Back to Journals » Clinical Ophthalmology » Volume 16
A Novel Cost-Effective Simulation Model for Continuous Curvilinear Capsulorhexis
Authors Solyman O ![]() , Abu Serhan H
, Abu Serhan H ![]() , Kamel HF, Eldib A, Abo Obaia AS, Aref A, Sayed-Ahmed IO, Khashaba M, Khodeiry MM, Abushanab MM
, Kamel HF, Eldib A, Abo Obaia AS, Aref A, Sayed-Ahmed IO, Khashaba M, Khodeiry MM, Abushanab MM ![]()
Received 20 June 2022
Accepted for publication 9 August 2022
Published 24 August 2022 Volume 2022:16 Pages 2759—2764
DOI https://doi.org/10.2147/OPTH.S378298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video 1 of "A Cost-Effective Simulation Model for CCC" [ID 378298].
Views: 630
Omar Solyman,1,2 Hashem Abu Serhan,3 Hesham F Kamel,1 Amgad Eldib,1,4– 6 Ahmed S Abo Obaia,1 Amr Aref,1 Ibrahim Osama Sayed-Ahmed,7,8 Mohamed Khashaba,9 Mohamed M Khodeiry,1,8 Mokhtar M Abushanab1
1Department of Ophthalmology, Research Institute of Ophthalmology, Giza, Egypt; 2Department of ophthalmology, Qassim University Medical City, Al-Qassim, Saudi Arabia; 3Department of Ophthalmology, Islamic Hospital, Amman, Jordan; 4Division of Paediatric Ophthalmology, Strabismus, and Adult Motility, UPMC Children’s Hospital of Pittsburgh, Pittsburgh, PA, USA; 5UPMC Eye Center, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 6University of Pittsburgh School of Medicine, Pittsburgh, PA, USA; 7Department of Ophthalmology, Baylor College of Medicine, Houston, TX, 77030, USA; 8Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, 33136, USA; 9Department of Anesthesiology, Research Institute of Ophthalmology, Giza, Egypt
Correspondence: Omar Solyman, Department of Ophthalmology, Research Institute of Ophthalmology, Giza, Egypt, Email [email protected]
Introduction: We describe and validate a low-cost simulation model for practicing anterior lens capsule continuous curvilinear capsulorhexis (CCC).
Methods: A simulation model for CCC was developed from widely available low-cost materials. Ophthalmologists attending the annual scientific meeting of the Research Institute of Ophthalmology, Giza, Egypt, were asked to perform a five CCC model task and then anonymously answer a questionnaire that assessed the realism and training utility of the model using a five-point Likert scale (1 = unacceptable, 2 = poor, 3 = acceptable, 4 = favorable and 5 = excellent).
Results: Twenty-seven ophthalmologists completed the task and the anonymous questionnaire. Overall, participants felt that the model simulated CCC step in cataract surgery well (mean: 3.5) and was comparable to other kinds of CCC simulation models (mean: 3.3). The model scored highly for its overall educational value (mean: 4.00) and for enlarging a small CCC (mean:3.7), while the feasibility of this model in practicing the management of a runaway leading edge of CCC scored 2.9.
Conclusion: This model may provide an alternative method for training for CCC and other anterior lens capsule-related maneuvers. This option may be particularly helpful for residency training programs with limited access to virtual reality simulators or commercially available synthetic eye models.
Keywords: cataract simulation, capsulorhexis, capsulotomy, microsurgical model
Introduction
Supervised training is the cornerstone in developing a competent eye surgeon.1 The COVID-19 pandemic has resulted in a huge disruption of postgraduate surgical training programs all over the world, secondary to lockdown consequences, resulting in reduction or suspension of elective surgeries. With the pandemic lasting more than expected, simulation-based training has played a significant role in residency and fellowship training programs across the world, to improve the surgical efficiency of the trainees and to reduce intraoperative complications.2 Phacoemulsification cataract surgery is notorious for its steep learning curve. The Continuous curvilinear capsulorhexis (CCC) is one of the most challenging steps of the procedure.3,4 A high-quality CCC is recognized by experienced surgeons as one of the most important early steps in safe phacoemulsification.5 Herein, we describe a novel, non-expensive method of microsurgical simulation of CCC.
Methods
This project was approved by the human research ethics committee of the Research Institute of Ophthalmology, Giza, Egypt, and was performed in accordance with all local laws and in compliance with the principles of the Declaration of Helsinki. A written informed consent was obtained from all study participants. Supplies of this simulation model of CCC are derived from widely available materials (Figure 1) and consist of an empty circular medication cell, a cellophane sheet (Outus Cello Sheets ®), a piece of facial tissue, an upholstery nail tack, staples, and a stapler. To assemble the simulation model (Supplementary video 1), a piece of cellophane sheet is placed underneath the medication cell. The head of the upholstery nail tack is placed between the two layers of the folded facial tissue and is placed below the cellophane sheet. The three layers consisting of the medication cell, the cellophane sheet, and the facial tissue are stapled together. A 3mm wide opening was made in the medication cell to act as the clear corneal incision. The model was then fixed to a piece of foam. A buttonhole was made in a latex glove to accommodate the circular tablet medication cell and the rest of the glove was wrapped around the model to act as the conjunctiva. The model was then fit into the eye space of a commercially available mask toy (Figure 2).
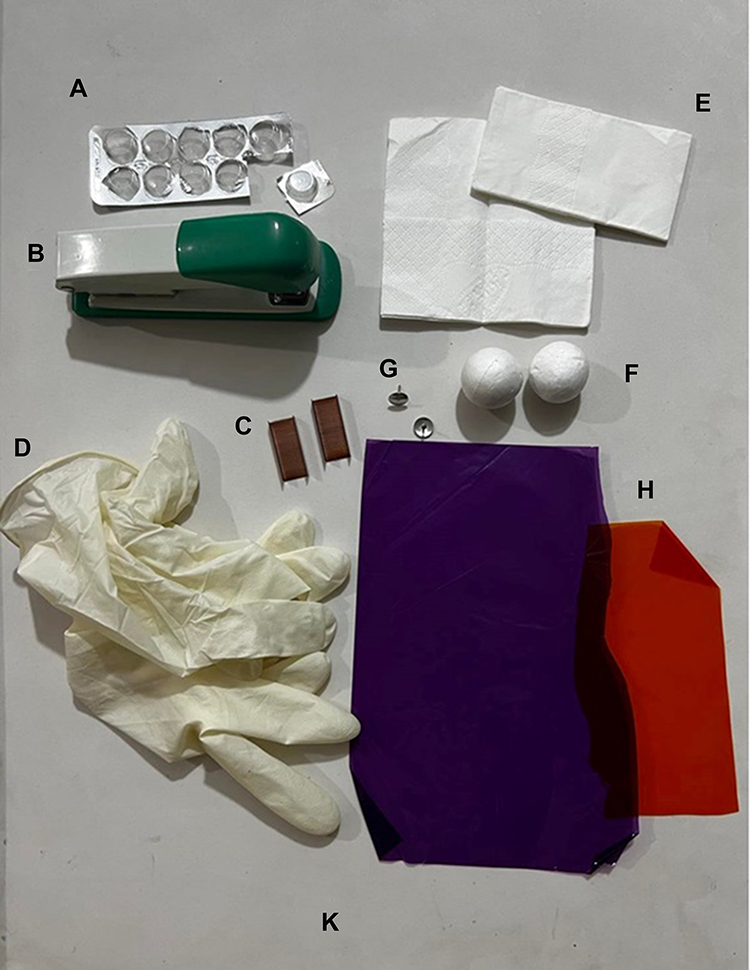 |
Figure 1 A photograph illustrating the supplies required to assemble this simulation model including circular medication pill strip (A), stapler (B), staples (C), Latex gloves (D), facial tissues (E), Upholstery nail tack (G), foam balls (F), cellophane sheets (H), and a cardboard (K). |
 |
Figure 2 A photograph illustrating the simulation model attached to a commercially available toy face mask ready for practicing. |
Ophthalmologists attending the 3-day annual meeting of the Research Institute of Ophthalmology, Giza, Egypt were asked to participate in this study. Each participant was asked to complete a task of performing CCC on five simulation models under a surgical microscope using five different CCC instruments including a cystotome, a Utrata forceps, an Akahoshi cross-action capsulorhexis forceps, an Inamura cross action capsulorhexis forceps, and a 20-gauge microsurgical capsulorhexis forceps. The questionnaire consisted of eight questions; five rating questions using a five-point Likert scale, two multiple-choice, and one yes/no question (Appendix 1).
Results
Twenty-seven ophthalmologists completed the questionnaire. The responses showed that our model can simulate real-life CCC (average rate = 3.5/5). In addition, >95% of the respondents recommended this model as a beneficial educational model (42.3% of them rated the model as an excellent educational value).
This model did simulate real-life CCC particularly when used with Utrata capsulorhexis forceps and cystotome capsulorhexis (85.19%, 77.78%); however, CCC could be reproducibly practiced using other different types of capsulorhexis forceps (Figure 3, Supplementary videos 2, 3, 4, 5, 6, 7, 8, and 9). In addition, the can opener anterior capsulotomy technique required for classic sutured extracapsular cataract extraction was successfully simulated using this model (66.67%).
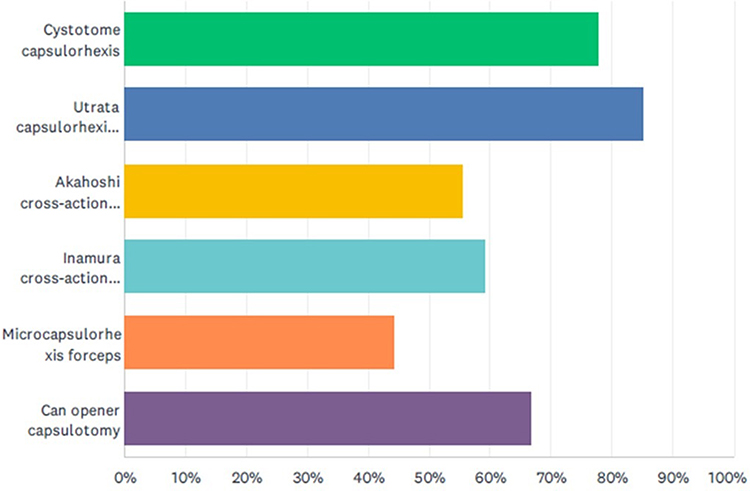 |
Figure 3 A graph showing the utility of this model for simulation of different capsulotomy techniques. |
Seventy-four percent of participants reported prior use of one or more CCC simulation models (Table 1). This CCC simulation model was felt to be overall comparable to other kinds of CCC simulation models experienced by participants (mean: 3.3).
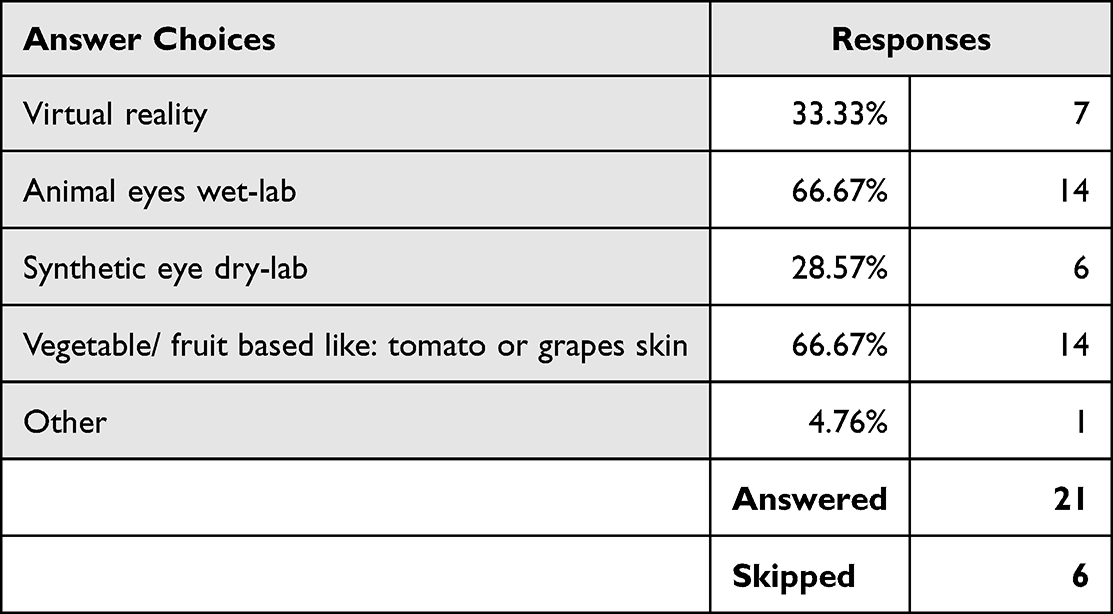 |
Table 1 Comparison Between Current Model and to Other Kinds of CCC Simulation Models Experienced by Participants |
Discussion
Described simulation techniques of CCC for microscopic surgical training include the use of pieces of fruit such as grapes and tomatoes.1,6 Despite being readily available and affordable, these models may render CCC unrealistically easier because of the absence of anterior chamber-like closed space and the unlimited access through a small incision. The use of eye bank human eyes,7 postmortem cadaveric human eyes,8 and animal eyes (including pig’s,9 rabbit’s10 and goat’s11 eyes) have also been described as an effective method of cataract surgery simulation that provided significant improvement of cataract surgical skills including extracapsular cataract extraction,12 and manual small incision cataract surgery.13 In addition to the cost, sterility, the need for special preservation and disposal, and safety to use in the operating room if a dedicated microsurgical training laboratory is not available are the main concerns. Moreover, the lens capsule in animal eyes has different behavior that is not close to reality compared to a human’s lens capsule. This may result in misconceptions for novice surgeons and the development of wrong surgical techniques.14 Virtual reality surgical simulators have become a standard training tool in cataract surgery in many ophthalmology residency training programs worldwide. Several studies using The Eyesi Surgical (VRmagic, Mannheim, Germany) virtual reality simulator demonstrated a reduction in the rate of complications in live cataract surgery following training on the virtual reality simulator.11 The high cost remains the main limitation towards the availability of such virtual reality microsurgical simulators in residency training programs in many developing countries.
Chalfin described the use of cellophane to serve as an artificial anterior lens capsule for CCC simulation under the surgical microscope.15 In a video presentation, Stoll and Gimbel simulated CCC by stretching a cellophane sheet over silly putty to provide different degrees of difficulties related to anterior lens capsule convexity.16 Currently, a variety of synthetic eyes are commercially available that employ the principle of using the cellophane sheet to simulate the anterior lens capsule for training on CCC such as The FCI Kitaro® DryLab (FCI S.A.S. - PARIS – France), and SimuloRhexis® (InsEYEt, LLC Westlake Village, CA, USA)12,17–19.
The advantages of this model include the affordability, and the ease of assembly from widely available materials. The use of latex glove to act as the conjunctiva allows the surgeon to use the other hand to prevent movement of the globe as per real-life surgery. The trainees can practice CCC as many times as needed using a cystotome and/or different types of capsulorhexis forceps to build their preferences. Cellophane-based anterior lens capsule CCC models behavior resembles en-vivo anterior lens capsule when viscoelastic is applied to it at the time of the practice.14 We found that wetting the cellophane with a few drops of water renders cellophane closely similar to the anterior lens capsule in behavior during intraoperative CCC which helped when viscoelastic was not available. This model also allows tailoring varying degrees of anterior capsule convexity and tension by conforming the facial tissue to different degrees of convexity and changing the stretch over the cellophane sheets before stapling them. Since cellophane can come in different textures, experimentation with different cellophane textures can help simulate different behaviors of the anterior lens capsule such as pediatric, stained, and aging anterior lens capsule.
Conclusion
This model can provide a viable, cost-effective alternative for CCC training and other anterior capsule-related maneuvers. This model may be particularly helpful for residency training programs with limited access to virtual reality simulators or commercially available synthetic eye models.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Figueira EC, Wang LW, Brown TM, et al. The grape: an appropriate model for continuous curvilinear capsulorhexis. J Cataract Refract Surg. 2008;34(9):1610–1611. doi:10.1016/j.jcrs.2008.04.049
2. Devaraj A, Satheesh AN, Panicker GJ, Kaliyaperumal S. Wetlab training during COVID-19 era; an ophthalmology resident’s perspective. Indian J Ophthalmol. 2021;69(1):158–159. doi:10.4103/ijo.IJO_3496_20
3. Dooley IJ, O’Brien PD. Subjective difficulty of each stage of phacoemulsification cataract surgery performed by basic surgical trainees. J Cataract Refract Surg. 2006;32(4):604–608. doi:10.1016/j.jcrs.2006.01.045
4. Gauba V, Tsangaris P, Tossounis C, Mitra A, McLean C, Saleh GM. Human Reliability Analysis of Cataract Surgery. Arch Ophthalmol Chic Ill. 2008;126(2):173–177. doi:10.1001/archophthalmol.2007.47
5. Webster R, Sassani J, Shenk R, Good N. A haptic surgical simulator for the continuous curvilinear capsulorhexis procedure during cataract surgery. Stud Health Technol Inform. 2004;98:404–406.
6. Benjamin L. Training in Surgical Skills. Community Eye Health. 2002;15(42):19–20.
7. Rootman DS, Marcovich A. Utilizing eye bank eyes and keratoplasty techniques to teach phacoemulsification. Ophthalmic Surg Lasers. 1997;28(11):957–960. doi:10.3928/1542-8877-19971101-15
8. Liu ES, Eng KT, Braga-Mele R. Using medical lubricating jelly in human cadaver eyes to teach ophthalmic surgery. J Cataract Refract Surg. 2001;27(10):1545–1547. doi:10.1016/s0886-3350(01
9. Hashimoto C, Kurosaka D, Uetsuki Y. Teaching continuous curvilinear capsulorhexis using a postmortem pig eye with simulated cataract(2)(2). J Cataract Refract Surg. 2001;27(6):814–816. doi:10.1016/s0886-3350(00)00728-8
10. Ruggiero J, Keller C, Porco T, Naseri A, Sretavan DW. Rabbit models for continuous curvilinear capsulorhexis instruction. J Cataract Refract Surg. 2012;38(7):1266–1270. doi:10.1016/j.jcrs.2012.01.034
11. Lee R, Raison N, Lau WY, et al. A systematic review of simulation-based training tools for technical and non-technical skills in ophthalmology. Eye. 2020;34(10):1737–1759. doi:10.1038/s41433-020-0832-1
12. Alwadani S. Cataract surgery training using surgical simulators and wet-labs: course description and literature review. Saudi J Ophthalmol. 2018;32(4):324–329. doi:10.1016/j.sjopt.2018.01.003
13. Ramani S, Pradeep TG, Sundaresh DD. Effect of wet-laboratory training on resident performed manual small-incision cataract surgery. Indian J Ophthalmol. 2018;66(6):793–797. doi:10.4103/ijo.IJO_1041_17
14. Stuart Stol. Lecture: using Simulation to Conquer the CCC. Available from: https://www.youtube.com/watch?v=KrU6kBV9b44.
15. Chalfin S. A simple device for teaching capsulorhexis technique. Invest Ophthalmol Vis Sci. 2015;37(3):S768.
16. Stoll S, Gimbel H. Learning Capsularhexis; 2006. Available from: https://vjcrgs.com/archive/2006.
17. Pandey SK, Sharma V. Cataract surgery training during ophthalmology residency in India: challenges and how to overcome them? Indian J Ophthalmol. 2017;65(12):1279–1280. doi:10.4103/ijo.IJO_1032_17
18. SimulEYE®. SimulEYE. Available from: https://www.simuleye.com.
19. Ophthalmics FCI. KITARO® COMBOLAB (Dry Lab + Wet Lab) Kit. FCI Ophthalmics. Available from: https://fci-ophthalmics.com/products/kitaro-dry-wet-lab.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.