Back to Journals » Drug Design, Development and Therapy » Volume 20
A Novel Standardized Dexmedetomidine Nasal Spray Formulation for Procedural Sedation During Venous Port Implantation: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial
Authors Tong J, Wei M, Ye Z, Gao H, Hong W, Cai P, Li W, Wang J, Zhou X, Liang C, Wang Z ![]()
Received 18 November 2025
Accepted for publication 23 March 2026
Published 8 April 2026 Volume 2026:20 582503
DOI https://doi.org/10.2147/DDDT.S582503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Jie Tong,1,* Mengping Wei,1,* Zhixiang Ye,1,* Huayuan Gao,1 Weifeng Hong,1 Peiling Cai,1 Wenjun Li,1 Jie Wang,2 Xiushi Zhou,3 Chao Liang,1,2,* Zhiyao Wang2,*
1Department of Anesthesiology, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, Fujian, People’s Republic of China; 2Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 3Department of Population Health Sciences, Duke University School of Medicine, Durham, NC, 27701, USA
*These authors contributed equally to this work
Correspondence: Zhiyao Wang, Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected] Chao Liang, Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Background: Noninvasive sedative approaches are increasingly valued in ambulatory anesthesia. The aim of this study was to evaluate the efficacy and safety of the novel standardized dexmedetomidine nasal spray for procedural sedation in adult patients undergoing port implantation under local anesthesia.
Methods: Eighty-two patients undergoing port implantation under local anesthesia were enrolled in this study. The patients were randomly allocated to receive nasal spray with 100μg dexmedetomidine or placebo with saline, 30 min prior to the procedure. The primary outcome was the postoperative anesthesia satisfaction assessed using Iowa Satisfaction with Anesthesia Scale (ISAS; 11-item mean score, − 3 to +3). The secondary outcomes included the Ramsay sedation scale (RSS), visual analog scale (VAS), postoperative sleep quality, hemodynamic changes, and the incidence of adverse events.
Results: Compared with placebo, dexmedetomidine significantly improved satisfaction with procedure (ISAS median [IQR] was 2.7 [2.5– 2.8] vs 2.1 [1.8– 2.4]; P< 0.001), indicating a clinically relevant improvement in patient experience during outpatient port implantation under local anesthesia, and postoperative sleep quality (4.4± 0.8 vs 3.1± 0.8, P< 0.001) during the first postoperative night. The incidence of adverse events and other secondary outcomes were comparable between the two groups.
Conclusion: A standardized dexmedetomidine nasal spray provided reliable, well-tolerated sedation, enhanced postoperative comfort, and improved postoperative sleep quality in adults undergoing minor procedures under local anesthesia. These findings support its feasibility as a noninvasive option for outpatient procedural sedation.
Keywords: dexmedetomidine, administration, intranasal, conscious sedation, vascular access devices, patient satisfaction, ambulatory surgical procedures
Introduction
Totally implantable venous access port (also known as port) is widely used in cancer patients who require long-term chemotherapy and has proven to be a safe and effective drug delivery device.1 In addition, it can also be used for the infusion of various liquids, including parenteral nutrient solutions and blood products.2,3 The most common site for port implantation is the anterior chest via the jugular vein or subclavian vein.4 This procedure is usually carried out under local anesthesia because it has been proven to be safe and has the advantages of saving materials and labor, improving cost-effectiveness, and accelerating patient discharge compared with general anesthesia.5–7 However, many patients experience substantial preoperative anxiety and discomfort during port implantation under local anesthesia, which may compromise overall procedural satisfaction.
Preoperative anxiety is very common among adult patients undergoing elective procedures.8,9 A retrospective study of ultrasound-guided central venous port implantation showed that 19 of 138 patients were switched to general anesthesia due to anxiety and intraoperative pain.10 Poorly managed preoperative anxiety and inadequate postoperative pain management are associated with detrimental postoperative recovery and reduced satisfaction with care.11–13 Thus, despite the many advantages of local anesthesia, achieving a comfortable and cooperative surgical experience during port implantation remains challenging. Moreover, a study found that the single oral sedative, lorazepam, did not improve patient satisfaction with port placement under local anesthesia.14 Patients may benefit from procedural sedation, which is defined as a technique using hypnotic and/or analgesic medications to enable effective performance of diagnostic or therapeutic procedures, while monitoring for potential adverse effects.15,16
Dexmedetomidine, a drug used for procedural sedation, is a highly selective agonist of α2-adrenergic receptor that exhibits sedative, anxiolytic and analgesic effects with minimal respiratory depression.17 In most clinical practice dexmedetomidine is often administered intravenously, an invasive approach that needs an IV-line for cannulation. As a non-invasive route, intranasal administration provides rapid onset of action and high bioavailability due to bypassing first-pass metabolism.18 Previous clinical studies have demonstrated the feasibility of intranasal dexmedetomidine in both pediatric19,20 and adult populations,21–25 however, these formulations often require manual dilution or nebulization.25,26 Such approaches lead to variations in dosing accuracy, sterility, and reproducibility, limiting their practicality for routine clinical use.
To address these limitations, a standardized dexmedetomidine nasal spray (Jiangsu Hengrui Pharmaceuticals, China) was developed as a ready-to-use formulation with precise actuation dosing (25 μg per spray) and high bioavailability (80–120% of label amount). Previous studies have evaluated its safety, tolerability, pharmacokinetics, and pharmacodynamics in healthy adults27 and have demonstrated its safety and effectiveness for preanesthetic sedation in children.28 However, its safety and sedative efficacy in adult cancer patients undergoing port implantation remains unclear. Therefore, this study aimed to evaluate the clinical feasibility, tolerability, and sedative performance of this standardized spray formulation in adult patients undergoing venous port implantation under local anesthesia. We hypothesized that intranasal dexmedetomidine would enhance perioperative satisfaction and comfort without increasing adverse events compared with placebo.
Materials and Methods
Ethics and Trial Registration
The study protocol was approved by the Ethics Committee of Zhongshan Hospital (Xiamen branch) Fudan University (Approval No. B2024-100R) and registered at the Chinese Clinical Trial Registry (ChiCTR2400093619). This study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants before enrollment. We followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines.
Study Participants
This clinical study was carried out at Zhongshan Hospital (Xiamen branch) of Fudan University from December 9, 2024, to May 30, 2025. The potential participants among patients scheduled for port implantation under local anesthesia were screened by an investigator. Eligibility criteria were: (1) patients aged 18–80 years; (2) American Society of Anesthesiologists (ASA) physical status I to III; (3) participation is voluntary and requires signed informed consent. The exclusion criteria were: (1) nasopharyngeal infection, tumor or structural nasal abnormalities; (2) patients allergic to the study drug; (3) current or recent medical conditions that may affect the absorption, distribution, metabolism, excretion, or response to the study drug; (4) history of heart disease (valvular insufficiency, severe left ventricular dysfunction), pacemaker, or electrocardiographic rhythm abnormalities (HR <50/min at rest, second- or third-degree atrioventricular block); (5) long-term use of opioids or other analgesic adjuvants; (6) participated in other clinical trials within one month; (7) pregnant, lactating, or patients with hepatic or renal impairment.
Randomization and Blindness
A random number generation software was used to randomly assign eligible patients in a 1:1 ratio to two groups: dexmedetomidine and placebo. Patients in dexmedetomidine group received nasal spray of dexmedetomidine (1 mL: 500 μg, Jiangsu Hengrui Pharmaceuticals Co., Ltd., China). Patients in placebo group received nasal spray of 0.9% saline solution. The allocation was concealed in sequentially numbered opaque envelopes until patients were enrolled. Dexmedetomidine or 0.9% saline was prepared by an anesthetic nurse who was uninvolved in the study. The spray bottle containing 0.9% saline solution and the bottle containing dexmedetomidine were identical in size, shape, color and weight, making them indistinguishable to both the investigators and the patients from each other in appearance. Anesthesiologists may have been aware of the study medications because of the potential sedation effects of preoperative administration. Therefore, they only perform intraoperative monitoring and do not participate in data collection or postoperative evaluation. All patients, surgeons and clinicians responsible for postoperative follow-up were blinded to group assignments. In case of emergency during the procedure, researcher can unblind the group allocation for the corresponding patient, but the patient will be excluded from the group.
Study Procedures
During the stay in the pre-operative holding area, patients were asked to clean their nostrils and sit upright with their heads slightly tilted forward approximately 30 min prior to being transferred to the operating room. The anesthesiologist then sprayed a prescribed amount of dexmedetomidine (25 μg dexmedetomidine or an equivalent amount of 0.9% saline) into each nostril according to the medicine instructions. After approximately 30 s, the anesthesiologist sprayed another spray into each nostril, for a total of 4 sprays. The bottle was held upright during spraying, and administration was completed within 2 min. The dosage was based on the package insert for dexmedetomidine hydrochloride nasal spray (Shanghai Hengrui Pharmaceutical Co., Ltd., Shanghai, China). Patients in the dexmedetomidine group received a total of 100 μg (four sprays), while those in the placebo group received an equivalent amount of 0.9% saline. This dose was also consistent with a previous pharmacokinetic study in healthy adults, in which a 100 μg dexmedetomidine nasal spray reached a median time to peak plasma concentrations at approximately 30 min after administration.27
After patient entered the operating room, electrocardiograms, non-invasive blood pressure and peripheral oxygen saturation were monitored. All measurements were repeated every 10 min during the procedure. Oxygen therapy was administered via face mask at a rate of 5L/min. The surgeons used verbal reassurance to encourage patient cooperation in both groups. After local infiltration anesthesia with 1% lidocaine and 0.375% ropivacaine, an intra-plane oblique puncture of the right internal jugular vein was performed under ultrasound guidance, and a B. Braun 14G central venous catheter was inserted. After ultrasound localization confirmed the catheter position, a port catheter was inserted over an exchange guidewire, with the distal end of the catheter connected to the port body. A 2-cm skin incision was made along the puncture site, and the subcutaneous tissue was separated to form a 3×4 cm pouch 15 cm from the puncture site. The port body was buried in the pouch, and catheter patency was confirmed. The wound was then sutured subcutaneously and intradermally with 4–0 absorbable sutures. All surgeries were performed by the same highly skilled team of doctors. All procedures were performed during routine daytime working hours (8:30–16:30). The distribution of morning and afternoon cases was balanced between the two groups, ensuring that the time of day did not act as a confounder for the postoperative sleep quality assessment.
Study Outcomes
The primary outcome of this study was patient satisfaction with the operative experience. Patient satisfaction was assessed using the ISAS at the time of discharge from the post-anesthesia care unit (PACU). The ISAS consists of 11 questions with 6 potential responses. For statistical analyses, responses were transformed according to the original algorithm (−3 to +3, with negatively worded items reverse-scored). The overall satisfaction score was calculated as the mean of all item scores. Higher scores indicate greater patient satisfaction29 (Supplemental Box 1).
Secondary outcomes included sedation level, pain intensity, postoperative sleep quality, intraoperative hemodynamic parameters, and adverse events.
Sedation level was assessed using the RSS (1 = anxious and agitated; 2 = cooperative, oriented and tranquil; 3 = responsive to commands only; 4 = brisk response to stimulus; 5 = sluggish response to stimulus; 6 = no response to stimulus).30 Pain intensity was evaluated using an 11-point VAS (0 = no pain; 10 = worst imaginable pain). Postoperative sleep quality was evaluated using the St. Mary’s Hospital Sleep Questionnaire (SMHSQ). Patients were interviewed on the day before surgery and the morning after surgery to reflect sleep during the night of surgery. The SMHSQ assesses multiple sleep dimensions, including quality of sleep (range: 1–6), depth of sleep (range: 1–7), satisfaction with sleep (range: 1–5), and number of awakenings during sleep (range: 0–7). Higher scores indicate better sleep quality.31
Hemodynamic parameters, including heart rate (HR), mean arterial pressure (MAP), and oxygen saturation (SpO2), were recorded at predefined time points: preoperative baseline (T0), start of surgery (T1), 10 minutes after the start of surgery (T2), 20 minutes after the start of surgery (T3), end of surgery (T4), 2 hours after surgery (T5), and 4 hours after surgery (T6). Adverse events were recorded from the end of surgery until hospital discharge and included drug-related reactions such as tachycardia, hypertension, bradycardia, hypotension, respiratory depression, dizziness, headache, drowsiness, nasal discomfort, nausea, and vomiting. Surgical complications within 30 days postoperatively were also documented, including port infection, surgical site infection, hematoma, thrombosis, pleural effusion, and other port-related complications.
Sample Size Estimation
The sample size was determined based on our internal pilot dataset (n=20), in which the mean (SD) ISAS scores (scored from −3 to +3 and averaged across 11 items) were 2.35±0.52 and 2.11±0.29 in the dexmedetomidine and control groups, respectively. The pilot data were used to estimate variability, yielding a pooled standard deviation of 0.42. Because an established minimal clinically important difference for ISAS is not available, sample size planning was based on detecting a standardized effect size in the moderate-to-large range (Cohen’s d≈0.76). Given the pooled SD (0.42), this corresponds to an absolute difference of approximately 0.32 in the ISAS mean score. With a two-sided α=0.05 and 90% power, a minimum of 37 patients per group was required. Allowing for a 10% dropout rate, we enrolled 41 patients per group. Sample size calculation was performed using PASS 15.0 (NCSS, LLC, Kaysville, UT, USA).
Statistics and Analysis
Statistical analyses were performed using GraphPad Prism version 10.2.3 (GraphPad Software, Boston, MA, USA) and IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Normally distributed continuous variables are presented as mean (SD), and non-normally distributed variables as median (IQR). Continuous variables with repeated measurements (eg, hemodynamic parameters) were analyzed using linear mixed-effects models, with Group, Time, and Group × Time as fixed effects and subject as a random effect. When a significant Group × Time interaction was detected, post-hoc pairwise comparisons between groups at each time point were performed with Bonferroni adjustment for multiple comparisons. Between-group comparisons of normally distributed continuous variables were performed using the independent-samples t test (Welch’s t test when variances were unequal). Between-group comparisons of non-normally distributed continuous variables (including the standardized ISAS scores) were performed using the Mann–Whitney U-test. Categorical variables are presented as n (%) and were compared using the chi-square test or Fisher’s exact test, as appropriate. A two-sided P value <0.05 was considered statistically significant.
Results
Patient Inclusion and Baseline Demographic Characteristics
A total of 102 patients were enrolled for this study and 20 were excluded before randomization. Ultimately, 82 patients were randomly allocated: 41 in Dexmedetomidine group and 41 in Placebo group. All patients completed the study, as illustrated in the CONSORT flow diagram (Figure 1). The cohort comprised 43 males (52.4%) and 39 females (47.6%), with an average age of 58.2 years (SD=10.9). Baseline data were comparable across the two groups as shown in Table 1. Demographic and clinical characteristics in terms of age, gender, weight, height, body mass index (BMI), ASA classification, operation history, comorbidities, preoperative sleep status and cancer types showed no significant differences between both groups.
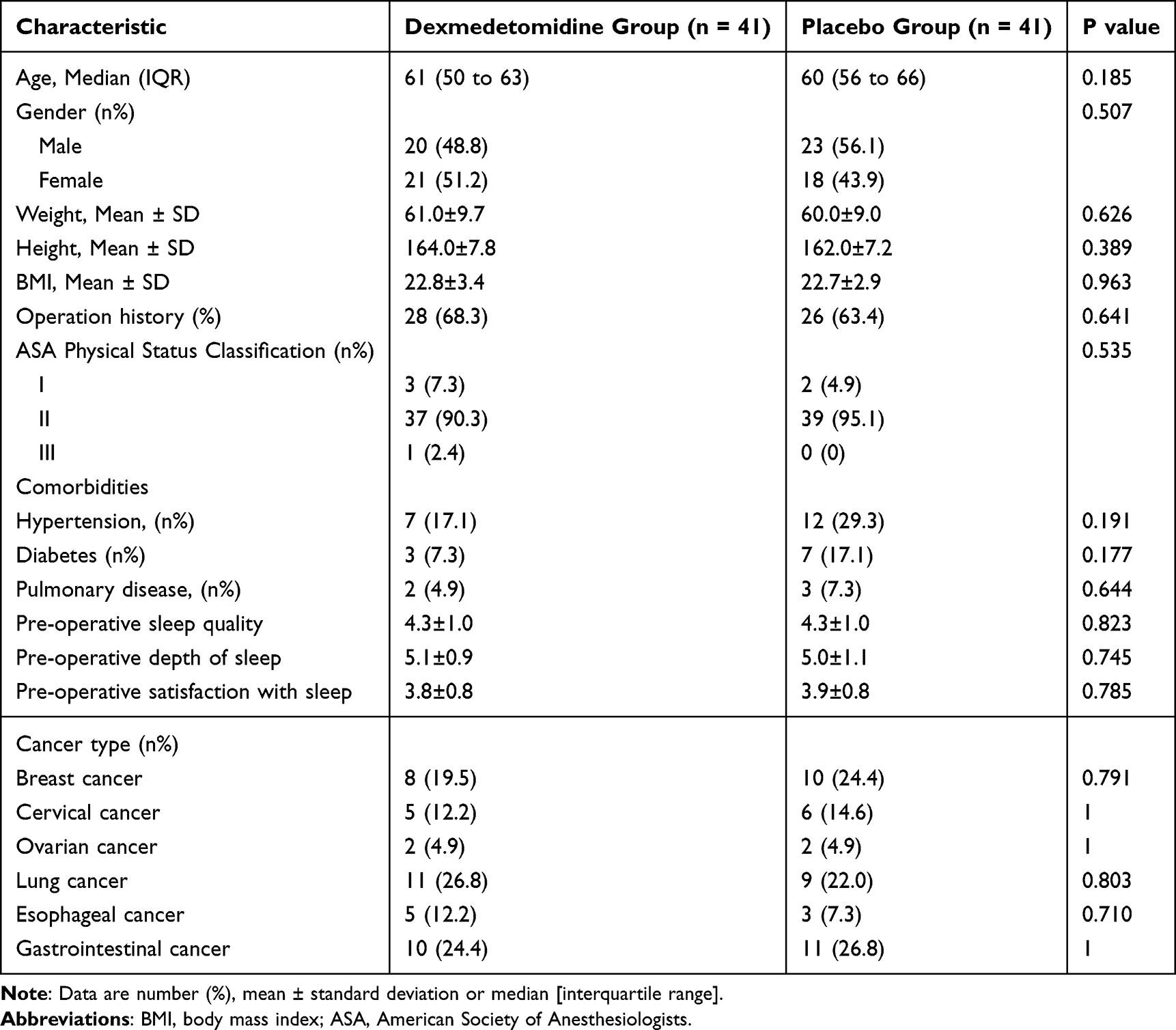 |
Table 1 Patient Demographic and Baseline Characteristics |
 |
Figure 1 Study population flow diagram. |
Patient Satisfaction Scores
The standardized ISAS scores were significantly higher in the dexmedetomidine group than in the placebo group. The median (IQR) ISAS score was 2.7 (2.5–2.8) in the dexmedetomidine group and 2.1 (1.8–2.4) in the placebo group (Figure 2), with a significant between-group difference by the Mann–Whitney U-test (P<0.001). For descriptive purposes, the mean (SD) ISAS score was 2.6±0.3 versus 2.1±0.4, respectively, indicating superior patient-reported satisfaction and perioperative experience in the dexmedetomidine group.
 |
Figure 2 Box plot of ISAS of two groups. |
Patient Postoperative Sleep Quality
The postoperative sleep quality scores were significantly higher in the Dexmedetomidine group than in the Placebo group (4.4±0.8 vs 3.1±0.8, P<0.001). In addition, the dexmedetomidine group experienced significantly improved sleep depth and sleep satisfaction, and fewer awakenings during sleep compared to the placebo group (Figure 3).
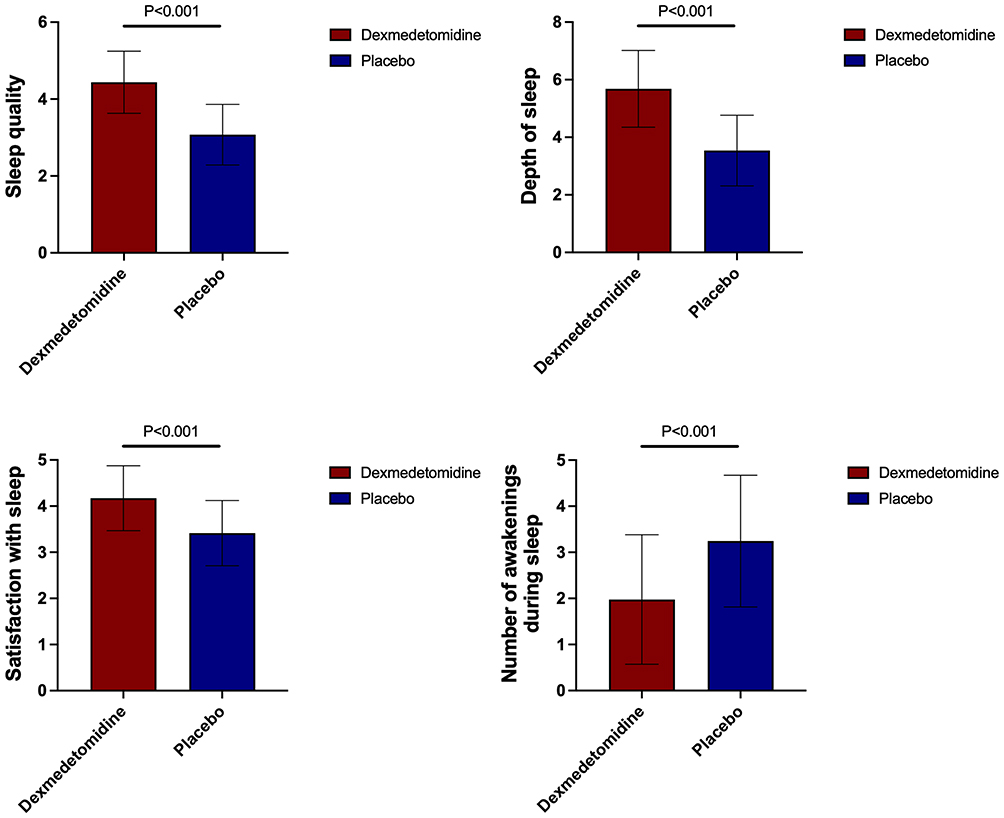 |
Figure 3 Mean score based on SMHSQ between two groups. |
VAS and RSS Scores
There were no significant differences at T0 and T6 in the VAS and RSS scores (Figure 4). Compared with Placebo group, VAS scores in Dexmedetomidine group were significantly lower within 2h after the start of procedure (T1, 1.5±0.6 vs 2.4±0.5, P<0.001; T2, 1.2±0.6 vs 2.1±0.5, P<0.001; T3, 1.8±0.8 vs 2.9±0.7, P<0.001; T4, 0.6±0.6 vs 1.1±0.5, P<0.001; T5, 0.4±0.5 vs 0.8±0.4, P<0.001), and the RSS scores significantly increased at T1 (1.8±0.4 vs1.0±0.2, P<0.001), T2 (2.8±0.7 vs 1.5±0.5, P<0.001), T3 (2.3±0.5 vs 1.2±0.4, P<0.001), T4 (1.8±0.4 vs 1.1±0.3, P<0.001) but not at T5 (1.2±0.4 vs 1.0±0.2, P=0.086).
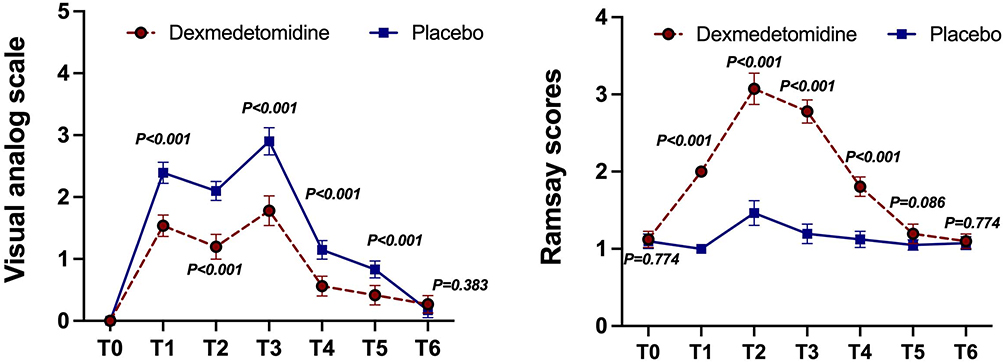 |
Figure 4 Mean (standard deviation) VAS and RSS values changes between the groups at different time points. VAS and RSS were collected at preoperative baseline (T0), surgery start (T1), 10min after the start of surgery (T2), 20min after the start of surgery (T3), end of surgery (T4), 2h after surgery (T5) and 4h after surgery (T6). |
Hemodynamic Results
Hemodynamic changes in two groups during the procedure are shown in (Figure 5). No significant differences were observed in HR and MAP at T0 (P>0.05) between two groups, whereas HR was significantly lower in Dexmedetomidine group than the Placebo group (72.1±7.7 vs 77.1±9.4, P<0.05) at T6. MAP in Dexmedetomidine group than in Placebo group was significantly lower at T1 (92.1±9.8 vs 97.1±12.2, P=0.040), T2 (86.8±9.1 vs 93.5±11.0, P=0.006), T3 (86.4±11.3 vs 92.3±8.5, P=0.014), T4 (89.3±10.4 vs 95.8±12.3, P=0.007), T5 (86.8±12.6 vs 93.8±10.0, P=0.004) and T6 (84.2±12.0 vs 92.2±8.7, P=0.001). No patient in either group experienced MAP < 65 mmHg or required vasoactive support. There were no significant differences between the two groups in SpO2 from T0 to T6.
 |
Figure 5 Hemodynamic parameters of patients in two groups at different time points. T0: preoperative baseline, T1: surgery start, T2: 10min after the start of surgery, T3: 20min after the start of surgery, T4: end of surgery, T5: 2h after surgery and T6: 4h after surgery. |
Incidence of Adverse Events
Overall, 18 sedation-related adverse events were observed by 8 patients in the Dexmedetomidine group and 10 patients in the Placebo group. There was no significant difference in the incidence of perioperative adverse events, including hypertension, hypotension, tachycardia, bradycardia, respiratory depression, headache, nasal discomfort, drowsiness, dizziness, nausea and vomiting.
For surgery-related adverse events, there was no complication on the day of surgery before discharge in the two groups. During follow-up to postoperative day 30, 1 out of 41 (2.4%) patients in the Dexmedetomidine group and 2 out of 41 (4.9%) patients in the Placebo group experienced postoperative complication, as shown in Table 2.
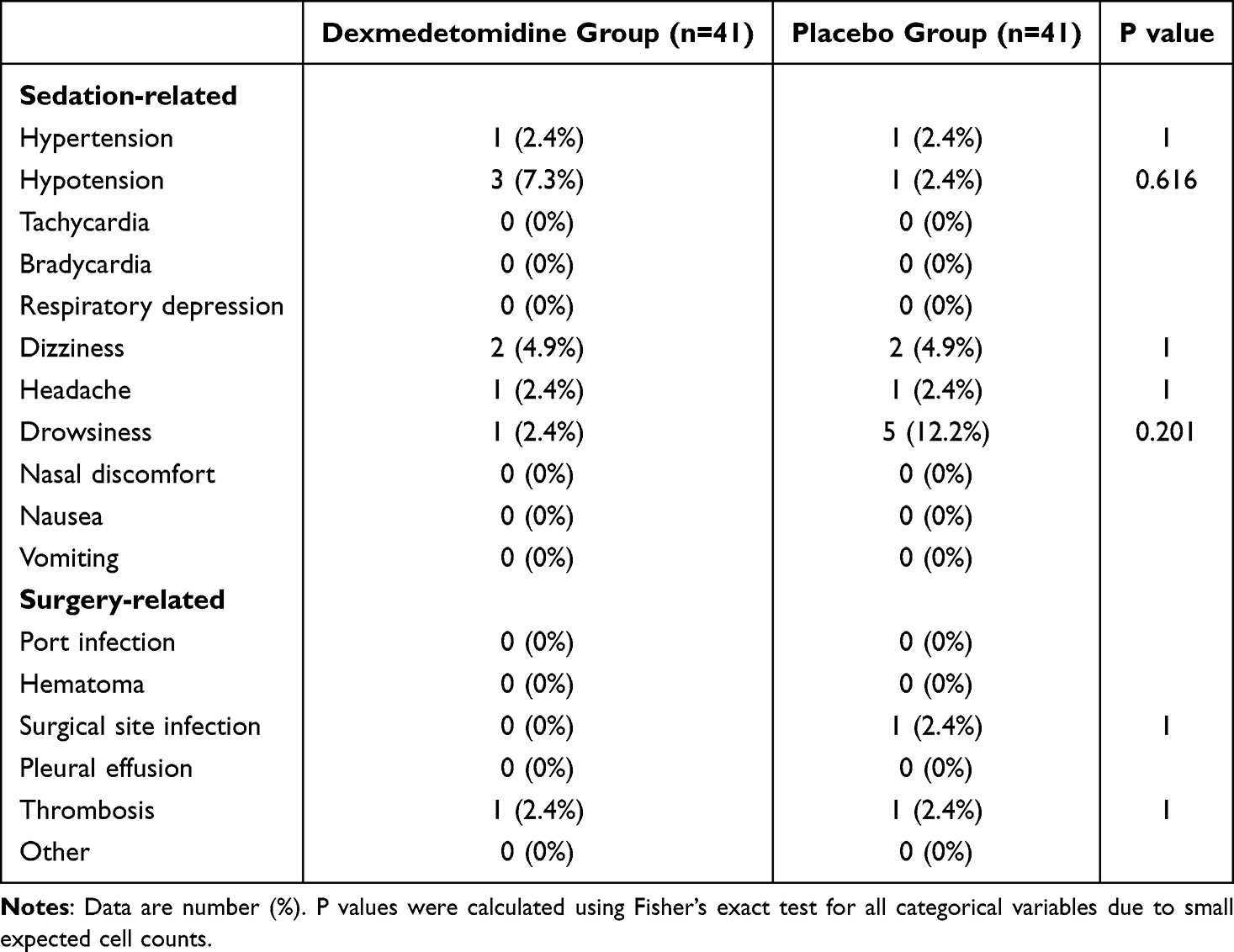 |
Table 2 Incidence of Adverse Events and Postoperative Complications |
Discussion
This trial demonstrates that a standardized dexmedetomidine nasal spray provided effective, well-tolerated procedural sedation and improved postoperative sleep quality in adults undergoing minor surgery under local anesthesia. Unlike compounded intranasal preparations, this ready-to-use spray eliminates the need for dilution or atomization and ensures consistent dosing accuracy. Our results suggested that dexmedetomidine nasal spray could improve patients’ satisfaction scores and sleep quality on the first night after surgery without increasing hemodynamic instability and the incidence of adverse events, thereby optimizing the perioperative experience. Patient satisfaction and patient experience are increasingly recognized as important patient-centered outcomes and are commonly evaluated using structured assessment tools in healthcare quality research.32 In the present study, satisfaction was measured using the ISAS, a validated anesthesia-specific instrument, to quantify patient-reported satisfaction with the procedural experience. Using a standardized satisfaction tool as the primary endpoint strengthens the interpretability and clinical relevance of the observed between-group difference in patient experience.
In our study, patients receiving dexmedetomidine nasal spray achieved deeper cooperative sedation within the expected onset window. Compared with the placebo group, 82.9% of patients in dexmedetomidine group achieved an RSS score of 3 points or higher within 45 min after administration, and the difference was statistically significant. This clinical profile is consistent with the pharmacologic characteristics of dexmedetomidine, which acts via postsynaptic α2-adrenergic receptors in the locus coeruleus to induce a sleep-like, easily arousable, and cooperative sedative state, typically without respiratory depression and with modest hemodynamic effects.17,33 More broadly, intranasal administration offers numerous practical advantages in procedural settings, such as avoiding injection pain and risks associated with intravenous access, while maintaining high patient acceptance, and has been used for multiple drugs, including fentanyl, sufentanil, ketamine, midazolam, and naloxone.34,35 Dexmedetomidine was approved by the US FDA in 2008 for sedation in perioperative and procedural settings,36 and our data support its suitability for noninvasive procedural sedation when delivered intranasally in a standardized formulation.
Our results also extend existing evidence on intranasal dexmedetomidine by demonstrating efficacy in an adult outpatient procedural population. Previous pharmacokinetic/pharmacodynamic studies reported that intranasal dexmedetomidine has a slower and more gradual onset than intravenous administration, but once sedation is established, the depth of sedation can be comparable.37 Consistently, Padmasree M.K et al has shown that both intravenous and intranasal dexmedetomidine attenuate stress responses to stimulating procedures such as laryngoscopy.38 Although the majority of intranasal dexmedetomidine studies have focused on pediatric populations,39–41 where benefits have been observed for emergence delirium and pain control,42 our findings indicate that similar cooperative sedation and patient-centered benefits can be achieved in adults undergoing minor procedures under local anesthesia.
One particularly noteworthy finding from our study was that postoperative sleep quality improved on the first night after surgery. Using the SMHSQ, we observed not only improved overall sleep quality but also increased sleep depth, improved sleep satisfaction, and reduced the number of awakenings during sleep in the dexmedetomidine group. These results align with prior adult studies suggesting that intranasal dexmedetomidine can reduce sleep disturbances among patients with preoperative anxiety-related insomnia,26,43 and with Huang et al’s systematic review evidence supporting dexmedetomidine’s role in improving postoperative sleep quality.44 Mechanistically, dexmedetomidine may promote more physiologic sleep-like states through central α2-mediated pathways and may reduce perioperative sympathetic arousal, which together could contribute to better first-night recovery.
From a drug delivery perspective, our study provides practical evidence to support standardized, device-free intranasal formulations. In previous studies, intranasal dexmedetomidine was commonly delivered as syringe drops, nebulization, or via a nasal mucosal atomization device (MAD).25,26,45 However, drops and nebulization may lead to variable absorption, whereas MAD performance can be influenced by formulation characteristics. In our study, a pre-formulated metered-dose spray enabled simplified administration and dosing accuracy without the need for additional devices. Based on pharmacokinetic data in healthy subjects, the median time to maximum plasma concentration after a 100 μg dexmedetomidine nasal spray is approximately 30–45 min,27 supporting our dosing protocol of administration 30 min before surgery and our observation of clinically meaningful sedation within 45 min. Importantly, while MAP and HR were modestly reduced compared with placebo, all values remained within clinically acceptable limits (MAP ≥65 mmHg). Moreover, there was no significant between-group difference in adverse event incidence and no serious adverse events occurred. These findings collectively support the safety, tolerability, and hemodynamic stability of standardized intranasal dexmedetomidine for outpatient procedural sedation. However, several limitations must be considered. Firstly, this study had a relatively small sample size and included only adult patients. Pharmacokinetic studies were not performed, and no active sedative control group was included. Secondly, this study utilized a standardized fixed dose of 100 µg dexmedetomidine for all patients, which does not account for individual variations in body weight. As weight can significantly influence the pharmacokinetics and pharmacodynamics of dexmedetomidine, this fixed-dose approach may have contributed to variable sedation depths across our study population. Future studies incorporating weight-adjusted dosing are necessary to refine the optimal therapeutic window for nasal spray formulations. In addition, individual variability in nasal absorption may affect the onset time and depth of sedation. These variability (eg, variations in nasal patency or mucosal condition, and drug deposition related to administration technique) may contribute to heterogeneity in sedation responses and may partially explain why 17.1% of patients did not achieve an RSS score ≥3 within the pre-specified assessment time. Future multicenter studies with larger, more diverse populations are warranted to determine the optimal dosing strategy and explore the use of nasal dexmedetomidine in elderly or high-risk patients. Although the nasal spray evaluated in this study is currently available in China, the concept of standardized, non-invasive sedative delivery has broad applicability and may inform future formulations.
Conclusion
In conclusion, the standardized dexmedetomidine nasal spray represents a feasible, patient-friendly, and well-tolerated approach for light-to-moderate procedural sedation. In adults undergoing minor procedures under local anesthesia, it improved patient satisfaction and significantly enhanced postoperative sleep quality on the first postoperative night, without increasing hemodynamic instability or adverse events. Its consistent dosing, noninvasive delivery, and favorable tolerability profile make it a promising option for outpatient anesthesia and minor surgical procedures.
Data Sharing Statement
For reasonable data requests, contact the corresponding author by Email (ZY. W, [email protected]).
Ethics Approval and Informed Consent
The trial protocol was authorized by the Ethics Committee of Zhongshan Hospital (Xiamen branch) Fudan University (Approval No. B2024-100R) and registered at the Chinese Clinical Trial Registry (ChiCTR2400093619). This study was conducted in accordance with the Declaration of Helsinki. All participating patients gave written informed consent.
Funding
There is no funding to report. This was an investigator-initiated, non-commercial study with no external financial support and no industry sponsorship.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tabatabaie O, Kasumova GG, Eskander MF, et al. Totally implantable venous access devices: a review of complications and management strategies. Am J Clin Oncol. 2017;40(1):94–13. doi:10.1097/COC.0000000000000361
2. Zhang KC, Chen L, Chinese A CR, et al. Chinese expert consensus and practice guideline of totally implantable access port for digestive tract carcinomas. World J Gastroenterol. 2020;26(25):3517–3527. doi:10.3748/wjg.v26.i25.3517
3. Biffi R, Pozzi S, Agazzi A, et al. Use of totally implantable central venous access ports for high-dose chemotherapy and peripheral blood stem cell transplantation: results of a monocentre series of 376 patients. Ann Oncol. 2004;15(2):296–300. doi:10.1093/annonc/mdh049
4. Song X, Chen S, Dai Y, et al. A novel incision technique of a totally implanted venous access port in the upper arm for patients with breast cancer. World J Surg Oncol. 2023;21(1):162. doi:10.1186/s12957-023-03043-4
5. Feo CF, Ginesu GC, Bellini A, et al. Cost and morbidity analysis of chest port insertion in adults: outpatient clinic versus operating room placement. Ann Med Surg Lond. 2017;21:81–84. doi:10.1016/j.amsu.2017.07.056
6. Schuld J, Richter S, Moussavian M, et al. [A totally implantable venous access device. Implantation in general or local anaesthesia? A retrospective cost analysis]. Zentralbl Chir. 2009;134(4):345–349. doi:10.1055/s-0028-1098787
7. Steinkraus KC, Feldmann H, Hunold LS, et al. Impact of virtual reality hypnosedation on perioperative pain and anxiety in port implantation under local anesthesia: a randomized controlled pilot trial (VIP Trial). Perioper Med. 2024;13(1):101. doi:10.1186/s13741-024-00454-z
8. Aust H, Eberhart L, Sturm T, et al. A cross-sectional study on preoperative anxiety in adults. J Psychosom Res. 2018;111:133–139. doi:10.1016/j.jpsychores.2018.05.012
9. Euteneuer F, Kampmann S, Rienmüller S, et al. Patients’ desires for anxiolytic premedication - an observational study in adults undergoing elective surgery. BMC Psychiatry. 2022;22(1):193. doi:10.1186/s12888-022-03845-y
10. Chang DH, Kabbasch C, Bovenschulte H, et al. [Experiences with power-injectable port systems: complications, patient satisfaction and clinical benefit]. Rofo. 2013;185(5):454–460. doi:10.1055/s-0032-1330713
11. Gu X, Zhang Y, Wei W, et al. Effects of preoperative anxiety on postoperative outcomes and sleep quality in patients undergoing laparoscopic gynecological surgery. J Clin Med. 2023;12(5):1835. doi:10.3390/jcm12051835
12. Stamenkovic DM, Rancic NK, Latas MB, et al. Preoperative anxiety and implications on postoperative recovery: what can we do to change our history. Minerva Anestesiol. 2018;84(11):1307–1317. doi:10.23736/S0375-9393.18.12520-X
13. Tola YO, Chow KM, Liang W. Effects of non-pharmacological interventions on preoperative anxiety and postoperative pain in patients undergoing breast cancer surgery: a systematic review. J Clin Nurs. 2021;30(23–24):3369–3384. doi:10.1111/jocn.15827
14. Chang DH, Hiss S, Herich L, et al. Implantation of venous access devices under local anesthesia: patients’ satisfaction with oral lorazepam. Patient Prefer Adherence. 2015;9:943–949. doi:10.2147/PPA.S80330
15. Sterkers N, Chabrol JL, De Troyer J, et al. Hypnosis as adjunct therapy to conscious sedation for venous access device implantation in breast cancer: a pilot study. J Vasc Access. 2018;19(4):382–386. doi:10.1177/1129729818757975
16. Hinkelbein J, Lamperti M, Akeson J, et al. European society of anaesthesiology and European board of anaesthesiology guidelines for procedural sedation and analgesia in adults. Eur J Anaesthesiol. 2018;35(1):6–24. doi:10.1097/EJA.0000000000000683
17. Weerink MAS, Struys MMRF, Hannivoort LN, et al. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
18. Keller LA, Merkel O, Popp A. Intranasal drug delivery: opportunities and toxicologic challenges during drug development. Drug Deliv Transl Res. 2022;12(4):735–757. doi:10.1007/s13346-020-00891-5
19. Yao Y, Sun Y, Lin J, et al. Intranasal dexmedetomidine versus oral midazolam premedication to prevent emergence delirium in children undergoing strabismus surgery: a randomised controlled trial. Eur J Anaesthesiol. 2020;37(12):1143–1149. doi:10.1097/EJA.0000000000001270
20. Shen F, Zhang Q, Xu Y, et al. Effect of intranasal dexmedetomidine or midazolam for premedication on the occurrence of respiratory adverse events in children undergoing tonsillectomy and adenoidectomy: a randomized clinical trial. JAMA Network Open. 2022;5(8):e2225473. doi:10.1001/jamanetworkopen.2022.25473
21. Liu S, Wang Y, Zhu Y, et al. Safety and sedative effect of intranasal dexmedetomidine in mandibular third molar surgery: a systematic review and meta-analysis. Drug Design Develop Ther. 2019;13:1301–1310. doi:10.2147/DDDT.S194894
22. Yuan Y-J, Zhou P, Xia F, et al. Intranasal dexmedetomidine combined with local anesthesia for conscious sedation during breast lumpectomy: a prospective randomized trial. Oncol Lett. 2020. doi:10.3892/ol.2020.11938
23. Seppänen S-M, Kuuskoski R, Mäkelä KT, et al. Intranasal dexmedetomidine reduces postoperative opioid requirement in patients undergoing total knee arthroplasty under general anesthesia. J Arthroplasty. 2021;36(3):978–985.e1. doi:10.1016/j.arth.2020.09.032
24. Xu X, Cao Y, Wu Y, et al. Intranasal dexmedetomidine in elderly patients (Aged > 65 Years) during maxillofacial surgery: sedative properties and safety analysis. J Oral Maxillofacial Surg. 2022;80(3):443–455. doi:10.1016/j.joms.2021.10.013
25. Ding X, Shi D, Cai H, et al. Intranasal atomized dexmedetomidine in combination with intranasal atomized butorphanol for dressing change sedation and analgesia in adult burn patients: a randomized clinical trial. J Burn Care Res. 2025;46(2):341–348. doi:10.1093/jbcr/irae158
26. Yang WY, Huang K, Lin Z-J, et al. Intranasal dexmedetomidine for the management of preoperative anxiety-related insomnia: a randomized, three-blinded, clinical trial compared with lorazepam and placebo. Drug Des Devel Ther. 2024;18:6061–6073. doi:10.2147/DDDT.S487463
27. Kuang Y, Wang S-Y, Wang M-N, et al. Safety, pharmacokinetics/pharmacodynamics, and absolute bioavailability of dexmedetomidine hydrochloride nasal spray in healthy subjects: a randomized, parallel, escalating dose study. Front Pharmacol. 2022;13:871492. doi:10.3389/fphar.2022.871492
28. Gao J, Wang F, Wang X, et al. Safety and efficacy of a novel dexmedetomidine nasal spray for pre-anesthetic sedation in children: a randomized, double-blind, placebo-controlled trial. BMC Anesthesiol. 2024;24(1). doi:10.1186/s12871-024-02708-1
29. Dexter F, Aker J, Wright WA. Development of a measure of patient satisfaction with monitored anesthesia care: the Iowa satisfaction with anesthesia scale. Anesthesiology. 1997;87(4):865–873. doi:10.1097/00000542-199710000-00021
30. Dawson R, von Fintel N, Nairn S. Sedation assessment using the Ramsay scale. Emerg Nurse. 2010;18(3):18–20. doi:10.7748/en2010.06.18.3.18.c7825
31. Ellis BW, Johns MW, Lancaster R, et al. The St. Mary’s Hospital sleep questionnaire: a study of reliability. Sleep. 1981;4(1):93–97. doi:10.1093/sleep/4.1.93
32. Moldovan F, Moldovan L. Assessment of patient matters in healthcare facilities. Healthcare. 2024;12(3):325.
33. Wang K, Wu M, Xu J, et al. Effects of dexmedetomidine on perioperative stress, inflammation, and immune function: systematic review and meta-analysis. Br J Anaesth. 2019;123(6):777–794. doi:10.1016/j.bja.2019.07.027
34. Corrigan M, Wilson SS, Hampton J. Safety and efficacy of intranasally administered medications in the emergency department and prehospital settings. Am J Health Syst Pharm. 2015;72(18):1544–1554. doi:10.2146/ajhp140630
35. Wolfe TR, Bernstone T. Intranasal drug delivery: an alternative to intravenous administration in selected emergency cases. J Emerg Nurs. 2004;30(2):141–147. doi:10.1016/j.jen.2004.01.006
36. Gao T, Liu X, Liu S, et al. Antianxiety effects of dexmedetomidine: systematic review and meta-analysis. Eur Arch Psychiatry Clin Neurosci. 2025. doi:10.1007/s00406-025-02017-9
37. Hoy SM, Keating GM. Dexmedetomidine: a review of its use for sedation in mechanically ventilated patients in an intensive care setting and for procedural sedation. Drugs. 2011;71(11):1481–1501. doi:10.2165/11207190-000000000-00000
38. Li A, Yuen VM, Goulay-Dufaÿ S, et al. Pharmacokinetic and pharmacodynamic study of intranasal and intravenous dexmedetomidine. Br J Anaesth. 2018;120(5):960–968. doi:10.1016/j.bja.2017.11.100
39. Padmasree MK, Nelamangala K. A comparative study between intranasal and intravenous dexmedetomidine and hemodynamic responses during endotracheal intubation. Cureus. 2023;15(2):e35196. doi:10.7759/cureus.35196
40. Ericksen AM, Kane TD, Tubog TD. Intranasal dexmedetomidine compared with intranasal midazolam for pediatric emergence delirium: a systematic review and meta-analysis. J Perianesth Nurs. 2025;40(5):1375–1385e2. doi:10.1016/j.jopan.2025.01.011
41. Wu H, Wu P, Xiang L, et al. Effect of different intranasal dexmedetomidine doses on pediatric postoperative delirium and agitation: network meta-analysis. Pediatr Res. 2025;98(4):1266–1275. doi:10.1038/s41390-025-03851-2
42. Liao Y, Xie S, Zhuo Y, et al. Intranasal dexmedetomidine-esketamine combination premedication versus monotherapy for reducing emergence delirium and postoperative behavioral changes in pediatric tonsillectomy and/or adenoidectomy: a randomized controlled trial. Drug Des Devel Ther. 2024;18:4693–4703. doi:10.2147/DDDT.S488706
43. Dai C, Zhao X, Li A, et al. Comparative evaluation of intravenous versus intranasal dexmedetomidine on emergence delirium and hemodynamics in pediatric patients undergoing adenotonsillectomy: a randomized controlled trial. Front Pharmacol. 2025;16:1543344. doi:10.3389/fphar.2025.1543344
44. Zeng W, Chen L, Liu X, et al. Intranasal dexmedetomidine for the treatment of pre-operative anxiety and insomnia: a prospective, randomized, controlled, and clinical trial. Front Psychiatry. 2022;13:816893. doi:10.3389/fpsyt.2022.816893
45. Huang X, Lin D, Sun Y, et al. Effect of dexmedetomidine on postoperative sleep quality: a systematic review. Drug Des Devel Ther. 2021;15:2161–2170. doi:10.2147/DDDT.S304162
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.