Back to Journals » Patient Preference and Adherence » Volume 20
A Network Analysis of Social Integration and Subjective Well-Being in Young and Middle-Aged Lymphoma Patients
Authors Zhang L ![]() , Wu Y, Zhang Y, Xu C, Zhu W
, Wu Y, Zhang Y, Xu C, Zhu W ![]()
Received 5 January 2026
Accepted for publication 24 March 2026
Published 18 April 2026 Volume 2026:20 593724
DOI https://doi.org/10.2147/PPA.S593724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Li Zhang,1 Yaru Wu,1 Yuting Zhang,1 Chunyan Xu,2,3 Wei Zhu3,4
1School of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Department of Gynecologic Surgery, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 3Health Care Research Center for Xinjiang Regional Population, Urumqi, Xinjiang, People’s Republic of China; 4Department of Lymphoma, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Wei Zhu, Department of Lymphoma, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China, Email [email protected]
Objective: To explore the network relationships between social integration and subjective well-being (SWB) and to identify key nodes within this network among young and middle-aged lymphoma patients.
Methods: This study was conducted at a tertiary cancer hospital in Urumqi, Xinjiang, China. From February to November 2025, a total of 315 young and middle-aged lymphoma patients were recruited using convenience sampling. Data were collected via a general information questionnaire, the Social Cohesion Scale, and the General Well-Being Schedule. We used network analysis to identify core and bridge nodes in the social integration and SWB network. A network comparison test (NCT) was performed to examine potential gender differences.
Results: The network analysis revealed that “Daily integration” demonstrated the strongest edge weight with “Relaxed or tense”. In terms of node centrality, “Depressed or happy mood” and “Daily integration” emerged as the core nodes with the highest strength centrality, while “Daily integration” and “Intimate integration” were identified as the pivotal bridge nodes connecting different network clusters. No gender differences were observed in the association network between social integration and SWB.
Conclusion: This study explores the network associations between social integration and SWB in young and middle-aged lymphoma patients. The findings suggest that intervention strategies may focus on improving emotional regulation, daily social interaction, and intimate relationships to enhance social integration and SWB in this population. Given the heterogeneity in clinical characteristics among lymphoma patients, future studies are warranted to validate the present findings across different subtypes and treatment backgrounds.
Keywords: young and middle-aged lymphoma patients, social integration, subjective well-being, network analysis
Introduction
According to 2022 data, there were approximately 85,200 new lymphoma cases in China.1 Lymphoma exhibits a trend toward younger onset worldwide, with patients aged 18–59 accounting for about 64% of global cases; in China, this proportion reaches as high as 78%.2 Meanwhile, continuous advances in diagnosis and treatment have gradually improved the five-year survival rate. Accordingly, the focus for patients has shifted from survival prolongation alone to social reintegration and enhanced quality of life.3
Social integration refers to the process whereby individuals achieve equal participation, mutual acceptance, and full inclusion within a social system.4 Young and middle-aged adults are at a pivotal stage for academic progression, career development, family establishment, and life goal pursuit. A diagnosis of lymphoma frequently disrupts their educational and vocational pathways, interrupts pre-existing life plans, and leads to impaired social role functioning,5,6 which severely compromises their social integration. Studies have demonstrated that poor social integration predicts a significantly increased risk of all-cause mortality.7 By contrast, favorable social integration is linked to enhanced physical functioning and activity,8 as well as alleviated depressive symptoms.9 Notably, social integration is critical in helping young cancer patients rebuild a sense of meaning in life.10 Thus, for young and middle-aged patients with lymphoma, social integration is not only vital for post-recovery social adaptation but also fundamental to fulfilling their core life developmental tasks.
Subjective well-being (SWB) is a core psychological indicator for measuring quality of life, encompassing mainly emotional balance (positive and negative emotions) and life satisfaction.11 Studies consistently show that cancer patients exhibit lower levels of SWB than healthy populations,12,13 and this pattern is particularly evident in young and middle-aged lymphoma patients, who report significantly reduced life satisfaction.14 Furthermore, a systematic review indicated that young patients with lymphoma experience substantial impairments in multiple dimensions of SWB and quality of life throughout diagnosis, treatment, and survivorship.15 Notably, SWB can influence health outcomes through four interrelated pathways: regulating stress hormones and immune-inflammatory responses, encouraging healthy behaviors, expanding social support networks, and enhancing psychological resilience. Together, these mechanisms reduce the risk of disease progression through both physical and psychological pathways.16 Therefore, improving SWB should be considered a key target for rehabilitation interventions among young and middle-aged lymphoma patients, as it may improve both disease prognosis and overall quality of life.
Social integration is a key psychosocial determinant of SWB, and this association has been confirmed across diverse populations, including migrant groups and older migrant workers.17,18 In oncology settings, robust social integration is strongly associated with higher levels of SWB and better mental health outcomes among cancer patients,19,20 and has also been shown to significantly improve SWB in patients undergoing chemotherapy.21 However, no targeted studies have yet investigated the relationship between social integration and SWB specifically in lymphoma patients. Moreover, the specific mechanisms through which social integration influences SWB remain unclear among young and middle-aged lymphoma patients, who face unique challenges related to their life stage and disease characteristics.
Previous studies22,23 have mostly used traditional statistical methods (eg, regression models, correlation analyses) to explore the association between social integration and SWB in patient populations As an emerging statistical approach, network analysis conceptualizes complex social and psychological phenomena as interconnected systems composed of interrelated variables. Using centrality indices, this method identifies the most influential components: core nodes, which have the greatest number and strength of connections to other variables, represent the core of the network structure and serve as key intervention targets; bridge nodes link different variable clusters, allowing for more precise and targeted interventions. This study applied network analysis to explore the relationship between social integration and SWB among young and middle-aged lymphoma patients, aiming to identify core and bridge nodes and clarify key interaction pathways. Identifying these central nodes will provide actionable targets for clinical psychosocial interventions, helping to develop tailored strategies for improving social integration and SWB in this population.
Methods
Study Design and Participants
This was a cross-sectional network analysis. Young and middle-aged patients with lymphoma were enrolled between February 2025 and November 2025 at a tertiary cancer hospital in Urumqi, Xinjiang. The inclusion criteria for participants were as follows: (1) pathologically confirmed lymphoma; (2) aged 18–59 years; (3) achieved partial or complete remission; (4) conscious and able to communicate effectively; and (5) provided voluntary written informed consent. The exclusion criteria were as follows: (1) history of other malignant tumors or severe comorbidities; (2) diagnosed psychiatric disorders; and (3) inability to perform basic self-care.
Sample Size
In network analysis, the number of parameters includes both node-level variables and pairwise associations calculated as [N(N−1)/2].24 With 8 nodes in this study, there were 8 node parameters and 28 pairwise association parameters, yielding a total of 36 parameters to be estimated. Assuming 3–5 participants per parameter and an anticipated 20% invalid response rate, the minimum required sample size was calculated to be 135. Ultimately, 315 valid questionnaires were collected, which adequately met the sample size requirement.
Measures
General Information Questionnaire
After a literature review, the researchers developed a dedicated study questionnaire, which collected demographic data including but not limited to gender, age, and marital status, as well as disease-related information such as tumor type, clinical stage, treatment modality, and disease duration.
Social Cohesion Scale (SCS)
The Social Cohesion Scale used in this study was adapted from the Neighborhood Cohesion Scale revised by Fone et al25 It was later translated and validated in the Chinese population by Han et al26 The scale comprises two dimensions and eight items, rated on a 5-point Likert scale (1 = “Strongly disagree” to 5 = “Strongly agree”). Total scores range from 8 to 40, with higher scores indicating better perceived social integration. In the present study, this scale demonstrated good internal consistency, with a Cronbach’s α of 0.845.
General Well-Being Schedule (GWBS)
The General Well‑Being Schedule used in this study was originally developed by the U.S. National Center for Health Statistics27 and later adapted and validated for the Chinese population by Duan.28 It has been widely used in health-related research, including studies on chronic diseases. The scale comprises 18 items across six dimensions. Total scores range from 14 to 120, with higher scores indicating better SWB. In the present sample, the scale demonstrated excellent internal consistency, with a Cronbach’s α of 0.920.
Data Collection
After rigorous screening according to the inclusion and exclusion criteria, eligible patients were invited to participate in this study. Researchers provided a detailed explanation of the study purpose and procedures, emphasizing that participants could withdraw at any time, and then obtained written informed consent. Disease-related information was uniformly extracted from electronic medical records by the research team. Subsequently, participants completed the self-administered questionnaire independently. For those who had difficulty completing the questionnaire, researchers assisted with specific items only with the patient’s explicit consent and on-site verification to ensure accuracy. A researcher was present throughout the process to provide clarification. All questionnaires were collected and checked for completeness on site. Incomplete questionnaires or those with logically inconsistent responses were excluded to ensure data quality. A total of 330 questionnaires were distributed, and 315 valid questionnaires were recovered, yielding a valid response rate of 95.45%.
Data Analysis
First, the Extended Bayesian Information Criterion (EBIC) was used to select optimal regularization parameters. The graphical lasso (glasso) method was applied to construct a Gaussian graphical model (GGM) network linking social integration and SWB, which enhanced both network sparsity and interpretability. In the analysis, each dimension of social integration and SWB was treated as a node, and each pairwise association between nodes was defined as an edge. Thicker edges indicated stronger correlations between nodes, while thinner edges represented weaker correlations; green and red edges denoted positive and negative correlations, respectively.
Subsequently, to assess the importance of nodes within the network, centrality indices were calculated using two primary metrics: strength centrality and bridge strength, which were used to identify core nodes and bridge nodes, respectively. For comparative and visualization purposes, the numerical values of node strength and bridge strength were standardized via Z-score transformation. The top two nodes in terms of strength were designated as core nodes; bridge nodes were screened using the 80th percentile threshold of bridge strength scores.
To validate the reliability and stability of the network, the accuracy of edge weights was evaluated using a 95% bootstrap confidence interval (CI), where a narrower CI indicated higher precision in edge weight estimation. Meanwhile, network stability was quantified using the correlation stability coefficient (CS-C), with a CS-C value > 0.5 indicating optimal stability.
Finally, to compare gender-based differences in the social integration and SWB networks, network structure tests, global strength tests, and edge invariance tests were conducted sequentially. The Holm-Bonferroni correction was applied to perform multiple comparisons on the strength of each edge between the two networks, effectively controlling Type I errors arising from multiple testing. All network analyses were performed using R software (version 4.5.2). The packages used included “ggplot2”, “qgraph”, “bootnet”, “networktools”, “mgm”, and “NetworkComparisonTest”.
Results
General Demographic Variables of Participants
The sample comprised 63.8% males and 62.9% individuals aged 45–59 years. The majority were married (89.8%) and had non-Hodgkin lymphoma (96.5%). Regarding treatment, 95.6% received chemotherapy with or without targeted therapy (Table 1).
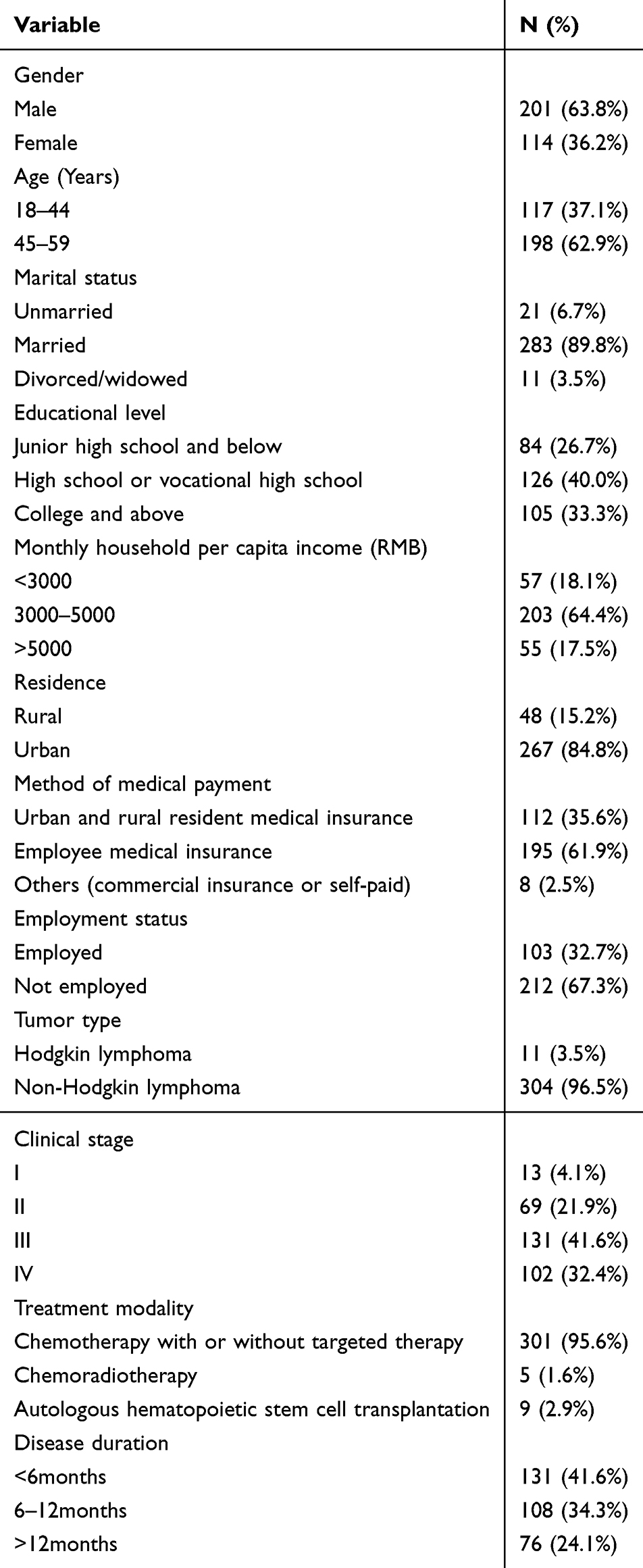 |
Table 1 Patient Demographic Characteristics (N=315) |
Network Structure, Central Nodes, and Bridge Nodes Associated with Social Integration and SWB
The network structure of social integration and SWB is illustrated in Figure 1A. Node predictability values ranged from 48.6% to 85.7% (Table 2). A total of 28 edges were estimated, of which 21 (75.0%) were non-zero and all were positive. Node strength and bridge strength are presented in Figure 1B. The results showed that “Depressed or happy mood” (SWB3, strength = 1.925) and “Daily integration” (SI1, strength = 1.100) were the two core nodes in the network. The bridge nodes were “Daily integration” (SI1, bridge strength = 1.897) and “Intimate integration” (SI2, bridge strength = 0.928).
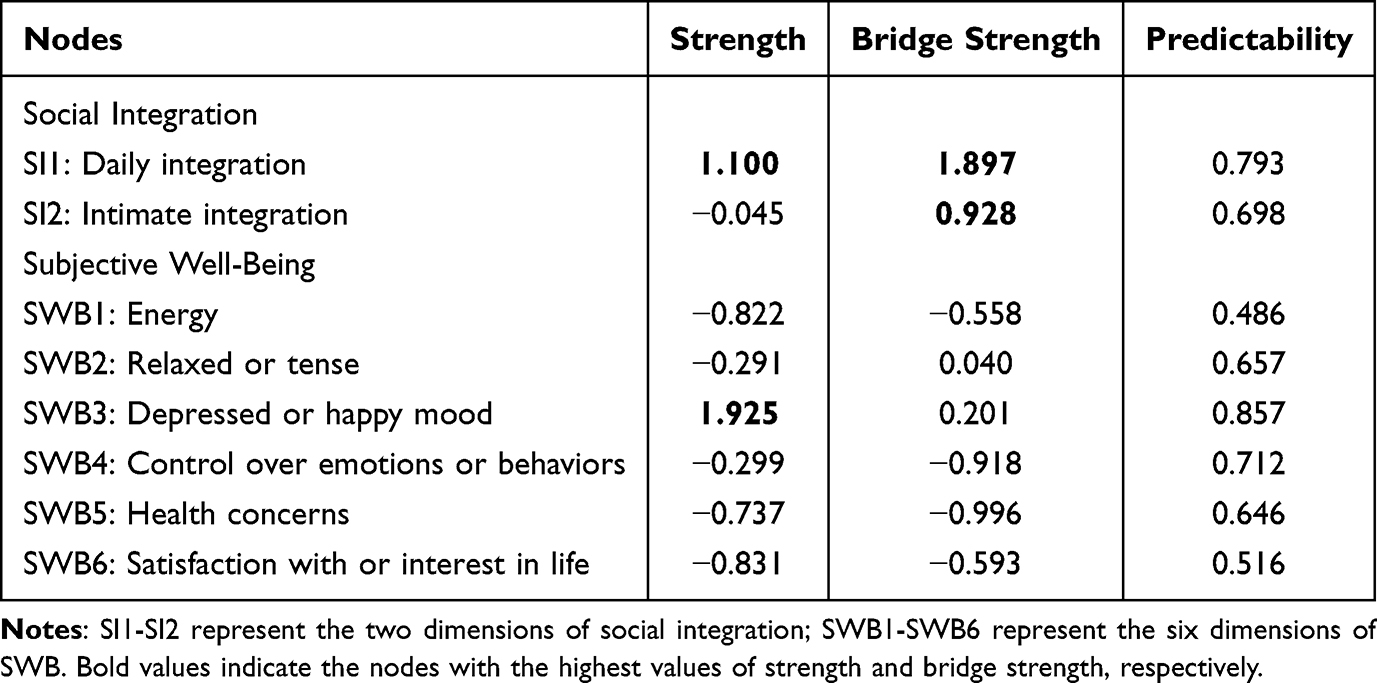 |
Table 2 Strength of All Nodes, Bridge Strength, and Predictability (N=315) |
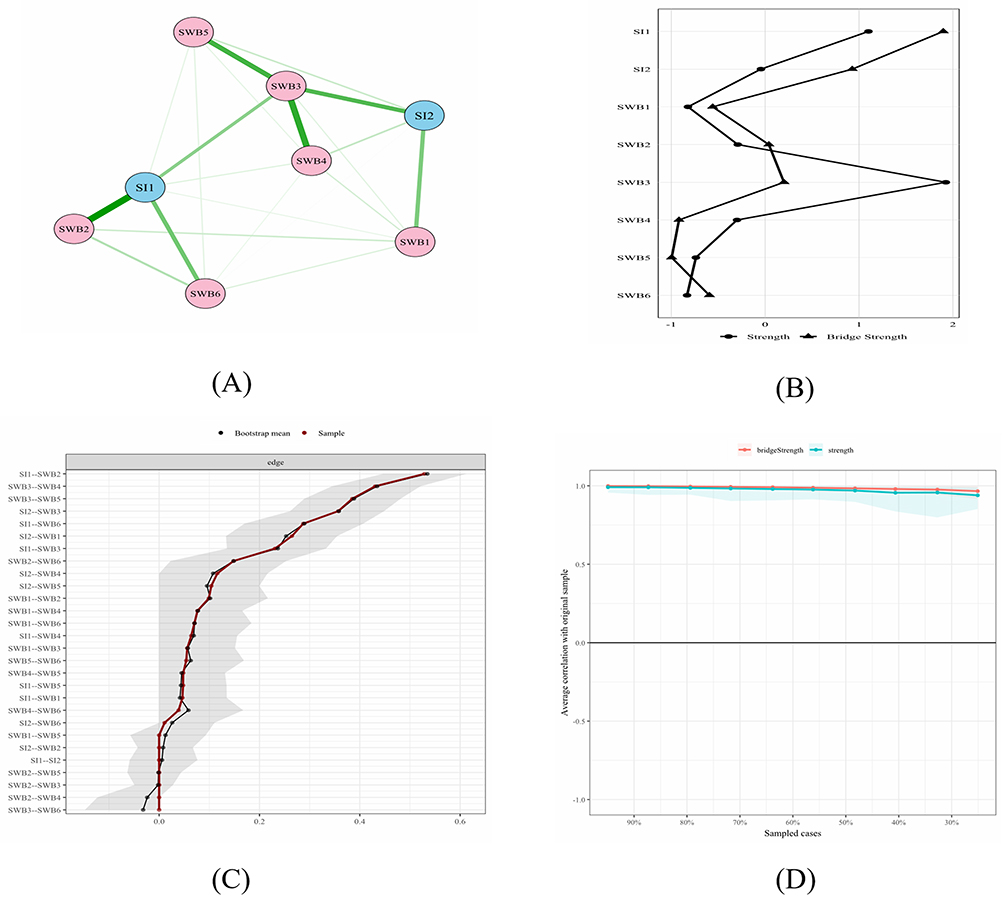 |
Figure 1 Network analysis of social integration and subjective well-being in young and middle-aged lymphoma patients. (A) Network structure of social integration and subjective well-being. (B) Node strength and bridge strength of all nodes. (C) Edge weight stability via bootstrap resampling. (D) Case-dropping stability test for node strength and bridge strength. Notes: SI1: Daily integration, SI2: Intimate integration; SWB1: Energy, SWB2: Relaxed or tense, SWB3: Depressed or happy mood, SWB4: Control over emotions or behaviors, SWB5: Health concerns, SWB6: Satisfaction with or interest in life. |
Accuracy and Stability of the Estimated Social Integration and SWB Network
The accuracy of edge weight estimation was supported by narrow 95% nonparametric bootstrap confidence intervals (Figure 1C). Furthermore, the network demonstrated excellent stability: the correlation stability coefficient (CS-C) for both strength and bridge strength was 0.749 (Figure 1D), exceeding the recommended threshold of 0.5 and confirming the robustness of the node centrality rankings.
Comparative Analysis of Social Integration and SWB Networks Based on Gender Grouping
A network comparison of social integration and SWB across gender groups revealed no significant differences in overall network structure (structure test: M = 0.205, P= 0.497). Similarly, there was no statistically significant difference in network global strength (Males = 3.538, Females = 3.338, S = 0.199, P= 0.334). All edge invariance tests yielded P > 0.05 after Benjamini-Hochberg (BH) correction, indicating no significant between-group differences. The gender-specific network structures are presented in the Supplementary Materials. Specifically, the network for male patients is shown in Supplementary Figure 1, and that for female patients in Supplementary Figure 2.
Discussion
To our knowledge, this study is the first to apply network analysis to investigate the association between social integration and SWB among young and middle-aged lymphoma patients, providing a novel perspective for elucidating the underlying mechanisms. Unlike previous research that focused on the overall relationship between total social integration scores and SWB, this study used network analysis to explore their interactive patterns and influence pathways. The results indicate that “Depressed or happy mood” (SWB3) and “Daily integration” (SI1) are core nodes that may serve as pivotal links between social integration and SWB. In addition, “Daily integration” (SI1) and “Intimate integration” (SI2) were identified as bridge nodes in the network. These findings suggest that targeted interventions on these key nodes have important practical implications for improving social integration and SWB in this population.
Network Characteristics of Social Integration and SWB
Within the estimated network, the strongest edge emerged between “Daily integration” (SI1) and “Relaxed or tense” (SWB2). This indicates that, for young and middle-aged lymphoma patients, their level of engagement in routine social activities is most directly and strongly associated with daily emotional regulation, specifically the ability to manage tension and achieve relaxation. This finding is consistent with previous studies suggesting that structured daily routines and social participation can buffer against anxiety, thereby improving well-being in younger individuals.29 Lymphoma patients often endure psychological and physical stress due to prolonged hospitalization, treatment-related isolation, and side effects, which may trigger anxiety.30 Routine social activities can enhance a sense of autonomy and effectively relieve psychological tension in patients.31 Furthermore, strong daily social connections reduce salivary amylase and cortisol secretion, directly weakening psychophysiological stress responses and alleviating tension.32 In the current network of social integration and SWB, the connection between “Depressed or happy mood” (SWB3) and “Control over emotions or behaviors” (SWB4) ranked second in strength. This finding suggests a close association between young and middle-aged lymphoma patients’ hedonic mood status and their ability to control emotions and behaviors. According to the broaden-and-build theory, positive affect broadens individuals’ attention and cognitive flexibility, thereby increasing the psychological resources available for regulating emotions and behaviors.33 Moreover, individuals with stronger control abilities tend to implement spontaneous emotion regulation, accompanied by significantly enhanced neural activity in both the executive control network and the emotion regulation network of the brain.34 Therefore, healthcare professionals should develop targeted interventions to help young and middle-aged lymphoma patients improve their daily social integration, emotional regulation, and self-control to promote their mental health.
Core Nodes in Social Integration and SWB Networks
Two core nodes were identified in the association between social integration and SWB: “Depressed or happy mood” (SWB3) and “Daily integration” (SI1). Among them, “Depressed or happy mood” (SWB3) was the most central node, suggesting that improving this node would most likely spread positive effects throughout the network of social integration and SWB via its connections with other nodes. On the one hand, depressed mood amplifies the distress caused by the disease and directly reduces patients’ SWB.35 On the other hand, depression weakens patients’ willingness to participate socially. For example, patients may reduce contact with relatives and friends, avoid peer support activities, and be reluctant to return to work or study,36 thereby lowering their level of social integration. A longitudinal study of prostate cancer survivors showed that patients’ level of depression was significantly associated with both social integration and SWB. Specifically, patients with higher social integration exhibited lower depression and higher SWB.37 Therefore, psychological interventions such as cognitive behavioral therapy (CBT) and mindfulness-based stress reduction (MBSR) could be implemented to target this core node. By alleviating depression, such interventions may simultaneously improve mental well-being and social integration.
“Daily integration” (SI1) was identified as another core node in this study, suggesting that it also plays an important role in the network of social integration and SWB. The present findings are consistent with a previous review,38 which indicated that sustained social interaction and regular participation in daily activities can help patients rebuild social roles and enhance self-worth, thus constituting an important pathway to achieving social integration. Treatment-related fatigue may easily lead to daily social withdrawal and reduced activity among young and middle-aged lymphoma patients, thereby hindering their social integration.39 In contrast, daily community interaction can help patients reconstruct diverse social identities, promote self-acceptance and reduce stigma,40 and ultimately improve SWB.41 Curtin et al20 also reported that regular engagement in daily life activities promotes social integration and favorable SWB in cancer patients. Therefore, healthcare professionals should emphasize daily integration in this population and implement targeted strategies to strengthen daily social participation and engagement, thereby improving patients’ overall social integration and SWB. Specifically, structured social participation guidance and personalized social skill-building programs can be provided to help patients master effective social communication skills, create a low-pressure social environment, alleviate disease-related anxiety, and promote self-acceptance, ultimately enhancing patients’ daily social integration and SWB.
Bridging Nodes in Social Integration and SWB Networks
Two critical bridge nodes were identified in the network of social integration and SWB: “Daily integration” (SI1) and “Intimate integration” (SI2), suggesting that these two factors may serve as key mechanisms linking social integration and SWB. Among them, “Daily integration” (SI1) was both a core node and the primary bridge connecting social integration and SWB, indicating its particularly strong association with SWB. Changes in daily integration are therefore more likely to directly influence SWB among young and middle-aged lymphoma patients. This finding is consistent with a previous study showing that daily and leisure activities are significantly associated with SWB in older adults, and that leisure activities play a mediating role between daily activities and SWB.42 Patients with lymphoma frequently experience disease-related psychological distress.43 In contrast, daily low-stress social interactions may stimulate oxytocin secretion, relieve physical and mental stress, and consequently enhance SWB.44 Furthermore, daily communication provides low-cost, high-frequency emotional connection, enhances individuals’ sense of normality, belonging, and self-worth,45 and effectively relieves loneliness and insecurity caused by treatment-related isolation and lost social roles.
“Intimate integration” (SI2) was identified as another bridge node connecting the network of social integration and SWB. This indicates that it has a strong correlation with SWB, and changes in this domain are more likely to lead to variations in SWB among young and middle-aged lymphoma patients. Our findings are consistent with a previous study suggesting that intimate relationships in older adults exert a continuous effect through long-term stability, thereby sustainably improving SWB over time.46 For young and middle-aged lymphoma patients, high-quality intimate support can enhance psychological resilience, reduce disease-related stress, and further alleviate negative emotions while improving SWB.47 In addition, a high level of intimacy and belonging can strengthen the positive association between social interaction frequency and individuals’ SWB.48 Therefore, interventions centered on intimate integration represent an effective approach to improving social integration and SWB in this population. Healthcare professionals are recommended to establish a precise and multi-level community support framework and implement differentiated interventions according to patients’ treatment stages and physical conditions: offline disease-specific communication activities for physically eligible patients, online home-based support and remote interaction for those in poor physical condition, and concurrent family support workshops. By establishing channels for emotional communication and social support, patients’ sense of intimacy and belonging can be enhanced, thereby improving their social integration and SWB.
Comparative Analysis of Gender Differences in Social Integration and SWB Networks
Finally, network comparison in the present study revealed no significant gender differences in the network structure of social integration and SWB. This may be attributed to similar impacts of common challenges, including treatment-related side effects and disrupted social roles, on patients of both genders, resulting in consistent core features of social integration and SWB. Future studies with larger sample sizes and longer follow-up periods are warranted to further explore the potential moderating role of gender in the association patterns between social integration and well-being across different disease stages and treatment intensities.
Limitations
Several limitations of this study should be noted. First, this study only recruited lymphoma patients from a single tertiary cancer hospital in Urumqi, which may limit the generalizability of the findings. Future multi-center and large-sample studies could be conducted to verify our results. Second, as a cross-sectional study, this research cannot infer causal relationships between social integration and SWB over time. Longitudinal study designs may be used in future work to explore dynamic network changes. Third, this study only performed network comparisons by gender and did not conduct further analyses incorporating clinical characteristics such as lymphoma subtype, disease severity, and remission status. Therefore, the conclusions may be heterogeneous across these clinical factors. Finally, the scales used in this study were based on patient self-reports, which may introduce reporting bias or recall bias. Future studies may consider including objective measures such as social interaction frequency and laboratory indicators, combined with more detailed clinical characteristics, to provide a more comprehensive and accurate analysis of the relationship between social integration and SWB and improve the clinical applicability of the conclusions.
Conclusions
This study employed a network analysis approach to elucidate the complex interplay between social integration and SWB among young and middle-aged patients with lymphoma. The findings identified negative emotions and basic social integration as central hubs underlying the psychosocial health of this population, and revealed no significant gender differences in the association network. The core value of this study lies in providing empirical evidence for psychosocial care in this population and clarifying the shift from general support to precise and individualized interventions. The core nodes and bridge nodes identified from the network structure can inform the development of targeted clinical care strategies to improve social adaptation and mental health outcomes in these patients.
Data Sharing Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author upon reasonable request.
Ethics and Informed Consent Statement
This study was conducted in strict accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of The Affiliated Cancer Hospital of Xinjiang Medical University (No. K-2024213). Written informed consent was obtained from all patients prior to participation.
Acknowledgments
We thank all the participants for their cooperation.
Funding
This study was funded by the “Tianshan Talents” Medical and Health High-Level Talent Training Program.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–11. doi:10.1016/j.jncc.2024.01.006
2. House086. Global and Chinese lymphoma patients’ survival status comparison report. Available from: https://www.house086.com/thread-222638-1-1.html. Accessed November 16, 2021.
3. Stepanishyna Y, Wolfromm A, De Wilde V. All you need to know about survivorship in lymphoma in adults and AYA patients. Curr Opin Oncol. 2025;37(5):424–432. doi:10.1097/cco.0000000000001161
4. Jung W, Thompson HJ, Byun E. Social integration: a concept analysis. Nurs Forum. 2022;57(6):1551–1558. doi:10.1111/nuf.12843
5. Juul SJ, Rossetti S, Kicinski M, et al. Work and education interruption in long-term Hodgkin lymphoma survivors: an analysis among patients from nine EORTC-LYSA trials. Acta Oncol. 2023;62(7):744–752. doi:10.1080/0284186x.2023.2195561
6. Ruan J, Qian Y, Zhuang Y, Zhou Y. The illness experiences of Chinese patients living with lymphoma: a qualitative study. Cancer Nurs. 2020;43(4):E229–e238. doi:10.1097/ncc.0000000000000717
7. Kroenke CH, Paskett ED, Cené CW, et al. Prediagnosis social support, social integration, living status, and colorectal cancer mortality in postmenopausal women from the women’s health initiative. Cancer. 2020;126(8):1766–1775. doi:10.1002/cncr.32710
8. Rice EL, Adair KC, Tepper SJ, Fredrickson BL. Perceived social integration predicts future physical activity through positive affect and spontaneous thoughts. Emotion. 2020;20(6):1074–1083. doi:10.1037/emo0000616
9. Matos J, Henriques A, Moura A, Alves E. Professional reintegration of stroke survivors and their mental health, quality of life and community integration. Qual Life Res. 2024;33(12):3259–3273. doi:10.1007/s11136-024-03797-8
10. Yi JS, Lee SY. Social reintegration experiences of young adult cancer survivors. Behav Sci. 2024;14(11):1101. doi:10.3390/bs14111101
11. Diener E. Subjective well-being. Psychol Bull. 1984;95(3):542–575. doi:10.1037/0033-2909.95.3.542
12. Yang K, Ren Y, Peng W, et al. Subjective well-being among Chinese breast cancer patients: the unique contributions of death anxiety, self-esteem, and social support. J Health Psychol. 2024;29(3):213–224. doi:10.1177/13591053231195391
13. Huang YY, Liu CY, Chien CH. Subjective well-being in patients with newly diagnosed colorectal cancer: an observational study. Cancer Nurs Jun. 2025;13. doi:10.1097/ncc.0000000000001520
14. Haydon MD, Hwang AE, Wadé NB, et al. Adverse late outcomes in long-term survivors of young adult Hodgkin lymphoma (YAHL) compared to their unaffected co-twins. Leuk Lymphoma. 2025;66(7):1254–1263. doi:10.1080/10428194.2025.2476664
15. Vena JA, Copel LC. Cancer survivorship and quality of life outcomes of adolescents and young adults with lymphoma: an integrative review. Eur J Oncol Nurs. 2021;52:101948. doi:10.1016/j.ejon.2021.101948
16. Diener E, Pressman SD, Hunter J, Delgadillo-Chase D. If, Why, and When subjective well-being influences health, and future needed research. Appl Psychol Health Well Being. 2017;9(2):133–167. doi:10.1111/aphw.12090
17. Fei C, Zhu Y, Jiang L, Zhou H, Yu H. Social integration, physical and mental health and subjective well-being in the floating population-a moderated mediation analysis. Front Public Health. 2023;11:1167537. doi:10.3389/fpubh.2023.1167537
18. Shen G, Yang X, Huang J, et al. Interplay of social integration, well-being, and fairness in older migrant workers: a four -year longitudinal analysis. Popul Health Metr. 2025;23(1):47. doi:10.1186/s12963-025-00411-y
19. Fox RS, Armstrong GE, Gaumond JS, et al. Social isolation and social connectedness among young adult cancer survivors: a systematic review. Cancer. 2023;129(19):2946–2965. doi:10.1002/cncr.34934
20. Curtin S, Galvin R, Robinson K. The relationship between cancer survivors’ well-being and participation in work, activities of daily living and social engagement: findings from the European Social Survey (2014). Scand J Occup Ther. 2021;28(7):531–541. doi:10.1080/11038128.2019.1695932
21. Salazar S, Dino MJS, Macindo JRB. Social connectedness and health-related quality of life among patients with cancer undergoing chemotherapy: a mixed method approach using structural equation modelling and photo-elicitation. J Clin Nurs. 2023;32(17–18):6298–6309. doi:10.1111/jocn.16675
22. Latinsky-Ortiz EM, Strober LB. Keeping it together: the role of social integration on health and psychological well-being among individuals with multiple sclerosis. Health Soc Care Community. 2022;30(6):e4074–e4085. doi:10.1111/hsc.13800
23. Choi NG, Marti CN, Zhou Y, Kunik ME. Social participation and psychological well-being among older adults with dementia. Dementia. 2025;14713012251375273. doi:10.1177/14713012251375273
24. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
25. Fone D, Dunstan F, Lloyd K, Williams G, Watkins J, Palmer S. Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. Int J Epidemiol. 2007;36(2):338–345. doi:10.1093/ije/dym004
26. Han J, Wang JQ, Xie BQ, Wang Y. Reliability and validity of the Chinese version of the Social Cohesion Scale in community-dwelling adults aged 75 years and older. J Nurses Train. 2021;(13). doi:10.16821/j.cnki.hsjx.2021.13.001
27. Fazio AF. A concurrent validational study of the NCHS general well-being schedule. Vital Health Stat. 1977;(73):1–53.
28. Duan JH. Application and analysis of the general well-being schedule in Chinese college students. Chin J Clin Psychol. 1996;(1):56–57.
29. Vilela-Estrada AL, Villarreal-Zegarra D, Mayo-Puchoc N, et al. Fluctuations in daily happiness and nervousness based on depressive and anxious symptoms in adolescents or young adults across 3 Latin American Cities: experience sampling study. JMIR Form Res. 2025;9:e65732. doi:10.2196/65732
30. Simon A, Nizard JJ, Chevalier P, et al. Impact of the practice of touch-massage® by a nurse on the anxiety of patients with hematological disorders hospitalized in a sterile environment, a randomized, controlled study. BMC Complement Med Ther. 2024;24(1):1. doi:10.1186/s12906-023-04302-3
31. Lemétayer F, Reinert P, Asselin M, Rotonda C. Relationship between negative emotions and physical activity engagement after colorectal cancer: a network analysis study. Support Care Cancer. 2025;33(5):437. doi:10.1007/s00520-025-09439-0
32. Stoffel M, Abbruzzese E, Rahn S, Bossmann U, Moessner M, Ditzen B. Covariation of psychobiological stress regulation with valence and quantity of social interactions in everyday life: disentangling intra- and interindividual sources of variation. J Neural Transm. 2021;128(9):1381–1395. doi:10.1007/s00702-021-02359-3
33. Garland EL, Fredrickson B, Kring AM, Johnson DP, Meyer PS, Penn DL. Upward spirals of positive emotions counter downward spirals of negativity: insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clin Psychol Rev. 2010;30(7):849–864. doi:10.1016/j.cpr.2010.03.002
34. Pan W, Long Y, Wang H, Yue C. More proactive but less efficient: the effect of trait self-control on emotion regulation and its neural mechanisms. Behav Brain Res. 2023;452:114567. doi:10.1016/j.bbr.2023.114567
35. Proctor CJ, Reiman AJ, Best LA. Cancer, now what? A cross-sectional study examining physical symptoms, subjective well-being, and psychological flexibility. Health Psychol Behav Med. 2023;11(1):2266220. doi:10.1080/21642850.2023.2266220
36. Yuan W, Jiang Y, Sun M, Zhao Q, Qiao G, Zheng Y. Factors influencing social avoidance and distress after radical lung cancer resection: a mediation analysis. Am J Transl Res. 2024;16(9):4770–4778. doi:10.62347/attp3522
37. Chen N, McGrath CB, Stopsack KH, et al. Social integration and long-term physical and psychosocial quality of life among prostate cancer survivors in the Health Professionals Follow-up Study. J Cancer Surviv. 2024;20:48–60. doi:10.1007/s11764-024-01632-0
38. Ruan J, Liu C, Ren R, Xing W. Post-treatment cancer survivors’ experience of social reintegration: a systematic review and meta-synthesis. Psychooncology. 2025;34(1):e70065. doi:10.1002/pon.70065
39. Behringer K, Goergen H, Müller H, et al. Cancer-related fatigue in patients with and survivors of Hodgkin Lymphoma: the impact on treatment outcome and social reintegration. J Clin Oncol. 2016;34(36):4329–4337. doi:10.1200/jco.2016.67.7450
40. Zheng S, Liu S, Yang Q, et al. The effectiveness of interventions to reduce cancer-related stigma: an integrative review. J Clin Nurs. 2024;33(7):2438–2455. doi:10.1111/jocn.17014
41. Sutton K, Moore J, Armes J, Briggs E. Perceptions and experiences of the subjective well-being of people with glioblastoma: a longitudinal phenomenological study. Neurooncol Pract. 2023;10(1):79–88. doi:10.1093/nop/npac064
42. Yang W, Tian G, Cui Y, et al. Associations between activities of daily living, leisure activities and subjective well-being in Chinese older adults. Gerodontology. 2024;41(3):415–423. doi:10.1111/ger.12721
43. Agostinelli G, Muzzatti B, Serpentini S, Spina M, Annunziata MA. Cancer-related psychological distress in lymphoma survivor: an Italian cross-sectional study. Front Psychol. 2022;13:872329. doi:10.3389/fpsyg.2022.872329
44. Zak PJ, Curry B, Owen T, Barraza JA. Oxytocin release increases with age and is associated with life satisfaction and prosocial behaviors. Front Behav Neurosci. 2022;16:846234. doi:10.3389/fnbeh.2022.846234
45. Grant MP, Philip JAM, Deliens L, Komesaroff PA. ‘It’s communication between people who are going through the same thing’: experiences of informal interactions in hospital cancer treatment settings. Support Care Cancer. 2023;31(7):440. doi:10.1007/s00520-023-07900-6
46. Abaei E, Martin P. The association between close relationships and happiness among older adults. Int J Aging Hum Dev. 2025;914150251352197. doi:10.1177/00914150251352197
47. Wang C, Liao Z, Li Z, Wang Y, Wu Y, Hu R. Identifying barriers to resilience from the perspective of young and middle-aged patients with lymphoma: a qualitative exploration. Eur J Oncol Nurs. 2023;64:102348. doi:10.1016/j.ejon.2023.102348
48. Kersten P, Borschel E, Neyer FJ, Mund M. The social side of personality: do affiliation and intimacy motives moderate associations of personal relationships with well-being? J Pers. 2023;91(4):992–1011. doi:10.1111/jopy.12746
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.