Back to Journals » Psychology Research and Behavior Management » Volume 15
A Narrative Review on the Non-Pharmacologic Interventions in Post-Stroke Depression
Authors Wijeratne T, Sales C, Wijeratne C
Received 30 October 2021
Accepted for publication 10 June 2022
Published 7 July 2022 Volume 2022:15 Pages 1689—1706
DOI https://doi.org/10.2147/PRBM.S310207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Video abstract presented by Tissa Wijeratne.
Views: 506
Tissa Wijeratne,1– 3 Carmela Sales,4 Chanith Wijeratne5
1School of Psychology and Public Health, La Trobe University, Melbourne, Australia; 2Department of Neurology, Western Health & University Melbourne, AIMSS, Level Three, WHCRE, Sunshine Hospital, St Albans, 3021, Australia; 3Department of Medicine, Faculty of Medicine, University of Rajarata, Saliyapura, Anuradhapura, Sri Lanka; 4Department of Medicine and Neurology, AIMSS, Melbourne Medical School, Sunshine Hospital, Western Health, St. Albans, Victoria, Australia; 5Monash Medical School, Clayton, Victoria, Australia
Correspondence: Tissa Wijeratne, Email [email protected]
Abstract: Stroke is a major cause of death and disability globally. Post-stroke depression (PSD) is a major driver for poor recovery and poor quality of life with extra burden for the patient and the caregiver. We have previously shown the inflammatory basis of PSD with associated bioenergetic failure, disruption of the blood-brain barrier, cell death, and persistent maladapted inflammation, making the PSD a norm rather than the exception, highlighting the unmet need for therapeutic intervention in PSD across the recovery trajectory. In this era, various interventions are focused on pharmacotherapy; however, non-pill-based medication should also be explored as post-stroke patients are likely to suffer from the adverse effects of polypharmacy. This narrated review explores the status of non-pharmacological interventions in managing PSD. We performed a PubMed search using pre-specified keywords looking at various non-pharmacologic approaches for the management of PSD. Worldwide, approaches such as non-invasive brain stimulation, behavioral and psychosocial therapy, as well as exercise, acupuncture, music, literature, and art therapies are available as monotherapy or adjunctive treatment for PSD. While current literature shows convincing results on the benefits of non-pharmacologic interventions, more robust studies are necessary to determine its utility in PSD.
Keywords: stroke, depression, non-pharmacological intervention, disability
Introduction
The Global Burden of Disease Study reported a steady decline in stroke-related mortality over the past three decades.1 However, cerebrovascular diseases remain to be one of the leading causes of morbidity worldwide with more than 80 million people being affected in 2016 alone.1 With a steep decline in mortality rates, long-term sequelae are expected among stroke survivors with staggering costs both for patients and their caregivers. While physical disability and cognitive complications significantly impact on patients’ well-being, studies suggest that persistent depression after stroke is predictive of poor quality of life in the long term.2
Post-stroke depression (PSD) is a growing burden worldwide. It is a common yet often unrecognized post-stroke complication. Sufferers feel hopelessness, increased levels of anxiety and general lack of interest, as well as experiencing sleep alteration.3 It affects one-third of patients with a history of stroke and with incidences highest in the first six months post-stroke and a second peak notable at 18 months after.4–6 In the first three months after a stroke, some of the risk factors identified which increase the risk of PSD include previous mental illness, female gender, age <70, neuroticism, family history, severity of stroke and the level of disability.7 On the other hand, longitudinal studies demonstrated that functional dependence and persistent relationship problems due to the antecedent stroke are the strongest predictors of PSD at 18 months.6
PSD is attributable to various neurochemical and anatomical alterations to their brain, regardless of the severity of the original stroke, and in association with various psychosocial influences.8 Depending on which vascular territory is affected, various cortical and subcortical structures have been noted to manifest mood disorders post-stroke.8 The biological hypothesis is thought to result from a cascade of processes activating the hypothalamic-pituitary axis, leading to altered responses of the neurogenic system and altered energy metabolism.9 Disruption of the glutaminergic system resulting in excitotoxicity may also contribute to the development of PSD, particularly coupled with the chronic, low grade neuroinflammatory state brought on by the patient’s stroke.10,11 Psychosocial variables such as baseline social ties and emotional support along with individual characteristics such as helplessness, passive coping, less acceptance, and perceived benefits have also been shown to impact significantly on PSD etiology.12
Management of PSD is equally complex, necessitating a multi-pronged approach using both pharmacologic and non-pharmacologic measures. Inadequate interventions have been shown to contribute to poor functional outcomes, increased stroke recurrence and increased mortality rates among PSD patients.8 Pharmacologic therapy with antidepressants such as noradrenaline reuptake inhibitors, tricyclic antidepressants and selective serotonin reuptake inhibitors (SSRIs) is undoubtedly a cornerstone of current PSD treatment.13 However, post-stroke patients have been observed to be poorly adherent to pharmacotherapy.14 In a large cohort study involving more than 12,000 patients, nearly half of all PSD patients involved were either poorly adherent to antidepressant regimens or not adherent at all, leading to poor clinical outcomes.14 Polypharmacy is likely a key factor contributing to this poor adherence,15 thus non-pharmacologic approaches are well worth exploring as alternatives.
In a recent Cochrane review of interventions for post-stroke depression, it has been determined that there is no strong evidence to suggest that pharmacologic interventions are effective in reducing depressive symptoms post-stroke.16 These conclusions, however, were drawn based on low-certainty evidence because of various forms of biases and high attrition rates noted in several studies.16 While more robust data are necessary to assess the efficacy of pharmacologic management, the need to evaluate non-pill-based management is likewise imperative which can be utilized as monotherapy or adjunct to the former. This is particularly useful for stroke patients who are prescribed with several medications and may be at a high risk for interactions with antidepressants.17 Its utility is further highlighted in special populations such as the elderly who may have a slightly increased risk for falls with anti-depressant therapy.18 In this narrative review, we discuss various non-pharmacologic approaches for the management of post-stroke depression.
Methodology
A PubMed literature search was performed from September to November 2021. The following topics were included: post-stroke depression; non-invasive brain stimulation; behavioral therapy; psychosocial interventions; acupuncture; exercise therapy; light therapy; music therapy and art therapy. Only literature in English and published in the past 25 years were included in this review. Outcomes of studies included should be various objective measures for the assessment of post-stroke depression. Summary of studies included in this review is outlined in Table 1.
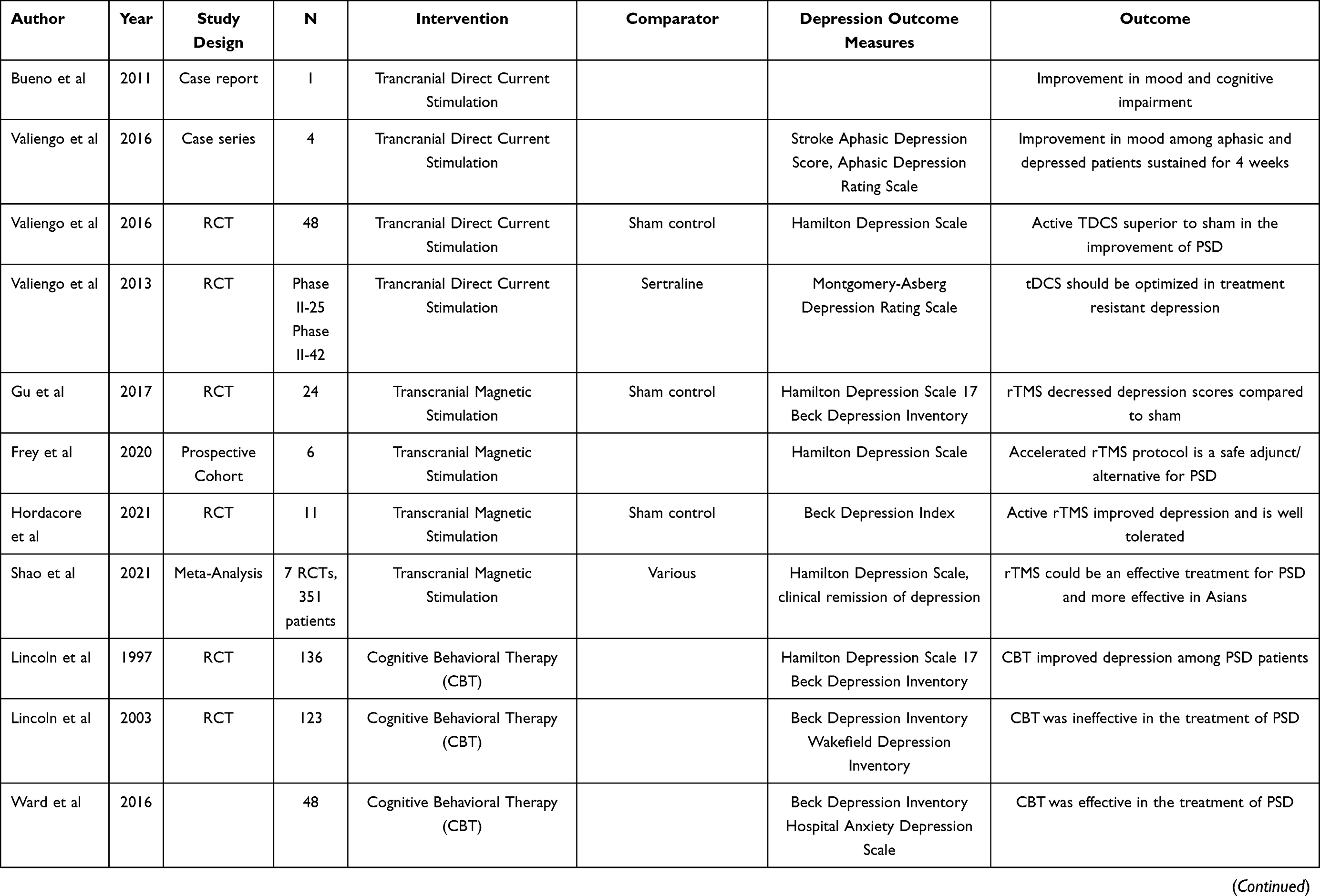 | 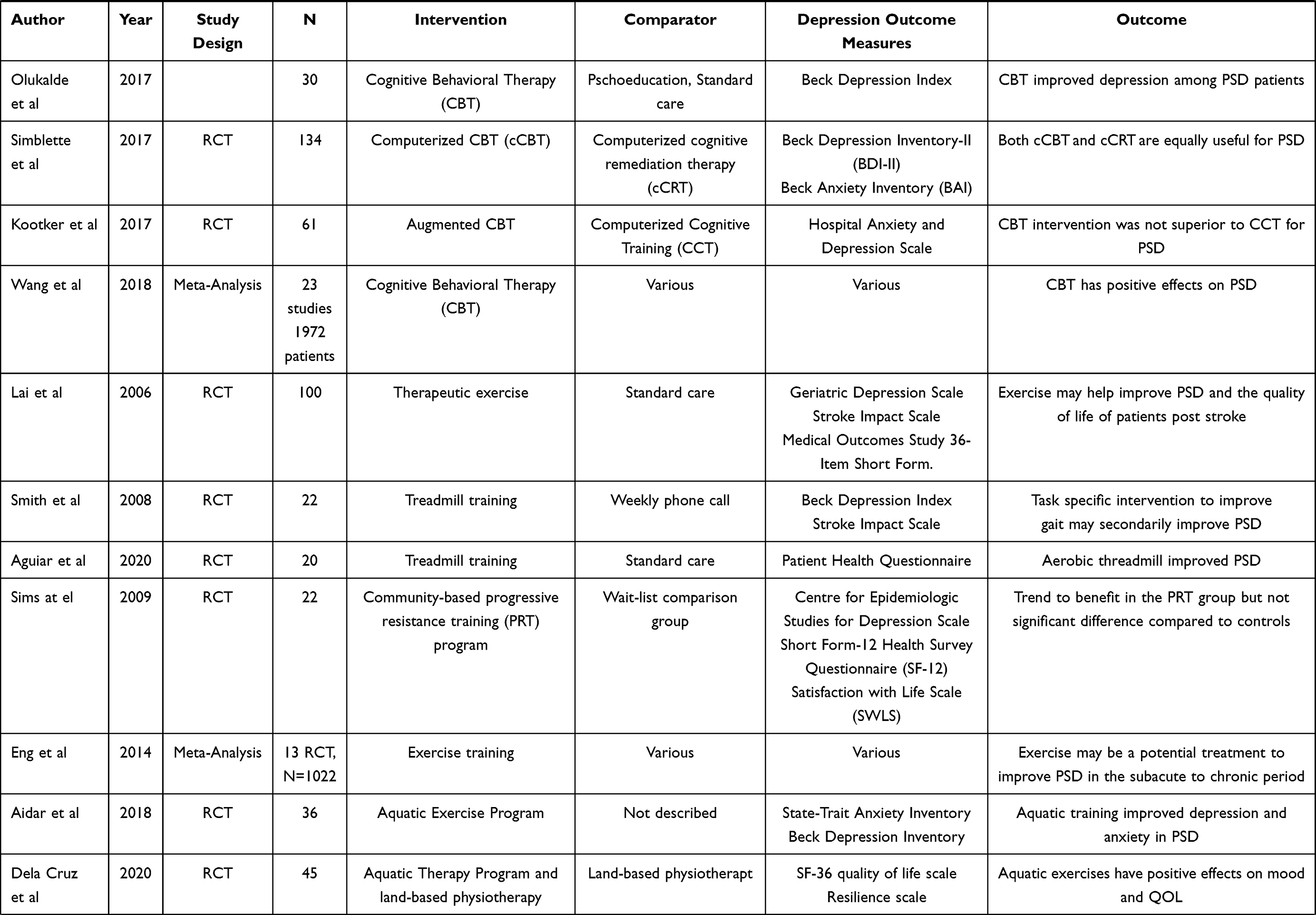 | 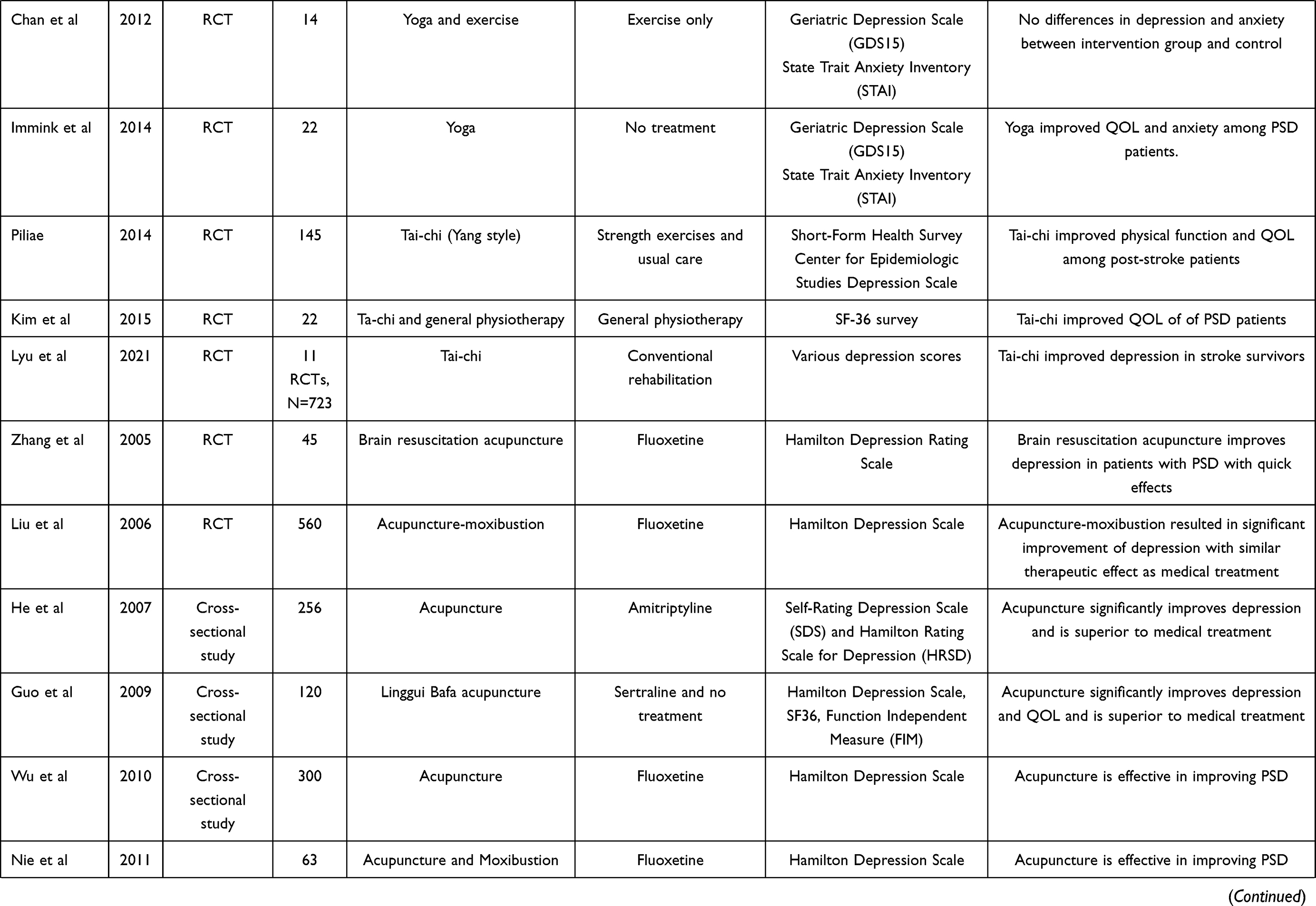 | 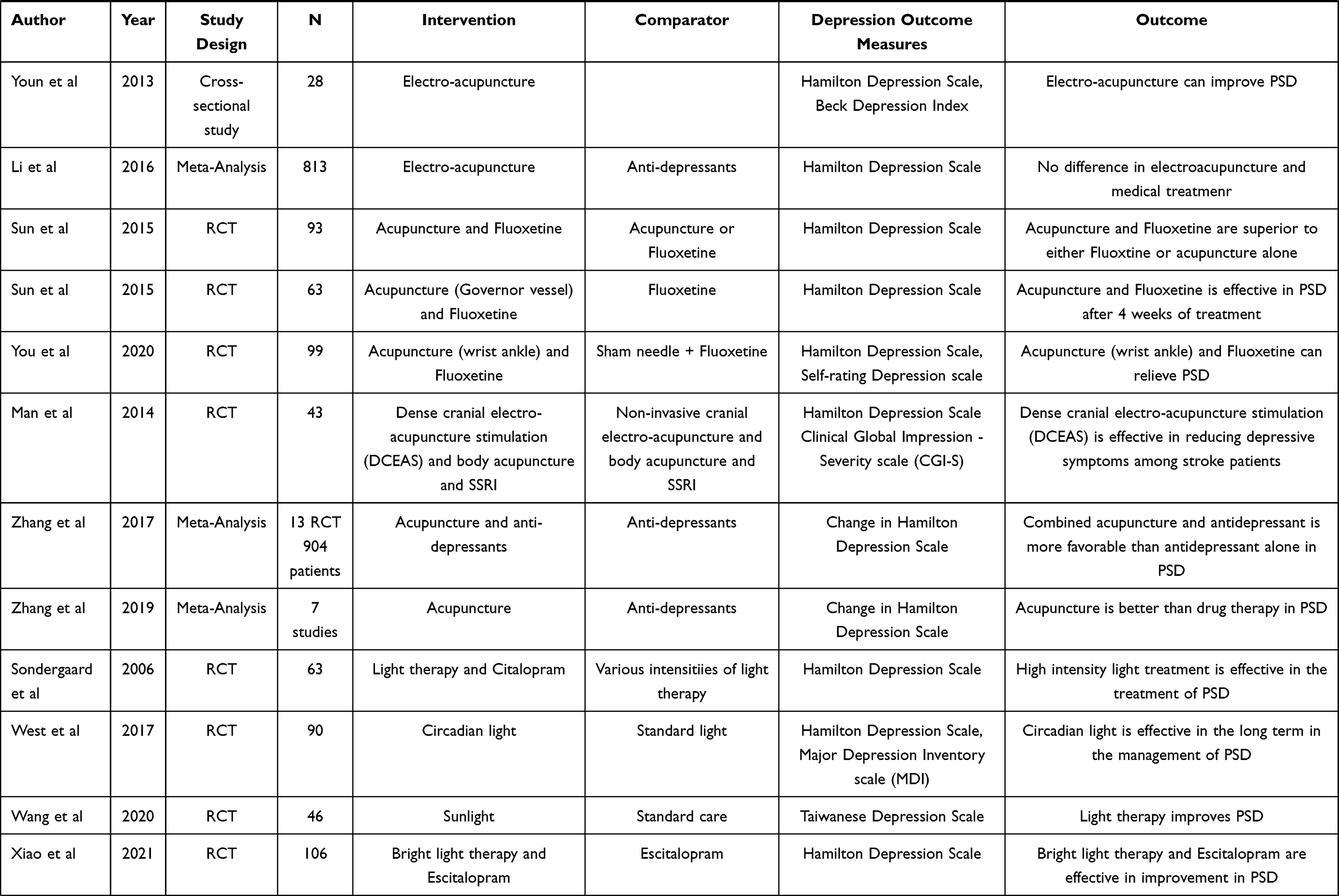 | 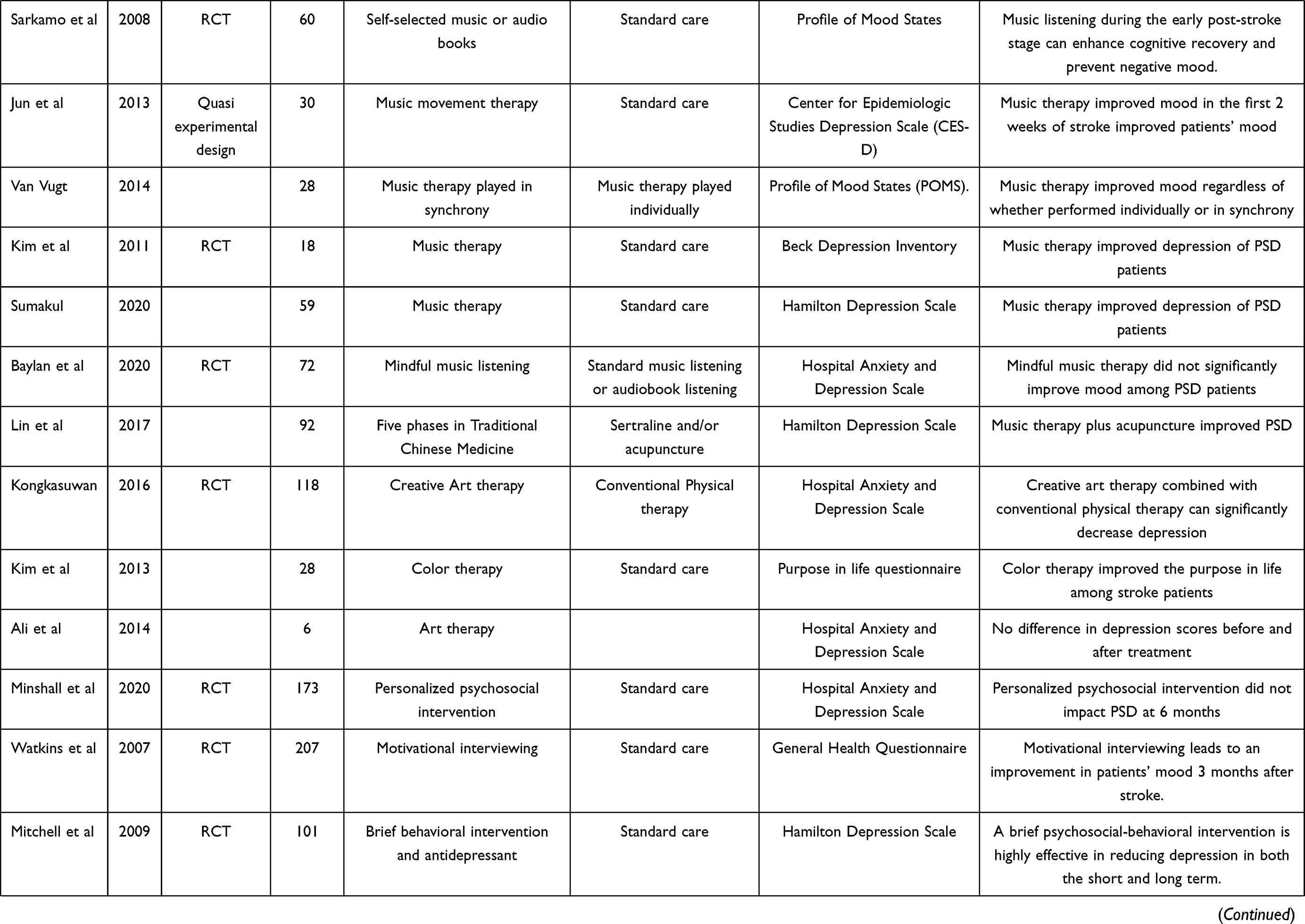 | 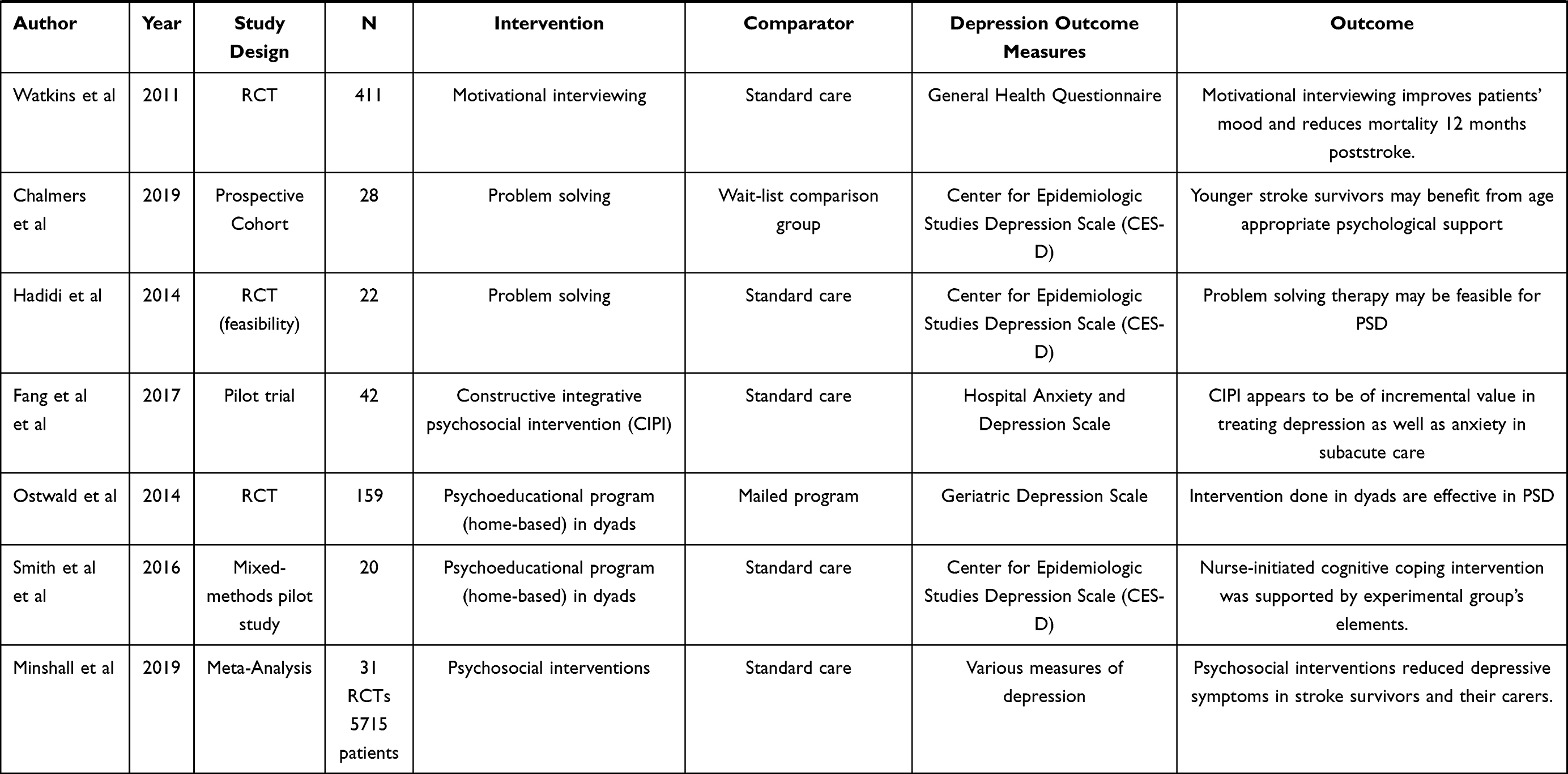 |
Table 1 Summary of Studies on the Non-Pharmacologic Interventions for PSD |
Non-Invasive Brain Stimulation
Non-invasive brain stimulation is an established non-pharmacologic treatment for patients with major depressive disorder. However, its utility in PSD still needs further investigation. Transcranial Direct Current Stimulation (tDCS) is one of the techniques that has been explored in this regard. The earliest reports suggesting tDCS may be potentially beneficial for PSD were published by Bueno et al.19 They reported a significant improvement in the mood and cognition of a post-stroke patient following 30-minute anodal stimulation of the left dorsal prefrontal cortex (DLFPC) for ten days.19 However, immediate relapse was noted three weeks after discontinuation, necessitating the need for further maintenance sessions.19 This regimen was also evaluated among aphasic patients with concomitant depression and bilateral DLFPC stimulation showed more than 50% improvement in their depressive scores.20 Following this, 48 PSD patients were randomised to tDCS and sham treatment over six weeks for a total of 14 sessions.21 This RCT proved that the former was significantly more effective in averting PSD with a number needed to treat of three.21 However, no long-term follow-up was established in this study, and previous studies on non-stroke patients have noted more than 50% relapse following discontinuation of treatment.22 Clearly, more studies on this intervention still need to be done, ideally performed using a larger population and with a longer follow-up period.
Repetitive Transcranial Magnetic Stimulation (rTMS) is another novel intervention in the field of neurorehabilitation. This involves stimulation or inhibition of various neural structures by application of electromagnetic impulses aimed at optimizing neuroplasticity to maintain residual neural function while also acquiring new skills.23 Repetitive Transcranial Magnetic Stimulation targeting the left dorsolateral prefrontal cortex has been beneficial in the management of patients with PSD. In a randomized control trial comparing patients who received ten sessions of 10Hz rTMS to those receiving sham controls, significant decreases in depression scale scores were noted in the former.24 In the Novel TMS for Stroke and Depression (NoTSAD) trial, an accelerated TMS protocol for PSD was employed, consisting of five sessions per day for four consecutive days within the subacute stroke period and likewise revealing beneficial results.25 Another RCT done in Australia provided evidence for the efficacy of high-frequency TMS in the reduction of Beck Depression Scores among PSD patients compared to sham controls.26 In this study, the authors also performed EEG to assess neurophysiologic correlation and noted enhanced theta frequency in the treatment group.26 This is suggestive of improved connectivity between the dorsolateral prefrontal cortex and the parietal cortex, areas potentially compromised in PSD.26 However, this remains speculative due to the small population size of this study. While the benefits of rTMS have likewise been replicated in a meta-analysis of 7 RCTs with 351 patients, its effects are likely limited to a short period.27 Furthermore, subgroup analysis suggests that it may be more effective in Asian subjects, although unblinded techniques in the former may be prohibitive of its generalizability.27 More studies involving more heterogenous populations are needed to assess the efficacy and safety of non-invasive brain stimulation among post-stroke patients developing depression.
Behavioral Therapy
Individualized behavioral therapies are also at the forefront of non-pharmacologic management of PSD. Cognitive behavioral therapy (CBT) is an established intervention rooted on the principle that psychological dilemmas are anchored on maladaptive patterns of thinking and unhelpful behavior.28,29 Techniques employed include distraction, activity scheduling and modification, graded task assignments and others that seek to defy this negative mentality.28
The first study to assess the efficacy of CBT to treat PSD was performed more than two decades ago in the United Kingdom. In this observational study, the authors noted that there might be a likelihood of symptom improvement following 10 CBT sessions for three months.28 However, they also noted that cognitive dysfunction after a stroke may be a limitation to its applicability.28 A randomized control trial initiated in the same institution was done a few years later involving CBT compared with attention placebo intervention and standard care, concluding no differences in depression and functional outcomes.29 Observational and small-scale RCTs, however, showed beneficial results30–33 The effects of a group cognitive behavioral therapy called Brainstorm were evaluated in a group of post-stroke survivors in Australia manifesting depressive symptoms.30 This tool kit involved monitoring of mood and activity and psychoeducation, as well as challenging negative thoughts.30 Depression scores significantly improved from baseline to one month after, however its effects were not sustainable at the end of six months.30 A prospective observational study in Nigeria also showed that, after nine sessions of CBT focused on activity stimulation, negative thoughts and people contacts, patients with PSD had better emotional well-being compared to controls.31 Computerized CBT has also been explored in the past but did not prove superior over conventional CBT although only feasibility trials and studies with small population are available to date.32,33 There is also an ongoing RCT on the use of an CBT-based iPAD application promoting self-reinforcement and positivity being performed among Japanese patients.34 Overall, it appears that CBT showed more improvement and higher remission and response rates with concomitant improvement in anxiety and functional neurological outcomes.35 To date, recent clinical guidelines in stroke rehabilitation recommend CBT as monotherapy or adjuvant to standard medical therapy among patients with PSD.36
Psychosocial Interventions
Psychosocial interventions prove to be an essential component for the management of PSD. As patients and their caregivers have a marked reduction in social participation and functioning after a stroke, approaches that involve motivational interviewing, transitional care, social support, and psychoeducation should be integral in stroke rehabilitation37 On an individual patient level, exploration of their respective needs, assessment of the potential barriers and supporting the skills and networks needed to achieve this has been suggested as an essential framework for recovery.38 These strategies should eventually aim to achieve self-efficacy, a factor which has been shown to be negatively associated with PSD.39,40
Various studies have provided evidence on the value of motivational interviewing and comprehensive psychosocial interventions for the improvement of post-stroke mood disorders.41,42 Motivational interviewing, described as patient-centered and talk-based therapy has been shown to improve PSD at three months and one year.41,43 The Living Well with Stroke study also showed that a brief psychosocial-behavioral intervention over a period of eight weeks in conjunction with antidepressant medication has sustained benefits for PSD until two years.42 A trend towards more beneficial effect has also been seen in problem-solving therapy to reduce post-stroke emotional distress in young and elderly stroke survivors.44,45 A more comprehensive approach called constructive integrative psychosocial intervention has been proposed by Fang et al. This method reinforces positive construction of experiences by the patient regarding his or her illness by incorporating psychoeducation, sharing of experiences in relation to previous illnesses, crisis management and activity participation.46
A dyadic approach which involves psycho-intervention for both caregivers and stroke patients has also been shown to be useful in the management of PSD in the latter.47,48 A home-based psycho-educational program over a six-month period for both the stroke patient and their spouses has demonstrated positive impact in the dyad’s depressive symptoms.47 Similar conclusions were drawn in another study where psychoeducational interventions were provided for stroke survivors and their spouses.48 A meta-analysis of 11 studies highlighted that psychosocial interventions focusing on the patients, caregivers or both have ameliorating effects in PSD.49 It is in this reason that authors emphasize the need to shift psycho-intervention for PSD towards a dyad approach in which the patient and the caregiver is considered a solitary unit.50 Guidelines have also stressed the need for psychosocial interventions such as motivation interviewing and problem-solving therapy before commencing anti-depressant medications for PSD.51 While the beneficial effects of this are promising, its main limitation is that it is largely human-resource intensive and that it can be time consuming. However, the evolving concepts of post-stroke neurorehabilitation post-stroke should focus on a wholistic and a biopsychosocial approach to reduce the improvement in the quality of life afflicted by post-stroke depression.
Exercise Therapy
Exercise is an important cornerstone in neurorehabilitation as it promotes neural alterations at the structural and biochemical level. Even if not structurally altered by the stroke process, there is evidence that alterations to the neuroplasticity of the hippocampus play an essential role in post-stroke depression52,53 Accumulating evidence from biochemical studies show that exercise increases the mBDNF/proBDNF ratio, which is one of the key biomarkers involved in the promotion of hippocampal neuroplasticity.52 Another neurochemical involved in PSD is phosphatase and tensin homologue (PTEN), a known tumor suppressor. Upregulation of this leads to neuronal apoptosis in the hippocampus.53 Experimental studies have shown that in mice models exercise induces PTEN downregulation, which results in t reduced levels of the inflammatory neurochemicals TLR4, NF-κB and NLRP3, all ameliorating PSD.54
Clinical studies also show substantial evidence that exercise promotes improvement in mood disorders post-stroke. One of the first randomised clinical trials examining the effect of a three-month structured exercise program on the occurrence of PSD among 100 stroke survivors was conducted in 2006.55 In this study, Lai et al noted that after three months PSD occurred in 14% of the subjects in the intervention group and 35% in controls (p = 0.03).55 After nine months percentages were still numerically lower in the experimental group, albeit not to statistically significant levels.55 Whilst aerobic exercises have been shown to be useful in improving gait and mobility after a stroke, clinical studies likewise confirm their secondary effect on PSD.56 Targeting aerobic training to achieve 60–80% of the heart rate reserve has been shown to be beneficial not only for the alleviation of PSD but also for overall quality of life.56 Apart from aerobic training, other exercise programs such as functional and resistance programs are also thought beneficial for PSD.57 Resistance training has the advantage of lesser incidence of falls, particularly critical for post stroke patients with balance and mobility issues.58 A study involving a community-based progressive resistance training regimen consisting of moderate-intensity exercises using machine weights documented reduced depression scores in the intervention group.58 Corollary to this, a meta-analysis of 13 studies involving more than 1700 stroke patients reported a beneficial effect among those undergoing structured exercises, with notable effects in the first six months post stroke.59 The same study also concludes that those involved in high-intensity programs, defined as at least 150 minutes of cardiorespiratory, resistance and aerobic activities, achieved the greatest benefit.59
Other forms of exercises have likewise been helpful for mood-related disorders after a stroke. Regular aquatic exercise consisting of two sessions per week each lasting for 45–60 minutes over a 12-week period has been shown to improve depression measures among PSD patients60 The authors argued that improvement in mood seems to be correlated with improvement of mobility.60 A novel form of aquatic therapy known as Ai Chi has also been shown to be beneficial. This form of therapy integrates body coordination and involves specific breathing exercises.61 A study performed in 45 patients who underwent alternating Ai Chi and usual physiotherapy had the advantage over controls, showing better mood and improved quality of life.61 Aquatic therapy has the additional advantage of providing additional external stimulation such as buoyancy and viscosity, which may impact neuroplasticity.62 While this form of therapy is largely trainer and resource dependent, it is generally deemed to be a safe and effective means of treatment in the motor and non-motor aspects of post-stroke rehabilitation.
Mind-body exercises also seem to be a promising form of neurorehabilitation among depressed post-stroke patients. This form of therapy integrates the body, spirit, and the external environment to promote a holistic sense of well-being.63 A complementary type of medicine which has originated in South Asia, yoga is a form of mind-body exercise which has demonstrated positive effects among patients with stroke. While yoga involves dynamic body positions, it has been proposed that yoga asana can be useful among post-stroke patients with significant limitations in their mobility.64 One of the first clinical trials looking at the impact of yoga in depression and anxiety post stroke was performed by Chan et al.65 In this small-scale randomized control trial performed in Australia, patients undergoing yoga in combination with usual post-stroke rehabilitation exercise had greater improvement in terms of anxiety and depression, although not statistically significant differences compared to controls.65 A few years later, another study provided evidence on the benefit of yoga asana in the mood-related complications of stroke with persistent hemiparesis.66 Tai Chi is another form of mind-body exercise which integrates martial arts and relaxation techniques. After a 12-week period of regular Yang tai chi exercises, a randomised control trial involving 145 patients with stroke demonstrated significant improvement in their physical function, fall rates and quality of life.67 The majority of studies looking at the effect of Tai Chi on PSD were performed in Asia and showed positive results,68–70 and its beneficial effect has also been confirmed in a meta-analysis of 11 RCTs.70 While the exact mechanism by which Tai Chi promotes emotional well-being in acute stroke is uncertain, it has been hypothesized that it largely impacts the prefrontal cortex, which modulates inputs from neural structures involved in mood stabilization.71 While most of these studies suggest mind-body exercises have beneficial effects regarding PSD, high-quality evidence is needed to substantiate these claims. As side effects are minimal, it is regardless not unreasonable to integrate these regimens in standard neurorehabilitative techniques.
Acupuncture
Acupuncture is an old yet fundamental aspect of Chinese traditional medicine. Various observational studies and clinical trials validate its use in PSD. Experimental studies in rat models show that the effectiveness of acupuncture in PSD lies in its effects in the PI3K/Akt/mTOR signaling pathway and its inhibition of hippocampal neuronal cell death.72 In addition to this, it may also be helpful in restoring the equilibrium of various hippocampal neurotransmitters such as norepinephrine, serotonin and dopamine.72,73
The first randomised clinical trial to evaluate the efficacy of Acupuncture in PSD was done in 2005 and compared it to Fluoxetine.74 Compared to controls receiving Fluoxetine, acupuncture showed no significant difference as measured by the HAM-D scores.74 However, the same study showed that onset of antidepressant effect was faster in the experimental group and free of side effects.74 Other studies have likewise shown no difference in treatment effects between medical and acupuncture groups.75 On the other hand, some literature has instead shown the superiority of acupuncture among PSD patients compared to Fluoxetine.76 In a randomized control trial of more than 270 patients, He et al noted a superior therapeutic effect of acupuncture performed twice a day for one month, with a notable improvement in Self-Rating Depression Hamilton Depression scales.76 Nie et al also observed that the onset of the therapeutic effect of Acupuncture Moxibustion is notable as early as the 2nd week of treatment and is superior to Paroxetine.79 Observational and randomized control trials also prove the superiority of Acupuncture over Fluoxetine and Sertraline after two and six months of intervention, respectively.77,78 Furthermore, it has also been suggested that patients with good motor function at onset who have received acupuncture for at least a month show a greater degree of improvement in their scores in the Beck Depression and HRDS compared to those with severe motor disability.81 Overall, a meta-analysis of randomized control trials involving more than 1500 patients did not show any significant difference in treatment effects in the acupuncture group compared to controls receiving antidepressants such as Fluoxetine, Citalopram and Sertraline, however, lesser adverse effects were noted in the former.82
It appears that combination therapy consisting of acupuncture and medical therapy is more effective than medical therapy alone in the management of PSD. Sun et al performed an RCT comparing patients receiving acupuncture and Fluoxetine versus acupuncture alone.83 Anchored on the midnight-noon ebb-flow theory, the ziwuliuzhu technique in combination with an antidepressant was more effective at alleviating mood symptoms than acupuncture alone.84 The same trend was observed in a single-blinded randomized control trial comparing PSD patients undergoing wrist-ankle acupuncture in combination with fluoxetine therapy versus sham control and fluoxetine treatment.85 Using depression and quality of life scales as outcome measures, the treatment group demonstrated greater improvement in depressive symptoms compared to controls.85 Another novel acupuncture technique that has been explored is the dense cranial electroacupuncture stimulation (DCEAS).86 This involves the principle of deep brain stimulation and delivers electrical activity at forehead acupoints, directly activating the sensory afferent pathways of the trigeminal nerves.86 Patients who received DCEAS in combination with SSRI and body electroacupuncture had better outcomes as measured by the Hamilton Depression Rating Scale (HAMD-17) and the Clinical Global Impression-Severity scale (CGI-S), and improvements have been noted as early as one week post treatment86 Two recent meta-analyses in 2019 and 2020 corroborate these findings, concluding that acupuncture combined with conventional drug therapy is more effective versus standard antidepressant alone.87,88 However, both studies recommend higher quality RCTs to increase confidence for recommendation. To date, the American Heart Association (AHA) recommends acupuncture as an add-on management for post-stroke complications such as dysphasia and shoulder pain, but not specifically for post-stroke depression.89
Light Therapy
Light therapy is considered a traditional form of Western Medicine and has been extensively used in the 19th century in the management of various diseases.90 In the modern day, this is otherwise known as brain photobiomodulation therapy and has been used in the management of various neuropsychiatric conditions.91,92 The antidepressant effect of light therapy lies in its effect on the retino-geniculo-habenular pathway, circuitry likely involved in depression and other mood disorders.93 At the molecular level, light therapy stimulates ATP synthesis via the mitochondrial respiratory chain and activates various pathways leading to neuronal and synaptic regeneration.94 Sondergaard et al were the first to explore the utility of light therapy in PSD (Sondergaard). In a randomized, double-blind study, the effect of high versus medium intensity artificial light therapy was evaluated among PSD patients taking escitalopram.95 Results showed that month-long high dose light therapy was more effective in the improvement of PSD symptoms than controls.95 Among admitted stroke patients, researchers from a Danish hospital observed that those receiving circadian lighting or the blue light spectrum had significantly lower Hamilton Rating Scale for Depression (HAM-D6) and Major Depression Inventory scale (MDI) scores post treatment.96 Alternatively, natural light exposure has also been shown to produce the same effects. Consistent sunlight exposure for at least 30 minutes per day for at least 14 days has been associated with improvement in the depression scores among Taiwanese patients.97 Not only does it improve mood among PSD patients, but light therapy has also likewise been shown to ameliorate insomnia in the same subset of patients.98 This is also very well tolerated with treatment-related adverse effects not significantly different from controls.98 While it is a generally safe treatment regimen for a variety of affective disorder, its use in PSD to date remains exploratory.
Music Therapy
Music therapy is another technique widely used in neurorehabilitation and is an accepted therapy for patients with mood disorders and other acquired brain injuries. It capitalizes on the principles of neuroplasticity by multisensory stimulation and consolidation of inputs from the frontal, parietal, temporal and occipital regions.99 Music medicine interventions are distinct from recreational music as the former usually involves a professionally trained music trainer who implements a specific type of music at the range of rhythmic auditory stimulation tailored to every patient’s experiences and needs.100
There is considerable information on the beneficial effects of music therapy for PSD. Sarkamo et al looked at how music impacted the mood of patients with middle cerebral artery infarcts in the acute setting.101 This single blind RCT reported that, among 60 patients involved in the study, there was a greater trend to improvement in depression in the intervention group than in controls at the end of three and six months, but this did not reach statistically significant differences.101 It is likely that the concomitant improvement in physical function and fine motor skills of patients within the acute to subacute period after undergoing music therapy contributes to the improvement of their mood and their sense of well-being.102,103 In the subacute to chronic post-stroke period, Korean stroke patients were likewise subjected to 40-minute structured music therapy in a four-week period.104 Depression scores as measured by the Beck Depression Inventory were lower in those participating in these sessions.104 The authors argued that this is likely related to how music also helps improve anxiety and pain perception.104 It appears that other forms of music therapy are also equally effective. Among Indonesian PSD patients, 30 minutes of instrumental music therapy in combination with standard home-based therapy was found effective at PSD alleviation.105 In the same way, mindfulness music, which integrates a brief period of mindfulness exercises, has also been shown to be beneficial.106 Additionally, traditional Chinese music following a five-phase music therapy has also been evaluated regarding its impact on affective disorders post-stroke.107 When combined with acupuncture, it provides more substantial reduction in depression scores among post-stroke patients.107 While the results of these studies are promising, a systematic review found that these studies are underpowered to assess efficacy.108 Furthermore, they reported significant heterogeneity between studies, which may preclude bias-free conclusions.108 The same findings were documented in a Cochrane systematic review on the effect of music interventions in acquired brain injury including stroke.100 Clearly, more well-controlled clinical trials are needed to allow unbiased conclusions to be formed.
Art Therapy
Art therapies are unrecognized regimens which may regardless be useful for PSD patients. Art therapy has been deemed particularly helpful for post-stroke patients as it provides them a method of venting conflicts and emotions, thus alleviating their mental and emotional concerns.109 Its utility in neurorehabilitation is based on the Hebbian principle of neuroplasticity, in which multimodal stimulation initiates neuronal activation leading to increased synaptogenesis.110 Kongkasuwan et al demonstrated that creative art therapy provided in an inpatient group setting significantly improved post-stroke patients’ mood, physical function and quality of life.111 In addition, positive changes in concentration, emotion, self-confidence and motivation were also appreciable among patients subjected to art therapy.111 Color therapy was also used in a cohort of Korean post-stroke patients in another study seeking to determine whether it impacted their “purpose in life”.112 In this study, a color transition was observed from monochromatic choices and colors of low tone early in the course of therapy to polychromatism and use of increased color tones towards the end of the rehabilitation period among patients with PSD.112 This pattern of color transition seems to correlate with improvement in their purpose in life objective measures.112 Interestingly, iPad art therapies seem to provide benefits as well regarding PSD. In a study by Ali et al, they demonstrated that art therapy supervised by psychotherapists over a six-week period provided some improvement in the Hospital and Anxiety Scores (HAD) of enrolled patients. While this exploratory study only involved six patients, the authors propose that this technique is feasible and should be further explored in a larger population.113
Conclusion
Non-pharmacologic interventions are an essential adjuvant in the management of post-stroke depression. These regimes work by activating pre and postsynaptic connections in the juxta and regions remote from stroke lesions, facilitating neuroplasticity and neuronal reactivation. Interventions such as non-invasive brain stimulation, acupuncture, behavioral and psychosocial approaches have been incorporated in some clinical guidelines while exercise, music, light, and art therapy remain investigational. While the effects of non-pharmacologic interventions are promising, more robust, large-sample studies are necessary to evaluate its efficacy in the short or long term. There is also a need to explore further on whether these interventions are effective as monotherapy or adjunctive treatment to antidepressant medications.
Funding
There is no funding to report.
Disclosure
Tissa Wijeratne and Carmela Sales share equal first author status. The authors report no conflicts of interest in this work.
References
1. Johnson CO, Nguyen M, Roth GA; GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439–458. PMID: 30871944; PMCID: PMC6494974. doi:10.1016/S1474-4422(19)30034-1
2. Li LJ, Yao XM, Guan BY, Chen Q, Zhang N, Wang CX. Persistent depression is a predictor of quality of life in stroke survivors: results from a 5-year follow-up study of a Chinese cohort. Chin Med J. 2019;132(18):2206–2212. PMID: 31436596; PMCID: PMC6797138. doi:10.1097/CM9.0000000000000400
3. Gabaldón L, Fuentes B, Frank-García A, Díez-Tejedor E. Poststroke depression: importance of its detection and treatment. Cerebrovasc Dis. 2007;24 Suppl 1(1):181–188. PMID: 17971654. doi:10.1159/000107394
4. Paul N, Das S, Hazra A, et al. Depression among stroke survivors: a community-based, prospective study from Kolkata, India. Am J Geriatr Psychiatry. 2013;21(9):821–831. PMID: 23871116. doi:10.1016/j.jagp.2013.03.013
5. De Ryck A, Fransen E, Brouns R, et al. Poststroke depression and its multifactorial nature: results from a prospective longitudinal study. J Neurol Sci. 2014;347(1–2):159–166. PMID: 25451004. doi:10.1016/j.jns.2014.09.038
6. De Ryck A, Fransen E, Brouns R, et al. Psychosocial problems associated with depression at 18 months poststroke. Int J Geriatr Psychiatry. 2014;29(2):144–152. PMID: 23625635. doi:10.1002/gps.3974
7. Shi Y, Yang D, Zeng Y, Wu W. Risk factors for post-stroke depression: a meta-analysis. Front Aging Neurosci. 2017;9:218. PMID: 28744213; PMCID: PMC5504146. doi:10.3389/fnagi.2017.00218
8. Wijeratne T, Sales C. Understanding why post-stroke depression may be the norm rather than the exception: the anatomical and neuroinflammatory correlates of post-Stroke depression. J Clin Med. 2021;10(8):1674. PMID: 33919670; PMCID: PMC8069768. doi:10.3390/jcm10081674
9. Villa RF, Ferrari F, Moretti A. Post-stroke depression: mechanisms and pharmacological treatment. Pharmacol Ther. 2018;184:131–144. PMID: 29128343. doi:10.1016/j.pharmthera.2017.11.005
10. Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry. 2020;66:70–80. PMID: 32717644. doi:10.1016/j.genhosppsych.2020.06.011
11. Wijeratne T, Sales C, Menon R, Karimi L, Jakovljevic M. Highlighting the role of universally available and innate immune cell counts in acute ischemic stroke: a scoping review. Sustainability. 2021;13(7):4069. doi:10.3390/su13074069
12. Glymour MM, Weuve J, Fay ME, Glass T, Berkman LF. Social ties and cognitive recovery after stroke: does social integration promote cognitive resilience? Neuroepidemiology. 2008;31(1):10–20. PMID: 18535395; PMCID: PMC2794277. doi:10.1159/000136646
13. Deng L, Sun X, Qiu S, et al. Interventions for management of post-stroke depression: a Bayesian network meta-analysis of 23 randomized controlled trials. Sci Rep. 2017;7(1):16466. PMID: 29184194; PMCID: PMC5705605. doi:10.1038/s41598-017-16663-0
14. Krivoy A, Stubbs B, Balicer RD, et al. Low adherence to antidepressants is associated with increased mortality following stroke: a large nationally representative cohort study. Eur Neuropsychopharmacol. 2017;27(10):970–976. PMID: 28886897. doi:10.1016/j.euroneuro.2017.08.428
15. Tajeu GS, Kent ST, Kronish IM, et al. Trends in antihypertensive medication discontinuation and low adherence among medicare beneficiaries initiating treatment from 2007 to 2012. Hypertension. 2016;68(3):565–575. PMID: 27432867; PMCID: PMC5215087. doi:10.1161/HYPERTENSIONAHA.116.07720
16. Allida S, Cox KL, Hsieh CF, House A, Hackett ML. Pharmacological, psychological and non-invasive brain stimulation interventions for preventing depression after stroke. Cochrane Database Syst Rev. 2020;5(5):CD003689. PMID: 32390167; PMCID: PMC7211517. doi:10.1002/14651858.CD003689.pub4
17. Jennum P, Baandrup L, Iversen HK, Ibsen R, Kjellberg J. Mortality and use of psychotropic medication in patients with stroke: a population-wide, register-based study. BMJ Open. 2016;6(3):e010662. PMID: 26956165; PMCID: PMC4785303. doi:10.1136/bmjopen-2015-010662
18. Flint AJ, Iaboni A, Mulsant BH, Rothschild AJ, Whyte EM, Meyers BS; STOP-PD Study Group. Effect of sertraline on risk of falling in older adults with psychotic depression on olanzapine: results of a randomized placebo-controlled trial. Am J Geriatr Psychiatry. 2014;22(4):332–336. PMID: 23642462; PMCID: PMC3805752. doi:10.1016/j.jagp.2013.01.067
19. Bueno VF, Brunoni AR, Boggio PS, Bensenor IM, Fregni F. Mood and cognitive effects of transcranial direct current stimulation in post-stroke depression. Neurocase. 2011;17(4):318–322. PMID: 21213180. doi:10.1080/13554794.2010.509319
20. Valiengo L, Casati R, Bolognini N, et al. Transcranial direct current stimulation for the treatment of post-stroke depression in aphasic patients: a case series. Neurocase. 2016;22(2):225–228. PMID: 26743441. doi:10.1080/13554794.2015.1130231
21. Valiengo LC, Goulart AC, de Oliveira JF, Benseñor IM, Lotufo PA, Brunoni AR. Transcranial direct current stimulation for the treatment of post-stroke depression: results from a randomised, sham-controlled, double-blinded trial. J Neurol Neurosurg Psychiatry. 2017;88(2):170–175. PMID: 27815324. doi:10.1136/jnnp-2016-314075
22. Valiengo L, Benseñor IM, Goulart AC, et al. The sertraline versus electrical current therapy for treating depression clinical study (select-TDCS): results of the crossover and follow-up phases. Depress Anxiety. 2013;30(7):646–653. PMID: 23625554. doi:10.1002/da.22079
23. León Ruiz M, Rodríguez Sarasa ML, Sanjuán Rodríguez L, Benito-León J, García-Albea Ristol E, Arce Arce S. Current evidence on transcranial magnetic stimulation and its potential usefulness in post-stroke neurorehabilitation: opening new doors to the treatment of cerebrovascular disease. Neurologia. 2018;33(7):459–472. English, Spanish. PMID: 27161423. doi:10.1016/j.nrl.2016.03.008
24. Gu SY, Chang MC. The effects of 10-Hz repetitive transcranial magnetic stimulation on depression in chronic stroke patients. Brain Stimul. 2017;10(2):270–274. PMID: 27839722. doi:10.1016/j.brs.2016.10.010
25. Frey J, Najib U, Lilly C, Adcock A. Novel TMS for stroke and depression (NoTSAD): accelerated repetitive transcranial magnetic stimulation as a safe and effective treatment for post-stroke depression. Front Neurol. 2020;11:788. PMID: 32849235; PMCID: PMC7431489. doi:10.3389/fneur.2020.00788
26. Hordacre B, Comacchio K, Williams L, Hillier S. Repetitive transcranial magnetic stimulation for post-stroke depression: a randomised trial with neurophysiologicalinsight. J Neurol. 2021;268(4):1474–1484. PMID: 33219421. doi:10.1007/s00415-020-10315-6
27. Shao D, Zhao ZN, Zhang YQ, et al. Efficacy of repetitive transcranial magnetic stimulation for post-stroke depression: a systematic review and meta-analysis of randomized clinical trials. Braz J Med Biol Res. 2021;54(3):e10010. PMID: 33470386; PMCID: PMC7812912. doi:10.1590/1414-431X202010010
28. Lincoln NB, Flannaghan T, Sutcliffe L, Rother L. Evaluation of cognitive behavioural treatment for depression after stroke: a pilot study. Clin Rehabil. 1997;11(2):114–122. PMID: 9199863. doi:10.1177/026921559701100204
29. Lincoln NB, Flannaghan T. Cognitive behavioral psychotherapy for depression following stroke: a randomized controlled trial. Stroke. 2003;34(1):111–115. PMID: 12511760. doi:10.1161/01.str.0000044167.44670.55
30. Ward SK, Turner A, Hambridge JA, et al. Group cognitive behavioural therapy for stroke survivors with depression and their carers. Top Stroke Rehabil. 2016;23(5):358–365. doi:10.1080/10749357.2016.1143706
31. Olukolade O, Osinowo HO. Efficacy of cognitive rehabilitation therapy on poststroke depression among survivors of first stroke attack in Ibadan, Nigeria. Behav Neurol. 2017;2017:4058124. PMID: 28720980; PMCID: PMC5504925. doi:10.1155/2017/4058124
32. Simblett SK, Yates M, Wagner AP, et al. Computerized cognitive behavioral therapy to treat emotional distress after stroke: a feasibility randomized controlled trial. JMIR Ment Health. 2017;4(2):e16. PMID: 28566265; PMCID: PMC5471343. doi:10.2196/mental.6022
33. Kootker JA, Rasquin SM, Lem FC, van Heugten CM, Fasotti L, Geurts AC. Augmented cognitive behavioral therapy for poststroke depressive symptoms: a randomized controlled trial. Arch Phys Med Rehabil. 2017;98(4):687–694. PMID: 27847195. doi:10.1016/j.apmr.2016.10.013
34. Uchida H, Hiragaki Y, Nishi Y, et al. An iPad application-based intervention for improving post-stroke depression symptoms in a convalescent rehabilitation ward: a pilot randomized controlled clinical trial protocol. Internet Interv. 2020;21:100340. PMID: 32944505; PMCID: PMC7481559. doi:10.1016/j.invent.2020.100340
35. Wang SB, Wang YY, Zhang QE, et al. Cognitive behavioral therapy for post-stroke depression: a meta-analysis. J Affect Disord. 2018;235:589–596. PMID: 29704854. doi:10.1016/j.jad.2018.04.011
36. Lanctôt KL, Lindsay MP, Smith EE, et al.; Management of Mood, Cognition and Fatigue Following Stroke Best Practice Writing Group, the Heart & Stroke Canadian Stroke Best Practices and Quality Advisory Committee; in collaboration with the Canadian Stroke Consortium. Canadian stroke best practice recommendations: mood, cognition and fatigue following stroke, 6th edition update 2019. Int J Stroke. 2020; 15(6):668–688. PMID: 31221036. doi:10.1177/1747493019847334
37. Minshall C, Castle DJ, Thompson DR, et al. A psychosocial intervention for stroke survivors and carers: 12-month outcomes of a randomized controlled trial. Top Stroke Rehabil. 2020;27(8):563–576. PMID: 32191569. doi:10.1080/10749357.2020.1738677
38. Woodman P, Riazi A, Pereira C, Jones F. Social participation post stroke: a meta-ethnographic review of the experiences and views of community-dwelling stroke survivors. Disabil Rehabil. 2014;36(24):2031–2043. PMID: 24597937. doi:10.3109/09638288.2014.887796
39. Chau JPC, Lo SHS, Zhao J, et al. Factors associated with post-stroke depression in Chinese stroke survivors. J Stroke Cerebrovasc Dis. 2021;30(11):106076. PMID: 34507255. doi:10.1016/j.jstrokecerebrovasdis.2021.106076
40. Chau JPC, Lo SHS, Zhao J, et al. Validation of a translated Chinese version of the participation strategies self-efficacy scale: a cross-sectional study. Disabil Rehabil. 2021:1–7. PMID: 34061687. doi:10.1080/09638288.2021.1933220
41. Watkins CL, Auton MF, Deans CF, et al. Motivational interviewing early after acute stroke: a randomized, controlled trial. Stroke. 2007;38(3):1004–1009. PMID: 17303766. doi:10.1161/01.STR.0000258114.28006.d7
42. Mitchell PH, Veith RC, Becker KJ, et al. Brief psychosocial-behavioral intervention with antidepressant reduces poststroke depression significantly more than usual care with antidepressant: living well with stroke: randomized, controlled trial. Stroke. 2009;40(9):3073–3078. PMID: 19661478; PMCID: PMC2777736. doi:10.1161/STROKEAHA.109.549808
43. Watkins CL, Wathan JV, Leathley MJ, et al. The 12-month effects of early motivational interviewing after acute stroke: a randomized controlled trial. Stroke. 2011;42(7):1956–1961. PMID: 21700946. doi:10.1161/STROKEAHA.110.602227
44. Chalmers C, Leathem J, Bennett S, McNaughton H, Mahawish K. The efficacy of problem solving therapy to reduce post stroke emotional distress in younger (18–65) stroke survivors. Disabil Rehabil. 2019;41(7):753–762. PMID: 29172817. doi:10.1080/09638288.2017.1408707
45. Hadidi NN, Lindquist R, Buckwalter K, Savik K. Feasibility of a pilot study of problem-solving therapy for stroke survivors. Rehabil Nurs. 2015;40(5):327–337. PMID: 24711062. doi:10.1002/rnj.148
46. Fang Y, Mpofu E, Athanasou J. Reducing depressive or anxiety symptoms in post-stroke patients: pilot trial of a constructive integrative psychosocial intervention. Int J Health Sci. 2017;11(4):53–58. PMID: 29085269; PMCID: PMC5654182.
47. Ostwald SK, Godwin KM, Cron SG, Kelley CP, Hersch G, Davis S. Home-based psychoeducational and mailed information programs for stroke-caregiving dyads post-discharge: a randomized trial. Disabil Rehabil. 2014;36(1):55–62. PMID: 23594060. doi:10.3109/09638288.2013.777806
48. Robinson-Smith G, Harmer C, Sheeran R, Bellino Vallo E. Couples’ coping after stroke-A pilot intervention study. Rehabil Nurs. 2016;41(4):218–229. PMID: 25865578. doi:10.1002/rnj.213
49. Minshall C, Pascoe MC, Thompson DR, et al. Psychosocial interventions for stroke survivors, carers and survivor-carer dyads: a systematic review and meta-analysis. Top Stroke Rehabil. 2019;26(7):554–564. PMID: 31258017. doi:10.1080/10749357.2019.1625173
50. McCarthy MJ, Lyons KS, Powers LE. Expanding poststroke depression research: movement toward a dyadic perspective. Top Stroke Rehabil. 2011;18(5):450–460. PMID: 22082696. doi:10.1310/tsr1805-450
51. Rudd A, Bowen A, Young G, James M. The latest national clinical guideline for stroke. Clin Med. 2017;17(2):154–155. doi:10.7861/clinmedicine.17-2-154
52. Luo L, Li C, Deng Y, Wang Y, Meng P, Wang Q. High-intensity interval training on neuroplasticity, balance between brain-derived neurotrophic factor and precursor brain-derived neurotrophic factor in poststroke depression rats. J Stroke Cerebrovasc Dis. 2019;28(3):672–682. PMID: 30503681. doi:10.1016/j.jstrokecerebrovasdis.2018.11.009
53. Xu CS, Liu AC, Chen J, et al. Overactivation of NR2B- containing NMDA receptors through entorhinal-hippocampal connection initiates accumulation of hyperphosphorylated tau in rat hippocampus after transient middle cerebral artery occlusion. J Neurochem. 2015;134(3):566–577. PMID: 25903928. doi:10.1111/jnc.13134
54. Li C, Xu X, Wang Z, et al. Exercise ameliorates post-stroke depression by inhibiting PTEN elevation-mediated upregulation of TLR4/NF-κB/NLRP3 signaling in mice. Brain Res. 2020;1736:146777. PMID: 32171705. doi:10.1016/j.brainres.2020.146777
55. Lai SM, Studenski S, Richards L, et al. Therapeutic exercise and depressive symptoms after stroke. J Am Geriatr Soc. 2006;54(2):240–247. PMID: 16460374. doi:10.1111/j.1532-5415.2006.00573.x
56. Smith PS, Thompson M. Treadmill training post stroke: are there any secondary benefits? A pilot study. Clin Rehabil. 2008;22(10–11):997–1002. PMID: 18955431. doi:10.1177/0269215508088988
57. Aguiar LT, Nadeau S, Britto RR, et al. Effects of aerobic training on physical activity in people with stroke: a randomized controlled trial. NeuroRehabilitation. 2020;46(3):391–401. PMID: 32250336. doi:10.3233/NRE-193013
58. Sims J, Galea M, Taylor N, et al. Regenerate: assessing the feasibility of a strength-training program to enhance the physical and mental health of chronic post stroke patients with depression. Int J Geriatr Psychiatry. 2009;24(1):76–83. PMID: 18613281. doi:10.1002/gps.2082
59. Eng JJ, Reime B. Exercise for depressive symptoms in stroke patients: a systematic review and meta-analysis. Clin Rehabil. 2014;28(8):731–739. doi:10.1177/0269215514523631.
60. Aidar FJ, Jacó de Oliveira R, Gama de Matos D, et al. A randomized trial of the effects of an aquatic exercise program on depression, anxiety levels, and functional capacity of people who suffered an ischemic stroke. J Sports Med Phys Fitness. 2018;58(7–8):1171–1177. PMID: 28488825. doi: 10.23736/S0022-4707.17.07284-X
61. Pérez-de la Cruz S. Influence of an aquatic therapy program on perceived pain, stress, and quality of life in chronic stroke patients: a randomized trial. Int J Environ Res Public Health. 2020;17(13):4796. PMID: 32635281; PMCID: PMC7369960. doi:10.3390/ijerph17134796
62. Becker BE. Aquatic therapy in contemporary neurorehabilitation: an update. PM R. 2020;12(12):1251–1259. PMID: 32536028. doi:10.1002/pmrj.12435
63. Zhao JL, Jiang WT, Wang X, Cai ZD, Liu ZH, Liu GR. Exercise, brain plasticity, and depression. CNS Neurosci Ther. 2020;26(9):885–895. PMID: 32491278; PMCID: PMC7415205. doi:10.1111/cns.13385
64. Patel NK, Newstead AH, Ferrer RL. The effects of yoga on physical functioning and health related quality of life in older adults: a systematic review and meta-analysis. J Altern Complement Med. 2012;18(10):902–917. PMID: 22909385. doi:10.1089/acm.2011.0473
65. Chan W, Immink MA, Hillier S. Yoga and exercise for symptoms of depression and anxiety in people with poststroke disability: a randomized, controlled pilot trial. Altern Ther Health Med. 2012;18(3):34–43. PMID: 22875560.
66. Immink MA, Hillier S, Petkov J. Randomized controlled trial of yoga for chronic poststroke hemiparesis: motor function, mental health, and quality of life outcomes. Top Stroke Rehabil. 2014;21(3):256–271. PMID: 24985393. doi:10.1310/tsr2103-256
67. Taylor-Piliae RE, Hoke TM, Hepworth JT, Latt LD, Najafi B, Coull BM. Effect of Tai Chi on physical function, fall rates and quality of life among older stroke survivors. Arch Phys Med Rehabil. 2014;95(5):816–824. PMID: 24440643. doi:10.1016/j.apmr.2014.01.001
68. Zhao B, Tang Q, Wang Y, et al. Effects of Taijiquan on motor function and depression in patients with post—stroke depression. Chin J Rehabil Theory Pract. 2017;23:334–337.
69. Kim H, Kim YL, Lee SM. Effects of therapeutic Tai Chi on balance, gait, and quality of life in chronic stroke patients. Int J Rehabil Res. 2015;38(2):156–161. doi:10.1097/MRR.0000000000000103
70. Lyu D, Wang J, Yang F, et al. Effect of Tai Chi on post-stroke non-motor disorders: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 2021;35(1):26–38. PMID: 32808532. doi:10.1177/0269215520951020
71. Yao Y, Ge L, Yu Q, et al. The Effect of Tai Chi Chuan on emotional health: potential mechanisms and prefrontal cortex Hypothesis. Evid Based Complement Alternat Med. 2021;2021:5549006. PMID: 34007290; PMCID: PMC8110391. doi:10.1155/2021/5549006
72. Sun PY, Li PF, Wang T, et al. [Effect of Tongdu Tiaoshenacupuncture on PI3K/Akt/mTOR signaling pathway and autophagy- related proteins of hippocampus in rats with post-stroke depression]. Zhongguo Zhen Jiu. 2020. 40(11):1205–1210. Chinese. PMID: 33788489. doi:10.13703/j.0255-2930.20200522-k0006
73. Sun PY, Cai RL, Li PF, et al. [Protective effects on hippocampal neurons and the influence on hippocampal monoamine neurotransmitters with acupuncture for promoting the circulation of the governor vessel and regulating the mental state in rats with post-stroke depression]. Zhongguo Zhen Jiu. 2019. 39(7):741–747. Chinese. PMID: 31286737. doi:10.13703/j.0255-2930.2019.07.017
74. Zhang C. The brain-resuscitation acupuncture method for treatment of post wind-stroke mental depression–a report of 45 cases. J Tradit Chin Med. 2005;25(4):243–246. PMID: 16447661.
75. Liu SK, Zhao XM, Xi ZM. [Incidence rate and acupuncture-moxibustion treatment of post-stroke depression]. Zhongguo Zhen Jiu. 2006;26(7):472–474. Chinese. PMID: 16903595.
76. He J, Shen PF. [Clinical study on the therapeutic effect of acupuncture in the treatment of post-stroke depression]. Zhen Ci Yan Jiu. 2007;32(1):58–61. Chinese. PMID: 17580443.
77. Guo RY, Su L, Liu LA, Wang CX. [Effects of Linggui Bafa on the therapeutic effect and quality of life in patients of post-stroke depression]. Zhongguo Zhen Jiu. 2009;29(10):785–790. Chinese. PMID: 19873912
78. Wu JP. [Clinical observation on acupuncture treatment of 150 cases of post-stroke depression according to syndrome differentiation]. Zhen Ci Yan Jiu. 2010;35(4):303–306. Chinese. PMID: 21090335.
79. Nie RR, Huang CH, Fu WB. [Observation of therapeutic effect on post stroke depression treated by differentiation of spleen and stomach]. Zhongguo Zhen Jiu. 2011;31(4):325–328. Chinese. PMID: 21528598.
80. Hu JF, Chen CJ, Bi XL, et al. [Effect of early intervention of liver-smoothing and blood-activating decoction combined with acupuncture on patients with post-stroke depression]. Zhongguo Zhong Yao Za Zhi. 2013;38(14):2403–2405. Chinese. PMID: 24199581.
81. Youn JI, Sung KK, Song BK, Kim M, Lee S. Effects of electro-acupuncture therapy on post-stroke depression in patients with different degrees of motor function impairments: a pilot study. J Phys Ther Sci. 2013;25(6):725–728. PMID: 24259839; PMCID: PMC3805010. doi:10.1589/jpts.25.725
82. Li XB, Wang J, Xu AD, et al. Clinical effects and safety of electroacupuncture for the treatment of post-stroke depression: a systematic review and meta-analysis of randomised controlled trials. Acupunct Med. 2018;36(5):284–293. PMID: 29776950. doi:10.1136/acupmed-2016-011300
83. Sun Y, Bao Y, Wang S, Chu J, Li L. [Efficacy on post-stroke depression treated with acupuncture at the acupoints based on ziwuliuzhu and prozac]. Zhongguo Zhen Jiu. 2015;35(2):119–122. Chinese. PMID: 25854014.
84. Sun P, Chu H, Li P, et al. [The effect of the acupuncture intervention of dredging Governor Vessel and regulating mentality for the medication treatment of post-stroke depression]. Zhongguo Zhen Jiu. 2015;35(8):753–757. Chinese. PMID: 26571884.
85. You Y, Zhang T, Shu S, Qian X, Zhou S, Yao F. Wrist-ankle acupuncture and Fluoxetine in the treatment of post-stroke depression: a randomized controlled clinical trial. J Tradit Chin Med. 2020;40(3):455–460. PMID: 32506860. doi:10.19852/j.cnki.jtcm.2020.03.014
86. Man SC, Hung BH, Ng RM, et al. A pilot controlled trial of a combination of dense cranial electroacupuncture stimulation and body acupuncture for post-stroke depression. BMC Complement Altern Med. 2014;14(255). PMID: 25038733; PMCID: PMC4223407. doi:10.1186/1472-6882-14-255
87. Zhang K, Cui G, Gao Y, Shen W. Does acupuncture combined with antidepressants have a better therapeutic effect on post-stroke depression? A systematic review and meta- analysis. Acupunct Med. 2020:964528420967675. PMID: 33334118. doi:10.1177/0964528420967675
88. Zhang XY, Li YX, Liu DL, Zhang BY, Chen DM. The effectiveness of acupuncture therapy in patients with post-stroke depression: an updated meta-analysis of randomized controlled trials. Medicine. 2019;98(22):e15894. PMID: 31145349; PMCID: PMC6708961. doi:10.1097/MD.0000000000015894
89. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98–e169. doi:10.1161/STR.0000000000000098
90. Liebert A, Kiat H. The history of light therapy in hospital physiotherapy and medicine with emphasis on Australia: evolution into novel areas of practice. Physiother Theory Pract. 2021;37(3):389–400. PMID: 33678141. doi:10.1080/09593985.2021.1887060
91. Hamblin MR. Photobiomodulation for traumatic brain injury and stroke. J Neurosci Res. 2018;96(4):731–743. Erratum in: J Neurosci Res. 2019 Mar;97(3):373.PMID: 29131369; PMCID: PMC5803455. doi:10.1002/jnr.24190
92. Cassano P, Petrie SR, Hamblin MR, Henderson TA, Iosifescu DV. Review of transcranial photobiomodulation for major depressive disorder: targeting brain metabolism, inflammation, oxidative stress, and neurogenesis. Neurophotonics. 2016;3(3):031404. PMID: 26989758; PMCID: PMC4777909. doi:10.1117/1.NPh.3.3.031404
93. Huang L, Xi Y, Peng Y, et al. A visual circuit related to habenula underlies the antidepressive effects of light therapy. Neuron. 2019;102(1):128–142.e8. PMID: 30795900. doi:10.1016/j.neuron.2019.01.037
94. Salehpour F, Mahmoudi J, Kamari F, Sadigh-Eteghad S, Rasta SH, Hamblin MR. Brain photobiomodulation therapy: a narrative review. Mol Neurobiol. 2018;55(8):6601–6636. PMID: 29327206; PMCID: PMC6041198. doi:10.1007/s12035-017-0852-4
95. Søndergaard MP, Jarden JO, Martiny K, Andersen G, Bech P. Dose response to adjunctive light therapy in citalopram-treated patients with post-stroke depression. A randomised, double-blind pilot study. Psychother Psychosom. 2006;75(4):244–248. PMID: 16785774. doi:10.1159/000092895
96. West A, Simonsen S, Zielinsky A, et al. Abstract 13: the effect of circadian light on depressive mood in POST stroke patient during admission for rehabilitation. Stroke. 2017;48(suppl_1). doi:10.1161/str.48.suppl_1.13
97. Wang SJ, Chen MY. The effects of sunlight exposure therapy on the improvement of depression and quality of life in post-stroke patients: a RCT study. Heliyon. 2020;6(7):e04379. PMID: 32695905; PMCID: PMC7364026. doi:10.1016/j.heliyon.2020.e04379
98. Xiao M, Feng L, Wang Q, Luan X, Chen S, He J. The therapeutic effects and safety of bright light therapy combined with escitalopram oxalate on insomnia in patients with poststroke depression. Int J Geriatr Psychiatry. 2021;36(1):182–189. PMID: 32830332. doi:10.1002/gps.5412
99. Altenmüller E, Schlaug G. Apollo’s gift: new aspects of neurologic music therapy. Prog Brain Res. 2015;217:237–252. PMID: 25725918; PMCID: PMC4425943. doi:10.1016/bs.pbr.2014.11.029
100. Magee WL, Clark I, Tamplin J, Bradt J. Music interventions for acquired brain injury. Cochrane Database Syst Rev. 2017;1(1):CD006787. PMID: 28103638; PMCID: PMC6464962. doi:10.1002/14651858.CD006787.pub3
101. Särkämö T, Tervaniemi M, Laitinen S, et al. Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain. 2008;131(3):866–876.
102. Jun EM, Roh YH, Kim MJ. The effect of music-movement therapy on physical and psychological states of stroke patients. J Clin Nurs. 2013;22(1–2):22–31. PMID: 22978325. doi:10.1111/j.1365-2702.2012.04243.x
103. Van Vugt FT, Ritter J, Rollnik JD, Altenmüller E. Music-supported motor training after stroke reveals no superiority of synchronization in group therapy. Front Hum Neurosci. 2014;8:315. PMID: 24904358; PMCID: PMC4033001. doi:10.3389/fnhum.2014.00315
104. Kim DS, Park YG, Choi JH, et al. Effects of music therapy on mood in stroke patients. Yonsei Med J. 2011;52(6):977–981. PMID: 22028163; PMCID: PMC3220261. doi:10.3349/ymj.2011.52.6.977
105. Sumakul VDO, Notobroto HB, Widani NL, Aima MH. Instrumental music therapy reduced depression levels in stroke patients. J Public Health Res. 2020;9(2):1847. PMID: 32728586; PMCID: PMC7376470. doi:10.4081/jphr.2020.1847
106. Baylan S, Haig C, MacDonald M, et al. Measuring the effects of listening for leisure on outcome after stroke (MELLO): a pilot randomized controlled trial of mindful music listening. Int J Stroke. 2020;15:149–158. PMID: 30940047; PMCID: PMC7045280. doi:10.1177/1747493019841250
107. Lin F, Gu Y, Wu Y, Huang D, He N. Effect of music therapy derived from the five elements in Traditional Chinese Medicine on post-stroke depression. J Tradit Chin Med. 2017;37(5):675–680. PMID: 32188229. doi:10.1016/S0254-6272(17)30322-9
108. Baylan S, Swann-Price R, Peryer G, Quinn T. The effects of music listening interventions on cognition and mood post-stroke: a systematic review. Expert Rev Neurother. 2016;16(11):1241–1249. PMID: 27548875. doi:10.1080/14737175.2016.1227241
109. Eum Y, Yim J. Literature and art therapy in post-stroke psychological disorders. Tohoku J Exp Med. 2015;235(1):17–23. PMID: 25744067. doi:10.1620/tjem.235.17
110. Attneave F, Hebb DO. The organization of behavior; A Neuropsychological Theory. Am J Psychol. 1950;63(4):633. doi:10.2307/1418888
111. Kongkasuwan R, Voraakhom K, Pisolayabutra P, Maneechai P, Boonin J, Kuptniratsaikul V. Creative art therapy to enhance rehabilitation for stroke patients: a randomized controlled trial. Clin Rehabil. 2016;30(10):1016–1023. PMID: 26396163. doi:10.1177/0269215515607072
112. Kim MK, Kang SD. Effects of art therapy using color on purpose in life in patients with stroke and their caregivers. Yonsei Med J. 2013;54(1):15–20. PMID: 23225793; PMCID: PMC3521264. doi:10.3349/ymj.2013.54.1.15
113. Ali K, Gammidge T, Waller D. Fight like a ferret: a novel approach of using art therapy to reduce anxiety in stroke patients undergoing hospital rehabilitation. Med Humanit. 2014;40(1):56–60. PMID: 24429732. doi:10.1136/medhum-2013-010448
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.