Back to Journals » Drug Design, Development and Therapy » Volume 20
A Pharmacist-Driven Closed-Loop Stewardship Model of Meropenem: Impact on Stability and Efficacy in Neurosurgery Patients
Authors Li T ![]() , Chen X, Xu J
, Chen X, Xu J ![]() , Qian J
, Qian J ![]() , Deng P, Xue C, Yang L, Huang S, Zhang Q, Ma M, Yu Y, Tang L
, Deng P, Xue C, Yang L, Huang S, Zhang Q, Ma M, Yu Y, Tang L
Received 21 September 2025
Accepted for publication 25 January 2026
Published 2 February 2026 Volume 2026:20 569180
DOI https://doi.org/10.2147/DDDT.S569180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Tongtong Li,1,* Xianglong Chen,1,* Jinhui Xu,1,* Jinhong Qian,2 Peng Deng,2 Chunmeng Xue,3 Lijuan Yang,1 Shenjia Huang,1 Qian Zhang,1 Mian Ma,2 Yanxia Yu,1 Lian Tang1,3
1Department of Pharmacy, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, Jiangsu, People’s Republic of China; 2Department of Neurosurgery, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, Jiangsu, People’s Republic of China; 3Gusu School, Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lian Tang, Department of Pharmacy, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, No. 26 Daoqian Street, Gusu District, Suzhou, 215002, People’s Republic of China, Tel +86 0512 6236 2325, Email [email protected] Yanxia Yu, Department of Pharmacy, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, No. 26 Daoqian Street, Gusu District, Suzhou, 215002, People’s Republic of China, Tel +86 0512 6236 2325, Email [email protected]
Purpose: To evaluate the impact of a pharmacist-driven closed-loop stewardship model on meropenem stability and therapeutic efficacy in neurosurgical patients with hospital-acquired pneumonia (HAP).
Patients and Methods: An interrupted time series study enrolled neurosurgical patients treated with meropenem for HAP. The patients from October 2019 to December 2021 were retrospectively collected as the control group, whereas the patients were prospectively enrolled from January 2022 to March 2025 as the intervention group. The intervention featured optimized drug preparation, prioritized administration, rapid specimen processing, real-time therapeutic drug monitoring and dynamic dose adjustments. Steady-state trough concentrations (Cmin) and open-ring metabolite (ORM) levels in serum and cerebrospinal fluid (CSF), and clinical outcomes were analyzed.
Results: A total of 227 patients was included (control group: n = 102; intervention group: n = 125). The intervention group demonstrated a significantly higher median Cmin [3.75 (1.45, 8.64) mg/L vs 0.78 (0.25, 2.74) mg/L, P < 0.001] and lower subtherapeutic exposure rate (35.48% vs 70.59%, P < 0.0001) compared to control group. The ratio of ORM/Cmin in serum [0.83 (0.62, 1.24) vs 1.97 (1.42, 2.65), P < 0.0001] and CSF [1.21 (0.84, 1.90) vs 2.05 (1.27, 2.81), P < 0.05] were also lower in the intervention group, indicating mitigated degradation. There were no significant differences in clinical response rates (72.5% vs 61.3%, P = 0.157) or bacterial eradication rates (68.1% vs 59.4%, P = 0.160). However, the bacterial eradication rates improved for Gram-negative isolates with Minimum inhibitory concentration (MIC) ≤ 8 mg/L in the intervention group than the control group (84.4% vs 69.1%, P < 0.05).
Conclusion: The closed-loop stewardship model effectively improved meropenem target concentration attainment by systematically reducing drug loss through degradation and metabolism. This optimized exposure profile correlated with improved eradication rates of Gram-negative sensitive bacteria.
Keywords: meropenem, closed-loop management of precision medication, concentration, open-ring metabolite, hospital-acquired pneumonia, acute brain injury
Introduction
Hospital-acquired pneumonia (HAP) is a common and severe complication in patients with acute brain injury (ABI), affecting disease recovery and prognosis.1 Meropenem is the first-line therapeutic agent for severe HAP and central nervous system infections due to its potent antimicrobial activity against multidrug-resistant Gram-negative organisms. However, characteristic pathophysiological alterations in neurosurgery patients-including disrupted blood-brain barrier (BBB) integrity, cerebrospinal fluid (CSF) drainage, diabetes insipidus, osmotic diuresis for cerebral edema, and augmented renal clearance-collectively accelerate meropenem elimination. These pharmacokinetic changes result in subtherapeutic plasma concentrations and compromising antimicrobial efficacy while promoting resistance.2,3 Our previous research identified craniocerebral injury as a significant risk factor of meropenem underexposure.4 While many studies have reported on the BBB permeability of meropenem in patients with central nervous system infections, there is limited research on its permeability in patients with HAP complicating traumatic brain injury. Critically, for neurosurgery patients with ABI, the efficacy of meropenem is not solely dependent on plasma concentrations—as CSF concentration emerges as a pivotal determinant of therapeutic success. Furthermore, the BBB permeability of meropenem in neurosurgery patients with ABI may be different with central nervous system infections. Therefore, there is an urgent need to optimize the dosing regimen of meropenem for neurosurgery patients with HAP.
Furthermore, meropenem demonstrates limited stability in aqueous solutions, maintaining therapeutic integrity for only 3–4 hours at room temperature (20–25°C) when reconstituted in 0.9% sodium chloride or 5% dextrose.5,6 Higher pH and temperature could accelerate the degradation, at temperatures exceeding 25°C, it degrades by more than 10% within 3.5 hours.5–7 The core mechanism underlying meropenem degradation lies in the irreversible cleavage of its pharmacologically active β-lactam ring. Specifically, in aqueous environments, water molecules act as nucleophiles to attack the electrophilic carbonyl carbon of the β-lactam ring’s amide bond, leading to irreversible ring opening and conversion to its sole inactive metabolite, the open-ring metabolite (ORM) (Supplementary Figure 1).8 This degradation process exhibits concentration dependence: more than 15% of meropenem is converted to ORM when stored for 12 or 24 hours at 4°C.9 Meanwhile, meropenem degradation persists across biological matrices, with plasma samples demonstrating progressive decomposition even at −20°C, necessitating long-term storage at −80°C for analytical validity.10 Current stabilization strategies involve incorporating 3-(N-morpholino) propane sulfonic acid (MOPS) buffer systems during sample processing, which enhances short-term stability.11 Meropenem showed higher stability at −80°C, and addition of MOPS might increase the short-term and extracted samples stability. However, meropenem still has the problem of degradation in the stages of intravenous infusion preparation, transportation and clinical infusion, especially for continuous infusion.7
 |
Figure 1 A Pharmacist-driven Closed-loop Stewardship Model Flowchart of Meropenem. |
The combined challenges of meropenem underexposure and inherent drug instability necessitate meticulous quality control throughout the therapeutic chain. Suboptimal handling during drug dissolution, intravenous administration, biological sampling, specimen storage, or analytical processing can further exacerbate meropenem degradation, ultimately diminishing antimicrobial effectiveness. Given that pharmacotherapy for these patients extends beyond individual pharmacokinetic adjustments to require systematic management of the entire treatment process, the closed-loop management model—characterized by integrated multidisciplinary collaboration and informatics-driven monitoring, enabling dynamic therapeutic strategy adjustments that significantly reduce antimicrobial medication errors and infection risks. Therefore, this study implemented a pharmacist-driven closed-loop stewardship model of the whole meropenem medication in the neurosurgery department of Suzhou Municipal Hospital and analyzed the in-vivo and in-vitro stability and the clinical efficacy before and after the clinical pharmacist intervention to facilitate the advancement of personalized meropenem dosing strategies.
Materials and Methods
Study Design and Ethics
This prospective intervention study employed an interrupted time series (ITS) design to assess the pharmacist-driven closed-loop stewardship model, with its primary endpoints including: meropenem exposure, the ORM/Cmin ratio and therapeutic effectiveness.
The intervention protocol received ethical approval from the Ethics Committee of Suzhou Municipal Hospital (Ethics Approval No. K-2021-082-H01) and was prospectively registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2100053649, Registration Date: November 26, 2021). All study procedures complied with the Declaration of Helsinki principles, with written informed consent obtained from participants or legally authorized representatives prior to data collection and intervention implementation.
Study Population
Neurosurgery patients diagnosed with HAP and treated with meropenem for anti-infective therapy from October 2019 to March 2025 were consecutively enrolled. Inclusion criteria: (1) age ≥18 years; (2) diagnosis of HAP or severe pneumonia based on ATS/IDSA criteria;12 (3) neurosurgery patients contained of traumatic brain injury (TBI), sub arachnoid hemorrhage, post-neurosurgery, and intracerebral hemorrhage after tracheostomy; (4) targeted or empirical antimicrobial therapy was administered using meropenem (Sumitomo Dainippon Pharma Co., Ltd., Oita Plant, National Drug Approval No. J20140169, 0.5 g per vial) for anti-infective treatment; (5) Availability of measured steady-state Cmin and ORM concentrations of meropenem. Exclusion criteria: (1) meropenem duration ≤3 days; (2) incomplete medical records or laboratory data; (3) withdrawal of consent.
Study Groups and Data Collection
Control Group: A retrospective case-control cohort analysis was performed on neurosurgical patients receiving meropenem for HAP from October 2019 to December 2021. Data extraction followed STROBE guidelines for observational studies. Intervention Group: Following the implementation of a clinical pharmacist-driven closed-loop stewardship program, we prospectively enrolled neurosurgical patients receiving meropenem for anti-infective treatment at our hospital from January 2022 to March 2025.
From the hospital information system (HIS), we systematically collected six data dimensions: (1) patient demographics: gender, age, weight, height, diagnosis; (2) infection-related indicators: infection site, microbiological culture, drug sensitivity; (3) therapeutic parameters: course of treatment, dosage regimen, combination antimicrobial therapy; (4) administration data: time from meropenem dissolution to the start of intravenous infusion; infusion duration; time from the blood sampling to the laboratory reception; Sample pretreatment and storage conditions; time of concentration determination; time of concentration report issuance; (5) laboratory indicators: blood tests, hepatic and renal function tests, meropenem Cmin or ORM concentrations; (6) clinical outcomes: microbiological eradication, related adverse reactions, 28-day survival rate and length of hospital stay Dual data entry with cross-validation was implemented. Creatinine clearance (CrCL) was calculated using the Cockcroft-Gault equation, and the equation is defined as:13

Construction of the Closed-Loop Management Precision Medication of Meropenem
This study established a pharmacist-driven closed-loop stewardship model for meropenem precision dosing. Under the leadership and coordination of pharmacists, a dedicated multidisciplinary team was formed, comprising pharmacists from clinical pharmacy department, intravenous admixture services and therapeutic drug monitoring (TDM) laboratory, alongside nurses and clinicians. This pharmacist-driven model integrated eight critical processes into a seamless workflow spanning from drug dispensing to individualized dosage regimen optimization, achieving comprehensive and fine-grained management of meropenem therapy (Figure 1). The processes, strategically designed under pharmacist direction, targeted two primary objectives:
Minimizing in vitro degradation—through pharmacists’ direct leadership in (1) developing and implementing optimized drug preparation protocols and (2) establishing prioritized medication administration workflows; and optimizing pharmacokinetic exposure while modulating in vivo metabolism—via pharmacists’ core coordination and oversight of (3) standardized TDM sampling procedures, (4) expedited specimen handling protocols, (5) validation of analytical methodologies, (6) delivery of evidence-based clinical decision support, (7) continuous therapeutic monitoring, and (8) dynamic dose optimization strategies. The specific interventions designed, initiated, and supervised by pharmacists at each of the eight stages are detailed in Table 1, which summarizes key process enhancements post-implementation.
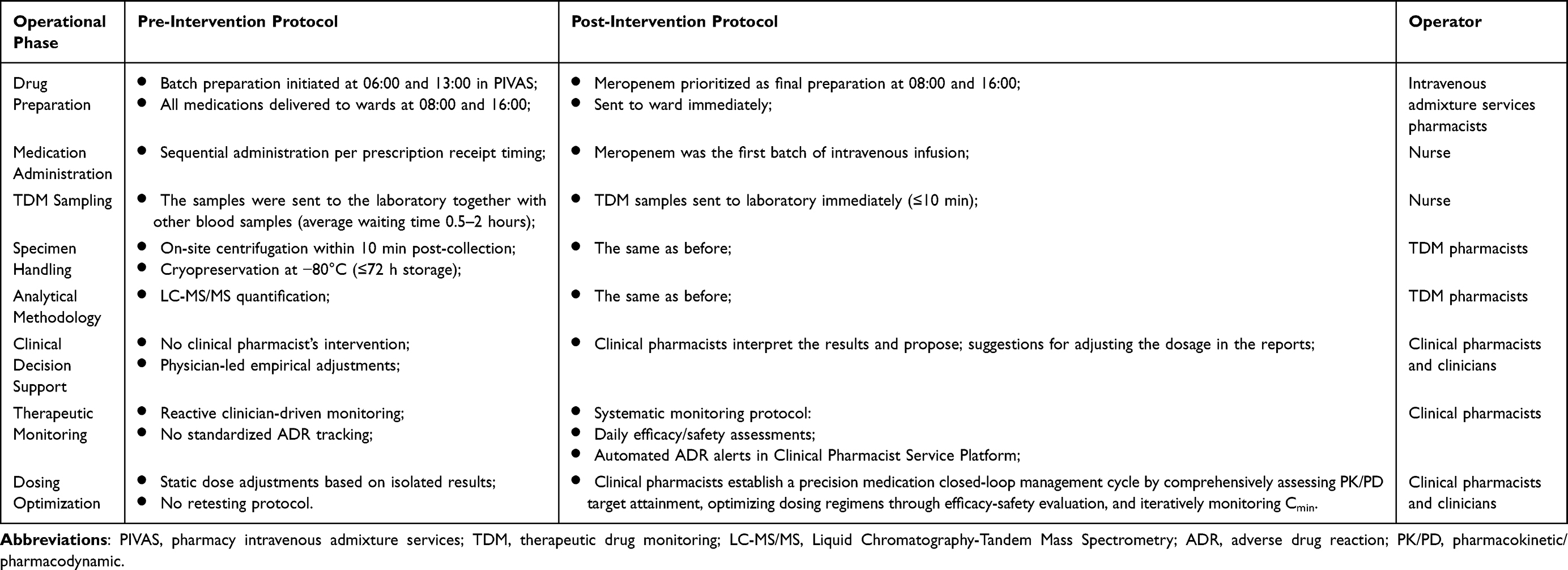 |
Table 1 Comparative Analysis of Meropenem Administration Protocols: Pre- vs Post- Implementation of Closed-Loop Precision Management |
Meropenem Dosing Regimen
The initial dosing regimen of meropenem was formulated based on the Sanford Guide to Antimicrobial Therapy (53rd Edition),5 ABX Guide (2nd Edition),14 and Manufacturer’s prescribing information. Dosage regimens were individualized based on the infection site, infection severity, and renal function stratification. Standard dosing ranged from 0.5 g q12h (mild infections) to 2 g q8h (CNS infections/septic shock), with adjustments based on Cmin, clinical efficacy, and safety.
Measurement of Meropenem Cmin and ORM Concentration
Steady-state Cmin and ORM samples were collected 30 minutes prior to the fifth meropenem dose administration. Venous blood (2 mL) sample was collected in a yellow-top vacuum tube (containing coagulant and separation gel), the CSF sample was collected in a sealed tube at the same time point of serum in CNS infections patients, centrifuged at 3000 rpm for 10 minutes, and the supernatant (0.5 mL) was stored in −80°C refrigerator for testing within 3 days. Among them, CSF sampling was performed opportunistically and was not mandatory for all patients; samples were collected only from patients with pre-existing clinical indications for lumbar puncture or external ventricular drainage (eg, intracranial pressure monitoring, suspected CNS infection) as part of standard neurosurgical care. No additional invasive procedures were conducted for research purposes.
For serum sample processing, a total volume of 25.0 μL of serum samples was combined with 100.0 μL internal standard solution, comprising a mixed solution containing meropenem-D6 and ORM-D6 at a concentration of 1.00 µg/mL, and vortexed thoroughly to ensure proper mixing. Centrifugation was followed for ten minutes at 13500 rpm, after which 50 μL of the supernatant was collected and diluted with 100 μL water before being vortexed again for uniform distribution. Subsequently, the prepared samples underwent LC-MS/MS analysis.
For CSF sample processing, a total volume of 25.0 μL of serum samples was combined with 100.0 μL internal standard solution, comprising a mixed solution containing meropenem-D6 and ORM-D6 at a concentration of 2.00 µg/mL, and vortexed thoroughly to ensure proper mixing. Centrifugation was followed for ten minutes at 13500 rpm, after which 50 μL of the supernatant was collected and diluted with 100 μL water before being vortexed again for uniform distribution. Subsequently, the prepared samples underwent LC-MS/MS analysis.
The serum and CSF concentrations of meropenem and its ORM were quantified using a validated LC-MS/MS method, comprehensive details regarding the analytical procedures are available in the Supplementary Material 1. The typical multiple reaction monitoring (MRM) chromatograms of meropenem, its ORM, and the internal standards (meropenem-D6 and ORM-D6) in human serum and CSF are presented in Supplementary Figure 2 and Supplementary Figure 3, respectively, illustrating the specificity and separation efficiency of the method. The method demonstrated a linear range of 0.1–100.0 μg/mL for both meropenem Cmin and its ORM in serum and CSF, with the corresponding standard curve equations provided in Supplementary Table 1. Additionally, intra- and inter-assay precision, stability, and reproducibility of the method were all within acceptable limits, and detailed validation results are summarized in Supplementary Material 1. The target range for steady-state Cmin was set at 2.0–16.0 mg/L (without MIC) or 100% fT > 1-8×MIC (with MIC).15,16
Efficacy and Safety Evaluation
Therapeutic outcomes were assessed in compliance with the Guidelines for Clinical Trials of Antimicrobial Drugs,17 the efficacy of anti-infective therapy was evaluated as follows: (1) Clinical efficacy: cure or failure. (2) Microbiological efficacy: eradication, presumed eradication, presumed non-eradication, or non-eradication. (3) Safety: adverse drug reactions (ADRs) were classified per WHO-UMC causality criteria: definite, probable, possible, possibly unrelated, unassessable, or unclassifiable. The first three categories were considered ADRs.18
Statistical Analysis
Analyses were conducted using SPSS 27.0 (IBM Corp.) and GraphPad Prism 9.4.1 (GraphPad Software) under a pre-specified α = 0.05 (two-tailed). To properly incorporate all concentration data, including beyond the limits of quantification which carry essential exposure information, a likelihood-based approach was employed as the gold standard method for data beyond quantification limits.19 Continuous variables with normal distribution were expressed as mean ± standard deviation (X ± s), and independent samples t-test was used for comparison between groups. Non-normally distributed data were expressed as median (Q25, Q75), and the Mann–Whitney U-test was used for comparison. Categorical data were described by frequency and percentage, and the chi-square test or Fisher’s exact test was used for comparison. P < 0.05 was considered statistically significant.
Results
Patient Characteristics
The study cohort comprised 227 neurosurgical patients determined meropenem concentrations, stratified into two groups: historical control cohort (n = 102) and prospective intervention cohort (n = 125). Comparative analysis revealed balanced baseline characteristics between groups, and no significant intergroup differences were observed across these variables, confirming cohort comparability. Comprehensive baseline data are presented in Table 2.
 |
Table 2 Characteristics of Patients in the Control Group and the Intervention Group |
Infection Site and Etiological Detection
Biological specimens for microbiological diagnosis were collected, with respiratory secretions (69.3%) constituting the primary source, followed by urinary tract (14.7%), bloodstream (9.0%), CSF (4.1%) and drainage fluid (2.9%) samples. The predominant Gram-negative pathogens isolated included Klebsiella pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa. Further analysis revealed Gram-positive bacterial detection rates of 29.2% in the control group versus 36.2% in the intervention group, with corresponding fungal isolation rates of 43.3% and 37.7%, respectively. Comparative analysis demonstrated comparable pathogen distributions between cohorts, with no significant intergroup differences in MIC values of meropenem, see Table 3 for detailed antimicrobial susceptibility profiles. However, 35.85% of Gram-negative isolates in the control group and 34.78% in the intervention group exhibited meropenem MIC values ≥16 mg/L.
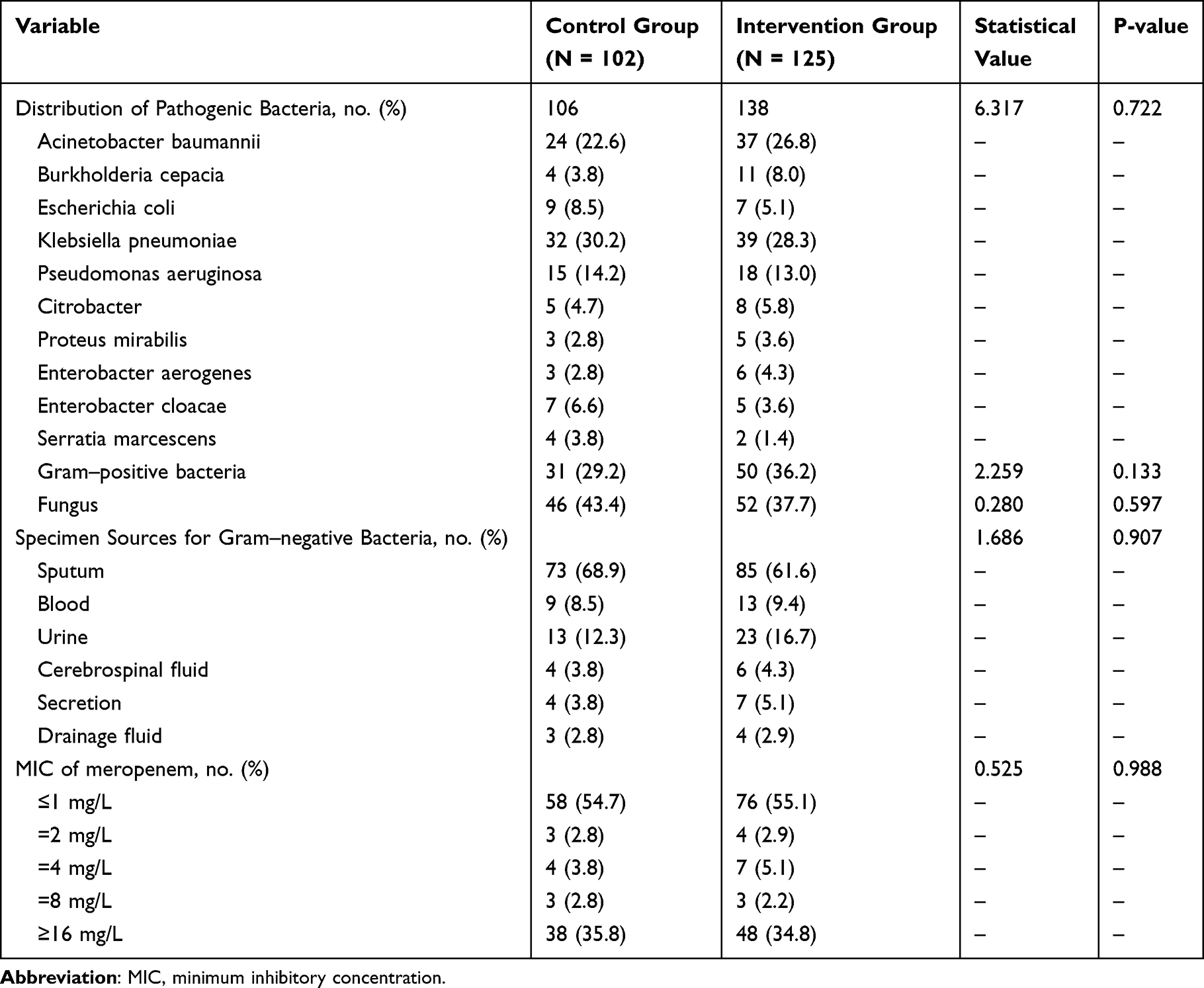 |
Table 3 Etiological Detection Distribution Results of Two Groups |
Distribution and Comparative Analysis of Meropenem Cmin and ORM Concentrations
A total of 495 valid quantified concentration points were included in the analysis, stratified by analyte (Cmin and ORM) and sample type (serum/CSF) across the two study groups. Specifically, for Cmin, 227 serum samples (Control: n = 102; Intervention: n = 125) and 63 CSF samples (Control: n = 20; Intervention: n = 43) were analyzed. For ORM, the analysis included 145 serum concentrations (Control: n = 58; Intervention: n = 87) and 61 CSF concentrations (Control: n = 19; Intervention: n = 42). ORM serum concentrations were measured only in some patients of control group (56.86%) and intervention group (69.60%) due to less volume of blood or the retrospective patients missed collecting blood samples or other patients’ subjective factors.
There were no statistically significant differences in the initial dosage and administration protocols of meropenem between the two groups (P > 0.05, Table 4). However, the Cmin exhibited a widely range, from 0.20 mg/L to 45.24 mg/L. The intervention group demonstrated significantly higher meropenem serum concentrations compared to the control group (Figure 2). Patients were stratified into three subcategories based on meropenem target attainment: subtherapeutic (Cmin< 2 mg/L), target exposure (Cmin at 2–16 mg/L), and supratherapeutic (Cmin> 16 mg/L). Notably, the control group exhibited a significantly higher proportion of subtherapeutic patients compared to the intervention group (70.59% vs 35.48%, P < 0.0001), as shown in Figure 3. Although the proportion of patients achieving the target exposure demonstrated no statistically significant difference between groups, the intervention group exhibited a trend toward higher attainment rates (50.81% vs 26.47%, P = 0.290).
 |
Table 4 Medication Information Evaluation of Two Groups of Patients |
 |
Figure 2 The comparison of meropenem Cmin and ORM concentration between the two groups. Note: ***Bonferroni-adjusted P < 0.001. |
 |
Figure 3 Target attainment of meropenem Cmin in the two groups. Notes: Therapeutic exposure is defined as Cmin of 2–16 mg/L for meropenem. Supratherapeutic exposure is defined as Cmin above the desired range, whereas subtherapeutic exposure is defined as Cmin below the desired range. ****Bonferroni-adjusted P < 0.0001. |
Meropenem was degraded to varying degrees in both groups of patients. The distribution of ORM concentration levels was shown in Figure 2. The ratio of ORM to Cmin in the control group was significantly higher than that in the intervention group, had statistically significant [serum: 1.97 (1,42, 2.65) vs 0.83 (0.62, 1.24), P < 0.0001; CSF: 2.05 (1.27, 2.81) vs 1.21 (0.84, 1.90), P < 0.05], as shown in Figure 4. The correlation between the serum Cmin of meropenem and ORM concentrations in the intervention group was lower than that in the control group (0.6603 vs 0.7314, P < 0.0001), as shown in Figure 5. There were 39 patients and 52 patients of intracranial infection in the control group and intervention groups, respectively. Among them, the CSF meropenem concentrations and ORM concentrations were simultaneously determined at the same time of serum samples in 19 and 43 patients, respectively. Similar with the results in serum, the Cmin and ORM concentrations of meropenem in both groups had pretty good correlations (Figure 6), and the correlation between the Cmin of meropenem and ORM concentrations in the intervention group was significantly lower than that of the control group (0.9294 and 0.6657, P < 0.0001).
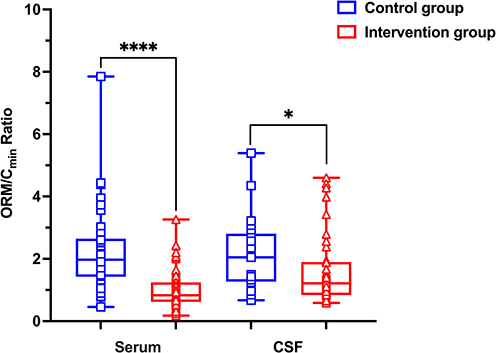 |
Figure 4 Distribution and comparison of ORM/Cmin Ratios in Serum and CSF between the two groups. Notes: ****Bonferroni-adjusted P < 0.0001 [serum: 1.97 (1,42, 2.65) vs 0.83 (0.62, 1.24)]; *Bonferroni-adjusted P < 0.05 [CSF: 2.05 (1.27, 2.81) vs 1.21 (0.84, 1.90)]. |
 |
Figure 5 The correlation analysis of (A) control group and (B) Intervention group between meropenem Cmin and its ORM concentration in the serum. Notes: The correlation coefficients (R2) were 0.7314 and 0.6603 for the meropenem Cmin in the two groups, respectively (P < 0.0001 vs P < 0.0001). |
 |
Figure 6 The correlation analysis of (A) control group and (B) Intervention group between meropenem Cmin and its ORM concentration in the cerebrospinal fluid. Notes: The correlation coefficients (R2) were 0.9294 and 0.6657 for the meropenem Cmin in the two groups, respectively (P < 0.0001 vs P < 0.0001). |
Clinical Efficacy and Safety Evaluation
In the control group, physician empirically adjusted the dosage and remeasured Cmin in 20 patients, only 7 patients had Cmin in the target range. However, 33 patients adjusted the dosage according to the suggestions of clinical pharmacists (increase or decrease the dosage and/or prolong the infusion time) in the intervention group, the results indicated that the rate of Cmin in the target range was significantly higher than that of the control group (66.7% vs 35.0%, P = 0.025).
There were no statistically significant differences between the control and intervention groups in the clinical efficacy rates (61.3% vs 72.5%, P = 0.157) or bacterial eradication rates (59.4% vs 68.1%, P = 0.160). Notably, subgroup analysis considering the restricted antibacterial activity of meropenem against carbapenem-resistant Gram-negative bacteria revealed that for patients infected with Gram-negative pathogens demonstrating meropenem MIC ≤ 8 mg/L, the intervention group achieved significantly superior pathogen clearance rates (84.4% vs 69.1%, P = 0.022). Laboratory analyses revealed statistically significant between-group differences in key inflammatory and hematologic parameters following meropenem therapy: haemoglobin (P = 0.034), eosinophils count (P = 0.016), CRP (P = 0.037), and PCT (P = 0.048). There was no statistically significant difference in the incidence of ADR between the two groups (P = 0.581). Additionally, although the intervention group exhibited lower 28-day hospital mortality compared to the control group (16.3% vs 21.0%), this difference did not reach statistical significance (P = 0.471). See Tables 4 and 5 for details.
 |
Table 5 Clinical Efficacy Evaluation of Two Groups of Patients |
Discussion
This prospective intervention study implemented a clinical pharmacist-driven closed-loop stewardship model for meropenem precise medication in neurosurgery patients. To the best of our knowledge, this is the first study establishing a clinical pharmacist-driven closed-loop meropenem stewardship program. Compared to traditional empirical dosing, this research represents the first deep integration of TDM technology with the closed-loop management concept. Through multidisciplinary collaboration led by clinical pharmacists, it facilitates a paradigm shift from empirical administration to a dynamic precision therapy model characterized by “monitoring-analysis-intervention-remonitoring”, providing a replicable paradigm for individualized antimicrobial therapy in neurosurgical critically ill patients. More importantly, our analysis of serum and CSF concentrations of meropenem Cmin and ORM demonstrated that this stewardship program effectively reduced meropenem degradation while simultaneously increasing systemic meropenem concentrations, thereby improving anti-infective therapeutic outcomes.
As a quintessential time-dependent antimicrobial agent, meropenem exerts bactericidal effects predominantly through persistent exposure to the parent compound rather than its metabolites.9 Extensive evidence documents its limited stability across various solvents and plasma, with rapid degradation and oxidative processes necessitating immediate processing or refrigeration/cryopreservation of blood specimens post-collection.5–7,9,10 Due to the massive dehydration and diuresis, coupled with the inherent instability of meropenem, these factors collectively decrease the meropenem steady-state trough concentration and compromise its anti-infective efficacy. Therefore, studies on patients with intracranial infections have reported that increasing the dosage of meropenem, prolonging the infusion time, or combining intrathecal administration are recommended strategies to increase plasma concentrations and improve anti-infective efficacy.5,20–24
Due to the presence of blood-brain barrier and hemodynamic changes in patients with central nervous system infection, meropenem has been recommended as a higher dosage of 2 g q8h or as a continuous infusion of 6 g/day.20,21 In refractory patients with poor efficacy, intrathecal injection of meropenem and vancomycin may even be required.22–24 Our preliminary investigations demonstrate that craniocerebral injury significantly accelerates meropenem clearance, resulting in a high incidence of subtherapeutic steady-state trough concentrations in this population, which may compromise clinical therapeutic efficacy.4 Notably, more than 60% of control group patients exhibited initial trough concentrations below the target ranges. Post-implementation of closed-loop meropenem management, the rate of suboptimal exposure decreased to 32.52%. Nevertheless, approximately 10% of patients failed to achieve therapeutic targets and showed poor therapeutic effect, even with maximal dosing (6g/d) and extended infusions, necessitating intrathecal administration.
Emerging evidence indicates that TDM and model-informed precision dosing (MIPD) can optimize meropenem concentration attainment and clinical outcomes.25,26 So far, this is the first study implemented the closed-loop intervention which focus on reducing the degradation and metabolism of meropenem. The closed-loop management of precise medication significantly improved meropenem exposure distribution and target attainment rates. Elevated ORM concentrations in control group reflected greater meropenem degradation and metabolism, with substantial interindividual variability, resulting in a weaker correlation between ORM concentrations and Cmin. The observed decrease in the ORM/Cmin ratio in the intervention group is likely attributable to the combined result of mitigating in vitro degradation through streamlined drug preparation and prioritized administration, as well as controlling in vivo metabolism via TDM-guided precision dosing. The serum ORM/Cmin ratio in the intervention group was consistent with the literature values (median 69.1%, range 19.7–186.7%) derived from 35-sample analyses.9 This study further demonstrated a significant positive correlation between ORM concentrations and Cmin. Notably, implementation of closed-loop management intervention attenuated this correlation coefficient, while simultaneously resulting in significantly higher Cmin in the intervention group compared to controls. This paradoxical phenomenon suggests that the closed-loop management system may enhance meropenem’s penetration capacity across physiological barriers (eg, blood-brain barrier [BBB]). However, given the substantial interindividual variability in BBB permeability-modulated by factors including P-glycoprotein expression levels and inflammatory status-the precise mechanistic underpinnings warrant further elucidation through large-scale, multicenter prospective studies.
While the closed-loop stewardship model did not yield statistically significant improvements in conventional clinical efficacy endpoints—likely due to the carbapenem- resistant Gram-negative bacteria (CR-GNB) in our cohort, which are intrinsically less susceptible to meropenem. First, in the subgroup analysis confined to infections caused by meropenem-susceptible GNB (MIC ≤ 8 mg/L), the intervention group demonstrated a significantly higher bacterial clearance rate (P < 0.05), confirming the program’s pharmacodynamically effectiveness. Furthermore, the intervention group exhibited accelerated normalization of infection-related inflammatory biomarkers (eg, CRP, PCT). Collectively, these findings position the closed-loop model not merely as a dosing optimization tool, but as a systems-based intervention that transitions meropenem therapy from empirical administration to a metric-driven, precision care paradigm.
Though ORM lacks intrinsic antimicrobial activity, simultaneous quantification of meropenem and ORM is of clinical interest: elevated ORM proportions may indicate (extended time interval between dissolvation of the compound and administration), and from pre-analytical issues (extended time interval between sampling and reception in the laboratory for centrifugation and freezing until analysis), enzymatic degradation by resistant pathogens, or enhanced non-renal clearance. Our prospective intervention confirms that controlling the degradation of meropenem at all stages of clinical application can effectively increase the Cmin of meropenem, thereby enhancing the clearance rate of Gram-negative sensitive bacteria. The closed-loop precision medication management for meropenem may significantly reduce the concentration variability, attenuating pharmacokinetic heterogeneity and facilitating personalized dosing optimization in clinical practice.
There are several limitations in this study. First, it was not a randomised controlled intervention study, the non-randomized design with retrospective controls introduces potential bias from unmeasured confounders and outcome assessment variability, including temporal changes in antimicrobial use policies, evolving medical technologies, and variations in clinical practice patterns. Second, our study analyzed the effect of clinical pharmacists’ intervention on optimizing the meropenem dosage regimen and all stages of clinical application; however, several clinical factors affected the efficacy, including infection severity, and the presence of co-morbidities. All these factors might have caused deviations in the results. Finally, the single-center design and limited sample size may restrict precise estimation of intervention effects, particularly for CSF concentrations, and precluded meaningful subgroup analyses based on clinically relevant variables such as intracranial infection status or surgery type, etc. Future larger-scale, multicenter studies are warranted to comprehensively verify the intervention effect of management model on the efficacy, safety and economic benefits of meropenem. Notwithstanding these constraints, this intervention study provides clinically meaningful insights for advancing precision antimicrobial management in neurosurgical populations.
Conclusion
Neurosurgery patients treated with meropenem exhibited a higher risk of having trough concentrations below the target range. This study innovatively developed a precision closed-loop management system for meropenem administration, establishing a comprehensive quality control framework through optimized integration of the whole operational phases. The intervention systematically decreased the degradation of meropenem, while concurrently elevating meropenem Cmin levels. This optimized exposure profile correlated with improved eradication rates of Gram-negative sensitive bacteria, confirming the program’s capacity to bridge pharmacological targets with clinical outcomes.
Data Sharing Statement
Deidentified individual participant data will be provided. The datasets generated and/or analyzed during the current study are available from the corresponding author Lian Tang ([email protected]) upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the Affiliated Suzhou Hospital of Nanjing Medical University (Ethics Approval No. K-2021-082-H01). Written informed consent was obtained from patients or substitute decision makers unless the requirement for informed consent was waived, according to local standards and legislation. A formal data creation and statistical analysis plan was approved for secondary use of the data.
Acknowledgments
The authors thank the patients and the nurse for performing meropenem administration and blood sample collection. The authors also thank all the clinicians and nurses for their assistance in carrying out this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Jiangsu Pharmaceutical Association Hospital Pharmacy Research Project (No. H202109; No. H202334); Jiangsu Research Hospital Association for Precision Medication (No. JY202203); Gusu Talent Program (No. GSWS2022069); Clinical Research Fund of Nanjing Medical University (No. 2024KF0237; No. 2024KF0256); China Medical and Health Development Foundation (No. 202427). Suzhou Pharmaceutical Association Hospital Pharmacy Research Project (No. Syhky202313; No. Syhky202312).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li S, Feng Q, Wang J, et al. A machine learning model based on CT imaging metrics and clinical features to predict the risk of hospital-acquired pneumonia after traumatic brain injury. Infect Drug Resist. 2024;17:3863–16. doi:10.2147/IDR.S473825
2. Lu C, Zhang Y, Chen M, et al. Population pharmacokinetics and dosing regimen optimization of meropenem in cerebrospinal fluid and plasma in patients with meningitis after neurosurgery. Antimicrob Agents Chemother. 2016;60(11):6619–6625. doi:10.1128/AAC.00997-16
3. Kumta N, Heffernan AJ, Cotta MO, et al. Plasma and cerebrospinal fluid population pharmacokinetics of meropenem in neurocritical care patients: a prospective two-center study. Antimicrob Agents Chemother. 2022;66(8):e0014222. doi:10.1128/aac.00142-22
4. Lu S, Fang C, Guangxian L, et al. Risk factors of substandard drug blood concentration of meropenem in patients with hospital-acquired pneumonia. China Pharm. 2022;33(19):2388–2392.
5. David N. Gilbert, Andrew T. Pavia, David O. Freedman, Douglas Black, Brian S. Schwartz, Kami Kim. The Sanford Guide to Antimicrobial Therapy 2023, 5th, Fifth, 5e Edn. Antimicrobial Therapy, Inc.; 2023.
6. Viaene E, Chanteux H, Servais H, Mingeot-Leclercq MP, Tulkens PM. Comparative stability studies of antipseudomonal beta-lactams for potential administration through portable elastomeric pumps (home therapy for cystic fibrosis patients) and motor-operated syringes (intensive care units). Antimicrob Agents Chemother. 2002;46(8):2327–2332. doi:10.1128/AAC.46.8.2327-2332.2002
7. Jamieson C, Allwood MC, Stonkute D, Wallace A, Wilkinson AS, Hills T. Investigation of meropenem stability after reconstitution: the influence of buffering and challenges to meet the NHS Yellow Cover Document compliance for continuous infusions in an outpatient setting. Eur J Hosp Pharm. 2020;27(e1):e53–e57. doi:10.1136/ejhpharm-2018-001699
8. Liebchen U, Rakete S, Vogeser M, et al. The role of non-enzymatic degradation of meropenem-insights from the bottle to the body. Antibiotics. 2021;10(6):715.
9. Rakete S, Schuster C, Paal M, Vogeser M. An isotope-dilution LC-MS/MS method for the simultaneous quantification of meropenem and its open-ring metabolite in serum. J Pharm Biomed Anal. 2021;197:113944. doi:10.1016/j.jpba.2021.113944
10. Gijsen M, Filtjens B, Annaert P, et al. Meropenem Stability in Human Plasma at −20 °C: detailed Assessment of Degradation. Antibiotics. 2021;10(4):449.
11. Liu T, Chen L, Yu P, Li Q, Lou J. Development and validation of a strong cation exchange chromatographic column coupled with high-performance liquid chromatography method for meropenem and evaluation of its stability in human plasma: application to the therapeutic drug monitoring. J Chromatogr Sci. 2023;61(7):656–664. doi:10.1093/chromsci/bmac086
12. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
13. Winter MA, Guhr KN, Berg GM. Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. Pharmacotherapy. 2012;32(7):604–612. doi:10.1002/j.1875-9114.2012.01098.x
14. John G. A. Bartlett, Paul G. Auwaerter, Paul A. Pham. The Johns Hopkins ABX Guide: Diagnosis & Treatment of Infectious Diseases 2010, 2nd, Second.
15. Abdul-Aziz MH, Alffenaar JC, Bassetti M, et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: a position paper(). Intensive Care Med. 2020;46(6):1127–1153. doi:10.1007/s00134-020-06050-1
16. Guilhaumou R, Benaboud S, Bennis Y, et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation-SFAR). Crit Care. 2019;23(1):104. doi:10.1186/s13054-019-2378-9
17. Drugs WGoGfCToAb. Guidance for clinical trials of anti-bacterial drugs. Chin J Clin Pharmacol. 2014;30(09):844–856.
18. Shukla AK, Jhaj R, Misra S, Ahmed SN, Nanda M, Chaudhary D. Agreement between WHO-UMC causality scale and the Naranjo algorithm for causality assessment of adverse drug reactions. J Family Med Prim Care. 2021;10(9):3303–3308. doi:10.4103/jfmpc.jfmpc_831_21
19. Wijk M, Wasmann RE, Jacobson KR, Svensson EM, Denti P. A pragmatic approach to handling censored data below the lower limit of quantification in pharmacokinetic modeling. CPT Pharmacometrics Syst Pharmacol. 2025;14(6):1042–1049. doi:10.1002/psp4.70015
20. Blassmann U, Roehr AC, Frey OR, et al. Cerebrospinal fluid penetration of meropenem in neurocritical care patients with proven or suspected ventriculitis: a prospective observational study. Crit Care. 2016;20(1):343. doi:10.1186/s13054-016-1523-y
21. Schneider F, Gessner A, El-Najjar N. Efficacy of vancomycin and meropenem in central nervous system infections in children and adults: current update. Antibiotics. 2022;11(2). doi:10.3390/antibiotics11020173
22. Zhang Q, Chen H, Zhu C, et al. Efficacy and safety of intrathecal meropenem and vancomycin in the treatment of postoperative intracranial infection in patients with severe traumatic brain injury. Exp Ther Med. 2019;17(6):4605–4609. doi:10.3892/etm.2019.7503
23. Li X, Wang X, Wu Y, et al. Plasma and cerebrospinal fluid population pharmacokinetic modeling and simulation of meropenem after intravenous and intrathecal administration in postoperative neurosurgical patients. Diagn Microbiol Infect Dis. 2019;93(4):386–392. doi:10.1016/j.diagmicrobio.2018.08.003
24. Chinese Medical Doctor Association NPB, Neurocritical Care Expert Committee; Beijing Medical Association, Neurosurgery Branch, Neurocritical Care Section. Chinese expert consensus on diagnosis and treatment of central nervous system infections in neurosurgery (2021 Edition). Chin Neurosurg J. 2021;37(1):1.
25. Chiriac U, Richter D, Frey OR, et al. Software- and TDM-guided dosing of meropenem promises high rates of target attainment in critically ill patients. Antibiotics. 2023;12(7). doi:10.3390/antibiotics12071112
26. Steffens NA, Zimmermann ES, Nichelle SM, Brucker N. Meropenem use and therapeutic drug monitoring in clinical practice: a literature review. J Clin Pharm Ther. 2021;46(3):610–621. doi:10.1111/jcpt.13369
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.