Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Neglected Narrative in the COVID-19 Pandemic: Epidemiological and Clinical Impacts of the COVID-19 Outbreak on Syphilis
Authors Liu M ![]() , Zhou J
, Zhou J ![]() , Lan Y
, Lan Y ![]() , Zhang H
, Zhang H ![]() , Wu M, Zhang X
, Wu M, Zhang X ![]() , Leng L, Mi X, Li J
, Leng L, Mi X, Li J ![]()
Received 17 April 2023
Accepted for publication 11 August 2023
Published 12 September 2023 Volume 2023:16 Pages 2485—2496
DOI https://doi.org/10.2147/CCID.S417522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Mingjuan Liu,1– 3 Jia Zhou,1,2 Yining Lan,1,2 Hanlin Zhang,1,2 Mengyin Wu,1,2 Xinyi Zhang,4 Ling Leng,1,2 Xia Mi,5 Jun Li1,2
1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 3 4+4 M.D. Program, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 4Departments of Internal Medicine and Cellular & Molecular Physiology, Yale School of Medicine, New Haven, CT, USA; 5Department of Dermatology, Strategic Support Force Medical Center, Beijing, People’s Republic of China
Correspondence: Xia Mi; Jun Li, Tel +86-69156699, Email [email protected]; [email protected]
Abstract: The COVID-19 pandemic has profoundly changed our lives. While healthcare resources were redistributed and mobilized to focus on dealing with the COVID-19 crisis, there have been unmet medical needs of patients with other diseases such as syphilis, weaving an integral but neglected component of the pandemic story. In different countries, the epidemiology of newly reported syphilis underwent diverse changes during the COVID-19 pandemic. Asymptomatic cases experienced the largest decline in number. From the perspective of transmission, on one hand, the implementation of lockdown measures led to a higher degree of abstinence and sex distancing in many countries, thereby reducing the transmission of syphilis. On the other hand, vertical transmission was reported to have increased significantly during COVID-19. Meanwhile, the volume of STI clinic capacity declined, and STI staff were redeployed to facilitate the contact tracing of COVID-19. As a result, many STI centers converted traditional in-person clinical services to telemedicine and self-testing. However, syphilis testing and clinical treatment cannot fully adapt to this conversion. In syphilis diagnosis, COVID-19 infection and vaccination were reported to cause false positivity in syphilis serological tests. Diverse cutaneous manifestations of COVID-19 could resemble the skin lesions in syphilis patients, requiring differential diagnosis from clinicians. As for the post-pandemic years, consequent to service interruptions and diagnosis delays, a surge in the number of confirmed cases of syphilis is expected. The COVID-19 pandemic has also been a meaningful lesson for the control and prevention of infectious diseases. The experience in combating COVID-19 has underscored the importance of maintaining a robust and well-supported medical system for the provision of sexual health services and better healthcare equality even during eras of crisis, not least for syphilis patients.
Keywords: COVID-19, syphilis, sexual behavior, STD prevention
Introduction
Since 2020, the COVID-19 pandemic has presented an unparalleled challenge to public health. Public attention and healthcare priorities have been primarily placed on this international threat, with almost every aspect of medicine profoundly impacted. The effective control of this pandemic was subject to the implementation of containment and closure policies. These restrictive social measures also exerted additional impacts on people’s sexual behavior and sexual health.
Syphilis is a sexually transmitted infection (STI) caused by Treponema pallidum (TP). Although treatable, syphilis has resurged in its recent incidence and constituted a modern plague afflicting millions of patients. Therefore, the syphilis epidemic become an emerging concern for public health and infectious diseases, especially after the pandemic considering healthcare interruptions.
This review inspects the intertwined picture of COVID-19 and syphilis, outlining its effects on epidemiological trends, clinical impacts, and future directions in syphilis management. Our aim is to shed light on how the disruption of the existing healthcare paradigm, driven by the pandemic, has inadvertently impacted the battle against syphilis, thus underscoring the need for an adaptable, comprehensive, and resilient healthcare system capable of addressing multifarious health implications even amidst a global health crisis.
Method
To investigate the epidemiological and clinical impacts of the COVID-19 outbreak on syphilis, we reviewed all existing scientific literature from PubMed, and Web of Science between December 2019 to March 2023. The string of keywords (COVID-19 OR SARS-CoV-2) AND (syphilis OR Treponema pallidum OR neurosyphilis) were used to search for literature including original articles, reviews, case reports, research letters and opinions on and around this topic. Duplicate papers are removed from the pool. The PRISMA flowchart with stage-based inclusion and exclusion process is shown in Figure 1, and the inclusion and exclusion criteria are listed as follows. Overall 76 studies and reports are included in this analysis.
 |
Figure 1 The PRISMA flowchart of studies and report inclusion and exclusion process to investigate the influence of the COVID-19 pandemic syphilis. |
Inclusion Criteria
- Studies published between December 2019 and March 2023.
- Research articles, reviews, case reports, research letters, and opinions found in PubMed and Web of Science that explore the influence and correlation between COVID-19 and syphilis, or studies that propose or assess approaches for managing syphilis in the context of the COVID-19 pandemic.
- Relevant policy documents, guidelines or STD reports from notable organizations including the World Health Organization (WHO), Public Health England, Centers for Disease Control and Prevention (CDC), and The National Coalition of STD Directors (NCSD), which directly address the impact or influence of COVID-19 on syphilis.
Exclusion Criteria
- Duplicate studies, or studies that substantially reproduce content from another source.
- Articles that are not in English, unless translation can be obtained.
- Studies focusing solely on COVID-19 or syphilis without any explicit link between the two.
- Non-peer-reviewed articles, opinion pieces without empirical data, or popular press articles.
- Studies published outside the specific time frame (December 2019–March 2023).
Changes in Newly Reported Cases of Syphilis During the Covid-19 Era
Variations in Reported Syphilis Epidemics
Most literature suggested a notable influence of the COVID-19 pandemic on newly reported syphilis cases, yet the course of the syphilis epidemiology differed as per the region of interest (Table 1). Most prominently, reductions in new cases of syphilis were observed in several countries and regions when the COVID-19 pandemic unfolded, including in China, Spain, Australia and the UK.1–8 In China, the actual national statistics of the newly reported cases of syphilis throughout 2020 were compared to the predicted value based on the historical data from pre-pandemic years. The comparison revealed a 100.4% decrease in new syphilis during the COVID-19 outbreak in February 2020 from the forecasted level.1 In the UK, the annual official statistics release of STI disclosed a nationwide 14% decrease when comparing the case count of syphilis in 2020 to that of 2019.3 However, reduced efforts in STI surveillance during COVID-19 can also account for a portion of the decline in syphilis case count, in which case the reported decrease may present potential underestimations of the actual circumstance.9,10
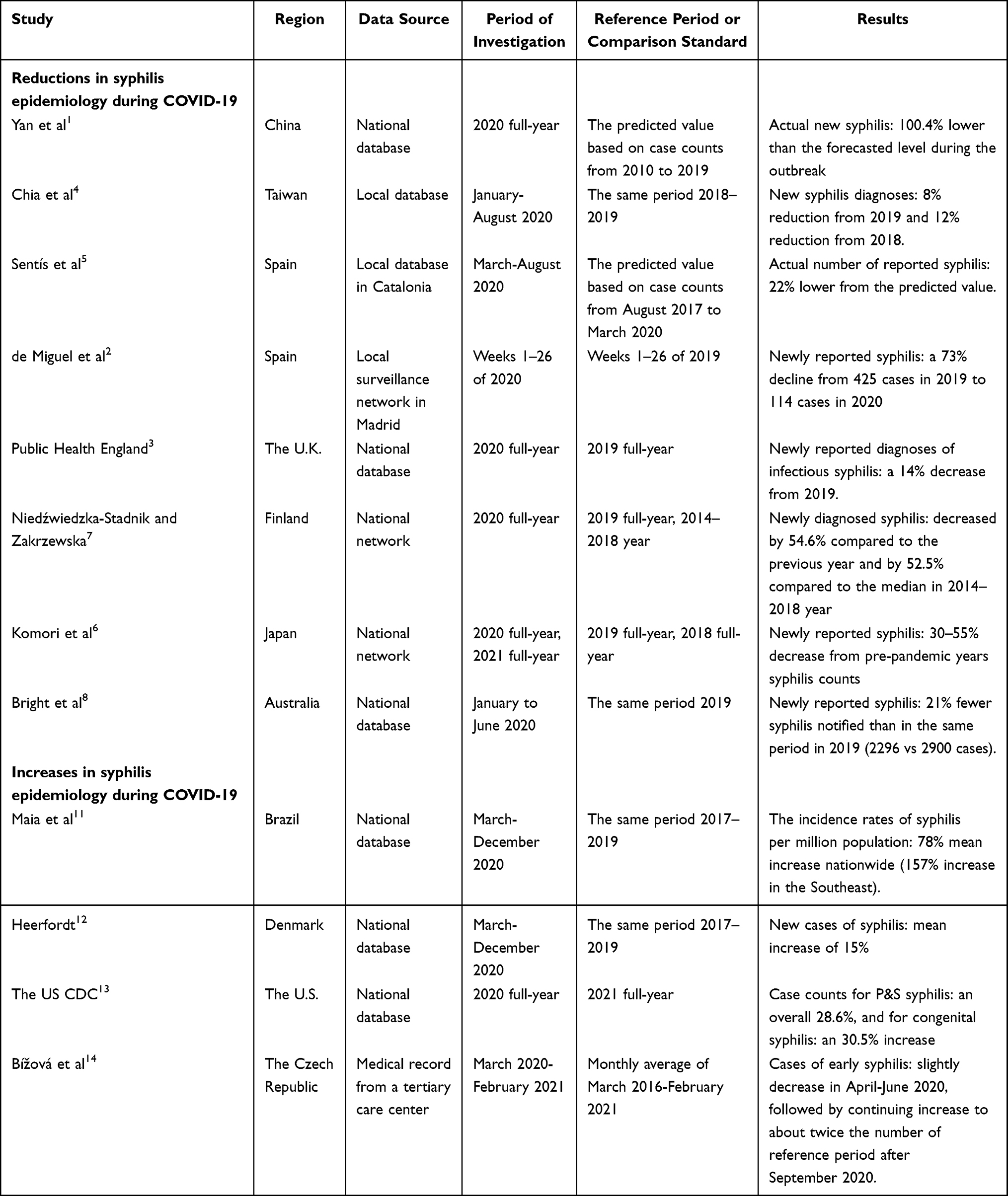 |
Table 1 Changes in Newly Reported Syphilis Case Counts in Different Countries During the COVID-19 Pandemic |
In contrast to the aforementioned sharp decrease in syphilis cases, some other countries, such as the US, Denmark and Brazil, experienced a notable increase in newly reported syphilis.11–14 Brazil witnessed the largest upward incidence of syphilis among reported countries; A direct comparison of syphilis cases from its national database revealed a surged incidence rate by 78% during the pandemic, denoting 161 additional syphilis patients per million population.11
The underlying reasons behind the divergence of syphilis epidemiology remain unclear. Some degree of epidemiological changes in STI during this era could potentially be attributed to the implementation of countermeasures against COVID-19 and modifications to people’s lifestyles (eg sexual behavior).15 A study in Cuba revealed that the incidence of syphilis declined under strict quarantine measures and vice versa.16 In China, Yan et al also found that the reported epidemic of sexually transmitted diseases (STDs) seemed inversely associated with the COVID-19 epidemics as well as local control policies, especially with measures that discouraged clinical visits.1
Changes in the Disease Spectrums for Syphilis and STIs
During the COVID-19 pandemic, the disease spectrum of syphilis underwent significant transformations as well. The most universal change lies in the sharp decline in reported asymptomatic and non-acute cases.17–20 As medical resources were mobilized to COVID-19, and people experienced more obstacles in accessing STI clinics, it was observed in the US and in Melbourne, Australia that screening for asymptomatic STDs was more adversely impacted in the pandemics than healthcare for symptoms-presenting conditions.19,21–24 In Europe, a survey covering 34 countries and different testing settings described that during March-May 2020, 95% of STI health services reported an over 50% reduction in their testing numbers from the expected volume.25 A sharp decline in numbers of asymptomatic syphilis patients were reported in Hungary and in some US regions, making latent syphilis a smaller part of the overall syphilis case spectrum than before.17,18,21 This change may also hint towards a likely underestimation of the actual prevalence of syphilis during this time period due to decreased screening.
Interestingly, several papers concerning STI epidemics during the COVID-19 pandemic have shown that the fluctuations in syphilis cases were relatively minor compared to other common STIs, such as chlamydia and gonorrhea.2,3,5,19,26,27 An epidemiological study in New York City revealed that syphilis cases decreased by 22% during the pandemic, in comparison to over 50% reductions in reported infections of HIV, Chlamydia, and Gonorrhea. Chow et al speculated that the overt clinical manifestations and serious symptoms of syphilis contributed to more active clinical attendance during the pandemic,19 as compared to other STIs.
Influence of Covid-19 on the Transmission Dynamics of Acquired and Congenital Syphilis
Syphilis is predominately acquired via sexual contact with infected mucosae or vertically transmitted from mothers to infants. During COVID-19, social distancing and lockdown orders brought numerous challenges to our everyday social life and routine clinical operations. Examining how these changes impacted sexual behavior and prenatal care provides a better picture of the transmission dynamics of syphilis.
The Transmission Dynamics of Acquired Syphilis
The fear of contracting COVID-19 discouraged sexual activities in this special time. During the first national emergency state of COVID-19 in Israeli, a local survey conducted among 2562 men who have sex with men (MSM) unveiled that only 3.2% of them could imagine themselves with sexual partners carrying COVID-19, compared with 30.1% accepting partners with HIV.28 A cross-national survey with 245 participants in Turkey revealed that 19.6% of men and 38.1% of women reported behavioral avoidance of sexual intimacy for fearing COVID-19 transmission.29 Another critical deterrence in sexual transmission came from multiple movement restrictions and lockdown measures. Entertainment events and large gatherings were canceled, and people may experience additional barriers to seeking casual sex in reality.1
With these barriers transforming people’s sexual life, one would postulate that sexual activities, especially casual and risky ones, would decrease during the COVID-19 pandemic. However, evidence on this matter is mixed. On the one hand, an online survey in China that included 270 male and 189 female participants revealed that the number of sexual partners declined in 44% of respondents, and sexual frequency decreased in 37% of the cohort during the lockdown.30 This abstinent transition was even more evident among participants with risky sexual behaviors,30 implying a prominent reduction in risks of STD transmission. Similarly, in Amsterdam, an online study encompassing 683 MSM observed that 73% of the respondents reported a decreased number of casual sex partners during the pandemic.31 However, a cross-sectional survey of 518 sexual minority males in the US found that on average respondents increased their number of sexual partners by 2.3 persons during the lockdown.32
Condom use also plays a critical role in preventing STD transmission. During COVID-19, Starks et al conducted a cohort-control study in US to compare condom use by comparing online responses from 455 adult respondents surveyed during the COVID-19 pandemic with matched samples surveyed pre-COVID. This comparison revealed a 45.2% unweighted reduction in people conducting condomless anal sex during the pandemic.33 Online surveys from Israel (N=2526) and Wales (N= 56) that involve mostly MSM also observed a similar increase in the frequency of condom use during this time.28,34 However, surveys among 731 MSM in China and 172 heterosexuals in Australia respectively revealed that their condom consumption declined significantly during COVID-19.35,36 The underlying reason for the discrepancy between condom use and sexual behavior frequency in different literature awaits investigation.35,36
The Transmission Dynamics of Congenital Syphilis
Although congenital transmission is less prevalent, its preventable and deleterious nature has drawn considerable clinical attention and healthcare resources. Eliminating mother-to-child transmissions requires maternal syphilis surveillance and continuous clinical treatment. The World Health Organization reported that antenatal care experienced a 56% service reduction during the COVID-19 era, constituting one of the most frequently disrupted healthcare services.37 The downgraded prenatal care support programs and lack of transportation access have led to increased susceptibility to congenital syphilis.38 For example, due to the cost and storage requirements of penicillin G benzathine, this first-line treatment is no longer available in some primary care centers in the US for affected mothers during the COVID-19 pandemic.38 As a result, it would be unsurprising that literature has consistently reported increases in syphilis vertical transmission during the pandemic. The US CDC report of STDs, 2021 revealed a 52.3% upsurge in primary and secondary (P&S) syphilis diagnoses for reproductive women and 30.5% for congenital syphilis.13 A retrospective medical record review in Texas, US claimed that syphilis infection almost doubled among underserved pregnant women in antenatal STI screenings during the pandemic.39 Estimates from the Lancet Global Health warned that healthcare disruptions during COVID-19 would lead to increased stillbirths and neonatal deaths from congenital syphilis.40
Syphilis-Related Medical Resources and Health-Seeking Choices During the Covid-19 Pandemic
The COVID-19 pandemic has posed severe challenges to the normal function of the public health system. As the COVID-19 pandemic unfolds, sexual health services have been seriously hindered by service disruptions, reallocation of STI professionals and restrictions for in-person visits.
Reduced Volume of Clinic Visits and Testing
From the perspective of healthcare-seeking behavior, several regions, including the US, Italy, and Portugal, have observed that patients display increased fear and hesitation in visiting in-person clinics, primarily due to concerns surrounding COVID-19 infection.41–46 Barriers to STI clinics during COVID-19 as a global experience may further compound the difficulties in clinic attendance.47 For people in need of sexual health services, an online survey in Canada with 1198 respondents showed that 66% of participating patients have avoided or postponed their clinic visits.48
Regarding STI care provision, there was an extensive reduction in patient volume and working hours that STI clinics provide. In worse cases, STI clinics announced the entire closure of in-person clinic visits. In many STI healthcare settings, ‘nonessential visits’ have been canceled to prioritize emergency and COVID-19 control.23 In April 2020, the CDC of the US offered guidelines for STD prevention programs (https://www.cdc.gov/std/dstdp/DCL-STDTreatment-COVID19-04062020.pdf) that recommended deferring routine screening visits until the emergency state is over. Regarding syphilis, the guidelines mentioned that STD clinic visits should prioritize neurosyphilis patients and pregnant women with syphilis. Based on a survey from the National Coalition of STD Directors in the US, 83% of STD program directors admit postponement of their STD services due to COVID-19.49 Similarly, in Australia, a nationwide survey revealed that all responded STD clinics (N=20) stated a reduced volume of consultations they offer, with 65% of them reporting at least a moderate decrease.50
The COVID-19 pandemic also had a negative impact on STI testing and screening, including on syphilis. The Boston Medical Center also reported a significant decline in syphilis testing during the pandemic. The number of monthly tests decreased by 74% during the peak-pandemic period, with a nadir of 314 tests in April 2020, as compared to a baseline pre-pandemic mean of 1186 tests/month.51 Similarly, a study analyzing the STI screening data from the French national health database revealed a 37% decrease in the total number of STI screenings in April 2020 during the first wave of COVID-19 compared to March 2020, with a 32% decrease in syphilis testing.52
Redeployment of essential staff was an important reason for the decreased supply of STI care in the COVID-19 era. Before COVID-19, contact tracing was an essential component in many STD monitoring and management strategies. However, the spread of COVID-19 demanded sexual health staff adapt their specialized skills and resources to COVID-19 tracing. A survey from the National Coalition of STD Directors in the US reported that 78% of their STI Disease Intervention Specialists were remobilized to control COVID-19 in 2020.49
These interruptions also resulted in underdiagnoses and undertreatment of STIs.23 Delayed or canceled diagnosis and treatment of syphilis may have precipitated serious complications such as neurosyphilis as well as increase the risk of transmission to additional sexual contacts and unborn infants.
The Shift to Telemedicine and Self-Testing
Following limitations for in-person visits, STI service suppliers in many countries emphasized transforming the service mode to telemedicine during COVID-19.48,49,53 Telehealth screening calls were even made a prerequisite by many STI clinics before in-person visits.54 STI management guidelines in King County recommended telephone or telemedicine clinics and oral medications for people with confirmed positive STI results.55 However, there was a concern that oral prescription of doxycycline for syphilis patients from telemedicine implies greater difficulty in adherence and cannot treat as effectively as the conventional first-line intramuscular penicillin.17
The COVID-19 pandemic also contributed to the accelerating development of STI self-testing tools.56 This alternative testing approach is frequently perceived as a more convenient and private method of STD testing. In 2019, WHO reviewed the self-testing evidence for common pathogens of STDs and recommended that self-testing for Neisseria gonorrhoeae and Chlamydia trachomatis “should be made available” while the self-testing of TP “may be considered”.57 The technical problem underlying self-testing syphilis might explain the difference in WHO recommendations. Syphilis testing currently requires a serum or blood sample for performance of treponemal and non-treponemal assays. Nontreponemal antibody titer can serve as an indicator of patients’ current infection status and treatment response. A common practice for self-collected blood samples often involves dry blood spots (DBS). While treponemal testing has established satisfactory results in DBSs, this approach fails to quantity antibody concentration or reach sufficient sensitivity in nontreponemal tests.56 As a result, though self-testing has been widely embraced for other STIs, the testing for syphilis is still ultimately subject to in-person clinical attendance and in-clinic examinations during the COVID-19 pandemic.56
Challenges of Syphilis Diagnosis Due to Covid-19
False Positivity in Nontreponemal Tests After COVID-19 Infection
VDRL test is a common nontreponemal test for the screening of syphilis. A case report described a young man whose VDRL tests turned positive after COVID-19 infection.58 He attended an STI clinic due to a positive VDRL from his donated blood. However, he appeared asymptomatic and claimed no sexual contact within a year. His TPHA test was negative and his VDRL results were negative during screenings before the COVID-19 infection. Without any syphilis treatment, his serum VDRL returned to non-reactive after weeks. This case report speculated that COVID-19 infection was probably responsible for this false positivity, as virus-induced polyclonal-gammopathy can produce false reactivity during such tests.58
Potential and Demonstrated Impact of COVID-19 Vaccination on Syphilis Diagnosis
RPR test is another nontreponemal test for screening active infections. A study at the University of Pittsburgh revealed that Moderna COVID-19 vaccines may lead to a high false-positive rate of RPR, with 7 out of 38 participants in their prospective cohort converted to reactive BioRad RPR results after vaccination.59 Subsequently, FDA Communication addressed that RPR tests were removed from the BioRad Syphilis Total and RPR Test Kit, announcing a suspension for this screening tool in the U.S.60
The Similarity in Clinical Manifestations of COVID-19 and Syphilis
Cutaneous manifestations of COVID-19 were observed in 20.4% of patients in a cross-sectional report in Italy.61 The dermatologic symptoms can occur in the early phase of COVID-19 infection before any respiratory signs and offer clues for the early diagnosis and triage. The exanthematous eruption is the most common dermatological sign of early COVID-19 infection, manifesting as widespread erythema, purpuric, maculopapular or morbilliform rashes.62 The polymorphic and non-specific nature of these cutaneous presentations challenged doctors in differentiating early COVID-19 infection from other diseases.
Syphilis is also known as the “Great Masquerader” for its diverse and systemic manifestations that resemble other diseases.63 Common symptoms during the secondary stage include fever, fatigue and myalgia to sore throat and diverse cutaneous lesions.63,64 A case report described a middle-aged male patient with a generalized rash, fever, cough and other systemic symptoms over two weeks amidst the COVID-19 outbreak.62 This patient was referred for a suspected COVID-19 infection, even when his nasopharyngeal swab was negative. A careful physical examination reveals morbilliform rashes on his trunk and erythematous rash on the face. A resolved genital rash was mentioned upon inquiry. Skin biopsy and serological tests confirmed secondary syphilis.62
The case report highlighted the similarity of both COVID-19 and syphilis being systemic diseases with heterogenous cutaneous manifestations. A review that examined cutaneous signs of COVID-19 warned that while urticarial rash with pyrexia is usually suggestive of COVID‐19 during the pandemic, syphilis should also be considered in such cases.65 Another review on COVID-19 cutaneous signs also mentioned syphilis as a potential reason for maculopapular rashes to be differentiated from COVID-19.66 Therefore, while detecting COVID-19 infection from cutaneous signs assists in early diagnosis, this consideration should not distract clinicians from identifying other common infections, such as syphilis.
The Control and Prevention of Syphilis After the Covid-19 Pandemic
Emphasizing the Continuing Provision of Sexual Health Services
While healthcare resources were primarily redistributed to deal with the COVID-19 crisis, the missed or postponed clinical services for STD patients had precipitated a parallel epidemic.67 Many countries have revealed remarkable surges in the reported cases of syphilis after the lockdown periods that well exceed pre-pandemic levels.1,14,16,68,69 Syphilis is a chronic systemic infection that requires continuous monitoring. Interruptions in healthcare practices for syphilis patients can lead to serious regressions in disease control and a heavier disease burden. In addition, the experience of dealing with COVID-19 has stressed the huge benefit of timely and sufficient diagnostic tools for infections. Similarly, screening projects are also an integral part of syphilis management and prevention that should not be compromised. The pandemic also highlighted the importance of developing quick and reliable self-testing tools for syphilis control for the provision of continuous monitoring.
Healthcare Barriers for Vulnerable Populations
The COVID-19 pandemic has highlighted the widening disparities in healthcare resources among different populations. A resurgence of syphilis incidence was witnessed in the United States with a greater increase among females and African-Americans.27,68 While health resources were more strained almost for everyone during the COVID-19 pandemic, accessing sexual health services became disproportionately harder for marginalized and underserved groups globally.25,70–76 For instance, the curtailing of public transport created additional barriers to clinical visits, especially for those without private vehicles.77 The transition to telemedicine could bring further problems to those disadvantaged people who were unequipped with the technologies and literacy for this new practice.71,77,78 Also, as the COVID-19 pandemic has led to adverse social-economic impacts worldwide, declined economic growth implies increasing vulnerability to poverty and withdrawal of health insurance for the minority groups, leading to additional STD health risks.79
Predicting the Future Course of Syphilis Epidemics
The longitudinal impact of COVID-19 on syphilis epidemics remains unclear. For countries that reported declines in syphilis, it remains crucial to determine whether this trend represents an actual decline due to safer sexual practices or an underestimation due to decreased testing and surveillance. Modeling and analysis in the literature revealed that this decline cannot be elucidated without considering significant interruptions in diagnoses and reporting,5,80,81 which might mask the actual rise of syphilis epidemics. Concerns have been raised about a potential rebound in STD incidence as society gradually recovers.9,17,81,82 The literature thus far has corroborated this concern.1,14,16,68,69 The sharp decrease in reported syphilis in some regions appeared mostly temporary. After the COVID-19 pandemic subsided and restrictive social measures softened, new syphilis diagnoses recovered quickly to approach pre-pandemic levels or even beyond.1,69 Based on an assumption that clinical interruptions persist for 18 months, a predictive model estimated over 57,000 STI cases in addition in 5 years just among MSM in Atlanta, Georgia, the U.S.52 Timely actions are desired for the control and prevention of syphilis in places where the resurgence has already taken place or where the resurgence of infections is predicted to unfold, such as the US.5,38,83,84
Conclusion
The narrative of the COVID-19 pandemic, as pivotal as it has been, forms a significant part of a broader tableau of how global health crises can shape and modulate the trajectory of various diseases, such as syphilis and other communicable diseases. We discovered the numerous epidemiological shifts and clinical implications that occurred in the world of syphilis following the advent of the COVID-19 pandemic, and the systemic changes it brought forth, both positive and negative. The pandemic influenced sexual behavior, care-seeking habits, diagnostic practices, and gave rise to service disruptions, but also drive innovative advances in telemedicine. As we traverse the aftermath of the COVID-19 pandemic, there exists an urgent necessity to address expected surges in syphilis diagnoses linked to service interruptions and delayed diagnoses. Aligning our focus on maintaining essential healthcare services and eliminating healthcare disparities for vulnerable communities is of paramount importance. Ultimately, the lessons learned from contending with COVID-19 serve as parables in the arena of healthcare, emphasizing the essence of a comprehensive, patient-centric, and adaptable medical system that stands as an unyielding fortress, even amidst the multifaceted and unforeseen challenges posed by future crises.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National High Level Hospital Clinical Research Funding (2022-PUMCH-B-092).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yan X, Wang X, Zhang X, Wang L, Zhang B, Jia Z. The epidemic of sexually transmitted diseases under the influence of COVID-19 in China. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.737817
2. de Miguel Buckley R, Trigo E, de la Calle-Prieto F, Arsuaga M, Díaz-Menéndez M. Social distancing to combat COVID-19 led to a marked decrease in food-borne infections and sexually transmitted diseases in Spain. J Travel Med. 2020;27(8). doi:10.1093/jtm/taaa134
3. Sexually transmitted infections and screening for chlamydia in England, 2020, The annual official statistics data release (data to end of December 2020). Public Health England; 2020. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1015176/STI_NCSP_report_2020.pdf.
4. Chia -C-C, Chao C-M, Lai -C-C. Diagnoses of syphilis and HIV infection during the COVID-19 pandemic in Taiwan. Sex Transm Infect. 2021;97(4):319. doi:10.1136/sextrans-2020-054802
5. Sentís A, Prats-Uribe A, López-Corbeto E, et al. The impact of the COVID-19 pandemic on sexually transmitted infections surveillance data: incidence drop or artefact? BMC Public Health. 2021;21(1):1637. doi:10.1186/s12889-021-11630-x
6. Komori A, Mori H, Naito T. The impact of the COVID-19 pandemic on other infections differs by their route of transmission: a retrospective, observational study in Japan. J Infect Chemother. 2022;28(12):1700–1703. doi:10.1016/j.jiac.2022.08.022
7. Niedźwiedzka-Stadnik M, Zakrzewska K. Syphilis in Poland in 2020. Przegl Epidemiol. 2022;76(3):391–401. doi:10.32394/pe.76.37
8. Bright A, Glynn-Robinson AJ, Kane S, Wright R, Saul N. The effect of COVID-19 public health measures on nationally notifiable diseases in Australia: preliminary analysis. Commun Dis Intell. 2020;44. doi:10.33321/cdi.2020.44.85
9. Yan J, Li Y, Zhou P. Impact of COVID-19 pandemic on the epidemiology of STDs in China: based on the GM (1,1) model. BMC Infect Dis. 2022;22(1):519. doi:10.1186/s12879-022-07496-y
10. Bell J, Canepa S, Kreis S, Taylor MM. Impact of COVID-19 lockdowns on sexual health care utilization and STD reporting, Maricopa County. Inquiry. 2021;58:469580211055583.
11. Maia CMF, Marques NP, Dias VO, Martelli DRB, Oliveira EA, Martelli-Junior H. Epidemiological trends in notified syphilis diagnoses during the COVID-19 pandemic in Brazil. Sex Transm Infect. 2021;98. doi:10.1136/sextrans-2021-055240
12. Heerfordt IM. STIs during the first and second wave of COVID-19 in Denmark. Sex Transm Infect. 2022;98(2):150–151. doi:10.1136/sextrans-2021-055021
13. Sexually Transmitted Disease Surveillance. Division of STD prevention, centers for disease control and prevention; 2022. Available from: https://www.cdc.gov/std/statistics/2021/overview.htm.
14. Bížová B, Rob F, Třešňák Hercogová J. Increase of early syphilis cases during the COVID-19 pandemic in the Czech Republic. Sex Transm Infect. 2022;98(3):231. doi:10.1136/sextrans-2021-055098
15. Hirae K, Hoshina T, Koga H. Impact of the COVID-19 pandemic on the epidemiology of other communicable diseases in Japan. Int J Infect Dis. 2023;128:265–271. doi:10.1016/j.ijid.2023.01.013
16. Rodríguez I, Hernández Y. Sexually transmitted diseases during the COVID-19 pandemic: a focus on syphilis and gonorrhoea in Cuba. Public Health Pract. 2021;2:100072. doi:10.1016/j.puhip.2020.100072
17. Johnson KA, Burghardt NO, Tang EC, et al. Measuring the Impact of the COVID-19 pandemic on sexually transmitted diseases public health surveillance and program operations in the state of California. Sex Transm Dis. 2021;48(8):606–613. doi:10.1097/OLQ.0000000000001441
18. Berzkalns A, Thibault CS, Barbee LA, Golden MR, Khosropour C, Kerani RP. Decreases in reported sexually transmitted infections during the time of COVID-19 in King County, WA: decreased Transmission or screening? Sex Transm Dis. 2021;48:S44–S49. doi:10.1097/OLQ.0000000000001463
19. Chow EPF, Hocking JS, Ong JJ, Phillips TR, Fairley CK. Sexually transmitted infection diagnoses and access to a sexual health service before and after the national lockdown for COVID-19 in Melbourne, Australia. Open Forum Infect Dis. 2021;8(1):ofaa536. doi:10.1093/ofid/ofaa536
20. Cusini M, Benardon S, Vidoni G, Brignolo L, Veraldi S, Mandolini PL. Trend of main STIs during COVID-19 pandemic in Milan, Italy. Sex Transm Infect. 2021;97(2):99. doi:10.1136/sextrans-2020-054608
21. Lőrincz K, Meznerics FA, Jobbágy A, et al. STIs during the COVID-19 pandemic in Hungary: gonorrhea as a potential indicator of sexual behavior. Int J Environ Res Public Health. 2022;19(15):9627. doi:10.3390/ijerph19159627
22. Wright SS, Kreisel KM, Hitt JC, Pagaoa MA, Weinstock HS, Thorpe PG. Impact of the COVID-19 pandemic on centers for disease control and prevention-funded sexually transmitted disease programs. Sex Transm Dis. 2022;49(4):e61–e63. doi:10.1097/OLQ.0000000000001566
23. Nagendra G, Carnevale C, Neu N, Cohall A, Zucker J. The Potential impact and availability of sexual health services during the COVID-19 pandemic. Sex Transm Dis. 2020;47(7):434–436. doi:10.1097/OLQ.0000000000001198
24. Bonett S, Teixeira da Silva D, Lazar N, Makeneni S, Wood SM. Trends in sexually transmitted infection screening during COVID-19 and missed cases among adolescents. Public Health. 2022;213:171–176. doi:10.1016/j.puhe.2022.10.007
25. Simões D, Stengaard AR, Combs L, Raben D. Impact of the COVID-19 pandemic on testing services for HIV, viral hepatitis and sexually transmitted infections in the WHO European Region, March to August 2020. Eurosurveillance. 2020;25(47):2001943. doi:10.2807/1560-7917.ES.2020.25.47.2001943
26. Crane MA, Popovic A, Stolbach AI, Ghanem KG. Reporting of sexually transmitted infections during the COVID-19 pandemic. Sex Transm Infect. 2021;97(2):101–102. doi:10.1136/sextrans-2020-054805
27. Braunstein SL, Slutsker JS, Lazar R, et al. Epidemiology of reported HIV and other sexually transmitted infections during the COVID-19 pandemic, New York City. J Infect Dis. 2021;224(5):798–803. doi:10.1093/infdis/jiab319
28. Shilo G, Mor Z. COVID-19 and the changes in the sexual behavior of men who have sex with men: results of an online survey. J Sex Med. 2020;17(10):1827–1834. doi:10.1016/j.jsxm.2020.07.085
29. Karagöz MA, Gül A, Borg C, et al. Influence of COVID-19 pandemic on sexuality: a cross-sectional study among couples in Turkey. Int J Impot Res. 2020;33(8):815–823. doi:10.1038/s41443-020-00378-4
30. Li W, Li G, Xin C, Wang Y, Yang S. Challenges in the practice of sexual medicine in the time of COVID-19 in China. J Sex Med. 2020;17(7):1225–1228. doi:10.1016/j.jsxm.2020.04.380
31. van Bilsen WPH, Zimmermann HML, Boyd A, et al. Sexual behavior and its determinants during COVID-19 restrictions among men who have sex with men in Amsterdam. J Acquir Immune Defic Syndr. 2021;86(3):288–296. doi:10.1097/QAI.0000000000002581
32. Stephenson R, Chavanduka TMD, Rosso MT, et al. Sex in the time of COVID-19: results of an online survey of gay, bisexual and other men who have sex with men’s experience of sex and HIV prevention during the US COVID-19 Epidemic. AIDS Behav. 2021;25(1):40–48. doi:10.1007/s10461-020-03024-8
33. Starks TJ, Jones SS, Sauermilch D, et al. Evaluating the impact of COVID-19: a cohort comparison study of drug use and risky sexual behavior among sexual minority men in the U.S.A. Drug Alcohol Depend. 2020;216:108260. doi:10.1016/j.drugalcdep.2020.108260
34. Gillespie D, Knapper C, Hughes D, et al. Early impact of COVID-19 social distancing measures on reported sexual behaviour of HIV pre-exposure prophylaxis users in Wales. Sex Transm Infect. 2021;97(2):85. doi:10.1136/sextrans-2020-054598
35. Booton RD, Fu G, MacGregor L, et al. The impact of disruptions due to COVID-19 on HIV transmission and control among men who have sex with men in China. J Int AIDS Soc. 2021;24(4):e25697. doi:10.1002/jia2.25697
36. Dacosta L, Pinkus RT, Morandini J, Dar-Nimrod I. Condom use during COVID-19: findings from an Australian sample of heterosexual young adults. Sexologies. 2021;30(1):e43–48. doi:10.1016/j.sexol.2020.1012.1007
37. World Health Organization. Pulse survey on continuity of essential health services during the COVID-19 pandemic. Interim report; 2020.
38. Nazir A, Masood W, Ahmad S, et al. Rise of syphilis surge amidst COVID-19 pandemic in the USA: a neglected concern. Ann Med Surg. 2022;80:104239. doi:10.1016/j.amsu.2022.104239
39. Stafford IA, Coselli JO, Wilson DF, Wang CY, Sibai BM. Comparison of sexually transmitted infections and adverse perinatal outcomes in underserved pregnant patients before vs during the COVID-19 pandemic in Texas. JAMA Netw Open. 2022;5(2):e220568. doi:10.1001/jamanetworkopen.2022.0568
40. Roberton T, Carter ED, Chou VB, et al. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020;8(7):e901–e908. doi:10.1016/S2214-109X(20)30229-1
41. Moroni F, Gramegna M, Ajello S, et al. Collateral damage: medical care avoidance behavior among patients with myocardial infarction during the COVID-19 pandemic. JACC Case Rep. 2020;2(10):1620–1624. doi:10.1016/j.jaccas.2020.04.010
42. Tao J, Napoleon SC, Maynard MA, et al. Impact of the COVID-19 pandemic on sexually transmitted infection clinic visits. Sex Transm Dis. 2021;48(1):e5–e7. doi:10.1097/OLQ.0000000000001306
43. Moore R, Purvis RS, Hallgren E, et al. ”I am hesitant to visit the doctor unless absolutely necessary”: a qualitative study of delayed care, avoidance of care, and telehealth experiences during the COVID-19 pandemic. Medicine. 2022;101(32):e29439. doi:10.1097/MD.0000000000029439
44. Hung KK, Walline JH, Chan EYY, et al. Health service utilization in Hong Kong during the COVID-19 Pandemic – a cross-sectional public survey. Int J Health Plann Manag. 2022;11(4):508–513. doi:10.34172/ijhpm.2020.183
45. Soares P, Leite A, Esteves S, et al. Factors associated with the patient’s decision to avoid healthcare during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(24):13239. doi:10.3390/ijerph182413239
46. Lazzerini M, Barbi E, Apicella A, Marchetti F, Cardinale F, Trobia G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc Health. 2020;4(5):e10–e11. doi:10.1016/S2352-4642(20)30108-5
47. Hannah V, Hamsadvani K, Elin CL, et al. Impact of the COVID-19 pandemic on access to and utilisation of services for sexual and reproductive health: a scoping review. BMJ Glob Health. 2022;7(10):e009594. doi:10.1136/bmjgh-2022-009594
48. Gilbert M, Chang H-J, Ablona A, et al. Accessing needed sexual health services during the COVID-19 pandemic in British Columbia, Canada: a survey of sexual health service clients. Sex Transm Infect. 2021;2021:sextrans-2021–055013.
49. COVID-19 & the State of the STD Field. National Coalition of STD Directors (NCSD); 2020. Available from: https://www.ncsddc.org/wp-content/uploads/2020/05/STD-Field.Survey-Report.Final_.5.13.20.pdf.
50. Phillips TR, Fairley CK, Donovan B, et al. Sexual health service adaptations to the coronavirus disease 2019 (COVID-19) pandemic in Australia: a nationwide online survey. Aust N Z J Public Health. 2021;45(6):622–627. doi:10.1111/1753-6405.13158
51. Lescure TN, Stewart J, Sperring H, Ruiz-Mercado G, Taylor JL. Impact of COVID-19 on sexually transmitted infection and HIV screening at an urban safety-net hospital. AIDS Patient Care STDS. 2023;37(4):199–204. doi:10.1089/apc.2022.0220
52. Viriot D, Lucas E, de Barbeyrac B, et al. Use of healthcare reimbursement data to monitor bacterial sexually transmitted infection testing in France, 2006 to 2020. Euro Surveill. 2022;27(39). doi:10.2807/1560-7917.ES.2022.27.39.2100618
53. Tang K, Zhang H, Jin H. Resuming work gradually in the context of COVID-19: experience from a tertiary dermatology department in China. Dermatol Ther. 2020;33(4):e13554–e13554. doi:10.1111/dth.13554
54. Sexual health clinics and our nation’s COVID-19 response: summary report describing the impact of the COVID-19 pandemic on sexual health clinics. national coalition of STD directors; 2020. Available from: https://www.ncsddc.org/wp-content/uploads/2020/10/Clinic-Call-Report-10.23.2020-final.pdf.
55. Barbee LA, Dombrowski JC, Hermann S, et al. ”sex in the time of COVID”: clinical guidelines for sexually transmitted disease management in an era of social distancing. Sex Transm Dis. 2020;47(7):427–430. doi:10.1097/OLQ.0000000000001194
56. Kersh EN, Shukla M, Raphael BH, Habel M, Park I. At-home specimen self-collection and self-testing for sexually transmitted infection screening demand accelerated by the COVID-19 pandemic: a review of laboratory implementation issues. J Clin Microbiol. 2021;59(11). doi:10.1128/JCM.02646-20
57. World Health Organization. Guidelines approved by the guidelines review committee. In: WHO Consolidated Guideline on Self-Care Interventions for Health: Sexual and Reproductive Health and Rights. Geneva: World Health Organization; 2019.
58. Ahmed G, George CA, Ganguly S. Post-COVID-19 biologically false-positive VDRL: a report. Int J STD AIDS. 2022;33(5):525–526.
59. Korentzelos D, Baloda V, Jung Y, Wheeler B, Shurin MR, Wheeler SE. COVID-19 mRNA vaccines may cause false reactivity in some serologic laboratory tests, including rapid plasma reagin tests. Am J Clin Pathol. 2022;158:162–166. doi:10.1093/ajcp/aqac025
60. Centers for Disease Control and Prevention. Guidance and resources during disruption of STD clinical services; 2021. Available from: https://www.cdc.gov/std/prevention/disruptionGuidance.htm..
61. Recalcati S Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol. 2020;34(5):e212–e213.
62. Di Buduo A, Atzori L, Pilloni L, Perla S, Rongioletti F, Ferreli C. Don’t forget about syphilis: sexually transmitted diseases during COVID-19 pandemic. J Public Health Res. 2020;9(4):2040. doi:10.4081/jphr.2020.2040
63. Brockshus A, Evans MO, Punch C. Secondary syphilis presentation and urticarial eruption after moderna COVID-19 vaccination. Mil Med. 2022;2022:usac191.
64. Baughn RE, Musher DM. Secondary syphilitic lesions. Clin Microbiol Rev. 2005;18(1):205–216. doi:10.1128/CMR.18.1.205-216.2005
65. Wollina U, Karadağ AS, Rowland-Payne C, Chiriac A, Lotti T Cutaneous signs in COVID-19 patients: A review. Dermatol Ther. 2020;33(5):
66. Gottlieb M, Long B. Dermatologic manifestations and complications of COVID-19. Am J Emerg Med. 2020;38(9):1715–1721. doi:10.1016/j.ajem.2020.06.011
67. Furlam TO, Pereira CC, Frio GS, Machado CJ. Efeito colateral da pandemia de Covid-19 no Brasil sobre o número de procedimentos diagnósticos e de tratamento da sífilis. Revista Brasileira de Estudos de População. 2022;39:e0184–e0184.
68. Pagaoa M, Grey J, Torrone E, Kreisel K, Stenger M, Weinstock H. Trends in nationally notifiable sexually transmitted disease case reports during the US COVID-19 pandemic, January to December 2020. Sex Transm Dis. 2021;48(10):798–804. doi:10.1097/OLQ.0000000000001506
69. Ghaznavi C, Tanoue Y, Kawashima T, et al. Recent changes in the reporting of STIs in Japan during the COVID-19 pandemic. Sex Transm Infect;2022. sextrans-2021–055378. doi:10.1136/sextrans-2021-055378
70. Silva DS, Smith MJ. Social distancing, social justice, and risk during the COVID-19 pandemic. Can J Public Health. 2020;111(4):459–461. doi:10.17269/s41997-020-00354-x
71. Khilnani A, Schulz J, Robinson L. The COVID-19 pandemic: new concerns and connections between eHealth and digital inequalities. J Inf Commun Ethics Soc. 2020;18(3):393–403. doi:10.1108/JICES-04-2020-0052
72. Dorn A, Cooney RE, Sabin ML. COVID-19 exacerbating inequalities in the US. Lancet. 2020;395(10232):1243–1244. doi:10.1016/S0140-6736(20)30893-X
73. Blundell R, Costa Dias M, Joyce R, Xu X. COVID-19 and Inequalities*. Fisc Stud. 2020;41(2):291–319. doi:10.1111/1475-5890.12232
74. Wang X, Shi L, Zhang Y, Chen H, Sun G. Policy disparities in fighting COVID-19 among Japan, Italy, Singapore and China. Int J Equity Health. 2021;20(1):33. doi:10.1186/s12939-020-01374-2
75. Raeside A, Handa M, Spitzer R. The disproportionate impact of COVID-19 on already marginalized communities: considerations for sexual and reproductive health care. J Obstet Gynaecol Can. 2021;43(11):1229–1230. doi:10.1016/j.jogc.2021.06.007
76. Kar A, Carrel AL, Miller HJ, Le HTK. Public transit cuts during COVID-19 compound social vulnerability in 22 US cities. Transp Environ. 2022;110:103435. doi:10.1016/j.trd.2022.103435
77. Chen KL, Brozen M, Rollman JE, et al. How is the COVID-19 pandemic shaping transportation access to health care? Transp Res Interdiscip Perspect. 2021;10:100338. doi:10.1016/j.trip.2021.100338
78. Katzow MW, Steinway C, Jan S. Telemedicine and health disparities during COVID-19. Pediatrics. 2020;146(2). doi:10.1542/peds.2020-1586
79. Prevention CfDCa. New data suggest STDs continued to increase during first year of the COVID-19 pandemic; 2022.
80. Joshi M, Yuan Y, Miranda W, Chung R, Rajulu DT, Hart-Malloy R. A peek into the future: how a pandemic resulted in the creation of models to predict the impact on sexually transmitted infection(s) in New York State (excluding New York City). Sex Transm Dis. 2021;48(5):381–384. doi:10.1097/OLQ.0000000000001377
81. Nowack N, Skaletz-Rorowski A, Potthoff A. Sexuell übertragbare Infektionen unter dem Einfluss der COVID-19-Pandemie [Sexually transmitted infections under the influence of the COVID-19 pandemic]. Dermatologie. 2023;74(2):129–136. Romanian. doi:10.1007/s00105-022-05099-x
82. Rogers B, Tao J, Murphy M, Chan PA. The COVID-19 pandemic and sexually transmitted infections: where do we go from here? Sex Transm Dis. 2021;48(7):e94–e96. doi:10.1097/OLQ.0000000000001445
83. Jenness SM, Le Guillou A, Chandra C, et al. Projected HIV and bacterial sexually transmitted infection incidence following COVID-19-related sexual distancing and clinical service interruption. J Infect Dis. 2021;223(6):1019–1028. doi:10.1093/infdis/jiab051
84. Tucker JD, Marley G, Marks M, Mabey D. Prioritizing syphilis control: now is the time for action. Front Med. 2022;9. doi:10.3389/fmed.2022.899200
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.