Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
A Nomogram Combining Platelet to Lymphocyte Ratio (PLR) and Systemic Inflammatory Response Index (SIRI) to Predict Patients with H. pylori -Positive Gastric Dysplasia
Authors Fang JW, She Q ![]() , Xia JL
, Xia JL ![]() , Chen YY, Liu ZQ, Yu Y, Fu XY, Jiang X, Li YY, Zhang M, Ding YB
, Chen YY, Liu ZQ, Yu Y, Fu XY, Jiang X, Li YY, Zhang M, Ding YB
Received 4 May 2025
Accepted for publication 4 October 2025
Published 18 October 2025 Volume 2025:18 Pages 6795—6809
DOI https://doi.org/10.2147/JMDH.S538329
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Jing-Wen Fang,* Qiang She,* Jian-Lei Xia, Yuan-Yuan Chen, Zhuo-Qi Liu, Yue Yu, Xin-Yu Fu, Xin Jiang, Yao-Yao Li, Min Zhang, Yan-Bing Ding
Department of Gastroenterology, The Affiliated Hospital of Yangzhou University, Yangzhou, Jiangsu Province, 225000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan-Bing Ding; Min Zhang, Department of Gastroenterology, The Affiliated Hospital of Yangzhou University, Yangzhou, Jiangsu Province, 225000, People’s Republic of China, Email [email protected]; [email protected]
Objective: Patients with Helicobacter pylori-positive gastric dysplasia are at a higher risk of progressing to gastric cancer (GC). Systemic inflammatory markers have been identified as predictors of poor prognosis in patients with GC. However, their role in gastric dysplasia remains elusive. The aim of this study is to evaluate the utility of systemic inflammatory markers as predictors in patients with H. pylori-positive gastric dysplasia.
Methods: This study included a total of 664 normal individuals and patients diagnosed with chronic gastritis from the Yangzhou screening cohort, as well as 135 patients with gastric dysplasia from the Affiliated Hospital of Yangzhou University, spanning the period from January 2017 to May 2024. The participants were randomly assigned to either a training group or a validation group in a ratio of 7:3. SPSS software was utilized to determine the optimal critical values for PLR and SIRI. Subsequently, univariate and multivariate regression analyses were conducted to assess the diagnostic utility of PLR and SIRI. A nomogram was developed to estimate the risk associated with gastric dysplasia. To evaluate model performance, receiver operating characteristic curves (ROC), calibration curves, decision curve analysis (DCA) and the Clinical Impact Curve (CIC) were generated.
Results: Eight independent risk factors, including the PLR and SIRI, were identified with a significance level of p < 0.1. The area under the ROC curve (AUC) was found to be 0.859 for the training set (95% CI: 0.808– 0.891) and 0.821 for the validation set (95% CI: 0.735– 0.906). The results from ROC analysis calibration curves, DCA and CIC demonstrated that the nomogram possessed significant predictive value.
Conclusion: PLR and SIRI are independent variables that influence the diagnosis of patients with gastric dysplasia. The nomogram model created using PLR and SIRI demonstrates a high predictive value for diagnosing individuals with gastric dysplasia.
Keywords: gastric dysplasia, systemic inflammation markers, nomogram, PLR, SIRI
Background
Gastric cancer ranks as the fifth most prevalent type of cancer and is the fifth leading cause of cancer-related mortality on a global scale.1 China is characterized by a notably high incidence of gastric cancer, with new cases and related deaths constituting 44.1% and 49.9% of the global totals, respectively. The age-standardized five-year survival rate stands at a mere 27.4%.2 Globally, Helicobacter pylori infection accounts for nearly 90% of the etiological factors of distal gastric cancer. Other well - validated risk factors include excessive body fat, smoking, and dietary habits featuring high salt intake and consumption of processed meats.3 In China, the primary risk factors for gastric cancer encompass H. pylori infection, family history, and an unhealthy lifestyle.4 Concurrently, patients diagnosed with gastric cancer often present with subtle early symptoms and exhibit limited treatment efficacy, resulting in an overall unfavorable prognosis.5 Implementing selective screening programs for high - risk populations in regions with a high incidence of gastric cancer can enhance the detection rate of gastric cancer.2 Additionally, screening young adults for H. pylori infection and treating individuals with positive test results has been demonstrated to be effective in preventing the incidence of gastric cancer.6 As the world’s largest developing country, China still shows a significant urban-rural disparity in the field of healthcare. Due to the limited accessibility of medical resources and the lower quality of medical services provided in rural areas, there are regional differences in cancer survival rates between urban and rural areas in China.7 Initiating treatment at an early stage, comprehensively understanding gastric cancer, and advancing relevant technologies may contribute to the decline in the mortality rate of gastric cancer.8
However, gastric carcinogenesis represents a multistep process that typically involves progression from normal mucosa through the stages of chronic gastritis, mucosal atrophy, and intestinal metaplasia, ultimately leading to dysplasia and carcinoma.9 This sequence of events may extend over several years and has been designated as Correa’s cascade of multistep gastric carcinogenesis.10 Among these conditions, gastric dysplasia, commonly referred to as intraepithelial neoplasia, represents a precursor lesion and constitutes the final stage preceding the development of gastric cancer.11 The presence of irregular blood vessels and glands, or the absence of glands accompanied by the disappearance of the intact architecture of the mucosa and blood vessels, heralds neoplastic alterations in the mucosa.12 Therefore, researchers have continuously sought new, simple, economical, and accurate diagnostic evaluation indices to improve the diagnosis of gastric dysplasia and prevent the onset of gastric cancer.
Among a multitude of risk factors, H. pylori infection represents the most significant known risk factor for gastric cancer.13 In Western countries, patients infected with CagA (cag pathogenicity island-encoded cytotoxin associated gene A) -positive H. pylori strains, along with those carrying the IL-1B promoter and the corresponding IL-1 receptor antagonist gene polymorphisms, exhibit a relatively higher risk of gastric cancer. In East Asian countries like China, preventive measures for gastric cancer should be focused on relatively younger populations. This is because the histological alterations induced by bacterial infection, such as atrophy and intestinal metaplasia, remain reversible at this stage.14 Eradicating Helicobacter pylori following endoscopic resection of gastric dysplasia may significantly diminish the risk of developing gastric cancer and metachronous gastric neoplasms.15 Novel formulation strategies, including extended-release gastro retentive drug delivery systems (GRDDS) and nanoformulations, hold promise in surmounting the challenge of poor patient compliance during long-term treatment resulting from polypharmacy.16 In the past decade, numerous prognostic predictive models have been developed for gastric cancer, which assist in predicting clinical outcomes and selecting therapeutic options for GC patients. However, there are limited models specifically designed for patients with H. pylori-positive gastric dysplasia. H. pylori infection is concomitant with notable physiological alterations in the stomach. It predominantly elicits local inflammatory reactions in the stomach.17 Given the significant clinical and molecular differences between H. pylori-positive and H. pylori-negative patients, it is essential to construct reliable signatures that are specific to different patient cohorts. Therefore, the selection of H. pylori-positive patients is necessary to eliminate the influence of H. pylori on the results.
Inflammation plays a pivotal role in tumor progression. Numerous cancers originate from areas characterized by infection, chronic irritation, and inflammation.18 H. pylori infection can trigger chronic inflammation in the body. Persistent inflammation may contribute to the progression of gastric dysplasia to gastric cancer. The inflammatory response of the body can be reflected by inflammatory markers in the blood.19 In established cancers, accumulating evidence suggests that local immune responses and systemic inflammation contribute to tumor progression and the survival of cancer patients.20 Chronic inflammation serves as the primary pathogenic factor underlying the development of gastric cancer. H. pylori infection is intricately associated with inflammation-mediated gastric carcinogenesis. The virulence factors of this bacterium, such as CagA and VacA (vacuolating cytotoxin A), appear to influence both the pathogenicity of the bacterium and the risk of gastric cancer progression.21 Various systemic inflammation markers derived from peripheral blood indicators, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammatory index (SII), pan-immune-inflammation value (PIV), and systemic inflammatory response index (SIRI), have been identified as potential predictors for multiple malignant tumors.22,23 Some of these systemic inflammatory markers may serve as diagnostic indicators for gastric cancer (GC) or even early-stage GC.24,25 NLR, PLR and SII may exhibit particular relevance to the diagnosis and prognosis of gastric cancer patients. As inflammatory markers, NLR, PLR and SII can be utilized as effective biomarkers for diagnosis and prognostic assessment in gastric cancer patients.26–28
Gastric dysplasia is a precancerous lesion of gastric cancer, and it is of great significance for the early detection and treatment of gastric cancer. Early detection, diagnosis, and treatment of high-risk populations can not only increase the survival rate of patients but also improve their quality of life and alleviate the economic burden on society. In contrast to large-scale gastroscopic screening, using systemic inflammatory markers is more convenient and can be more readily implemented. This approach can reduce the physical discomfort associated with invasive endoscopic examinations. However, gastric dysplasia exhibits an ambiguous relationship with systemic inflammatory markers. While the correlation between gastric cancer and systemic inflammatory markers has been established, their utility in the diagnosis of gastric dysplasia necessitates further investigation. Consequently, this study aims to examine the association between systemic inflammatory markers and gastric dysplasia, as well as to develop a practical prediction model for diagnosing this condition. Subsequently, we will assess its reliability and clinical effectiveness.
Methods
Patients
From January 2017 to May 2024, 2992 normal individuals or chronic gastritis patients from the Yangzhou screening cohort and 161 patients with gastric dysplasia from The Affiliated Hospital of Yangzhou University were enrolled in this study.
The following are the eligibility criteria for patients participating in this study: (1) pathological confirmation of gastric dysplasia or non-atrophic gastritis (clinically regarded as approximately normal), along with the presence of normal gastric mucosa; (2) absence of acute or chronic inflammation; (3) presence of no other serious comorbidities and a well-functioning organism; (4) no medical contraindications that would significantly impact anesthesia and surgical procedures; (5) availability of complete medical history information; (6) inclusion of H. pylori-positive patients.
Patients were excluded if they met any of the following criteria: (1) those with incomplete medical history data or who were lost to follow-up; (2) individuals diagnosed with diabetes; (3) patients experiencing gastric ulcers; (4) patients having hematological diseases or other tumors; (5) individuals suffering from severe uncontrolled recurrent infections or other serious comorbidities that are not well-managed; (6) patients requiring immunosuppressive therapy or hormone therapy due to organ transplantation; (7) H. pylori-negative patients.
The flowchart outlining the screening process for eligible patients is depicted in Figure 1. A total of 135 patients diagnosed with gastric dysplasia and 664 normal individuals were screened, resulting in an overall sample size of 799 patients. Among these participants, 560 patients were allocated to the training cohort, while the remaining 239 patients were designated for the validation cohort.
 |
Figure 1 Flowchart of patient selection process in the study. |
Data Collection and Processing
The collection of clinical parameters included basic demographic information such as age, sex, history of hypertension, coronary heart disease, and lifestyle factors such as alcohol consumption and smoking status. Hematological parameters were also assessed, which comprised white blood cell count, red blood cell count, neutrophil count, lymphocyte count, monocyte count, eosinophil count, basophil count, platelet count, and hemoglobin levels. All laboratory blood test data were obtained from tests conducted on patients prior to the initiation of any relevant treatment. Additionally, seven composite inflammatory markers were derived from hematological indexes. The NLR was calculated using the ratio of Neutrophil (Neu) counts to Lymphocyte (Lym) counts. The PLR was determined by dividing Platelet (Plt) counts by Lym counts. The Lymphocyte-to-Monocyte Ratio (LMR) was computed as the ratio of Lym counts to Monocyte (Mono) counts. The Neutrophil-to-Platelet Ratio (NPR) was derived by dividing Neu counts by Plt counts. The SII index was established through the formula: Plt counts multiplied by Neu counts divided by Lym counts. Similarly, SIRI was calculated as Mono counts multiplied by Neu counts divided by Lym counts. Finally, PIV was computed using the equation: Plt counts multiplied by Neu counts multiplied by Mono counts divided by Lym counts. Receiver Operating Characteristic (ROC) analysis was employed to ascertain optimal cutoff values for composite inflammatory markers through the computation of maximal Youden index scores.
Development and Validation of the Nomogram
Univariate and multivariate logistic regression analyses were employed to identify independent predictive factors from the training cohort. Following this, a nomogram was developed based on the independent variables determined through multivariate analysis. The predictive performance of the nomogram was evaluated using the area under the receiver operating characteristic curves (AUC) along with calibration curves. Additionally, decision curve analysis (DCA) was conducted to assess the clinical utility of the nomogram by quantifying its net benefits. The Clinical Impact Curve (CIC) was plotted to evaluate the clinical practicality and applicability net benefits of the model with the optimal diagnostic value.29
Statistical Analysis
The statistical analysis was conducted using SPSS software (IBM SPSS Statistics 25.0) and R Studio (version 4.3.1). Categorical variables were assessed with the χ2 test or Fisher’s exact test, while continuous variables were analyzed using the Student’s t-test. A p-value of less than 0.05 was considered statistically significant. Univariate logistic regression analysis was employed to examine clinical variables, and those included in the multivariable logistic regression model were selected based on univariate results as well as professional expertise. In the univariate analysis, we set the p-value to be <0.05. Appropriately increasing the p-value threshold can include more risk factors that are clinically relevant in the multivariate analysis, thereby preventing the omission of crucial influencing factors. Therefore, in the multivariate analysis, we set the p-value to be <0.1. An odds ratio (OR) value greater than 1 indicates a risk factor, while an OR value less than 1 represents a protective factor. Statistically significant indicators were refined through stepwise backward regression analysis. The “rms” package was utilized for nomogram visualization and calibration curve plotting. Receiver Operating Characteristic (ROC) curves, which assess the discriminatory power of the nomogram and identify optimal cut-off values, were generated using the pROC package. Additionally, decision curve analysis was performed utilizing the “rmda” package.
Results
Baseline Characteristics
A total of 799 patients were included in the study, comprising 365 males (46%) and 434 females (54%). The median age at screening was 57 years, with an age range of 51 to 65 years. Participants were randomly assigned to two cohorts by R software in a ratio of 7:3, there was a training group with 560 patients and a validation group with 239 patients. The differences in age between the two groups were statistically significant (p<0.05). Aside from age, no other variables exhibited statistically significant differences between the training and validation cohorts, indicating that both sets had comparable baseline characteristics as presented in Table 1.
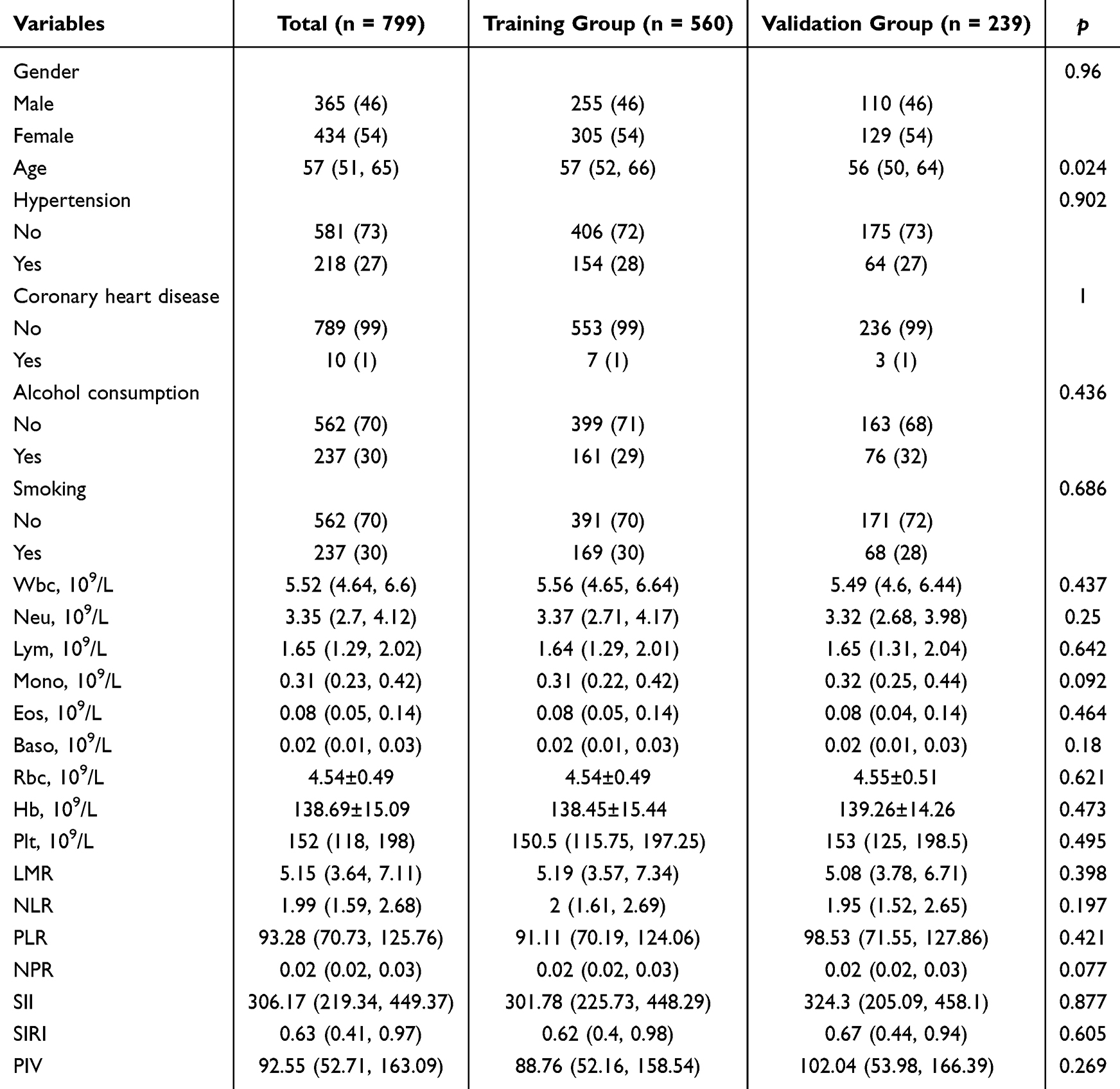 |
Table 1 Baseline Clinical Characteristics of Patients in the Training Cohort and Validation Cohort |
ROC Curve of Peripheral Blood Parameters NLR, PLR, SII, SIRI, PIV
ROC was employed to evaluate systemic inflammation markers from peripheral blood indicators for predicting gastric dysplasia, including NLR, PLR, SII, SIRI, and PIV. The optimal cut-off point, sensitivity, and specificity were established based on the maximum Youden index. The area under the ROC curve (AUC) for PLR was 0.695, with an optimal cut-off value of 108.94 corresponding to the peak Youden index. In contrast, the AUC for SIRI was 0.605, with an optimal cut-off value of 0.38988 associated with its maximum Youden index. Our findings revealed that the AUC value for PLR significantly surpassed those of the other indices, indicating superior predictive efficacy of PLR compared to its counterparts as illustrated in Figure 2.
 |
Figure 2 Receiver Operating Characteristic (ROC) curves for neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammatory index (SII), systemic inflammatory response index (SIRI), and pan-immune-inflammation value (PIV). |
Predictive Factors Selection and Construction of Nomogram
Univariate analysis of the training set presented in Table 2 revealed that several variables were significantly associated with gastric dysplasia (p<0.05). These variables included gender, age, hypertension, drinking history, Lym, Mono, Baso, Plt, PLR, SIRI, among others. Multivariate logistic regression analysis was utilized to evaluate variables identified as significant in the univariate logistic analysis. The findings indicated that gender[odds ratio (OR) = 1.173, p<0.001, 95% CI: 0.097–0.308], age (OR = 1.030, p=0.060, 95% CI: 0.999–1.061), hypertension (OR = 2.040, p=0.012, 95% CI: 1.168–3.563), drinking history (OR = 0.176, p<0.001, 95% CI: 0.088–0.354), Baso(OR = 2.166, p=0.007, 95% CI: 1.241–3.780), Plt (OR = 1.776, p=0.073, 95% CI: 0.947–3.330), PLR (OR = 2.459, p=0.004, 95% CI: 1.339–4.515), and SIRI (OR = 4.397, p=0.001, 95% CI: 1.766–10.948) constituted independent risk factors for gastric dysplasia. A nomogram model was developed based on predictive variables isolated through multivariate logistic regression analysis as illustrated in Figure 3. Using the points indicated above the nomogram, a score for each risk factor can be determined. After obtaining the individual score for each factor, sum these scores together; the total score represents the probability of that patient developing gastric dysplasia. The higher the total score, the nearer the diagnostic rate approaches 100%, and the greater the accuracy of predicting gastric dysplasia.
 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Patients |
 |
Figure 3 Nomogram for predicting gastric dysplasia risk in patients. |
Validation and Clinical Use of Nomogram
The AUC values of our nomogram for predicting distant metastasis were 0.859 (95% CI: 0.808–0.891) in the training set and 0.821 (95% CI: 0.735–0.906) in the validation set. These results indicate that the predictions made by this nomogram correspond well with actual observations, as illustrated in Figure 4. In addition, AUC values for both the training set and the validation set ranged from 0.7 to 0.9, indicating that the prediction models exhibited good discriminatory ability in both datasets. For predicting the risk of internal gastric dysplasia using Boosted cross-validation, the nomogram was executed 1000 times, yielding mean error rates of 0.019 and 0.027 for the two models respectively, as illustrated in Figure 5. This demonstrates that the nomogram possesses superior stability. DCA indicated that our nomogram provided a positive net benefit when compared to the all-or-none scheme, with threshold probabilities ranging from 10% to 95% in both the training and testing sets, as illustrated in Figure 6. The CIC reveals that within the most favorable threshold probability range, the expected number of high - risk patients consistently exceeded the actual number of patients, accompanied by an acceptable cost - benefit ratio. The CIC visually demonstrated that the nomogram conferred a high clinical net benefit and verified the clinical value of the predictive model, as illustrated in Figure 7.
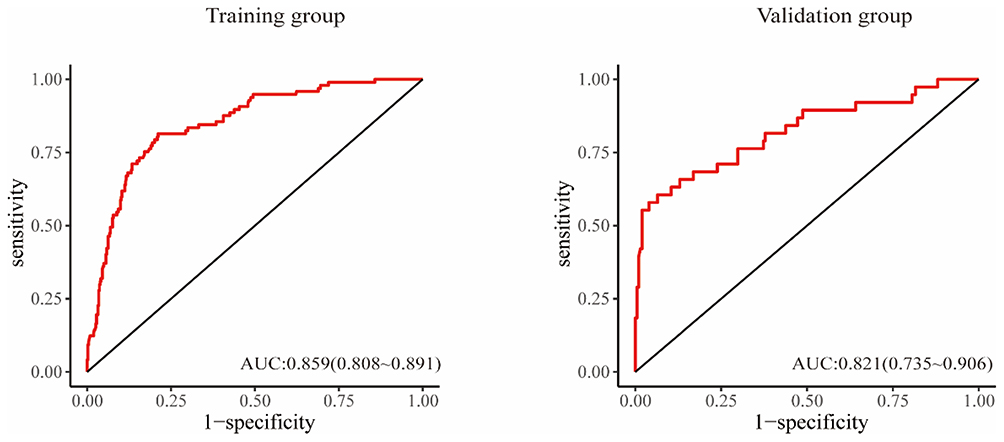 |
Figure 4 Receiver Operating Characteristic (ROC) curve of the nomogram for the prediction of gastric dysplasia patients in the training cohort and validation cohort. |
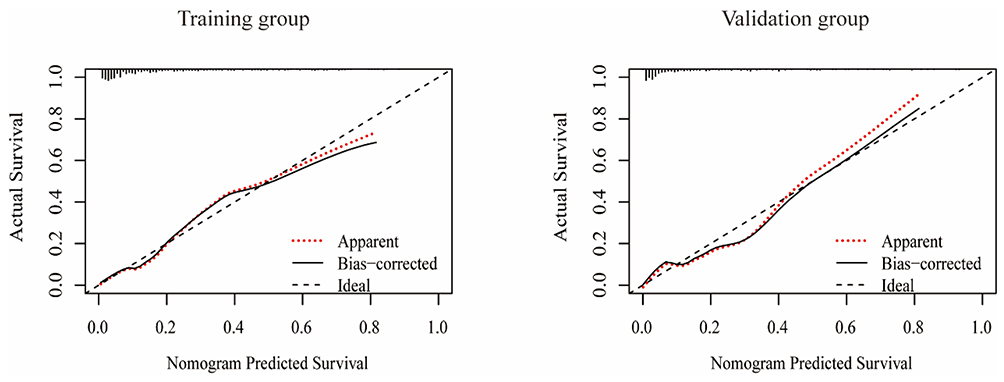 |
Figure 5 The calibration curve of nomogram for the prediction of gastric dysplasia patients in the training cohort and validation cohort. |
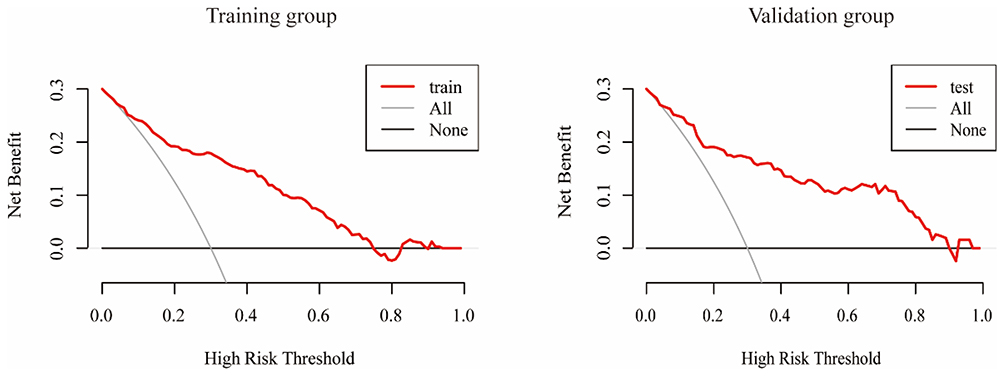 |
Figure 6 Decision curve analysis (DCA) of the nomogram for the prediction of gastric dysplasia patients in the training cohort and validation cohort. |
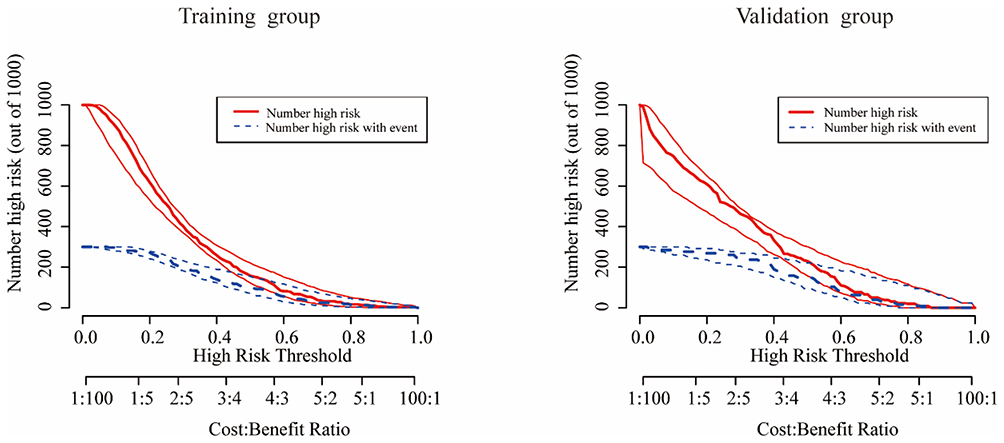 |
Figure 7 Clinical impact curve (CIC) of the nomogram for the prediction of gastric dysplasia patients in the training cohort and validation cohort. |
Discussion
The progression from normal gastric mucosal cells to cancerous cells is not a gradual process; occurring through an intermediate stage referred to as gastric precancerous lesions.13 Gastric dysplasia signifies the terminal phase in the evolution from gastric precancerous lesions to gastric cancer. Traditional tumor markers, including carcinoembryonic antigen (CEA), carbohydrate antigen 19–9 (CA199),28 the ratio of serum pepsinogen I to II (PG I/II), Gastrin-17, and H. pylori antibodies, hold the potential to identify patients with gastric dysplasia. These biomarkers can be detected via serological assays. However, endoscopy is an essential technique for identifying early-stage gastric cancer and related precancerous lesions. In regions with high prevalence of gastric cancer, it has prompted the establishment of population screening programs.25 It is widely acknowledged that the combination of image-enhanced endoscopy and biopsy sampling for histopathological examination represents the most effective strategy to enhance early detection rates.30 Biopsy serves as the gold standard for the diagnosis of gastric dysplasia. Optimizing biopsy specimens via image-enhanced endoscopy can enhance the accuracy of diagnosing gastric dysplasia. Nevertheless, pathological biopsy is inherently invasive to the human body and necessitates a certain level of proficiency on the part of the endoscopists. As such, it is not amenable to large-scale screening initiatives.
It was difficult to execute nationally due to the varying proficiency of pathologists and economic development. There is an urgent need for accessible and sensitive biomarkers to facilitate the detection of patients with gastric dysplasia. Accurate prediction of gastric dysplasia prior to treatment is pivotal for preventing progression to gastric cancer and devising optimal treatment regimens.
Inflammation is recognized as a fundamental characteristic of cancer, significantly influencing the formation and progression of malignancies.18 Tumors instigate an inflammatory response, referred to as tumor-associated inflammation, in reaction to an insult, specifically malignant cells. This inflammatory response serves a purpose akin to that of wound healing: its objective is to eradicate the harmful stimulus.31 Inflammation is typically characterized by alterations in key hematological indicators, including neutrophil count, lymphocyte percentage, and platelet count, as observed in routine blood tests. Platelets play a crucial role in enhancing tumor-related coagulation and provide protection to tumor cells from immune attacks by aggregating around them. Concurrently, platelets secrete various growth factors and chemokines that inhibit the immune environment, promote tumor angiogenesis, and contribute to tumor proliferation and metastasis.32 Despite constituting a minimal fraction of circulating blood leukocytes, basophils serve as potent immune effector cells. Basophils play a crucial role in IgE-mediated reactions by infiltrating inflammatory lesions and releasing pro-inflammatory mediators along with regulatory cytokines. These factors are central to the pathogenesis of allergic diseases.33 Increases and decreases in peripheral blood basophil levels have been associated with the progression of specific human solid tumors.34 In the context of gastric cancers, evidence has been reported indicating a deleterious role of circulating or tissue-infiltrating basophils.35 In addition to their recognized role in cancer, our research indicates that platelets and basophils also serve as independent risk factors for gastric dysplasia. Lymphocytes represent essential constituents of the anti-tumor immune response, with T cells identified as pivotal mediators of anti-tumor immunity.36 Antibodies, exclusively produced by B cells, play a crucial role in activating the complement cascade and enhancing natural killer (NK) cell-mediated tumor cytotoxicity through antibody-dependent cell-mediated cytotoxicity.37 Among them, PLR refers to the ratio of platelets to lymphocytes. In the extensive prospective UK Biobank cohort study exploring the relationship between systemic inflammation and cancer risk, the researchers identified positive associations for PLR across seven of the seventeen cancer sites examined.38 An elevated PLR signifies an activated inflammatory response, along with a stimulating transcription factor and pro-inflammatory cytokines. These proteins are essential in tumor cell proliferation, survival, migration, and invasion. They facilitate epithelial–mesenchymal transition (EMT), as well as angiogenesis, metastasis, and the response to chemotherapy.39 It was found that the systemic inflammatory marker PLR is more valuable for diagnosing GC compared to traditional tumor markers such as CEA and CA19-9.29 In both univariate and multivariate analyses, the PLR was identified as an independent risk factor for gastric dysplasia and may serve as a reliable predictive marker for this condition. Furthermore, neutrophils, as components of the innate immune system, are traditionally regarded as key indicators for assessing the inflammatory status of the immune response. Neutrophils recruited to inflammatory sites predominantly facilitate the initiation of cancer through mechanisms such as augmenting DNA damage, promoting angiogenesis, and inducing immunosuppression.40 In cancer, which has been characterized as “wounds that do not heal”, dysfunctional monocyte-derived macrophages play a crucial detrimental role overall.41 Monocytes serve as a crucial link between innate and adaptive immune responses. They can influence the tumor microenvironment through various mechanisms that promote immune tolerance, facilitate angiogenesis, and enhance the dissemination of tumor cells. Monocytes modulate the transcriptional programs of derived cells via crucial signaling pathways, namely the STAT3, NF-κB, and PI3Kγ pathways. This modulation facilitates the accumulation of pro-tumor cells that possess properties related to angiogenesis, trophic support, and immunosuppression.42 Circulating monocytes have the capacity to infiltrate solid tissues and differentiate into macrophages, thereby participating in both immune defense mechanisms and tissue repair processes. In contrast, lymphocytes play a crucial role in regulating the immune system through cytokine secretion and cytolytic activity. Consequently, SIRI, which is derived from the counts of peripheral neutrophils, monocytes, and lymphocytes, may serve as a robust and reliable marker for indicating inflammatory conditions. SIRI has demonstrated effectiveness in comprehensively reflecting both the inflammatory state and overall status of the immune system within the body as an integrative index of inflammation.43 As systemic inflammation markers, PLR and SIRI not only exhibit significant diagnostic and prognostic value in both general and gastric cancers, but also play a substantial role in predicting gastric dysplasia. In summary, the association between gastric cancer and systemic inflammatory markers has been well-established. However, there is no relevant literature yet that studies the relationship between systemic inflammatory markers and gastric dysplasia. The diagnostic value of these markers for gastric dysplasia remains to be fully elucidated. This study aims to investigate the association between systemic inflammatory markers and gastric dysplasia, develop a practical diagnostic prediction model for gastric dysplasia, and systematically assess the reliability and clinical utility of this model.
Given that H. pylori is the most significant identified risk factor for gastric cancer,11 we enrolled H pylori-positive patients. In this model, both normal individuals and patients with gastric dysplasia are infected with H. pylori, thus having no significant impact on the efficacy of the diagnostic prediction model. Correa initially put forward a disease model, which elucidated the malignant transformation process from H. pylori infection to gastric cancer. This process encompasses the development of chronic atrophic gastritis under persistent inflammatory stimuli. Subsequently, intestinal metaplasia may gradually progress to precancerous lesions, such as gastric dysplasia, ultimately resulting in gastric adenocarcinoma.9 This study, to the best of our knowledge, represents the first effort to develop a novel nomogram that integrates peripheral blood markers and clinical factors for the prediction of gastric dysplasia. The nomogram serves as a visual tool designed to estimate the probability of event occurrence based on statistical models incorporating multiple variables.44 The capability of clinical nomogram prediction models to enhance the accuracy of individual disease risk assessment, taking into consideration various patient conditions, may facilitate informed clinical decision-making.45
The multivariate analysis revealed that gender, age, hypertension, drinking history, Baso, PLT, PLR, and SIRI are each independent predictors of diagnosis in patients with gastric dysplasia. Gender is significantly associated with each stage of the Correa cascade. Moreover, with each cascade step, the influence of gender shows a monotonically increasing trend.46 In comparison to men, women serve as protective factors for gastric dysplasia. Previous studies have shown that both males and H. pylori are major risk factors for the development of gastric cancer.47 Similarly, in the predictive model, being male is a risk factor for patients with H. pylori -positive gastric dysplasia. Interestingly, alcohol consumption appears to act as a protective factor for gastric dysplasia, which contradicts prevailing assumptions. Alcohol exerts both stimulatory and detrimental effects on gastric mucosal cells.48 Additionally, it may exhibit cytotoxicity towards atypically hyperplastic gastric mucosal cells. While alcohol consumption does not protect the gastric mucosa, it may contribute to the inhibition of atypical hyperplasia. Although the study establishes an association between heavy alcohol use and GC in the United States,49 there is still no clear research on exactly what impact moderate drinking has on the progression of gastric cancer.50 In one meta-analysis, A J-shaped relationship was observed between alcohol consumption and all cancer mortality including gastric cancer, with an inverse association at light exposure levels (≤12.5g/day).51 Both genders exhibited similar negative effects when exposed to low levels of alcohol, consistent with previous findings across all types of cancer.52 The criteria for light alcohol consumption in women are more stringent compared to those in men. To minimize the risk of mortality, women should maintain a lower daily alcohol intake.51 Under conditions of moderate to heavy alcohol consumption, women exhibit a higher risk of all-cause mortality compared to men.52 This may be attributed to an elevated risk of cancer. During the data collection process, we did not quantify the drinking behavior. Given that both the frequency and dosage of alcohol consumption can significantly influence the final outcomes, it would be inappropriate to disregard the drinking history. Therefore, further large-scale cohort studies are warranted to precisely assess the impact of alcohol on gastric dysplasia. Traditional tumor markers, including carcinoembryonic antigen (CEA), are generally elevated only in the advanced stages of cancer.28 In contrast, inflammatory indices have emerged as novel markers and are recognized as independent risk factors for gastric dysplasia. Our findings indicate that an increase in the PLR and SIRI can be observed at the stage of gastric dysplasia, a precancerous lesion associated with gastric cancer.
In this study, we developed a predictive nomogram model incorporating the PLR and SIRI. This nomogram serves as an accurate scoring system, as evidenced by both decision curve analysis and calibration curve supporting its clinical applicability. It is important to note that all the information necessary for constructing this nomogram can be acquired during the screening process, particularly in instances where endoscopic procedures are restricted. When the total score of patients exceeds 550, the probability that they suffer from gastric dysplasia increases to nearly 95%. In such cases, it may be more appropriate for gastroenterologists to assess whether these patients require further endoscopic evaluation.
However, this study has several limitations. Firstly, it is a single-center retrospective analysis with a limited number of cases, which may introduce selection bias. The diagnostic value of the PLR and SIRI requires validation through multi-center prospective studies. Secondly, certain indicators that could be pertinent to the study were not included, such as dietary habits and Body Mass Index (BMI). The specific dietary patterns were associated with the risk of gastric cancer.53 Obesity (BMI 25 kg/m2 or greater but less than 30 kg/m2) was associated with increased risk of early gastric cancer.54 Incorporating indicators associated with gastric dysplasia, such as dietary patterns and BMI, can elevate AUC of the model, optimize calibration, and strengthen its clinical utility. The primary reason for this omission is that these indicators were not routinely assessed and recorded during hospitalization, leading to their absence in the dataset. The influence of these factors warrants further investigation. Thirdly, while PLR and SIRI were identified as independent predictors of gastric dysplasia and demonstrated superior performance compared to other inflammatory markers, their sensitivity and specificity remain suboptimal. Therefore, further prospective studies are necessary to establish an appropriate cutoff value. In addition, due to a lack of data, we performed only internal validation for our nomogram mo external validation including a larger cohort of patients from several medical centers is still pending.
Conclusions
This study represents the first comprehensive examination of the relationship among gender, age, medical history, smoking, drinking habits and inflammatory indicators, particularly PLR and SIRI, in patients with gastric dysplasia. Additionally, these factors were found to be independent risk factors for gastric dysplasia in the multivariate analysis. Additionally, it establishes a scoring system aimed at guiding clinical practice, which is straightforward to compute and readily accessible. Compared with traditional tumor marker detection and gastroscopy screening methods, the system’s scoring model not only effectively predicts precancerous gastric lesions but also demonstrates significant advantages in practical application and widespread promotion.
Ethics Declarations
The retrospective design of the study received approval from the Ethics Committee of The Affiliated Hospital of Yangzhou University. The ethic number was 2025-YKL02-07. This research has been performed in accordance with the Declaration of Helsinki.
Consent to Participate
All human participants provided informed consent prior to their inclusion in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82404358, No. 82273084); Key Project in the Health and Wellness Category of the Yangzhou Municipal Basic Research Program (Joint Special Project), Grant Number: 2024-1-05.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Gao K, Jun W. National trend of gastric cancer mortality in China (2003–2015): a population-based study. Cancer Commun (Lond). 2019;39(1):24. doi:10.1186/s40880-019-0372-x
3. Thrift AP, Wenker TN, El-Serag HB. Global burden of gastric cancer: epidemiological trends, risk factors, screening and prevention. Nat Rev Clin Oncol. 2023;20(5):338–349. doi:10.1038/s41571-023-00747-0
4. Zong L, Abe M, Seto Y, et al. The challenge of screening for early gastric cancer in China. Lancet. 2016;388(10060):2606. doi:10.1016/S0140-6736(16)32226-7
5. Gullo I, Grillo F, Mastracci L, et al. Precancerous lesions of the stomach, gastric cancer and hereditary gastric cancer syndromes. Pathologica. 2020;112(3):166–185. doi:10.32074/1591-951X-166
6. Yeh JM, Kuntz KM, Ezzati M, et al. Exploring the cost-effectiveness of Helicobacter pylori screening to prevent gastric cancer in China in anticipation of clinical trial results. Int J Cancer. 2009;124(1):157–166. doi:10.1002/ijc.23864
7. Zeng H, Zheng R, Guo Y, et al. Cancer survival in C hina, 2003–2005: a population-based study. Int J Cancer. 2015;136(8):1921–1930. doi:10.1002/ijc.29227
8. Zou WB, Yang F, Li ZS. How to improve the diagnosis rate of early gastric cancer in China. J ZheJiang Univ Med Sci. 2015;44:9–14.
9. Correa P. Human gastric carcinogenesis: a multistep and multifactorial process--first American cancer society award lecture on cancer epidemiology and prevention. Cancer Res. 1992;52(24):6735–6740.
10. Xiao S, Lu H, Xue Y, et al. Long-term outcome of gastric mild-moderate dysplasia: a real-world clinical experience. Clin Gastroenterol Hepatol. 2022;20(6):1259–1268. doi:10.1016/j.cgh.2021.10.032
11. Choi IJ, Kook MC, Kim YI, et al. Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer. N Engl J Med. 2018;378(12):1085–1095. doi:10.1056/NEJMoa1708423
12. Pimentel-Nunes P, Libânio D, Marcos-Pinto R, et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): european Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy. 2019;51(4):365–388. doi:10.1055/a-0859-1883
13. Wang H, Wu R, Xie D, et al. A combined phytochemistry and network pharmacology approach to reveal the effective substances and mechanisms of Wei-Fu-Chun tablet in the treatment of precancerous lesions of gastric cancer. Front Pharmacol. 2020;11:558471. doi:10.3389/fphar.2020.558471
14. Prinz C, Schwendy S, Voland P. H pylori and gastric cancer: shifting the global burden. World J Gastroenterol. 2006;12(34):5458–5464. doi:10.3748/wjg.v12.i34.5458
15. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
16. Gupta A, Shetty S, Mutalik S, et al. Treatment of H. pylori infection and gastric ulcer: need for novel Pharmaceutical formulation. Heliyon. 2023;9(10):e20406. doi:10.1016/j.heliyon.2023.e20406
17. Peek Jr RM, Blaser MJ. Helicobacter pylori and gastrointestinal tract adenocarcinomas. Nature Rev Cancer. 2002;2:28–37.
18. Diakos CI, Charles KA, McMillan DC, et al. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
19. Valenzuela MA, Canales J, Corvalán AH, et al. Helicobacter pylori-induced inflammation and epigenetic changes during gastric carcinogenesis. World J Gastroenterol. 2015;21(45):12742–12756. doi:10.3748/wjg.v21.i45.12742
20. Zhang J, Zhang L, Duan S, et al. Single and combined use of the platelet-lymphocyte ratio, neutrophil-lymphocyte ratio, and systemic immune inflammation index in gastric cancer diagnosis. Front. Oncol. 2023;13:1143154. doi:10.3389/fonc.2023.1143154
21. Ferreira RM, Machado JC, Figueiredo C. Clinical relevance of helicobacter pylori vacA and cagA genotypes in gastric carcinoma. Best Pract Res Clin Gastroenterol. 2014;28(6):1003–1015. doi:10.1016/j.bpg.2014.09.004
22. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
23. Zhang X, Zhao W, Yu Y, et al. Clinicopathological and prognostic significance of platelet-lymphocyte ratio (PLR) in gastric cancer: an updated meta-analysis. World J Surg Oncol. 2020;18(1):1–12. doi:10.1186/s12957-020-01952-2
24. Schietroma M, Romano L, Schiavi D, et al. Systemic inflammation response index (SIRI) as predictor of anastomotic leakage after total gastrectomy for gastric cancer. Surg Oncol. 2022;43:101791. doi:10.1016/j.suronc.2022.101791
25. Young E, Philpott H, Singh R. Endoscopic diagnosis and treatment of gastric dysplasia and early cancer: current evidence and what the future may hold. World J Gastroenterol. 2021;27(31):5126–5151. doi:10.3748/wjg.v27.i31.5126
26. Tan S, Zheng Q, Zhang W, et al. Prognostic value of inflammatory markers NLR, PLR, and LMR in gastric cancer patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Front Immunol. 2024;15:1408700. doi:10.3389/fimmu.2024.1408700
27. Jing Y, Ren M, Li X, et al. The Effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Early Gastric Cancer. J Inflamm Res. 2024;17:10273–10287. doi:10.2147/JIR.S499094
28. Fang T, Wang Y, Yin X, et al. Diagnostic Sensitivity of NLR and PLR in Early Diagnosis of Gastric Cancer. J Immunol Res. 2020;2020:9146042. doi:10.1155/2020/9146042
29. Hou N, Li M, He L, et al. Predicting 30-days mortality for MIMIC-III patients with sepsis-3: a machine learning approach using XGboost. J Transl Med. 2020;18(1):462. doi:10.1186/s12967-020-02620-5
30. Banks M, Graham D, Jansen M, et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut. 2019;68(9):1545–1575. doi:10.1136/gutjnl-2018-318126
31. Kennel KB, Bozlar M, De Valk AF, et al. Cancer-Associated Fibroblasts in Inflammation and Antitumor Immunity. Clin Cancer Res. 2023;29(6):1009–1016. doi:10.1158/1078-0432.CCR-22-1031
32. Bambace NM, Holmes CE. The platelet contribution to cancer progression. J Thromb Haemost. 2011;9(2):237–249. doi:10.1111/j.1538-7836.2010.04131.x
33. Poto R, Gambardella AR, Marone G, et al. Basophils from allergy to cancer. Front Immunol. 2022;13:1056838. doi:10.3389/fimmu.2022.1056838
34. Marone G, Schroeder JT, Mattei F, et al. Is there a role for basophils in cancer? Front Immunol. 2020;11:2103. doi:10.3389/fimmu.2020.02103
35. Wu J, Ge XX, Zhu W, et al. Values of applying white blood cell counts in the prognostic evaluation of resectable colorectal cancer. Mol Med Rep. 2019;19(3):2330–2340. doi:10.3892/mmr.2019.9844
36. van der Leun AM, Thommen DS, Schumacher TN. CD8+ T cell states in human cancer: insights from single-cell analysis. Nat Rev Cancer. 2020;20(4):218–232. doi:10.1038/s41568-019-0235-4
37. Yuen GJ, Demissie E, Pillai S. B lymphocytes and cancer: a love-hate relationship. Trends Cancer. 2016;2(12):747–757. doi:10.1016/j.trecan.2016.10.010
38. Nøst TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
39. Minici R, Siciliano MA, Ammendola M, et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio (NLR), Lymphocyte-to-Monocyte Ratio (LMR), Platelet-to-Lymphocyte Ratio (PLR) and Lymphocyte-to-C Reactive Protein Ratio (LCR) in Patients with Hepatocellular Carcinoma (HCC) undergoing Chemoembolizations (TACE) of the Liver: the Unexplored Corner Linking Tumor Microenvironment, Biomarkers and Interventional Radiology. Cancers (Basel). 2022;15(1):257. doi:10.3390/cancers15010257
40. Xiong S, Dong L, Cheng L. Neutrophils in cancer carcinogenesis and metastasis. J Hematol Oncol. 2021;14(1):173. doi:10.1186/s13045-021-01187-y
41. Conte E. Targeting monocytes/macrophages in fibrosis and cancer diseases: therapeutic approaches. Pharmacol Ther. 2022;234:108031. doi:10.1016/j.pharmthera.2021.108031
42. Ugel S, Canè S, De Sanctis F, et al. Monocytes in the Tumor Microenvironment. Annu Rev Pathol. 2021;16:93–122. doi:10.1146/annurev-pathmechdis-012418-013058
43. Xia Y, Xia C, Wu L, et al. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: a 20-Year Follow-Up Cohort Study of 42,875 US Adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
44. Wan G, Gao F, Chen J, et al. Nomogram prediction of individual prognosis of patients with hepatocellular carcinoma. BMC Cancer. 2017;17(1):91. doi:10.1186/s12885-017-3062-6
45. Yang J, Wang X, Jiang S. Development and validation of a nomogram model for individualized prediction of hypertension risk in patients with type 2 diabetes mellitus. Sci Rep. 2023;13(1):1298. doi:10.1038/s41598-023-28059-4
46. Sun D, Lei L, Xia C, et al. Sociodemographic disparities in gastric cancer and the gastric precancerous cascade: a population-based study. Lancet Reg Health West Pac. 2022;23:100437. doi:10.1016/j.lanwpc.2022.100437
47. de Vries AC, van Grieken NC, Looman CW, et al. Gastric cancer risk in patients with premalignant gastric lesions: a nationwide cohort study in the Netherlands. Gastroenterology. 2008;134(4):945–952. doi:10.1053/j.gastro.2008.01.071
48. Rehm J, Mathers C, Popova S, et al. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009;373(9682):2223–2233. doi:10.1016/S0140-6736(09)60746-7
49. Laszkowska M, Rodriguez S, Kim J, et al. Heavy Alcohol Use Is Associated With Gastric Cancer: analysis of the National Health and Nutrition Examination Survey From 1999 to 2010. Am J Gastroenterol. 2021;116(5):1083–1086. doi:10.14309/ajg.0000000000001166
50. Yu Z, Zuo T, Yu H, et al. Outcomes of upper gastrointestinal cancer screening in high-risk individuals: a population-based prospective study in Northeast China. BMJ Open. 2022;12(2):e046134. doi:10.1136/bmjopen-2020-046134
51. Jin M, Cai S, Guo J, et al. Alcohol drinking and all cancer mortality: a meta-analysis. Ann Oncol. 2013;24(3):807–816. doi:10.1093/annonc/mds508
52. Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan, Inoue M, Nagata C, Tsuji I, et al. Impact of alcohol intake on total mortality and mortality from major causes in Japan: a pooled analysis of six large-scale cohort studies. J Epidemiol Community Health. 2012;66(5):448–456. doi:10.1136/jech.2010.121830.
53. Wu X, Zhang Q, Guo H, et al. Dietary patterns and risk for gastric cancer: a case-control study in residents of the Huaihe River Basin, China. Front Nutr. 2023;10:1118113. doi:10.3389/fnut.2023.1118113
54. Kim HJ, Kim N, Kim HY, et al. Relationship between body mass index and the risk of early gastric cancer and dysplasia regardless of Helicobacter pylori infection. Gastric Cancer. 2015;18(4):762–773. doi:10.1007/s10120-014-0429-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.