Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
A Nurse-Guided, Family-Involved Individualized Perioperative Management Multidisciplinary Team Model in Older Patients Underwent Cardiac Surgery
Authors Cao M, Wang T ![]() , Tang Y, Wang J
, Tang Y, Wang J ![]() , Jin S
, Jin S
Received 16 September 2025
Accepted for publication 20 January 2026
Published 24 January 2026 Volume 2026:19 568010
DOI https://doi.org/10.2147/JMDH.S568010
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Miaomiao Cao,1 Tingting Wang,2 Yangchen Tang,3 Juan Wang,3 Song Jin3
1Department of Cardiac Surgery, the First Affiliated Hospital of USTC, Hefei, 230001, People’s Republic of China; 2Department of Cardiology, the First Affiliated Hospital of USTC, Hefei, 230001, People’s Republic of China; 3Department of Geriatrics, the First Affiliated Hospital of USTC, Hefei, 230001, People’s Republic of China
Correspondence: Song Jin, Department of Geriatrics, the First Affiliated Hospital of USTC, No. 1, Tianehu Road, Zhengwu District, Hefei, Anhui, 230001, People’s Republic of China, Tel +86-15395014716, Email [email protected]
Introduction: This study evaluated a novel multidisciplinary team (MDT) approach—integrating nurse guidance, family involvement, and individualized perioperative care—on outcomes in older cardiac surgery patients.
Methods: A retrospective analysis included 198 patients aged ≥ 60 years (99 conventional care, 99 MDT) from November 2021 to January 2024. Outcomes included pneumonia, delirium, functional recovery (Barthel Index), and hospitalization metrics.
Results: : Baseline characteristics were comparable. The MDT group had significantly shorter ICU stay (2.5± 1.9 vs 3.7± 4.8 days, p=0.019) and lower pneumonia incidence (29.3% vs 60.6%, p< 0.001). Total hospital stay and delirium rates did not differ significantly, but the MDT group showed a trend toward greater functional improvement (Barthel change: 20.6± 13.9 vs 15.6± 22.6).
Conclusion: The MDT model significantly improved critical postoperative outcomes, notably reducing ICU stay and pneumonia. These results advocate for nurse-led, family-centered multidisciplinary care in geriatric surgery, warranting further prospective validation.
Keywords: nursing, older adults, multidisciplinary team, perioperative, cardiac surgery
Introduction
Aging is a significant risk factor for adverse surgical outcomes, primarily due to the comorbidities often associated with it, such as frailty, type 2 diabetes mellitus, and hypertension,1,2 and the risks related to cardiac surgery.3,4 Advancements in surgical techniques and myocardial protection have reduced mortality related to cardiopulmonary bypass and anesthesia, thereby enabling older adult patients to undergo cardiac surgery. A Germany survey found that the average age of cardiac surgery patients increased from 55.8 years in 1990 to 68.8 years in 2007, with 9.8% of the surgical population being aged between 80 and 90 years.5
Although the success and postoperative survival rates for older adult patients undergoing cardiac surgery have significantly improved, 20% to 40% of these patients experience complications such as frailty, delirium, and infection during hospitalization. These complications often result in a decline in physical function and severely impact long-term prognosis.6 To mitigate these risks, multidisciplinary team (MDT) approaches have been increasingly adopted. MDTs bring together cardiac surgeons, cardiologists, anesthesiologists, geriatricians, and nurses to jointly assess patients and create integrated perioperative management plans.7,8 Such nursing models are highly relevant since many complications of cardiac surgery tend to occur after surgery.9,10 Nurses play a central role in perioperative care because of their frequent contact with patients and families, enabling them to provide ongoing assessment, communication, and individualized support. A nurse-led MDT model has shown benefits in older adults undergoing mitral valve surgery,11 but their families were not actively involved. The potential value of a nurse-guided, family-involved individualized perioperative management MDT model in older adult patients who underwent cardiac surgery is unknown. This study aimed to evaluate the MDT nurse-guided, patient- and family-involved, individualized perioperative management model on the outcomes of older patients who had undergone cardiac surgery.
Materials and Methods
Study Design and Populations
This retrospective study enrolled patients who underwent open-heart surgery in the author’s hospital. Based on the hospital nursing quality improvement project’s implementation timeframe, the study population was divided into two groups: a conventional group and an MDT group. The conventional group enrolled from November 2021 to July 2022, while the MDT group enrolled from November 2022 to January 2024. The study was approved by the Ethics Committee of the author’s hospital. The requirement for individual informed consent was waived by the committee because of the retrospective nature of the study.
The inclusion criteria were 1) patients underwent open-heart surgery, 2) aged ≥60 years, 3) no delirium at admission, and 4) a hospital stay of > 2 days. The exclusion criteria were 1) patients with unstable vital signs, 2) those with severe aphasia or significant communication barriers, 3) patients with severe mental disorders or associated with irritability and dangerous behaviors, 4) patients requiring respiratory and contact isolation due to airborne transmission (eg, tuberculosis, influenza, COVID-19, etc)., or 5) patients with severe immunodeficiency requiring protective isolation (eg, severe neutropenia). Patients in conventional group received the standard perioperative management model of cardiac surgery, which involved three-tier ward rounds by the cardiac surgery medical team and daily nursing rounds led by the head nurse of the ward, who carried out perioperative nursing care. A comprehensive geriatric assessment was not part of the routine care for such patients.
The MDT group included cardiac surgeons, geriatricians, cardiac surgery nurses, geriatric nurses, clinical nutritionists, rehabilitation therapists, and family members or caregivers. The trained nurses were responsible for conducting the comprehensive geriatric assessments upon patient admission, including the Barthel Index, the Sleep Status Self-Rating Scale (SSRS), the Hospital Anxiety and Depression Scale (HAD), the Nutrition Risk Screening (NRS2002), the Frail Scale, the Mini-Cog, and the Numerical Pain Rating Scale (NPRS) and assisted rehabilitation therapists and clinical nutritionists in implementing the individualized perioperative management plan developed by the MDT. Family members provided daily assistance with memory training and offer emotional support. The perioperative plans included orientation communication, cognitive maintenance, pain scoring, and maintaining regular bowel movements through dietary improvements or medication. The cardiac surgeons and geriatricians were focusing on maintaining internal environmental stability, managing polypharmacy, correcting hypoxia, and promptly treating infections. The assessments were performed postoperatively, on postoperative day 7, and at discharge.
Data Collection and Outcomes
All data used in this study were collected from the patients’ medical records, including demographic details, medical history and laboratory results.
The primary outcomes were the occurrence of major postoperative complications, including delirium and pneumonia. Delirium is an acute brain dysfunction primarily triggered by central nervous system diseases, drug overdose or withdrawal reactions, poisoning, metabolic disorders, and infections. Patients generally recover within a few hours to several days.12 The Barthel Index is a widely used tool to assess a patient’s ability to perform basic activities of daily living (ADLs).13 Pneumonia is an infection that inflames the air sacs (alveoli) in one or both lungs. The air sacs may fill with fluid or pus, causing symptoms such as cough, fever, chills, difficulty breathing, and chest pain.14 The secondary outcomes were intensive care unit (ICU) length of stay, total hospital length of stay, change in Barthel Index scores from admission to discharge.
Statistical Analysis
All data were processed and analyzed using SPSS 27 (IBM, Armonk, NY, USA). GraphPad Prism 10.1.2 (GraphPad Software Inc., San Diego, CA, USA) was used to plot the graphs. The continuous data was tested for normal distribution using the Kolmogorov–Smirnov test. They were expressed as means ± standard deviation (SD) or median (range) and analyzed using Student’s t-test or the Mann–Whitney U-test. The categorical data were presented as n (%) and analyzed using the chi-squared test. Two-sided P-values <0.05 were considered statistically significant.
Results
Basic Characteristics of the Patients
A total of 198 patients were included, with 99 patients in each group (Figure 1). There were no significant differences in age (70.80±3.83 years vs 70.17±5.20 years), male sex (73.74% vs 64.65%), or Comorbidity index (5.77±1.56 vs 5.79±1.62) between MDT group and convention group, but the conventional group had a lower level of education, with a higher proportion of illiteracy (39.39% vs 13.13%) compared with the MDT group. In addition, the patients in the conventional group had worse cardiac function, with a higher proportion of NYHA functional classes III and IV (67.72% vs 96.97%, P < 0.001). The MDT group had higher Barthel Index scores (86.77±8.82 vs 80.86±14.14, P < 0.001) and body mass index (BMI) (24.56±3.31 vs 23.56±2.95 kg/m2, P = 0.026) than the conventional group (Table 1).
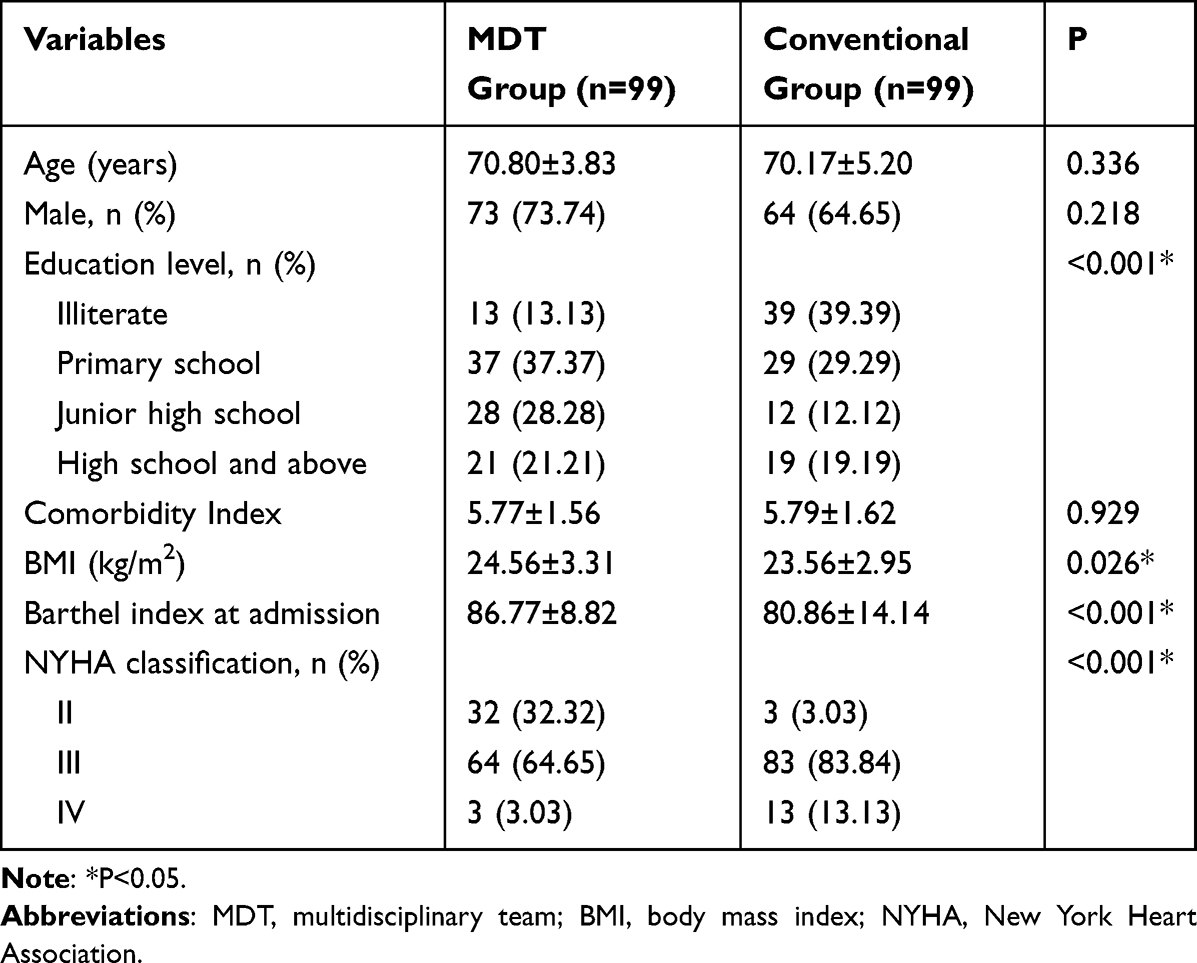 |
Table 1 Characteristics of the Patients |
 |
Figure 1 Flowchart for Screening Research Population. |
Preoperative Characteristics of the Patients
There were no significant differences between the two groups in creatinine (Cr) levels (85.17±50.74 vs 76.35±27.99 umol/L), alanine aminotransferase (ALT) levels (25.90±45.92 vs 26.03±26.40 IU/L), aspartate aminotransferase (AST) levels (28.33±23.12 vs 27.32±15.97 IU/L), left ventricular end-diastolic diameter (LV) (56.83±7.78 vs 56.64±8.18 mm), left atrial anteroposterior diameter (LA) (46.41±8.18 vs 44.62±8.05 mm), left ventricular ejection fraction (LVEF) (0.60±0.10 vs 0.59±0.11), N-terminal pro-brain natriuretic peptide (NT-proBNP) levels (1535.17±2932.08 vs 1960.30±3785.45 pg/mL), or EURO-score II (0.02±0.02 vs 0.03±0.02). On the other hand, the MDT group had significantly higher values for albumin (ALB) (38.50±3.74 vs 37.04±4.08 g/L, P = 0.009) and preoperative hemoglobin (Hb) (129.32±15.29 vs 121.92±16.49 g/L, P = 0.001) compared with the conventional group (Table 2).
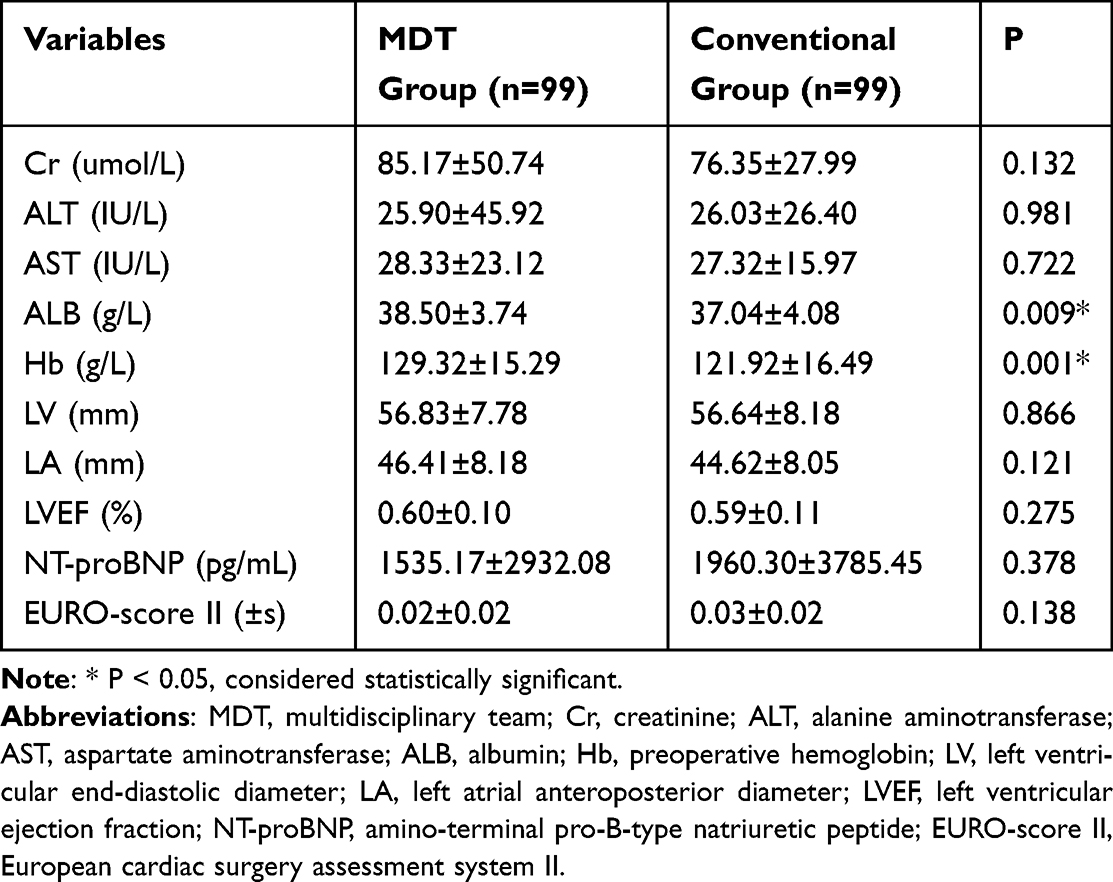 |
Table 2 Comparison of Preoperative Indicators |
There were no significant differences between groups in the types of surgery performed, with valve surgery (43.43% vs 36.36%) and coronary artery bypass grafting (CABG) (42.42% vs 52.53%) being the most common, cardiopulmonary bypass (54.55% vs 47.47%), and duration of surgery (5.15±1.29 vs 5.13±1.52 h) (Table 3).
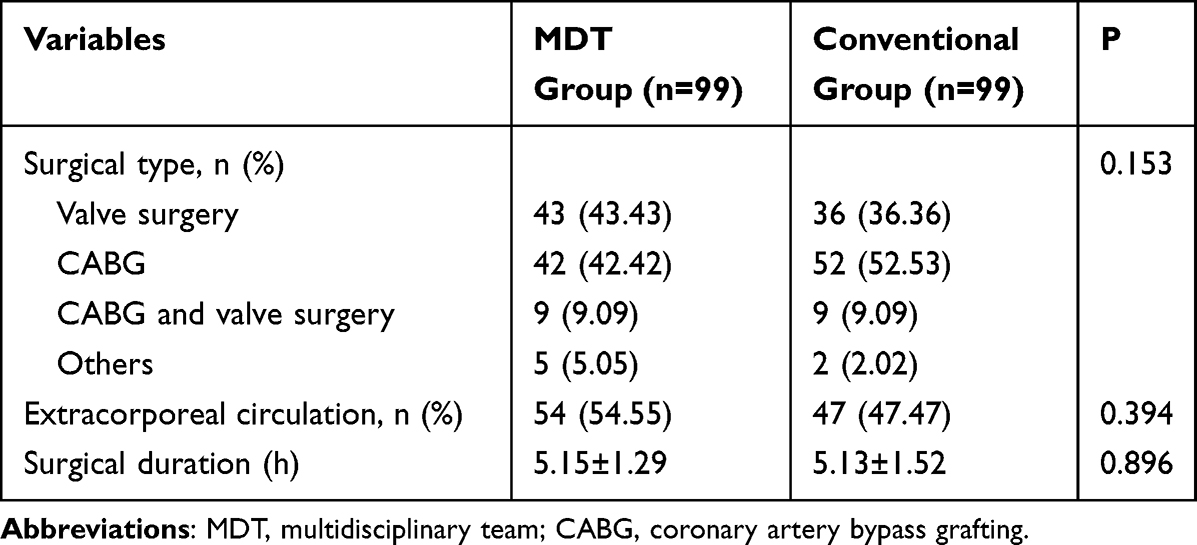 |
Table 3 Comparison of Surgical-Related Data |
Comprehensive Geriatric Assessment and Inpatient Outcomes
Only the patients in the MDT group received a comprehensive geriatric assessment. The individualized perioperative care plans were developed by the MDT based on the assessment results. As shown in Figure 2, the overall sleep quality of the MDT group was suboptimal, with a median score of 19. The anxiety and depression levels were moderate, with median scores of 2 (0, 5) and 3 (1, 6), respectively. Most patients had no significant nutritional risk, with an NRS2002 score of 2 (1, 2). The patients were not significantly frail preoperatively, with a median frailty score of 1 (0, 2). The cognitive function of the patients was relatively preserved, with a Mini-Cog score of 4 (3, 5). Postoperatively, patients exhibited significant pain, with a median pain score of 6 (6, 6). In the MDT group, 9 (9.09%) patients experienced anxiety, 16 (16.16%) had depression, 22 (22.22%) were at risk of malnutrition, 10 (10.10%) patients were frail, 58 (58.58%) were in the pre-frailty stage, and 20 (20.20%) had some degree of cognitive impairment (Figure 2).
 |
Figure 2 Boxplot of the overall sleep quality of the multidisciplinary treatment (MDT) group. |
No significant differences between the MDT and conventional groups in terms of length of hospital stay (29.31±9.84 vs 28.40±10.96 days), the incidence of delirium during hospitalization (22.22% vs 31.31%), or the difference in Barthel Index scores at discharge compared with admission (20.56±13.90 vs 15.59±22.55). Nevertheless, the study revealed that the MDT group had significantly shorter ICU stays (2.49±1.91 vs 3.73±4.79 days, P = 0.019) and a lower incidence of pneumonia (29.3% vs 60.6%, P < 0.001) compared with the conventional group (Table 4).
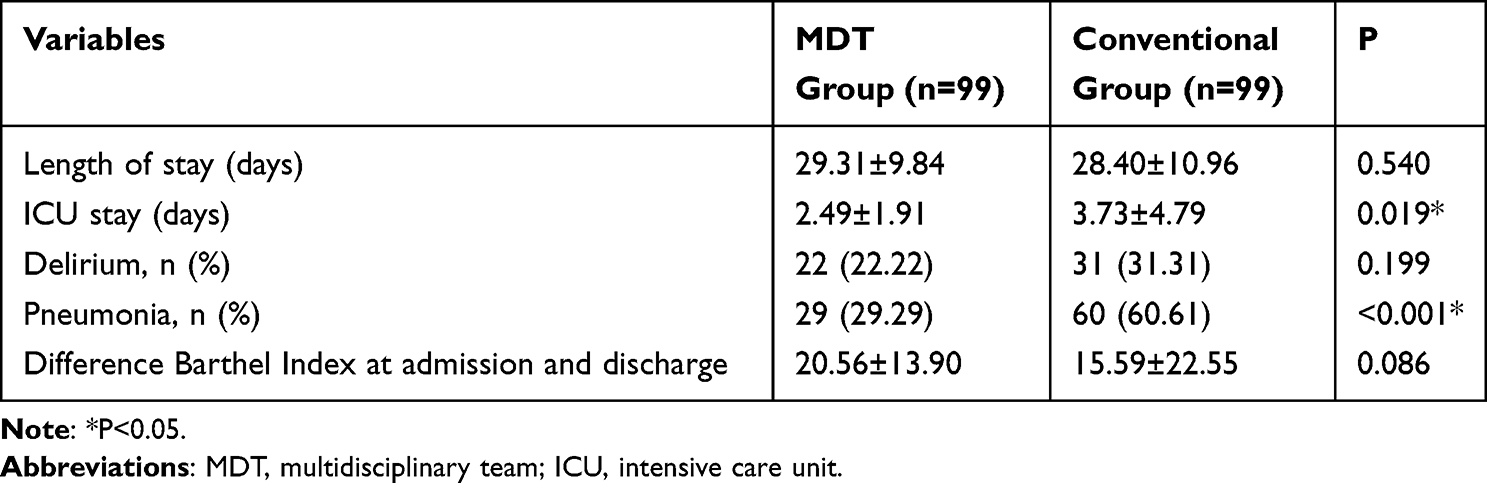 |
Table 4 Comparison of Hospital Outcomes |
Discussion
The study found that the MDT group had a significantly shorter ICU stay and a lower incidence of pneumonia compared to the conventional group. These findings suggest a potential association between MDT-supported perioperative care and improved short-term outcomes among older adults undergoing cardiac surgery.
The present study found that the average ICU stay for the MDT group was 2.49 ± 1.91 days, compared to 3.73 ± 4.79 days for the conventional group, with the difference being statistically significant. However, there were no significant differences in total hospital stays between the two groups. A small-scale study conducted in China (involving 76 patients) demonstrated that adjusting nursing plans based on the results of comprehensive geriatric assessments could reduce ICU stay by approximately 2 days and total hospital stay by about 5 days,15 supporting the present study regarding the ICU stay. The observed discrepancy in total hospital stay could be explained by differences in sample size and surgical procedures. Specifically, the previous study included 76 patients who underwent valve surgery and coronary artery bypass grafting, whereas the present study encompassed a broader range of surgical procedures. Additionally, a study of older patients who underwent cardiac surgery in Australia and New Zealand found that 95.6% of patients had an ICU stay of less than 7 days, with only 1.3% exceeding 14 days.16 The duration of ICU stay in the present study was similar.
In this study, postoperative delirium did not differ significantly between groups, while postoperative pneumonia occurred less frequently in the MDT cohort. A study conducted in Japan found that addressing potential delirium triggers and enhancing delirium prevention education reduced the incidence of postoperative delirium following cardiac surgery from 53.3% to 37.0%.17 This contrasts with the present study, which may be attributed to the inclusion of higher-risk delirium patients. Indeed, older adult patients undergoing cardiac surgery are more susceptible to delirium compared to those undergoing non-cardiac surgery. Furthermore, there are currently no standardized, effective protocols for the prevention of postoperative delirium.18
In terms of preventing postoperative pneumonia, the present study indicates that an enhanced nursing model may correlate with lower pneumonia rates following cardiac surgery, as supported by a previous study.19 The impact of ICU stay duration on the occurrence of postoperative pneumonia has been reported, with each day of ICU stay increasing the risk of pneumonia.20 The reduced incidence of postoperative pneumonia in the MDT group may be attributed to the standardized education provided to patients and patients’ care givers on preventing pulmonary infections during postoperative care, as well as to the closer assessments and monitoring conducted within the MDT framework. In future clinical practice, a more thorough evaluation of patients may be necessary, ensuring that both patients and their families are actively involved in implementing strategies to prevent postoperative complications under multidisciplinary guidance. A study conducted in resource-limited settings demonstrated that effective training significantly reduced the incidence of surgical site infections, central line-associated bloodstream infections, ventilator-associated pneumonia, and catheter-associated urinary tract infections.21 Each dollar invested could save $236 in infection-related costs.21 Similar studies have reported that preoperative exercise can improve the Barthel index,22 and strengthening cardiopulmonary reserve exercises19 can significantly reduce ICU stay duration, thereby decreasing the overall length of hospitalization.
The observed reductions in ICU length of stay and postoperative pneumonia incidence likely reflect the impact of the multidisciplinary team (MDT) intervention, given the stable hospital environment and absence of infectious disease outbreaks during the study period. The MDT approach, through structured pulmonary education, early mobilization, nutritional assessment, and close monitoring, aligns with established strategies known to improve postoperative recovery and prevent complications. While residual unmeasured confounding cannot be entirely excluded due to the before-after study design, these findings reinforce the potential clinical benefit of structured multidisciplinary care in enhancing postoperative outcomes.
Regarding postoperative pneumonia, the MDT model appeared effective in reducing its incidence. Mechanistically, this reduction may be attributed to several factors. Comprehensive assessments allowed for early identification of at-risk patients, prompting targeted interventions such as enhanced pulmonary care, patient mobilization, and standardized education for both patients and caregivers. Closer monitoring within the MDT framework facilitated timely recognition and management of complications. Previous studies have shown that each additional day of ICU stay increases the risk of pneumonia, emphasizing the importance of strategies that reduce ICU duration. Evidence from resource-limited settings also indicates that effective staff training and structured protocols can markedly reduce infections such as surgical site infections, central line-associated bloodstream infections, and ventilator-associated pneumonia, demonstrating both clinical and economic benefits.
The comprehensive assessment of older adult patients who underwent open-heart surgery revealed that all patients exhibited varying degrees of sleep disturbances, with a median self-reported sleep score of 19. Sleep disorders are highly prevalent among perioperative patients, particularly in older adults, and factors such as anxiety, depression, and unfamiliar hospital environments can exacerbate these conditions.23 Hedges et al found that 53% of patients who underwent coronary artery bypass surgery experienced sleep disorders preoperatively.24 In other non-cardiac surgeries, such as total hip replacement, the incidence of sleep disorders was reported to be 59%.25 The highest incidence of sleep disorders was observed in patients who underwent lower limb surgeries, with 89% of such patients affected, according to Kunze et al.26 Sleep disorders are therefore common among surgical patients and should be addressed to improve patient outcomes. In the present study, the proportions of patients with frailty, malnutrition risk, and cognitive decline were relatively low. The COVID-19 Vascular Service in Australia (COVER-AU) study conducted in Australia found that during the early stages of the COVID-19 pandemic, 22.1% of patients who underwent vascular surgery were frail, while only 12 patients (5.9%) who underwent cardiac aortic surgery were frail.27 Cognitive dysfunction in surgical patients can lead to increased postoperative complications, such as delirium. A retrospective study indicated that 18% of patients who underwent urological cancer surgery exhibited preoperative cognitive decline.28 A survey at the Department of Cardiothoracic Surgery of Karolinska University Hospital revealed that from 2013 to 2016, 15% of patients who underwent cardiac surgery experienced preoperative anxiety or depression.29 The rates were markedly lower in the MDT group in the present study, but those parameters were not systematically assessed in the conventional group, preventing conclusions about the effect of MDT.
Limitations
This study has several limitations. First, its before-after, non-randomized design is subject to temporal confounding and potential group incompatibility. Second, the retrospective nature may introduce information and selection bias, limiting causal inference. Third, although surgical principles were similar, procedural heterogeneity may have influenced outcomes. Fourth, some geriatric assessments (eg, frailty, cognition, and sleep) were systematically performed only in the MDT group, precluding direct baseline comparisons. Finally, the modest sample size limits generalizability, and larger multicenter studies are warranted to validate these findings.
Future research should address these methodological limitations. Cluster-randomized or parallel-group designs would reduce contamination in shared wards while allowing more rigorous evaluation of MDT effects. Prospective multicenter studies with stratified recruitment could improve comparability between cohorts and mitigate temporal confounding. Additionally, the development of modified geriatric assessment tools suitable for unstable or communication-impaired patients may allow future studies to include populations who were excluded in this analysis but who may potentially benefit from MDT care.
Conclusion
A nurse-guided, family-involved, individualized perioperative management strategy based on comprehensive geriatric assessment was associated with a shorter ICU stay duration and a lower incidence of postoperative pneumonia in older adults undergoing cardiac surgery. This approach may offer potential benefits for this patient population and may be particularly relevant in the context of an aging population and the projected increase in the incidence and prevalence of cardiovascular disease. Further studies are needed to optimize the MDT evaluation and enhance the effectiveness of this strategy.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (2024-RE-391). The study was approved by the Institutional Review Board, and the requirement for informed consent was waived due to the retrospective design. All patient data were anonymized and treated confidentially in accordance with institutional and international guidelines. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ho VP, Schiltz NK, Reimer AP, Madigan EA, Koroukian SM. High-risk comorbidity combinations in older patients undergoing emergency general surgery. J Am Geriatr Soc. 2019;67(3):503–10. doi:10.1111/jgs.15682
2. Mistry PK, Gaunay GS, Hoenig DM. Prediction of surgical complications in the elderly: can we improve outcomes? Asian J Urol. 2017;4(1):44–49. doi:10.1016/j.ajur.2016.07.001
3. Lemaire A, Soto C, Salgueiro L, Ikegami H, Russo MJ, Lee LY. The impact of age on outcomes of coronary artery bypass grafting. J Cardiothorac Surg. 2020;15(1):158. doi:10.1186/s13019-020-01201-3
4. Afilalo J, Mottillo S, Eisenberg MJ, et al. Addition of frailty and disability to cardiac surgery risk scores identifies elderly patients at high risk of mortality or major morbidity. Circ Cardiovasc Qual Outcomes. 2012;5(2):222–228. doi:10.1161/CIRCOUTCOMES.111.963157
5. Friedrich I, Simm A, Kotting J, Tholen F, Fischer B, Silber RE. Cardiac surgery in the elderly patient. Dtsch Arztebl Int. 2009;106(25):416–422. doi:10.3238/arztebl.2009.0416
6. Morisawa T, Saitoh M, Otsuka S, et al. Association between hospital-acquired functional decline and 2-year readmission or mortality after cardiac surgery in older patients: a multicenter, prospective cohort study. Aging Clin Exp Res. 2023;35(3):649–657. doi:10.1007/s40520-022-02335-1
7. Pozzi M, Mariani S, Scanziani M, et al. The frail patient undergoing cardiac surgery: lessons learned and future perspectives. Front Cardiovasc Med. 2023;10:1295108. doi:10.3389/fcvm.2023.1295108
8. Smoor RM, van Dongen EPA, Daeter EJ, et al. The association between preoperative multidisciplinary team care and patient outcome in frail patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2024;168(2):608–616e605. doi:10.1016/j.jtcvs.2023.05.037
9. Mali S, Haghaninejad H. Pulmonary complications following cardiac surgery. Arch Med Sci Atheroscler Dis. 2019;4:e280–e285. doi:10.5114/amsad.2019.91432
10. Song X, Wang H, Kashani KB, Wang C. Extracorporeal membrane oxygenation using a modified cardiopulmonary bypass system. J Transl Int Med. 2022;10(2):175–177. doi:10.2478/jtim-2022-0015
11. Li S, Zhang H, Chen M, Wang Z, Lin Y. A multidisciplinary team nursing model in the treatment of patients undergoing transapical mitral valve clamping: a prospective study. J Cardiothorac Surg. 2021;16(1):203. doi:10.1186/s13019-021-01588-7
12. Sadeghirad B, Dodsworth BT, Schmutz Gelsomino N, et al. Perioperative factors associated with postoperative delirium in patients undergoing noncardiac surgery: an individual patient data meta-analysis. JAMA Netw Open. 2023;6(10):e2337239. doi:10.1001/jamanetworkopen.2023.37239
13. Coyan GN, Chin H, Shah A, et al. Charlson comorbidity index is associated with longer-term mortality and re-admissions following coronary artery bypass grafting. J Surg Res. 2022;275:300–307. doi:10.1016/j.jss.2022.02.012
14. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
15. Lu W. Study on the impact of geriatric comprehensive assessment nursing on postoperative complications and rehabilitation in cardiac surgery patients. Contemporary Nurse. 2023;6(30):77–79.
16. Shah V, Ahuja A, Kumar A, et al. Outcomes of prolonged ICU stay for patients undergoing cardiac surgery in Australia and New Zealand. J Cardiothorac Vasc Anesth. 2022;36(12):4313–4319. doi:10.1053/j.jvca.2022.08.026
17. Enomoto K, Kosaka S, Kimura T, et al. Prevention of postoperative delirium after cardiovascular surgery: a team-based approach. J Thorac Cardiovasc Surg. 2023;165(5):1873–1881e1872. doi:10.1016/j.jtcvs.2021.07.027
18. Mattimore D, Fischl A, Christophides A, et al. Delirium after cardiac surgery-a narrative review. Brain Sci. 2023;13(12):1682. doi:10.3390/brainsci13121682
19. Alwekhyan SA, Alshraideh JA, Yousef KM, Hayajneh F. Nurse-guided incentive spirometry use and postoperative pulmonary complications among cardiac surgery patients: a randomized controlled trial. Int J Nurs Pract. 2022;28(2):e13023. doi:10.1111/ijn.13023
20. Thanavaro J, Taylor J, Vitt L, Guignon MS, Thanavaro S. Predictors and outcomes of postoperative respiratory failure after cardiac surgery. J Eval Clin Pract. 2020;26(5):1490–1497. doi:10.1111/jep.13334
21. Singh S, Kumar RK, Sundaram KR, Kanjilal B, Nair P. Improving outcomes and reducing costs by modular training in infection control in a resource-limited setting. Int J Qual Health Care. 2012;24(6):641–648. doi:10.1093/intqhc/mzs059
22. Zheng YT, Zhang JX. Preoperative exercise and recovery after cardiac surgery: a meta-analysis. BMC Cardiovasc Disord. 2020;20(1):2. doi:10.1186/s12872-019-01308-z
23. Lin D, Huang X, Sun Y, Wei C, Wu A. Perioperative Sleep Disorder: a Review. Front Med. 2021;8:640416. doi:10.3389/fmed.2021.640416
24. Hedges C, Redeker NS. Comparison of sleep and mood in patients after on-pump and off-pump coronary artery bypass surgery. Am J Crit Care. 2008;17(2):
25. Clarkson SJ, Yayac MF, Rondon AJ, Smith BM, Purtill JJ. Melatonin does not improve sleep quality in a randomized placebo-controlled trial after primary total joint arthroplasty. J Am Acad Orthop Surg. 2022;30(2):e287–e294. doi:10.5435/JAAOS-D-21-00243
26. Kunze KN, Farivar D, Wu K, et al. Patients with chronic foot and ankle conditions experience significant improvements in sleep quality following surgical intervention. Foot Ankle Spec. 2023;16(5):470–475. doi:10.1177/19386400211009365
27. Australian New Zealand Vascular Trial Network; Aitken SJ, Allard B, Altaf N, et al. Frail patients having vascular surgery during the early COVID-19 pandemic experienced high rates of adverse perioperative events and amputation. ANZ J Surg. 2022;92(9):2305–2311. doi:10.1111/ans.17810
28. Yajima S, Nakanishi Y, Matsumoto S, et al. The Mini-Cog: a simple screening tool for cognitive impairment useful in predicting the risk of delirium after major urological cancer surgery. Geriatr Gerontol Int. 2022;22(4):319–324. doi:10.1111/ggi.14367
29. Stenman M, Sartipy U. Depression Screening in Cardiac Surgery Patients. Heart Lung Circ. 2019;28(6):953–958. doi:10.1016/j.hlc.2018.04.298
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Importance-Performance Analysis of Patient-Safety Nursing in the Operating Room: A Cross-Sectional Study
Shin J, Kim NY
Risk Management and Healthcare Policy 2024, 17:715-725
Published Date: 26 March 2024
Risk Factors and Predictive Model for Stress Hyperglycemia After Cardiac Surgery in Non-Diabetic Patients
Zhang M, Wu J, Wang L, Huang H, Duan H, Xue F
Journal of Multidisciplinary Healthcare 2025, 18:2247-2262
Published Date: 22 April 2025