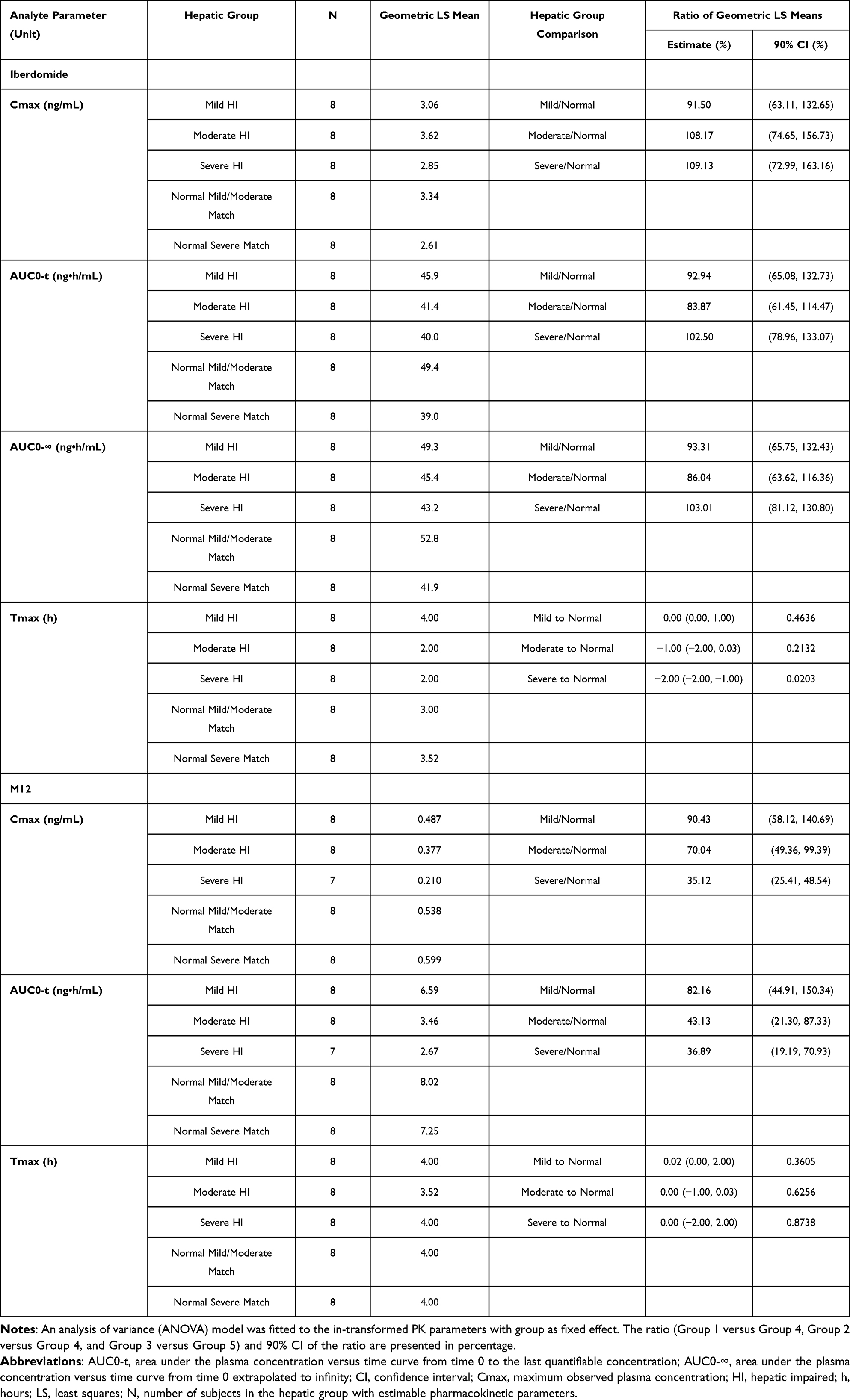 |
Table 3 Statistical Analysis of Plasma Pharmacokinetic Parameters of Iberdomide and M12 |
Mild HI subjects showed similar M12 exposures (Cmax and AUC0-t) as compared to their normal matched controls. M12 Cmax was 30% and 65% lower in moderate and severe HI as compared to their respective normal matched controls. Similarly, AUC0-t was 57% and 63% lower in moderate and severe HI as compared to normal matched controls, demonstrating a significant reduction in M12 exposure in moderate and severe HI subjects.
A statistically significant (p=0.0203) higher Tmax was observed for iberdomide in severe HI subjects. There was no statistically significant difference for iberdomide Tmax between mild and moderate HI subjects and their respective normal matched controls; the 90% CI for the difference in median estimates included zero.
The Tmax difference for M12 between mild, moderate, or severe HI and their respective controls was not statistically significant as the 90% CI for the difference in median estimates included zero.
Relationships Between Plasma Iberdomide and M12 PK Parameters and Liver Function Parameters at Baseline
The relationship between hepatic functions at baseline (baseline serum albumin, prothrombin time, baseline serum bilirubin and Child-Pugh score,) with iberdomide and M12 PK parameters was assessed graphically and using a linear regression analysis model as permitted by data. A summary of the regression coefficients and p-values from each regression analysis was presented in Table 4. An absence of significant association was noted between iberdomide PK parameters and any tested liver function parameters (p>0.05).
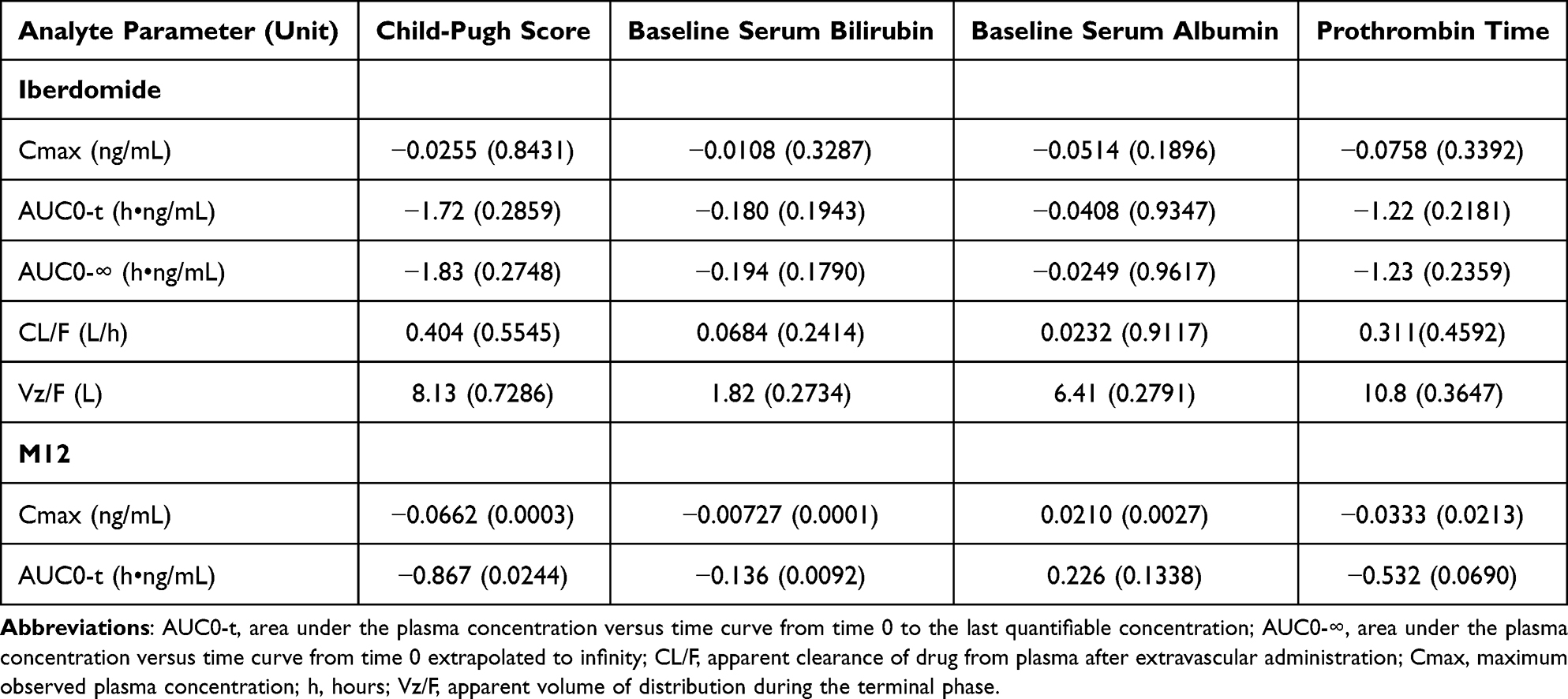 |
Table 4 Summary of Regression Analysis (Regression Coefficient [p-value]) of Pharmacokinetic Parameters for Plasma Iberdomide and M12 versus Baseline Liver Function Parameters |
For the metabolite M12, all liver function parameters showed significant correlations with Cmax (p ≤ 0.02). Two measures, Child-Pugh score and serum bilirubin at baseline were significantly negatively correlated with AUC0-t. The association tends to be negative for Cmax and AUC0-t across all baseline liver function parameters, suggesting a decreased exposure with higher baseline values, except for baseline serum albumin, which was positive, indicating higher exposure with higher baseline albumin.
Safety
Overall, iberdomide is well-tolerated in all subjects. Six (6) of 40 subjects (15.0%) reported TEAE at least once: mild diarrhea reported by two severe HI subjects; mild hordeolum reported by one subject in group 4; mild nasopharyngitis reported by one subject in group 5; mild dizziness reported by one subject with moderate HI; and mild pruritus reported by one subject in group 4. No mild HI subjects reported TEAEs. By the end of the study all TEAEs were resolved. No SAEs or deaths was reported during the study. The mean values at baseline for platelets, albumin, ALP (alkaline phosphatase), AST (aspartate aminotransferase), BILI (bilirubin), direct BILI, and GGT (gamma-glutamyl transferase) were outside of the reference ranges in HI subjects, which was as expected. There’s no notable change of aforementioned lab tests after dosing compared to those observed at baseline. No clinically relevant abnormal ECG results and vital signs was observed among groups.
Discussion and Conclusion
Evaluating the impact of HI on drug’s PK exposure is important. According to regulatory guidance, a HI clinical study is recommended if the metabolism and/or excretion of liver pathway constitutes a substantial proportion (>20% of the absorbed drug) of the elimination of a parent drug or active metabolite.19,21 The ADME study of iberdomide suggested that absorbed drug is extensively metabolized. This result, together with an in vitro assessment of CYP3A on iberdomide metabolism and a clinical drug–drug interaction study for iberdomide with strong CYP3A modulators,15 collectively suggested that the liver is heavily involved in the elimination of iberdomide. Therefore, it is important to evaluate the influence of HI on the PK of iberdomide.
The study results showed that lower M12 exposure was observed in moderate and severe HI subjects while no changes in the parent (iberdomide) PK. This is possibly because M12 is formed by CYP3A metabolism from iberdomide. Therefore, hepatic impairment (CYP3A decrease) lead to a decrease in the CYP3A-mediated M12 formation. However, based on the data from ADME study, M12 constitutes only 14% of total TRA. The observed 65% decreasing in M12 formation (severe HI compared to normal control) is equivalent to around 9% increase of iberdomide. This increase, comparing with the associated PK variabilities (24% to 44% based on Table 1), is thus unlikely to be detectable.
Notably, although the M12 PK is significantly reduced in moderate and severe HI subjects, it represents less than 1/5 of the iberdomide concentration in plasma (with a M12 to iberdomide ratio (AUC) of 17% to 20% in normal subjects and 7% in severe HI subjects). Hence, the decrease of M12 exposure from healthy subjects to severe HI only contributes to a 6% to 8% decrease of total iberdomide related exposure (iberdomide + M12).
Findings from the current study are in line with the results from an integrated popPK analysis of iberdomide,8 in which hepatic parameters, including hepatic impairment (ie, mild or moderate), total BILI (0.2 to 3.7 mg/dL), AST (6 to 84 U/L), ALP (21 to 300 U/L) and ALT (5 to 63 U/L), were evaluated on the PK of iberdomide and none of the covariates was found to be statistically significant. Consistently, PK parameters obtained herein were generally comparable with other iberdomide clinical studies in which PK data were available,14–16 suggesting that the current study was well-designed. In addition, unbound fraction was not determined in this study given that the plasma binding of iberdomide and M12 are moderate (78% and 67%). Based upon regulatory guidance,19 unbound fraction is recommended to be determined for drugs that are extensively bound to plasma protein (fraction unbound < 10%).
In summary, 1 mg single oral dose of iberdomide was generally well tolerated in this study. Iberdomide PK exposure was comparable between HI subjects and their respective matched normal controls. However, for M12 PK exposure, moderate and severe HI subjects had over 30% reduction as compared to matched normal controls. Given the relative limited proportion of M12 exposure as compared to iberdomide, the changes were not deemed to be clinically meaningful. In conclusion, the study shows that HI (mild, moderate and severe) is unlikely to impact iberdomide PK in a clinically relevant extent and therefore, dose adjustments are not needed for hepatically impaired subjects when administering iberdomide.
Data Sharing Statement
Data sharing of BMS may be found at https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html.
Acknowledgment
The authors acknowledge PPD, Inc. (Austin, TX, USA) who conducted the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
Bristol Myers Squibb funded and sponsored this work.
Disclosure
Y.C., Y.Y, A.Ga., Y.X., A.W., and Y.L. are employees and hold equity ownership in Bristol Myers Squibb. SZ is an employee of Aurinia Pharma and owns Bristol Myers Squibb stocks. A.Gh. was employed by Bristol Myers Squibb at the time of this manuscript. The authors report no other conflicts of interest in this work.
References
1. Werth V, Merrill J, Furie R, et al. OP0132 Effect of iberdomide on cutaneous manifestations in systemic lupus erythematosus: results of a 24-week, placebo-controlled, Phase 2 study. Ann Rheum Dis. 2021;80(Suppl 1):76–77. doi:10.1136/annrheumdis-2021-eular.2181
2. Thakurta A, Pierceall WE, Amatangelo MD, Flynt E, Agarwal A. Developing next generation immunomodulatory drugs and their combinations in multiple myeloma. Oncotarget. 2021;12(15):1555–1563. doi:10.18632/oncotarget.27973
3. van de Donk NW, Popat R, Larsen J, et al. First results of iberdomide (IBER; CC-220) in combination with dexamethasone (DEX) and daratumumab (DARA) or bortezomib (BORT) in patients with relapsed/refractory multiple myeloma (RRMM). Blood. 2020;136(Supplement 1):16–17. doi:10.1182/blood-2020-137743
4. Maples KT, Joseph NS, Harvey RD. Current developments in the combination therapy of relapsed/refractory multiple myeloma. Expert Rev Anticancer Ther. 2020;20(12):1021–1035. doi:10.1080/14737140.2020.1828071
5. Rivellese F, Manou-Stathopoulou S, Mauro D, et al. Effects of targeting the transcription factors Ikaros and Aiolos on B cell activation and differentiation in systemic lupus erythematosus. Lupus Sci Med. 2021;8(1):e000445. doi:10.1136/lupus-2020-000445
6. Bjorklund CC, Kang J, Amatangelo M, et al. Iberdomide (CC-220) is a potent cereblon E3 ligase modulator with antitumor and immunostimulatory activities in lenalidomide- and pomalidomide-resistant multiple myeloma cells with dysregulated CRBN. Leukemia. 2020;34(4):1197–1201. doi:10.1038/s41375-019-0620-8
7. Matyskiela ME, Zhang W, Man HW, et al. A cereblon modulator (CC-220) with improved degradation of Ikaros and Aiolos. J Med Chem. 2018;61(2):535–542. doi:10.1021/acs.jmedchem.6b01921
8. Cheng Y, Xue Y, Chen L, et al. Model-based analysis for the population pharmacokinetics of iberdomide and its major active metabolite in healthy subjects and patients with relapsed and refractory multiple myeloma. Br J Clin Pharmacol. 2022;2022:254.
9. Lonial S, Popat R, Hulin C, et al. Iberdomide plus dexamethasone in heavily pretreated late-line relapsed or refractory multiple myeloma (CC-220-MM-001): a multicentre, multicohort, open-label, phase 1/2 trial. Lancet Haematol. 2022;9:e822–e832.
10. van de Donk NW, Raab MS, Besemer B, et al. P-279: efficacy, safety, and pharmacokinetics of iberdomide plus dexamethasone in patients with relapsed/refractory multiple myeloma by renal function: a subgroup analysis of the CC-220-MM-001 trial. Clin Lymphoma Myeloma Leuk. 2022;22:S191–S192. doi:10.1016/S2152-2650(22)00609-7
11. Thieblemont C, Munoz J, Tucci A, et al. Iberdomide (CC-220) monotherapy or in combination with an anti-CD20 monoclonal antibody as effective therapy in patients with relapsed/refractory lymphoma: early results from a phase 1/2 study. Blood. 2022;140(Supplement 1):569–572. doi:10.1182/blood-2022-162559
12. Amatangelo M, Cheng Y, Pierceall W, et al. P-231: biomarker analysis to support dose optimization of iberdomide (IBER) as monotherapy and in combination with standard of care treatments for multiple myeloma from a phase 1/2 trial. Clin Lymphoma Myeloma Leuk. 2022;22:S162. doi:10.1016/S2152-2650(22)00561-4
13. Amatangelo M, Cheng Y, Pierceall W, et al. P865: biomarker analysis to support dose optimization of iberdomide as monotherapy and in combination with standard of care treatments for multiple myeloma from a phase 1/2 trial. Hemasphere. 2022;6(Suppl):758–759. doi:10.1097/01.HS9.0000846340.95760.ac
14. Ye Y, Gaudy A, Schafer P, et al. First-in-human, single- and multiple-ascending-dose studies in healthy subjects to assess pharmacokinetics, pharmacodynamics, and safety/tolerability of iberdomide, a novel cereblon E3 ligase modulator. Clin Pharmacol Drug Dev. 2021;10(5):471–485. doi:10.1002/cpdd.869
15. Gaudy A, Atsriku C, Ye Y, et al. Evaluation of iberdomide and cytochrome p450 drug-drug interaction potential in vitro and in a phase 1 study in healthy subjects. Eur J Clin Pharmacol. 2021;77(2):223–231. doi:10.1007/s00228-020-03004-w
16. Cheng Y, Xue Y, Chen L, et al. Model-based analysis for the population pharmacokinetics of iberdomide and its major active metabolite in healthy subjects and patients with relapsed and refractory multiple myeloma. Br J Clin Pharmacol. 2023;89(1):316–329. doi:10.1111/bcp.15498
17. Demirel S, Coskun F, Nak S, Ozyener F. Assessment of pulmonary functions with spirometry method in hepatic impairment patients. Ann Med Res. 2021;28(1):106–112.
18. Manns MP, Burra P, Sargent J, Horton R, Karlsen TH. The Lancet-EASL Commission on liver diseases in Europe: overcoming unmet needs, stigma, and inequities. Lancet. 2018;392(10148):621–622. doi:10.1016/S0140-6736(18)31734-3
19. FDA. Pharmacokinetics in Patients with Impaired Hepatic Function: Study Design, Data Analysis, and Impact on Dosing and Labeling. FDA Guidance. FDA; 2003.
20. Li Y, Wang X, Liu L, et al. An open-label, phase 1 study to assess the effects of hepatic impairment on pomalidomide pharmacokinetics. Clin Pharmacol Drug Dev. 2019;8(3):346–354. doi:10.1002/cpdd.470
21. EMA. Guideline on the Evaluation of the Pharmacokinetics of Medicinal Products in Patients with Impaired Hepatic Function. EMA; 2005.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dose Adjustment of Poly (ADP‑Ribose) Polymerase Inhibitors in Patients with Hepatic or Renal Impairment
Zhao D, Long X, Wang J
Drug Design, Development and Therapy 2022, 16:3947-3955
Published Date: 14 November 2022