Back to Journals » Clinical Interventions in Aging » Volume 20
A Nomogram Model for Predicting Prolonged Postoperative LOS After Total Knee Arthroplasty in Osteoarthritis Patients
Authors Qi H ![]() , Zhang B, Lu D, Lian F
, Zhang B, Lu D, Lian F
Received 28 July 2025
Accepted for publication 1 December 2025
Published 9 December 2025 Volume 2025:20 Pages 2481—2492
DOI https://doi.org/10.2147/CIA.S556772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Zhi-Ying Wu
Haoran Qi,1 Bo Zhang,1 Daifeng Lu,1 Feng Lian1,2
1Department of Orthopaedic Surgery, The Fourth Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, 150001, People’s Republic of China; 2Centre for Leading Medicine and Advanced Technologies of IHM, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China
Correspondence: Feng Lian, Email [email protected]
Purpose: The purpose of this study was to construct and validate a preoperative and intraoperative factor-based nomogram model to predict the risk of prolonged postoperative length of stay after primary total knee arthroplasty for osteoarthritis patients.
Materials and Methods: The study included patients undergoing primary TKA for knee osteoarthritis between June 2022 and November 2024. Patients were randomly split into training (70%) and validation (30%) cohorts. Potential predictors were screened using LASSO regression and subsequently incorporated into a multivariate logistic regression to build the nomogram. The model’s performance was assessed using the area under the receiver operating characteristic curve, calibration curves, and decision curve analysis.
Results: A total of 295 patients were included, with an average age of 66.58 ± 6.88 years. Least absolute shrinkage and selection operator regression identified 12 potential predictors, and multivariate logistic regression further refined these to four independent risk factors: age, knee flexion range of motion, operation time, and American Society of Anesthesiologists classification. The nomogram demonstrated strong predictive performance, with the area under the receiver operating characteristic curve values of 0.912 (95% CI: 0.858– 0.966) in the training set and 0.817 (95% CI: 0.697– 0.938) in the validation set. Calibration curves showed excellent agreement between predicted and observed outcomes, and decision curve analysis indicated significant clinical utility across a wide range of threshold probabilities.
Conclusion: The model, based on age, knee flexion range of motion, operation time, and American Society of Anesthesiologists classification, provides a practical tool for clinicians to assess individual risks, optimize resource allocation, and improve patient outcomes. It is important to note that this was a single-center, retrospective study, and further validation in multi-center, prospective cohorts is recommended to confirm its generalizability.
Keywords: osteoarthritis, knee arthroplasty, prolonged postoperative length of stay, nomogram, risk prediction
Introduction
Osteoarthritis (OA) affects 7% of the global population, over 500 million people worldwide.1 Knee OA (KOA) is a leading cause of chronic pain and long-term disability in the elderly.2,3 The progression of KOA is typically accompanied by declining joint function and a marked reduction in quality of life. The central therapeutic goals are to relieve pain and restore function, beginning with conservative measures such as lifestyle modification and pharmacological treatment.4 Pharmacotherapy includes oral analgesics/anti-inflammatory drugs and intra-articular injections of hyaluronic acid, platelet-rich plasma (PRP), or botulinum toxin, which aim to alleviate symptoms and potentially slow disease progression.5 When these conservative and minimally invasive interventions fail to control symptoms in end-stage disease, patients often proceed to total knee arthroplasty (TKA), widely regarded as the definitive treatment for advanced KOA.6
By the year 2030, worldwide TKA procedure volumes are anticipated to surpass the million mark each year.7 As the number of surgeries continues to rise, how to effectively manage postoperative recovery, particularly how to reduce the length of hospital stay (LOS) during hospitalization, has become a key goal in medical practice.8,9 Prolonged LOS may not only increase the risk of hospital-acquired infections but also significantly raise treatment costs and hospital operating expenses.10 Therefore, reducing prolonged LOS has become an important measure to optimize medical resources and reduce healthcare costs.
A nomogram can integrate multiple clinical variables to generate an intuitive risk assessment model. By presenting complex data in a graphical format, it transforms the information into charts that are easier to understand, enabling clinicians to more accurately assess a patient’s postoperative recovery progress and make more informed treatment decisions.11–15
Although previous studies have examined factors influencing LOS after TKA, multivariable nomograms built solely from readily available pre-operative data remain scarce.10,16,17 We therefore hypothesized that integrating pre- and intra-operative variables could yield a high-performance nomogram capable of accurately predicting prolonged LOS. Prolonged LOS was defined as any hospital stay exceeding the 75th percentile of the LOS distribution among all enrolled patients, a threshold commonly used in previous studies to flag outliers with exceptionally long stays.18,19 This study sought to develop and internally validate such a model to enable early identification of high-risk patients, optimize resource allocation, and facilitate personalized care.
Materials and Methods
Patients
This study retrospectively analyzed patients who underwent TKA at the Fourth Affiliated Hospital of Harbin Medical University from June 20, 2022, to November 18, 2024. The inclusion criteria were as follows: (1) patients aged between 50 and 90 years with knee OA; (2) undergoing TKA for the first time.
The exclusion criteria were as follows: (1) incomplete medical records; (2) undergoing bilateral surgery or revision surgery; (3) patients with a history of previous TKA. (4) postoperative infection or deep vein thrombosis. (5) Non-osteoarthritic causes, such as rheumatoid arthritis and traumatic injury, necessitated TKA.
All included TKAs were performed by two experienced arthroplasty surgeons (>100 annual procedures) using consistent surgical protocols and identical implant materials.
All patients followed the same standardized rehabilitation protocol and were discharged upon meeting the following criteria: (1) stable laboratory test results; (2) dry surgical wound without signs of complications; and (3) ability to ambulate independently with assistive devices.
This study was conducted in strict accordance with the principles of the Declaration of Helsinki. All patient data were de-identified before collection and analysis; informed consent was waived because of the retrospective design. The study protocol was approved by the Medical Ethics Committee of the Fourth Affiliated Hospital of Harbin Medical University (approval No. 2025-llsc-22).
Sample Size Justification
The sample size was calculated on the basis of the events per variable (EPV) metric, a widely recommended method for ensuring the stability and generalizability of logistic regression models.20–22 The sample size was estimated as (number of variables × EPV) ÷ event rate. In our training cohort, the incidence of prolonged LOS was approximately 20%. With four predictor variables and an EPV of 10, the required sample size was 200.
Potential Predictive Factors
The predictive factors used in this study include: (1) socio-demographic variables such as age, sex, body mass index (BMI), marital status, insurance status, and household registration, (2) comorbidities such as hypertension, diabetes, (3) preoperative variables such as American Society of Anesthesiologists’ physical status classification (ASA), duration of symptoms, knee flexion range of motion, range of knee extension deficit, previous knee surgery, walking ability, stair-climbing ability, red blood cell count (RBC), white blood cell count (WBC), platelet count (PLT), hemoglobin (Hb), sodium, creatinine, total bilirubin (TBIL), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and Hip-Knee-Ankle (HKA) angle, (4) intraoperative variables such as anesthesia, operation side, blood loss, and operation time, (5) other variables such as seasonality of admission, and seasonality of discharge. Due to possible high collinearity between underlying comorbidities (including pulmonary, cardiovascular, and liver diseases, stroke, and other chronic conditions) and ASA classification, only ASA grades were recorded in this study.
Outcome
The outcome of the study is to predict the risk of prolonged postoperative LOS in patients who have knee osteoarthritis undergoing primary total knee arthroplasty. The LOS is defined as the difference between the discharge and admission dates, both of which were automatically recorded by the hospital’s electronic health record system.23 If admission and discharge occur on the same day, the LOS is counted as one day. The average length of hospital stay in our institution was 10.87 ± 3.13 days. According to previous literature, prolonged LOS is defined as a hospital stay duration exceeding the 75th percentile of all patients’ LOS.18,19 According to this hospital’s data, LOS exceeding 12 days is defined as prolonged LOS.
Data Analyses
The dataset from the Fourth Affiliated Hospital of Harbin Medical University was randomly divided into groups, with 70% of the samples included in the training set to establish a predictive model, and 30% of the samples included in the validation set for internal validation. Variables with >15% missing values were excluded; those with ≤15% missing were imputed using multiple-imputation methods. The description of data analyses was presented in the form of mean ± standard deviation (x±s). For categorical data, descriptive statistics were presented as counts and relative frequencies. Numerical variables were assessed through independent samples t-tests, whereas qualitative variables were evaluated using either Pearson’s chi-square test or Fisher’s exact probability test, depending on distributional assumptions. The least absolute shrinkage and selection operator (LASSO) method was used for variable selection to determine the best predictive variables among the risk factors of prolonged LOS after TKA. In the LASSO regression model, the optimal λ value was determined through cross-validation, and feature variables with non-zero coefficients were screened out. Then, the non-zero coefficient variables screened out by LASSO regression analysis were included in multivariable logistic regression analysis to further identify the independent risk factors for prolonged LOS. Finally, a nomogram prediction model was developed based on the identified independent risk factors. The performance of the model was assessed through the receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA). In this study, results were considered statistically significant when the p-value was less than 0.05.
All data analyses in this study were conducted using R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria). LASSO regression was implemented using the “glmne”” package. Multivariate logistic regression analysis was performed using the““gl”” function. Nomograms and calibration curves were generated using the““rm”” package. The net benefit of the predictive model in this study was assessed using decision curve analysis, which was plotted using the““rmd”” package. ROC and the area under the curve (AUC) were calculated using the““pRO”” package.
The figure below provides a detailed depiction of the study design and methodological steps (Figure 1).
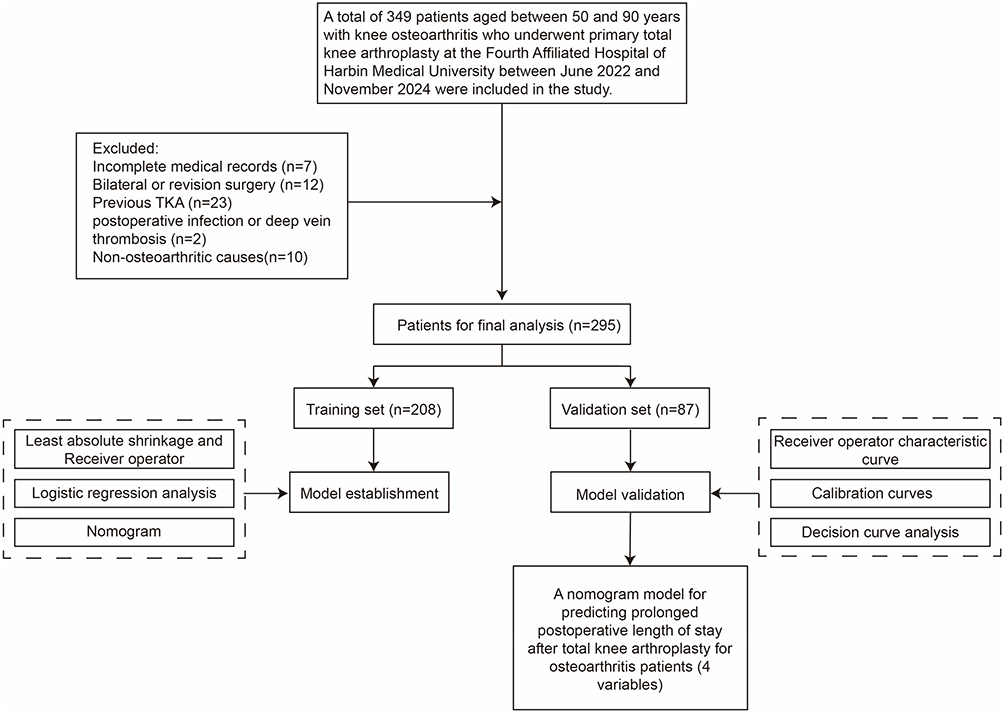 |
Figure 1 Flowchart of this study. Abbreviations: OA, osteoarthritis; TKA, total knee arthroplasty; ROC curve, receiver operating characteristic curve; DCA, decision curve analysis. |
Results
Patients’ Characteristics
This study enrolled a total of 295 participants, with an average age of 66.58±6.88. The participants were divided into a training set (n=208) and a validation set (n=87) in a 7:3 ratio. Table 1 and Supplementary Table 1 summarize the baseline characteristics of the training and validation sets, showing no significant differences in clinical variables between the two cohorts.
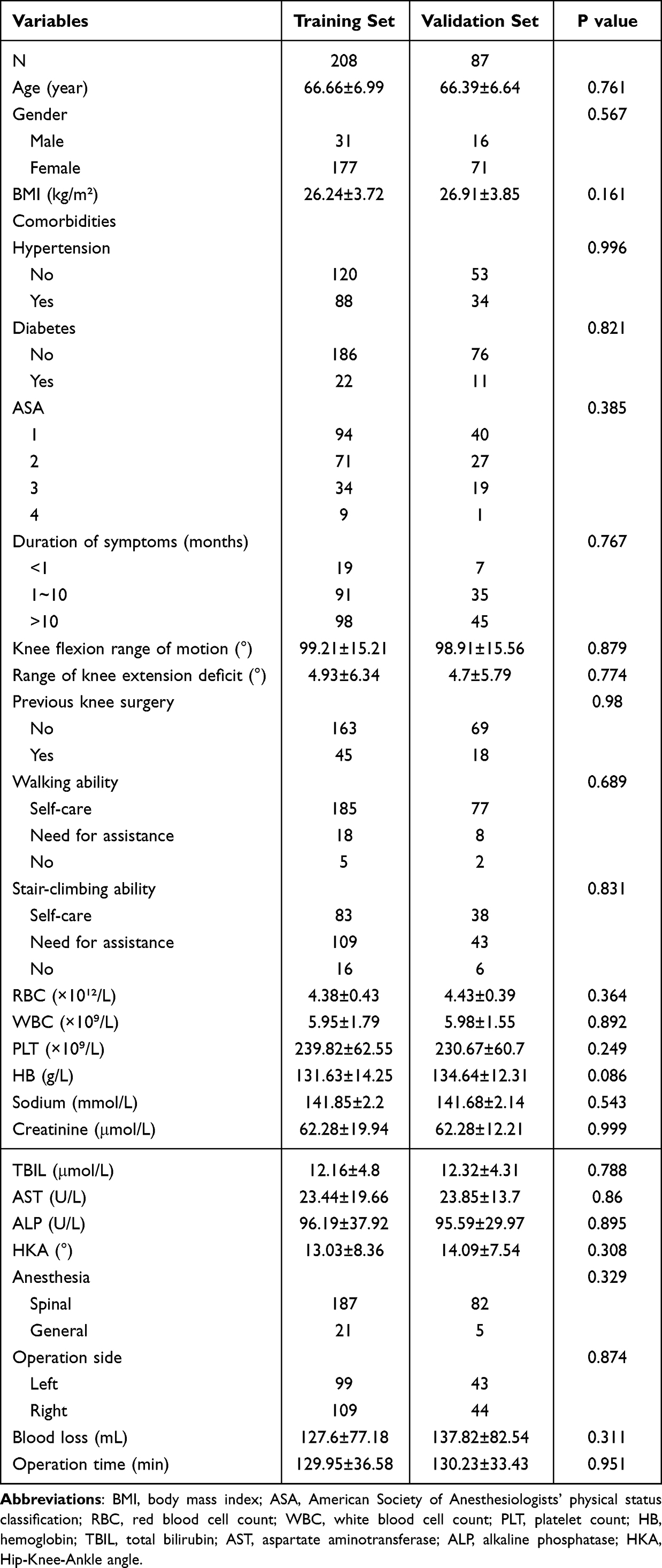 |
Table 1 Characteristics of Participants in the Training Set and the Validation Set |
Variable Selection
In this study, LASSO regression analysis method was employed to screen 31 candidate variables for feature selection, aiming to optimize the model fitting performance. Through LASSO regression analysis, a total of 12 potential predictive factors were identified, including: age, knee flexion range of motion, range of knee extension deficit, operation time, RBC, WBC, HB, creatinine, household registration, hypertension, seasonality of admission, ASA (Figure 2). Subsequently, the selected variables were incorporated into multivariate logistic regression analysis, ultimately identifying four independent risk factors with statistical significance (p<0.05): age, knee flexion range of motion, operation time, and ASA (Table 2).
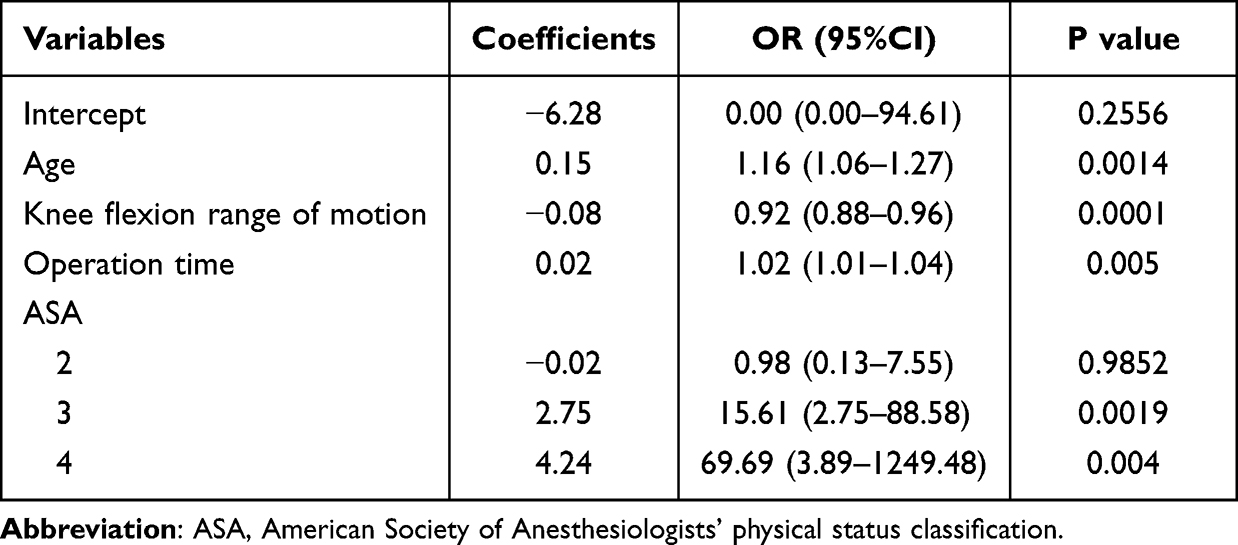 |
Table 2 Results of Multivariate Logistic Regression Analysis Based on LASSO Regression |
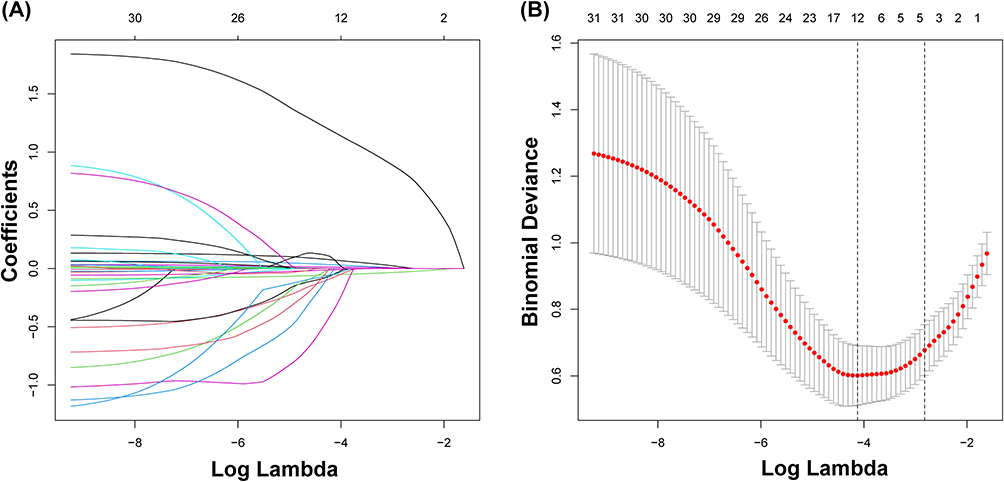 |
Figure 2 Results of LASSO regression. (A) Distribution of LASSO coefficients for the 31 features. Each curve represents the trajectory of changes in the coefficients of the independent variables. The vertical axis indicates the coefficients, while the horizontal axis represents log lambda. (B) Cross-validation plot of LASSO. The optimal parameter lambda is 0.016, indicating that the prediction model achieves the minimum error at this value. Abbreviation: LASSO, the least absolute shrinkage and selection operator. |
Construction of the Nomogram Model
The final predictive nomogram was developed by incorporating the four independent risk factors selected through a two-stage analytical approach: initial variable screening via LASSO regression followed by confirmation through multivariate logistic regression analysis (Figure 3). This model visually presents the scores for each risk factor, allowing users to obtain corresponding scores on the scale line of each variable based on the patient’s specific conditions. Subsequently, the scores of all variables are summed to obtain a total score, and the predicted probability of prolonged LOS after TKA surgery for OA patients can be read on the total score scale line. To facilitate bedside use, we further translated the nomogram into a freely accessible, web-based calculator that provides instantaneous risk estimates for any combination of predictor values (https://prediction-for-outcome.shinyapps.io/dynnomapp/).
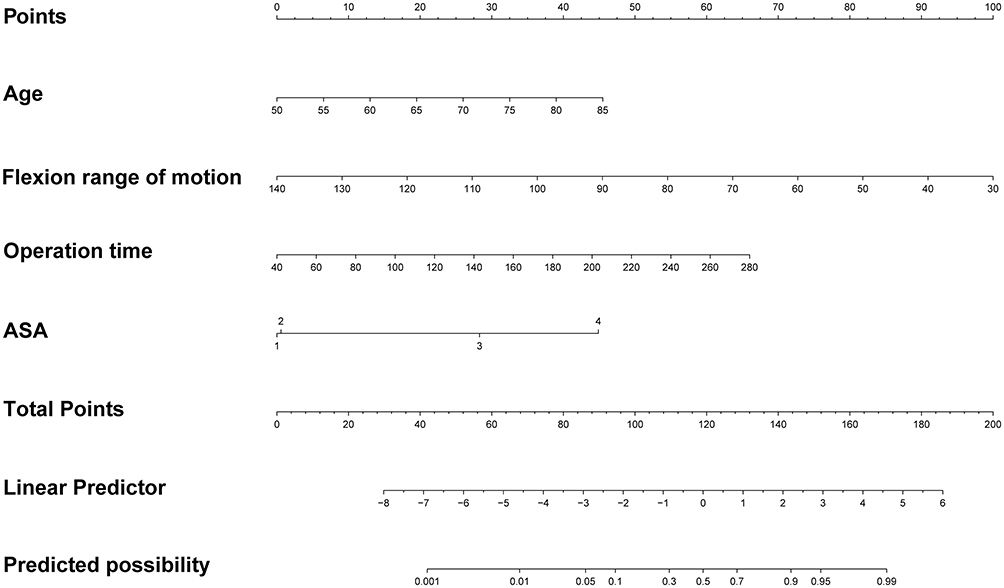 |
Figure 3 Nomogram for predicting prolonged postoperative LOS risk after TKA in OA patients. Abbreviations: LOS, the length of hospital stay; TKA, total knee arthroplasty; OA, osteoarthritis; ASA, American Society of Anesthesiologists’ physical status classification. |
Test and Evaluation
The nomogram model’s discriminative ability was evaluated by plotting ROC curves. The AUC for the training set was 0.912 (95% CI 0.858–0.966) with 79.5% sensitivity, 92.9% specificity and a maximum Youden index of 0.72, while the validation set achieved an AUC of 0.817 (95% CI 0.697–0.938) with 63.2% sensitivity and 94.1% specificity, indicating strong discriminative performance of the nomogram (Figure 4). Furthermore, the Hosmer–Lemeshow test returned χ² = 5.98 (P = 0.649) for the training set and χ² = 7.43 (P = 0.545) for the validation set, while the calibration plots for both cohorts closely tracked the ideal 45-degree line; together these findings indicate excellent agreement between predicted and observed probabilities of prolonged LOS and confirm the good calibration of the nomogram (Figure 5). Finally, DCA indicated that the model yielded a positive net benefit over the entire threshold range of 2–100% in the training set and 4–98% in the validation set (Figure 6).
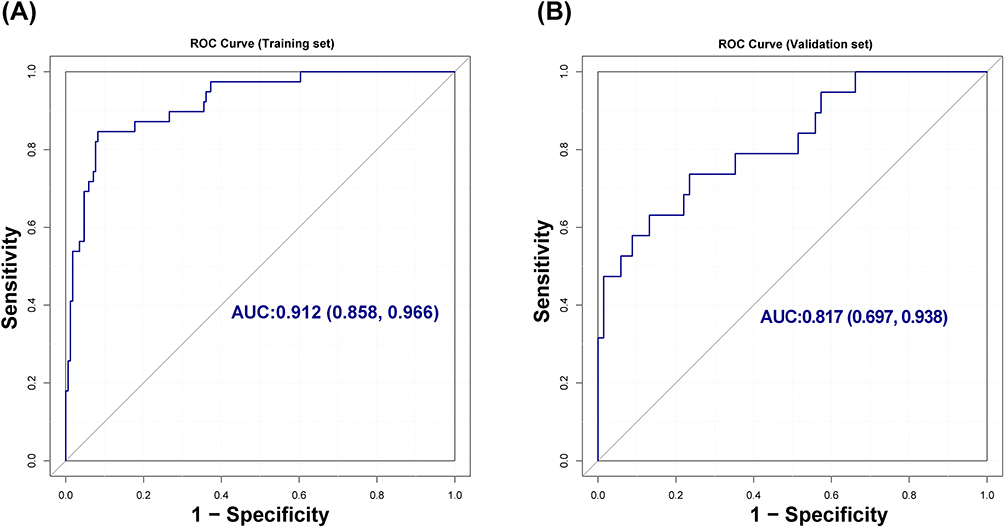 |
Figure 4 ROC curves. (A) The ROC curve of the training set, 0.912 (95% CI 0.858–0.966). (B) The ROC curve of the validation set, 0.817 (95% CI 0.697–0.938). |
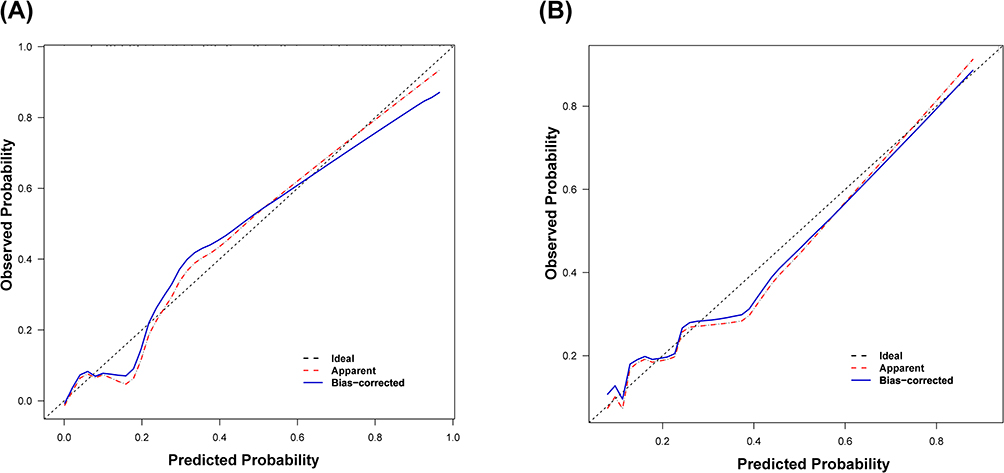 |
Figure 5 Calibration curve. (A) The calibration curve of the training set. (B) The calibration curve of the validation set. |
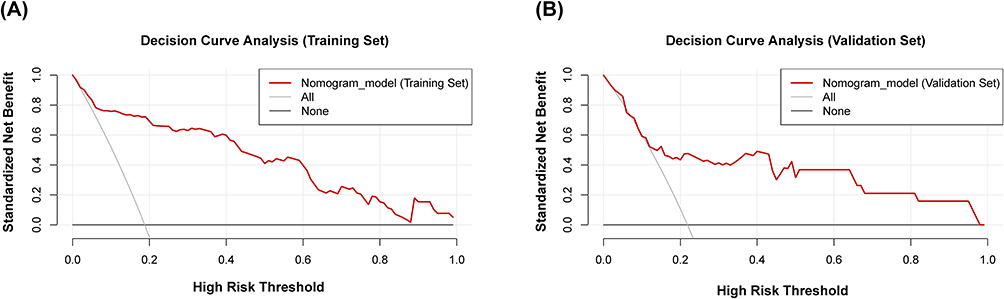 |
Figure 6 DCA curves. (A) The DCA curve of the training set. (B) The DCA curve of the validation set. Abbreviation: DCA, decision curve analysis. |
Discussion
This study utilized LASSO regression analysis and multivariate logistic regression analysis to identify four independent risk factors: age, knee flexion range of motion, operation time, and ASA. Based on these factors, a nomogram prediction model was constructed. The model demonstrated excellent discriminative ability in both the training and validation sets, with AUC values of 0.912 and 0.817, respectively. The calibration curve analysis demonstrates a strong agreement between the predicted probabilities and the observed prolonged LOS in both the training and validation sets. Further confirmation through DCA showed that the model provided significant net benefits across a wide range of thresholds, supporting its value in clinical decision-making.
Advanced age is significantly associated with prolonged postoperative LOS. Due to the decline in physiological functions and reduced organ reserve capacity, the overall health status of elderly patients is generally poorer compared to younger patients. Studies have shown that the prevalence of comorbidities, such as cardiovascular diseases, diabetes, and chronic respiratory diseases, significantly increases with age.24,25 These comorbidities not only elevate surgical risks but also impede postoperative recovery. Additionally, elderly patients are more prone to perioperative complications, including deep vein thrombosis, pulmonary infections, and cognitive dysfunction, which often lead to extended hospital stays.26–28 Therefore, in clinical practice, special attention must be paid to the perioperative management of elderly patients undergoing TKA.
ASA classification, as an important indicator of preoperative health status, aligns with our findings, as many studies have shown that higher ASA grades are associated with longer LOS.29–31 Operative time directly reflects the complexity of the surgery and intraoperative risks, serving as a key variable in predicting postoperative recovery. Bohl et al32 analyzed NSQIP data from 165,474 patients who underwent primary total joint arthroplasty (TJA) between 2006 and 2013, finding that every 15-minute increase in operative time was associated with a 9% higher risk of prolonged LOS (>4 days) (P < 0.001). Similarly, Sodhi et al33 analyzed NSQIP data from 225,344 patients who underwent primary TKA between 2008 and 2016, demonstrating that each 30-minute increase in operative time was significantly correlated with prolonged LOS (P < 0.001). These findings consistently indicate that prolonged operative time is a significant predictor of extended postoperative hospitalization.
Preoperative knee flexion range of motion is negatively correlated with prolonged postoperative LOS. The preoperative range of motion (ROM) of the knee joint directly reflects the functional status of the periarticular soft tissues as well as the degree of pathological changes in the joint itself. Patients with poor preoperative ROM typically indicate a higher degree of synovial fibrosis and more severe OA.34 Previous studies have demonstrated that preoperative ROM status significantly influences the final ROM after TKA, and patients with knee stiffness typically exhibit poorer postoperative outcomes compared to those with better preoperative ROM.35,36 Therefore, patients with limited preoperative knee flexion range of motion may require longer rehabilitation interventions and physical therapy during the postoperative recovery process, thereby increasing their LOS. Furthermore, Matassi et al37 analyzed data from 122 patients with arthropathy and found that systematic preoperative functional exercise significantly promotes rapid postoperative recovery in patients with knee arthritis. This finding suggests that preoperative rehabilitation training should be incorporated into the overall treatment plan for patients.
The significant advantage of this research lies in its comprehensive evaluation of a broader range of potential risk factors. In the assessment of knee joint function, prior studies often had a vague conceptualization of knee range of motion.38,39 In addition to knee flexion, this study also included an extension deficit and systematically screened a wide range of candidate variables, such as household registration and the HKA angle. Although these factors were not retained in the final parsimonious model, this comprehensive selection process strengthens our confidence in the robustness of the ultimately chosen predictors. Notably, unlike previously published models, our nomogram uniquely incorporates pre-operative knee-flexion range of motion—an objective functional marker—and is restricted entirely to variables available before or during surgery, maximising clinical utility. Furthermore, moving beyond traditional paper-based scoring tools, we translated the nomogram into a freely accessible web calculator that allows surgeons to obtain an instant, precise risk estimate in the outpatient clinic and to tailor peri-operative care and rehabilitation pathways to each patient.
Despite the positive outcomes achieved in model construction and validation, this study has some limitations. First, although the internal validation was robust, the single-center retrospective design and limited sample size may restrict the model’s generalizability; external validation in larger, multicenter cohorts is therefore essential. Second, the relatively large number of initial predictor variables compared with the sample size entails a potential risk of overfitting in the prediction model. Third, the definition of “prolonged LOS” in this study was based on the 75th percentile of the LOS distribution observed at our institution. Although this relative, distribution-derived cut-off is commonly used in statistical modeling, it may somewhat limit the direct comparability of the model across institutions with different baseline LOS patterns. In addition, this study aims to enable doctors to quickly predict the LOS after TKA using only preoperative and intraoperative variables. Postoperative factors that may potentially prolong LOS (such as rehabilitation training, complications, and knee function scores) were not collected.
Conclusion
In summary, this study investigated the correlation between preoperative and intraoperative variables and the prolonged postoperative LOS in patients who have knee osteoarthritis undergoing primary total knee arthroplasty. Through LASSO regression analysis and multivariate logistic regression analysis, four independent risk factors were ultimately identified: age, knee flexion range of motion, operation time, and ASA. Based on these four risk factors, we constructed a nomogram model for prolonged LOS, designed to accurately predict the risk of prolonged postoperative LOS in patients who have knee osteoarthritis undergoing primary total knee arthroplasty. Future multicenter, prospective studies are recommended to further validate and refine this model, ensuring its generalizability across diverse healthcare settings.
Ethics Statement
All patient data were de-identified before collection and analysis; informed consent was waived because of the retrospective design. The study protocol was approved by the Medical Ethics Committee of the Fourth Affiliated Hospital of Harbin Medical University (approval No. 2025-llsc-22).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Research Funds of Centre for Leading Medicine and Advanced Technologies of IHM (2023IHMO1072) and the Natural Science Foundation of Heilongjiang Province (PL2024H141). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou H, Shen X, Yan C, et al. Extracellular vesicles derived from human umbilical cord mesenchymal stem cells alleviate osteoarthritis of the knee in mice model by interacting with METTL3 to reduce m6A of NLRP3 in macrophage. Stem Cell Res Ther. 2022;13(1):322. doi:10.1186/s13287-022-03005-9
2. Zhuang Z, Si L, Wang S, et al. Knee cartilage defect assessment by graph representation and surface convolution. IEEE Transactions Med Imaging. 2023;42:368–379. doi:10.1109/tmi.2022.3206042
3. Atik I, Gul E, Atik S. Evaluation of the relationship between knee osteoarthritis and meniscus pathologies. Malawi Med J. 2024;36:48–52. doi:10.4314/mmj.v36i1.8
4. Poenaru D, Sandulescu MI, Potcovaru CG, Cinteza D. High-intensity laser therapy in pain management of knee osteoarthritis. Biomedicines. 2024;12:
5. Poenaru D, Sandulescu MI, Cinteza D. Pain modulation in chronic musculoskeletal disorders: botulinum toxin, a descriptive analysis. Biomedicines. 2023;11:
6. Giordano R, Ghafouri B, Arendt-Nielsen L, Petersen KK. Inflammatory biomarkers in patients with painful knee osteoarthritis: exploring the potential link to chronic postoperative pain after total knee arthroplasty-a secondary analysis. Pain. 2024;165:337–346. doi:10.1097/j.pain.0000000000003042
7. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision Hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Hoint Surg Am. 2007;89:780–785. doi:10.2106/jbjs.F.00222
8. Long H, Zeng C, Shi Y, Wang H, Xie D, Lei G. Length of stay and inpatient charges of total knee arthroplasty in China: analysis of a national database. Chin Med J. 2023;136:2050–2057. doi:10.1097/cm9.0000000000002220
9. Maman D, Laver L, Becker R, Mahamid A, Berkovich Y. Robotic-assisted total knee arthroplasty reduces postoperative complications and length of stay without increased cost compared to navigation-guided techniques: a national analysis. Knee Surg Sports Traumatol Arthroscopy. 2024. doi:10.1002/ksa.12348
10. Tornese D, Robustelli A, Ricci G, Rancoita PMV, Maffulli N, Peretti GM. Predictors of postoperative hospital length of stay after total knee arthroplasty. Singapore Med J. 2024;65:68–73. doi:10.11622/smedj.2021142
11. Yang X, Yang Y, Weng X, Zhang M. Nomogram for predicting disease-specific survival in osteosarcoma. Chin Med J. 2022;135:1126–1128. doi:10.1097/cm9.0000000000001837
12. Tian W, Luo L, Xu X, et al. Nomogram for predicting intolerable postoperative early enteral nutrition following definitive surgery for small intestinal fistula: a cohort study. Int J Surg. 2024;110:5595–5604. doi:10.1097/js9.0000000000001655
13. Liao T, Lu Y, Su T, et al. Development and validation of prognostic nomogram for cirrhotic patients with acute kidney injury upon ICU admission. Int Emerg Med. 2024;19:49–58. doi:10.1007/s11739-023-03436-z
14. Lyu X, Liu J, Gou Y, Sun S, Hao J, Cui YJV. Development and validation of a machine learning‐based model of ischemic stroke risk in the Chinese elderly hypertensive population. View. 2024;5:20240059.
15. Yuan Y, Zhang X, Wang Y, et al. Multimodal data integration using deep learning predicts overall survival of patients with glioma. View. 2024;5:20240001.
16. Sayegh MJ, Garbarino LJ, Gold PA, et al. Does time spent in the post-anesthesia care unit affect hospital lengths of stay following primary total knee arthroplasty? J Knee Surg. 2024;37:43–48. doi:10.1055/s-0042-1759791
17. Johnson DJ, Castle JP, Hartwell MJ, D’Heurle AM, Manning DW. Risk factors for greater than 24-hour length of stay after primary total knee arthroplasty. J Arthroplasty. 2020;35:633–637. doi:10.1016/j.arth.2019.10.037
18. Liu H, Xing F, Jiang J, Chen Z, Xiang Z, Duan X. Random forest predictive modeling of prolonged hospital length of stay in elderly Hip fracture patients. Front Med. 2024;11:1362153. doi:10.3389/fmed.2024.1362153
19. Vollmer A, Nagler S, Hörner M, et al. Performance of artificial intelligence-based algorithms to predict prolonged length of stay after head and neck cancer surgery. Heliyon. 2023;9:e20752. doi:10.1016/j.heliyon.2023.e20752
20. van Smeden M, Moons KG, de Groot JA, et al. Sample size for binary logistic prediction models: beyond events per variable criteria. Stat Meth Med Res. 2019;28:2455–2474. doi:10.1177/0962280218784726
21. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165:710–718. doi:10.1093/aje/kwk052
22. Yuan X, Xu Q, Du F, et al. Development and validation of a model to predict cognitive impairment in traumatic brain injury patients: a prospective observational study. EClinicalMedicine. 2025;80:103023. doi:10.1016/j.eclinm.2024.103023
23. Kong G, Wu J, Chu H, et al. Predicting prolonged length of hospital stay for peritoneal dialysis-treated patients using stacked generalization: model development and validation study. JMIR Med Inform. 2021;9:e17886. doi:10.2196/17886
24. Kitridis D, Tsikopoulos K, Givissis P, Chalidis B. Mortality and complication rates in nonagenarians and octogenarians undergoing total Hip and knee arthroplasty: a systematic review and meta-analysis. Eur Geriatric Med. 2022;13:725–733. doi:10.1007/s41999-022-00610-y
25. Varady NH, Amen TB, Rudisill SS, Adcock K, Bovonratwet P, Ast MP. Same-day discharge total knee arthroplasty in octogenarians. J Arthroplasty. 2023;38:96–100. doi:10.1016/j.arth.2022.08.013
26. Gonçalves TJM, Gonçalves S, Nava N, et al. Perioperative immunonutrition in elderly patients undergoing total hip and knee arthroplasty: impact on postoperative outcomes. JPEN J Parenter Enteral Nutr. 2021;45:1559–1566. doi:10.1002/jpen.2028
27. Delsmann MM, Schmidt C, Mühlenfeld M, et al. Prevalence of osteoporosis and osteopenia in elderly patients scheduled for total knee arthroplasty. Arch Orthopaedic Trauma Surg. 2022;142:3957–3964. doi:10.1007/s00402-021-04297-x
28. Kappenschneider T, Maderbacher G, Weber M, et al. Special orthopaedic geriatrics (SOG) - a new multiprofessional care model for elderly patients in elective orthopaedic surgery: a study protocol for a prospective randomized controlled trial of a multimodal intervention in frail patients with Hip and knee replacement. BMC Musculoskeletal Disorders. 2022;23:1079. doi:10.1186/s12891-022-05955-w
29. Li H, Jiao J, Zhang S, Tang H, Qu X, Yue B. Construction and comparison of predictive models for length of stay after total knee arthroplasty: regression model and machine learning analysis based on 1826 cases in a single singapore center. J Knee Surg. 2022;35:7–14. doi:10.1055/s-0040-1710573
30. Keswani A, Lovy AJ, Robinson J, Levy R, Chen D, Moucha CS. Risk factors predict increased length of stay and readmission rates in revision joint arthroplasty. J Arthroplasty. 2016;31:603–608. doi:10.1016/j.arth.2015.09.050
31. Goltz DE, Sicat CS, Levin JM, et al. A validated pre-operative risk prediction tool for extended inpatient length of stay following primary total hip or knee arthroplasty. J Arthroplasty. 2023;38:785–793. doi:10.1016/j.arth.2022.11.006
32. Bohl DD, Ondeck NT, Darrith B, Hannon CP, Fillingham YA, Della Valle CJ. Impact of operative time on adverse events following primary total joint arthroplasty. J Arthroplasty. 2018;33:2256–2262.e2254. doi:10.1016/j.arth.2018.02.037
33. Sodhi N, Anis HK, Gold PA, et al. Operative times can predict and are correlated with lengths-of-stay in primary total knee arthroplasty: a nationwide database study. J Arthroplasty. 2019;34:1328–1332. doi:10.1016/j.arth.2019.03.024
34. Hodgeson S, O’Brien S, Simkin J, et al. Differences in synovial fibrosis relative to range of motion in knee osteoarthritis patients. J Orthopaedic Res. 2022;40:584–594. doi:10.1002/jor.25061
35. Liao CD, Tsauo JY, Huang SW, Chen HC, Chiu YS, Liou TH. Preoperative range of motion and applications of continuous passive motion predict outcomes after knee arthroplasty in patients with arthritis. Knee Surg Sports Traumatol Arthroscopy. 2019;27:1259–1269. doi:10.1007/s00167-018-5257-z
36. Winemaker M, Rahman WA, Petruccelli D, de Beer J. Preoperative knee stiffness and total knee arthroplasty outcomes. J Arthroplasty. 2012;27:1437–1441. doi:10.1016/j.arth.2011.12.015
37. Matassi F, Duerinckx J, Vandenneucker H, Bellemans J. Range of motion after total knee arthroplasty: the effect of a preoperative home exercise program. Knee Surg Sports Traumatol Arthroscopy. 2014;22:703–709. doi:10.1007/s00167-012-2349-z
38. van den Belt L, van Essen P, Heesterbeek PJ, Defoort KC. Predictive factors of length of hospital stay after primary total knee arthroplasty. Knee Surg Sports Traumatol Arthroscopy. 2015;23:1856–1862. doi:10.1007/s00167-014-3313-x
39. Khanna V, Gurava Reddy AV, Daultani D, et al. When can I go home after my knee replacement? Factors affecting the duration of in-hospital stay after knee replacement. Euro J Orthopaedic Surg Traumatol. 2019;29:1719–1728. doi:10.1007/s00590-019-02485-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.