Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Novel Nomogram Model for Predicting the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Infection
Authors Wu Y, Wang M ![]() , Zhang Z
, Zhang Z ![]() , Chen G
, Chen G ![]() , Zhang B
, Zhang B
Received 20 December 2024
Accepted for publication 5 April 2025
Published 16 April 2025 Volume 2025:12 Pages 765—775
DOI https://doi.org/10.2147/JHC.S512471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Yanfang Wu,1,* Meixia Wang,2,* Zhenzhen Zhang,1,* Guobin Chen,1 Boheng Zhang1
1Department of Hepatic Oncology, Zhongshan Hospital, Fudan University (Xiamen Branch), Xiamen Clinical Research Center for Cancer Therapy, Clinical Research Center for Precision medicine of abdominal tumor of Fujian Province, Xiamen, 361015, People’s Republic of China; 2Department of Hospital Infection Management, Zhongshan Hospital, Fudan University (Xiamen Branch), Xiamen, Fujian, 361015, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Boheng Zhang, Department of Hepatic Oncology, Zhongshan Hospital, Fudan University (Xiamen Branch), Xiamen Clinical Research Center for Cancer Therapy, Clinical Research Center for Precision medicine of abdominal tumor of Fujian Province, Xiamen, 361015, People’s Republic of China, Tel/Fax +86-592-3569583, Email [email protected]
Purpose: Hepatitis B virus (HBV) infection is a major cause of hepatocellular carcinoma (HCC). This study aimed to construct a novel nomogram model for predicting the risk of HCC in patients with HBV infection.
Patients and Methods: This retrospective study analyzed clinical data from healthcare databases in Xiamen, encompassing 5161 adults with HBV infection without HCC and 2819 adults with HBV-related HCC between January 2016 and December 2020. Subsequently, the patients were randomly divided into a training set (n=5586) and testing set (n=2394). The training set was used to identify the risk factors for HCC development and to construct an HCC risk prediction nomogram model. The predictive accuracy of the model was assessed using the receiver operating characteristic (ROC) curve analysis and decision curve analysis (DCA) in both sets. Furthermore, the performance of the nomogram model was compared with that of the existing models.
Results: Multivariate analysis revealed that age, sex, liver cirrhosis, neutrophil/platelet count ratio (NLR), serum bilirubin (TBIL), aspartate aminotransferase (AST), serum albumin (ALB), serum alpha-fetoprotein (AFP), and HBV DNA were independently associated with HCC. A nomogram model was developed by incorporating these risk factors. The the receiver operating characteristic curve (AUC) of the nomogram model were 0.897 and 0.902 for the training and testing sets, respectively. Analysis of the AUC demonstrated that the nomogram model exhibited significantly enhanced predictive performance for HCC compared to the alternative risk scores in both sets. Furthermore, DCA indicated that the nomogram model provided a broad range of threshold probabilities related to the net clinical benefits. A web-based calculator was developed(https://nomogram-model-hcc.shinyapps.io/DynNomapp/).
Conclusion: The novel nomogram model, which includes age, sex, liver cirrhosis, NLR, TBIL, AST, ALB, AFP, and HBV DNA as factors, precisely predicts the risk of HCC in patients with chronic hepatitis B(CHB) and outperforms the existing models.
Keywords: HBV infection, HCC, neutrophil/platelet count ratio, prediction
Introduction
Hepatocellular carcinoma (HCC) is a prevalen malignant tumor in China and globally.1 The prognosis of HCC is extremely poor, with a 5-year survival rate of only 14.1%.2 Chronic hepatitis B virus (HBV) infection is the leading cause of HCC worldwide.3 The risk for CHB patients is 5 to 100 times higher compared to that of healthy individuals.4 Early diagnosis of HCC enhances therapeutic curability and prolongs overall survival, particularly emphasizing the critical need for systematic surveillance in high-risk populations.5 Recently, numerous HCC predictive models have been extensively utilized in clinical settings; however, these models also exhibit certain limitations. For instance, the Toronto HCC Risk Index (THRI)6 is utilized to estimate the risk of HCC in patients with cirrhosis. The aMAP model7 is appropriate for predicting HCC risk in patients with multi-cause chronic liver disease but may not adequately capture the risk in some CHB patients. Models such as PAGE-B,8 mPAGE-B,8 HCC-Rescure,9 AASL,10 and SAGE-B models11 are primarily used to assess the risk of HCC following antiviral therapy for HBV. Since antiviral therapy effectively suppresses viral replication in the majority of CHB patients, above HCC risk prediction models developed for the post-antiviral treatment era, such as the PAGE-B score,8 have excluded conventional virological markers including HBV DNA and HBeAg status. The PAGE-B scoring system, which was specifically developed and validated in nucleos(t)ide analog (NA)-treated cohorts, incorporates three non-virological parameters: age, male gender, and platelet count(PLT) as clinically relevant predictors of HCC development. In the real world, a large proportion of CHB patients do not receive antiviral treatment or undergo regular follow-ups. Therefore, the development of many models, such as the chronic hepatitis B(REACH-B)12 and AGED models,13 relies on the data of patients who have not received antiviral treatment, including HBVDNA and HBeAg. However, both the REACH-B and AGED models have notable limitations in that they exclude patients with cirrhosis, a condition widely recognized as a significant risk factor for HCC. The REACH-B model excluded patients older than 65 years. There are also models that apply regardless of antiviral treatment, such as the CU-HCC model.14 One of the most fatal flaws in this model is the absence of sex as an important metric. It is well known that male is an important risk factor for HCC development.4
It is noteworthy that our team has previously characterized the features of HCC in Xiamen.15 One significant observation is the increasing proportion of patients with HBV ralated HCC who also suffer from systemic chronic conditions such as fatty liver and obesity, particularly since 2019 and 2020. This trend may indicate a potential link between systemic inflammatory responses and the progression of HCC. As is well established, inflammatory responses play critical roles in various stages of tumor progression, including initiation, promotion, malignant transformation, invasion, and metastasis.16 The NLR serves as a prognostic indicator for patients with advanced HCC who have undergone treatment with molecular-targeted agents and immunotherapy.17 A systematic review and meta-analysis of 100 studies involving over 40,000 patients confirmed that an elevated NLR, defined as a value exceeding 4–5, was significantly associated with poorer overall survival (OS) and progression-free survival (PFS).18 Specifically, an NLR greater than 4 was associated with poor outcomes in HCC patients treated with lenvatinib.19 However, there currently lacks an inflammation-related predictive model specifically for HBV-ralated HCC. Therefore, we aimed to develop a novel HCC prediction model tailored to CHB patients, regardless of their antiviral therapy status.
Materials and Methods
Patients
This multicenter, retrospective study was conducted. The medical records of 12144 adult (≥18 years) of chronic HBV infection without HCC (CHB-nonHCC), and 3763 adult patients with HCC (CHB-HCC) patients at Xiamen hospitals in China between January 2016 and December 2020 were included using the Xiamen Healthcare Big Data platform for retrospective analysis. CHB was defined as positivity for hepatitis B surface antigen (HBsAg) for > 6 months. HCC was diagnosed in accordance with the standard practice guidelines of the American Association for the Study of Liver Diseases.20 The clinical data of the patients who were first diagnosed with CHB were retrospectively analyzed. We excluded data that was missing all laboratory results, as well as cases where the interval from the initial record of HBV infection to HCC diagnosis was less than six months, or where follow-up duration was less than six months. Patients diagnosed with HCC without prior CHB records were also excluded from the study. Finally, 5161 CHB-nonHCC patients and 2819 CHB-HCC patients were included in this study. The patients were randomly divided into a 70% training set (n= 5586) and a 30% testing set (n=2394) (Figure 1). The training set was utilized to identify the risk factors associated with the development of HCC and to construct an HCC risk prediction nomogram model, whereas the testing set was employed to validate the developed model. The study was approved by the institutional review committee of Zhongshan Hospital, Fudan University (Xiamen Branch)(authorization number B2020-020R), adhered to the principles outlined in the Declaration of Helsinki, and followed good clinical practice guidelines. All patients provided written informed consent for the use of anonymized data (anonymously) for research purposes.
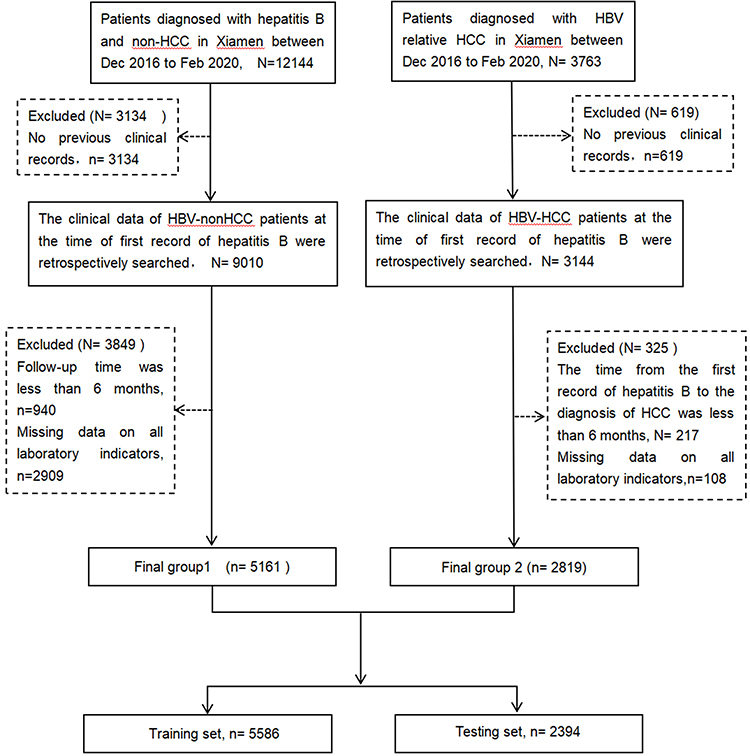 |
Figure 1 Diagram of patient selection in the present study. |
Evaluation of Clinical Data
The following data were obtained at the time of HBV infection: age (years), sex, Body Mass Index (BMI, BMI=weight (kg)/height (m2)) and history of hypertension, diabetes, alanine aminotransferase(ALT)(U/L), aspartate aminotransferase (AST) (U/L), serum albumin (ALB)(g/L), TBIL (µmol/L), serum alpha-fetoprotein (AFP) (ng/mL), HBsAg or HBs antibody (HBsAb), HBe antigen (HBeAg), serum HBV DNA (copies/mL) levels, white blood cell count(WBC)(×109/L), neutrophil count (×109/L), blood platelet count(PLT)(×109/L), and neutrophil/platelet count ratio (NLR). The diagnostic criteria of liver cirrhosis were according to the Chinese Guidelines for the diagnosis and treatment of liver cirrhosis.21
Statistical Analyses
For demographic data, categorical variables were expressed as percentages, while continuous variables were reported as means and standard deviations. Differences in variable distributions between the testing and validation sets were analyzed using the Mann–Whitney U-test, χ²-test, or Fisher’s exact test, as appropriate. In this study, we adopted a cut-off value of 4 for the NLR, as recommended by previous studies.19,22 We applied the mice v3.13.0 package (R software version 3.5.1) for multiple imputations if the missing values were less than 20%. Twelve variables were entered into the variable-selection process. Variables with P < 0.05, from univariate analysis and least absolute shrinkage and selection operator (LASSO) logistic regression, were employed to select variables. The most predictive risk factors were selected on the basis of the minimum value (λmin). Subsequently, variables identified by LASSO regression analysis were entered into Cox proportional hazards regression models. The hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. A nomogram model was constructed based on the Cox proportional hazards regression analysis to predict the risk of HCC. The predictive accuracy and discriminative ability of the model were evaluated using receiver operating characteristic (ROC) curves and calibration curve. The AUC was calculated The decision curve analysis (DCA) was applied to evaluate whether the nomogram model improved clinical decision-making or which of the two models led to better decisions. Statistical analyses were conducted using R software version 3.5.1.
Results
Baseline Characteristics of Patients
In this study, 7980 patients with CHB were included in the analysis at the initial diagnosis of CHB, among whom 2819 developed HCC during the follow-up period. A total of 5586 patients were randomly assigned to the training set and 2394 to the testing set. The baseline characteristics of the two sets are listed in Table 1. Most patients in the HBV-HCC group were male and exhibited cirrhosis, older age, elevated neutrophil-to-lymphocyte ratio, high bilirubin levels, low albumin levels, increased transaminase levels, elevated alpha-fetoprotein (AFP) levels, and high HBV DNA levels.
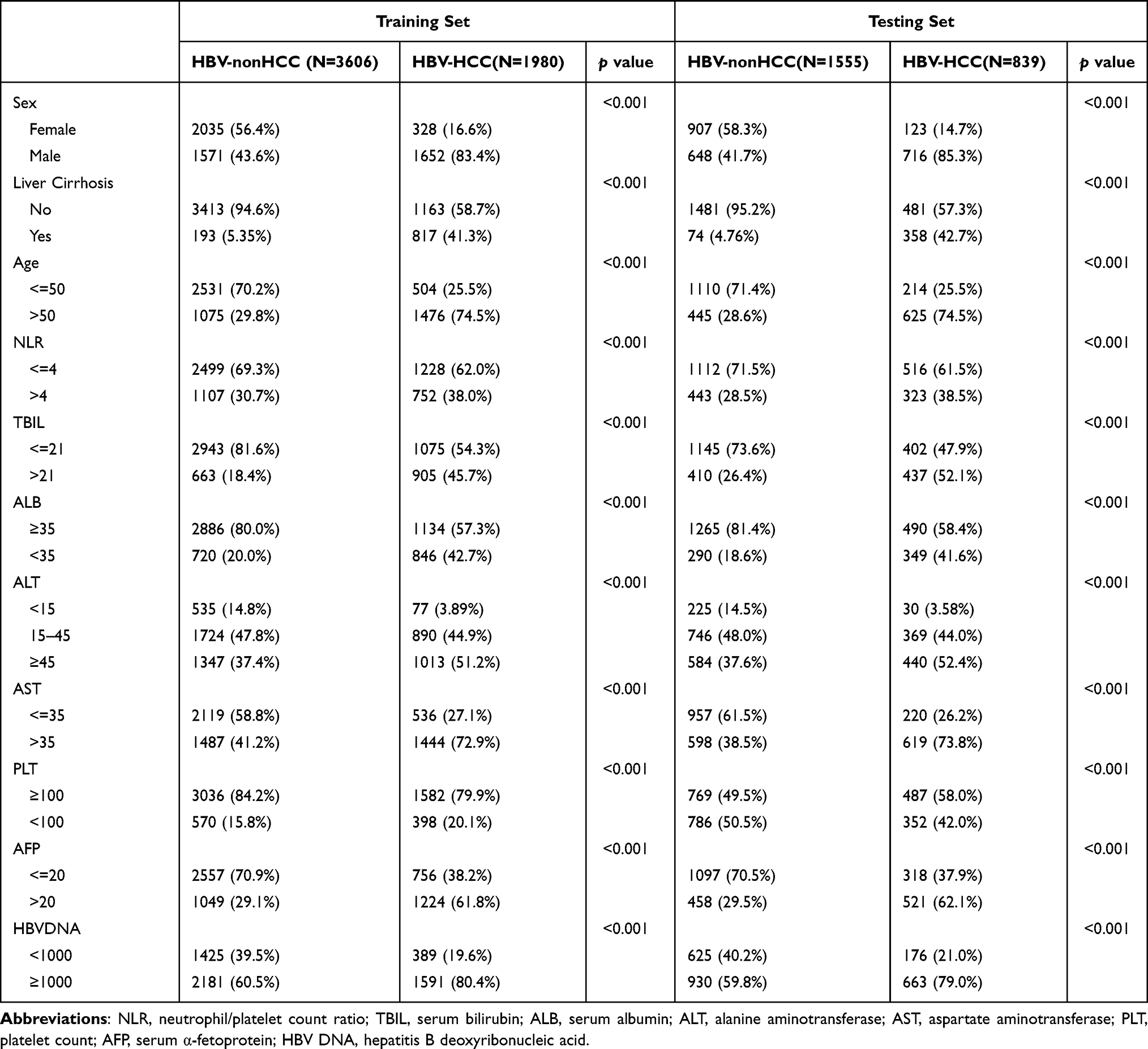 |
Table 1 Demographics and Clinical Characteristics at the Time of Their First Diagnosis with Hepatitis B Between CHB-nonHCC and CHB-HCC Group in Both the Training and Testing Sets |
Development and Validation of HCC Prediction Nomogram Model
To construct a novel HCC prediction nomogram model, we probed the risk factors associated with HCC development in the training set (n=5586). Table 2 presents the results of the univariate and multivariate analyses conducted on the training set. The univariate Cox manifested that age (HR: 4.723, P < 0.001), sex (HR:4.16, P < 0.001), liver cirrhosis (HR: 4.352, P < 0.001), NLR (HR: 1.392, P < 0.001), TBIL (HR: 2.293, P < 0.001), ALT (HR: 3.02, P < 0.001), AST (HR: 2.987, P < 0.001), ALB (HR: 1.998, P < 0.001), PLT (HR: 1.332, P < 0.001), AFP (HR: 2.828, P < 0.001), and HBV DNA (HR: 2.503, P < 0.001) were correlated with CHB-HCC patients. Nine predictive risk factors were selected to enter Cox proportional hazards regression models by LASSO regression analysis (Supplementary Figures 1–2). Multivariate Cox proportional hazards regression analysis indicated that age (hazard ratio [HR]:2.919, P < 0.001), sex (HR:2.559, P < 0.001), liver cirrhosis (HR:1.741, P < 0.001), NLR (HR:1.152, P < 0.001), TBIL (HR:1.045, P < 0.001), AST (HR: 1.533, P < 0.001), ALB (HR: 1.31, P < 0.001), AFP level (HR:2.019, P < 0.001), and HBV DNA level (HR:2.107, P < 0.001) independently predicted HCC development.
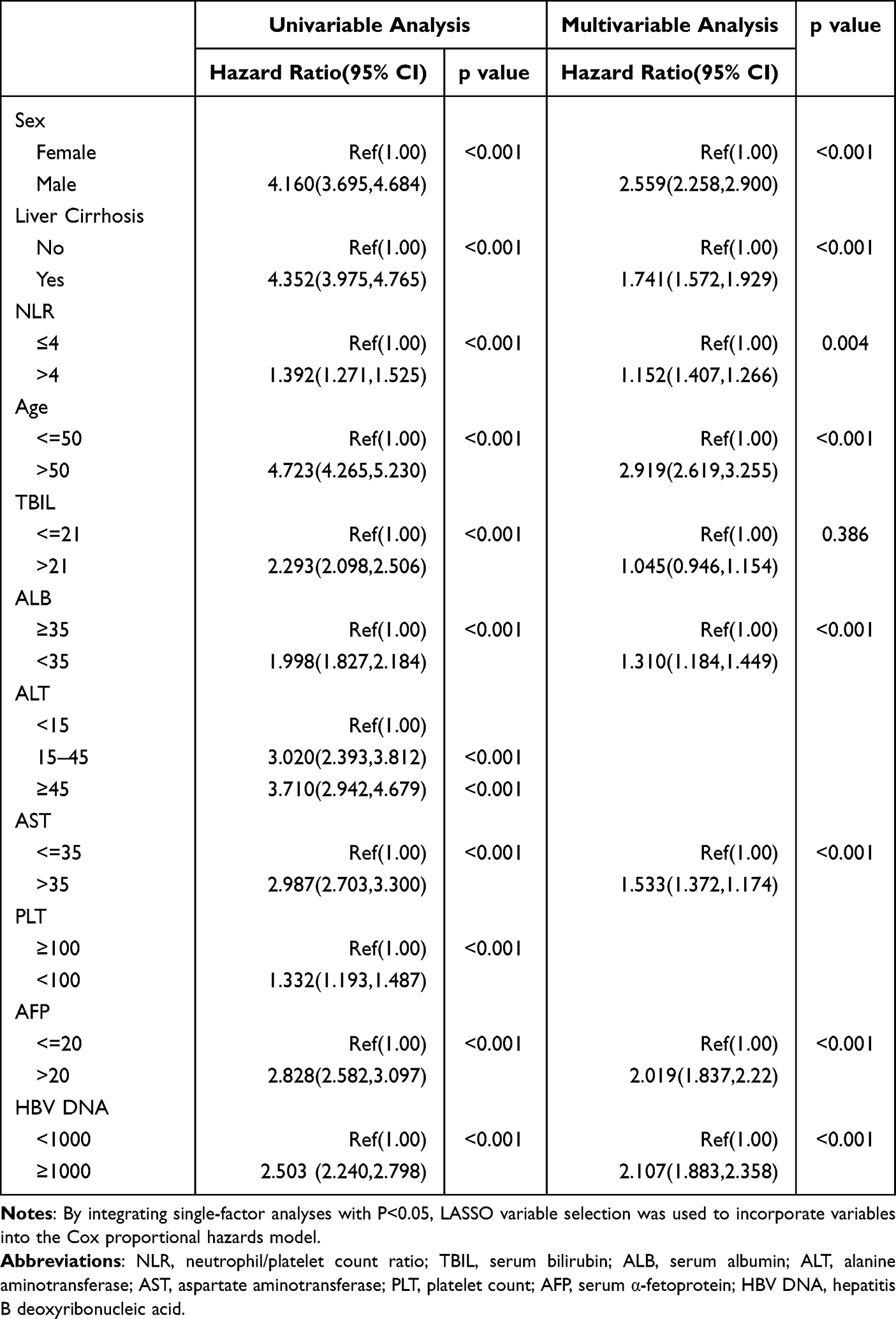 |
Table 2 Variables Associated with HCC in the Training Set |
A nomogram model was constructed based on the risk factors identified through multivariate Cox proportional hazards regression analysis, the results are illustrated in Figure 2. Each variable was assigned a corresponding score based on its value and these scores were summed to obtain the total score. The total score was used to assess the risk of developing HCC, with a risk range of 0–20. The AUC of our prediction nomogram model was 0.896 for the training set and 0.902 for the testing set (Figure 3). In addition, the calibration curves demonstrated a degree of concordance between the actual and predicted results(Supplementary Figure 3). A calculator has been developed(https://nomogram-model-hcc.shinyapps.io/DynNomapp/), which will be beneficial for daily practice.
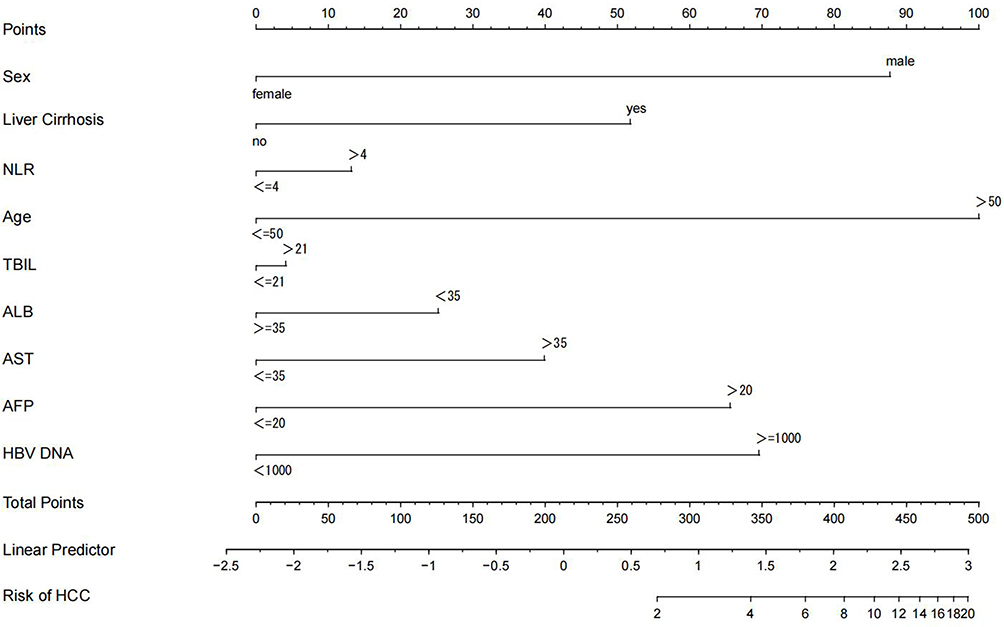 |
Figure 2 The nomogram model for the prediction of hepatocellular carcinoma (HCC). Abbreviations: NLR, neutrophil/platelet count ratio; TBIL, serum bilirubin; ALB, serum albumin; AST, aspartate aminotransferase; AFP, serum alpha-fetoprotein; HBV DNA, hepatitis B virus deoxyribonucleic acid. |
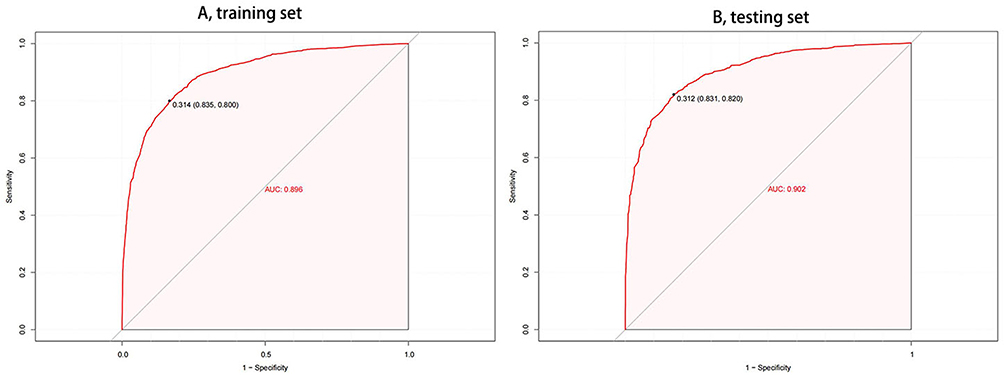 |
Figure 3 The AUC of the nomogram model in the training (A) and testing set (B). |
A Comparative Analysis of the Predictive Performance Between the Nomogram Model and Other Established HBV-Related HCC Risk Scores Models
The five existing HCC risk scores— aMAP, PAGE-B, HCC Rescue, AASL, and CU-HCC—were calculated based on the parameters we collected. The AUC analysis demonstrated that the nomogram model exhibited significantly superior predictive performance for HCC compared with the other risk scores in both the training and testing sets (Figure 4). The AUC ranged from 73.7% to 85% for the previous models. The AUC for the nomogram model reached 89.7%, which was higher than that of previous models.
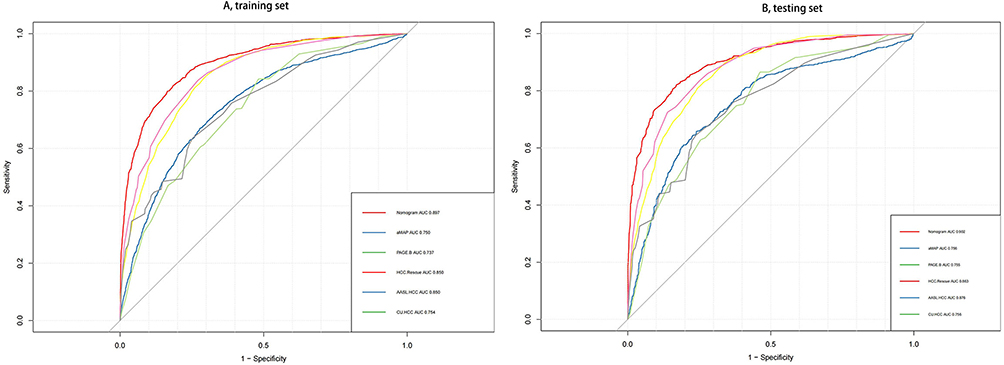 |
Figure 4 A comparative analysis of the area under the receiver operating characteristic curve (AUC) for the five HCC prediction models in both training set (A) and testing set (B). |
Figure 5 shows the DCA for the nomogram model and the previous models in the training and testing sets. The DCA indicated that the nomogram model provided a wide spectrum of threshold probabilities associated with net clinical benefits. The nomogram model improved clinical decision-making (Figure 5). These findings suggest that the nomogram model possesses a robust discriminative ability and accurate predictive performance.
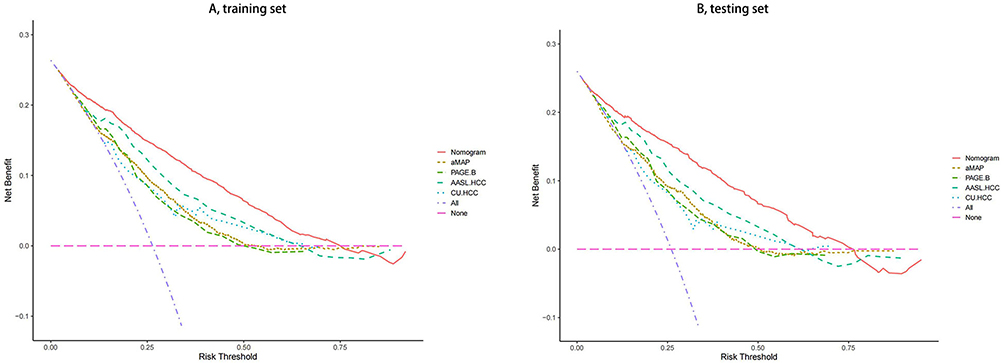 |
Figure 5 Decision curve analysis (DCA)for the nomogram model and previous models in training (A) set and testing set (B). |
Discussion
The global burden of HCC is primarily attributed to HBV infection, particularly in the East Asian and African countries. 23 Although HBV infection is a major cause of HCC, only 6.2%–9.5% of HBV-infected patients develop HCC in the absence of cirrhosis during their lifetimes, 1.7% of the 10-year cumulative incidence of liver cancer in patients with HBV infection in the immune tolerance phase.24 The annual incidence of HCC in patients with chronic HBV-related cirrhosis related cirrhosis is 3%-6%.25 Therefore, hepatitis B-related cirrhosis is categorized as a high-risk condition, both domestically and internationally, necessitating biannual HCC screening. However, individuals classified as average risk apart from the high-risk group do not benefit from semiannual screening, which exacerbates patient suffering and imposes an economic burden on the nation. Consequently, HCC risk was stratified into different risk groups to establish appropriate screening intervals. However, a single risk-stratification model cannot cover all patients with HCC. Therefore, numerous independent risk factors for HBV-related HCC and their associated predictive models have been identified. However, each exhibits distinct advantages and disadvantages across diverse populations, which limits their universal applicability. The aforementioned prediction model of antiviral therapy in hepatitis B patients does not include key virological markers such as HBV DNA and HBeAg. Additionally, hepatitis B patients who did not receive antiviral treatment lacked important indicators like advanced age, gender and cirrhosis. In contrast, our novel nomogram model covers hepatitis B patients irrespective of their antiviral treatment status and incorporates critical variables such as gender, advanced age, cirrhosis, and key virological markers including HBV DNA.
The scope of our nomogram model encompasses hepatitis B patients irrespective of antiviral treatment status and incorporates two crucial variables: cirrhosis and gender. In this study, we introduced a novel model designed to forecast the likelihood of HCC occurrence in CHB patients by utilizing commonly accessible clinical and laboratory data. This nomogram model encompasses adult CHB patients regardless of their treatment status and aims to assess the risk of HCC development, specifically in Xiamen City, southern China. In our study, age is most important predictor in our model, followed by sex, HBVDNA, AFP, cirrhosis, AST, ALB, NLR, TBIL. In line with prior research, age, sex, HBV DNA levels and cirrhosis status were significantly associated with the incidence of HCC.26,27
Consistent with a previous study,28 our findings demonstrated that the predictive performance of AASL for HCC development surpassed that of the PAGE-B and CU-HCC models in this investigation. In line with the aMAP study,7 we observed higher AUC values for the aMAP model than for the PAGE-B and CU-HCC risk scores; however, our results indicate comparable AUC values among these three scoring systems. This discrepancy may be attributed to the inclusion of various liver disease etiologies in the aMAP model, but its diminished accuracy in predicting HCC, specifically in patients with HBV etiology, highlighting the limited applicability of the current HCC stratification criteria for hepatitis B patients in China. Notably, our novel nomogram model exhibited significantly superior predictive performance (AUC=0.897) for HCC development compared with existing models, such as aMAP, PAGE-B, HCC Rescue, AASL, and CU-HCC models. The simplicity and efficiency, coupled with enhanced suitability, make our novel model an effective tool for predicting HCC risk in individuals with CHB.
Our study possesses several notable advantages that distinguish it from existing prediction models. First, this study encompassed a diverse patient population, including both individuals who received antiviral treatment and those who did not, and those whose antiviral treatment status remains unknown.
Second, compared with CU-HCC, our model incorporates gender - the most influential predictor in HCC risk stratification. Unlike REACH-B’s age limitation, our algorithm accommodates patients >65 years, addressing a critical gap in elderly population risk assessment. Furthermore, the inclusion of cirrhosis status provides superior discriminative capacity for risk stratification compared with AGED models that lack this critical parameter. In conclusion, this model incorporated common predictive factors post-antiviral treatment, such as age, gender, and presence of liver cirrhosis. Additionally, it included predictive indicators specific to non-antiviral treatment, such as HBV DNA levels, thereby enhancing its applicability to a wider spectrum of hepatitis B patients.
Third, unlike earlier models that predominantly emphasized liver cirrhosis, viral load, and liver enzyme levels, our model incorporated additional indicators reflecting inflammatory status, which may impact HCC development. While it is widely acknowledged that the NLR is linked to HCC recurrence,29 there is a paucity of predictive studies specifically addressing HCC. Our study demonstrates that a high NLR is associated with an increased risk of HCC, underscoring the significant connection between inflammation and HCC development This finding aligns with our previous descriptive study of HCC in the Xiamen,15 which showed that higher inflammatory markers, such as an elevated NLR, are associated with a higher prevalence of HCC. This further substantiates the hypothesis that inflammation plays a crucial role in the development of HCC.
Fourth, to facilitate the clinical application of the nomogram, an online tool was developed to assist healthcare providers in accurately estimating the risk of HCC among patients with HBV infection. While our study did not directly compare the diagnostic accuracies of the nomogram and Chinese screening methods, the nomogram demonstrates promising clinical utility due to its objectivity, affordability, and ease of use.
The current predictive nomogram model has several limitations. First, this study was a retrospective case-control analysis that relied on existing data rather than prospective clinical trials, which may have introduced biases and constraints in data collection and interpretation. Second, the focus on patients with hepatitis B from specific regions may restrict the generalizability of our findings to a broader population. Third, there was a potential selection bias in this study due to the reliance on available medical records to define the study population. Fourth, cirrhosis is diagnosed through a combination of radiological, endoscopic, and clinical evaluation. Patients with CHB who achieve a complete viral response (CVR) often experience fibrosis regression, including reversal of cirrhosis after five years of nucleos(t)ide analog treatment. Fifth, several studies have reported associations between HBV genotypes, core promoter mutations, sub-genotypes, and HBeAg status, and the development of HCC in CHB patients. Unfortunately, genetic analyses of these genotypes were not conducted for most participants in this study; thus, detailed indicators related to hepatitis B were not collected and we were unable to assess the impact of these factors on HCC risk. However, identifying these predictive factors in primary healthcare settings is challenging. Consequently, these predictive markers offer limited utility to general practitioners for managing patients with chronic hepatitis infections. Finally, individuals co-infected with HCV or human immunodeficiency virus (HIV) were excluded from this study; therefore, these populations may not be applicable to our model. Additionally, patients with other etiologically related liver diseases, such as autoimmune hepatitis and metabolic liver disease, were deemed ineligible.
Conclusion
In conclusion, a novel nomogram model incorporating nine factors—age, sex, liver cirrhosis, NLR, TBIL, AST, ALB, AFP, and HBV DNA—was developed to predict the risk of HCC in patients with CHB. This model demonstrated a significantly superior predictive performance for HCC development compared with the aMAP, PAGE-B, HCC Rescue, AASL and CU-HCC models. However, prospective studies across diverse populations are needed to validate the accuracy and applicability of this model. Despite its limitations, our study utilized commonly available indicators for the early screening of HBV-related HCC. Additionally, a web-based calculator (https://nomogram-model-hcc.shinyapps.io/DynNomapp/) has been developed, offering healthcare professionals a convenient and efficient tool to aid in their clinical decision-making processes.
Statement of Ethics
This study was reviewed and approved by the Ethics Committee of Zhongshan Hospital, Fudan University (Xiamen Branch)(authorization number B2020-020R).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded in part by the Medical and Health Guidance Project of Xiamen City (3502Z20244ZD1107 to Yanfang Wu), Foundation of Science and Technology Bureau of Xiamen City (3502Z20224ZD1082 to Zhenzhen Zhang), Natural Science Foundation Project of Xiamen Natural(3502Z20227386 to Guobin Chen), and Foundation of the Natural Science Foundation of Fujian Province (grant number 2022J011428 to Boheng Zhang).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (Concord-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391(10125):1023–1075. doi:10.1016/S0140-6736(17)33326-3
3. Ringelhan M, Heikenwalder M, Protzer U. Direct effects of hepatitis B virus-encoded proteins and chronic infection in liver cancer development. Dig Dis. 2013;31(1):138–151. doi:10.1159/000347209
4. El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142(6):1264–1273.e1. doi:10.1053/j.gastro.2011.12.061
5. European Association for the Study of the Liver. Electronic address: [email protected]; European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
6. Sharma SA, Kowgier M, Hansen BE, et al. Toronto HCC risk index: a validated scoring system to predict 10-year risk of HCC in patients with cirrhosis. J Hepatol;2017. S0168–8278(17)32248–1. doi:10.1016/j.jhep.2017.07.033
7. Fan R, Papatheodoridis G, Sun J, et al. aMAP risk score predicts hepatocellular carcinoma development in patients with chronic hepatitis. J Hepatol. 2020;73(6):1368–1378. doi:10.1016/j.jhep.2020.07.025
8. Papatheodoridis G, Dalekos G, Sypsa V, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J Hepatol. 2016;64(4):800–806. doi:10.1016/j.jhep.2015.11.035
9. Sohn W, Cho JY, Kim JH, et al. Risk score model for the development of hepatocellular carcinoma in treatment-naïve patients receiving oral antiviral treatment for chronic hepatitis B. Clin mol Hepatol. 2017;23(2):170–178. doi:10.3350/cmh.2016.0086
10. Yu JH, Suh YJ, Jin YJ, et al. Prediction model for hepatocellular carcinoma risk in treatment-naive chronic hepatitis B patients receiving entecavir/tenofovir. Eur J Gastroenterol Hepatol. 2019;31(7):865–872. doi:10.1097/MEG.0000000000001357
11. Papatheodoridis GV, Sypsa V, Dalekos GN, et al. Hepatocellular carcinoma prediction beyond year 5 of oral therapy in a large cohort of Caucasian patients with chronic hepatitis B. J Hepatol. 2020;72(6):1088–1096. doi:10.1016/j.jhep.2020.01.007
12. Yang HI, Yuen MF, Chan HL, et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and validation of a predictive score. Lancet Oncol. 2011;12(6):568–574. doi:10.1016/S1470-2045(11)70077-8
13. Fan C, Li M, Gan Y, et al. A simple AGED score for risk classification of primary liver cancer: development and validation with long-term prospective HBsAg-positive cohorts in Qidong, China. Gut. 2019;68(5):948–949. doi:10.1136/gutjnl-2018-316525
14. Wong VW, Chan SL, Mo F, et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J Clin Oncol. 2010;28(10):1660–1665. doi:10.1200/JCO.2009.26.2675
15. Zhang Z, Wang M, Wu Y, Chen G, Zhang B. Epidemiological and clinical characteristics of hepatocellular carcinoma in Xiamen. Cancer Epidemiol. 2024;93:102691. doi:10.1016/j.canep.2024.102691
16. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
17. Nakano M, Kuromatsu R, Niizeki T, et al. Immunological inflammatory biomarkers as prognostic predictors for advanced hepatocellular carcinoma. ESMO Open. 2021;6(1):100020. doi:10.1016/j.esmoop.2020.100020
18. Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124
19. Tada T, Kumada T, Hiraoka A, et al. Neutrophil-to-lymphocyte ratio is associated with survival in patients with unresectable hepatocellular carcinoma treated with lenvatinib. Liver Int. 2020;40(4):968–976. doi:10.1111/liv.14405
20. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
21. Xu XY, Ding HG, Li WG, et al. Guidelines for the diagnosis and treatment of liver cirrhosis. J Clin Hepatobiliary Dis. 2019;11.
22. Motomura T, Shirabe K, Mano Y, et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J Hepatol. 2013;58(1):58–64. doi:10.1016/j.jhep.2012.08.017
23. de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e180–e190. doi:10.1016/S2214-109X(19)30488-7
24. Lee HA, Lee HW, Kim IH, et al. Extremely low risk of hepatocellular carcinoma development in patients with chronic hepatitis B in immune-tolerant phase. Aliment Pharmacol Ther. 2020;52(1):196–204. doi:10.1111/apt.15741
25. Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. [The guidelines of prevention and treatment for chronic hepatitis B (2019 version)]. Zhonghua Gan Zang Bing Za Zhi. 2019;27(12):938–961. Chinese. doi:10.3760/cma.j.issn.1007-3418.2019.12.007
26. Papatheodoridis GV, Chan HL, Hansen BE, Janssen HL, Lampertico P. Risk of hepatocellular carcinoma in chronic hepatitis B: assessment and modification with current antiviral therapy. J Hepatol. 2015;62(4):956–967. doi:10.1016/j.jhep.2015.01.002
27. Hsu YC, Wu CY, Lane HY, et al. Determinants of hepatocellular carcinoma in cirrhotic patients treated with nucleos(t)ide analogues for chronic hepatitis B. J Antimicrob Chemother. 2014;69(7):1920–1927. doi:10.1093/jac/dku041
28. Wu S, Zeng N, Sun F, et al. Hepatocellular carcinoma prediction models in chronic hepatitis B: a systematic review of 14 models and external validation. Clin Gastroenterol Hepatol. 2021;19(12):2499–2513. doi:10.1016/j.cgh.2021.02.040
29. Najjar M, Agrawal S, Emond JC, et al. Pretreatment neutrophil-lymphocyte ratio: useful prognostic biomarker in hepatocellular carcinoma. J Hepatocell Carcinoma. 2018;5:17–28. doi:10.2147/JHC.S86792
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
MRI-Based Deep Learning and Radiomics Nomogram for Predicting Hepatocellular Carcinoma Recurrence Within Six Months After Thermal Ablation
Chen Y, Zhao Y, Guan W, Wu D, Zheng L, Chen C, Geng X, Qi H, Song HY, Hu H
Journal of Hepatocellular Carcinoma 2025, 12:2247-2261
Published Date: 6 October 2025