Back to Journals » Clinical Ophthalmology » Volume 20
A Novel Surgical Strategy for Choroidal Avulsion in Complex Ocular Trauma: Choroidal Suturing Technique Using 9-0 Double-Armed Polypropylene Sutures
Authors Niu L, Xu H ![]() , Shi J
, Shi J ![]() , Jiang C, Jiang R
, Jiang C, Jiang R ![]()
Received 21 March 2026
Accepted for publication 21 May 2026
Published 3 June 2026 Volume 2026:20 610928
DOI https://doi.org/10.2147/OPTH.S610928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Supplementary video of “Choroidal Avulsion in Complex Ocular Trauma” [610928].
Views: 23
Liangliang Niu,1– 4,* Huan Xu,1– 4,* Jiemei Shi,1– 4 Chunhui Jiang,1– 4 Rui Jiang1– 4
1Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China; 2NHC Key Laboratory of Myopia and Related Eye Diseases; Key Laboratory of Myopia and Related Eye Diseases, Chinese Academy of Medical Sciences, Shanghai, 200031, People’s Republic of China; 3Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, 200031, People’s Republic of China; 4Ocular Trauma Center, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunhui Jiang, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China, Email [email protected] Rui Jiang, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China, Email [email protected]
Purpose: To describe a novel choroidal refixation technique using 9-0 double-armed polypropylene sutures combined with vitreoretinal surgery for severe ocular trauma complicated by choroidal avulsion, and to evaluate its anatomical and functional outcomes.
Methods: This retrospective case series included eight consecutive patients with severe zone III open-globe injuries complicated by choroidal avulsion who were treated at the Ocular Trauma Center of the Eye and ENT Hospital of Fudan University between January and July 2025. All patients underwent vitreoretinal surgery within two weeks after primary globe repair. Choroidal avulsion was confirmed intraoperatively, and refixation was performed using 9-0 double-armed polypropylene sutures. Demographic characteristics, injury features, surgical details, and follow-up outcomes were reviewed. Best-corrected visual acuity (BCVA), intraocular pressure (IOP), axial length, and globe survival were evaluated.
Results: All eight cases involved open-globe injuries, including three eyes with 360° choroidal avulsion. The mean age was 52.87 ± 17.81 years, and 88.5% of patients were male. The baseline BCVA was 2.93 ± 0.21 logMAR, and the mean Ocular Trauma Score was 27.25 ± 3.53, indicating severe ocular injury. After a mean follow-up of 7.37 ± 1.51 months, the mean BCVA demonstrated a mild improvement, reaching 2.46 ± 0.74 logMAR. Mean IOP showed a mild increase from 9.56 ± 4.63 mmHg preoperatively to 11.48 ± 6.19 mmHg at final follow-up, while axial length remained stable Globe preservation was achieved in all cases, with no progression to phthisis bulbi. Four eyes underwent silicone oil tamponade, while the remaining four received implantation of a foldable capsular vitreous body.
Conclusion: This novel choroidal refixation technique 9-0 double-armed polypropylene sutures appears to be a feasible surgical approach for severe ocular trauma with choroidal avulsion, enabling successful globe preservation in eyes with a poor initial prognosis.
Keywords: choroidal avulsion, complex ocular trauma, choroidal suturing technique, globe survival
Introduction
Mechanical ocular trauma, including both open-globe and closed-globe injuries, is characterized by complex and heterogeneous clinical presentations and may result in irreversible impairment of functional vision.1–3 Ocular trauma frequently affects multiple ocular structures and may be complicated by intraocular hemorrhage, retinal or choroidal detachment, intraocular foreign bodies, cyclodialysis, and other vision-threatening sequelae.4–7 In the most severe forms of ocular trauma, approximately 4.2% of cases may progress to choroidal avulsion. Among these patients, up to 92.2% experience an extremely poor clinical prognosis, often resulting in irreversible visual loss.8
Choroidal avulsion is a severe complication of ocular trauma, characterized by complete or extensive separation (avulsion) of the choroid from the sclera. It is often accompanied by discontinuity of the choroidal tissue itself, and in severe cases, the ciliary body may be involved, resulting in en bloc detachment at the scleral spur. Uveal avulsion alters intraocular compartmentalization, permitting unrestricted fluid exchange between the suprachoroidal space and the vitreous cavity, which promotes chronic hypotony and hinders successful retinal reattachment.8,9 Without timely and appropriate intervention, these conditions can further progress to devastating outcomes, including phthisis bulbi and permanent visual loss.
The management of choroidal avulsion and associated complex posterior segment injuries remains technically demanding. Previous studies have reported the use of fibrin glue injected into the suprachoroidal space to promote choroidal reattachment.10 In recent years, with advances in vitrectomy techniques, vitrectomy combined with suturing strategies has shown promising progress in the treatment of choroidal avulsion. These approaches include pars plana vitrectomy combined with 10-0 nylon scleral suturing,11 transscleral mattress suturing using 10-0 polypropylene sutures,9,12 intraocular suturing with 8-0 sutures,9 and a single-suture technique employing 7-0 nylon.12 Delayed or inadequate surgical intervention may further exacerbate tissue ischemia, proliferative vitreoretinopathy, and progressive globe atrophy, ultimately resulting in phthisis bulbi.
In the present study, a novel suturing technique, choroidal suturing using 9-0 double-armed polypropylene sutures combined with vitreous surgery, was developed to refix the avulsed choroid in severe ocular trauma, and postoperative outcomes were systematically evaluated.
Subjects and Methods
Subject Enrollment
This investigation was conducted as a retrospective cohort study in compliance with the Declaration of Helsinki. Given the retrospective nature of the study and the emergent setting of severe ocular trauma, informed consent for the surgical procedures (eg, vitrectomy and related interventions) was obtained as part of routine clinical practice. Informed consent for study participation was waived or not specifically required, as approved by the Ethics Committee.
Participants were consecutively enrolled at the Ocular Trauma Center of the Eye and ENT Hospital of Fudan University from January 2025 to July 2025. To ensure procedural consistency, all surgical interventions were carried out by a single senior chief physician specializing in ocular trauma (J.R).
Inclusion Criteria
Inclusion criteria were as follows:
(1) patients hospitalized for the management of severe mechanical ocular trauma involving Zone III, including open-globe or closed-globe injuries, as defined by the Birmingham Eye Trauma Terminology (BETT) system;13,14
(2) eyes in which choroidal avulsion was confirmed intraoperatively and choroidal refixation was performed. Because choroidal avulsion is frequently accompanied by extensive intraocular hemorrhage that limits preoperative visualization, the decision to perform choroidal suturing was made during surgery; and
(3) a postoperative follow-up duration of at least six months. To enhance the robustness and consistency of outcome assessment, only patients meeting this minimum follow-up requirement were included in the final analysis.
Data Collection and Evaluation
Clinical data were retrieved from the hospital’s electronic medical record system and included demographic characteristics (age and sex), mechanism of injury, imaging findings, surgical details, and clinical outcomes at the final follow-up. Intraoperative observations of the posterior segment were systematically documented in all cases.
Before surgery, all patients underwent a comprehensive ophthalmic assessment, comprising best-corrected visual acuity (BCVA) evaluation, slit-lamp biomicroscopy, intraocular pressure (IOP) measurement, and axial length determination using the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany). Ancillary diagnostic examinations, including B-scan ultrasonography, ultrasound biomicroscopy (UBM), and computed tomography (CT), were performed as clinically indicated.
BCVA was documented using Snellen notation and converted to logMAR units for analysis. Qualitative VA levels were assigned corresponding logMAR values as follows: counting fingers (CF), 2.10; hand motion (HM), 2.40; light perception (LP), 2.70; and no light perception (NLP), 3.00.15,16
For patients with severe open- or closed-globe injuries involving Zone III, the BETT classification, BETT grade, and Ocular Trauma Score (OTS) were recorded.17
According to the BETT classification, injury severity was graded based on initial BCVA at presentation. Initial BCVA measured at the first ophthalmic examination was categorized into five grades: Grade 1 (≥20/40), Grade 2 (20/50–20/100), Grade 3 (worse than 20/100 to 5/200), Grade 4 (worse than 4/200 to LP), and Grade 5 (NLP).
The OTS, commonly used for prognostic assessment in ocular trauma, was calculated using a standardized two-step method. Baseline points were assigned according to initial BCVA at presentation (≥20/40, 100 points; 20/50–20/100, 90 points; worse than 20/100–5/200, 80 points; worse than 4/200–LP, 70 points; and NLP, 60 points). Penalty points were then cumulatively subtracted for predefined adverse clinical factors, including globe rupture (−23), endophthalmitis (−17), perforating injury (−14), retinal detachment (−11), and relative afferent pupillary defect (RAPD; −10). The final OTS was calculated by summing the baseline score and all applicable penalty points.
Surgical Technique and Intraoperative Management
Vitreoretinal surgery was performed under retrobulbar anesthesia within two weeks after the initial ocular trauma repair. Given that all cases involved severe Zone III injuries, vitrectomy approach was carefully planned. Sclerotomies were created approximately 2.5–3.0 mm posterior to the limbus to minimize the risk of inadvertent trocar entry into the suprachoroidal space and to avoid iatrogenic retinal–choroidal injury.
Because all eyes presented with extensive intraocular hemorrhage, recombinant tissue plasminogen activator (rt-PA; 25 µg/0.05 mL) was injected into the vitreous cavity at the beginning of surgery to facilitate clot liquefaction. Dense hemorrhage was then meticulously and progressively removed to restore visualization, allowing stepwise identification of intraocular structures, including the retina and choroid, as well as anatomical compartments such as the vitreous cavity and suprachoroidal space.
Careful intraoperative exploration was subsequently performed to identify choroidal avulsion, defined as separation of the choroid from the sclera and frequently accompanied by choroidal discontinuity. In the most severe cases, complete avulsion of the choroid and ciliary body from the scleral spur was observed. Once identified, choroidal suturing was performed using 9-0 double-armed polypropylene sutures (MANI, Japan).
A schematic illustration of the surgical steps for traumatic choroidal avulsion repair is shown in Figure 1. A pair of double-curved needles (Needle I and Needle II) connected by a continuous 9-0 polypropylene suture was utilized. Depending on the extent of the avulsion, one or two suture sets were applied to achieve optimal anatomical realignment, with intraoperative adjustments made as needed based on surgical findings.
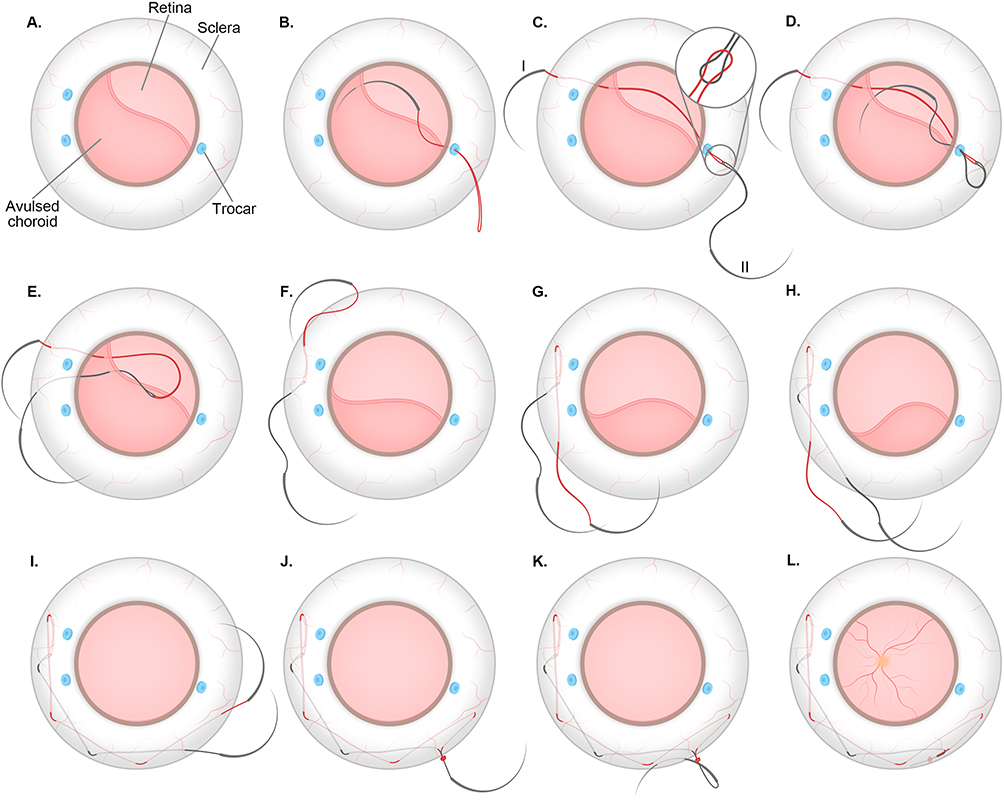 |
Figure 1 Schematic illustration of the surgical technique for choroidal refixation using 9-0 double-armed polypropylene sutures. (A) Schematic illustration of traumatic choroidal avulsion prior to suturing. (B) Needle I was introduced through a pars plana trocar on the side opposite the choroidal avulsion, passed through the avulsed choroid, and externalized through the corresponding scleral and conjunctival site, leaving a suture loop intraocularly. (C) Needle II was threaded through the loop of Needle I, connecting the two needles. (D–F) Needle II was inserted through an anterior trocar (D) and passed through the choroid approximately 1 clock hour away from the entry point of Needle I (E); tightening the sutures approximated the avulsed choroid toward the sclera (F). (G–I) Sequential alternating passes of Needles I (G) and II (H) were performed with clock-hour spacing (I) to secure the entire avulsed choroidal area. (J and K) Final knot tying was completed (J), and the knot was buried within the scleral layers (K). (L) Schematic illustration of traumatic choroidal avulsion following suturing. |
Initial suture placement (Needle I): Through a trocar positioned opposite the site of choroidal avulsion, Needle I was introduced into the eye, passed through the avulsed choroid, typically near the equator, and exited at the corresponding scleral site. The needle was then externalized through the conjunctiva, leaving a suture loop outside the trocar (Figure 1A and B).
Connecting the second needle (Needle II): Needle II was threaded through both the loop created by Needle I and its own suture loop, thereby linking the two needles (Figure 1C). Needle II was inserted through an anterior trocar, passed through the choroid approximately 1 clock hour from the entry point of Needle I, and externalized through the corresponding scleral and conjunctival site. Gentle tension on both sutures facilitated approximation of the avulsed choroid toward the sclera (Figure 1D–F).
Sequential continuous suturing: Needle I was reinserted near its scleral exit site and advanced parallel to the limbus, crossing Needle II, and passed through the choroid approximately 2 clock hours from the initial entry point. Needle B was advanced in a similar fashion, maintaining approximately 1 clock hour spacing between the needles. This alternating, sequential maneuver was repeated until the entire avulsed choroidal segment was secured (Figure 1G–I).
Final knotting and burial: Finally, Needles I and II were retrieved through the scleral layers near the exit site of the opposite needle. A fringe knot was tied and buried within the scleral layers. The knot was secured by gently grasping the underlying scleral tissue with fine forceps, and each suture end was passed intralamellarly for approximately 1 clock hour to ensure complete embedding (Figure 1J–L).
Following successful choroidal refixation, additional vitreoretinal procedures were performed as indicated. The retinal funnel was flattened, and retinal reattachment was achieved through adjunctive maneuvers including epiretinal and subretinal membrane peeling, retinotomy or limited retinectomy when necessary, application of perfluorocarbon liquid (PFCL), endolaser photocoagulation, and tamponade with silicone oil.
Outcome Evaluation
Postoperatively, patients underwent routine follow-up examinations, including slit-lamp biomicroscopy, assessment of BCVA, IOP measurement, and axial length evaluation. In addition, ultra-widefield fundus photography (Optos PLC, Dunfermline, UK) was performed to assess the condition of the posterior segment. Optical coherence tomography (OCT; Spectralis, Heidelberg Engineering, Germany) was used to obtain detailed macular imaging in eyes with sufficiently clear optical media. Globe survival was also documented as a key postoperative outcome measure.
Results
Patient Demographics
The demographic and clinical characteristics of the study cohort are summarized in Table 1. The mean age of the participants was 52.87 ± 17.81 years (range, 18–72 years), and the majority were male (87.5%, 7/8). Regarding the mechanisms of injury, two patients sustained occupational injuries, two were injured in motor vehicle accidents, two suffered assault-related injuries, and two sustained firework-related injuries.
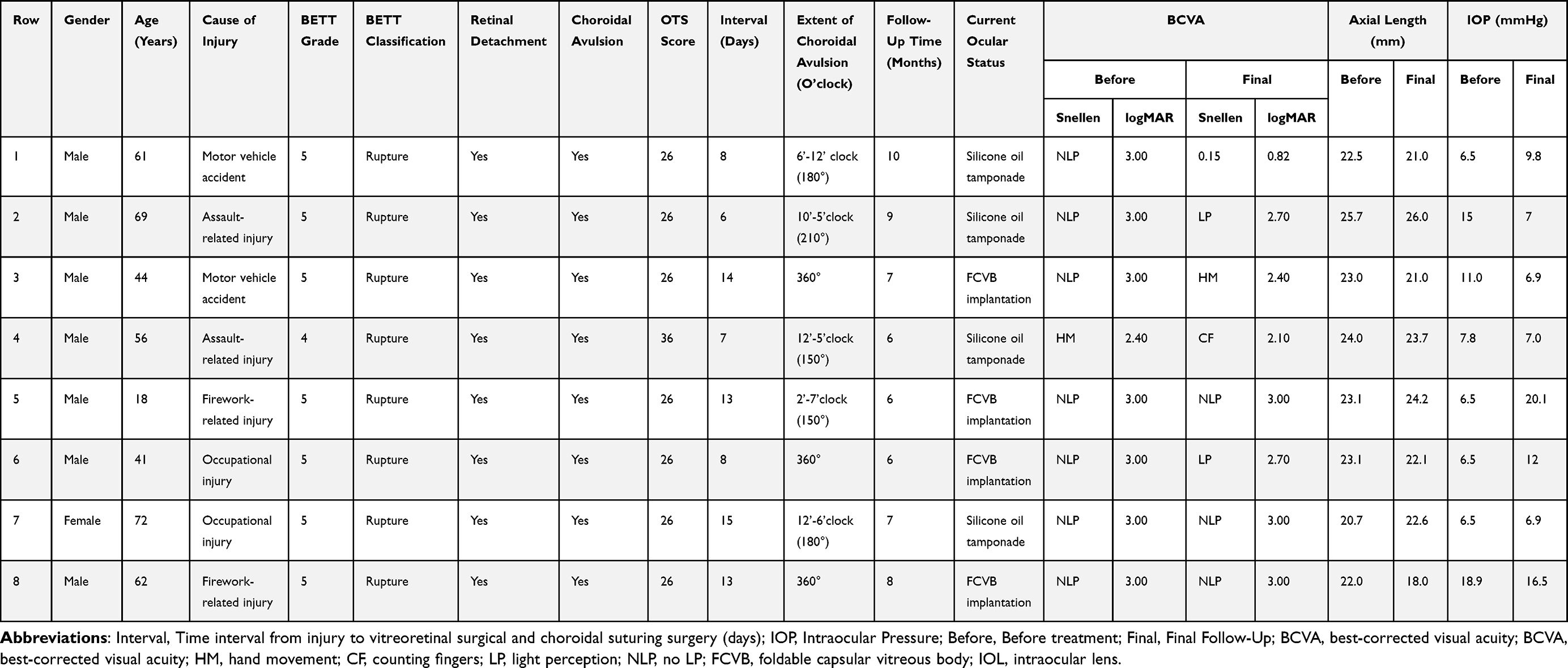 |
Table 1 Individual Results of All 8 Patients Related to Choroidal Avulsion in Complex Ocular Trauma |
All patients had zone III open-globe injuries complicated by retinal detachment and choroidal avulsion. At initial presentation, BCVA was HM in one patient and NLP in the remaining seven patients, with a mean visual acuity of 2.93 ± 0.21 logMAR. Accordingly, all eyes were classified as severe ocular trauma, with BETT grades ranging from 4 to 5 (mean 4.87 ± 0.35).
Based on the initial BCVA and preoperative comorbidities, the OTS was calculated. One patient had an OTS of 36, whereas the remaining seven had scores of 26. The mean OTS was 27.25 ± 3.53, indicating severe ocular injury. At initial presentation, the mean IOP was 9.56 ± 4.63 mmHg, and the mean axial length was 23.00 ± 1.46 mm.
These assessments highlight the extent of ocular injury at presentation and serve as a reference for understanding postoperative outcomes.
Intraoperative Findings
All patients with open-globe injuries had undergone primary globe repair for rupture either in the emergency department of our institution or at other hospitals. Within 10.50 ±3.58 days after the initial ocular trauma, vitreoretinal surgery was performed under retrobulbar anesthesia.
Careful intraoperative exploration was conducted to identify choroidal avulsion, which was defined as separation of the choroid from the sclera and was frequently accompanied by choroidal discontinuity. In the most severe cases, complete avulsion of the choroid and ciliary body from the scleral spur was observed. During vitrectomy, varying degrees of choroidal avulsion were identified in all eight patients. Specifically, three patients exhibited 360° choroidal avulsion, one patient had a 210° avulsion, two patients had 180° avulsion, and two patients had 150° avulsion.
Once identified, refixation of the avulsed choroid was achieved using 9–0 double-armed polypropylene sutures. Vitreoretinal surgical maneuvers were subsequently continued and modified according to the extent of residual vitreous hemorrhage and other intraoperative findings.
In one patient (Row 6), owing to a circumferential (360°) choroidal avulsion with complete tissue inversion, two sets of 9-0 double-armed polypropylene sutures were required to achieve satisfactory refixation. Representative intraoperative images and corresponding clinical data from selected patients (Rows 1, 2, 4, and 6) are presented in Figures 2–5. The surgical procedure in the patient from Row 1 is additionally demonstrated in Supplementary Video 1.
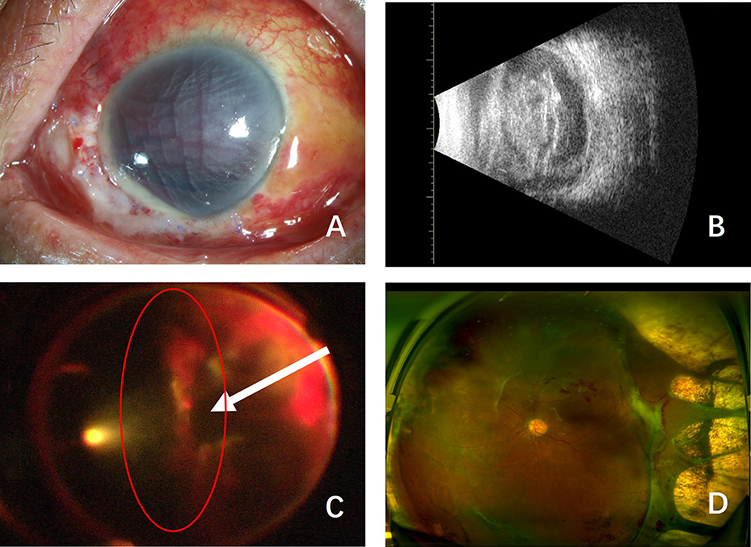 |
Figure 2 Clinical course of a representative patient in Row 1. A 61-year-old male sustained a left globe rupture in a motor vehicle accident and presented with NLP. Emergency primary globe repair was performed, followed by vitrectomy combined with choroidal avulsion suturing 8 days after injury. (A and B) Preoperatively, the cornea was obscured by blood staining, preventing visualization of intraocular structures (A). B-scan ultrasonography revealed massive vitreous hemorrhage accompanied by retinal detachment and choroidal detachment (B). (C) Intraoperatively, after clearance of dense vitreous hemorrhage, a 180° temporal choroidal avulsion inverted toward the nasal side was identified. The avulsed choroid was repaired using 9-0 double-armed sutures (see Supplementary Video 1 for surgical details). (D) At the most recent follow-up, BCVA improved to 0.15. The left eye remained silicone oil–filled, with a flat retina, temporal scleral exposure, and a residual choroidal defect. Red circle and white arrow denote the choroidal avulsion identified during intraoperative exploration. Abbreviations: NLP, no light perception; BCVA, best-corrected visual acuity. |
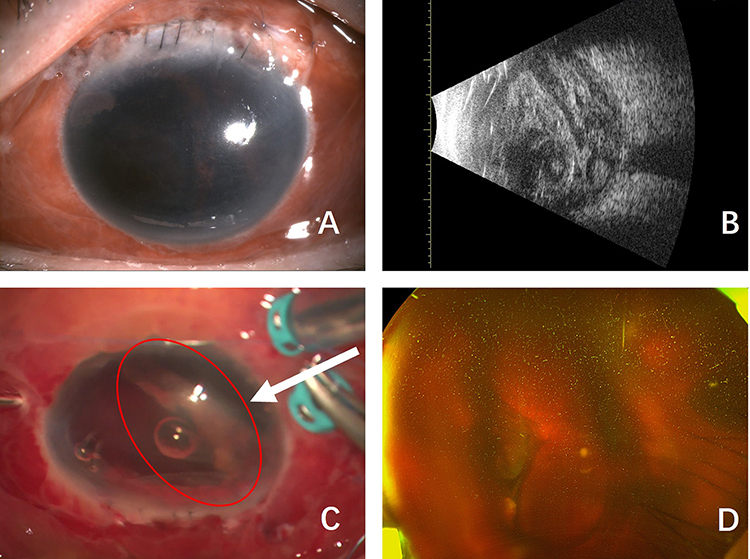 |
Figure 3 Clinical course of a representative patient in Row 2. A 69-year-old male sustained a left globe rupture due to an assault-related injury and presented NLP. Emergency primary globe repair was performed, followed by vitrectomy combined with choroidal avulsion suture fixation 6 days after injury. (A and B) Preoperatively, the cornea was obscured by blood staining, precluding visualization of the intraocular structures (A). B-scan ultrasonography demonstrated massive vitreous hemorrhage associated with retinal detachment and choroidal detachment (B). (C) Intraoperatively, after corneal epithelial debridement and clearance of dense vitreous hemorrhage, a 210° temporal choroidal avulsion inverted toward the nasal side was identified. The avulsed choroid was repaired using 9-0 double-armed polypropylene sutures. (D) At the most recent follow-up, BCVA was limited LP. Owing to persistent corneal blood staining, the fundus remained unobservable. Further surgical intervention was not performed because the patient traveled abroad. Red circle and white arrow denote the choroidal avulsion identified during intraoperative exploration. Abbreviations: NLP, no light perception; LP, light perception; BCVA, best-corrected visual acuity. |
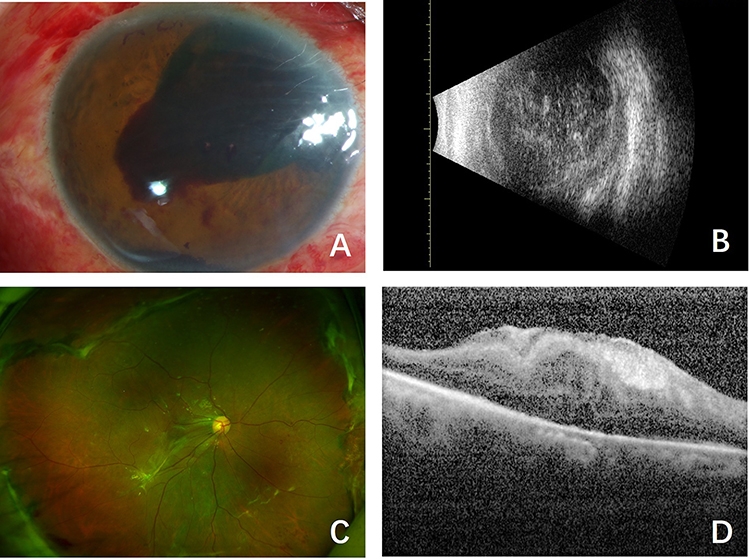 |
Figure 4 Clinical course of a representative patient in Row 4. A 56-year-old male sustained a right globe rupture due to an assault-related injury and presented with a BCVA of HM. Emergency primary globe repair was performed, followed by vitrectomy combined with choroidal avulsion suture fixation 7 days after injury. (A and B) Preoperatively, slit-lamp examination revealed corneal epithelial edema, hyphema involving the pupillary area, and a superonasal iris defect accompanied by a fibrovascular membrane, with suspected ciliary body avulsion (A). B-scan ultrasonography demonstrated massive vitreous hemorrhage associated with retinal detachment and choroidal detachment (B). (C and D) Intraoperatively, after clearance of dense vitreous hemorrhage, a 150° choroidal avulsion involving the superior and nasal quadrants was identified. The avulsed choroid was repaired using 9–0 double-armed polypropylene sutures. At the most recent follow-up, BCVA improved to FC. Subsequently, proliferative traction was observed in the peripheral (C) and posterior (D) retina, and the patient has been scheduled for hospital admission for silicone oil removal and membrane peeling surgery. Abbreviations: HM, hand motion; CF, counting fingers; BCVA, best-corrected visual acuity. |
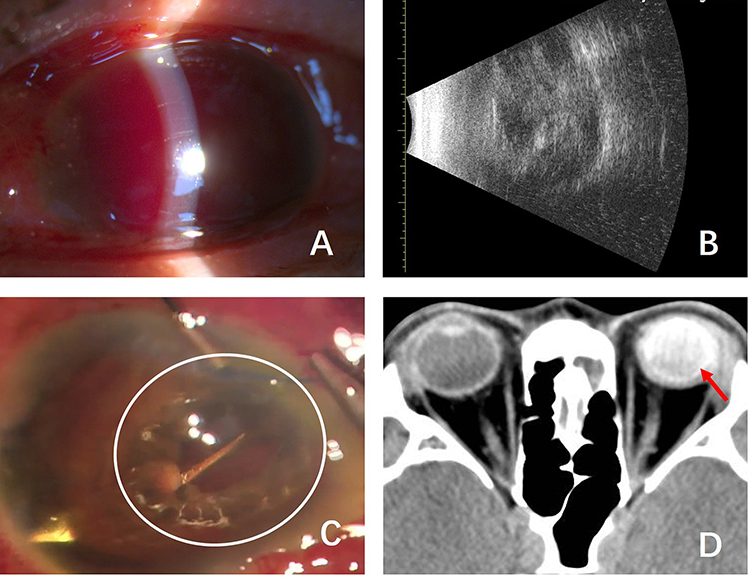 |
Figure 5 Clinical course of a representative patient in Row 6. A 41-year-old male sustained a left globe rupture due to an assault-related injury and presented with NLP. Emergency primary globe repair was performed, followed by vitrectomy combined with choroidal avulsion suture fixation 8 days after injury. (A and B) Preoperatively, the cornea was obscured by blood staining, precluding visualization of the intraocular structures (A). B-scan ultrasonography demonstrated massive vitreous hemorrhage associated with retinal detachment and choroidal detachment (B). (C) Intraoperatively, after corneal epithelial debridement and clearance of dense vitreous hemorrhage, a 360° circumferential choroidal avulsion was identified. The avulsed choroid was repaired using two sets of 9-0 double-armed polypropylene sutures. Owing to the presence of only minimal residual retinal tissue, implantation of a FCVB was subsequently performed one week later to preserve globe integrity(D). At the most recent follow-up, BCVA was limited to LP. White circle denotes the choroidal avulsion identified during intraoperative exploration; Red arrow notes the FCVB. Abbreviations: NLP, no light perception; LP, light perception; BCVA, best-corrected visual acuity; FCVB, foldable capsular vitreous body. |
Among the eight patients included in this study, only one patient (Row 4) had residual iris and lens structures identifiable preoperatively. In the remaining seven patients, both structures had been lost at the time of trauma due to injury severity. In the Row 4 patient, lensectomy was performed during the combined procedure.
Follow-Up Outcomes
All eight patients with severe ocular trauma complicated by choroidal avulsion were followed for a mean duration of 7.37 ± 1.51 months. At presentation, all cases were classified as Zone III injuries with BETT Grade 4–5 and OTS scores of 26–36, indicating a poor visual prognosis.
The mean BCVA showed mild improvement during follow-up, from 2.93 ± 0.21 logMAR at presentation to 2.46 ± 0.74 logMAR at the final visit. Globe preservation was achieved in all cases, yielding a 100% globe survival rate, with no evidence of phthisis bulbi. The mean axial length remained stable, measuring 23.00 ± 1.46 mm at presentation and 22.46 ± 2.48 mm at the final follow-up.
The mean intraocular pressure increased slightly from 9.56 ± 4.63 mmHg at presentation to 11.48 ± 6.19 mmHg at the final visit and remained relatively stable thereafter.
Due to the severe damage to both the anterior and posterior segments at the initial presentation of ocular trauma, common postoperative anterior segment complications included corneal opacity (75%, 6/8 cases). At the final follow-up, fundus visualization was possible in only two patients (Row 1 and Row 4). Therefore, fundus-related complications were not systematically assessed, and the outcome measures were limited to globe survival, axial length, and intraocular pressure.
Given that all patients in this study sustained extremely severe ocular trauma, one of the primary surgical goals was globe preservation. The choice between silicone oil tamponade and foldable capsular vitreous body (FCVB) implantation was determined based on comprehensive intraoperative findings and postoperative follow-up, with particular consideration of the condition of the retina and choroid, as well as clinical parameters such as intraocular pressure and axial length.
In cases where the retina and choroid were largely preserved and intraocular pressure and axial length remained relatively stable, silicone oil tamponade was preferred, followed by close observation and consideration of subsequent silicone oil removal or additional interventions as clinically indicated. In contrast, FCVB implantation was selected for patients with extensive retinal and choroidal defects, persistently low intraocular pressure, marked axial shortening, and a tendency toward globe atrophy, as a means of maintaining globe integrity.
The FCVB implantation procedure was performed as follows: a scleral incision was created at the pars plana for silicone oil removal, followed by maximal flattening of the residual retina. An appropriately sized FCVB was then implanted according to the axial length, and silicone oil was injected into the capsule to provide internal support.
Globe preservation was achieved in all cases, and none progressed to phthisis bulbi. At the final follow-up, four patients (Rows 1, 2, 4, and 7), who exhibited relatively preserved posterior segment structures, remained aphakic with silicone oil tamponade, and will undergo further surgical management as needed based on their clinical course. The remaining four patients (Rows 3, 5, 6, and 8), characterized by extensive retinal and choroidal damage or advanced globe atrophy, underwent FCVB implantation to maintain globe integrity.
Discussion
Choroidal avulsion represents one of the most devastating forms of posterior segment injury in ocular trauma and is associated with profound hypotony, retinal loss, and a high risk of phthisis bulbi.8,9 In this study, we describe a novel choroidal suturing technique using 9-0 double-armed polypropylene sutures combined with vitreoretinal surgery and demonstrate favorable anatomical preservation and stabilization of intraocular pressure in a cohort of eyes with extremely poor baseline prognoses. Despite severe zone III injuries and very low initial OTS, globe survival was achieved in all cases, and mean IOP improved and stabilized during follow-up.
The pathophysiological basis of poor outcomes in choroidal avulsion lies in disruption of uveal–scleral continuity and breakdown of intraocular compartmentalization. Separation of the choroid from the sclera allows persistent communication between the suprachoroidal space and vitreous cavity, leading to chronic hypotony, impaired retinal reattachment, and progressive globe atrophy [8]. Therefore, restoration of anatomical continuity between the choroid and sclera is critical not only for structural repair but also for re-establishing intraocular pressure homeostasis. The present technique directly addresses this mechanism through mechanical re-approximation of the avulsed choroid to the scleral wall.
Choroidal avulsion, as a severe complication of ocular trauma, is generally associated with a poor prognosis, and effective treatment approaches remain limited. Jiang et al were the first to report, in 2010, the use of fibrin glue injected into the suprachoroidal space during pars plana vitrectomy. At 6 months postoperatively, a slightly elevated scar formed at the site of the original choroidal rupture, contributing to reattachment of the avulsed choroid.10
Most subsequent reports have focused on suturing techniques for the management of choroidal avulsion. Ma et al described creating full-thickness transscleral incisions (1–4.2 cm) based on the location and extent of the avulsion, followed by transscleral suturing with 10-0 nylon to reapproximate the choroid to the sclera.11 Chen et al and Iwase et al reported mattress suturing techniques using long-curved 10-0 polypropylene needles passed from the sclera through the avulsed choroid.9,12 In addition, Chen et al described an intraocular suturing approach in which an 8-0 polyglactin suture was introduced through a 20-gauge scleral incision, passed through the full thickness of the choroid, scleral lamella, and choroid again, and then retrieved into the vitreous cavity for fixation.9 Iwase et al also reported the use of 7-0 nylon sutures, placing two sutures in each quadrant for multidirectional fixation.
These techniques represent different surgical strategies and suture selections, each with potential advantages and practical considerations depending on the specific clinical context. For example, finer sutures such as 10-0 polypropylene may allow more delicate manipulation, whereas thicker sutures such as 7-0 nylon may facilitate needle passage and handling in certain situations. However, direct comparisons between these methods remain challenging due to differences in case characteristics and surgical conditions across studies.
While these approaches have contributed to the surgical management of choroidal avulsion, certain challenges may still be encountered, particularly in cases with extensive or circumferential avulsion or involvement of more posterior regions. In this context, the use of 9-0 double-armed polypropylene sutures, as applied in the present study, represents one possible technical approach.
The use of double-curved needles with a relatively long span (15 mm) may facilitate access to the equatorial region of the globe, and their curvature may allow controlled passage through the equatorial and postequatorial choroid. A sequential suturing strategy can be employed to achieve stepwise reapproximation of the detached choroid to the sclera, which may help distribute tension along the avulsed margin and promote tissue apposition.
The present series included eyes with extremely poor initial visual acuity, most of which were classified as severe ocular trauma with very low OTS. Although visual recovery remained limited in many cases—likely reflecting the severity of the primary retinal and choroidal injury—globe preservation and stabilization of intraocular pressure were observed during follow-up. In the setting of severe ocular trauma, preservation of globe integrity may represent a clinically meaningful outcome, as it may reduce the risk of phthisis bulbi and maintain the possibility of subsequent reconstructive procedures.
This technical feature in the current study may contribute to maintaining choroid–sclera contact and may have a role in limiting persistent suprachoroidal fluid or hypotony; however, such effects remain difficult to determine given the limited sample size and follow-up. In cases of more extensive avulsion, additional sutures may be placed as needed, although the optimal strategy has not been established.
This study has several limitations. First, the sample size was small, reflecting the rarity and severity of choroidal avulsion. Second, the retrospective design and the absence of a control group limit direct comparison with other suturing techniques. Third, the follow-up duration was relatively short; therefore, larger case series and longer-term observation are essential, particularly for monitoring potential late complications such as phthisis bulbi and proliferative vitreoretinopathy (PVR), and for more accurately evaluating postoperative stability over time.
In addition, the prognosis of severe ocular trauma is closely related to the extent of injury, and inter-individual variability among patients is unavoidable. Differences in injury severity, associated ocular injuries, and adjunctive surgical procedures may have influenced functional recovery.
Future studies with larger multicenter cohorts and comparative designs are warranted to further validate the reproducibility and long-term benefits of this technique. Quantitative assessment of postoperative suprachoroidal space dynamics and IOP stabilization may also provide mechanistic insight into the relationship between anatomical repair and functional preservation.
Conclusions
Choroidal suturing with 9-0 double-armed polypropylene sutures combined with vitreoretinal surgery appears to be a feasible approach for managing severe choroidal avulsion. By restoring choroidal–scleral continuity and stabilizing intraocular pressure, this novel technique may improve globe survival in eyes that otherwise carry an extremely poor prognosis.
Ethical Approval
This retrospective study was approved by the Ethics Committee of the Eye and ENT Hospital of Fudan University (Reference No. 2024146), and informed consent was obtained from all participants before inclusion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by National Natural Science Foundation of China (grant nos. 82101087 to LN, grant nos. 82201226 to HX).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Illanes JO. Epidemiology and trends of ocular trauma hospitalizations in Chile from 2001 to 2020. J Fr Ophtalmol. 2022;45(9):1055–12. doi:10.1016/j.jfo.2022.03.007
2. He CH, Poulsen DM, Parsikia A, Mbekeani JN. Characteristics of ocular trauma in the United States. Arq Bras Oftalmol. 2022;85(3):240–248. doi:10.5935/0004-2749.20220035
3. Iftikhar M, Canner JK, Latif A, Shah SMA, Justin GA, Woreta FA. Epidemiology of ophthalmic trauma in the United States from 2009-2018: a Nationwide Emergency Department Sample Analysis. Injury. 2024;55(3):111209. doi:10.1016/j.injury.2023.111209
4. Almendárez JE, Vargas DM, González C, Takane M, Koga W. Ultrasound findings in ocular trauma. Arch Soc Esp Oftalmol. 2015;90(12):572–577. doi:10.1016/j.oftal.2015.07.010
5. Yucel OE, Demir S, Niyaz L, Sayin O, Gul A, Ariturk N. Clinical characteristics and prognostic factors of scleral rupture due to blunt ocular trauma. Eye. 2016;30(12):1606–1613. doi:10.1038/eye.2016.194
6. González-Martín-Moro J, Contreras-Martín I, Muñoz-Negrete FJ, Gómez-Sanz F, Zarallo-Gallardo J. Cyclodialysis: an update. Int Ophthalmol. 2017;37(2):441–457. doi:10.1007/s10792-016-0282-8
7. Sethi A, Udenia H, Beri N, et al. Surgical management of cyclodialysis cleft: an update. J Curr Glaucoma Pract. 2025;19(3):143–152. doi:10.5005/jp-journals-10078-1469
8. Chen HJ, Feng K, Feng XF, Wang CG, Ma ZZ. Traumatic choroidal injuries - classification, incidence, diagnosis and prognosis twenty-year results of eye injury vitrectomy study. Acta Ophthalmol. 2021;99(3):e387–e393. doi:10.1111/aos.14578
9. Chen H, Yang J, Wang C, Feng X, Feng K, Ma Z. Novel suturing methods for the management of traumatic choroidal avulsion in globe injuries. Front Med. 2022;8:801068. doi:10.3389/fmed.2021.801068
10. Jiang YR, Tao Y, Jonas JB. Traumatic choriodialysis treated by intraocular fibrin glue. Acta Ophthalmol. 2010;88(4):e129–30. doi:10.1111/j.1755-3768.2009.01542.x
11. Ma J, Tong Y, Shen Z, Ye P. Efficacy of combined vitreous surgery and choroidal suture fixation on choroidal avulsion. Eye Sci. 2011;26(3):143–147. doi:10.3969/j.issn.1000-4432.2011.03.004
12. Iwase T, Nishiyama S, Sato M. A novel suturing technique for choroidal avulsion. J Clin Med. 2022;11(18):5344. doi:10.3390/jcm11185344
13. Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15(2):139–43,v. doi:10.1016/s0896-1549(02)00004-4
14. Kuhn F, Morris R, Witherspoon CD, Mester V. The Birmingham Eye Trauma Terminology system (BETT). J Fr Ophtalmol. 2004;27(2):206–210. doi:10.1016/s0181-5512(04)96122-0
15. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99(6):e963–e965. doi:10.1111/aos.14659
16. Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories “hand motion” and “counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
17. Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmol Clin North Am. 2002;15(2):163–5,vi. doi:10.1016/s0896-1549(02)00007-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.