Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
A Novel Diagnostic Prediction Model for Vestibular Migraine
Authors Zhou C, Zhang L, Jiang X, Shi S, Yu Q, Chen Q, Yao D, Pan Y
Received 27 March 2020
Accepted for publication 3 July 2020
Published 29 July 2020 Volume 2020:16 Pages 1845—1852
DOI https://doi.org/10.2147/NDT.S255717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Chang Zhou, Lei Zhang, Xuemei Jiang, Shanshan Shi, Qiuhong Yu, Qihui Chen, Dan Yao, Yonghui Pan
Department of Neurology, The First Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang Province, 150000, People’s Republic of China
Correspondence: Yonghui Pan
Department of Neurology, The First Affiliated Hospital of Harbin Medical University, No. 199 Dazhi Street, Nangang District, Harbin City, Heilongjiang 150000, People’s Republic of China
Tel +86 13945693065
Email [email protected]
Background: Increasing morbidity and misdiagnosis of vestibular migraine (VM) gravely affect the treatment of the disease as well as the patients’ quality of life. A powerful diagnostic prediction model is of great importance for management of the disease in the clinical setting.
Materials and Methods: Patients with a main complaint of dizziness were invited to join this prospective study. The diagnosis of VM was made according to the International Classification of Headache Disorders. Study variables were collected from a rigorous questionnaire survey, clinical evaluation, and laboratory tests for the development of a novel predictive diagnosis model for VM.
Results: A total of 235 patients were included in this study: 73 were diagnosed with VM and 162 were diagnosed with non-VM vertigo. Compared with non-VM vertigo patients, serum magnesium levels in VM patients were lower. Following the logistic regression analysis of risk factors, a predictive model was developed based on 6 variables: age, sex, autonomic symptoms, hypertension, cognitive impairment, and serum Mg2+ concentration. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was 0.856, which was better than some of the reported predictive models.
Conclusion: With high sensitivity and specificity, the proposed logistic model has a very good predictive capability for the diagnosis of VM. It can be used as a screening tool as well as a complementary diagnostic tool for primary care providers and other clinicians who are non-experts of VM.
Keywords: headache, dizziness, cognitive function, motion sickness, magnesium ion, predictive model
Introduction
Vestibular migraine (VM) is regarded as the second most common cause of vertigo and the most common cause of spontaneous episodic vertigo, which has been recognized as a diagnostic entity over the past three decades.1 It affects about 1% of the general population and 7% of patients in dizziness clinics.2 A retrospective cohort study of adult patients with dizziness in the neurology clinic indicated that VM accounted for 19.3% and ranked second in the diagnosis of common vertigo.3 The presentation and duration of VM vary. The duration of attacks ranges from a few seconds to several days. Usually, VM attacks last between a few minutes and a few hours, and most episodes occur independently of headaches. Symptoms of VM include spontaneous and positional vertigo, ataxia, head motion vertigo/dizziness with nausea and vomiting.4 In addition, patients may have dizziness, spontaneous positional vertigo, and episodic vertigo attacks due to visual stimuli or head movements. Although a more accurate description of the disease was published by the Consensus Report of the Bárány Society and the International Headache Society than the initial version identified in 2001,5,6 due to the variation of symptoms, it is still not easy to confirm the diagnosis of VM.
A number of pathophysiological research and clinical studies have been carried out to explore the biomarkers for the diagnosis of VM.7,8 Recently, a clinical study including 67 patients was performed in China.9 The assessments focused on standardized neuro-otology bedside examination, neurological imaging, pure-tone audiogram, bithermal caloric testing, cervical X-ray or magnetic resonance imaging, and Doppler ultrasound of cerebral arteries. To differentiate central vestibular disorders (CVD) from VM, a subjective visual vertical (SVV) bucket test was conducted, and ABCD2 (age, blood pressure, clinical features, duration of symptoms, and presence of diabetes), headache/vertigo history, presence of focal neurological signs, nystagmus, and clinical head impulse testing data were collected.10 To differentiate VM patients from patients with Ménière’s disease (MD), the gene expression profile in peripheral blood mononuclear cells, levels of 14 cytokines, and levels of 11 chemokines in 129 MD patients, 82 VM patients, and 66 healthy controls were studied.11
Despite new diagnostic studies carried out, VM remains poorly understood. Today, no physical signs or test abnormalities have been identified that are pathognomonic for VM, consequently leading to misdiagnosis or mismanagement. The updated diagnostic criteria were developed by an expert panel, which may not be able to cover every aspect of the diagnosis of VM. Some modifications may be necessary for the application of the criteria to a different population. Hence, it is of great importance to conduct clinical studies and discuss operational diagnosis, in particular, to develop a predictive model to facilitate the screening and the diagnosis of VM for the primary care providers who may not be experts of VM.12 The present study was carried out considering the aforementioned significance of a predictive model.
Materials and Methods
Patients
Between August and December 2018, consecutive patients with a main complaint of dizziness from the First Affiliated Hospital of Harbin Medical University were invited to participate in this study. The diagnoses of VM were made according to the International Classification of Headache Disorders, 3rd edition (beta version).6 Only those who met the inclusion criteria were enrolled for this study. The inclusion criteria were: 1) no blindness; 2) no deafness; 3) can participate in normal communication; 4) can read and fill out the questionnaire; and 5) has signed the informed consent. Exclusion criteria were: 1) pregnant women; 2) with severe gastrointestinal diseases; 3) with metabolic diseases; 4) with mental illnesses; 5) with malignant tumors; 6) with severe heart diseases; 7) with hematological diseases; 8) with severe liver and kidney diseases; and 9) refused to sign informed consent. VM patients were assigned as the derivation cohort, and non-VM patients were assigned as controls.
This study was approved by the Ethic Committee of the First Affiliated Hospital of Harbin Medical University, Harbin, China. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consents were obtained from all of the participants.
Study Variables
Study variables were selected according to literature review and clinical experience. In this study, variables included: 1) demographic information (gender, age, history of dizziness, history of migraine); 2) clinical characteristics (duration and frequency of episodes, autonomic symptoms, -otological symptoms, imbalance, position induction, hypertension, cognitive function); and 3) laboratory test results. A rigorous questionnaire was used to collect the baseline information. The scale of Addenbrooke's Cognitive Examination Rrevised (ACE-R) was used, which was designed from the Cambridge Comprehensive Assessment Scale and revised for a large number of experiences to assess cognitive function.13
Laboratory tests mainly focused on blood sample testing. All patients were hospitalized, and their blood samples were collected during the attack of the diseases. Complete blood count, lipids, blood glucose, and serum Ca,2+ Mg2+, and folic acid were tested.
A score model was built to compare the accuracy of our logistic predictive model. To build the score model, the value of each variable was assigned according to its contribution to Logistic Regression Model 2. For example, “No autonomic symptoms” was assigned the value 1 as a reference. “Having autonomic symptoms” was assigned the value 2. The value of each variable was increased gradually and analyzed repeatedly until a maximum area under the curve (AUC) is achieved. The process was realized through custom macros.
Statistical Analyses
Quantitative data were expressed as mean±SD (standard deviation) or median (interquartile range, IQR). For the data following normal distribution, the difference between two groups was assessed by Student’s t-test. Otherwise, Wilcoxon's two-sample test was applied. Qualitative variables were presented as either absolute numbers or percentages and were analyzed by the chi-squared test or Fisher’s exact test. Statistically significant variables between VM patients and non-VM patients were included into the stepwise logistic regression model study. A receiver operating characteristic (ROC) curve plotted the true positive rate (sensitivity) against the false positive rate (1 – specificity) for all possible cutoff values. A cutoff point was obtained at the maximum Youden’s index. The predictive capacity of the logistic model was compared with that of a score model. Two-tailed tests were applied to all statistical analysis using SAS 9.2 software and p<0.05 was considered statistically significant.
Results
In total, 259 patients were invited to participate in the baseline interview and answer the questionnaire. As a result, 24 patients were excluded from this study due to lack of some important information. Eventually, 235 patients were enrolled in this study. Among them, 73 (31.06%) participants were diagnosed with VM, which constituted the derivation cohort for the development of the predictive model. The rest of the patients were diagnosed with benign paroxysmal positional vertigo (BPPV), MD, and other non-VM diseases (Table 1). It is notable that about 45% of the participants were diagnosed with cerebrovascular diseases.
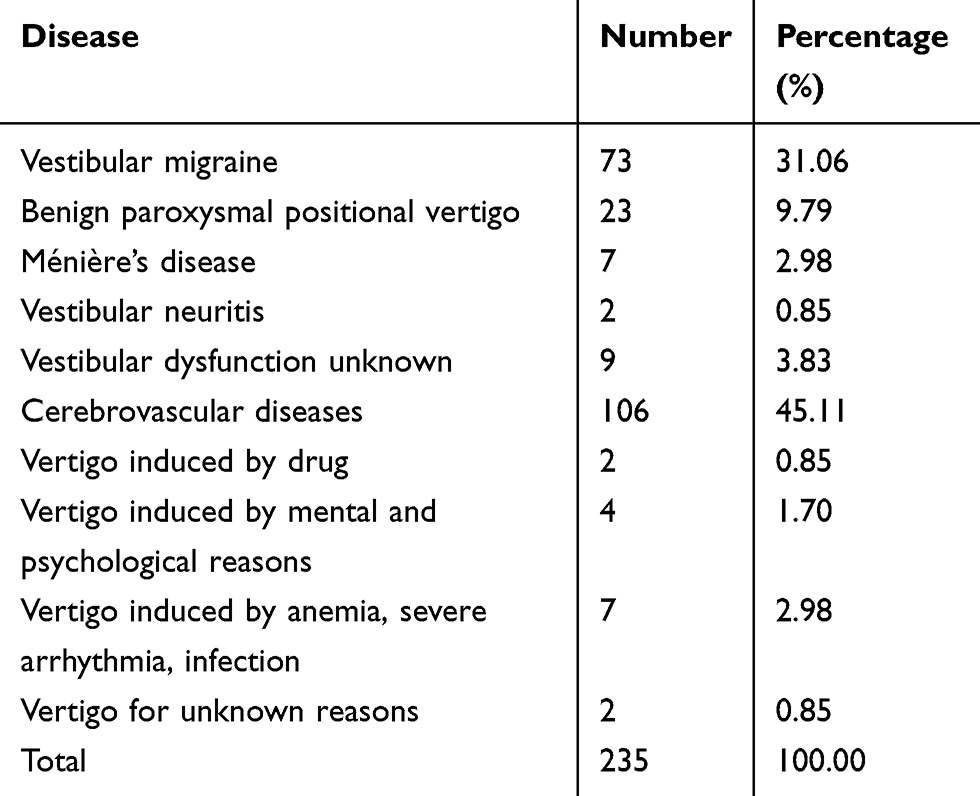 |
Table 1 Diagnostic Results of the Patients with a Main Complaint of Dizziness |
As shown in Table 2, 107 (45.53%) participants were male and 128 (54.47%) participants were female. A total of 59 out of 73 VM patients were female, who were more likely to suffer from VM (p<0.001). The average age of all participants was 62.72±10.46 years. However, the average age at diagnosis of VM was 58.3±9.26 years, which was much younger than non-VM (p<0.001). VM patients were more likely to have a longer history of dizziness, more serious symptoms of migraine, autonomic symptoms, as well as memory decline and cognitive impairment. However, the duration of symptoms, otological symptoms, imbalance, position induction, attention deficit, influence in language, and vision space drop were not significantly different between the VM and non-VM groups. In addition, the concentration of serum Mg2+ and hemoglobin in VM patients were lower than those of non-VM patients, while platelet count and the concentration of folic acid were in the opposite situation. Non-VM patients were more likely to have high blood pressure during the attack period.
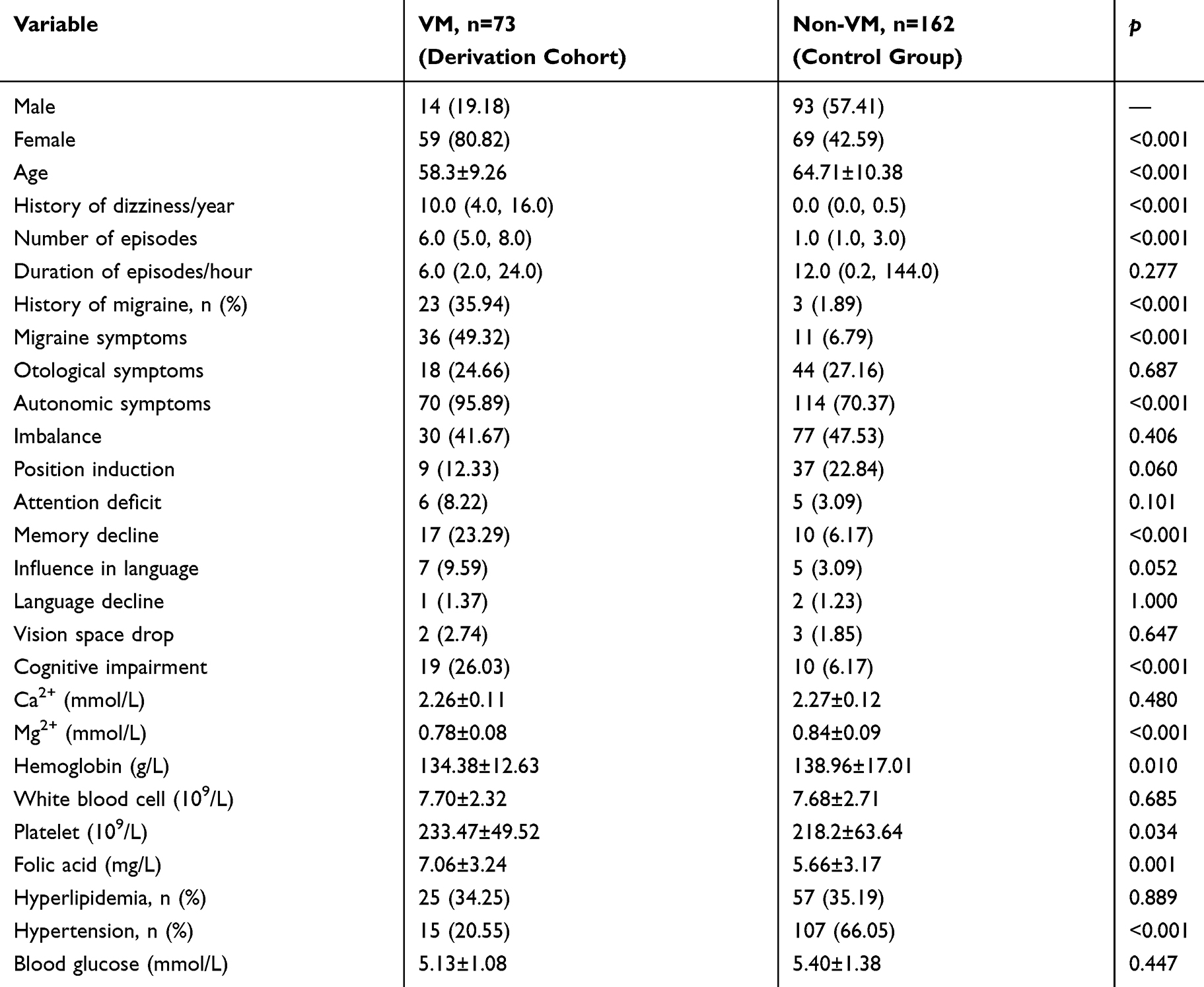 |
Table 2 Demographics and Clinical Characteristics of the Patients |
Seven out of 73 VM patients complained about auras before the attack of VM. Among them, 6 patients experienced sleepiness, fatigue, and yawning. Another one had visual problems, either blurry vision or visual blind spot. Considering the incidence of these auras were not common and the uncertainty of the causal relationship between them and VM, pertinent data were not included in the statistical analysis. In addition, 14 out of 73 VM patients and 2 out of 162 non-VM patients reported family history of migraine. Due to a lack of reliable medical records and possible recall bias, family history was not included in the statistical analysis as a risk factor either.
All patients were hospitalized due to acute attack or acute symptoms. However, we noticed interictal symptomatic states in patients. Progressive autonomic symptoms were observed in VM patients. Major autonomic symptoms included motion sickness, nausea, vomiting, movement intolerance, and fainting. Some of the VM patients experienced nervousness at the beginning, followed by nausea and vomiting. Some experienced excessive sweating and a sense of impending doom, struggling to get up and call for help. They also suffered from bowel and bladder dysfunction.
Based on the statistical significance of the study variables listed in Table 2, logistic models were built for the prediction of VM. Table 3 displays the variables (risk factors) included in Logistic Model 1, namely age, Mg2+, hemoglobin, platelet, folic acid, female, autonomic symptoms, hypertension, memory decline, and cognitive impairment. Logistic Model 2 was established by stepwise regression of Logistic Model 1. An independent variable of Logistic Model 2 was selected if the p value of one variable in Logistic Model 1 was less than 0.05. Based on the modeling study, the linear predictor (LP) for VM is shown below:
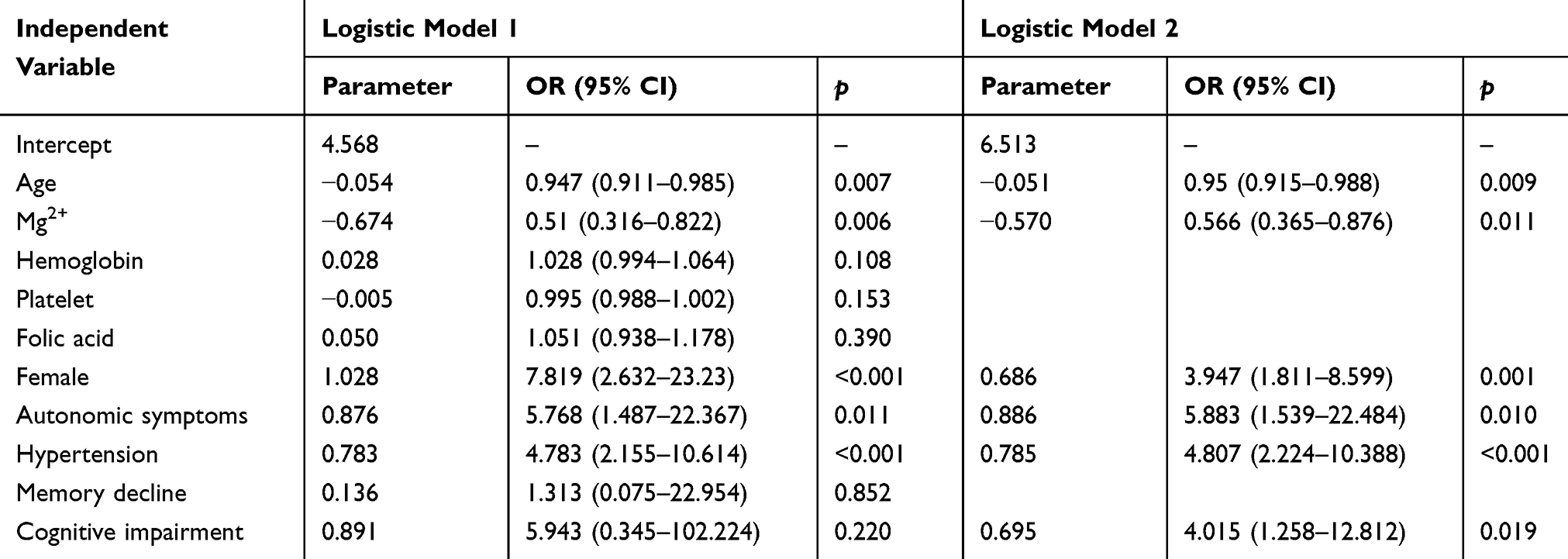 |
Table 3 Variables and Stepwise Logistic Modeling for the Prediction of Vestibular Migraine |
LPVM= 6.513 – 0.051 age + 0.686 female + 0.886 autonomic symptoms + 0.785 hypertension + 0.695 cognitive impairment – 0.570 Mg2+
To evaluate the predictive capacity of the proposed logistic model, a Score Model was developed based on the score method. Table 4 shows different variables and their scores for the development of Score Model. Receiver operating characteristic (ROC) curves of each independent variable, Logistic Model 2 and the Score Model are plotted in Figure 1. The comparison of the differentiation capacity of Logistic Model 2 and the Score Model is listed in Table 5. No statistically significant difference was found between these two models. However, the AUC of Logistic Model 2 was greater than that of the Score Model.
 |
Table 4 Levels and Scores of Different Variables in the Score Method |
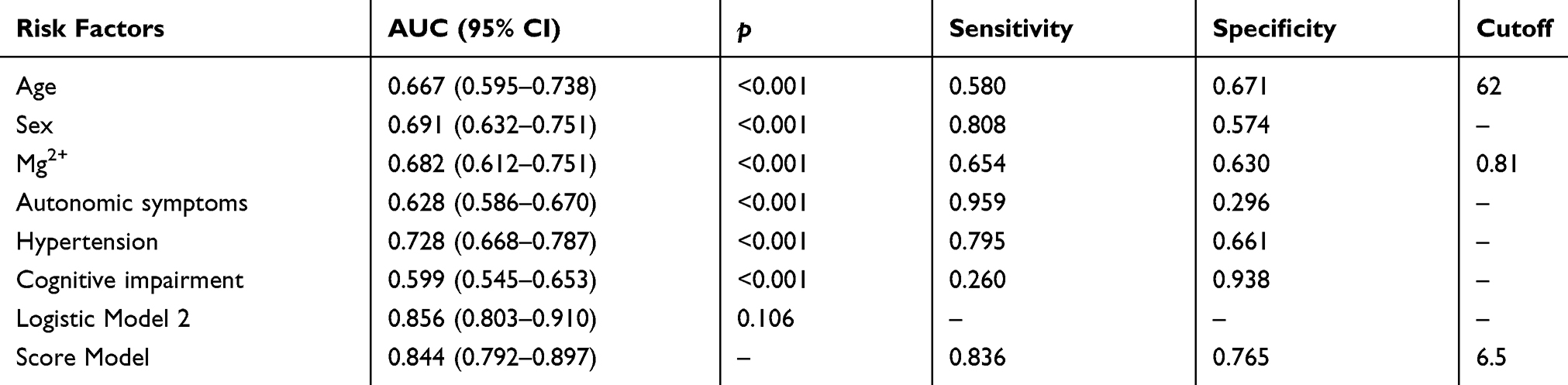 |
Table 5 Comparison of Prediction Capacity Between Logistic Model 2 and Score Model |
 |
Figure 1 Receiver operating characteristic (ROC) curves of Logistic Model 2 and the Score Model illustrating the predictive capacity of different models. The area under the curve (AUC) of ROC curves of individual variables, namely age, gender, hypertension, magnesium ion, autonomic symptoms, cognitive decline, Logistic Model 2, and the Score Model, were all greater than 0.5. Sensitivity and specificity are listed in Table 5. |
Discussion
VM has been increasingly recognized as one of the most common symptoms in clinical practice. The prevalence and morbidity of VM were variable in different populations. It was diagnosed in 10.3% of patients in Korean neurological clinics, and in 16.0% of the cases in a Belgian otorhinolaryngological clinic.14,15 The occurrence in females was 1.5–5 times higher than in males. It mainly attacks men in the fourth decade and in the third and fifth decades in women. Recently, the a cross-sectional multicentric study revealed that the age of onset of migraine was 23 years, while onset of vertigo was at 38 years.16 In another similar study carried out in Spain and Italy, the first headache occurred at 21.8±9 years old, while the first vertigo at 37.4±13.1 years old. The onset of migraine preceded the onset of vertigo by around 15 years, while the age of the first episode of migraine in VM patients does not demonstrate differences with that of the general migraineurs population.17 In this study, the average age at diagnosis of VM was 58.3±9.26 years, which was older than previous studies. The possible reason for the discrepancy in age could be that the age reported in this study was the age of diagnosis of VM, which was possible to be older than the first onset age of headache or vertigo. In addition, genetic background, lifestyle, and other environmental factors may play a role in the development of VM, leading to different onset or diagnosis age of VM.
Among the 235 patients with a main complaint of dizziness visiting the Department of Neurology in the First Affiliated Hospital of Harbin Medical University, about 31% of them were diagnosed with VM, and the occurrence of VM in females was 4 times as high as that of the males. These findings were in accordance with reported studies.18–20 In addition, about 45% of the patients were diagnosed with cerebrovascular diseases, followed by about 10% and 3% of them with BPPV and MD. The occurrence of VM is about 10 times that of MD, very similar to a previous study.21
Familial aggregation has been widely observed in migraine and episodic vertigo, and both disorders may arise from the interplay between genetic predisposition and environmental factors. In this study, only 19% of the VM patients reported a positive family history of VM, which was much lower than the reported 70.2% for migraine and 66.3% for vertigo.16 The major reason was the lack of reliable medical record and possible recall bias. Hence, family history was not discussed as a risk factor in the present study.
Although a vast number of studies have been carried out to investigate the pathognomonic changes, explore the mechanism of VM, or investigate new tests for the purpose of improving the diagnosis of VM,22–24 clinical definitive diagnosis is still hampered due to the implementation of diagnostic criteria and differential diagnosis from other vestibular disorders such as BPPV, MD, phobic postural vertigo, unilateral vestibular neuritis, posterior inferior cerebellar artery (PICA) infarction, transient ischemic attack, posterior circulation ischemia, or peripheral vestibular vertigo.25,26 In the absence of specific pathophysiological indicators, the differential diagnosis of VM is based on a history of recurrent episodes, and the symptoms or complaints could be very ambiguous because of the overlapping of symptoms and the potential need for a long period of follow-up.27 Therefore, to develop an efficient predictive model that can help the clinicians to segregate VM patients from vestibular patients whose symptoms are not because of migraine is of great clinical value.
Some studies have been carried out to develop algorithms to make the diagnosis of vertigo and dizziness easier and correct.28 One approach was the usage of standardized questionnaires.29 The predicted diagnoses from the questionnaire were compared with the “gold standard diagnosis” made by an expert panel based on clinical history, examination, and symptoms. However, due to the design of the questionnaire and the uncertainty of the causal relationship between the diagnostics and VM, the predictive accuracy for diagnosis ranges from 87% to 92%.30–32 Linear discrimination analysis was another strategy applied in predictive studies. Logistic regression identified IL-1β, CCL3, CCL22, and CXCL1 levels as capable of differentiating VM patients from MD patients. The AUC could be as great as 0.995, suggesting a high diagnostic value of these markers in patients with symptoms overlap.11
In the present study, referring to our statistical analysis of the results of a questionnaire, clinical evaluation, and blood test, a novel predictive diagnosis model for VM was developed. Only 6 variables, namely age, sex, autonomic symptoms, hypertension, cognitive impairment, and serum Mg2+ concentration, were involved in this novel logistic model. The AUC under ROC was as high as 0.856, which means the predictive capability of this model is better than some reported models.12,30
Due to the disruption of transmembrane ionic gradients, increasing the intracellular concentrations of Ca2+ and the extracellular concentrations of H+, K+, and other signaling molecules in the synaptic cleft, cortical spreading depression (CSD) could be the neurophysiological correlate of migraine aura.33 We have studied extracellular concentrations of cations and found that Mg2+ was a significant variable between VM and non-VM patients. To our knowledge, this was the first time that serum Mg2+ was included in a predictive model for the diagnosis of VM. This may be because of the strong relationship between serum Mg2+ concentration and VM. Mg2+ is associated with the synthesis and release of 5-hydroxytryptamine (5-HT), calcitonin gene-related peptide (CGRP), catecholamine, norepinephrine, and histamine.34 Mg2+ deficiency leads to central neurotransmitter 5-HT and the release of adrenaline activates abnormal excitation of cortical neurons.35 In addition, Mg2+ can significantly inhibit the vasoconstrictor activity of catecholamine, histamine, and other neurotransmitters.36 These evidences suggest that Mg2+ may play an important role in the development of VM. Furthermore, auras were only present in a few VM patients in this study. Whether it was because of a silent aura mechanism or another reason and the role of Mg2+ in the initiation of VM need further study.
This study has some limitations. Some patients reported family history of migraine. However, they failed to confirm the diagnosis or provide reliable medical records. Hence, family history was not studied as a possible risk factor. Some patients were bothered by their symptoms and were impatient when they were answering the questionnaire. Some patients were confused by some medical terms or individual episode and the period during which they have multiple episodes. Some patients were not able to evaluate the degree of headache objectively. Chances were that recall bias and confounding bias may not be well controlled from the patients’ side when they were responding to the questionnaire.37 To evaluate the performance of the proposed model, external validation should be performed in a future study.
Conclusion
With high sensitivity and specificity, the proposed logistic model has a very good predictive capability for the diagnosis of VM, which is better than some of the models reported previously. It can be used as a screening tool as well as a complementary diagnostic tool for primary care providers and other clinicians who are non-expert of VM.
Abbreviation
VM, vestibular migraine; ROC curve, receiver operating characteristic curve; AUC, area under the curve; IQR, interquartile range; BPPV, benign paroxysmal positional vertigo; MD, Ménière’s disease.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
All of the authors declare that they have no conflicts of interest.
References
1. Bisdorff AR. Management of vestibular migraine. Ther Adv Neurol Disord. 2011;4:183–191. doi:10.1177/1756285611401647
2. Takeuti AA, Favero ML, Zaia EH, Gananca FF. Auditory brainstem function in women with vestibular migraine: a controlled study. BMC Neurol. 2019;19:144. doi:10.1186/s12883-019-1368-5
3. Muelleman T, Shew M, Subbarayan R, et al. Epidemiology of dizzy patient population in a neurotology clinic and predictors of peripheral etiology. Otol Neurotol. 2017;38:870–875. doi:10.1097/mao.0000000000001429
4. Alghadir AH, Anwer S. Effects of vestibular rehabilitation in the management of a vestibular migraine: a review. Front Neurol. 2018;9:440. doi:10.3389/fneur.2018.00440
5. Lempert T, Olesen J, Furman J, et al. [Vestibular migraine: diagnostic criteria: consensus document of the Barany Society and the International Headache Society]. Der Nervenarzt. 2013;84(4):511–516. doi:10.1007/s00115-013-3768-x. German.
6.. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202.
7. King S, Priesol AJ, Davidi SE, et al. Self-motion perception is sensitized in vestibular migraine: pathophysiologic and clinical implications. Sci Rep. 2019;9(1):14323. doi:10.1038/s41598-019-50803-y
8. Udagatti VD, Dinesh Kumar R. Migraine related vertigo. Indian J Otolaryngol Head Neck Surg. 2017;69(4):563–567. doi:10.1007/s12070-017-1101-x
9. Zhang Y, Kong Q, Chen J, et al. International Classification of Headache Disorders 3rd edition beta-based field testing of vestibular migraine in China: demographic, clinical characteristics, audiometric findings and diagnosis statues. Cephalalgia. 2016;36(3):240–248. doi:10.1177/0333102415587704
10. Chang TP, Winnick AA, Hsu YC, Sung PY, Schubert MC. The bucket test differentiates patients with MRI confirmed brainstem/cerebellar lesions from patients having migraine and dizziness alone. BMC Neurol. 2019;19(1):219. doi:10.1186/s12883-019-1442-z
11. Flook M, Frejo L, Gallego-Martinez A, et al. Differential proinflammatory signature in vestibular migraine and meniere disease. Front Immunol. 2019;10:1229. doi:10.3389/fimmu.2019.01229
12. Friedland DR, Tarima S, Erbe C, Miles A. Development of a statistical model for the prediction of common vestibular diagnoses. JAMA Otolaryngol Head Neck Surg. 2016;142:351–356. doi:10.1001/jamaoto.2015.3663
13. Ridley N, Batchelor J, Draper B, et al. Cognitive screening in substance users: diagnostic accuracies of the mini-mental state examination, addenbrooke’s cognitive examination-revised, and montreal cognitive assessment. Journal of Clinical and Experimental Neuropsychology. 2018;40(2):107–122. doi:10.1080/13803395.2017.1316970
14. Van Ombergen A, Van Rompaey V, Van de Heyning P, Wuyts F. Vestibular migraine in an otolaryngology clinic: prevalence, associated symptoms, and prophylactic medication effectiveness. Otol Neurotol. 2015;36:133–138. doi:10.1097/mao.0000000000000596
15. Cho SJ, Kim B-K, Kim B-S, et al. Vestibular migraine in multicenter neurology clinics according to the appendix criteria in the third beta edition of the International classification of headache disorders. Cephalalgia. 2016;36(5):454–462. doi:10.1177/0333102415597890
16. Teggi R, Colombo B, Albera R, et al. Clinical features, familial history, and migraine precursors in patients with definite vestibular migraine: the VM-phenotypes projects. Headache. 2018;58(4):534–544. doi:10.1111/head.13240
17. Teggi R, Colombo B, Albera R, et al. Clinical features of headache in patients with diagnosis of definite vestibular migraine: the VM-phenotypes projects. Front Neurol. 2018;9:395. doi:10.3389/fneur.2018.00395
18. Dieterich M, Obermann M, Celebisoy N. Vestibular migraine: the most frequent entity of episodic vertigo. J Neurol. 2016;263 Suppl 1:S82–89. doi:10.1007/s00415-015-7905-2
19. Geser R, Straumann D. Referral and final diagnoses of patients assessed in an academic vertigo center. Front Neurol. 2012;3:169. doi:10.3389/fneur.2012.00169
20. Vukovic V, Plavec D, Galinović I, et al. Prevalence of vertigo, dizziness, and migrainous vertigo in patients with migraine. Headache. 2007;47:1427–1435. doi:10.1111/j.1526-4610.2007.00939.x
21. Cherchi M, Hain TC. Migraine-associated vertigo. Otolaryngol Clin North Am. 2011;44:
22. Maranhao ET, Maranhao-Filho P, Luiz RR, Vincent MB. Migraine patients consistently show abnormal vestibular bedside tests. Arq Neuropsiquiatr. 2016;74:22–28. doi:10.1590/0004-282X20150180
23. Yang YJ, Choi JE, Kim MT, et al. Measurement of horizontal ocular deviation on magnetic resonance imaging in various disease with acute vertigo. PLoS One. 2019;14(10):e0224605. doi:10.1371/journal.pone.0224605
24. Kang WS, Lee SH, Yang CJ, et al. Vestibular function tests for vestibular migraine: clinical implication of video head impulse and caloric tests. Front Neurol. 2016;7:166. doi:10.3389/fneur.2016.00166
25. Salmito MC, Morganti LOG, Nakao BH, et al. Vestibular migraine: comparative analysis between diagnostic criteria. Braz J Otorhinolaryngol. 2015;81(5):485–490. doi:10.1016/j.bjorl.2015.07.007
26. Stroke & Vertigo Association of Chinese Stroke. A. Multidisciplinary experts consensus for assessment and management of vestibular migraine. Chin Med J (Engl). 2019;132(2):183–189. doi:10.1097/CM9.0000000000000064.
27. Radtke A, Neuhauser H, von Brevern M, Hottenrott T, Lempert T. Vestibular migraine–validity of clinical diagnostic criteria. Cephalalgia. 2011;31:906–913. doi:10.1177/0333102411405228
28. Luo J, Erbe C, Friedland DR. Unique clinical language patterns among expert vestibular providers can predict vestibular diagnoses. Otol Neurotol. 2018;39:1163–1171. doi:10.1097/mao.0000000000001930
29. Pavlou M, Whitney SL, Alkathiry AA, et al. Visually induced dizziness in children and validation of the pediatric visually induced dizziness questionnaire. Front Neurol. 2017;8:656. doi:10.3389/fneur.2017.00656
30. Lampl C, Rapoport A, Levin M, Brautigam E. Migraine and episodic Vertigo: a cohort survey study of their relationship. J Headache Pain. 2019;20:33. doi:10.1186/s10194-019-0991-2
31. Zhao JG, Piccirillo JF, Spitznagel EL
32. Feil K, Feuerecker R, Goldschagg N, et al. Predictive capability of an iPad-based medical device (medx) for the diagnosis of vertigo and dizziness. Front Neurol. 2018;9:29. doi:10.3389/fneur.2018.00029
33. Espinosa-Sanchez JM, Lopez-Escamez JA. New insights into pathophysiology of vestibular migraine. Front Neurol. 2015;6:12. doi:10.3389/fneur.2015.00012
34. van Dongen RM, Zielman R, Noga M, et al. Migraine biomarkers in cerebrospinal fluid: A systematic review and meta-analysis. Cephalalgia. 2017;37:49–63. doi:10.1177/0333102415625614
35. Rinosl H, Skhirtladze K, Felli A, Ankersmit HJ, Dworschak M. The neuroprotective effect of magnesium sulphate during iatrogenically-induced ventricular fibrillation. Magnesium Res. 2013;26(3):109–119. doi:10.1684/mrh.2013.0345
36. Pedersen SH, Ramachandran R, Amrutkar DV, et al. Mechanisms of glyceryl trinitrate provoked mast cell degranulation. Cephalalgia. 2015;35:1287–1297. doi:10.1177/0333102415574846
37. Edlow JA, Gurley KL, Newman-Toker DE. A new diagnostic approach to the adult patient with acute dizziness. J Emerg Med. 2018;54(4):469–483. doi:10.1016/j.jemermed.2017.12.024
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.