")
Back to Journals » Patient Preference and Adherence » Volume 17
A Participatory Approach Involving Patients with Cystic Fibrosis and Healthcare Professionals for the Co-Design of an Adherence-Enhancing Intervention Toolkit
Authors Viprey M , Mougeot F, Dima AL , Haesebaert J, Occelli P, Durieu I, Rouzé H , Reynaud Q, Touzet S
Received 8 November 2022
Accepted for publication 22 March 2023
Published 10 April 2023 Volume 2023:17 Pages 995—1004
DOI https://doi.org/10.2147/PPA.S389792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Marie Viprey,1,2 Frédéric Mougeot,3 Alexandra Lelia Dima,2,4 Julie Haesebaert,2,5 Pauline Occelli,2,5 Isabelle Durieu,2,6 Héloïse Rouzé,2,5 Quitterie Reynaud,2,6 Sandrine Touzet2,7
1Hospices Civils de Lyon, Pôle Santé Publique, Service des Données de Santé, Lyon, France; 2Research on Healthcare Performance RESHAPE, INSERM U1290, Université Claude Bernard Lyon 1, Lyon, France; 3Centre Max Weber, UMR 5283 - ENSEIS, Villeurbanne, France; 4Health Technology Assessment in Primary Care and Mental Health (PRISMA) Research Group, Parc Sanitari Sant Joan de Déu, Institut de Recerca Sant Joan de Déu, Barcelona, Spain; 5Hospices Civils de Lyon, Pôle Santé Publique, Service Recherche et Epidémiologie Cliniques, Lyon, France; 6Hospices Civils de Lyon, Centre Hospitalier Lyon Sud, Centre de Référence Adulte de la Mucoviscidose, Pierre Bénite, France; 7Hospices Civils de Lyon, Pôle Santé Publique, Service de Santé au Travail, Lyon, France
Correspondence: Marie Viprey, Hospices Civils de Lyon, Service des Données de Santé, 162 Avenue Lacassagne, Lyon, 69003, France, Tel +33 4 72 11 51 39, Fax +33 4 72 11 57 20, Email [email protected]
Purpose: Cystic fibrosis (CF) is an inherited life-shortening disease involving a significant treatment burden. Few interventions have been proven effective in improving adherence, and of these fewer have been adopted for implementation. Patient participation in research is increasingly desired in developing relevant health care services. A participatory approach was implemented in an adult CF center to co-design an adherence-enhancing intervention toolkit. We aimed to report on the participatory process and the results regarding the co-designed intervention.
Patients and Methods: Two focus group sessions and four working sessions were conducted at 4-week intervals with three healthcare professionals (HCP; physician, nurse, physiotherapist), eight patients, and two researchers (sociologist, public health pharmacist). The two initial focus group sessions were dedicated to the collection of narratives about CF treatment experiences to identify drivers of adherence. The next four working sessions were dedicated to the reflection on solutions that could alleviate the difficulties identified and be used in current clinical practice. The researchers observed during all sessions the interactions between participants, group dynamics, and process of implementation of the collective reflection.
Results: The process facilitated an active participation of patients and HCP, who contributed equally to the intervention development. The co-design adherence-enhancing intervention toolkit consisted in a self-questionnaire to be completed by patients before the medical consultation and used as a communication support during the consultation, plus a toolkit of solutions to be proposed by the HCP for each barrier identified by patients, and to be followed up during the next consultation.
Conclusion: This study demonstrated that a participatory approach involving CF patients and HCP lead to the development of an adherence-enhancing intervention toolkit, using a 6-session format; the benefits of the co-designed intervention on the medication adherence have yet to be tested in a multicenter, open-label study in 3 centers in France.
Keywords: cystic fibrosis, chronic treatment, medication adherence, patient engagement, participatory research
Introduction
Cystic fibrosis (CF) is an inherited disease that leads to dysfunction in multiple organ systems and progressive respiratory failure, and eventually to death or lung transplantation.1 In France, the systematization of early diagnosis since 2002 and the use of new treatment strategies have led to a significant improvement in the life expectancy over the past decades.2 Due to the treatment burden, the question of patients’ medication adherence thus arises in CF, as in other chronic pathologies.3,4 Published studies have reported that adherence ranges from 35% to 75% and depends on the age, therapeutic class, and regimen complexity.5–7 Importantly, low adherence may lead to worse health outcomes and quality of life, and greater health-care use.6,8–10 Few interventions have been developed to improve patient adherence in the context of CF11–16 and fewer have been shown to be effective enough to be recommended for implementation.
Patient participation in research is increasingly desired in developing relevant health care services.17–19 Some studies used the participation of CF patients in the identification of research priorities,20 in clinical guideline development,21 or in a quality improvement program22 have demonstrated the relevance of the participation of these patients who have a experiential knowledge of their disease.23 The interests of involving patients, healthcare professionals, and researchers in the co-design of a program aiming at improving medication adherence are multiple. First, involving patients enables to understand the difficulties they encounter in the administration of their treatments, according to their life situations, and the factors determining their adherence. Second, it allows their participation in the choice of the tools that seem the most relevant to them in a patient-need-centered intervention.
A participatory approach was therefore implemented in the adult CF center of the Hospices Civils de Lyon (Lyon, France), in order to co-design an adherence-enhancing intervention toolkit. We aimed in the present study to report on the participatory process and the results regarding the co-designed intervention.
Materials and Methods
Study Design and Setting
We conducted a patient engagement study, in accordance with the INVOLVE principles,24 in the context of a participatory research25 based on two focus groups and four working sessions. We used the GRIPP2 (Guidance for Reporting Involvement of Patients and the Public) reporting checklist to guide the reporting.26 The study took place in an adult CF center located in a university hospital center in Lyon, France (Hospices Civils de Lyon, 600 adult CF patients). The group (see next section) met in an independent meeting room of the hospital. Two-hour sessions were scheduled each month from January to June 2018. The sessions were scheduled during working hours, and patients were able to obtain medical proof of attendance to submit to their employers. The specificity of CF, in particular the risk of respiratory tract infection, required patients to wear a mask during the sessions. Masks were available at the entrance of the meeting room.
Participants
The group consisted of three healthcare professionals (HCP; a physician, a nurse, and a physiotherapist), eight adult patients, and two researchers (a sociologist who was the group facilitator -FM-, and a public health pharmacist who was the observer of the functioning of the group -MV). The inclusion criteria for HCP were: (1) practicing in a CF expert center; (2) being available to participate in the focus groups. The inclusion criteria for patients were: (1) being diagnosed with CF; (2) being at least 18 years old; (3) having sufficient cognitive abilities and French language skills to discuss one’s experience with CF and its treatment. The patient recruitment was performed at the discretion of the treating physician. The recruitment was realized in order to represent the diversity of patients in terms of age, sex, health status, social and professional status, treatment burden, and physician impression of adherence (adherence was not measured quantitatively prior to participation). The patient’s characteristics presented in Table 1 were collected from patients’ medical record.
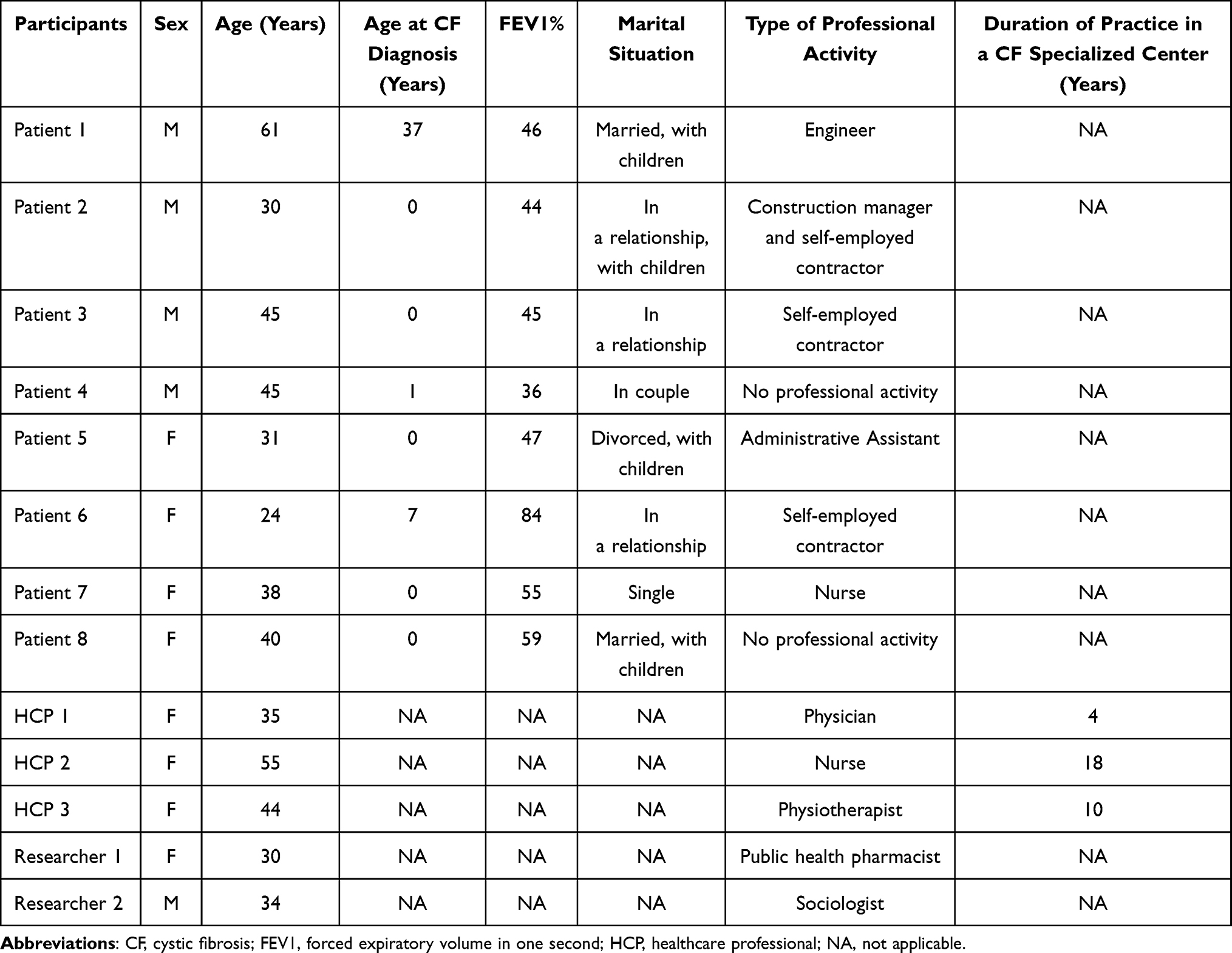 |
Table 1 Characteristics of the Participants |
The participation to single working sessions of different actors was solicited when necessary in the process: a public health physician (ST) as an observer, a hospital pharmacist (HR) who presented existing tools for improving medication adherence, and a health psychology researcher (AD) who made a proposal for structuring the process from problem identification to solution development.
Analysis of the Participatory Approach
The sociologist (FM) and the public health specialist (MV) were present during all the sessions and observed the interactions between the participants, the dynamics of the group, as well as the process of implementation of the collective reflection on medication adherence of CF patients within the framework of this participatory approach. Based on the discussion reports and materials generated for and during the discussions, and the lived experience of the sessions, the sociologist (FM) applied a qualitative analysis process informed by clinical sociology27–30 to produce an individual report focusing on the participatory processes and aiming to assess to which extent 1) participation was balanced among group members, and 2) participants commonly agreed on features of the intervention toolkit. Then public health specialists (MV and ST) read the report and revised it according to their own perceptions of their experience of the process.
Intervention Co-Design
The first two sessions consisted in focus groups dedicated to the collection of narratives about the experiences of CF treatments according to the method of clinical sociology.27–30 The objective was to co-construct a common understanding of the experience of the disease and its treatments, to identify the factors determining medication adherence. For the following four working sessions, the group was invited to reflect on solutions that could alleviate the difficulties highlighted and to validate their feasibility and use in current clinical practice. To help with this, the pharmacist (HR) gave a presentation on all the studies that investigated the effect of adherence-enhancing intervention programs or tools in the context of CF11,31–40 (3rd session). Then the psychologist specialized in medication adherence (AD) presented a methodology for structuring the process of identifying solutions to the problems identified during the two focus group sessions (4th session).
The sociologist (FM) was responsible for leading the group and moderating the discussion (following a framework of questions prepared in advance and available upon reasonable request to the corresponding author). A discussion report was written at the end of each session by the sociologist (FM), and distributed to all participants for approval at the beginning of the following session. Participants could, if they wanted to, exchange ideas and documents between sessions via a google sheet.
Ethics
The present study complies with the Declaration of Helsinki. The participation in the group and the sessions was on a voluntary basis. Prior to their inclusion, participants were informed about the objectives of the research, as well as the expectations and functioning of the group through an information letter. All participants provided informed consent.
A participation charter was written by the researchers and approved by all the participants. This charter outlined ethical aspects of group interactions, especially on ensuring an equal distribution of conversational turn-taking among participants, whether they were HCP or patients, and on the respect by all participants of the confidentiality of the information shared during the sessions. The study was approved by the local Institutional review board.
Results
Participants Characteristics and Conduct of Sessions
The eight patients ranged in age from 24 to 61 years, half were male and half were female. One patient was single, while all the others were in a relationship, with or without children. The FEV1% ranged from 36 to 84% (Table 1). All patients were treated with mucolytics and respiratory physiotherapy, and most of them were treated with inhaled antibiotics. Two patients were treated for CF-related diabetes and one patient was waiting for a lung transplant. Regarding the HCP, all were women and had between 4 and 18 years of experience in a specialized CF center (Table 1).
The two focus group sessions and the four working sessions were conducted as initially planned. All participants attended all sessions, except for two sessions for which two patients were absent (one absent for each of the two sessions).
Participatory Approach
The high participation was instrumental in creating a group stability, which enabled the building of shared representations of medication adherence difficulties and solutions during the 6 sessions. Patients, HCP, and researchers contributed equally to the focus groups: exchanges were balanced in terms of time and content. During the first two sessions, HCP and researchers were less talkative in order to leave to patients more opportunities to express themselves, they participated more actively in the remaining four sessions. This resulted in conversations between HCP, patients, and researchers to which all group members contributed by expressing their views on the ongoing discussion topics. For the first two sessions, the fact that patients took the initiative to express themselves indicated their shared interest in the topic of medication adherence. As all CF patient has experienced problems in taking their treatments at one time or another, the first two sessions really intended to get the patients talking about issues they themselves struggled with. The solutions to be found were based on consensus, which were not difficult to reach. Interactions between the participants were illustrative of an unexpectedly positive group cohesion, as it led to the continuation of formal or informal exchanges between the sessions via email or the information exchange platform Google Docs. At the end of the six sessions, patients expressed their willingness to get involved in the development and implementation of these tools built collectively. In addition, HCP and patients expressed their interest in participating in further participatory approaches.
Intervention Codesigned by the Group
The group found that while practitioners recognized the importance of the issue of adherence, the assessment of patient adherence was not carried out in the usual practices by HCP. To address this issue, the group proposed a self-questionnaire to be completed by patients before the medical consultation and then used as a communication support during the consultation (Appendix 1). This questionnaire is composed of two parts: 1) a visual analogue scale to assess their level of adherence to respiratory physiotherapy, aerosol therapy, drugs, and physical activity, and 2) questions about the main barriers to adherence encountered by the patients and identified by the group. Depending on the barriers identified by each patient, the HCP can propose during the consultation the solutions identified by the group for each barrier. A traceability of these exchanges allows a follow-up on the proposed solutions during the next consultation. The barriers and solutions identified are detailed below and summarized in Table 2.
 |
Table 2 Barriers of Adherence and Related Tools and Solutions Identified by the Group |
Firstly, the group agreed that it could be difficult for both HCP and patients to best organize all the treatments to be taken (airway clearance techniques, mucolytics, anti-inflammatory drugs, and antibiotics). CF treatments are time-consuming and require patients to organize their daily life for good medication adherence. Furthermore, any change in the professional or personal life can significantly affect the unstable balance between life and the disease, and its treatments. One patient proposed to use in the adherence support toolkit a breathing diary, a tool taking the form of one week agenda allowing to visualize the time slots dedicated to the different activities and treatments in order to best organize treatment intake.41 The group suggested that this document could be completed with the HCP in case of difficulties encountered in the organization of treatment intake.
Secondly, periods of life “at risk” in terms of poor medication adherence were identified: the teenage crisis and entry into adulthood, entry into student life, entry into working life, the birth of a child, the pre-grafting period that may lead fatigue, stress, or difficulties in projecting oneself into the future. The group stressed the need for information and the lack of social support during these periods. Information booklets for CF patients containing the words of patients and HCP were constructed in a participatory manner during the focus group sessions, to address the questions encountered by patients during these periods. To make up for the lack of interlocutors, a list of referring patients, the COMUCOs, was drawn up so that HCP can put patients in contact with each other on the basis of common problems. This companionship should enable patients to better project themselves in the future by benefiting from the experience of a peer. A charter for the COMUCO group was drawn up.
Thirdly, the group agreed that the introduction of a new treatment was a particularly risky time for non-adherence. A contact between patients and HCP after the introduction of the new drug faster than the usual delay between two consultations would allow a better visibility on the perceived effects of this treatment and its tolerance, and thus reduce the risk of non-adherence. It was suggested by the group that HCP could contact patients by email or text message one month after any treatment initiation, to ensure that they do not encounter any difficulty with it. A breathing diary was also included as a potential help to integrate the new treatment into the patient’s daily life, especially for particularly time-consuming treatments such as aerosols and insulin.
Fourthly, it appeared to the group that adherence fluctuated according to the type of treatment: oral treatments (such as digestive enzymes), for which adherence is good, were differentiated from other treatments, in particular aerosols and respiratory physiotherapy, for which adherence is lower, due to their constraining and time-consuming nature. The group considered which solutions could be provided to patients to save time with these therapies: for example, patients might ask for help from relatives to clean the aerosols, respiratory physiotherapy could be organized at home or at the workplace. Vitamins were also cited among the treatments for which the adherence is poor. Their periodicity of administration does not allow them to be included in the routine daily functioning. Two solutions were suggested to address this problem: to record the intake of vitamins on an electronic diary associated with a reminder system, or for vitamins that are taken every three months, to take it at the CF center at the time of their quarterly appointment. In addition to drugs, CF patients must have a physical activity, which is thought to be an additional treatment to increase life expectancy and quality of life. The group proposed that HCP should offer patients a more systematic follow-up by a sports coach available in the CF center, which would facilitate the integration of physical activity into their daily lives.
Fifthly, the group mentioned the fact that CF patients are connected to a variety of HCP (physicians, nurses, physiotherapists, psychologists, dieticians), and that because of the chronicity of the disease, some HCP-patient relationships may falter over time. The solution mentioned was to exchange with different HCP of the same profession in order to have different insights. This alternation between HCP can be organized within the CF center.
Finally, the group agreed that CF, as a chronic disease, could test the relationship between patients and their relatives, particularly because of the anxiety generated by this disease for the patients’ relatives. This can lead patients to not perform certain treatments in their presence, such as aerosols, which can be impressive for their entourage. To overcome this issue, it has been proposed that consultations could be opened more frequently to patients with their relatives.
Discussion
This participatory study led to the emergence of areas of understanding regarding the mechanisms of medication adherence in the management of CF, and to the co-design by a group of patients, HCP, and researchers of tools and solutions that can be integrated into routine clinical practice to meet the challenge of improving medication adherence.
As previously reported by George et al,42 the group indicated that consultations and interaction with the CF team could be a facilitator for self-management and support their attempts to adhere to their regimen. However, it was also mentioned that the issue of medication adherence was not systematically raised during the consultations, as previously shown in the study of Riekert et al.43 The barriers to adherence identified by the group were consistent with those identified in the qualitative study by George et al,42 such as the treatment burden with the difficulty to plan medication intake schedules for multiple medications and to reconcile it with family life and work, or during periods of significant life changes, and the difficulty to perform treatments in presence of family and friends. Similarly, the solutions proposed by the group were related to facilitators already identified in this previous study: support and reminders, and the establishment of a routine.
This study showed that therapeutic adherence can be understood in participatory research based on the experiential knowledge44 of patients and the medical knowledge of HCP. Experiential knowledge is the knowledge constructed over time from one’s subjective and intimate experience of a problem, subject, or in this case disease. This experiential knowledge is already driving health care service improvement in many domains and countries.45 Exchanges with patients showed that they are real experts in their care and that they do not question the expertise of HCP. Patients’ experience enriched the expertise of HCP, and the expertise of HCP strengthened the patients’ understanding of the health system and the constraints of HCP in their care.
A concern of such approaches is that the asymmetrical relationship between HCP and patients may interfere with the dynamics of such a group,46,47 but this was not observed here. The observers noted that from the first focus group session, patients were able to share their narratives freely in the presence of HCP. Over the course of the various sessions, the mutual understanding of the issues specific to each actor was strengthened. This can be explained by the chronicity, complexity, and early onset of the condition, which requires close collaboration in care (consultation every three months in CF center) and high levels of health literacy and self-management skills by patients.23
Between the various sessions, the members of the group were forthcoming with making proposals, sharing documents, and producing them. This high-quality engagement, not remunerated, was undoubtedly related to the ability to express oneself and to listening skills of participants, but it was also related to the importance of the issues addressed and to the solicitation of their experiential knowledge of users.48
The involvement of patients and HCP in the sessions allowed the development of pragmatic tools and solutions which could lead to the implementation of low-cost intervention that could be easily integrated into clinical practice. Patients have not favored particularly innovative or technological tools or interventions previously tested in published studies such as feedback by connected objects14,49,50 or building a web or mobile application.11,51 On the contrary, they invested more in relational spaces mobilizing the lay expertise of patients and the transmission of this experiential knowledge. This is the case of the COMUCOs, this network of expert patients who can be mobilized by other users regarding sensitive issues related to their experience of daily life with the disease. This is also the case for information brochures that mobilized the expert knowledge of HCP and the experiential knowledge of users. Some of the pragmatic tools and solutions combined to lead to the co-designed intervention have shown their feasibility in published studies: reminder or follow-up by text message or phone,35,36 or physiotherapy at home.35
Strengths and Limitations
This study has some limitations. First, the group was composed of patients and HCP from a single CF center, and those were among the most willing to engage in discussions about medication adherence, which may limit generalizability. However, we were able to create a heterogeneous group in terms of socio-demographic characteristics and clinical severity for patients, and in terms of professional categories represented. Second, in addition to the observation by the sociologist, it might have been interesting to complete the evaluation of the participatory approach by asking the participants about their experience of this process using a questionnaire.
Conclusion
This study demonstrated that a participatory approach involving CF patients and HCP lead to the development of an adherence-enhancing intervention toolkit, using a 6-session format; the benefits on the medication adherence have yet to be tested. The co-designed intervention will be tested in a multicenter, open-label study in 3 centers in France (ClinicalTrials.gov Identifier: NCT03226795).
Ethics Approval
The study was approved by the Institutional review board (Comité de protection des personnes ouest IV – Nantes).
Acknowledgments
We thank the patients and healthcare professionals who participated in the group, and Stéphanie Poupon-Bourdy for study coordination. We also thank Hélène Boyer and Shanez Haouari Hospices Civils de Lyon) for help in manuscript preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by a grant from the Programme Hospitalier de Recherche Clinique Interrégional (PHRC-I 2016-015) from the French ministry of health (Ministère chargé de la Santé, Direction de l’Hospitalisation et de l’Organisation des Soins).
Disclosure
Dr Marie Viprey reports grants from DGOS, during the conduct of the study; grants from EPI-PHARE (Agence Nationale de Sécurité du Médicament et des Produits de Santé, ANSM), outside the submitted work. Dr Héloïse Rouzé reports grants from French ministry of health (Ministère chargé de la Santé, Direction de l’Hospitalisation et de l’Organisation des Soins), during the conduct of the study. The authors report no other conflict of interest related to this study.
References
1. O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet Lond Engl. 2009;373(9678):1891–1904. doi:10.1016/S0140-6736(09)60327-5
2. Vaincre la Mucoviscidose. French cystic fibrosis registry annual data report 2020; 2020. https://www.vaincrelamuco.org/sites/default/files/french_cf_registry_2020_annual_report_v1.pdf.
3. Sawicki GS, Sellers DE, Robinson WM. High treatment burden in adults with cystic fibrosis: challenges to disease self-management. J Cyst Fibros. 2009;8(2):91–96. doi:10.1016/j.jcf.2008.09.007
4. Sawicki GS, Ren CL, Konstan MW, et al. Treatment complexity in cystic fibrosis: trends over time and associations with site-specific outcomes. J Cyst Fibros. 2013;12(5):461–467. doi:10.1016/j.jcf.2012.12.009
5. O’Donohoe R, Fullen BM. Adherence of subjects with cystic fibrosis to their home program: a systematic review. Respir Care. 2014;59(11):1731–1746. doi:10.4187/respcare.02990
6. Narayanan S, Mainz JG, Gala S, Tabori H, Grossoehme D. Adherence to therapies in cystic fibrosis: a targeted literature review. Expert Rev Respir Med. 2017;11(2):129–145. doi:10.1080/17476348.2017.1280399
7. Rouzé H, Viprey M, Allemann S, et al. Adherence to long-term therapies in cystic fibrosis: a French cross-sectional study linking prescribing, dispensing, and hospitalization data. Patient Prefer Adherence. 2019;13:1497–1510. doi:10.2147/PPA.S211769
8. Nasr SZ, Chou W, Villa KF, Chang E, Broder MS. Adherence to dornase alfa treatment among commercially insured patients with cystic fibrosis. J Med Econ. 2013;16(6):801–808. doi:10.3111/13696998.2013.787427
9. Quittner AL, Zhang J, Marynchenko M, et al. Pulmonary medication adherence and health-care use in cystic fibrosis. Chest. 2014;146(1):142–151. doi:10.1378/chest.13-1926
10. Eakin MN, Riekert KA. The impact of medication adherence on lung health outcomes in cystic fibrosis. Curr Opin Pulm Med. 2013;19(6):687–691. doi:10.1097/MCP.0b013e3283659f45
11. Marciel KK, Saiman L, Quittell LM, Dawkins K, Quittner AL. Cell phone intervention to improve adherence: cystic fibrosis care team, patient, and parent perspectives. Pediatr Pulmonol. 2010;45(2):157–164. doi:10.1002/ppul.21164
12. Duff AJA, Latchford GJ. Motivational interviewing for adherence problems in cystic fibrosis. Pediatr Pulmonol. 2010;45(3):211–220. doi:10.1002/ppul.21103
13. Savage E, Beirne PV, Ni Chroinin M, Duff A, Fitzgerald T, Farrell D. Self-management education for cystic fibrosis. Cochrane Database Syst Rev. 2014;2014(9):CD007641. doi:10.1002/14651858.CD007641.pub3
14. Hind D, Drabble SJ, Arden MA, et al. Supporting medication adherence for adults with cystic fibrosis: a randomised feasibility study. BMC Pulm Med. 2019;19(1):77. doi:10.1186/s12890-019-0834-6
15. Quittner AL, Eakin MN, Alpern AN, et al. Clustered randomized controlled trial of a clinic-based problem-solving intervention to improve adherence in adolescents with cystic fibrosis. J Cyst Fibros. 2019;18(6):879–885. doi:10.1016/j.jcf.2019.05.004
16. Arden MA, Hutchings M, Whelan P, et al. Development of an intervention to increase adherence to nebuliser treatment in adults with cystic fibrosis: CFHealthHub. Pilot Feasibility Stud. 2021;7(1):1. doi:10.1186/s40814-020-00739-2
17. Brett J, Staniszewska S, Mockford C, et al. A systematic review of the impact of patient and public involvement on service users, researchers and communities. Patient. 2014;7(4):387–395. doi:10.1007/s40271-014-0065-0
18. Domecq JP, Prutsky G, Elraiyah T, et al. Patient engagement in research: a systematic review. BMC Health Serv Res. 2014;14:89. doi:10.1186/1472-6963-14-89
19. Carman KL, Dardess P, Maurer M, et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Aff Proj Hope. 2013;32(2):223–231. doi:10.1377/hlthaff.2012.1133
20. Hollin IL, Donaldson SH, Roman C, et al. Beyond the expected: identifying broad research priorities of researchers and the cystic fibrosis community. J Cyst Fibros. 2019;18(3):375–377. doi:10.1016/j.jcf.2018.11.010
21. Hempstead SE, Fredkin K, Hovater C, Naureckas ET. Patient and family participation in clinical guidelines development: the cystic fibrosis foundation experience. J Particip Med. 2020;12(3):e17875. doi:10.2196/17875
22. Pougheon Bertrand D, Minguet G, Gagnayre R, Lombrail P. Lessons from patient and parent involvement (P&PI) in a quality improvement program in cystic fibrosis care in France. Orphanet J Rare Dis. 2018;13(Suppl 1):19. doi:10.1186/s13023-017-0751-9
23. Sabadosa KA, Batalden PB. The interdependent roles of patients, families and professionals in cystic fibrosis: a system for the coproduction of healthcare and its improvement. BMJ Qual Saf. 2014;23(Suppl 1):i90–94. doi:10.1136/bmjqs-2013-002782
24. INVOLVE. What is public involvement in research? https://www.invo.org.uk/find-out-more/what-is-public-involvement-in-research-2/.
25. Slattery P, Saeri AK, Bragge P. Research co-design in health: a rapid overview of reviews. Health Res Policy Syst. 2020;18(1):17. doi:10.1186/s12961-020-0528-9
26. Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engage. 2017;3:13. doi:10.1186/s40900-017-0062-2
27. de Gaulejac V. On the origins of clinical sociology in france: some milestones. In: Fritz JM, editor. International Clinical Sociology. Springer; 2008:54–71. doi:10.1007/978-0-387-73827-7_5
28. Fritz JM, Clark EJ. Overview of the field: definitions and history. Sociol Pract. 1989;7:9–14.
29. Wirth L. Clinical sociology. Am J Sociol. 1931;37(1):49–66. doi:10.1086/215618
30. Rhéaume J. Community development and empowerment: a clinical sociology perspective. In: Fritz JM, Rhéaume J, editors. Community Intervention: Clinical Sociology Perspectives. Clinical Sociology: Research and Practice. Springer; 2014:59–72. doi:10.1007/978-1-4939-0998-8_5
31. Garavaglia L, Duncan C, Toucheque M, Farley A, Moffett KS. A quality improvement initiative to improve patient adherence to vitamin supplementation in cystic fibrosis. J Pediatr Gastroenterol Nutr. 2017;64(2):292–295. doi:10.1097/MPG.0000000000001273
32. Downs JA, Roberts CM, Blackmore AM, Le Souëf PN, Jenkins SC. Benefits of an education programme on the self-management of aerosol and airway clearance treatments for children with cystic fibrosis. Chron Respir Dis. 2006;3(1):19–27. doi:10.1191/1479972306cd100oa
33. Jones S, Babiker N, Gardner E, et al. Promoting adherence to nebulized therapy in cystic fibrosis: poster development and a qualitative exploration of adherence. Patient Prefer Adherence. 2015;9:1109–1120. doi:10.2147/PPA.S82896
34. Narayan O, Davies S, Tibbins C, Rees JM, Lenney W, Gilchrist FJ. Developing a handheld record for patients with cystic fibrosis. Patient Relat Outcome Meas. 2015;6:225–228. doi:10.2147/PROM.S86298
35. Chrysochoou EA, Hatziagorou E, Kirvassilis F, Tsanakas J. Telephone monitoring and home visits significantly improved the quality of life, treatment adherence and lung function in children with cystic fibrosis. Acta Paediatr Oslo Nor. 2017;106(11):1882. doi:10.1111/apa.13996
36. Morton RW, Elphick HE, Edwards E, Daw WJ, West NS. Investigating the feasibility of text message reminders to improve adherence to nebulized medication in children and adolescents with cystic fibrosis. Patient Prefer Adherence. 2017;11:861–869. doi:10.2147/PPA.S123723
37. Knudsen KB, Pressler T, Mortensen LH, et al. Coach to cope: feasibility of a life coaching program for young adults with cystic fibrosis. Patient Prefer Adherence. 2017;11:1613–1623. doi:10.2147/PPA.S141267
38. Shakkottai A, Kaciroti N, Kasmikha L, Nasr SZ. Impact of home spirometry on medication adherence among adolescents with cystic fibrosis. Pediatr Pulmonol. 2018;53(4):431–436. doi:10.1002/ppul.23950
39. Cummings E, Hauser J, Cameron-Tucker H, et al. Enhancing self-efficacy for self-management in people with cystic fibrosis. Stud Health Technol Inform. 2011;169:33–37.
40. Gur M, Nir V, Teleshov A, et al. The use of telehealth (text messaging and video communications) in patients with cystic fibrosis: a pilot study. J Telemed Telecare. 2017;23(4):489–493. doi:10.1177/1357633X16649532
41. David V, Iguenane J, Greffier C, Gagnayre R, Ravilly S. Groupe de travail éducation thérapeutique et mucoviscidose (GÉTHEM). Le conducteur pédagogique: une aide pour mener des séances d’éducation thérapeutique [Working group on therapeutic education and cystic fibrosis (GETHEM). The educational guide: an aid for conducting therapeutic education sessions]. Rev Mal Respir. 2008;25(10):1322–1325. French. doi:10.1016/S0761-8425(08)75096-4
42. George M, Rand-Giovannetti D, Eakin MN, Borrelli B, Zettler M, Riekert KA. Perceptions of barriers and facilitators: self-management decisions by older adolescents and adults with CF. J Cyst Fibros. 2010;9(6):425–432. doi:10.1016/j.jcf.2010.08.016
43. Riekert KA, Eakin MN, Bilderback A, Ridge AK, Marshall BC. Opportunities for cystic fibrosis care teams to support treatment adherence. J Cyst Fibros. 2015;14(1):142–148. doi:10.1016/j.jcf.2014.10.003
44. Jouet E, Flora LG, Las Vergnas O. Construction et reconnaissance des savoirs expérientiels des patients [Construction and recognition of patients' experiential knowledge]. Prat Form. 2010;58–59. French.
45. Richards T, Montori VM, Godlee F, Lapsley P, Paul D. Let the patient revolution begin. BMJ. 2013;346:f2614. doi:10.1136/bmj.f2614
46. Kitzinger J. The methodology of Focus Groups: the importance of interaction between research participants. Sociol Health Illn. 1994;16(1):103–121. doi:10.1111/1467-9566.ep11347023
47. Krueger R. Moderating Focus Groups. Sage Publications; 1998. doi:10.4135/9781483328133
48. Rowbotham NJ, Smith S, Leighton PA, et al. The top 10 research priorities in cystic fibrosis developed by a partnership between people with CF and healthcare providers. Thorax. 2018;73(4):388–390. doi:10.1136/thoraxjnl-2017-210473
49. Wildman MJ, Hoo ZH. Moving cystic fibrosis care from rescue to prevention by embedding adherence measurement in routine care. Paediatr Respir Rev. 2014;15(Suppl 1):16–18. doi:10.1016/j.prrv.2014.04.007
50. Geller DE, Madge S. Technological and behavioral strategies to reduce treatment burden and improve adherence to inhaled antibiotics in cystic fibrosis. Respir Med. 2011;105(Suppl 2):S24–S31. doi:10.1016/S0954-6111(11)70024-5
51. Thee S, Stahl M, Fischer R, et al. A multi-centre, randomized, controlled trial on coaching and telemonitoring in patients with cystic fibrosis: conneCT CF. BMC Pulm Med. 2021;21(1):131. doi:10.1186/s12890-021-01500-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.