Back to Journals » Infection and Drug Resistance » Volume 15
A Peptidomic Approach to Identify Novel Antigen Biomarkers for the Diagnosis of Tuberculosis
Authors Chen H, Li S ![]() , Zhao W, Deng J, Yan Z, Zhang T, Wen SA, Guo H, Li L, Yuan J, Zhang H, Ma L
, Zhao W, Deng J, Yan Z, Zhang T, Wen SA, Guo H, Li L, Yuan J, Zhang H, Ma L ![]() , Zheng J, Gao M, Pang Y
, Zheng J, Gao M, Pang Y ![]()
Received 13 May 2022
Accepted for publication 1 August 2022
Published 18 August 2022 Volume 2022:15 Pages 4617—4626
DOI https://doi.org/10.2147/IDR.S373652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hongmei Chen,1,* Shanshan Li,2,* Weijie Zhao,3,* Jiaheng Deng,4,* Zhuohong Yan,5 Tingting Zhang,2 Shu’ an Wen,2 Haiping Guo,2 Lei Li,6 Jianfeng Yuan,6 Hongtao Zhang,5 Liping Ma,1 Jianhua Zheng,4,* Mengqiu Gao,1 Yu Pang2
1Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 2Department of Bacteriology and Immunology, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 3Clinical Trial Agency Office, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 4Key Laboratory of Systems Biology of Pathogens, Institute of Pathogen Biology, and Center for Tuberculosis Research, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 5Department of Central Laboratory, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 6Electral Safety Research & Development Center, Beijing Normal University, Zhuhai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Pang, Department of Bacteriology and Immunology, Beijing Chest Hospital, Capital Medical University/ Beijing Tuberculosis & Thoracic Tumor Research Institute, No. 9, Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel +86 10 8950 9359, Email [email protected] Mengqiu Gao, Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University/ Beijing Tuberculosis & Thoracic Tumor Research Institute, No. 9, Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel +86 10 8950 9302, Email [email protected]
Background: Here, we conducted a peptidomic study in murine model to identify novel antigen biomarkers for the diagnosis of tuberculosis (TB) with improved performance.
Methods: Four recombinant proteins, including Mycobacterium tuberculosis protein 32 (MPT32), Mycobacterium tuberculosis protein 64 (MPT64), culture filtrate protein 10 (CFP10), and phosphate ABC transporter substrate-binding lipoprotein (PstS1) were expressed and intravenously injected into BALB/c mice. The serum were analyzed by liquid chromatography-tandem mass spectrometry (LC-MS/MS). The concentrations of candidate peptides in serum of suspected TB patients were determined using competitive enzyme-linked immunosorbent assay.
Results: A total of 65 peptides from 4 MTB precursor recombinant proteins were identified in mouse serum by LC-MS/MS, of which 5 peptides were selected as candidates for serological analysis. The concentrations of peptides MPT64-2, CFP10-2 and PstS1-2 in TB patients were significantly higher than those in non-TB patients. MPT64-2 exhibited the most promising sensitivity (81.4%), followed by PstS1-2 and CFP10-2. In addition, PstS1-2 had the highest specificity (93.3%), followed by CFP10-2 and MPT64-2. According to the area under the curve (AUC), MPT64-2 (AUC = 0.863), PstS1-2 (AUC = 0.812) and CFP10-2 (AUC = 0.809) exhibited better diagnostic validity.
Conclusion: We develop an effective approach to identify new antigen biomarkers via LC-MS/MS-based peptidomics. Multiple peptides exhibit promising efficacy in diagnosis of active TB patients.
Keywords: tuberculosis, peptidomics, enzyme-linked immunosorbent assay, Mycobacterium tuberculosis protein 64, diagnostics
Introduction
Tuberculosis (TB) which is caused by Mycobacterium tuberculosis (MTB) complex with 9.9 million incidence cases and 1.30 million deaths recorded worldwide, remains one of the most serious public health concerns.1 It is important to develop rapid and accurate diagnosis of active TB and initiate of effective treatment in order to prevent onward transmission of the disease.2,3 Whereas many people with TB symptoms do not have access to adequate initial diagnosis.1 According to World Health Organization (WHO) reports, nearly 30% of incident cases remained undiagnosed in 2019,3 highlighting that TB case detection continues to be challenging in clinical practice. Therefore, the major advancements in TB diagnostics will be required to commit WHO END TB strategy by 2035.
The conventional diagnosis of TB relies on detection of tubercle bacilli in clinical specimens, including smear microscopy for acid-fast bacilli and mycobacterial culture.4 Smear microscopy is a rapid and simple tool for diagnosing TB cases, and the disadvantage is that the sensitivity is low and it is impossible to distinguish MTB from nontuberculous mycobacteria.5 Mycobacterial culture is considered the “gold standard” for diagnosing TB and it is more analytically sensitive than smear microscopy. However, it takes 8 weeks to yield culture results due to the slow growth rate of MTB.2 The long turnaround time in laboratory medicine hence can worsen the quality of TB patient care. Several molecular diagnostics have been developed to assist the diagnosis of pulmonary and extrapulmonary TB, including GeneXpert MTB/RIF assay.6,7 Although the speed of diagnosis and clinical sensitivity of multiple specimen types have been improved,8,9 these trials have low clinical sensitivity to cases of paucibacillary TB. Another obvious limitation of molecular diagnostics is that they could not distinguish between live and dead tubercle bacilli,2 which should not be applied to monitor response to anti-TB treatment. Hence, new rapid diagnostic methods with improved performance are urgently required to promote the rapid identification of pulmonary and extrapulmonary TB.
To address the identified shortcomings of current diagnostics, the WHO gave priority to developing a non-sputum-based biomarker test in 2014.10 A commercial assay is employed to detect of urine mycobacterial lipoarabinomannan (LAM) antigen for diagnostics of pulmonary TB.11,12 Owing to its poor diagnostic accuracy in HIV-naïve populations, this assay was conditionally endorsed in HIV-positive patients with a low CD4 count13. Recently, Chang Liu et al identified Mtb-specific peptide fragments in serum and develop a NanoDisk-MS method to diagnosis active TB with high sensitivity and specificity.14 NanoDisk-MS is a blood-based biomarker detection method and holds promise for the diagnostics of pulmonary TB in the primary evaluation.14,15 By targeting 10-kDa MTB-derived culture filtrate protein 10 (CFP-10) and 6-kDa early secreted antigenic target (ESAT-6) in serum samples, the method could accurately distinguish between active and non-TB cases with an overall sensitivity of 88% and a specificity of 96%.14 The need for sophisticated pre-processing and matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS) instrument has become a major constraint to use NanoDisk-MS as a point-of-care test in many resource-limited settings. Nevertheless, these novel assays highlight the potential use of MTB specific peptides as TB biomarkers towards the WHO’s non-sputum TB diagnostic assay.
MTB robustly secretes multiple proteins either to the extracellular environment or directly into the host cell that are required for growth during infection.16,17 For example, CFP10 are actively secreted and can be detected early after MTB infection, implying that its presence in serum can be used to diagnose active Mtb infection.18,19 MTB protein 64 (MPT64) is a 24-kDa important mycobacterial secreted protein. Many studies showed that MPT64 exhibits good diagnostic efficiency for MTB.20,21 Phosphate ABC transporter substrate-binding lipoprotein (PstS1) is a member of ABC transporters family and can be found intracellularly and extracellular. Alcaide et al developed a Multiplex Real-Time PCR assay for the quantitative detection of whiB3 and PstS1 and the results revealed high sensitivity and specificity especially for diagnosis of smear negative pulmonary TB.22 MTB protein 32 (MPT32) is a well- characterized secreted Mtb protein and can strongly induce the immunoreactivity. It may be a useful candidate in the development of vaccines and diagnostics.23 These proteins comprise fundamental antigen biomarkers for novel diagnostic assays. When entering into the host niche, these exogenous proteins are naturally processed by antigen-presenting cells.17 Considering that this spontaneous procedure is catalyzed by enzyme cocktails,24 the specific cleavage site recognized by human protease will lead to the presence of predominant peptides circulating in blood throughout the course of TB disease, and these predominant peptides could be recognized as biomarkers for early diagnosis of TB patients. To address this question, four major secreted proteins during MTB replication, CFP10, MPT64, MPT32, and PstS1 were recombinantly expressed and analyzed for degraded peptidomic in serum of murine model to identify novel antigen biomarkers for the diagnosis of TB. Then, the diagnostic performance of these peptides was evaluated in a cohort of pulmonary TB patients.
Materials and Methods
Recombinant Protein Expression
The workflow of this study is depicted in Figure 1. The coding sequences of 4 recombinant proteins, including CFP10, MPT32, MPT64, and PstS1, were synthesized by Sangon Biothech (Shanghai, China) with 6×His tag incorporation, and were cloned into pET-28b vectors (Novagen, CA, USA) as previously described.25 The recombinant proteins were expressed using Escherichia coli Rosetta (DE3) cells. After purification with High Affinity Ni-NTA resin (Qiagen, Valencia, CA, USA), the protein concentrations were examined using a non-interference protein assay kit (Sangon Biotech, Shanghai, China). Four purified recombinant proteins were assessed by SDS-PAGE with >95% purity and lyophilized and stored at −80°C refrigerator. Prior to animal experiments, the proteins were dissolved in normal saline at 0.25 mg/mL.
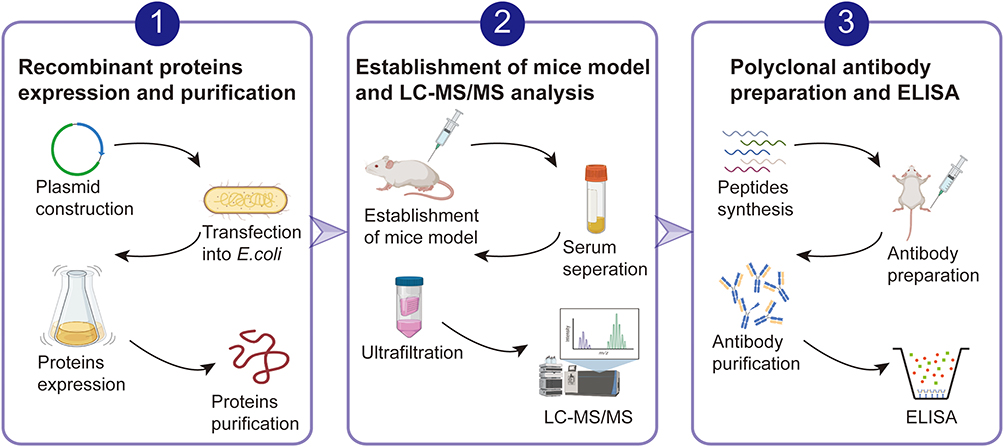 |
Figure 1 A schematic of the experimental design. First, recombinant MTB secreted proteins were expressed and purified. Then those proteins were intravenously injected in the tail vein of BALB/c mice and serum was separated and processed for LC-MS/MS analysis. Based on the frequency appeared in the results of LC-MS/MS and antigenicity analysis, 5 peptides from MPT64, CFP10, PstS1 and MPT32 were selected for serological analysis. Directed competitive ELISA were used for detection of those 5 peptides degraded from MTB secreted proteins in serum. ROC with 95% confidence intervals (CI) were used to analyze the diagnostic validity. |
Animal
Twelve BALB/c male mice aged 6 weeks (19–21 g) were ordered from Beijing Vital River Laboratory Animal Technology Co. Ltd (Beijing, China). The animals were housed in four groups under a temperature-controlled animal room (22–25°C) with a 12-hour light/12-hour dark cycle for at least five days before experiments. Mice were randomly assigned to each experimental group. Two hundred microlitre of protein solutions (50 μg) in normal saline were injected into the mouse caudal vein, whereas 0.2 mL of normal saline were used as control. The mice were euthanatized 24 h after injection, and mouse peripheral blood was collected from the inferior vena cava. After centrifugation at 2000 × g for 10 min, the serum was harvested and stored in a −80°C freezer for further peptidomic study. The animal study was reviewed to compliance with Guidelines for the ethical review of laboratory animal welfare of People’s Republic of China National Standard (GB/T 35892-2018) and approved by the Experimental Animal Committee of Beijing Chest Hospital affiliated to Capital Medical University (2020-022).
LC-MS/MS Analysis and Data Processing
The serum samples were firstly processed with ProteoExtract Albumin/IgG Removal Kit (Merck, Germany) to remove high abundant albumin and immunolgobulin G as the manufacturer’s instructions. Then the serum pools were ultrafiltered through Millipore 10 KD filters (Merck Millipore, Germany). The peptides were reduced using 5 mM dithiothreitol at 37°C for 45 min and alkylated using 10 mM iodoacetamide at room temperature keep away from light for 30 min. All the peptide mixtures were concentrated using a Speed-vac centrifuge (Eppendorf, Germany), dissolved in 0.1% formic acid, and analyzed in an ultra-performance liquid chromatograph (UPLC) system (Waters, Milford, MA) coupled with an LTQ Orbitrap Velos mass spectrometer (ThermoFisher Scientific, Waltham, MA) as previously reported.26,27 Proteome Discoverer software (version 2.4.0.305, Thermo Fisher Scientific, Waltham, MA) were used to process the raw data with search algorithms SEQUEST (version 1.3, Thermo Fisher Scientific, Waltham, MA) against Mycobacterium tuberculosis (strain ATCC 25618/H37Rv) database from Swiss-Prot database (release 2021_04). All the serum samples from the same condition were pooled and the LC-MS/MS analysis was performed in three technical replicates.
Peptide Synthesis and Polyclonal Antibody Preparation
The sequences of peptides with high frequency in the results of LC-MS/MS were sent to Genscript (Nanjing, China) for antigenicity analysis by GenScript OptimumAntigenTM design tool and synthesis. Polyclonal antibodies were produced in New Zealand rabbit and IgG were purified by Genscript (Nanjing, China) for further analysis.
Participants
Patients who seek health care in the Beijing Chest Hospital in China between December 2019 and January 2020 were enrolled in this study. Each person was classified into one of three diagnostic categories following the Diagnosis for Pulmonary Tuberculosis (WS288-2017) Guidelines: (i) confirmed TB patients: clinical TB symptoms with at least one sputum sample culture- and/or Xpert-positive for MTB; (ii) clinically diagnosed TB patients: clinical TB symptoms without any positive laboratory evidence by culture and Xpert plus clinical response to anti-TB treatment; (iii) non-TB patients: no evidence of TB based on laboratory and clinical examinations. Two milliliters of blood were collected from each patient, and centrifugated at 2000 × g for 10 min to separate serum. The serum samples were stored at −80°C refrigerator immediately. Demographic and clinical characteristics were obtained by reviewing the medical records. This study was approved by the Ethics Committee of the Beijing Chest Hospital, affiliated to Capital Medical University (2020–030). The patients provided the signed informed consent prior to enrolment.
Direct Competitive Enzyme-Linked Immunosorbent Assay (ELISA)
The competitive ELISA was performed as previously described with slight modifications.28 Briefly, polystyrene microtiter plates were coated with 400 ng polyclonal IgG obtained from rabbits immunized by polypeptides in pH 9.6 carbonate-bicarbonate buffer overnight at 4°C. After three washes with phosphate buffer saline with 0.5% Tween 20, 300 μL of 5% skim milk were used to block remaining protein-binding sites. 50 μL diluted serum samples (1:2) were added to the wells, and 50μL proper diluted polypeptide coupled with horseradish peroxidase (HRP) using EZ-Link Plus Activated Peroxidase Kit (Thermo Scientific, Rockford, IL, USA) were added as quickly as possible. Then mix thoroughly, and the plates were incubated for 2 h at room temperature. After three washes, TMB substrate solution were added and the reactions were incubated for 30 min in dark. Then, 50 μL of 2 M H2SO4 was added to stop the reactions and optical density (OD) values were read at 450nm by a microplate reader. A standard curve was prepared meantime by plotting standard peptides (Genscript, Nanjing, China) concentration on x-axis versus OD values on the y-axis to determine the antigen concentrations of unknown tested samples. All tests were performed in triplicate on each plate.
Statistical Analysis
Chi-square test and odds ratios (OR) with 95% confidence intervals (95% CI) were used to explore the relationship between TB patients and non-TB patients with age and sex. The data analysis of hematology parameters and ELISA was used Microsoft Excel 2011 and GraphPad Prism 6.0 using 2-tailed unpaired student t test if data were normally distributed. Non-parametric Mann–Whitney U-test was used for data that were not normally distributed. Results are shown as mean ± standard deviations (SD). P < 0.05 were considered statistically significant. A receiver operating characteristic analysis (ROC) was conducted using GraphPad Prism 6.0. The cut-off values of the positive tests were set as those maximized the Youden’s J Index. Sensitivity was defined as true-positives/(true-positives+ false-negatives). Specificity was defined as true-negatives/(true-negatives+ false-positives).
Results
Identification of MTB-Specific Peptides in Mouse Serum by LC-MS/MS
After intravenous injection into BALB/c mice, serum specimens were collected 24 hours after injection for mass spectrometry analysis. A total of 65 peptides from 4 MTB precursor recombinant proteins were identified in mouse serum by LC-MS/MS (Table S1). 27 peptides from MPT32, 9 peptides from MPT64, 24 peptides from PstS1 and 5 from CFP10 were identified respectively. The numbers of amino acids in the target peptides ranged from 4 to 50.
Demographic and Clinical Characteristics of Enrolled TB Patients and Non-TB Patients
A total of 43 pulmonary TB patients and 30 non-TB patients were included in our analysis. There was no significant difference in age between two groups. In contrast, males were more common in TB patients than in non-TB group (P=0.028). 46.5% of TB patients were diagnosed on the basis of laboratory evidence, whereas the remaining 53.5% patients were only diagnosed on the presence of clinical symptoms.
To gain a comprehensive understanding of blood background of enrolled patients, the related biochemical clinical factors and blood cytology index used in routine clinical care were also collected and compared. The pulmonary TB patients had characteristic changes in blood parameters (Tables S2 and S3).
Serum Levels of Mtb-Specific Peptides in Pulmonary TB Patients
Based on the results of LC-MS/MS and antigenicity analysis, 5 peptides from MPT64, CFP10, PstS1 and MPT32 were selected as candidates for serological analysis (Table S4, Figure S1). Standard calibration curves for antigen quantitation were generated by ELISA using standard peptides respectively. As shown in Figure 2, the 5 peptides in pulmonary TB patients’ serum could be recognized by corresponding polyclonal antibodies respectively. The results of directed competitive ELISA with peptides MPT64-2, CFP10-2, PstS1-2 and corresponding antibodies showed that there were significant differences between two cohorts.
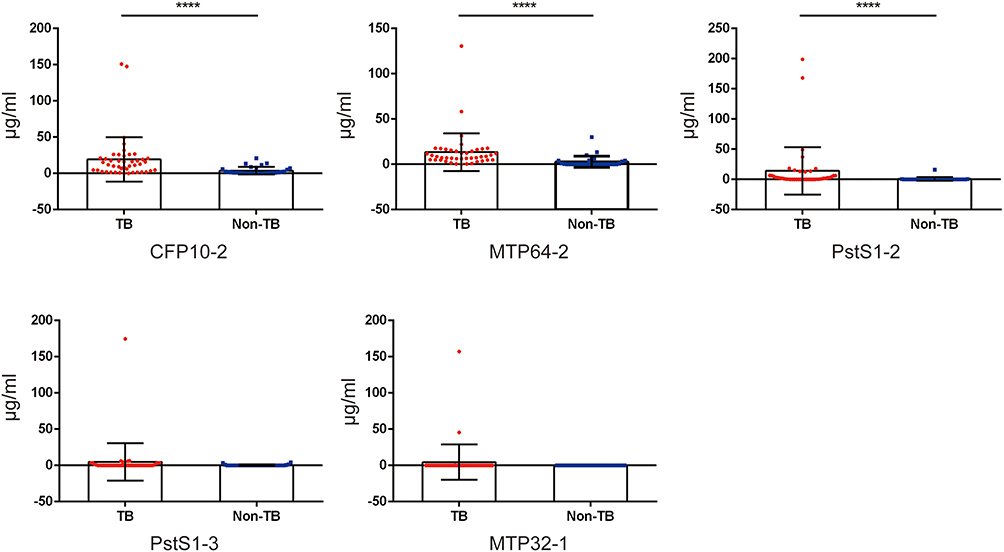 |
Figure 2 Comparative analysis of MPT64, CFP10, PstS1 and MPT32 ELISA. A total of 73 serum samples were used for ELISA analysis, including 43 from patients with pulmonary TB and 30 from non-TB patients. ****, P<0.0001. |
Accuracy of MTB-Specific Peptides for Diagnosis of Pulmonary TB
ROC with 95% confidence intervals (CI) was used to analyze the results (Table 1 and Figure 3A). MPT64-2 exhibited the most promising sensitivity (81.4%; 95% CI, 66.6%–91.6%), followed by PstS1-2 (67.4%; 95% CI, 51.3%–80.5%) and CFP10-2 (60.5%; 95% CI, 44.4%–75.0%). In contrast, PstS1-2 had the highest specificity (93.3%; 95% CI, 76.5%–98.8%), followed by CFP10-2 (86.7%; 95% CI, 69.3%–96.2%) and MPT64-2 (83.3%; 95% CI, 65.3%–94.4%). We also analyzed the diagnostic accuracy of the combined use of peptide MPT64-2 and CFP10-2 or PstS1-2, respectively; but it could not improve the sensitivity and specificity simultaneously. According to the area under the curve (AUC), MPT64-2 (AUC = 0.863, P<0.0001) had better diagnostic validity. A one-to-one match between laboratory evidence and ELISAs were conducted (Figure 3B) and the integrated results of GeneXpert, MPT64-2 ELISA, CFP10-2 ELISA and PstS1-2 ELISA showed that only 2 sample (2/43, 4.65%) was demonstrated as negative by all methods. And there were no significant differences in the levels of serum MTB-specific peptides between TB patients on the basis of laboratory evidence or clinical symptoms.
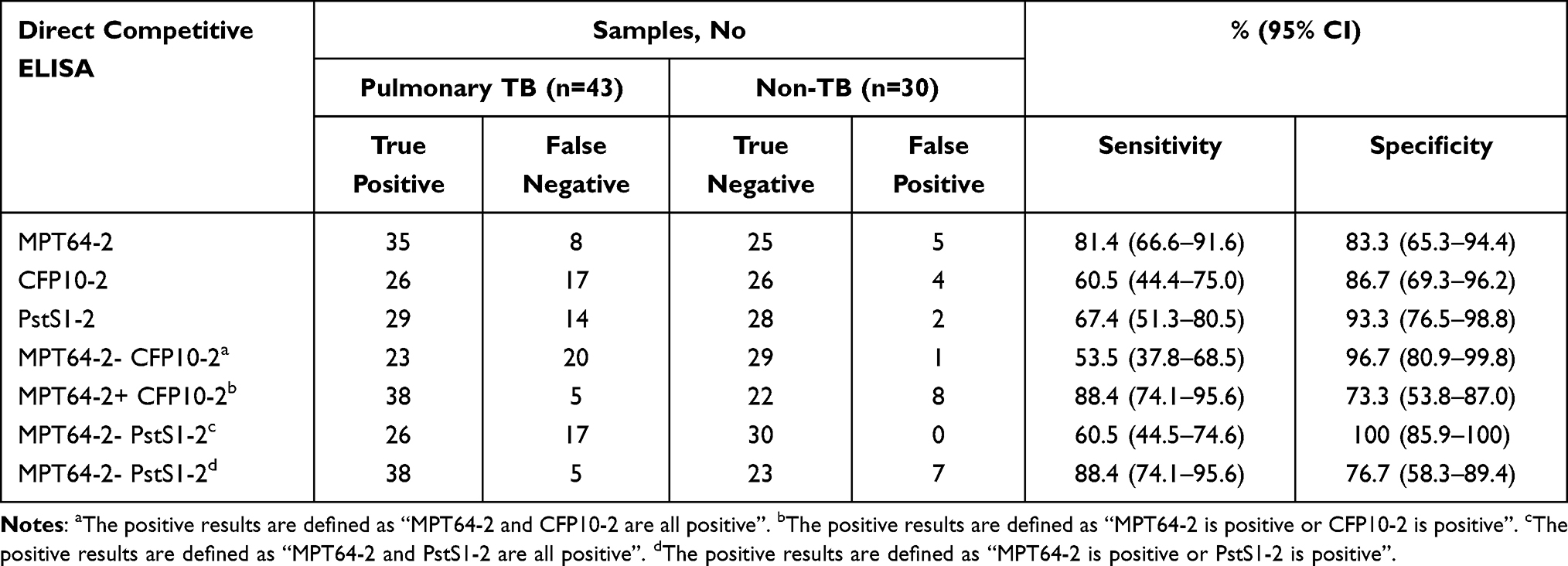 |
Table 1 Diagnostic Validity of MPT64-2, CFP10-2 and PstS1-2 Direct Competitive ELISA with Human Serum Samples |
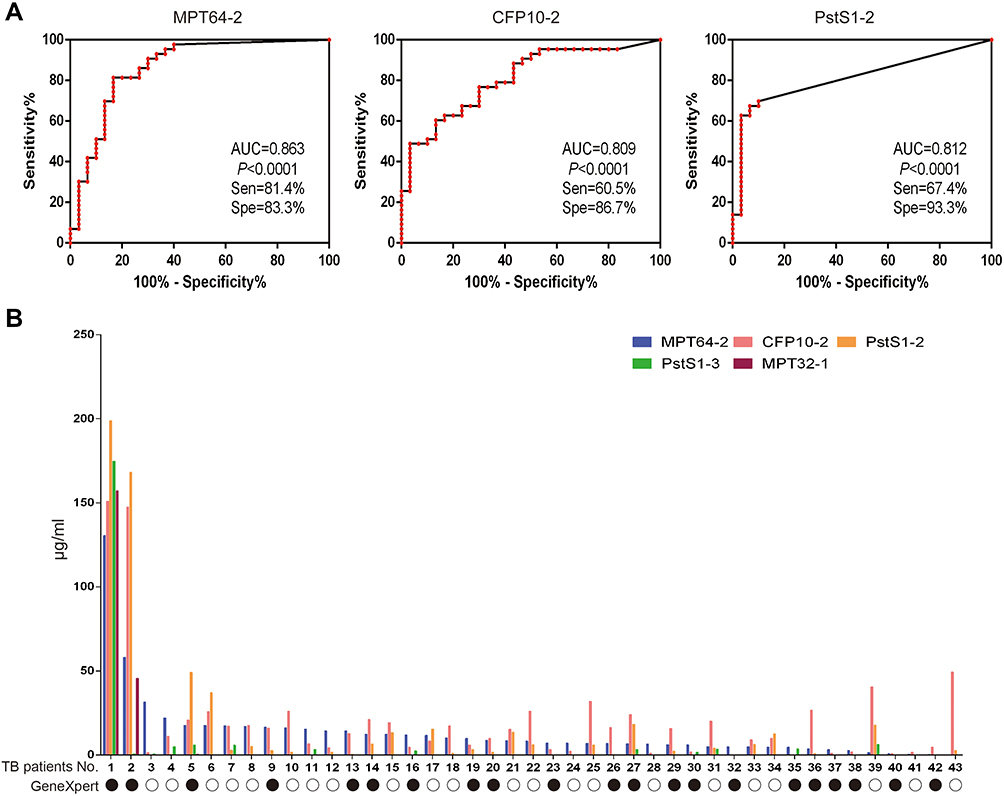 |
Figure 3 Receiver operating characteristic analysis (ROC) of MPT64-2, CFP10-2 and PstS1-2 (A) and one to one match results between laboratory evidence and ELISAs (B). Solid circle: TB patients with positive results by GeneXpert; hollow circle, TB patients with negative results by GeneXpert. |
Discussion
The diagnosis of active TB patients remains challenging despite years of efforts, especially for patients with paucibacillary TB. Novel biomarkers are urgently required for point of care TB diagnostics.14 In this study, we firstly developed an effective approach to identify new antigen biomarkers via mass spectrometry-based peptidomics. Our preliminary results revealed that the predominant fraction of the peptides in the experimental animal model came from mouse. This is not surprising, since the serum serves as reservoir for large quantities of peptides that are released by degradation of proteins in mouse blood. As a consequence, the identification of proteolytic peptides from low-abundance protein is generally hampered by the presence of the more abundant protein in serum, such as albumin, immunoglobulins, transferrin, and lipoproteins.29 Tuberculosis secreted proteins that gain access to the blood circulation is likely in a low abundance in infected human, thus the amounts of tuberculosis peptides are beyond the detection limits of the mass spectrum. Although the utilization of high‐resolution mass spectrometer help enhancing detection of low-abundance peptides, issues related to low reproducibility of these peptides remains open. Using a mouse model, we showed that the intravenous injection of candidate proteins could significantly amplify the production of MTB-specific peptides circulating in peripheral blood. Whereas the immune system, metabolic process, stress response, and the activity of some genes varies between mice and human, we should take into account systematic difference between species but mouse is still an excellent model for aspects of human biology.30–32 Our approach had the benefit of directly identifying antigen biomarkers of exogenous pathogens. Importantly, further validation of these peptides suggested that human and mouse share a very similar pattern of protein degradation system, thereby boosting its potential feasibility for identify antigen biomarkers of infectious diseases.
In the present study, a set of MTB-specific antigens were identified in mouse serum, as well as serum samples from active TB patients. ROC curve analysis demonstrated that MPT64-2 could diagnose active TB patients with a good performance (AUC = 0.863), despite it was not the most frequently detected peptide in animal model. This discrepancy could be due to the diversity between mice and human and the affinity between antibody and antigen. Peptides derived from exogenous antigens and were generated by proteasomal degradation. The duration of this intermediate phase of antigen cross-presentation can vary between different experimental systems, types of dendritic cells (DCs), and maturation stimuli.33 In most cases, it lasts at least 16–20 h before cross-presentation is shut down 20–24 h after the initiation of DC activation.33 So, we selected 24h after intravenous injection in this study. However, the antigen-derived peptides may be changed over time due, which may influence the sensitivity and specificity of selected peptides. Moreover, a proteomics study by Malen et al showed that MPT64 and its homologs constituted a major part of the exported proteins from MTB H37Rv.34 We speculate that the higher MPT64 excretion is positively associated with the higher numbers of degraded peptides compared with CFP10 and PstS1, thereby resulting in increased diagnostic accuracy. Notably, the combined use of MPT64-2 and CFP-10 or MPT64-2 and PstS1-2 did not significantly improve the sensitivity for detection of active TB patients, reflecting the substantial diagnostic overlap between two biomarkers. In view of our preliminary data, future research should pay more attention to identify peptides derived from highly abundant secreted protein.
The need for a rapid, simple and affordable point-of-care test (POCT) for tuberculosis remains unmet despite great advances in molecular diagnostics. Our clinical performance results have the potential to meet the WHO sensitivity (>65%) and specificity (>87%) targets for a non-sputum-based test in detecting tuberculosis.10 In addition, this antigen-based method has several advantages over traditional methods. On one hand, sputum-bacilli tests require sufficient bacilli-containing sputum samples;35 however, they are difficult to obtain, especially from subclinical TB patients and children.36,37 Therefore, the detection of MTB-specific antigen using serological immunofluorescent assays outperform the traditional methods in the accessibility of specimens for sputum-scarce individuals within 1 hour, thus conceivably helping reduce the delay before diagnosis and enable early treatment. On the other hand, the cost of diagnostic tests in an important concern that appropriately influences the utilization for patients with symptoms suggestive of active TB. The WHO has highlighted that a price target of US$ 4.00 would be affordable in the high-burden countries,10 which becomes a cost barrier to widespread of molecular diagnostics. The serological tests based on MTB-specific antigen holds great promise for achieving this target. Detection of MTB antigens in patient blood samples could provide direct evidence of TB and the approach to detect peptides derived from MTB proteins rather than MTB full-length proteins fully take into account the problem induced by endogenous proteasome degradation. Taken together, our results support the further development and optimization of serological immunofluorescent assays based on MTB peptides to meet the WHO’s target product profiles for new TB diagnostics.
The present study has several limitations. First, only polyclonal antibody rather than monoclonal antibody was used for assessing the performance of novel biomarkers in our cohort. We believed that the monoclonal antibody would allow an improvement in the sensitivity and specificity of antigen-based assays. Second, several previous studies demonstrated that molecules circulating in the blood had a capacity to filter across the glomerular basement membrane of the kidneys into urine.38 Of note, the concentration of LAM in urine, a major component of cell envelope in tubercle bacilli, was 10 times higher than that in serum.38,39 Thus, further confirmation is required for identifying the performance of MTB-specific peptides in urine specimens. Third, we also found that the peptides from the four proteins existed distinct abundance in each individual, which indicated that the antigen-presenting process varied in each TB-positive patient and may influence the performance of antigen-derived peptides. Finally, we failed to confirm the association of the increased bacterial load with higher antigen concentration. A plausible explanation for this finding is the varying capability in secreting antigen across clinical MTB isolates. In addition, the sample size of our active TB cohort may be another reason for poor correlation between antigen concentration and bacterial load of TB patients. Further study will be carried out to validate our results.
In conclusion, we develop an effective approach to identify new antigen biomarkers via mass spectrometry-based peptidomics. The intravenous injection of candidate proteins could significantly amplify the production of MTB-specific peptides circulating in peripheral blood. In addition, multiple peptides exhibit promising efficacy in diagnosis of active TB patients. Further studies are urgently needed to develop and optimize serological immunofluorescent assays based on MTB peptides to meet the WHO’s target product profiles for new TB diagnostics.
Data Sharing Statement
All of the raw mass spectra files in the present study have been deposited into the publicly accessible database PeptideAtlas and are available under dataset Identifier PASS01715 with dataset password AX5346dgh (http://www.peptideatlas.org/PASS/PASS01715).
Ethical Approval
The animal study was reviewed and approved by the Experimental Animal Committee of Beijing Chest Hospital affiliated to Capital Medical University (2020-022). All procedures performed on human samples were carried out according to the tenets of the World Medical Association’s Declaration of Helsinki and was approved by the Ethic Committee of Beijing Chest Hospital affiliated to Capital Medical University (2020-030).
Funding
This study was supported by the Beijing Hospitals Authority Ascent Plan (DFL20191601), the Capital’s Funds for Health Improvement and Research (2020-1-1041), the Beijing Hospitals Authority Clinical Medicine Development of Special Funding (ZYLX202122), CAMS Innovation Fund for Medical Sciences (2021-I2M-1-037) and the National Science and Technology Major Project of China (2017ZX10201301-002-003). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of manuscript.
Disclosure
The authors declare that there are no competing financial interests.
References
1. World Health Organization. Global tuberculosis report 2021. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
2. Pai M, Nicol MP, Boehme CC. Tuberculosis diagnostics: state of the art and future directions. Microbiol Spectr. 2016;4:5.
3. Schito M, Migliori GB, Fletcher HA, et al. Perspectives on advances in tuberculosis diagnostics, drugs, and vaccines. Clin Infect Dis. 2015;61(Suppl 3):S102–18.
4. Wolinsky E. Conventional diagnostic methods for tuberculosis. Clin Infect Dis. 1994;19(3):396–401.
5. Tan Y, Su B, Cai X, et al. An automated smear microscopy system to diagnose tuberculosis in a high-burden setting. Clin Microbiol Infect. 2019;25(12):1553–1559.
6. Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005–1015.
7. Iwamoto T, Sonobe T, Hayashi K. Loop-mediated isothermal amplification for direct detection of Mycobacterium tuberculosis complex, M. avium, and M. intracellulare in sputum samples. J Clin Microbiol. 2003;41(6):2616–2622.
8. Horne DJ, Kohli M, Zifodya JS, et al. Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2019;6:CD009593.
9. Denkinger CM, Schumacher SG, Boehme CC, Dendukuri N, Pai M, Steingart KR. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2014;44(2):435–446.
10. Qin YM, Hu CY, Pang Y, Kastaniotis AJ, Hiltunen JK, Zhu YX. Saturated very-long-chain fatty acids promote cotton fiber and Arabidopsis cell elongation by activating ethylene biosynthesis. Plant Cell. 2007;19(11):3692–3704. doi:10.1105/tpc.107.054437
11. Broger T, Sossen B, du Toit E, et al. Novel lipoarabinomannan point-of-care tuberculosis test for people with HIV: a diagnostic accuracy study. Lancet Infect Dis. 2019;19(8):852–861. doi:10.1016/S1473-3099(19)30001-5
12. Nicol MP, Allen V, Workman L, et al. Urine lipoarabinomannan testing for diagnosis of pulmonary tuberculosis in children: a prospective study. Lancet Glob Health. 2014;2(5):e278–84. doi:10.1016/S2214-109X(14)70195-0
13. Qin Y-M, Pujol FM, Hu C-Y, et al. Genetic and biochemical studies in yeast reveal that the cotton fibre-specific GhCER6 gene functions in fatty acid elongation. J Exp Bot. 2006;58(3):473–481. doi:10.1093/jxb/erl218
14. Liu C, Zhao Z, Fan J, et al. Quantification of circulating Mycobacterium tuberculosis antigen peptides allows rapid diagnosis of active disease and treatment monitoring. Proc Natl Acad Sci USA. 2017;114(15):3969–3974.
15. Liu C, Lyon CJ, Bu Y, et al. Clinical evaluation of a blood assay to diagnose paucibacillary tuberculosis via bacterial antigens. Clin Chem. 2018;64(5):791–800.
16. Dheda K, Gumbo T, Maartens G, et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017;5(4):291–360.
17. Boom WH, Canaday DH, Fulton SA, Gehring AJ, Rojas RE, Torres M. Human immunity to M. tuberculosis: t cell subsets and antigen processing. Tuberculosis. 2003;83(1–3):98–106.
18. Bekmurzayeva A, Sypabekova M, Kanayeva D. Tuberculosis diagnosis using immunodominant, secreted antigens of Mycobacterium tuberculosis. Tuberculosis. 2013;93(4):381–388.
19. Tang XL, Zhou YX, Wu SM, Pan Q, Xia B, Zhang XL. CFP10 and ESAT6 aptamers as effective Mycobacterial antigen diagnostic reagents. J Infect. 2014;69(6):569–580.
20. Cheon HJ, Lee SM, Kim SR, et al. Colorimetric detection of MPT64 antibody based on an aptamer adsorbed magnetic nanoparticles for diagnosis of tuberculosis. J Nanosci Nanotechnol. 2019;19(2):622–626.
21. Hoel IM, Sviland L, Syre H, et al. Diagnosis of extrapulmonary tuberculosis using the MPT64 antigen detection test in a high-income low tuberculosis prevalence setting. BMC Infect Dis. 2020;20(1):130.
22. Alcaide F, Trastoy R, Moure R, et al. Multiplex real-time PCR-shortTUB assay for detection of the mycobacterium tuberculosis complex in smear-negative clinical samples with low Mycobacterial loads. J Clin Microbiol. 2019;57:8.
23. Harriff MJ, Wolfe LM, Swarbrick G, et al. HLA-E presents glycopeptides from the Mycobacterium tuberculosis protein MPT32 to human CD8(+) T cells. Sci Rep. 2017;7(1):4622.
24. Mehrpour M, Esclatine A, Beau I, Codogno P. Overview of macroautophagy regulation in mammalian cells. Cell Res. 2010;20(7):748–762.
25. Pan SH, Malcolm BA. Reduced background expression and improved plasmid stability with pET vectors in BL21 (DE3). Biotechniques. 2000;29(6):1234–1238.
26. Zheng J, Chen L, Liu L, et al. Proteogenomic analysis and discovery of immune antigens in Mycobacterium vaccae. Mol Cell Proteomics. 2017;16(9):1578–1590.
27. Liu L, Deng J, Yang Q, et al. Urinary proteomic analysis to identify a potential protein biomarker panel for the diagnosis of tuberculosis. IUBMB Life. 2021;73(8):1073–1083.
28. Kohl TO, Ascoli CA. Direct competitive Enzyme-Linked Immunosorbent Assay (ELISA). Cold Spring Harb Protoc. 2017;2017(7):pdb prot093740.
29. Tirumalai RS, Chan KC, Prieto DA, Issaq HJ, Conrads TP, Veenstra TD. Characterization of the low molecular weight human serum proteome. Mol Cell Proteomics. 2003;2(10):1096–1103.
30. Lin S, Lin Y, Nery JR, et al. Comparison of the transcriptional landscapes between human and mouse tissues. Proc Natl Acad Sci U S A. 2014;111(48):17224–17229.
31. Yue F, Cheng Y, Breschi A, et al. A comparative encyclopedia of DNA elements in the mouse genome. Nature. 2014;515(7527):355–364.
32. Cheng Y, Ma Z, Kim BH, et al. Principles of regulatory information conservation between mouse and human. Nature. 2014;515(7527):371–375.
33. Alloatti A, Kotsias F, Magalhaes JG, Amigorena S. Dendritic cell maturation and cross-presentation: timing matters! Immunol Rev. 2016;272(1):97–108.
34. Malen H, Berven FS, Fladmark KE, Wiker HG. Comprehensive analysis of exported proteins from Mycobacterium tuberculosis H37Rv. Proteomics. 2007;7(10):1702–1718.
35. Warsinske H, Vashisht R, Khatri P. Host-response-based gene signatures for tuberculosis diagnosis: a systematic comparison of 16 signatures. PLoS Med. 2019;16(4):e1002786.
36. Drain PK, Bajema KL, Dowdy D, et al. Incipient and subclinical tuberculosis: a clinical review of early stages and progression of infection. Clin Microbiol Rev. 2018;31(4):e00021–18.
37. Reuter A, Hughes J, Furin J. Challenges and controversies in childhood tuberculosis. Lancet. 2019;394(10202):967–978.
38. Bulterys MA, Wagner B, Redard-Jacot M, et al. Point-of-care urine LAM tests for Tuberculosis diagnosis: a status update. J Clin Med. 2019;9(1):111.
39. Broger T, Tsionksy M, Mathew A, et al. Sensitive electrochemiluminescence (ECL) immunoassays for detecting lipoarabinomannan (LAM) and ESAT-6 in urine and serum from tuberculosis patients. PLoS One. 2019;14(4):e0215443.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.