Back to Journals » Patient Preference and Adherence » Volume 19
A Novel Screening Method to Prioritise Cardiovascular Patients Receiving a Pharmaceutical Care Intervention and the Effects on Patients’ Difficulties with Managing Their Drug Treatment
Authors Jungreithmayr V ![]() , Bittmann JA
, Bittmann JA ![]() , Wurmbach VS, Degen M, Dierkes T, Obersteiner S, Bruns B, Estel S, Bugaj TJ, Seidling HM
, Wurmbach VS, Degen M, Dierkes T, Obersteiner S, Bruns B, Estel S, Bugaj TJ, Seidling HM ![]()
Received 15 June 2025
Accepted for publication 9 October 2025
Published 28 November 2025 Volume 2025:19 Pages 3807—3818
DOI https://doi.org/10.2147/PPA.S543261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Viktoria Jungreithmayr,1 Janina A Bittmann,1 Viktoria S Wurmbach,1 Miriam Degen,1– 3 Theresa Dierkes,1 Sofia Obersteiner,1 Bastian Bruns,4,5 Stephanie Estel,4 Till Johannes Bugaj,4,* Hanna M Seidling1,*
1Heidelberg University, Medical Faculty Heidelberg / Heidelberg University Hospital, Internal Medicine IX - Department of Clinical Pharmacology and Pharmacoepidemiology, Cooperation Unit Clinical Pharmacy, Heidelberg, 69120, Germany; 2Division of Clinical Epidemiology and Aging Research, German Cancer Research Center (DKFZ), Heidelberg, 69120, Germany; 3Faculty of Medicine, University of Heidelberg, Heidelberg, 69115, Germany; 4Department of General Internal Medicine and Psychosomatics, Heidelberg University Hospital, Heidelberg, 69120, Germany; 5Department of Cardiology, Angiology and Pneumology, Heidelberg University Hospital, Heidelberg, 69120, Germany
*These authors contributed equally to this work
Correspondence: Hanna M Seidling, Heidelberg University, Medical Faculty Heidelberg / Heidelberg University Hospital, Internal Medicine IX - Department of Clinical Pharmacology and Pharmacoepidemiology, Cooperation Unit Clinical Pharmacy, Im Neuenheimer Feld 410, Heidelberg, 69120, Germany, Tel +49 0 6221 56 38736, Fax +49 0 6221 56 4642, Email [email protected]
Purpose: Hospitalisation is usually accompanied by changes in patients’ drug regimen followed by increased information need. To identify inpatients most suitable for pharmaceutical care interventions addressing these information needs, different prioritisation strategies exist. Here, we present a novel screening method taking particularly patient-reported needs into account. We aimed to test (i) whether the screening method is able to identify patients who benefit most from an intervention, and (ii) whether the intervention can actually reduce patients’ difficulties with managing their drug treatment.
Patients and Methods: This study comprised of an admission screening, a pharmaceutical care intervention during the inpatient stay, and a follow-up phone call after discharge. During screening, patients answered questionnaires regarding e. g., their beliefs about medicine, adherence, and complexity of drug treatment. According to predefined criteria, patients were selected for the intervention. During intervention, patients received counselling and information leaflets according to their needs. After the inpatient visit, all screened patients were contacted for a follow-up call. During intervention and follow-up, patients were asked applicable key questions on factors potentially increasing complexity of drug treatment to identify difficulties with managing their drug treatment.
Results: Among 128 screened patients, 105 were deemed suitable for the intervention. Patients receiving the intervention showed less difficulties with managing their drug treatment after discharge (mean difficulties during intervention = 1.3 vs mean difficulties during follow-up = 0.9, p = 0.040). However, at follow-up, the number of patients’ difficulties did not differ between patients suitable or unsuitable for the intervention and between suitable patients receiving or not receiving the intervention (p = 0.434).
Conclusion: The novel screening method identified many patients with high information needs, but its effectiveness for prioritisation is limited. While the intervention reduced patients’ difficulties with managing drug treatment over time, no significant differences were observed between intervention groups.
Keywords: screening method, pharmaceutical care intervention, tertiary care, difficulties with managing drug treatment
Introduction
Usually, inpatient care is only a brief interruption in the long-term care of patients in primary care. However, hospitalisation continues to impact primary care, especially regarding patients’ medication. During most inpatient stays, a patient’s medication list is adapted with changes, additions, or removals of medication orders.1 Yet, after discharge, patients are typically required to take over responsibility for their drug administration and adhere to these changes made. This makes it important to prepare patients even during their hospital stay in the best possible way for the time after they are discharged from hospital. However, patients showed to be inadequately informed about their medication upon discharge.2 As a result, discharged patients often struggle to manage their new medication regimen correctly.3,4 Nonadherence, wrong drug application, and other medication errors can lead to avoidable patient harm and hospital readmissions.5,6 Vice versa, pharmaceutical care interventions during transitions of care have been shown effective in reducing drug-related problems and the use of healthcare services.7,8 Patients with cardiovascular diseases are both a large and important target group, as adherence to preventive therapies is particularly poor.9 Pharmaceutical care interventions can play an important role in improving adherence, controlling risk factors and ultimately preserving life.10 However, one difficulty with sustaining intervention effects is the lack of post-discharge monitoring and follow-up of patients. Additionally, staffing shortages and time constraints limit the sustained and widespread deployment of pharmaceutical care interventions in many hospitals around the globe.11 Strategies to prioritise those patients who benefit the most from a pharmaceutical care intervention are therefore needed. Existing prioritisation strategies mostly focus on (semi-)automatized detection of certain high-risk scenarios in patients’ electronic health records e. g., high-risk drugs, patients’ age, or comorbidities. However, persisting problems with these strategies include their low specificity due to the inclusion of quite ubiquitous parameters and the dependence of the scoring results on the individual assessment and expertise of the pharmacist.12 Additionally, many tools are meant for stratifying patients in terms of the order they receive a pharmaceutical care intervention, rather than actually prioritising which patients receive an intervention and which do not.12
In this study, we developed an alternative strategy to prioritise patients for pharmaceutical care interventions. According to patients’ self-declared needs and difficulties, enquired through several questionnaires, we aimed to identify the patients benefitting the most of a pharmaceutical care intervention. A three-step study concept was chosen to prioritise patients, perform the pharmaceutical care intervention, and follow-up with the patients after discharge. The aim of this study is to test (i) whether this novel screening method is able to identify patients who benefit from a pharmaceutical care intervention concerning the management of their drug treatment in the inpatient setting, and (ii) whether the intervention can actually reduce patients’ difficulties with managing their drug treatment even after discharge.
Methods
Setting
This prospective, pseudo-controlled trial was performed at an inpatient ward at Heidelberg University Hospital where pharmacists were involved in routine patient care. The study ward is an integrated cardiologic general internal medicine ward with a focus on cardiac, vascular, and pulmonary diseases. As general internal medicine at Heidelberg University Hospital is provided by the (combined) Department of General Internal Medicine and Psychosomatics, this ward also has a great deal of expertise in psychosocial co-treatment of somatic diseases, such as depression or anxieties. This results in a heterogenous patient collective allocated to 20 beds. Patients are predominantly older people (mean age 68.4 years), experiencing polypharmacy (mean number of drugs 11.8) and stay at the ward for a mean of 5.4 days. The study was approved by the Ethics Committee of the Medical Faculty Heidelberg (S-576/2021) and was registered a priori at the German Clinical Trials Registry (DRKS00026088). Patients received written and oral study information upon screening. Informed consent was obtained prior to study commencement. The study complies with the Declaration of Helsinki.
Design
This study was set up in collaboration with the Department of Clinical Pharmacology and Pharmacoepidemiology and the Department of General Internal Medicine and Psychosomatics. The study design was based upon a pilot study. According to this pilot study, planned methodological approaches like the measurement of patients’ difficulties with managing their drug treatment or the suitability criteria for the intervention were adapted.13 The final study concept comprised three steps: (I) an admission screening, (II) a pharmaceutical care intervention during the inpatient stay, and (III) a follow-up phone call after discharge (Figure 1). The study design and parts of the results were presented as a poster at two congresses.14,15
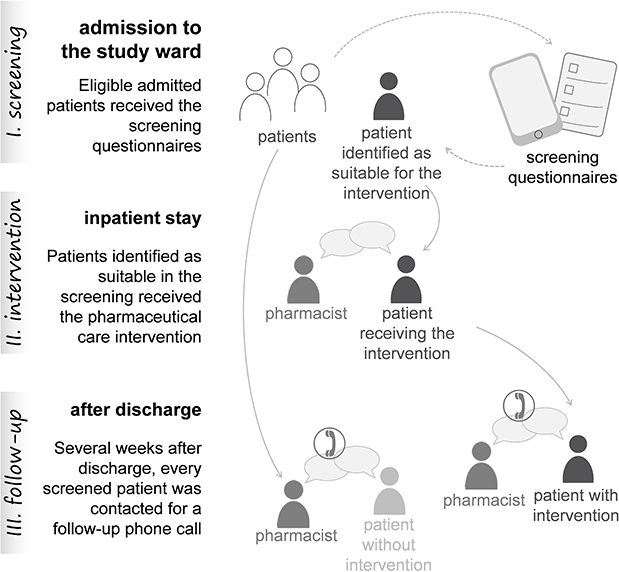 |
Figure 1 Study procedure following the three steps: screening, intervention, and follow-up. |
Screening
Patients were eligible for the screening if they were admitted to the study ward and linguistically and cognitively able to answer the screening questionnaires and participate in the intervention. Depending on patients’ abilities, the questionnaires were either distributed in a paper-based, self-administered version or all questions were asked by a member of the study team and patients’ answers were entered electronically in a tablet version. For instance, patients with diseases that affect motor skills e. g., Parkinson’s disease, or patients with difficulties reading were screened by a member of the study team. This approach ensured we screened a greater number of patients than would have been possible with a self-administered version alone. The screening questionnaire consisted of the German version of the Beliefs about Medicines Questionnaire (BMQ-D),16,17 the A-14 scale for assessment of adherence and individual barriers,18 and self-developed questions on patient involvement, complexity of drug treatment, and general key questions on potential difficulties with managing their drug treatment. In total, the screening comprised 41 – 43 questions, depending on their applicability to the patients. The majority of the self-developed questions, namely those on complexity of drug treatment and the general key questions on difficulties with managing their drug treatment, were rigorously developed, pilot tested, and applied in former studies.19 Additionally, patients had the option to indicate the wish for advice regarding their drug administration (see Supplement 1 for the full questionnaire). According to predetermined criteria, patients were deemed suitable for a pharmaceutical care intervention. Suitability for the intervention was fulfilled if at least two of the following criteria were fulfilled: (i) the BMQ-D scored <19 for the necessity-scale or >12 for the concerns-scale, (ii) below 50 points were reached on the A14 scale, (iii) one or more questions on patient activation were answered with “disagree strongly” or “disagree”, (iv) complexity of drug treatment was rated as “very complicated” or “rather complicated”, (v) at least one general key question on difficulties with managing their drug treatment was answered with “yes”, or (vi) the patient indicated a wish for advice regarding his/her drug administration, or (vii) the patient asked a specific question related to pharmaceutical-pharmacological aspects during the screening, or (viii) the patient got new medication prescribed for which a self-developed information leaflet (one-pager or drug administration leaflet) was available.
Intervention
If a patient was suitable for the intervention, it was prepared and adapted according to the information gathered during the screening and the patient’s current medication list (Table 1). The intervention was performed by either a) a pharmacist, b) a pharmacy trainee in their pre-registration year, or c) both of them and consisted of an in-person consultation with the patient where relevant information material was distributed. The pharmaceutical care intervention was performed by means of an interview guide (Supplement 2). To identify difficulties with managing their drug treatment, specific key questions on factors potentially increasing complexity of drug treatment for individual patients – so-called complexity factors – were asked. According to the patients’ current inpatient medication list, we identified which of the total 43 complexity factors were applicable and assessed their relevance for patients asking the specific key questions rigorously developed in a former study.19 For example, if the patient was prescribed half a tablet, the key question “Do you find it difficult to split your tablets consistently into pieces that have the same size?” was asked. If patients considered the key question as difficult, it was deemed as having a difficulty with managing their drug treatment. Following, solutions were proposed how the difficulties can be addressed which consisted of specific counselling and/or the distribution of information material. Also, one open question regarding difficulties in administering their medication was asked to each patient, as well as a question on remaining open questions. Several information materials were developed prior to the study start: one-pagers, drug administration leaflets, and a patient diary. For a selection of drugs that are commonly newly prescribed at the study ward, one-pagers that contain essential information in plain language were developed by two pharmacists using the dual-control principle and approved by a senior physician. In total, 13 one-pagers on the following active ingredients were developed: acetyl-salicylic acid, atorvastatin, carvedilol, clopidogrel, fluvastatin, metoprolol, nitro spray, pravastatin, ramipril, rivaroxaban, rosuvastatin, simvastatin, and ticagrelor. The one-pagers covered information on the indication, mode of action, administration, storage, adverse reactions, consequences of non-adherence, circumstances under which the drug must not be taken, and actions when a dose was missed or taken more than prescribed. The drug administration leaflets were developed in a rigorous, 4-step process in earlier studies and included plain language information and infographics on drug administration of different dosage forms.20,21 The patient diary served as a documentation tool for the patients to track their own medication taking and potential side effects. After the intervention, the conducting pharmacist evaluated whether and which of 24 risk factors for nonadherence were addressed by the patient (see Supplement 2). This was based on a pre-defined list of risk factors contributing to nonadherence, which were identified through a preceding literature review.22 All patients suitable for the intervention were visited for the intervention directly at their beds. Patients did not receive the intervention if they were transferred, discharged, unresponsive, or uncapable of participating in the intervention at the time of visit.
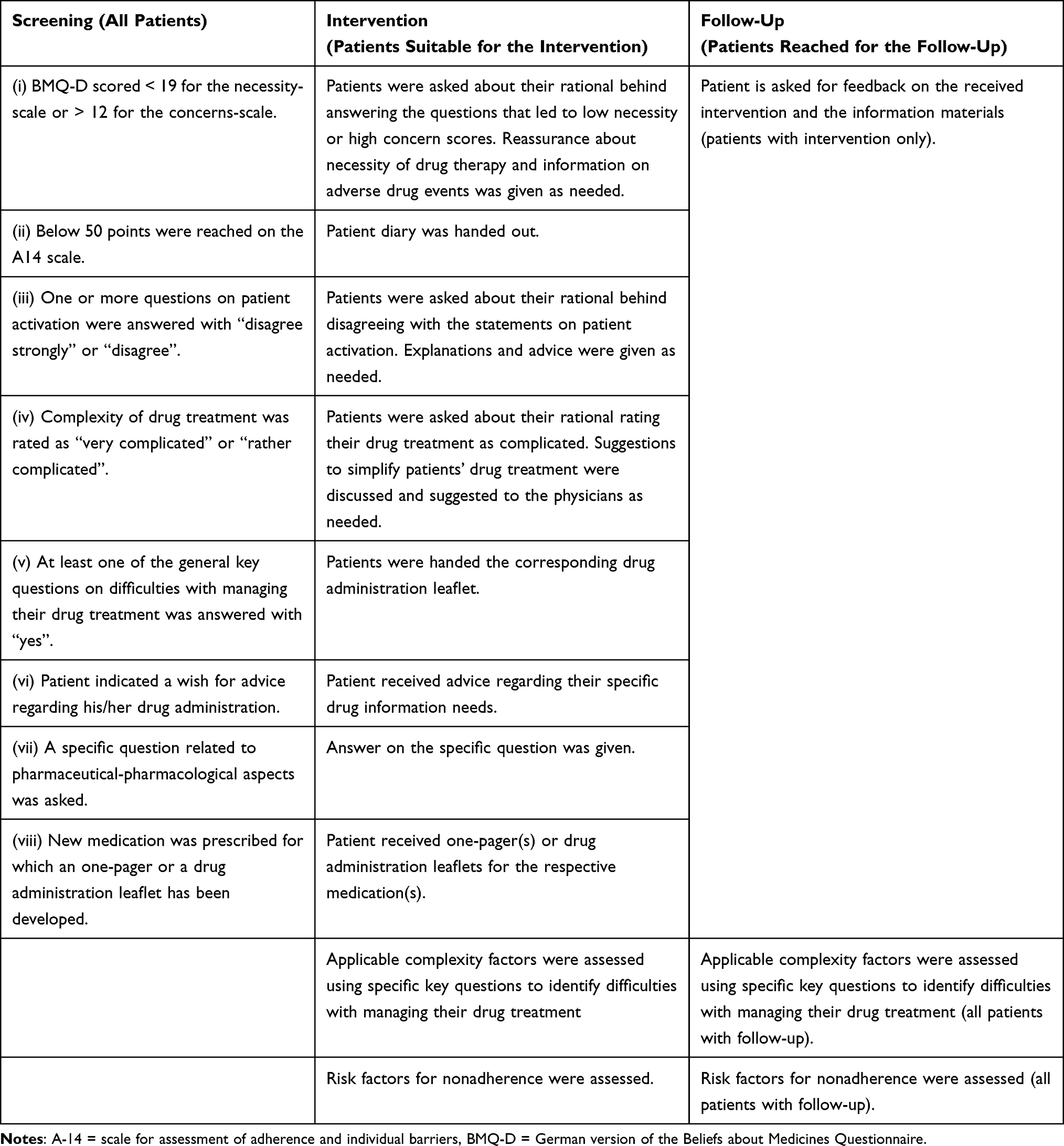 |
Table 1 Possible Constellations of Screening Results and Derived Intervention and Follow-up Components |
Follow-Up
At least 6 weeks after discharge, all screened patients were contacted for a follow-up phone call. In preparation of the follow-up call, the patient’s discharge medication list and, if applicable, the content of the intervention was consulted. The follow-up calls were performed according to an interview guide and, again, applicable specific key questions and the two open questions on difficulties in administering medication and remaining open questions were asked (Supplement 3). Additionally, a question on patients’ symptoms or side effects was asked with the aim to understand patients’ well-being with and knowledge of their drug therapy. No formal tools or causality assessment were used to assess patients’ side effects. Patients who received the intervention were asked about their opinions on the intervention, the received information material, and the patient diary, where applicable. Also, risk factors for nonadherence were assessed after the follow-up phone call. If a patient could not be reached three times on different days and time points, he or she was deemed lost to follow up.
Data Collection
Screening questionnaires answered electronically were automatically uploaded in a database. Paper-based screening questionnaires were manually transferred into the electronic database. Interventions and follow-up phone calls were manually documented on paper-based interview guides. Data was manually entered into Microsoft® Excel® 2019 (version 16.0) sheets.
Data Analysis
All questionnaires without missing values were used to calculate the scores for the questionnaire scales. We calculated the median and interquartile range for every question or overarching scale.
We performed descriptive, exploratory analyses of the intervention and follow-up contents. No a priori sample size calculation was performed due to the exploratory nature of the study. To analyse the results, patients were characterised according to six groups:
- group A = patients suitable for the intervention, receiving the intervention and the follow-up;
- group B = patients suitable for the intervention, receiving the intervention but not the follow-up;
- group C = patients suitable for the intervention, not receiving the intervention but receiving the follow-up;
- group D = patients suitable for the intervention, receiving neither the intervention nor the follow-up;
- group E = patients unsuitable for the intervention, receiving the follow-up;
- group F = patients unsuitable for the intervention, not receiving the follow-up.
Comparisons between time points for patients receiving both the intervention and the follow-up were calculated with Wilcoxon test. Comparisons between patient groups at the follow-up were calculated using Kruskal–Wallis test. A two-tailed p-value < 0.05 was considered as statistically significant. Data analysis was performed with IBM® SPSS® Statistics (version 29). The R packages tidyverse, ggpubr, and ggplot2 (version 4.3.1, R Foundation for Statistical Computing, Vienna, Austria) and Microsoft® PowerPoint® 2019 (version 1808) were used for data visualisation.
Results
The flowchart of patients included in each stage of the study is depicted in Figure 2.
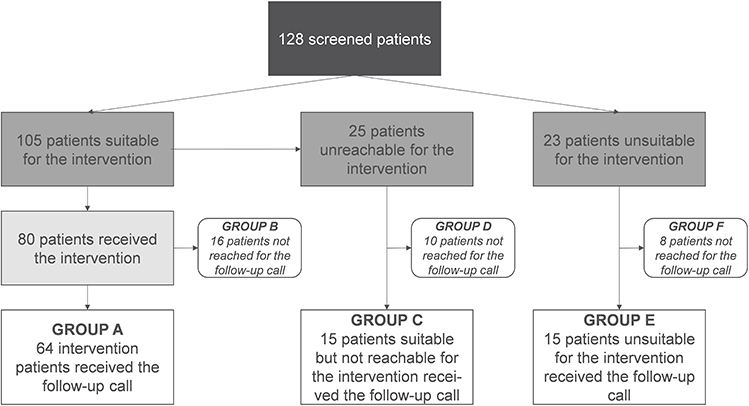 |
Figure 2 Flowchart of patients included in the study. |
Screening
We screened 128 patients in the study period between March and December 2023. Of these, 105 patients (82.0%) were deemed suitable for the intervention according to the prespecified criteria. Patient characteristics, answers to the screening questions, and reasons for intervention suitability are reported in Table 2.
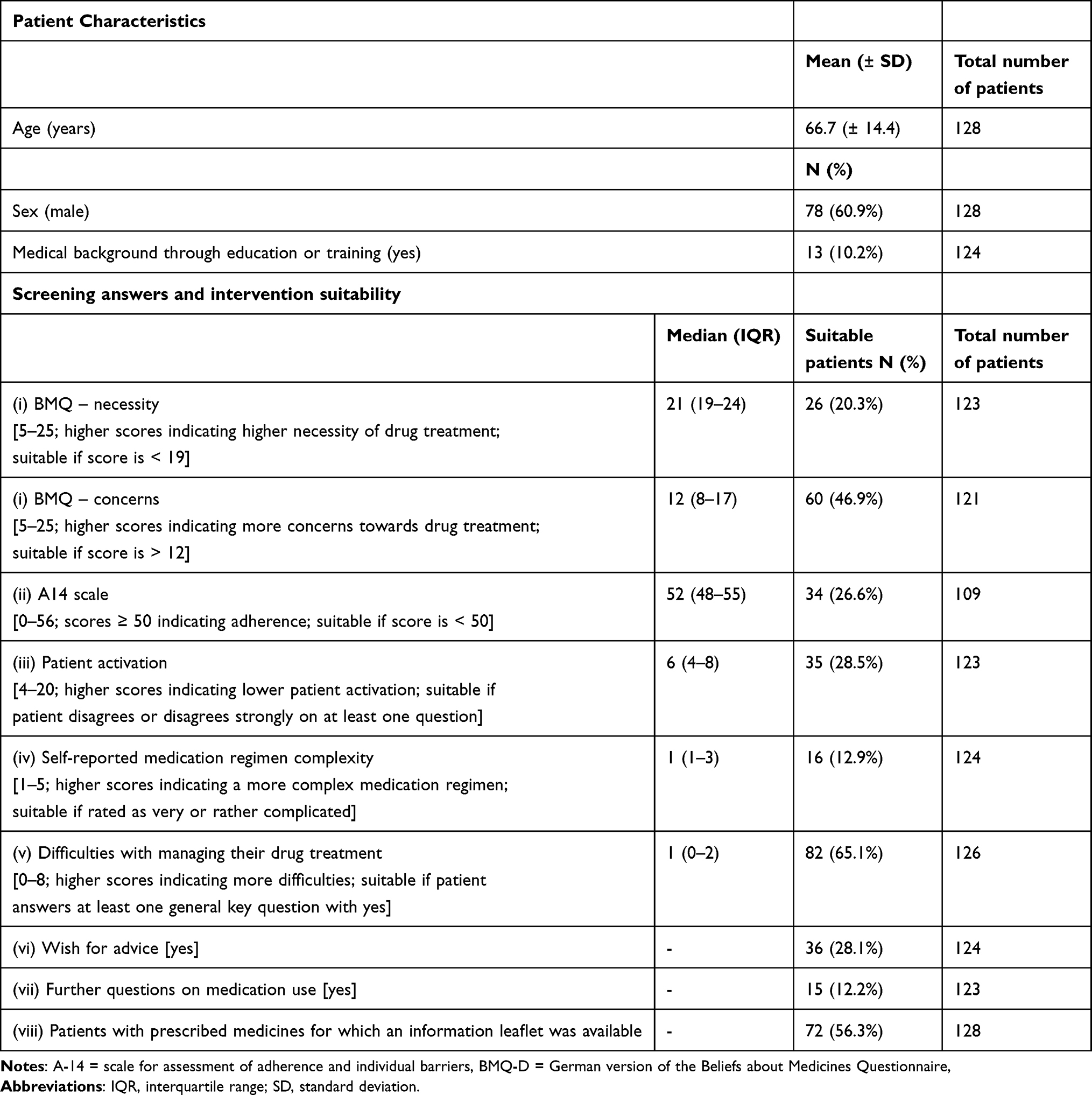 |
Table 2 Patient Characteristics, Screening Answers, and Intervention Suitability |
Intervention
From the 105 suitable patients, 25 could not receive the intervention due to early transfer or discharge from the study ward, unresponsiveness at the time of the intervention visit, or linguistic barriers. In total, 80 patients (76.2% of all suitable patients) received the intervention. The intervention lasted 17 min (± 8 min) on average. The number of patients receiving information materials is depicted in Table 3. Patients most commonly received one-pagers on acetyl-salicylic acid (29 patients), ticagrelor (24 patients), and atorvastatin (20 patients). Most commonly distributed drug administration leaflets were on subcutaneous injection (16 patients), swallowing difficulties (12 patients), and inhalation devices (11 patients). The main results on difficulties with managing their drug treatment are shown in Table 3. The most frequently applicable complexity factors were on the total number of 5 or more drugs (67 patients), meal-dependent administration (54 patients), and administration at lunch time (27 patients). Patients without regular medication prescribed before hospital admission were not asked any key questions (11 patients). In total, including the open question on difficulties with administering their medication, 64.5% (49 out of n = 76 patients, missings = 4) of the patients mentioned at least one difficulty. As answers on the open question regarding difficulties in administering their medication, patients mentioned difficulties with frequent changes in drug manufacturers, adverse drug reactions, and deblistering of medications. Most commonly mentioned risk factors for nonadherence were concerns about drug treatment, experienced side effects, and lack of knowledge regarding disease/ drug treatment.
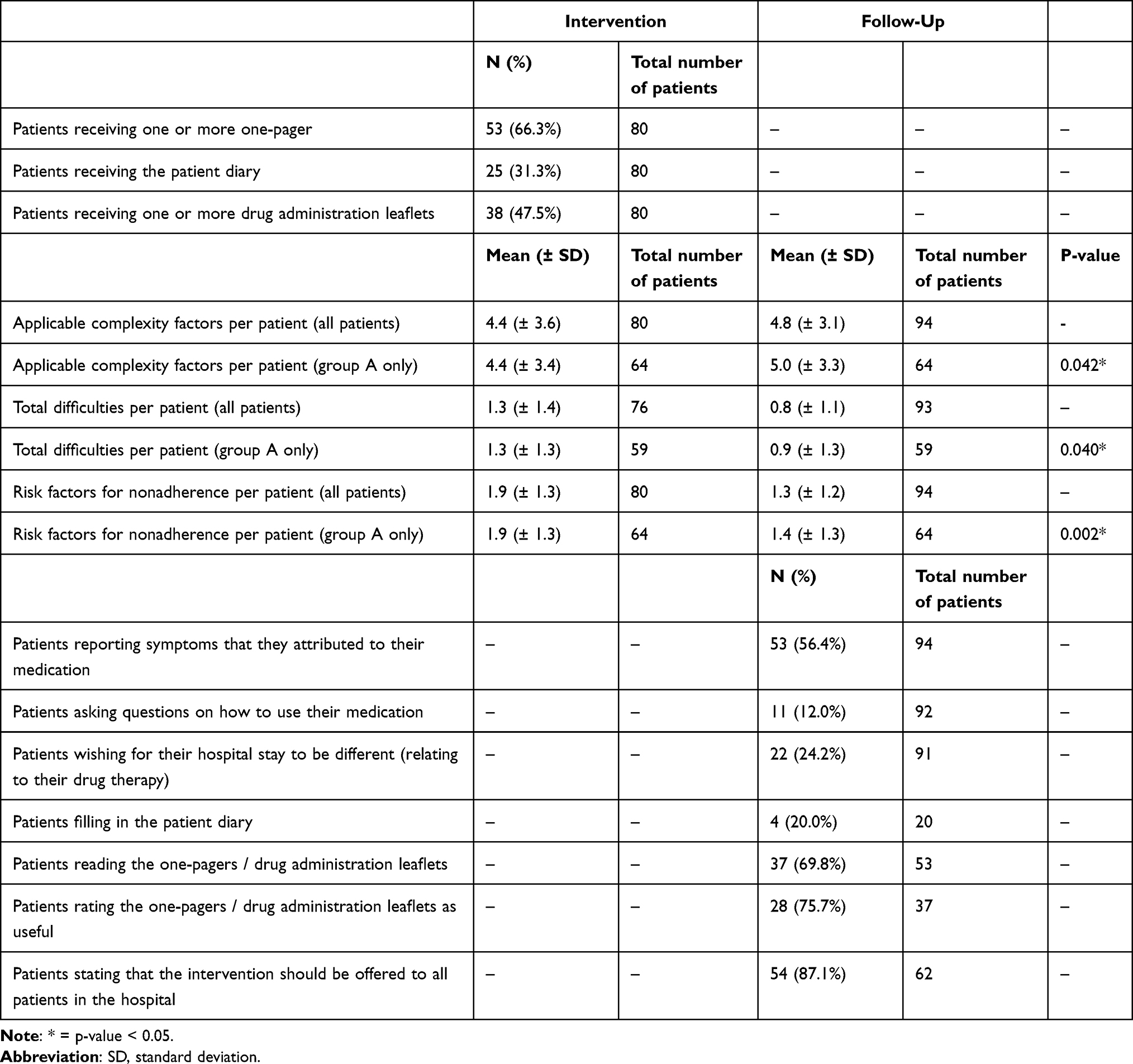 |
Table 3 Main Results of the Intervention and Follow-up |
Follow-Up
In total, 94 patients (73.4%, n = 128) were reached for the follow-up telephone call – 64 with a positive screening and the intervention (group A), 15 with a positive screening and without intervention (group C), and 15 with a negative screening and without intervention (group E). Follow-up calls were conducted between 6 and 24 weeks after discharge. The mean duration of follow-up calls was 15 minutes (± 8 min). Due to time constraints, 3 of the 94 patients reached for the follow-up call terminated the call prematurely and, hence, did not answer all of the follow-up questions. In this case, patients’ available answers were included in data analysis while some questions remained with missing values. A majority of patients experienced medication changes after discharge (60 out of n = 93 patients, 64.5%, missings = 1). Applicable key questions were asked considering the changes in patients’ discharge medication. The main results of the exploratory analyses are depicted in Table 3. The most frequently applicable complexity factors were on the total number of 5 or more drugs (91 patients), meal-dependent administration (83 patients), and tablet splitting (31 patients). In total, including the open question on difficulties with administering their medication, 50.5% (47 out of n = 93 patients, missings = 1) of all patients mentioned at least one difficulty. Group A patients mentioned less difficulties than during the intervention (p = 0.040, Figure 3). Male and female patients did not differ in the number of difficulties with managing their drug treatment (p = 0.278). Similarly, whether the patients had any prior medical knowledge did not affect the number of difficulties mentioned in the follow-up (p = 0.628). Among the difficulties not covered by key questions, patients mentioned predominantly difficulties with adverse drug reactions. Other difficulties concerned the readability and comprehensibility of package leaflets, persisting symptoms, and logistical difficulties with managing their medication. Reasons for patients wishing for their hospital stay to be different were more information or support needs regarding their drug therapy and difficulties at transitions of care. The most prominent reasons for not filling in the patient diary were losing it and forgetting about it. Patients with an intervention and follow-up mentioned less risk factors for nonadherence during the follow-up compared to during the intervention (p = 0.002). Most commonly mentioned risk factors for nonadherence were experienced side effects, interpretation of dosing instructions, and low satisfaction with/trust in healthcare/doctor.
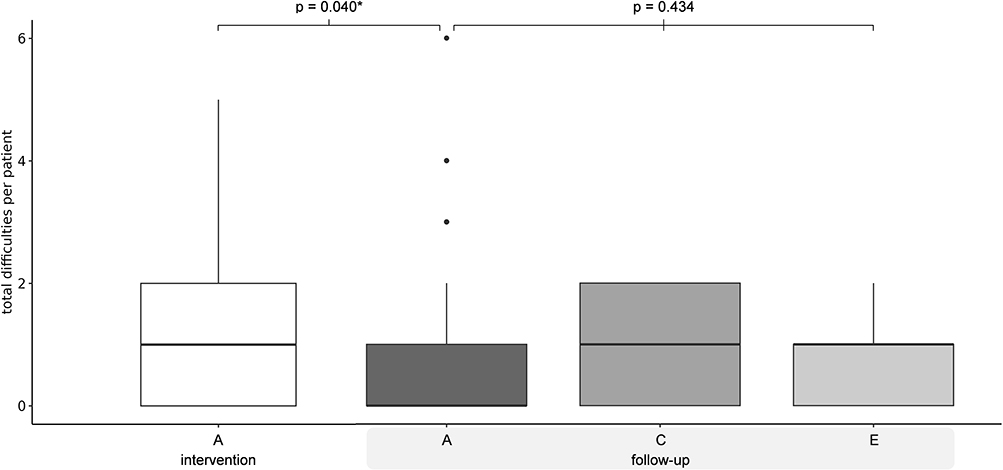 |
Figure 3 Total difficulties with managing their drug treatment identified per patient. * = p-value < 0.05; group A = patients suitable for the intervention, receiving the intervention and the follow-up; group C = patients suitable for the intervention, not receiving the intervention but receiving the follow-up; group E = patients unsuitable for the intervention, receiving the follow-up. |
Between group A (0.9 ± 1.3, n = 63), C (1.0 ± 0.8, n = 15), and E (0.6 ± 0.6, n = 15), no differences in the number of difficulties during the follow-up were detected (p = 0.434, Figure 3). Likewise, there was no difference between these groups in the number of risk factors for nonadherence (p = 0.422).
Discussion
To our knowledge, this study was the first to develop and apply a screening method for a pharmaceutical care intervention based on patient-reported difficulties. It showed that a pharmaceutical care intervention during the inpatient stay was effective in reducing difficulties with managing their drug treatment after discharge. The novel screening method comprising of questionnaires identified a high need for comprehensive drug information upon admission to the study ward. However, the screening method proved to be inappropriate for effectively prioritising patients for the pharmaceutical care intervention. This is reflected by the high rate of patients identified as suitable for the intervention (82%) and the lack of differences between the number of difficulties mentioned in the follow-up between suitable and unsuitable patients.
This could mean that, in general, patients need more medication-related information during their inpatient stay, independent from their underlying medication beliefs or pre-existing difficulties. Patients’ medication knowledge after discharge has been shown to be poor in a cardiology patient population,23 which is likely to translate into adverse patient outcomes. Pharmacists’ medication counselling at hospital discharge can increase patients’ confidence in their medication knowledge.24 In our study, patients showed a high rate of risk factors relating to concerns about drug treatment and lack of knowledge regarding disease or drug treatment during the intervention. During the follow-up, the rate of these risk factors diminished. Patients showed more applicable complexity factors during the follow-up than during the intervention. Likely, this is due to changes in patients’ medication regimen after discharge which the majority of patients experienced. Nevertheless, patients mentioned fewer difficulties during the follow-up which could be due to the successful pharmaceutical care intervention. The number of applicable complexity factors per patient and the rate of patients confirming at least one of them as difficult is similar to a previous study.25 There are differences in the most frequently applicable complexity factors, however, this is easily explained by the different settings and patient collectives considered.25 The intervention and the follow-up phone calls were short enough (17 and 15 minutes, respectively) to be incorporated into the inpatient stay. The mean duration is similar to other counselling interventions (e. g.26). However, the preparation time for the intervention and the follow-up were considerably longer. This means that, all in all, the time requirement for pharmacists was high, which underpins the need for an effective prioritisation method. The duration of preparation times was not measured, but is estimated to equal those of similar studies.26
This study has several strengths and limitations. The study does not have a randomised control group. However, the aim was to test whether a suitable control group could be created by the screening itself by distinguishing between patients with and without a high information need. Consequently, comparing the different intervention groups also provides a reliable control mechanism. The novel screening method, as well as the method to identify patients’ difficulties asking key questions on complexity factors have the opportunity to elicit patient preferences and their information needs. This patient-centred approach acknowledges patients’ individual care needs. We hypothesise that the patients’ answers to the key questions are subject to social desirability and may depend on patients’ underlying health literacy and ability for self-observation. The identification of risk factors for nonadherence is based on the judgement of the pharmacist conducting the patient conversation and is, thus, subjective.
The pharmaceutical care intervention can be implemented in other locations. The information leaflets (one-pagers and drug administration leaflets) were developed according to a standardised process and are accessible online.27 Similarly, the asked key questions have been published and can be used elsewhere. With the pharmaceutical care intervention applied in this study, we showed to reduce patients’ difficulties with managing their drug treatment, as well as their risk factors for nonadherence. We cannot know for sure whether this translates into better clinical outcomes. However, based on the results of other trials, it is possible that pharmaceutical interventions based on patient education improve clinical outcomes.10 Patients themselves rated the information leaflets and the intervention itself highly useful and informative. This, in combination with the high rate of patients identified as suitable during the screening, proves that additional information on drug treatment by pharmacists during the inpatient stay is needed and wanted. Even patients with prior medical knowledge showed difficulties with managing their drug treatment during the follow-up. In future studies, it may be interesting to tailor the patient education provided based on patients’ prior medical knowledge. Cardiovascular disease patients have been shown to struggle with achieving guideline standards for secondary prevention, with a high prevalence of patients keeping unhealthy lifestyle habits like smoking or physical inability.28 Drug nonadherence and insufficient medication knowledge can further jeopardize patients’ achievement of treatment goals. This study presents is a valuable piece of the puzzle in efforts to provide better care for cardiovascular patients. In future studies, efforts should be directed towards establishing effective prioritisation methods for pharmacist interventions without losing focus on patient preferences. Ideally, a risk-based, data-driven approach could be combined with patients’ communicated information needs to provide pharmaceutical care where it is needed and effective.
Conclusion
This study showed that a pharmaceutical care intervention during the inpatient stay diminished patient-reported difficulties with managing their drug treatment after discharge. The novel screening method to prioritise patients for a pharmaceutical care intervention based on questionnaires was unsuitable for effective prioritisation due to the high rate of positively screened patients and the lack of differences in difficulties between patients with positive or negative screening. Incorporating patient preferences and needs in pharmaceutical care interventions proves to be important and effective. However, the question remains how pharmacists’ scarce availabilities can be employed in a resource-efficient way.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request. The screening questionnaire as well as the interview guides are accessible in the supplements and may be used in other studies upon approval of the corresponding author. Copyright holders of the BMQ questionnaire and the A14 questionnaire were informed about usage of the questionnaire as part of this study to grant permission for use.
Acknowledgments
We thank Christine Faller and Sophia Klasing for their valuable contributions to the pilot study preceding this work. We thank Dierk Thomas for his expertise and help in creating the one-pagers. For the publication fee we acknowledge financial support by Heidelberg University.
Miriam Degen's affilation when the research was done was: Heidelberg University, Medical Faculty Heidelberg / Heidelberg University Hospital, Internal Medicine IX - Department of Clinical Pharmacology and Pharmacoepidemiology, Cooperation Unit Clinical Pharmacy, Im Neuenheimer Feld 410, 69120 Heidelberg, Germany; Miriam Degen's current affiliations are: Division of Clinical Epidemiology and Aging Research, German Cancer Research Center (DKFZ), Heidelberg, Germany and Faculty of Medicine, University of Heidelberg, Heidelberg, Germany.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Prof. Dr. Hanna Seidling reports grants from g-BA Innovationsfond, grants from BfArM, grants from BMG, grants from BMBF, grants from Förderinitative Pharmazeutische Betreuung e.V., grants from LAK Baden-Württemberg, personal fees from Chamber of pharmacists, professional organisations, publishing houses, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Grimmsmann T, Schwabe U, Himmel W. The influence of hospitalisation on drug prescription in primary care--a large-scale follow-up study. Eur J Clin Pharmacol. 2007;63(8):783–790. doi:10.1007/s00228-007-0325-1
2. Freyer J, Greißing C, Buchal P, et al. Discharge medication - what do patients know about their medication on discharge? Dtsch Med Wochenschr. 2016;141(15):e150–156. doi:10.1055/s-0042-108618
3. Kripalani S, Henderson LE, Jacobson TA, Vaccarino V. Medication use among inner-city patients after hospital discharge: patient-reported barriers and solutions. Mayo Clin Proc. 2008;83(5):529–535. doi:10.1016/S0025-6196(11)60724-6
4. Tomlinson J, Silcock J, Smith H, Karban K, Fylan B. Post-discharge medicines management: the experiences, perceptions and roles of older people and their family carers. Health Expect. 2020;23(6):1603–1613. doi:10.1111/hex.13145
5. Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170(3):345–349.
6. El Morabet N, Uitvlugt EB, van den Bemt BJF, van den Bemt P, Janssen MJA, Karapinar-Çarkit F. Prevalence and preventability of drug-related hospital readmissions: a systematic review. J Am Geriatr Soc. 2018;66(3):602–608. doi:10.1111/jgs.15244
7. Villeneuve Y, Courtemanche F, Firoozi F, et al. Impact of pharmacist interventions during transition of care in older adults to reduce the use of healthcare services: a scoping review. Res Social Adm Pharm. 2020;17(8):1361–1372. doi:10.1016/j.sapharm.2020.11.006
8. Zhang S, Zhang GB, Huang P, et al. Drug-related problems in hospitalized patients with chronic kidney diseases and clinical pharmacist interventions. BMC Geriatr. 2023;23(1):849. doi:10.1186/s12877-023-04557-y
9. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125(9):882–7.e1. doi:10.1016/j.amjmed.2011.12.013
10. Rattanavipanon W, Chaiyasothi T, Puchsaka P, et al. Effects of pharmacist interventions on cardiovascular risk factors and outcomes: an umbrella review of meta-analysis of randomized controlled trials. Br J Clin Pharmacol. 2022;88(7):3064–3077. doi:10.1111/bcp.15279
11. Abousheishaa AA, Sulaiman AH, Huri HZ, et al. Global scope of hospital pharmacy practice: a scoping review. Healthcare. 2020;8(2). doi:10.3390/healthcare8020143
12. Alshakrah MA, Steinke DT, Lewis PJ. Patient prioritization for pharmaceutical care in hospital: a systematic review of assessment tools. Res Social Adm Pharm. 2019;15(6):767–779. doi:10.1016/j.sapharm.2018.09.009
13. Jungreithmayr V, Bittman JA, Faller CK, et al. Novel screening method to identify patients that benefit from the implementation of a pharmaceutical care intervention in the inpatient setting—a pilot study. 13th PCNE working conference abstract number 592. Int J Clin Pharm. 2023;45(2):515–541.
14. Jungreithmayr V, Bittmann JA, Wurmbach VS, et al. From screening and a pharmaceutical care intervention to follow-up calls – how can we effectively solve patients’ difficulties in handling their medication in the inpatient setting? Res Social Adm Pharm. 2024;20(12, Part B):25–26. doi:10.1016/j.sapharm.2024.08.069
15. Jungreithmayr V, Bittmann JA, Wurmbach VS, et al. Beurteilung potentieller Risikofaktoren für Nonadhärenz im Rahmen einer pharmazeutischen Intervention auf Station und eines Follow-Up Telefonats nach Entlassung. Krankenhauspharmazie. 2025;46(01):48–59.
16. Horne R, Weinman J, Hankins MJP. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24.
17. Mahler C, Hermann K, Horne R, Jank S, Haefeli WE, Szecsenyi J. Patients’ beliefs about medicines in a primary care setting in Germany. J Eval Clin Pract. 2012;18(2):409–413. doi:10.1111/j.1365-2753.2010.01589.x
18. Jank S, Bertsche T, Schellberg D, Herzog W, Haefeli WE. The A14-scale: development and evaluation of a questionnaire for assessment of adherence and individual barriers. Pharm World Sci. 2009;31(4):426–431. doi:10.1007/s11096-009-9296-x
19. Wurmbach VS, Schmidt SJ, Lampert A, et al. Development and pilot-testing of key questions to identify patients’ difficulties in medication administration. Patient Prefer Adherence. 2021;15:2479–2488. doi:10.2147/PPA.S328380
20. Lampert A, Wien K, Haefeli WE, Seidling HM. Guidance on how to achieve comprehensible patient information leaflets in four steps. Int J Qual Health Care. 2016;28(5):634–638. doi:10.1093/intqhc/mzw077
21. Wurmbach VS, Schmidt SJ, Lampert A, et al. Development of an algorithm to detect and reduce complexity of drug treatment and its technical realisation. BMC Med Inform Decis Mak. 2020;20(1):154. doi:10.1186/s12911-020-01162-6
22. Schmidt SJ, Wurmbach VS, Lampert A, et al. Individual factors increasing complexity of drug treatment-a narrative review. Eur J Clin Pharmacol. 2020;76(6):745–754. doi:10.1007/s00228-019-02818-7
23. Custodis F, Rohlehr F, Wachter A, Böhm M, Schulz M, Laufs U. Medication knowledge of patients hospitalized for heart failure at admission and after discharge. Patient Prefer Adherence. 2016;10:2333–2339. doi:10.2147/PPA.S113912
24. O’Mahony E, Kenny J, Hayde J, Dalton K. Development and evaluation of pharmacist-provided teach-back medication counselling at hospital discharge. Int J Clin Pharm. 2023;45(3):698–711. doi:10.1007/s11096-023-01558-0
25. Wurmbach VS, Schmidt SJ, Lampert A, et al. Prevalence and patient-rated relevance of complexity factors in medication regimens of community-dwelling patients with polypharmacy. Eur J Clin Pharmacol. 2022;78(7):1127–1136. doi:10.1007/s00228-022-03314-1
26. Walker SA, Lo JK, Compani S, et al. Identifying barriers to medication discharge counselling by pharmacists. Can J Hosp Pharm. 2014;67(3):203–212. doi:10.4212/cjhp.v67i3.1357
27. Abteilung für Klinische Pharmakologie und Pharmakoepidemiologie [homepage on the Internet]. Downloads für Patient:innen und Fachpersonal: Arzneimittel richtig anwenden. 2018. Available from: https://www.klinikum.uni-heidelberg.de/kliniken-institute/kliniken/zentrum-fuer-innere-medizin-krehl-klinik/abt-klinische-pharmakologie-und-pharmakoepidemiologie/downloads.
28. Kotseva K, De Backer G, De Bacquer D, et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur J Prev Cardiol. 2019;26(8):824–835. doi:10.1177/2047487318825350
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.