Back to Journals » International Journal of General Medicine » Volume 14
A Nomogram Based on Comorbidities and Infection Location to Predict 30 Days Mortality of Immunocompromised Patients in ICU: A Retrospective Cohort Study
Received 1 November 2021
Accepted for publication 8 December 2021
Published 24 December 2021 Volume 2021:14 Pages 10281—10292
DOI https://doi.org/10.2147/IJGM.S345632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xuequn Guo,1 Donghao Guo2
1Department of Respiratory Medicine, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, Fujian, People’s Republic of China; 2Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Donghao Guo
Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
Email [email protected]
Background: The existing comorbidity indexes, like Charlson Comorbidity Index (CCI) and the Elixhauser Comorbidity Index (ECI), do not take infection factors into account for critically ill patients with immunocompromise, bringing about a decrease of prediction accuracy. Therefore, we attempted to incorporate infection location into the analysis to construct a rapid comorbidity scoring system independent of laboratory tests.
Methods: Data were extracted from the Multiparameter Intelligent Monitoring in Intensive Care III database. A total of 3904 critically ill patients with immunocompromise admitted to ICU were enrolled and assigned into training or validation sets according to the date of ICU admission. The predictive nomogram was constructed in the training set based on logistic regression analysis and then undergone validation in the validation set in comparison with SOFA, CCI and ECI.
Results: Factors eligible for the nomogram included patient’s age, gender, ethnicity, underlying disease of immunocompromise like metastatic cancer and leukemia, possible infection on admission including pulmonary infection, urinary tract infection and blood infection, and one comorbidity, coagulopathy. The nomogram we developed exhibited better discrimination than SOFA, CCI and ECI with an area under the receiver operating characteristic curve (AUC) of 0.739 (95% CI 0.707– 0.771) and 0.746 (95% CI 0.713– 0.779) in the training and validation sets, respectively. Combining the nomogram and SOFA could bring a new prediction model with a superior predictive effect in both sets (training set AUC = 0.803 95% CI 0.777– 0.828, validation set AUC = 0.818 95% CI 0.783– 0.854). The calibration curve exhibited coherence between the nomogram and ideal observation for two cohorts (p> 0.05). Decision curve analysis revealed the clinical usefulness of the nomogram in both sets.
Conclusion: We established a nomogram that could provide an accurate assessment of 30 days ICU mortality in critically ill patients with immunocompromise, which can be employed to evaluate the short-term prognosis of those patients and bring more clinical benefits without dependence on laboratory tests.
Keywords: immunocompromised patients, intensive care unit, large observational database, 30 days ICU mortality, nomogram
Introduction
From the clinical point of view, the treatments of critically ill patients have always been a difficult point. Immunocompromise, accounting for a growing proportion of patients with severe illness, makes managements for those even harder.1 More severe comorbidities and more vulnerability to infection in immunocompromised patients might bring about the increased need of medical resources including a number of tests, the followed treatments, and extra nursing care. Some uncommon diseases or conditions in the ICU, like AIDS, malignant tumors, leukemia, lymphoma, autoimmune diseases, stem cells or organ transplants, will lead to decrease in immune cells or long-term and high-dose use of corticosteroids and immunosuppressors, finally immunocompromise followed by a bad ending.2,3 Nowadays, more and more people are suffering from these disorders. For example, there are nearly 37.8 million person living with HIV worldwide, corresponding to about 50% increase since the early 2000s.4 Similarly, the global prevalence of autoimmune diseases is approximately 3%, up to 25% require hospitalization and, of these, above 30% call for ICU admission.5 The same is true for malignant tumors, with one malignancy diagnosis in every six patients treated in European ICUs.6 Immunocompromise is defined as having a weakened immune system with less resistance to infections and more fragility to some comorbidities. For these patients, multidisciplinary treatments and nursing are required for better outcomes.
For critically ill patients, SOFA score can provide an accurate assessment for prognosis, but the reliance on laboratory tests makes it limited. As a classic non-specific comorbidity assessment tool, Charlson Comorbidity Index (CCI) and the Elixhauser Comorbidity Index (ECI) can be used for rapid prognosis evaluation of admitted patients without the support of laboratory tests, which has gained increasing attention in clinical practice.7,8 An increasing number of studies have demonstrated that, both CCI and ECI could effectively predict the prognosis of severely ill patients, enabling more detailed managements to be conducted in the patients with poor prognosis in the first place.9–11
However, there are some limitations of CCI and ECI, such as failure to include certain conditions that would make patients ineligible to be assigned to an arm of a study,12 Especially, with the absence of attention to infection, CCI and ECI have noteworthy limitations in predicting the prognosis of immunocompromised patients, for whom infection is an important cause of ICU admission.13 To our knowledge, few studies have been conducted to determine a comorbidity score as a predictor of prognosis for critically ill patients with immunocompromise. Therefore, the purpose of our study is to generate a better prediction model to evaluate the prognosis of immunocompromised patients in ICU more accurately and more promptly.
Materials and Methods
Data Source
Our observational study was conducted using data retrieved from the Medical Information Mart for Intensive Care (MIMIC III v1.4) open-source clinical database, which is licensed under a Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0). This database contains information for more than 58,000 patients who were admitted to the intensive care unit (ICU) of the Beth Israel Deaconess Medical Center from 2001 to 2012.14 All data in the database was classified into 26 tables recording various individual information, such as demographic characteristics, treatment measures, nursing notes, and laboratory tests. Besides, it contains prognostic data obtained from the hospital and laboratory health record systems reporting the hospital mortality, or from the Social Security Administration Death Master File recording the out-of-hospital survival data. To access the database, we completed courses in protecting human research participants, signed an agreement to use data from the database appropriately and not to divulge patients’ information and finally got official permission.14 PgAdmin (version 4.1, Bedford, USA), a working platform used to operate structured query language (SQL), was performed to extract data.
Study Population
Inclusion criteria: patients with 1) at least one of the immunocompromised conditions; 2) age between 18 and 100 years; 3) spending at least 24 hours in the ICU. The immunocompromised condition was defined by suffering from underlying diseases, including human immunodeficiency virus (HIV) infection or acquired immune deficiency syndrome (AIDS), solid tumor with or without metastasis, leukemia, lymphoma, stem cell or solid organ transplantation and autoimmune disease.15–17 Those diseases were established by the ICD-9-CM codes, which has been repeatedly verified and widely used in various studies.18,19 Exclusion criteria are pregnancy or some surgically related comorbidities like severe trauma, burns and vital organ surgery. For all patients, only the data of the first ICU admission was included in our study.
Data Extraction
Data of the demographic features (age, gender, BMI, and ethnicity), bacteriological laboratory outcomes, types of immunocompromised condition (including HIV/AIDS, solid-state tumors, metastatic cancer, transplantation, leukemia, lymphoma, and autoimmune disease), presence of any comorbidities or complications (including congestive heart failure, cardiac arrhythmias, valvular disease, chronic pulmonary disease, etc.), disease severity scores, and comorbidity indexes on the ICU admission was elicited from the MIMIC-III database. The site of infection was first identified through the diagnosis provided by the database, which was determined by clinicians based on symptoms, physical assessment, and history taking, and then further verified by positive culturing results.20 Comorbidities were erected by the Elixhauser, a table created from past retrieval code summarized in the ICD-9-CM codes. Data extraction was performed by PostgreSQL (version 10, www. postgresql.org). No missing data was found in all comorbidities’ variables and most of the commonly used information. To deal with missing data on height and weight, regression imputation was used to estimate the missing value.
Statistical Analysis and Nomogram Development
Descriptive statistics were represented at baseline using mean with standard deviations or median with interquartile ranges for continuous variables and frequencies (percentage) for categorical variables. According to the time of ICU admission, the earlier 70% patients were selected as the training set (t set), and the other 30% patients from later time period as the validation set (v set). Patient characteristics were compared between survivors and non-survivors in both sets. The Student’s t-test, Wilcoxon rank-sum test, or Kruskal–Wallis test was performed for comparisons of continuous baseline characteristics as appropriate. Chi-square test was performed for categorical data.
In the training set, univariate logical analysis was used to preliminarily identify the risk factors for 30 days ICU mortality, and then the stepwise forward logical analysis was employed to verified these factors. Variance inflation factor (VIF) was taken to test collinearity between continuous variables, and VIF ≤ 5 was seen as non-collinearity.21 Then, the independent risk factors (p < 0.05) obtained from the above analysis, like age, gender, ethnicity, metastatic cancer, leukemia, pulmonary infection, urinary tract infection, blood infection, and coagulopathy, were included in the full model to acquire a nomogram in predicting the probability of short-term ICU death. Then, a new model was obtained by combining the nomogram and the SOFA with univariate logical analysis to further verify the clinical value of the nomogram. The discriminative ability of the nomogram and the nomogram merged with SOFA was assessed in comparison with SOFA, CCI and ECI in the training and validation sets by estimating the area under the receiver operating characteristic curve (AUROC).22,23 The calibration curve was used to evaluate the coherence between the nomogram and ideal observation. The clinical practicality of the predictive nomogram was conducted by the decision curve analysis. Stata/IC 15.1 software (StataCorp, Texas, USA) and R software (version 4.0.0, www.r-project.org) were employed for the statistical analysis.
Results
Characteristics of Participants
After screening by the inclusion and exclusion criteria, a total of 3904 patients were included in our analysis. Training and validation sets were obtained by a ratio of 7:3 according to the time of ICU admission (an earlier time period for model development and later years in the study period for validation), and then the baseline characteristics of both sets of patients are exhibited in Table 1. The 30 days ICU mortality of the training set and verification set were 13.8% and 12.4%, respectively. Significant differences in SOFA (t and v set p<0.001) were observed between the survivors and the non-survivors in both sets, the same to CCI (t and v set p=0.010) and ECI (t and v p<0.001). Patients with diseases causing immunocompromise, like solid-state tumors (t set p=0.003, v set p=0.325), metastatic cancer (t set p=0.002, v set p=0.001), leukemia (t set p=0.021, v set p=0.620), or organ transplantation (t set p=0.112, v set p=0.005), have been found to have a higher 30 day ICU mortality. Besides, participants with congestive heart failure (t set p=0.418, v set p=0.031), pulmonary circulatory disease (t set p=0.014, v set p=0.755), diabetes with complications (t set p=0.046, v set p=0.848), coagulopathy (t and v set Patients’ characteristics at ICU admission0.001) and renal failure (t set p=0.031, v set p=0.345), are more likely to die in a short term during ICU stay.
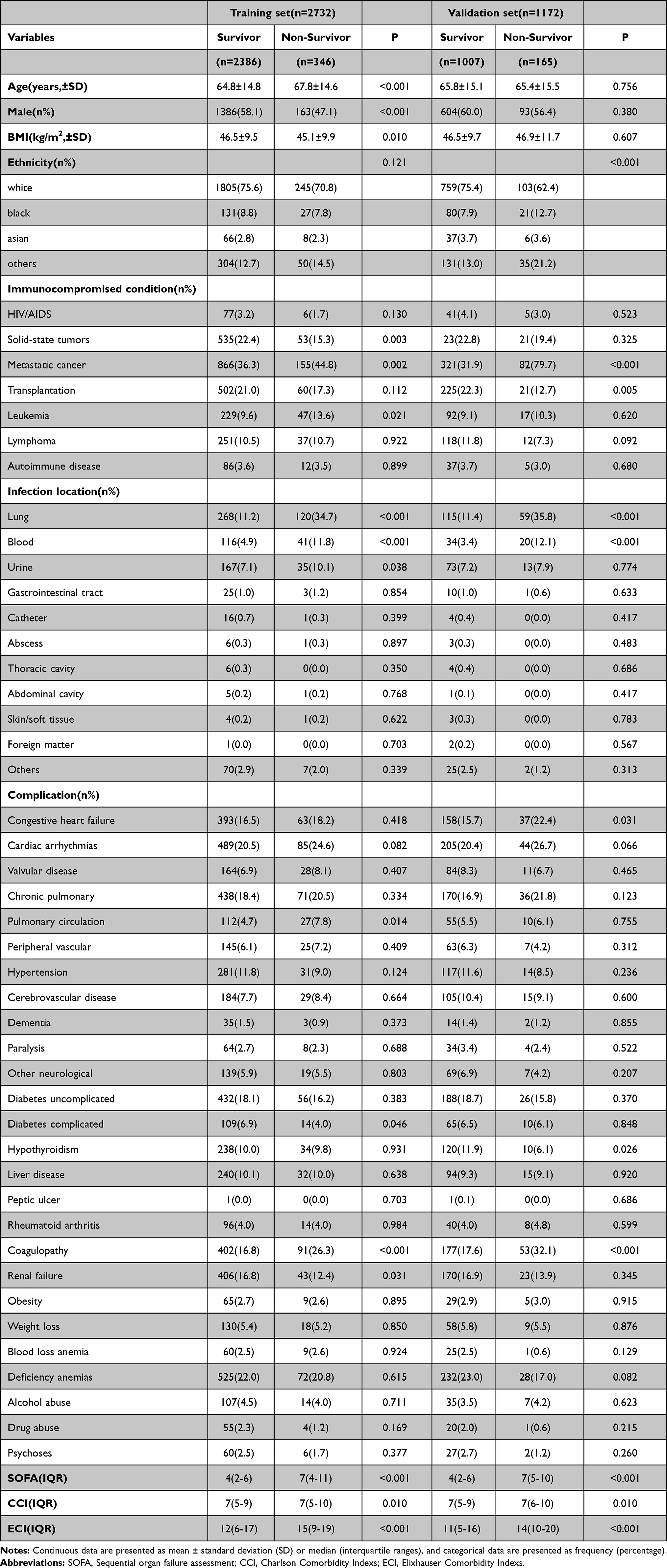 |
Table 1 Patients’ characteristics at ICU admission |
Development of a Nomogram in the Training Set
The univariate logistic model was conducted to identify significant variables. Then, by further verification of the stepwise forward logical analysis, the independent risk parameters related to 30 days ICU mortality of critically ill patients with immunocompromise were confirmed as shown in Table 2. Finally, the predicted nomogram was plotted by assigning a weighted score for each of the independent risk predictive factors. The higher total scores calculated from the sum of the appointed points for each prognostic indicator in the nomogram, the higher the risk of decease. The nomogram is shown in Figure 1. To employ the nomogram for calculation of the survival probability, we first draw a vertical line from each variable upward to the points axis to obtain the value for each variable and then sum up all the values to get the total points (ie, with pulmonary infection = 10 points). Lastly, we draw a vertical line from the total points axis to the prob line, then the predicted probability of 30 days ICU death is achieved.
 |
Table 2 Independent risk factors associated with 30 days ICU mortality of critically ill patients with immunocompromise in the training group |
 |
Figure 1 Nomograms predicting 30 days ICU mortality of critically ill patients with immunocompromise on ICU admission. |
Validation of the Nomogram
The nomogram model was validated in the training and the validation sets. The good predictive performance of the nomogram was confirmed for predicting 30 days ICU survival with an area under curve (AUC) of 0.739 (95% CI 0.707–0.771) in the training sets and an AUC of 0.746 (95% CI 0.713–0.779) in the validation sets (Figure 2). As shown in Figure 3, calibration curves revealed that prediction of 30 days ICU survival by the nomogram in both sets had a high fitting degree with the actual survival values.
 |
Figure 2 The ROC curve of the prediction nomogram, SOFA, CCI, ECI and the nomogram SOFA combined model in the training set (A) and validation set (B). Abbreviations: SOFA, sequential Organ Failure Assessment; CCI, Charlson Comorbidity Indexes; ECI, Elixhauser Comorbidity Indexes. |
 |
Figure 3 The calibration curves for the prediction of 30 days ICU mortality of critically ill patients with immunocompromise in the training set (A) and validation set (B). |
Comparison of Nomogram, SOFA, CCI, ECI and Nomogram Merged with SOFA
Nomogram and SOFA were combined into a new variable through logical analysis, followed by subsequent analysis. The AUC of the receiver operating characteristic curves (ROC) was used to compare the predictive accuracy of nomogram, SOFA, CCI, ECI and the nomogram merged with SOFA for 30 days ICU mortality of critically ill patients with immunocompromise. As shown in Figure 2, we found that the AUC of nomogram (t set AUC=0.741, v set AUC=0.734) was close to that of SOFA (t set AUC=0.724, v set AUC=0.759), and greater than those of CCI (t set AUC=0.543, v set AUC=0.562) and ECI (t set AUC=0.603, v set AUC=0.642) in both sets, indicating that the predictive nomogram had better discrimination than CCI and ECI in predicting the 30 days ICU mortality of critically ill patients with Immunocompromise, meanwhile, as good as SOFA. When we merged the nomogram and SOFA to obtain a new prediction model, the AUC results suggested that the model had a superior predictive effect on ICU short-term mortality in both sets (t set AUC=0.803, v set AUC=0.818; more details exhibited in Table 3). The calibration plot revealed fit of the nomogram predicting the risk of death in both sets. In addition, decision curve analysis (DCA) revealed that nomogram and SOFA could bring the most net benefits for clinical application with great diagnostic value and uniting of the two could highly strengthen the benefits (Figure 4). All of the above testified the stability and superior predictive effects of this nomogram.
 |
Table 3 Comparison of predictive models in predicting the 30 days ICU mortality of critically ill patients with immunocompromise |
 |
Figure 4 The DCA curve of medical intervention in critically ill patients with immunocompromise with the nomogram, SOFA, CCI, ECI and the nomogram+SOFA model in the training set (A) and validation set (B). Abbreviation: DCA, decision curve analysis. |
Discussion
Up to now, there have been many disease severity scores that can be used to make a preliminary assessment of the prognosis of severe patients. Most of them have been proved accurate by repeated clinical trials. Among them, SOFA is very representative and widely adopted in clinical work. Hence, SOFA was selected as a comparison of the nomogram in our research. SOFA was established in the early 1990s and has been suggested to play a useful role in assessing the prognosis of critically ill patients since then. It is now widely used in ICU as an evaluation standard for sepsis.24 However, its dependence on laboratory results makes it impracticable to conduct a prognostic assessment for the first time of admission. Herein, we developed the nomogram independent of laboratory test results. Our research show that the nomogram could be applied as a well-performing prediction model for assessing critically ill patients under the risk of 30-day mortality, which might improve the practicability with similar predictive performance compared to SOFA.
As critically ill patients are usually accompanied with a variety of comorbidities, the condition of comorbidities obtained by a simple inquiry at the time of admission could serve as the earliest clinical data for doctors to assess the patient’s prognosis. Through systematic scoring system, the understanding of comorbidities on treatment outcome is becoming more and more mature.12 Among them, CCI and ECI, which have been fully validated in a number of studies, are most widely used,25,26 to predict the prognosis of critically ill patients without laboratory results.7,12 Therefore, we focused our attention on the prognostic value of the two for critically ill patients with immunocompromise. Unfortunately, according to our preliminary analysis, the efficacy of CCI and ECI in evaluating the short-term survival of critically ill patients with immunocompromise is not satisfactory (AUC < 0.65). It is well known that patients with immunocompromised status, such as AIDS, malignant tumors, organ transplantation, etc, are more likely to acquire infection, and infection is often the root cause of exacerbation of other complications and deterioration of general conditions, eventually leading to ICU admission.13,27–29 We therefore suggest the inclusion of infections in the comorbidity index system. The results showed that our prediction nomogram could serve as a more reliable prediction model with better discrimination than CCI and ECI, which could reach the SOFA level without the support of laboratory test results. And when we combine the nomogram with SOFA, a much better predictor of short-term mortality will be achieved (AUC > 0.8). DCA results also showed more net benefits of treatment guided by the current nomogram than CCI and ECI. Furthermore, more net benefits could be achieved when the nomogram and SOFA were combined.
As indicated in the nomogram, malignancy with metastasis and leukemia are associated with poor prognosis in the underlying diseases leading to immunocompromise. More attention should be paid when we are dealing with such immunocompromised patients. However, AIDS, which is highly emphasized in CCI, is not an independent influence factor in our analysis. We assumed the fundamental reason might lie in the inclusion of infection factors. From various studies, infections are closely related to the short-term outcome of AIDS.30 Thus, the inclusion of infections will lessen the impact of AIDS and ultimately lead to its exclusion.
After taking into account a variety of comorbidities, our nomogram shows that coagulopathy significantly affects the short-term survival of critically ill immunocompromised patients. None of the congestive heart failure (CHF), arrhythmia, and chronic obstructive pulmonary disease (COPD) are identified as independent risk factors in our study, divergent from the marking criterion of CCI and ECI. We assume the reason might be that most common diseases, like CHF, COPD and so on, could be well settled with low short-term mortality following the current clinical practice guidelines.31,32 Nevertheless, the occurrence of coagulopathy has been certified by many studies to be related to the poor prognosis of patients with immunocompromised status such as malignant tumor and organ transplantation.33–35 Meanwhile, dynamic changes in coagulopathy are considered to be associated with the prognosis of severe infection.36 This reminds us that immunocompromised patients with coagulopathy require to be given more attention in ICU.
The nomogram shows that, after the effects of age and other factors are standardized, the top three with the strongest influence on the predictive ability of short-term prognosis are all infectious diseases, as expected.37,38 Among them, pulmonary infection is the most influential, followed by blood infection and urinary tract infection, of which similar results have been reported in previous studies39−44. These are the sites of infection associated with short-term death in immunocompromised patients admitted to ICU, and previous studies have confirmed that immunocompromised patients suffer from these infections tend to have poorer prognosis, like longer hospital stays, more difficult to relieve symptoms, or higher mortality.45–50 This means that consideration of immunocompromised patients with these types of infections on ICU admission requires to be strengthened.
With regard to demographic factors, after standardizing the effects of factors such as comorbidities and infections, we found that gender could influence participants’ short-term prognosis. Among patients with immunocompromise, women had a higher short-term ICU mortality rate than men. Current researches have produced conflicting results as to whether gender affect outcomes of critically ill patients.51,52 The reason for such a phenomenon may be related to the difference in physical quality or some other factors, for example, the fact that currently established treatment guidelines do not distinguish between genders.
Immunocompromised is a very broad term and is poorly defined. A study published in JMMA 2018 by Azoulay et al defined immunocompromise as long-term or high-dose use of steroids or other immunosuppressant drugs, organ transplants history, and accompanied by tumors or some diseases cause immune system damaged.15 In recent years, Sheth et al16 and Lu et al17 used this definition in respective research with data extracted from MIMIC database. Therefore, we also refer to the above author’s scheme and define immunocompromised by a similar way (carrying diseases including HIV/AIDS, solid-state tumors, metastatic cancer, transplantation, leukemia, lymphoma, or autoimmune disease). Of course, these seven conditions cannot completely include all immunocompromised stations. However, since there is no precise international specification for immunocompromise, this definitional method is relatively feasible and practical.17
Using Mimic III database, one of the biggest advantages of our research is the sufficient sample size, which gives us a large number of data to include numerous variables for analysis, greatly increasing the statistical power of our results. Some shortcomings in our research should be addressed as well. First, data of Mimic III database recorded from 2001, which is relatively backward in terms of treatment. For example, the lack of some current advanced treatment options, like ECMO, may cause overestimation the risks of some factors. Second, both the training set and validation set are derived from the same database. If validation set could use another existing clinical data, the conclusion of our research will be more persuasive since database bias could be excluded. In addition, due to the lack of relevant data, long-term use of corticosteroids and reduction of immune cells is not adopted as the criteria for the definition of immunocompromised status. Instead, diseases accompanying or causing immunocompromise were employed as the inclusion criteria, which may lead to underestimation. Finally, for the limitations of Mimic III database, we could only analyze the infection location based on the results instead of the time-based dynamic analysis, which will produce certain deviations in our results. Also, because regression imputation was used to deal with missing data on height and weight, the standard error is reduced.53
Conclusion
We established a nomogram based on demographic characteristics, comorbidities, and possible infection localization to provide an accurate assessment of 30 days ICU mortality in critically ill patients with immunocompromise. This may enable patients with poor short-term prognosis to be recognized and to receive adequate attention and treatments before the results of the laboratory tests are reported, thus leading to a greater degree of benefit in terms of short-term prognosis.
Data Sharing Statement
The full datasets used in this study are available from the corresponding author on reasonable request. However, reanalysis of the full data for other use requires approval by the MIMIC-III Institute.
Ethics Approval and Consent to Participate
All the data presented in this study were extracted from MIMIC-III online database, which was approved by the Massachusetts Institute of Technology (Cambridge, MA) and Beth Israel Deaconess Medical Center (Boston, MA), and consent was obtained for the original data collection. Therefore, the ethical approval statement and the need for informed consent were waived for this manuscript.
Funding
There is no funding to report.
Disclosure
There is no conflict of interest related to this work.
References
1. Soares M, Bozza FA, Angus DC, et al. Organizational characteristics, outcomes, and resource use in 78 Brazilian intensive care units: the ORCHESTRA study. Intensive Care Med. 2015;41(12):2149–2160. doi:10.1007/s00134-015-4076-7
2. Darmon M, Ranzani OT, Azoulay E. Focus on immunocompromised patients. Intensive Care Med. 2017;43(9):1415–1417. doi:10.1007/s00134-017-4857-2
3. Azoulay E, Soares M, Benoit D. Focus on immunocompromised patients. Intensive Care Med. 2016;42(3):463–465. doi:10.1007/s00134-016-4224-8
4. Barbier F, Mer M, Szychowiak P, et al. Management of HIV-infected patients in the intensive care unit. Intensive Care Med. 2020;46(2):329–342. doi:10.1007/s00134-020-05945-3
5. Morales-Tisnes T, Quintero-Ortiz L, Quintero-Munoz E, Sierra-Matamoros F, Arias-Aponte J, Rojas-Villarraga A. Prevalence of hospital readmissions and related factors in patients with autoimmune diseases. J Transl Autoimmun. 2021;4:100121. doi:10.1016/j.jtauto.2021.100121
6. Buchtele N, Lobmeyr E, Cserna J, et al. Prevalence and impact of vitamin D deficiency in critically ill cancer patients admitted to the intensive care unit. Nutrients. 2020;13(1):22. doi:10.3390/nu13010022
7. Ladha KS, Zhao K, Quraishi SA, et al. The Deyo-Charlson and Elixhauser-van Walraven Comorbidity Indices as predictors of mortality in critically ill patients. BMJ Open. 2015;5(9):e008990. doi:10.1136/bmjopen-2015-008990
8. Sharabiani MT, Aylin P, Bottle A. Systematic review of comorbidity indices for administrative data. Med Care. 2012;50(12):1109–1118. doi:10.1097/MLR.0b013e31825f64d0
9. Southern DA, Quan H, Ghali WA. Comparison of the Elixhauser and Charlson/Deyo methods of comorbidity measurement in administrative data. Med Care. 2004;42(4):355–360.
10. Lieffers JR, Baracos VE, Winget M, Fassbender K. A comparison of Charlson and Elixhauser comorbidity measures to predict colorectal cancer survival using administrative health data. Cancer. 2011;117(9):1957–1965. doi:10.1002/cncr.25653
11. Shin JH, Worni M, Castleberry AW, et al. The application of comorbidity indices to predict early postoperative outcomes after laparoscopic Roux-en-Y gastric bypass: a nationwide comparative analysis of over 70,000 cases. Obes Surg. 2013;23(5):638–649. doi:10.1007/s11695-012-0853-3
12. Austin SR, Wong YN, Uzzo RG, Beck JR, Egleston BL. Why summary comorbidity measures such as the Charlson Comorbidity Index and Elixhauser Score Work. Med Care. 2015;53(9):e65–72. doi:10.1097/MLR.0b013e318297429c
13. Koulenti D, Vogelaers D, Blot S. What’s new in invasive pulmonary aspergillosis in the critically ill. Intensive Care Med. 2014;40(5):723–726. doi:10.1007/s00134-014-3254-3
14. Johnson AE, Pollard TJ, Shen L, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035. doi:10.1038/sdata.2016.35
15. Azoulay E, Lemiale V, Mokart D, et al. Effect of high-flow nasal oxygen vs standard oxygen on 28-day mortality in immunocompromised patients with acute respiratory failure: the HIGH randomized clinical trial. JAMA. 2018;320(20):2099–2107. doi:10.1001/jama.2018.14282
16. Sheth M, Benedum CM, Celi LA, Mark RG, Markuzon N. The association between autoimmune disease and 30-day mortality among sepsis ICU patients: a cohort study. Crit Care. 2019;23(1):93. doi:10.1186/s13054-019-2357-1
17. Lu X, Wang X, Gao Y, et al. Efficacy and safety of corticosteroids for septic shock in immunocompromised patients: a cohort study from MIMIC. Am J Emerg Med. 2021;42:121–126. doi:10.1016/j.ajem.2020.02.002
18. Johnson AE, Stone DJ, Celi LA, Pollard TJ. The MIMIC code repository: enabling reproducibility in critical care research. J Am Med Inform Assoc. 2018;25(1):32–39. doi:10.1093/jamia/ocx084
19. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
20. Peker N, Couto N, Sinha B, Rossen JW. Diagnosis of bloodstream infections from positive blood cultures and directly from blood samples: recent developments in molecular approaches. Clin Microbiol Infect. 2018;24(9):944–955. doi:10.1016/j.cmi.2018.05.007
21. Marcoulides KM, Raykov T. Evaluation of variance inflation factors in regression models using latent variable modeling methods. Educ Psychol Meas. 2019;79(5):874–882. doi:10.1177/0013164418817803
22. Le Gall JR, Klar J, Lemeshow S, et al. The Logistic Organ Dysfunction system. A new way to assess organ dysfunction in the intensive care unit. ICU Scoring Group. JAMA. 1996;276(10):802–810. doi:10.1001/jama.1996.03540100046027
23. Van Den Berg HA. Occam’s razor: from Ockham’s via moderna to modern data science. Sci Prog. 2018;101(3):261–272. doi:10.3184/003685018X15295002645082
24. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23(1):374. doi:10.1186/s13054-019-2663-7
25. Mehta HB, Sura SD, Adhikari D, et al. Adapting the Elixhauser comorbidity index for cancer patients. Cancer. 2018;124(9):2018–2025. doi:10.1002/cncr.31269
26. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
27. Alp E, Damani N. Healthcare-associated infections in intensive care units: epidemiology and infection control in low-to-middle income countries. J Infect Dev Ctries. 2015;9(10):1040–1045. doi:10.3855/jidc.6832
28. Salzberger B, Hitzenbichler F, Hanses F. [Treatment of infections in the critically ill under immunosuppression: what must be considered?]. Z Rheumatol. 2019;78(10):940–946. German. doi:10.1007/s00393-019-00706-0
29. Florescu DF, Stohs EJ. Approach to infection and disease due to adenoviruses in solid organ transplantation. Curr Opin Infect Dis. 2019;32(4):300–306. doi:10.1097/QCO.0000000000000558
30. Zeng L, Ma Y. [Application of different death evaluation indicators for HIV/AIDS prevention and treatment]. Zhonghua Liu Xing Bing Xue Za Zhi. 2016;37(5):745–748. Chinese. doi:10.3760/cma.j.issn.0254-6450.2016.05.033
31. Rogers RL, Feller ED, Gottlieb SS. Acute congestive heart failure in the emergency department. Cardiol Clin. 2006;24(1):115–123, vii. doi:10.1016/j.ccl.2005.09.004
32. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
33. Ball S, Nugent K. Microparticles in hematological malignancies: role in coagulopathy and tumor pathogenesis. Am J Med Sci. 2018;355(3):207–214. doi:10.1016/j.amjms.2017.11.014
34. Wang H, Liu W, Tian M, et al. Coagulopathy associated with poor prognosis in intrahepatic cholangiocarcinoma patients after curative resection. Biosci Trends. 2017;11(4):469–474. doi:10.5582/bst.2017.01080
35. Sabate A, Dalmau A, Koo M, Aparicio I, Costa M, Contreras L. Coagulopathy management in liver transplantation. Transplant Proc. 2012;44(6):1523–1525. doi:10.1016/j.transproceed.2012.05.004
36. Dhainaut JF, Shorr AF, Macias WL, et al. Dynamic evolution of coagulopathy in the first day of severe sepsis: relationship with mortality and organ failure. Crit Care Med. 2005;33(2):341–348. doi:10.1097/01.CCM.0000153520.31562.48
37. Fang WF, Chen YM, Lin CY, et al. Immune profiles and clinical outcomes between sepsis patients with or without active cancer requiring admission to intensive care units. PLoS One. 2017;12(7):e0179749. doi:10.1371/journal.pone.0179749
38. Takeda K, Sawada Y, Kumamoto T, Tanaka K, Endo I. Severe sepsis after living donor liver transplantation: risk factors and outcomes. Transplant Proc. 2016;48(6):2124–2129. doi:10.1016/j.transproceed.2016.03.040
39. Rosenow EC, Wilson WR, Cockerill FR. Pulmonary disease in the immunocompromised host. 1. Mayo Clin Proc. 1985;60(7):473–487. doi:10.1016/S0025-6196(12)60872-6
40. Beck JM, Rosen MJ, Peavy HH. Pulmonary complications of HIV infection. Report of the fourth NHLBI workshop. Am J Respir Crit Care Med. 2001;164(11):2120–2126. doi:10.1164/ajrccm.164.11.2102047
41. Bajaj SK, Tombach B. Respiratory infections in immunocompromised patients: lung findings using chest computed tomography. Radiol Infect Dis. 2017;4(1):29–37. doi:10.1016/j.jrid.2016.11.001
42. Vazquez Guillamet C, Hsu JL, Dhillon G, Vazquez Guillamet R. Pulmonary infections in immunocompromised hosts: clinical. J Thorac Imaging. 2018;33(5):295–305. doi:10.1097/RTI.0000000000000351
43. De Carvalho Parahym AM, De Melo LR, De Morais VL, Neves RP. Candidiasis in pediatric patients with cancer interned in a university hospital. Braz J Microbiol. 2009;40(2):321–324. doi:10.1590/S1517-83822009000200020
44. Tandogdu Z, Cai T, Koves B, Wagenlehner F, Bjerklund-Johansen TE. Urinary tract infections in immunocompromised patients with diabetes, chronic kidney disease, and kidney transplant. Eur Urol Focus. 2016;2(4):394–399. doi:10.1016/j.euf.2016.08.006
45. Van de Louw A, Mirouse A, Peyrony O, Lemiale V, Azoulay E. Bacterial pneumonias in immunocompromised patients. Semin Respir Crit Care Med. 2019;40(4):498–507. doi:10.1055/s-0039-1696961
46. Ramirez JA, Musher DM, Evans SE, et al. Treatment of community-acquired pneumonia in immunocompromised adults: a consensus statement regarding initial strategies. Chest. 2020;158(5):1896–1911. doi:10.1016/j.chest.2020.05.598
47. Azoulay E, Russell L, Van de Louw A, et al. Diagnosis of severe respiratory infections in immunocompromised patients. Intensive Care Med. 2020;46(2):298–314. doi:10.1007/s00134-019-05906-5
48. McCreery RJ, Florescu DF, Kalil AC. Sepsis in immunocompromised patients without human immunodeficiency virus. J Infect Dis. 2020;222(Suppl 2):S156–S165. doi:10.1093/infdis/jiaa320
49. Florescu DF, Kalil AC. Cytomegalovirus infections in non-immunocompromised and immunocompromised patients in the intensive care unit. Infect Disord Drug Targets. 2011;11(4):354–364. doi:10.2174/187152611796504773
50. Geerlings SE, Mulvey MA, Stapleton AE, Klumpp DJ. Clinical presentations and epidemiology of urinary tract infections. Microbiol Spectr. 2016;4(5). doi:10.1128/microbiolspec.UTI-0002-2012
51. Valentin A, Jordan B, Lang T, Hiesmayr M, Metnitz PG. Gender-related differences in intensive care: a multiple-center cohort study of therapeutic interventions and outcome in critically ill patients. Crit Care Med. 2003;31(7):1901–1907. doi:10.1097/01.CCM.0000069347.78151.50
52. Mahmood K, Eldeirawi K, Wahidi MM. Association of gender with outcomes in critically ill patients. Crit Care. 2012;16(3):R92. doi:10.1186/CC11355
53. Eslami MH, Rybin DV, Doros G, Siracuse JJ, Farber A. External validation of Vascular Study Group of New England risk predictive model of mortality after elective abdominal aorta aneurysm repair in the Vascular Quality Initiative and comparison against established models. J Vasc Surg. 2018;67(1):143–150. doi:10.1016/j.jvs.2017.05.087
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.