Back to Journals » International Journal of General Medicine » Volume 15
A New Nomogram for Predicting the Postoperative Overall Survival in Patients with Middle-Aged and Elderly Rectal Cancer: A Single Center Retrospective Study in Chinese Population
Authors Zheng H, Li Z ![]() , Zheng S, Li J, Yang J, Zhao E
, Zheng S, Li J, Yang J, Zhao E
Received 15 March 2022
Accepted for publication 19 May 2022
Published 25 May 2022 Volume 2022:15 Pages 5197—5209
DOI https://doi.org/10.2147/IJGM.S365947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Honghong Zheng,1,* Zhehong Li,2,* Shuai Zheng,1 Jianjun Li,1 Ji Yang,1 Enhong Zhao1
1Department of Gastrointestinal Surgery, The Affiliated Hospital of Chengde Medical University, Chengde, 067000, People’s Republic of China; 2Department of Orthopedic, The Affiliated Hospital of Chengde Medical University, Chengde, 067000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Enhong Zhao, The Affiliated Hospital of Chengde Medical University, No. 36 Nanyingzi St., Chengde, 067000, People’s Republic of China, Email [email protected]
Purpose: Patients with middle-aged and elderly rectal cancer (MERC) usually have poor prognosis after surgery. This study aimed to develop a nomogram to achieve individualized prediction of overall survival (OS) in patients with MERC and to guide follow-up and subsequent diagnosis and treatment plans.
Patients and Methods: A total of 349 patients were randomly assigned to the training and validation cohorts in a 7:3 ratio. Multivariate Cox regression analysis was performed using the results of univariate Cox regression analysis to confirm independent prognostic factors of OS. Thereafter, the nomogram was built using the “rms” package. Subsequently, discriminative ability and calibration of the nomogram were evaluated using receiver operating characteristic (ROC) curves, calibration curves, and decision curve analysis (DCA). Integrated discrimination improvement (IDI), net reclassification improvement (NRI), and the area under the ROC curves (AUC) were compared between the nomogram and the tumor-node-metastasis (TNM) staging system (8th edition). Finally, we established a predictive model to assess the survival benefit of patients with MERC by calculating nomogram scores for each patient.
Results: Six variables were identified as independent prognostic factors and included in the nomogram: smoking history, family history, hematochezia, tumor size, N stage, and M stage. Based on these factors, we successfully constructed a nomogram and evaluated its discriminative and predictive abilities using ROC curves, calibration curves, and DCA. ROC curves, IDI, and NRI showed that the nomogram had outstanding clinical utility compared with the TNM staging system (8th edition) for OS prediction. The predictive model successfully distinguished between high-, medium-, and low-risk MERC patients.
Conclusion: Our nomogram provided a more satisfactory survival prediction ability than the TNM staging system (8th edition) for MERC patients. In addition, the nomogram was able to accurately categorize patients into different risk groups after surgery.
Keywords: nomogram, rectal cancer, web-based nomogram, overall survival, prognosis
Introduction
Colorectal cancer (CRC) is one of the most common malignant tumors of the gastrointestinal tract. According to global epidemiological oncology statistics published by the International Agency for Research on Cancer, it is estimated that there will be 1.93 million new cases of CRC and 940,000 CRC related deaths worldwide in 2020, ranking third and second among all types of malignancies, respectively.1 China has a large population and even if the incidence of CRC is lower than the global level, the number of new cases and CRC related deaths are the highest among all countries. Rectal cancer accounts for approximately 40% of all CRC cases and constitutes a severe global public health burden.2 Moreover, the number of patients with middle-aged and elderly rectal cancer (MERC) is expected to increase as the population ages.3–5 Surgery is the first treatment choice for rectal cancer; however, most MERC patients undergoing surgery have various comorbidities and typical age-related decline in essential physiological functions, which lead to poor postoperative prognosis in these patients.6 Therefore, identification of high-risk MERC patients for intervention is an important research direction for gastrointestinal surgeons.
Currently, the eighth edition of the tumor-node-metastasis (TNM) staging system of the American Joint Commission on Cancer, which is commonly used for rectal cancer staging, does not include important prognostic factors such as smoking history, family history, hematochezia, and tumor markers.7 Furthermore, there is heterogeneity in the postoperative situation of patients with the same TNM staging system, suggesting that this tool is limited in predicting prognosis and directing the clinical management of rectal cancer after surgery.8 In recent years, nomograms have been used widely in the fields of oncology and medicine, showing higher accuracy of prognostic prediction than the TNM staging system.9,10 In addition, the web-based nomogram, which is a dynamic nomogram, can elicit patient survival over a specified time period through precise numbers and visual graphics, guiding clinicians in optimizing clinical treatment plans and improving patients’ quality of life.11,12
The Affiliated Hospital of Chengde Medical University is one of the first medical institutions in Hebei Province, China, offering considerable resources for management of rectal cancer cases. More importantly, we were the first to create a nomogram for predicting MERC patients’ postoperative overall survival (OS), incorporating new clinical variables, such as smoking history, family history, tumor size, and hematochezia. The aim of the present study was to develop a web-based nomogram, which is more clinically guided and can be used online by both clinicians as well as patients to predict and evaluate the OS at 1, 2, and 3-year after surgery for MERC.
Patients and Methods
Patients
This study utilized the Affiliated Hospital of Chengde Medical University database to obtain the clinical data of MERC patients from 2013 to 2018. The inclusion criteria were: (I) patients with MERC aged ≥35 years, (II) pathological diagnosis of rectal adenocarcinoma, (III) access to primary rectal tumor resection, and (IV) availability of complete follow-up information. The exclusion criteria were: (I) patients with MERC aged <35 years, (II) non-primary rectal tumors, (III) physical intolerance to primary tumor resection, and (IV) incomplete follow-up information. Consistent with previous studies, this study used the TNM system for tumor staging.13,14 We randomly divided all included patients into training (70%) and validation (30%) cohorts. This study was approved by the Ethics Review Committee of the Affiliated Hospital of Chengde Medical University (permit number: LL2020397) and signed informed consent was obtained from all participants prior to study initiation. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Data Collection
Data pertaining to pathological and clinical patient variables such as age, sex, smoking history (yes or no), drinking history (yes or no), family history (yes or no), neoadjuvant therapy (yes or no), hypertension classification (normal, grade 1, grade 2, and grade 3), hematochezia (yes or no), tumor markers [carcinoembryonic antigen (CEA), and carbohydrate antigen 19–9 (CA 19–9)], tumor size, distance between the tumor and the dentate line, T stage (T1, T2, T3, and T4), N stage (N0, N1, and N2) and M stage (M0 and M1) were extracted from the Affiliated Hospital of Chengde Medical University database. Distance between the tumor and the dentate line was measured after intraoperative dilation of the anus under general anesthesia. In addition, hypertension grade was assigned as follows: normal hypertension was defined as a systolic blood pressure <140 mmHg or (and) diastolic blood pressure <90 mmHg, hypertension grade 1 was defined as the systolic blood pressure of 140–159 mmHg or (and) the diastolic blood pressure of 90–99 mmHg, hypertension grade 2 was defined as the systolic blood pressure of 160–179 mmHg or (and) the diastolic blood pressure of 100–109 mmHg, and hypertension grade 3 was defined as systolic blood pressure ≥ 180 mmHg or (and) diastolic blood pressure ≥110 mmHg. In this study, OS was the primary outcome of interest and it was calculated from the date of surgery to the date of death or the date of the last follow-up.
Construction and Validation of the Nomogram
Univariate Cox regression analysis was performed for all variables that may affect the postoperative OS of patients with MERC. Based on the results of the univariate Cox regression analysis, a multivariate Cox regression analysis was conducted, after controlling for confounding variables, to identify independent prognostic factors of MERC. Thereafter, a prognostic nomogram for OS was created according to the identified independent prognostic factors, using the “rms” package. Furthermore, receiver operating characteristic (ROC) curves, calibration curves, and decision curve analysis (DCA) curves were used to assess the predictive performance and accuracy of the nomogram. The net reclassification improvement (NRI), integrated discrimination improvement (IDI), and area under the ROC curves (AUC) were calculated to determine the overall improvement in the predictive accuracy by using the nomogram in place of the traditional TNM staging system (8th edition). Based on the X-tile program, we divided all patients into three groups: low-risk, medium-risk, and high-risk groups. We tested the prognostic value of the nomogram using the Kaplan–Meier (K–M) analysis. Finally, a web-based nomogram was created that conformed to the new nomogram. This predictive model allowed us to calculate nomogram scores for different patients with MERC and assess their postoperative survival benefit.
Statistical Analysis
We used the chi-square test and Fisher’s exact test to compare categorical data represented as frequencies and proportions. Variables significantly associated with OS were analyzed in the multivariate analysis using the Cox regression model to determine the independent predictive factors of OS, along with the corresponding 95% confidence intervals (CIs). Based on these independent predictors, we developed and created a new nomogram and a practical web-based nomogram. AUC was used to assess the prognostic accuracy of the nomogram and TNM staging system. Thereafter, calibration curves were assessed by plotting the relationship between the predicted and actual probabilities for each outcome. DCA demonstrated the clinical utility of the nomogram. In addition, we evaluated the net benefits of the nomogram and TNM staging system by using IDI and NRI. All statistical analyses were performed using R statistical software (version 4.1.1; R Foundation for Statistical Computing, Vienna, Austria). p-value <0.05 was considered to be statistically significant.
Results
Flowchart
A detailed workflow of the study is shown in Figure 1.
 |
Figure 1 Detailed workflow of study design and analysis. |
Patient Characteristics
A total of 349 postoperative patients with MERC were included in this study, of which 211 were men and the mean age of the participants was 60.70±10.09 years. Among the 349 patients, 245 (70.20%) were allocated to the training cohort. There were 133 (38.11%), 126 (36.10%), and 41 (11.75%) patients with a smoking, drinking, and family history, respectively. Patients receiving neoadjuvant therapy accounted for 58.74% of all patients (n=349). Hypertension was graded as normal hypertension, grade 1, grade 2, and grade 3 in 260 (74.50%), 64 (18.34%), 23 (6.59%), and 2 (0.57%) patients, respectively. Hematochezia before surgery was reported in 78 (22.35%) patients. The average tumor size was 5.28±1.91 cm. The average distance between the tumor and the dentate line was 6.18±3.47 cm. Elevated CEA and CA 19–9 levels were noted in 136 (38.97%) and 62 (17.77%) patients, respectively. There were 36 (10.32%) patients with T1–T2 stage and 313 (89.68%) patients with T3-T4 stage tumor. A total of 228 (65.33%), 74 (21.20%), and 47 (13.47%) patients had N0, N1, and N2 stage tumors, respectively. M0 stage disease was present in 316 (90.54%) patients, while 33 (9.46%) patients had M1 stage disease. The demographic and clinicopathological characteristics of the patients with MERC are shown in Table 1.
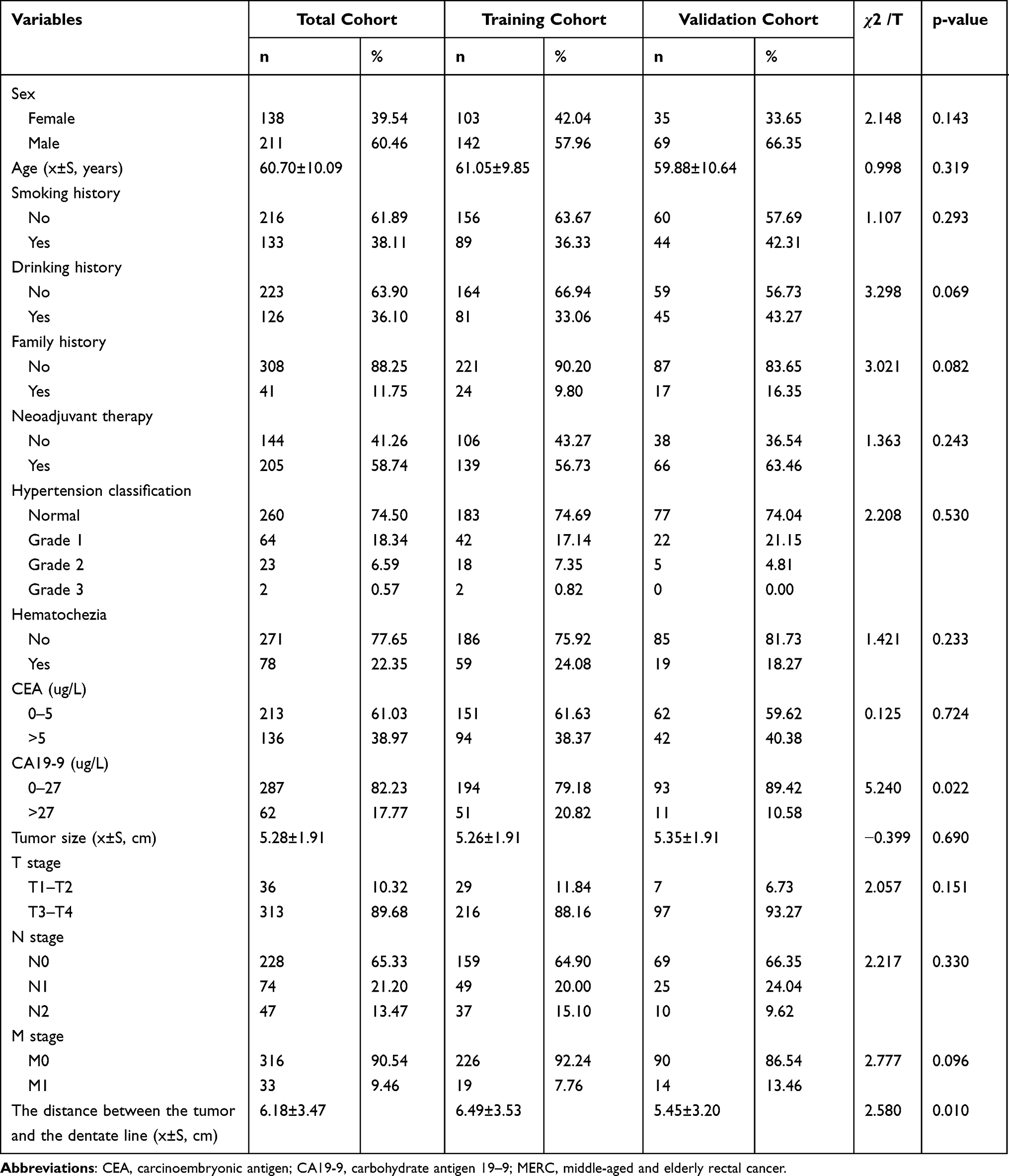 |
Table 1 Demographic and Clinicopathological Characteristics of Patients with MERC |
Prognostic Factors Influencing Postoperative Patient Survival
Univariate Cox regression analysis showed that smoking history, family history, hematochezia, CEA, CA 19–9, tumor size, N stage, and M stage were relevant prognostic factors for postoperative OS in patients with MERC. Multivariate Cox regression analysis showed that smoking history (Yes: hazard ratio (HR)=2.905, 95% CI=1.545–5.461, p-value=0.001; No as a reference), family history (Yes: HR=3.163, 95% CI=1.706–5.864, p-value<0.001; No as a reference), hematochezia (Yes: HR=0.316, 95% CI=0.135–0.739, p-value=0.008; No as a reference), tumor size (HR=1.331, 95% CI=1.145–1.546, p-value <0.001), N stage (N1: HR=1.920, 95% CI=1.003–3.674, p-value=0.049; N2: HR=2.238, 95% CI=1.132–4.425, p-value=0.020; N0 as a reference), M stage (M1: HR =15.795, 95% CI=7.69–32.439, p-value<0.001; M0 as a reference) were independent prognostic factors for postoperative OS in patients with MERC. The results of univariate and multivariate Cox regression analyses of survival in patients with MERC are summarized in Table 2.
 |
Table 2 Univarate and Multivariate Cox Regression Analyses of Survival in Patients with MERC |
Construction and Validation of the Nоmоgram
We created a novel nomogram based on the independent prognostic factors of OS mentioned above. As shown in Figure 2, the nomogram predicted the OS of patients with MERC at 1-, 2-, and 3-year after surgery. ROC curves were used to compare the accuracy of the predicted 1-, 2-, and 3-year OS rates. In the training cohort, the AUCs for the nomogram predicting 1-, 2-, and 3-year OS were 0.957, 0.945, and 0.918, respectively, whereas those for the TNM staging system were 0.840, 0.828, and 0.799, respectively (Figure 3A–C). In the validation cohort, the AUC of the nomogram predicting 1-year OS was not significantly different from that of the TNM staging system (Figure 3D). The nomogram predicting OS at 2-and 3-year showed a more satisfactory AUC than the TNM staging system (Figure 3E and F). Therefore, the new nomogram developed in this study was found to superior to the TNM staging system in terms of its discriminatory ability. The calibration curves yielded good agreement between the predicted and observed outcomes for the 1-, 2-, and 3-year OS (Figure 4). The DCA curves also showed good clinical utility of this nomogram (Figure 5). In addition, the K-M survival curves showed that the prediction model could accurately distinguish between the high-, medium-, and low-risk groups of MERC patients (Figure 6).
 |
Figure 2 Nomogram. Nomogram for predicting 1-, 2-, and 3-year OS in patients with MERC. Abbreviations: OS, overall survival; MERC, middle-aged and elderly rectal cancer. |
 |
Figure 3 ROC curves. ROC curves for predicting 1-year (A), 2-year (B), and 3-year (C) overall survival between the nomogram and TNM staging system in the training cohort; ROC curves for predicting 1-year (D), 2-year (E), and 3-year (F) overall survival between the nomogram and TNM staging system in the validation cohort. Abbreviation: ROC, receiver operating characteristic. |
 |
Figure 4 Calibration curves. Calibration curves of the nomogram for the 1-year (A), 2-year (B), and 3-year (C) OS prediction in the training cohort; 1-year (D), 2-year (E), and 3-year (F) OS prediction in the validation cohort. Abbreviation: OS, overall survival. |
 |
Figure 5 Decision curve analysis (DCA). DCA of the nomogram for predicting the 1-year, 2-year, and 3-year (A) OS in the training cohort; 1-year, 2-year, and 3-year (B) OS in the validation cohort. Abbreviations: DCA, decision curve analysis; OS, overall survival. |
 |
Figure 6 Kaplan-Meier curves. Kaplan-Meier curves of the low-, medium-, and high-risk groups in the training cohort (A) and validation cohort (B). |
Clinical Value of the Nomogram
The new nomogram showed superior clinical discrimination in the ROC curves analysis compared to the TNM staging system (8th edition). Most importantly, patients could benefit greatly due to the ability of the nomogram in predicting individual survival outcomes. In the IDI analyses, our new nomogram based on MERC patients, offered superior performance over the TNM staging system. In the training cohort, the IDI values for the 1-, 2-, and 3-year OS were 0.030 (p =0.166), 0.131 (p <0.001), and 0.123 (p <0.001), respectively. In the validation cohort, the IDI values for the 1-, 2-, and 3-year OS were 0.024 (p =0.349), 0.127 (p =0.019), and 0.121 (p =0.008), respectively. From the above results, it was inferred that there was no statistical difference between the new nomogram and the TNM staging system in terms of OS prediction in the first year. However, the predictive ability of the nomogram with respect to the 2- and 3-year OS was higher than that of the TNM staging system. In addition, the NRI values for 1-, 2-, and 3-year OS were 0.372 (95% CI=−0.083–0.819), 0.429 (95% CI=0.193–0.964), and 0.443 (95% CI=0.165–0.914) in the training cohort and 0.094 (95% CI=−0.857–1.045), 0.408 (95% CI=−0.094–1.091), and 0.149 (95% CI=−0.286–1.019) in the validation cohort, respectively.
Establishment of a Web-Based Nomogram
A dynamic web-based probability calculator (https://zhenghh.shinyapps.io/spprcc/) was constructed to predict the postoperative OS of patients with MERC based on the above results. The survival curves for a patient with MERC, who had smoking history, family history, no hematochezia, and a tumor size of 2 cm at N1 and M0 stages (Figure 7A) are shown in Figure 7B. Survival rates and 95% CI at 1-year (Figure 7C, black line), 2-year (Figure 7C, blue line) and 3-year (Figure 7C, red line) are also displayed on the operator interface. In addition, specific figures were summarized to improve predictive accuracy (Figure 7D).
 |
Figure 7 Web-based nomogram. Operation page of web-based nomogram (A), survival curve of a patient with MERC, who had smoking history, family history, no hematochezia, and a tumor size of 2 cm at N1 and M0 stages (B), Survival rates and 95% confidence intervals at 1-year (black line), 2-year (blue line), and 3-year (red line) (C), the prediction accuracy of the nomogram for the same patient (D). |
Discussion
The number of individuals with MERC continues to increase with a rise in the aging population worldwide. Patients with MERC often have atypical symptoms and most patients are diagnosed at an advanced stage of the disease. Moreover, even when surgery is feasible in MERC patients, the prognosis is significantly poorer compared to the younger patients with rectal cancer.15,16 Keeping this in mind, many researchers have focused on the role of neoadjuvant therapy in rectal cancer.17–19 However, only a few studies have evaluated postoperative survival in patients with MERC, and even fewer have developed prognostic nomograms to assess postoperative OS. In the present research, we were able to successfully develop and create the first nomogram for predicting the postoperative OS of patients with MERC using the Affiliated Hospital of Chengde Medical University database. By using this model, clinicians can accurately identify patients with poor prognosis after surgery and conduct a closer follow-up or start adjuvant treatment, if necessary. According to the results of AUC, NRI, and IDI analyses, the well-established nomogram seems to be more predictive than the TNM staging system, especially in the second and third years after surgery.
In contrast to the other similar studies, this study is first to include the clinical variables of smoking history and family history as independent risk factors in the survival prediction model.18,20 Previous studies have confirmed that smoking significantly affects survival in older people,21,22 and plays a more decisive role in rectal cancer than in colon cancer.23 Furthermore, the prognosis of colorectal cancer patients who smoke, even if they undergo surgery, is unfortunate, which is consistent with our findings.24,25 It has been proven that the prognosis of patients with a family history of colorectal cancer is worse than that of patients without a family history.26,27 We suspect that this is primarily attributable to genetic factors. A previous study reported that 6.7% of patients with rectal cancer had a family history of colorectal cancer.26 According to our nomogram, the presence or absence of smoking history and family history indicates that patients can receive different scores and display different 1-, 2-and 3-year OS rates, even if their tumors have the same TNM stage. The additive predictive power provided by these variables undoubtedly contributed to the superior power of the nomogram for predicting OS compared with the 8th edition of the TNM staging system.
In addition, there was a significant difference in postoperative OS between patients with and without hematochezia. Therefore, hematochezia appears to affect the survival rate of patients with MERC after surgery. In the early stages of rectal cancer, 80% of patients notice blood in the stool. Middle-aged and elderly patients need to be on high alert for the risk of rectal cancer if they develop unexplained symptoms of hematochezia. With the continuous improvement of people’s living standards and the gradual strengthening of health awareness, there has been an increase in the proportion of patients seeking early treatment for hematochezia.28 Moreover, the department of gastrointestinal oncology of our hospital is highly specialized, where gastroscopy or e-colonoscopy is frequently performed for investigating the cause of hematochezia. Early detection and prompt surgical treatment are keys to good prognosis in rectal cancer patients. In recent years, it has been found that high levels of CEA and CA 19–9 before surgery are closely related to the poor postoperative survival rate of colorectal cancer patients.29,30 In our study, tumor markers (CEA and CA 19–9) were not identified as independent prognostic factors in patients with MERC after surgery, even though the results of the univariate analysis showed significance. A larger study cohort may be needed to confirm the role of these two factors in postoperative OS of MERC patients. Moreover, the role of these oncological indicators in supporting colorectal cancer screening and diagnosis is still controversial.29–32 In summary, we did not include tumor markers (CEA and CA 19–9) in the nomogram, taking into account previous clinical studies and statistical results of the present study.
It is known that the depth of tumor invasion determines the T stage of the tumor and affects adjuvant treatment strategy as well as the postoperative prognosis of a cancer patient.33 The present study revealed an interesting phenomenon; the classical T stage of the TNM staging system (8th edition) failed to show independent predictive significance in overall patient survival, and tumor size was proven to be an independent predictor in OS analysis. These results are similar to those reported previously.34,35 Previous studies have analyzed tumor size according to an optimal threshold for tumor size;36 however, we insisted on adopting a continuous variable to describe tumor size. As an essential risk factor for tumor progression, the larger the tumor, the higher is the possibility of invading blood vessels and lymphatic channels.36 Therefore, it is essential to consider the impact of tumor size on postoperative OS. Further precision can be achieved using our predictive model to determine exactly how the patient’s postoperative OS rate decreases as the tumor size increases. In this sense, tumor size can be considered as a better predictor of OS than the depth of tumor invasion; larger the tumor volume, lower will be the postoperative OS.
Besides the above stated factors, the N and M stages of the TNM staging system were identified as significant predictors of survival in MERC patients, a finding that was consistent with several previous reports.37–40 Studies have shown that the surgical margin status of rectal cancer significantly impacts patient survival. To estimate survival more accurately, all patients included in this study underwent radical resection, and the effect of resection margins on survival was found to be minimal. Therefore, in the nomogram, each factor derived from the multivariate Cox proportional hazards regression model was attributed to the total number of weighted points, implying survival prognosis. This established nomogram will make it easier for physicians to assess various patient and tumor parameters with enhanced objectivity and precision, and to distinguish MERC patients after radical resection into subgroups with different prognoses. As we see, there can be two primary applications of this nomogram. First, as a quantitative scoring system, the nomogram can predict the survival of patients with MERC. Second, for patients with high scores calculated using the established nomogram, close follow-up or appropriate treatment may be required. Combining the main elements from the TNM staging system and other tumor-associated indices, including smoking history, family history, hematochezia, and tumor size, would contribute towards improved discriminatory power of the nomogram in predicting survival. The nomogram established in our present research can be utilized as a practical tool to predict clinical disease outcomes and has potential applicability in the follow-up treatment decision making of postoperative patients with MERC.
This study has some limitations that need to be addressed. First, this was a retrospective study that relied on the database of a single research center in China. Further verification of our results using an extensive, comprehensive, and scientific multicenter database is required. Second, despite the establishment of strict standards for inclusion and exclusion, statistical deviations were inevitable.
Conclusions
Based on the Affiliated Hospital of Chengde Medical University database, a new nomogram was established for the first time to predict the OS of patients with MERC at 1, 2, and 3-year after surgery. This model can provide more accurate predictive power and clinical benefits than the TNM staging system (8th edition) and guide clinicians in optimizing treatment plans for MERC cases.
Abbreviations
CRC, colorectal cancer; MERC, middle-aged and elderly rectal cancer; OS, overall survival; ROC, receiver operating characteristic; DCA, decision curve analysis; IDI, integrated discrimination improvement; NRI, net reclassification improvement; AUC, area under the curve; TNM, tumor-node-metastasis; K–M, Kaplan–Meier; CEA, carcinoembryonic antigen; CA 19-9, carbohydrate antigen 199; CI, confidence interval; HR, hazard ratio.
Data Sharing Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Approval and Informed Consent
This study was approved by the Ethics Review Committee of the Affiliated Hospital of Chengde Medical University (permit number: LL2020397), and signed informed consent was obtained from all participants prior to study initiation.
Acknowledgments
The authors are grateful for the invaluable support and useful discussions with other members of the general surgery department.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study is funded by the 2020 Hebei Provincial Finance Department Grant for Outstanding Talents in Clinical Medicine (No. 2020397).
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Sung H, Ferlay J, Siegel RL. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Feng RM, Zong YN, Cao SM, et al. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. 2019;39(1):22. doi:10.1186/s40880-019-0368-6
4. Kim JY, Jang ES, Park SY, et al. Distinct characteristics of colorectal cancer and frequency of right colon cancer in elderly patients of Korea. J Korean Geriatr Soc. 2010;14(3):147. doi:10.4235/jkgs.2010.14.3.147
5. Claassen Y, Vermeer N, Iversen LH, et al. Treatment and survival of rectal cancer patients over the age of 80 years: a EURECCA international comparison. Br J Cancer. 2018;4(119):517–522. doi:10.1038/s41416-018-0215-6
6. Sarfati D, Koczwara B, Jackson C. The impact of comorbidity on cancer and its treatment. Cancer J Clin. 2016;66(4):337–350. doi:10.3322/caac.21342
7. Austin AM, Kapadia NS, Brooks GA, et al. Comparison of treatment of early-stage breast cancer among Nurses’ Health Study participants and other Medicare beneficiaries. Breast Cancer Res Treat. 2019;174(3):759–767. doi:10.1007/s10549-018-05098-4
8. Lin KY, Tai C, Hsu JC, et al. Overexpression of nuclear protein kinase CK2 alpha catalytic subunit (CK2alpha) as a poor prognosticator in human colorectal cancer. PLoS One. 2011;6(2):e17193. doi:10.1371/journal.pone.0017193
9. Guo Q, Peng YY, Yang H, et al. Prognostic nomogram for postoperative patients with gastroesophageal junction cancer of no distant metastasis. Front Oncol. 2021;11:643261. doi:10.3389/fonc.2021.643261
10. Li Z, Wei J, Gan X, et al. Construction, validation and, visualization of a web-based nomogram for predicting the overall survival and cancer-specific survival of leiomyosarcoma patients with lung metastasis. J Thorac Dis. 2021;13(5):3076–3092. doi:10.21037/jtd-21-598
11. Wang HH, Dai KN, Li AB, Nomogram Predicting A. Overall and cancer-specific survival of patients with primary bone lymphoma: a large population-based study. Biomed Res Int. 2020;2020(4):4235939. doi:10.1155/2020/4235939
12. Battersby NJ, Bouliotis G, Emmertsen KJ, et al. Development and external validation of a nomogram and online tool to predict bowel dysfunction following restorative rectal cancer resection: the POLARS score. Gut. 2018;67(4):688–696. doi:10.1136/gutjnl-2016-312695
13. Lu J, Zheng ZF, Xie JW, et al. Is the 8th edition of the AJCC TNM staging system sufficiently reasonable for all patients with noncardia gastric cancer? A 12,549-patient international database study. Ann Surg Oncol. 2018;25(7):2002–2011. doi:10.1245/s10434-018-6447-0
14. Sl A, Mc A, Gm A, et al. Topographic lymph node staging system shows prognostic superiority compared to the 8th edition of AJCC TNM in gastric cancer A western monocentric experience. Surg Oncol. 2020;34:223–233.
15. Rutten H, Dulk MD, Lemmens V, et al. Survival of elderly rectal cancer patients not improved: analysis of population based data on the impact of TME surgery. Eur J Cancer. 2007;43(15):2295–2300. doi:10.1016/j.ejca.2007.07.009
16. Liu L, Cao Y, Zhang G, Zhang L, Wang P, Gong J. Long-term outcomes after laparoscopic total mesorectal excision for advanced rectal cancer. South African journal of surgery. Suid Afrikaanse tydskrif vir chirurgie. 2011;49(4):186–189.
17. Wei FZ, Mei SW, Chen JN, et al. Nomograms and risk score models for predicting survival in rectal cancer patients with neoadjuvant therapy. World J Gastroenterol. 2020;26(42):6638–6657. doi:10.3748/wjg.v26.i42.6638
18. Song J, Chen Z, Huang D, et al. Nomogram predicting overall survival of resected locally advanced rectal cancer patients with neoadjuvant chemoradiotherapy. Cancer Manag Res. 2020;12:7375–7382. doi:10.2147/CMAR.S255981
19. Zhang Y, Yan L, Wu Y, et al. Worse treatment response to neoadjuvant chemoradiotherapy in young patients with locally advanced rectal cancer. BMC Cancer. 2020;20(1):854. doi:10.1186/s12885-020-07359-2
20. Liu LL, Sun JD, Xiang ZL. A nomogram to predict the prognosis of patients with unresected rectal adenocarcinoma undergoing chemoradiotherapy: a population-based study. J Cancer. 2021;12(16):4745–4761. doi:10.7150/jca.61642
21. Phipps A, Baron J, Newcomb P. Prediagnostic smoking history, alcohol consumption, and colorectal cancer survival: the Seattle Colon cancer family registry. Cancer. 2011;117(21):4948–4957. doi:10.1002/cncr.26114
22. Zhu Y, Yang SR, Wang PP, et al. Influence of pre-diagnostic cigarette smoking on colorectal cancer survival: overall and by tumour molecular phenotype. Br J Cancer. 2014;110(5):1359–1366. doi:10.1038/bjc.2014.6
23. Liang PS, Chen TY, Giovannucci E. Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer. 2010;124(10):2406–2415. doi:10.1002/ijc.24191
24. Nickelsen T, Jørgensen T, Kronborg O, et al. Lifestyle and 30-day complications to surgery for colorectal cancer. Acta Oncologica. 2005;44(3):218–223. doi:10.1080/02841860510029707
25. Walter V, Jansen L, Hoffmeister M, et al. Smoking and survival of colorectal cancer patients: systematic review and meta-analysis. Ann Oncol. 2014;25(8):1517–1525. doi:10.1093/annonc/mdu040
26. Deo S, Kumar S, Bhoriwal S, et al. Colorectal cancers in low- and middle-income countries-demographic pattern and clinical profile of 970 patients treated at a tertiary care cancer center in India. JCO Glob Oncol. 2021;7:1110–1115. doi:10.1200/GO.21.00111
27. Jennifer A. Association of family history with cancer recurrence and survival among patients with stage III colon cancer. JAMA. 2008;299(21):2515. doi:10.1001/jama.299.21.2515
28. Tong GX, Chai J, Cheng J, et al. Diagnostic value of rectal bleeding in predicting colorectal cancer: a systematic review. Asian Pac J Cancer Prev. 2014;15(2):1015–1021. doi:10.7314/APJCP.2014.15.2.1015
29. Kim CG, Ahn JB, Jung M, et al. Preoperative serum carcinoembryonic antigen level as a prognostic factor for recurrence and survival after curative resection followed by adjuvant chemotherapy in stage III colon cancer. Ann Surg Oncol. 2017;24(1):227–235. doi:10.1245/s10434-016-5613-5
30. Shin JK, Kim HC, Lee WY, et al. High preoperative serum CA 19-9 levels can predict poor oncologic outcomes in colorectal cancer patients on propensity score analysis. Ann Surg Treat Res. 2019;96(3):107–115. doi:10.4174/astr.2019.96.3.107
31. Morita S, Nomura T, Fukushima Y, Morimoto T, Hiraoka N, Shibata N. Does serum CA19-9 play a practical role in the management of patients with colorectal cancer? Dis Colon Rectum. 2004;47(2):227–232. doi:10.1007/s10350-003-0041-6
32. Katoh H, Yamashita K, Kokuba Y. Diminishing impact of preoperative carcinoembryonic antigen (CEA) in prognosis of Dukes’ C colorectal cancer. Anticancer Res. 2008;28:1933–1941.
33. Wei J, Huang R, Guo S. ypTNM category combined with AJCC tumor regression grade for screening patients with the worst prognosis after neoadjuvant chemoradiation therapy for locally advanced rectal cancer. Cancer Manag Res. 2018;10:5219–5225. doi:10.2147/CMAR.S179151
34. Chen C, Hsieh M, Hsiao P, et al. A critical reappraisal for the value of tumor size as a prognostic variable in rectal adenocarcinoma. J Cancer. 2017;8(10):1927–1934. doi:10.7150/jca.17930
35. P Kornprat, MJ Pollheimer, RA Lindtner, et al. Value of tumor size as a prognostic variable in colorectal cancer: a critical reappraisal. Am J Clin Oncol. 2011;34(1):43–49. doi:10.1097/COC.0b013e3181cae8dd
36. Liang Y, Li Q, He D, Chen Y, Li J. Tumor size improves the accuracy of the prognostic prediction of T4a stage colon cancer. Sci Rep. 2021;11(1):16264. doi:10.1038/s41598-021-95828-4
37. Numata M, Yamaguchi T, Kinugasa Y, et al. Index of estimated benefit from lateral lymph node dissection for middle and lower rectal cancer. Anticancer Res. 2017;37(5):2549–2555. doi:10.21873/anticanres.11598
38. Yang J, Chen Q, Li J, et al. Short-term clinical and oncological outcome of prolonging operation interval after neoadjuvant chemoradiotherapy for locally advanced middle and low rectal cancer. Cancer Manag Res. 2020;12:2315–2325. doi:10.2147/CMAR.S245794
39. Ding L, Liu GW, Zhao BC, et al. Artificial intelligence system of faster region-based convolutional neural network surpassing senior radiologists in evaluation of metastatic lymph nodes of rectal cancer. Chin Med J. 2019;132(4):379–387. doi:10.1097/CM9.0000000000000095
40. Benedek Z, Boer ST, Bauer O, et al. An overview of five-year survival in rectal cancer in relation to lymph node status. Chirurgia. 2020;115(6):747–755. doi:10.21614/chirurgia.115.6.747
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.