Back to Journals » Drug Design, Development and Therapy » Volume 13
A nucleoside-sparing regimen of dolutegravir plus ritonavir-boosted atazanavir in HIV-1-infected patients with virological failure: the DOLATAV study
Authors Spagnuolo V ![]() , Galli L
, Galli L ![]() , Poli A, Bigoloni A, Fumagalli L, Gianotti N
, Poli A, Bigoloni A, Fumagalli L, Gianotti N ![]() , Nozza S, Ferrari D, Locatelli M, Lazzarin A, Castagna A
, Nozza S, Ferrari D, Locatelli M, Lazzarin A, Castagna A
Received 24 October 2018
Accepted for publication 9 January 2019
Published 24 January 2019 Volume 2019:13 Pages 477—479
DOI https://doi.org/10.2147/DDDT.S192124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Vincenzo Spagnuolo,1,2 Laura Galli,2 Andrea Poli,2 Alba Bigoloni,2 Luca Fumagalli,2 Nicola Gianotti,2 Silvia Nozza,2 Davide Ferrari,3 Massimo Locatelli,3 Adriano Lazzarin,2 Antonella Castagna1,2
1Vita-Salute San Raffaele University, Faculty of Medicine and Surgery, Milan, Italy; 2Clinic of Infectious Diseases, Istituto di Ricerca e Cura a Carattere Scientifico (IRCCS) San Raffaele Scientific Institute, Milan, Italy; 3Laboratory Medicine Service, IRCCS San Raffaele Hospital, Milan, Italy
Introduction
The increased exposure of dolutegravir (DTG) when given with atazanavir/ritonavir (ATV/r), as well as the acceptable safety profile, may suggest the use of this combination as a two-drug regimen both in virologically suppressed and treatment-failing subjects.1–5
This nucleoside reverse transcriptase inhibitors (NRTIs)-sparing regimen, characterized by a high genetic barrier, may represent an option in patients who have failed previous regimens and developed pharmacoresistance mutations to NRTIs and nonnucleoside reverse transcriptase inhibitors (NNRTIs).
However, no data on DTG plus boosted ATV in patients with virological failure are currently available.
Therefore, the aim of the DOLATAV study was to investigate the efficacy, safety, and pharmacokinetics of ATV/r 300/100 mg once-daily plus DTG 50 mg once-daily
Introduction
The increased exposure of dolutegravir (DTG) when given with atazanavir/ritonavir (ATV/r), as well as the acceptable safety profile, may suggest the use of this combination as a two-drug regimen both in virologically suppressed and treatment-failing subjects.1–5
This nucleoside reverse transcriptase inhibitors (NRTIs)-sparing regimen, characterized by a high genetic barrier, may represent an option in patients who have failed previous regimens and developed pharmacoresistance mutations to NRTIs and non-nucleoside reverse transcriptase inhibitors (NNRTIs).
However, no data on DTG plus boosted ATV in patients with virological failure are currently available.
Therefore, the aim of the DOLATAV study was to investigate the efficacy, safety, and pharmacokinetics of ATV/r 300/100 mg once-daily plus DTG 50 mg once-daily in treatment-failing HIV-1-infected patients.
Methods
DOLATAV is a prospective, single-arm, monocentric, open label, pilot study (NCT02542852). It was approved by the Ethics Committee of the San Raffaele Scientific Institute, conducted in accordance with the Declaration of Helsinki, and all participants in it signed the study’s informed consent at screening. The study was conducted on HIV-infected subjects with virological failure, defined as two consecutive viral loads ≥200 copies/mL, without a history of ATV failure and ATV resistance and without any exposure to integrase strand transfer inhibitors.
Patients were assessed at screening, baseline (ATV/r plus DTG initiation), day 8, weeks 4, 8, 12, 16, and 24 (or study discontinuation).
Treatment failure was defined as virological failure (confirmed rebound in plasma HIV-RNA levels ≥50 copies/mL after prior confirmed suppression to <50 copies/mL or a plasma HIV-1 RNA level ≥50 copies/mL at week 24) or study discontinuation for any reason. Ctrough of ATV and DTG were evaluated at each time-point after baseline by sensitive liquid chromatography tandem mass spectrometry.
Results were described as median (IQR) or frequency (%). The ANOVA for repeated measures was used to evaluate differences in laboratory parameters over time. Significant changes at each time-point were assessed by the Wilcoxon signed-rank test; the Bonferroni correction was applied.
Results
We screened 16 subjects (5 screening failures for HIV-RNA <200 copies/mL, 1 withdrawal of consent) and enrolled 10 participants with a median age of 47 (42–50) years. Patients had a known HIV infection of 14.4 (11.7–28.9) years and 10.7 (5.1–18.0) years of antiretroviral therapy exposure. Sixty percent of patients were on a failing boosted protease inhibitor (PI)-based regimen and 40% on a NNRTIs-based treatment; HIV-RNA was 2.77 (2.09–2.98) log10 copies/mL at baseline. In addition, 80% of the patients had NRTIs or NNRTIs mutations and one subject showed archived PIs mutations at HIV genotype screening (Table 1).
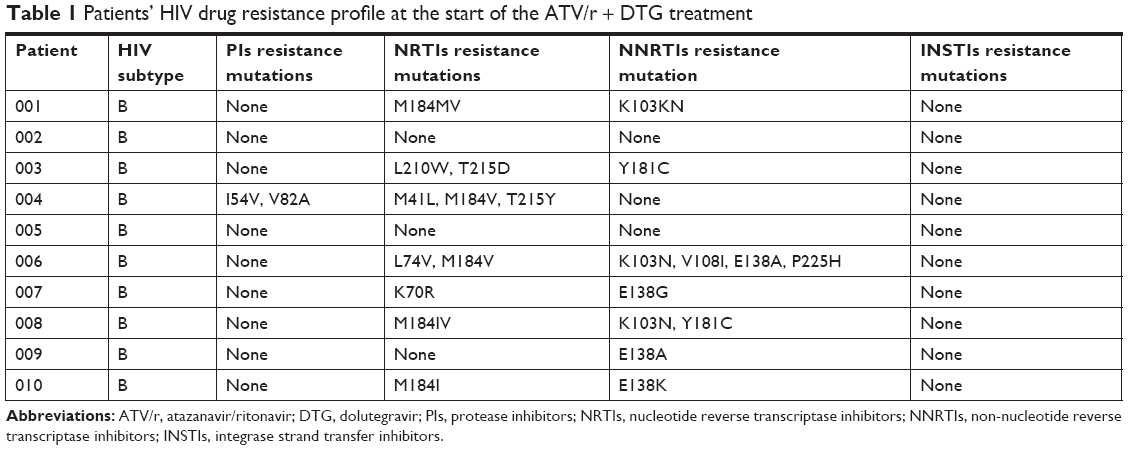 | Table 1 Patients’ HIV drug resistance profile at the start of the ATV/r + DTG treatment |
At week 24, the proportion of virological efficacy (HIV-RNA <50 copies/mL) was 100% and the corresponding 95%CI extended from 68% to 100%, in both the intention-to-treat and on-treatment analyses. None of the enrolled participants discontinued the treatment regimen.
Six clinical adverse events (AEs) occurred in five participants: three subjects experienced a drug-related clinical event (scleral jaundice) of grade 2 (one participant) or grade 1 (two participants); three participants had non-drug related AEs (a grade-1 pharyngitis, a grade-2 subcutaneous abscess and a grade-2 accidental nasal fracture). No clinical event was serious and no neuropsychiatric events were reported.
A significant increase of total bilirubin (+1.97 mg/dL [+0.77; +3.44]; P=0.004) and a marginally significant decline in eGFR (−9.5 mL/min/1.73 m2 [−16; −2]; P=0.084) were observed during the treatment with DTG plus ATV/r.
No significant variations during follow-up were found in immunological, hepatic and hematological parameters or lipid and glucose levels.
ATV and DTG plasma concentrations were stable during follow-up as shown in Table 2.
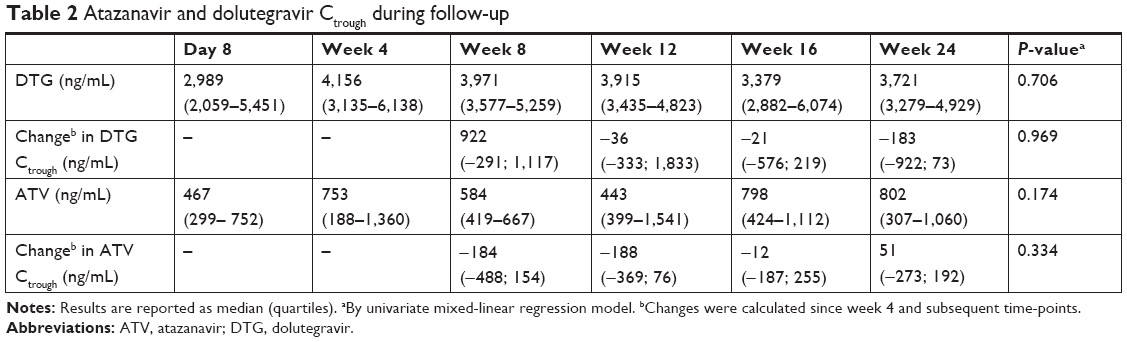 | Table 2 Atazanavir and dolutegravir Ctrough during follow-up |
Discussion and conclusion
To our knowledge, our study investigated for the first time the association of DTG plus ATV/r as rescue therapy in patients with virological failure. However, our trial has several limitations, such as the monocentric and single arm design of the study. In addition, given the small number of participants, mainly due to the low number of observed virological failures in our cohort during the enrollment period, another clear limitation of this study is the low statistical power.
In conclusion, this pilot study showed that in HIV-infected subjects with virological failure, a long antiretroviral therapy exposure and resistance to NRTIs and NNRTIs, a dual regimen with DTG plus ATV/r may represent a novel and well-tolerated therapeutic option with excellent efficacy and a high genetic barrier.
Data sharing statement
Individual participant data that underlie the results reported in this article, after de-identification (text and tables) will be shared with researchers who provide a proposal, beginning 3 months and ending 5 years after article publication. Proposals may include individual participant data meta-analysis and should be directed to [email protected] to get access to the data. The study protocol and the statistical analysis plan are available at https://clinicaltrials.gov/ct2/show/NCT02542852.
Acknowledgments
The authors should like to thank Editage for editing and reviewing this manuscript for English language usage. Bristol–Myers Squibb supported the study and provided ATV/r; ViiV Healthcare provided DTG.
Author contributions
VS conceived the study, followed the patients and wrote the first draft of the manuscript; AC conceived the study and reviewed and edited the manuscript; LG and AP performed statistical analyses and reviewed and edited the manuscript; DF and ML performed pharmacokinetic analyses and reviewed and edited the manuscript; AB, NG, SN, LF, and AL followed the patients and reviewed and edited the manuscript. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
AC, AL, SN, and NG have received consultancy payments and speaking fee from Bristol–Myers Squibb, Gilead, ViiV Healthcare, Merck Sharp Dohme, Janssen. VS has received consultancy payments and speaking fee from Gilead, ViiV Healthcare and Janssen-Cilag. The authors report no other conflicts of interest in this work.
References
Cottrell ML, Hadzic T, Kashuba AD. Clinical pharmacokinetic, pharmacodynamic and drug-interaction profile of the integrase inhibitor dolutegravir. Clin Pharmacokinet. 2013;52(11):981–994. | ||
Song I, Borland J, Chen S, et al. Effect of atazanavir and atazanavir/ritonavir on the pharmacokinetics of the next-generation HIV integrase inhibitor, S/GSK1349572. Br J Clin Pharmacol. 2011;72(1):103–108. | ||
Eron JJ, Clotet B, Durant J, et al. Safety and efficacy of dolutegravir in treatment-experienced subjects with raltegravir-resistant HIV type 1 infection: 24-week results of the Viking study. J Infect Dis. 2013;207(5):740–748. | ||
Lanzafame M, Lattuada E, Nicolè S, et al. Dolutegravir 50mg thrice weekly plus atazanavir 400mg daily in a long-term virologically suppressed HIV-infected patient. Int J STD AIDS. 2017;28(7):726–728. | ||
Pontali E, Torresin AA, Cenderello G, et al. Low dose of unboosted atazanavir plus dolutegravir as simplification strategy for HIV-infected patients receiving antiretroviral therapy. 9th Italian conference on AIDS and antiviral research, 2017, June 12–14; Siena, Italy, poster 101. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.