Back to Journals » Psoriasis: Targets and Therapy » Volume 9
A narrative review of psoriasis and multiple sclerosis: links and risks
Authors Silfvast-Kaiser AS ![]() , Homan KB
, Homan KB ![]() , Mansouri B
, Mansouri B
Received 4 May 2019
Accepted for publication 6 August 2019
Published 22 August 2019 Volume 2019:9 Pages 81—90
DOI https://doi.org/10.2147/PTT.S186637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Annika S Silfvast-Kaiser,1 Katie B Homan,2 Bobbak Mansouri3–5
1Department of Dermatology, Baylor Scott and White, Dallas, TX, USA; 2Department of Dermatology, Baylor Scott and White Medical Center, Temple, TX, USA; 3Austin Institute for Clinical Research, Pflugerville, TX, USA; 4Sanova Dermatology – Pflugerville, Pflugerville, TX, USA; 5U.S. Dermatology Partners - Tyler, TX, USA
Correspondence: Bobbak Mansouri
US Dermatology Partners - Tyler, TX 1367 Dominion Plaza, Pflugerville, TX 75703, USA
Email [email protected]
Abstract: The association of psoriasis (PsO) with other autoimmune and autoinflammatory diseases has long been a topic of interest. Although previous studies have attempted to clarify the specific relationship between PsO and multiple sclerosis (MS), it remains obscure, with limited and conflicting evidence regarding a link between the two entities. Herein, we review the etiology, pathogenesis, and treatment of each disease and present the available literature to-date regarding a possible relationship between PsO and MS. We conclude that further study is necessary to discern whether there may be a significant relationship between PsO and MS. In the meantime, clinicians may find it appropriate to screen for MS in patients with PsO, allowing for timely referral to a neurologist should it be necessary.
Keywords: psoriasis, multiple sclerosis, incidence, prevalence, links, risk factors
Introduction
Psoriasis (PsO) has been associated with an increased risk of multiple comorbidities including psoriatic arthritis (PsA), cardiovascular disease, diabetes mellitus, metabolic syndrome, inflammatory bowel disease, and certain malignancies.1,2 Multiple sclerosis (MS) has also been reported as a comorbidity in individuals with PsO, and vice versa.3,4 This link between the two diseases may be somewhat unsurprising as both PsO and MS are inflammatory disorders and exhibit similarities in genetic risk variants and inflammatory pathways. Currently, limited and inconclusive evidence exists regarding the relationship between the two conditions.5–8 This review explores the possible link between PsO and MS and whether each condition serves as a potential risk factor for the development of the other.
Etiology and pathogenesis
Psoriasis
PsO is a T-cell mediated, systemic inflammatory disease that affects the skin and joints. It occurs in approximately 2–4% of the US population with similar estimates in Europe.9,10 Although it can occur at any age, PsO most commonly presents between the ages of 15 and 35 years with a second peak occurring in the late 1950s to early 1960s. It affects both men and women equally but preferentially affects persons of white European ancestry.11,12
PsO is characterized by an excessive and rapid growth of the epidermal skin layer. Clinically, it typically presents as well-demarcated, erythematous plaques with overlying silvery scale, most commonly on the extensor surfaces of the skin.13 An increased risk of developing other chronic diseases also accompanies the diagnosis of PsO, some of which include PsA, metabolic syndrome, non-alcoholic fatty liver disease, cardiovascular disorders, anxiety, depression, Crohn’s disease, and lymphoma.14,15 Approximately one-third of PsO patients will develop concomitant PsA.16
The etiology of PsO is multifactorial with complex feedback loops and cross-talk occurring between the innate and adaptive immune systems. Contributing factors to the development of PsO include a genetic predisposition, a proposed environmental or antigenic trigger, and dysregulation of the innate and adaptive immune systems.17 Native immune cells, including T-helper cells (Th1 and Th17), dendritic cells, and keratinocytes, are thought to be activated by an initial antigenic stimulus, which results in the production of pro-inflammatory cytokines. Activated dendritic cells produce tumor necrosis factor (TNF)-alpha and IL-23, among other cytokines. Antigen-presenting cells in the skin activate T-cells by secreting IL-12 and IL-23, leading to a cascade of various cytokines, which generates the chronic inflammatory state of PsO. This cascade of events, along with the TNF-alpha-governed pro-inflammatory environment, leads to the development of cutaneous psoriatic plaques and augmented inflammation which additionally contributes to the underlying comorbid conditions of PsO.18,19
Multiple sclerosis
MS is the most common demyelinating disease of the central nervous system (CNS).20–22 It affects young adults, usually between the ages of 20 and 40 years, and has a strong female predominance.23,24 It is defined by neurological symptoms that characteristically affect variable locations of the CNS over periods of time.25 Typical presenting symptoms include visual disturbances, sensory disturbances (such as paresthesias or hypoesthesia), motor weakness, cognitive deficits, fatigue, and pain.24 There is wide variation in the presentation of MS. Symptoms can range from mild, benign symptoms to rapidly progressive, debilitating disease. MS has also been associated with a decreased life expectancy by 7–14 years compared to the general, healthy population.25
The definitive pathogenesis of MS remains elusive, but, similar to PsO, it is thought to be an immune-mediated inflammatory disorder, with both genetic and environmental influences.21,25,26 It is hypothesized that an as-of-yet unknown self-antigen, possibly a myelin-associated antigen, is presented by antigen-presenting cells resulting in the production of autoreactive T-helper cells (Th1 and Th17 cells) that then cross the blood–brain barrier and release proinflammatory cytokines like IL-1, interferon (IFN)-gamma, TNF-alpha, and lymphotoxin, resulting in the early inflammation of MS.24,26,27 Furthermore, studies have indicated that there is an absence of Treg cells in lesions of MS, which provide protection against inflammatory processes, suggesting a loss of a T-cell suppression mechanism in the CNS.20,28 This immune cell-mediated inflammatory environment leads to demyelination, gliosis, macrophage activation, and neuroaxonal degeneration, ultimately resulting in the pathologic plaques in MS, characterized by confluent areas of demyelinated white and gray matter involving the spinal cord and brain. As a result, the typical neurological symptoms seen in MS arise.24,25 Later lesions of MS are dominated by infiltration of B cells into the CNS, which are then able to produce IgM and IgG leading to oligoclonal bands that can be detected in the cerebrospinal fluid.25
Multiple sclerosis and psoriasis: links
The concomitance of PsO and MS may be related to shared genetic and environmental causes leading to an overactive immune system, or may also be related to general immune system dysregulation, for which each condition is characterized by individual alterations.
Environmental factors
A variety of known and unknown environmental factors are also thought to play a role in both PsO and MS. As both are believed to be multifactorial diseases, environmental triggers may play a large role in genetically susceptible individuals. Increased UV radiation exposure, low vitamin D levels, Ebstein-Barr virus infection, and smoking have all been associated with an increased risk of MS.26,29 Various infections (e.g., Streptococcus, Staphylococcus aureus, Helicobacter pylori, HIV, and fungal infections) and medications (e.g., lithium, NSAID, anti-malarials, beta-blockers, and angiotensin-converting enzyme inhibitors), smoking, obesity, and increased stress levels have all been associated with an increased risk of PsO.30
Shared genetic factors and genetic predispositions
Th17 cells and IL-23 receptor (R) polymorphisms are both associated with MS and PsO, along with a number of other autoimmune inflammatory conditions. Multiple studies regarding the association of these polymorphisms and the development of PsO and MS have been conducted. While separate polymorphisms of the receptor are related to each condition, the two diseases seem to have unique associated polymorphisms.6,28,31–34
Shared cytokine profiles
Both MS and Pso are T-cell mediated inflammatory conditions involving similar cytokines. The IL-23/IL-17 axis is central to the pathogenesis of both MS and PsO.35 IL-23 plays a role in both PsO and MS by reinforcing the Th17 population expansion, serving as a pro-inflammatory cytokine in both diseases.20,35,36 The inflammatory response in PsO is promoted by Th17 cells, and similarly, CNS infiltration of Th17 cells with the production of IL-17 occurs in MS patients.6,32
Additionally, TNF-alpha is a key cytokine in both diseases. As with IL-17, increased levels of TNF-alpha are found in both PsO and MS plaques, underlining the central role of these inflammatory mediators in both diseases.6,37,38
IL-27 is an additional cytokine involved in both MS and PsO, although in contrasting roles. IL-27 acts to promote the differentiation of Th1 cells and inhibit the differentiation of Th17 cells. In MS, the levels of IL-27 are significantly lower when compared to patients without MS, resulting in relative lack of inhibition of Th17 differentiation. In contrast, patients with PsO have higher levels of IL-27 relative to healthy patients, increasing the representation of the Th1 profile. This is thought to act to prevent the progression of inflammation in PsO. In the population of patients with comorbid MS and PsO, there is evidence of slower progression of MS. It is hypothesized that the higher expression of IL-27/Th1 seen in PsO that results in decreased Th17 differentiation and cytokine expression is able to counterbalance the effects of decreased IL-27 expression and increased Th17 profile seen with MS.39
Demyelinating disorders associated with anti-TNF-alpha therapy
Another link between MS and PsO is illustrated with the use of anti-TNF-alpha therapy. TNF-alpha inhibitors are a well-known treatment option for PsO. However, a potential link between TNF-alpha inhibitors and demyelinating disease has been suggested.40–44 Demyelinating diseases with possible association to anti-TNF-alpha therapy include MS, optic neuritis, Guillain–Barre syndrome, transverse myelitis, and other peripheral neuropathies.42,45–47 The use of TNF-alpha inhibitors in PsO patients with a personal history of a demyelinating disorder or with a first-degree relative with MS is not recommended. However, one study has suggested that the number needed to treat in patients with PsO and MS is at least an order of magnitude smaller than the number needed to harm across all comparisons of anti-TNF-alpha therapies and first-degree relative relationships, suggesting TNF-alpha-inhibitor therapy could remain a treatment option for these patients after all other systemic treatment classes have been exhausted, in close collaboration with neurology colleagues, and while weighing the risks and benefits with the patient.48 After all, based on prior studies, it is unclear whether TNF-alpha inhibitors cause MS in patients who may be predisposed or rather unmask MS that would have presented at a later date. Several theories regarding the argument both for and against a pathogenic relationship between TNF-alpha inhibitors and demyelination have been proposed.45
Multiple sclerosis and psoriasis: is there an increased risk?
Although an association between MS and PsO has not been clearly elucidated, studies have attempted to determine if an association does exist and whether having either disease places one at a higher risk of developing the comorbid disease. To date, findings have been conflicting.49,50 (Table 1)
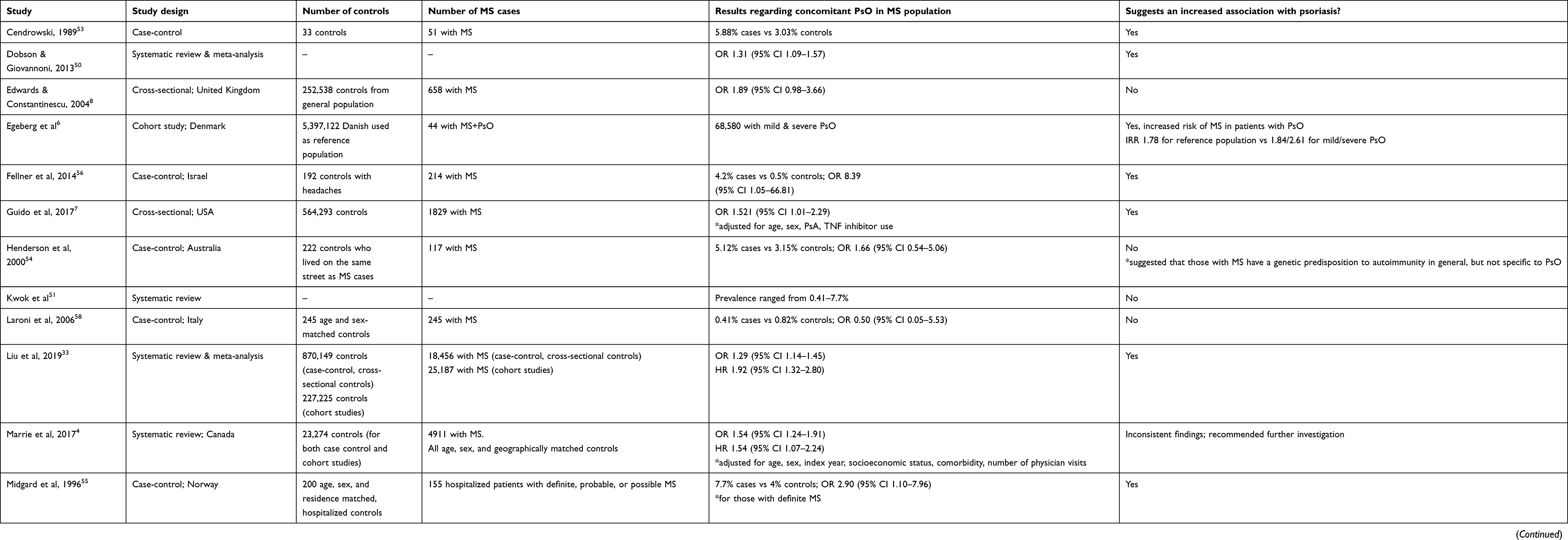 |
Table 1 Comorbid multiple sclerosis and psoriasis: characteristics of discussed studies |
Studies suggesting positive correlation
Cendrowski was the first to observe an increased prevalence of PsO in Polish MS patients, reported in 1989. He reviewed medical records of 51 patients with clinically probable MS as well as 33 controls, and reported a higher incidence of PsO in the MS group (1 in 17 vs 1 in 33, respectively).51 However, he later published a more robust series of three groups of MS patients (n=285), including these aforementioned 51 patients, and determined that PsO showed no convincing association with MS.52 A small case-control study reported an increased prevalence of PsO in patients with MS as compared to controls (6 of 117 vs 7 of 222, respectively).53 First-degree relatives of MS patients were also noted to have an increased prevalence of PsO.
In one large, single-center, retrospective, cross-sectional study, PsO (n=5097) and MS (n=1829) patients were identified via medical record from 2001 to 2014. Twenty-six patients were found to have concomitant diagnoses of PsO and MS. Five of these patients were diagnosed with PsA, as well. An association between PsO and MS was found to be significant after adjusting for confounding variables such as sex, age, PsA, and prior exposure to TNF-alpha agents (OR=1.521; 95% CI 1.01–2.29;P=0.04).54
A Danish study examined the risk of new-onset MS in patients with mild (n=58,628) or severe (n=9952) PsO using a nationwide registry and found significantly increased incidence rates for MS in both mild and severe PsO compared to the reference population, suggesting that PsO may confer a risk of MS which increases with PsO disease severity. Incidence rates for MS per 10,000 person-years were 1.78 (95% CI for the reference population, 1.74–1.82) and for mild PsO and severe PsO, were 3.22 (95% CI, 2.57–4.04), and 4.55 (95% CI, 2.52–8.22), respectively. When incidence rates were adjusted for age, gender, socioeconomic status, smoking, medication, comorbidity, and UV phototherapy, an increased risk of MS was also seen (incidence rate ratio [IRR]=1.84, 95% CI 1.46–2.30 in mild PsO; IRR=2.61, 95% CI 1.44–4.74 in severe PsO). When analyses included adjustments for family history of MS, prior TNF-inhibitor treatment, or diagnosis of PsA, similar results were also seen.6
Another study investigated various chronic inflammatory diseases and their association with MS by looking at 155 patients with MS and 200 controls from 1976 to 1986.55 MS patients had a significantly increased prevalence of PsO as compared to controls (OR=2.01, CI 0.73–5.83). This study also supported prior studies showing that families of MS patients experience no different rates of occurrence for autoimmune diseases when compared to control families.
In 2013, a meta-analysis of autoimmune disease in those with MS was performed.49 Eight studies that analyzed the risk of PsO in the MS population as well as their families were included. These studies found an overall increased risk for PsO in MS patients (OR=1.31, 95% CI 1.09–1.57, P<0.0001). There was no significantly increased risk for PsO in their first-degree relatives (OR=1.17, 95% CI 0.94–1.46, P=0.16).
A retrospective case-control study in Israel investigated the impact of PsO on the disease activity and progression of MS.39 This study included 3456 patients with PsO and MS who had been followed in excess of 5 years. Cases were compared to a matched control cohort of patients with only an MS diagnosis. This study found that 1.3% of MS patients had PsO as a comorbid diagnosis, and 78% (35 of 45) of these patients had PsO precede their MS diagnosis. Patients with PsO onset before their relapsing-remitting MS onset had later MS disease onset in life, slower progression of MS disability compared to patients without concurrent PsO, and significantly longer time to both second relapse and until significant neurological disability.
One case-control study investigated whether patients with a diagnosis of MS had higher rates of concomitant PsO.56 They found that 9 of the 214 MS patients and 1 of the 192 consecutive controls had comorbid PsO. Six of the 9 MS patients with PsO had been diagnosed with PsO prior to their MS diagnosis.
Most recently, a systematic review and meta-analysis of observational studies performed in 2018 reported increased OR and HR of PsO in MS patients (OR 1.29, 95% CI, 1.14–1.45; HR 1.92, 95% CI 1.32–2.80).32
Studies suggesting no correlation
In contrast, there have been several studies to suggest no association between PsO and MS. For example, a prospective study of patients diagnosed with MS in England did not detect an association with PsO.7 In this study, comorbidities of 658 consecutive patients attending a large MS specialty clinic in Nottingham were recorded during 2002–2003. There were 454 females and 204 males that participated (18–80 years old, median age=45) in the study. The prevalence of PsO in MS patients compared to the general population did not differ significantly.7
Similarly, one of the largest published multicenter studies evaluated autoimmune disease risk in MS patients as well as their families, comparing rates of occurrence to their first-degree relatives, as well as in their unrelated spouses.8 In this study, 5031 MS patients along with 30,529 of their first-degree relatives and spouses (n=2707 spouses) were analyzed. The frequency of PsO in MS patients was found to be no different than for their spousal controls (5.8% of MS population vs 5.4% of controls, P=0.44). No significant difference in genders or in first-degree relatives of MS patients compared to controls was found.
In 2015, a systematic review of published studies to estimate the incidence and prevalence of comorbid autoimmune disease in MS was performed.33 This study also assessed the quality of these reviewed studies, finding less than half of the available studies to be of high quality. The prevalence of PsO in MS varied widely, ranging from 0.39% to 7.74% in previously published studies. The highest estimate was reported by Midgard et al’s population-based study (7.7% in MS patients vs 4% in controls).
A population-based cohort study utilizing the Danish Health Registration system compared MS patients to the general population, estimating the relative risk of other autoimmune diseases in patients with MS and their first-degree relatives.57 They reported a small, insignificant, increased risk of PsO in patients with MS and no increased incidence in their first-degree relatives. Laroni et al also failed to show an increased prevalence of PsO in patients with MS when compared to controls (0.41% vs 0.82%, respectively).58 Similarly, a systematic review of the literature also did not find an increased prevalence of PsO in patients with MS.50
Finally, a comorbidity survey conducted by the National Psoriasis Foundation which spanned from 2003 to 2011 did not show an increased incidence of MS in patients with PsO.59
Limitations of existing studies
An inherent limitation of most studies regarding the relationship between PsO and MS is a small sample size, and often, an observational or retrospective design. Large patient numbers and a reduction in selection bias have been attained in some studies that use nationwide databases, but these databases often introduce a lack of diversity and therefore, limit the ability to extrapolate results to larger, more ethnically diverse populations. A limitation of nationwide database use or electronic medical record systems is also a reliance on correct coding, introducing the possibility of unverified or incorrect diagnoses. In studies that included patient-reported conditions or histories, the potential for ascertainment or reporting bias is large. Some of the above studies also used prevalence data available in the literature, without age and sex matching, instead of obtaining a control population from the same or a similar environment. Meta-analyses are limited by the quality of the studies included and the manner in which the information was obtained or collected in those studies. Psoriasis patients may also receive increased medical attention compared to patients without the disease which could lead to earlier, more frequent diagnoses of comorbid MS.
Management and treatment
Psoriasis
Most patients with mild-to-moderate PsO can be well controlled on topical medications (i.e., corticosteroids, vitamin D analogs, coal tar, calcineurin inhibitors, retinoids, anthralin) and/or phototherapy. For moderate-to-severe disease, systemic agents and/or biologic agents are often indicated. Oral systemic therapies for PsO include methotrexate (MTX), acitretin, cyclosporine (CYA), and apremilast. Biological therapies approved for use in PsO include TNF-alpha inhibitors (adalimumab, etanercept, certolizumab pegol, infliximab), an IL-12/23p40 inhibitor (ustekinumab), inhibitors of IL-17A (secukinumab, ixekizumab) the IL-17 receptor inhibitor (brodalumab), and IL-23p19 inhibitors (guselkumab, tildrakizumab).
Multiple sclerosis
Treatment of MS varies based on the type of MS being treated and treatment goals. Progressive types of MS are more difficult to treat successfully compared to relapsing forms of MS. Disease-modifying treatment options for relapsing-remitting forms of MS include IFN-beta, glatiramer acetate, dimethyl fumarate, teriflunomide, fingolimod, natalizumab, or alemtuzumab.60–64 The treatment of progressive types of MS, with evidence of active inflammation, relies primarily on immunosuppressive therapies, which unfortunately have self-limiting side effects with chronic use. Treatment options for secondary progressive MS in addition to the disease-modifying treatments, although of modest or lacking efficacy, include intravenous (IV) glucocorticoids, IV cyclophosphamide, and MTX.65–67 Options for primary progressive MS include ocrelizumab (the only drug approved for this type of MS), along with IV glucocorticoids, MTX, cladribine, mitoxantrone, and IVIg.65,66,68–71 More recently, the use of IL-17 inhibitors, specifically secukinumab, has shown reduction in the number of active brain lesions on magnetic resonance imaging (MRI) scans in patients with relapsing-remitting MS.72,73
Treatment of psoriasis in patients with concomitant multiple sclerosis
As seen above, MS and PsO exhibit overlapping treatments including the use of fumarates (used mainly in Northern Europe), IFN-beta with MTX, and IL-17 inhibitors. MTX and CYA are both indicated for the treatment of PsO, and both also improve MS symptoms and reduce relapse rates.74–79 Dimethylfumarate works by downregulating Th1 and Th17 cells, which are upregulated in PsO and MS. This reduces the production of proinflammatory cytokines, including, but not limited to, IL-12, IL-17 and IL-23, which have been implicated in PsO and MS.32 In a small study, the addition of MTX to IFN-beta for the treatment of MS showed improvement of MS lesions.80 On the other hand, PsO outbreaks have been described with IFN-beta treatment for MS.
Secukinumab, an IL-17 inhibitor, is approved for use in PsO and PsA, and appears to be safe in patients with MS. As mentioned above, secukinumab causes significant reduction in MRI lesion activity in MS patients as well.6,72 The shared polymorphisms of the IL-23 receptor gene associated with MS and PsO may explain the efficacy of fumarates in both diseases, in addition to the successful use of IL-17A inhibitors in both conditions.31,34,81
Ustekinumab is an IL-12/23p40 inhibitor approved for use in PsO and PsA. During a Phase II clinical trial, ustekinumab did not improve or worsen relapsing remitting MS, and there are no reports of worsening neurological disease with ustekinumab, allowing ustekinumab to remain as a treatment option in concomitant MS and PsO.82,83
As mentioned above, there is a possible increase in MS exacerbations, and demyelinating disorders in general, with patients on anti-TNF alpha therapies.6,84,85
Phototherapy is not only efficacious in PsO treatment, but also benefits patients with MS, likely due to an increase in vitamin D levels which are deficient in patients with higher risk of MS and increased severity of disease.39
Areas of current and future research (e.g., IL-35)
The most recently identified potential therapeutic target in inflammatory diseases, including PsO and MS, involves IL-35. IL-35 is a more recently identified member of the IL-12 cytokine family and is secreted primarily by regulatory T cells (Tregs).86,87 IL-35 is also uniquely an immunosuppressive cytokine that plays a pivotal role in the function of Tregs and their immunoregulatory activity.86 Both PsO and MS, among other autoimmune inflammatory diseases, have abnormal IL-35 expression, making IL-35 a potential new focus of therapeutic strategies.87
Another potential treatment for both MS and PsO in recent literature lies in the properties of mesenchymal stem cells (MSCs). MSCs have the capabilities of modulating immune properties and exerting anti-inflammatory effects making them an alluring potential therapy in autoimmune inflammatory conditions.88 In a recent study, human embryonic (hE)-MSC transplantation resulted in the dramatic reduction of Th1 and Th17 cytokines in mice with imiquimod-induced PsO-like dermatitis.88 There have been a relatively larger number of studies regarding MSC transplantation in the treatment of MS, many of them also showing promise, especially in comparison to current disease-modifying options, for the effective treatment of MS.89 Further studies are needed to determine the efficacy of MSC and the most promising cell origin as a therapy for both MS and PsO.
Conclusion
The data regarding the association between PsO and MS are overall inconsistent and conflicting. Smaller studies suggest that there may be an association and the few larger studies that have been conducted report no significant association between PsO and MS. Further study to verify or reject this association is warranted as uncovering the relationship between these two diseases could lead to the discovery of common mechanisms and genetic or environmental causes that could be of substantial value in the diagnosis and management of both diseases. Until then, dermatologists and other treating physicians alike may find it appropriate to screen for MS symptoms in patients with PsO so that timely referral to a neurologist can occur if necessary.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gottlieb AB, Chao C, Dann F. Psoriasis comorbidities. J Dermatolog Treat. 2008;19(1):5–21. doi:10.1080/09546630701364768
2. Elmets C, Leonardi C, Davis D, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J Am Acad Derm. 2019;80(4):1073–1113. doi:10.1016/j.jaad.2018.11.058
3. Islam MM, Poly TN, Yang HC, Wu CC, Li YC. Increase risk of multiple sclerosis in patients with psoriasis disease: an evidence of observational studies. Neuroepidemiology. 2019;52(3–4):152–160. doi:10.1159/000495112
4. Marrie RA, Patten SB, Tremlett H, Wolfson C, Leung S, Fisk JD. Increased incidence and prevalence of psoriasis in multiple sclerosis. Mult Scler Relat Disord. 2017;13:81–86. doi:10.1016/j.msard.2017.02.012
5. Langer-Gould A, Albers KB, Van Den Eeden SK, Nelson LM. Autoimmune diseases prior to the diagnosis of multiple sclerosis: a population-based case-control study. Mult Scler. 2010;16(7):855–861. doi:10.1177/1352458510369146
6. Egeberg A, Mallbris L, Gislason GH, Skov L, Hansen PR. Risk of multiple sclerosis in patients with psoriasis: a Danish nationwide cohort study. J Invest Dermatol. 2016;136(1):93–98. doi:10.1038/JID.2015.350
7. Edwards LJ, Constantinescu CS. A prospective study of conditions associated with multiple sclerosis in a cohort of658 consecutive outpatients attending a multiple sclerosis clinic. Mult Scler. 2004;10(5):575–581. doi:10.1191/1352458504ms1087oa
8. Ramagopalan SV, Dyment DA, Valdar W, et al. Autoimmune disease in families with multiple sclerosis: a population-based study. Lancet Neurol. 2007;6(7):604–610. doi:10.1016/S1474-4422(07)70132-1
9. Parisi R, Symmons DP, Griffiths CE, et al. Identification and management of PsO and associated comorbidiTy (IMPACT) project team. Global epidemiology of PsO: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339
10. Christophers E. Psoriasis – epidemiology and clinical spectrum. Clin Exp Dermatol. 2001;26(4):314–320.
11. Kupetsky EA, Keller M. Psoriasis vulgaris: an evidence-based guide for primary care. J Am Board Fam Med. 2013;26(6):787–801. doi:10.3122/jabfm.2013.06.130055
12. Weller R, Hunter JAA, Savin J, Dahl M. Clinical Dermatology.
13. Ouyang W. Distinct roles of IL-22 in human psoriasis and inflammatory bowel disease. Cytokine Growth Factor Rev. 2010;21(6):435–441. doi:10.1016/j.cytogfr.2010.10.007
14. Griffiths CEM, Barker JNWN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271. doi:10.1016/S0140-6736(07)61128-3
15. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361(5):496–509. doi:10.1056/NEJMra0804595
16. Henes JC, Ziupa E, Eisfelder M, et al. High prevalence of psoriatic arthritis in dermatological patients with psoriasis: a cross-sectional study. Rheumatol Int. 2014;34(2):227–234. doi:10.1007/s00296-013-2876-z
17. Hugh JM, Weinberg JM. Update on the pathophysiology of psoriasis. Cutis. 2018;102(5S):6–12.
18. Lynde C, Poulin Y, Vender R, Bourcier M, Khalil S. Interleukin 17A: toward a new understanding of PsO pathogenesis. J Am Acad Dermatol. 2014;71(1):141–150. doi:10.1016/j.jaad.2013.12.036
19. Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
20. Tzartos JS, Friese MA, Craner MJ, et al. Interleukin-17 production in central nervous system-infiltrating T cells and glial cells is associated with active disease in multiple sclerosis. Am J Pathol. 2008;172(1):146–155. doi:10.2353/ajpath.2008.070724
21. Ramagopalan SV, Sadovnick AD. Epidemiology of multiple sclerosis. Neurol Clin. 2011;29(2):207–217. doi:10.1016/j.ncl.2010.12.010
22. Karussis D. The diagnosis of multiple sclerosis and the various related demyelinating syndromes: a critical review. J Autoimmun. 2014;48–49:134–142. doi:10.1016/j.jaut.2014.01.022
23. Vidal-Jordana A, Montalban X. Multiple sclerosis: epidemiologic, clinical, and therapeutic aspects. Neuroimaging Clin N Am. 2017;27(2):195–204. doi:10.1016/j.nic.2016.12.001
24. Dendrou CA, Fugger L, Friese MA. Immunopathology of multiple sclerosis. Nat Rev Immunol. 2015;15(9):545–558. doi:10.1038/nri3871
25. Files DK, Jausurawong T, Katrajian R, Danoff R. Multiple sclerosis. Prim Care. 2015;42(2):159–175. doi:10.1016/j.pop.2015.01.007
26. Willer CJ, Ebers GC. Susceptibility to multiple sclerosis: interplay between genes and environment. Curr Opin Neurol. 2000;13(3):241–247.
27. Galetta KM, Bhattacharyya S. Multiple sclerosis and autoimmune neurology of the central nervous system. Med Clin North Am. 2019;103(2):325–336. doi:10.1016/j.mcna.2018.10.004
28. Ghaffari SA, Nemati M, Hajghani H, Ebrahimi H, Sheikhi A, Jafarzadeh A. Circulating concentrations of interleukin (IL)-17 in patients with multiple sclerosis: evaluation of the effects of gender, treatment, disease patterns and IL-23 receptor gene polymorphisms. Iran J Neurol. 2017;16(1):15–25.
29. Munger KL, Ascherio A. Risk factors in the development of multiple sclerosis. Expert Rev Clin Immunol. 2007;3(5):739–748. doi:10.1586/1744666X.3.5.739
30. Lee EB, Wu KK, Lee MP, Bhutani T, Wu JJ. Psoriasis risk factors and triggers. Cutis. 2018;102(5S):18–20.
31. Cargill M, Schrodi SJ, Chang M, et al. A large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genes. Am J Hum Genet. 2006;80(2):273–290. doi:10.1086/511051
32. Liu CY, Tung TH, Lee CY, et al. Association of multiple sclerosis with psoriasis: a systematic review and meta-analysis of observational studies. Am J Clin Dermatol. 2019;20(2):201–208. doi:10.1007/s40257-018-0399-9
33. Marrie RA, Reider N, Cohen J, et al. A systematic review of the incidence and prevalence of autoimmune disease in multiple sclerosis. Mult Scler. 2015;21(3):282–293. doi:10.1177/1352458514564490
34. Nunez C, Dema B, Cenit MC, et al. IL23R: a susceptibility locus for celiac disease and multiple sclerosis? Genes Immun. 2008;9(4):289–293. doi:10.1038/gene.2008.16
35. Tang C, Chen S, Qian H, Huang W. Interleukin-23: as a drug target for autoimmune inflammatory diseases. Immunology. 2012;135(2):112–124. doi:10.1111/j.1365-2567.2011.03522.x
36. Langrish CL, Chen Y, Blumenschein WM, et al. IL-23 drives a pathogenic T cell population that induces autoimmune inflammation. J Exp Med. 2005;201(2):233–240. doi:10.1084/jem.20042565
37. Kebir H, Kreymborg K, Ifergan I, et al. Human TH17 lymphocytes promote blood-brain barrier disruption and central nervous system inflammation. Nat Med. 2007;13(10):1173–1175. doi:10.1038/nm1651
38. Speeckaert R, Lambert J, Grine L, Van Gele M, De Schepper S, van Geel N. The many faces of interleukin-17 in inflammatory skin diseases. Br J Dermatol. 2016;175(5):892–901. doi:10.1111/bjd.2016.175.issue-5
39. Miron G, Gurevich M, Baum S, Achiron A, Barzilai A. Psoriasis comorbidity affects multiple sclerosis neurological progression: a retrospective case–control analysis. J Eur Acad Dermatol Venereol. 2017;31(12):2055–2061. doi:10.1111/jdv.14403
40. Cruz Fernandez-Espartero M, Perez-Zafrilla B, Naranjo A, et al. Demyelinating disease in patients treated with TNF antagonists in rheumatology: data from BIOBADASER, a pharmacovigilance database, and a systematic review. Semin Arthritis Rheum. 2011;41(3):524–533. doi:10.1016/j.semarthrit.2011.05.003
41. Kay J, Fleischmann R, Keystone E, et al. Golimumab 3-year safety update: an analysis of pooled data from the long-term extensions of randomised, double-blind, placebo-controlled trials conducted in patients with rheumatoid arthritis, psoriatic arthritis or ankylosing spondylitis. Ann Rheum Dis. 2015;74:538–546. doi:10.1136/annrheumdis-2013-204195
42. Mohan N, Edwards ET, Cupps TR, et al. Demyelination occurring during anti-tumor necrosis factor alpha therapy for inflammatory arthritides. Arthritis Rheum. 2001;44(12):2862–2869. doi:10.1002/1529-0131(200112)44:12<2862::aid-art474>3.0.co;2-w
43. Ramos-Casals M, Roberto Perez A, Diaz-Lagares C, Cuadrado MJ, Khamashta MA. Autoimmune diseases induced by biological agents: a double-edged sword? AutoimmunRev. 2010;9(3):188–193.
44. Tristano AG. Neurological adverse events associated with anti-tumor necrosis factor alpha treatment. J Neurol. 2010;257:1421–1431. doi:10.1007/s00415-010-5591-7
45. Kemanetzoglou E, Andreadou E. CNS demyelination with TNF-α blockers. Curr Neurol Neurosci Rep. 2017;17(4):36. doi:10.1007/s11910-017-0742-1
46. Simsek I, Erdem H, Pay S, Sobaci G, Dinc A. Optic neuritis occurring with anti-tumour necrosis factor alpha therapy. Ann Rheum Dis. 2007;66(9):1255–1258. doi:10.1136/ard.2006.066787
47. Shin IS, Baer AN, Kwon HJ, Papadopoulos EJ, Siegel JN. Guillain-Barre and Miller Fisher syndromes occurring with tumor necrosis factor alpha antagonist therapy. Arthritis Rheum. 2006;54(5):1429–1439. doi:10.1002/art.21814
48. Mansouri B, Horner ME, Menter A. Tumor necrosis factor-alpha inhibitor use in psoriasis patients with a first-degree relative with multiple sclerosis. J Drugs Dermatol. 2015;14(8):876–878.
49. Dobson R, Giovannoni G. Autoimmune disease in people with multiple sclerosis and their relatives: a systematic review and meta-analysis. J Neurol. 2013;260(5):1272–1285. doi:10.1007/s00415-012-6790-1
50. Kwok T, Loo WJ, Guenther L. PsO and multiple sclerosis: is there a link? J Cutan Med Surg. 2010;14(4):151–155. doi:10.2310/7750.2010.09063
51. Cendrowski W. [Multiple sclerosis and PsO]. Wiad Lek. 1989;56:819–822.
52. Cendrowski W. Multiple sclerosis and diseases of autoimmune or related origin. Pol J Med Pharm. 1989;21(4):327–329.
53. Henderson RD, Bain CJ, Pender MP. The occurrence of autoimmune diseases in patients with multiple sclerosis and their families. J Clin Neurosci. 2000;7(5):434–437. doi:10.1054/jocn.2000.0693
54. Guido N, Cices A, Ibler E, et al. Multiple sclerosis association with psoriasis: a large U.S. population, single centre, retrospective cross-sectional study. J Eur Acad Dermatol Venereol. 2017;31(9):e397–e398. doi:10.1111/jdv.14205
55. Midgard R, Gronnin M, Riise T, et al. Multiple sclerosis and chronic inflammatory diseases: a case-control study. Acta Neurol Scand. 1996;93(5):322–328.
56. Fellner A, Dano M, Regev K, Mosek A, Karni A. Multiple sclerosis is associated with psoriasis. A case-control study. J Neurol Sci. 2014;338(1–2):226–228. doi:10.1016/j.jns.2014.01.003
57. Neilsen NM, Frisch M, Rostgaard K, et al. Autoimmune diseases in patients with multiple sclerosis and their first-degree relatives: a nationwide cohort study in Denmark. Mult Scler. 2008;14(6):829–832.
58. Laroni A, Calabrese M, Perini P, et al. Multiple Sclerosis and autoimmune diseases: epidemiology and HLA-DR association in northeast Italy. J Neurol. 2006;253(5):636–639. doi:10.1007/s00415-006-0084-4
59. Armstrong AW, Schupp C, Bebo B. Psoriasis comorbidities: results from the National Psoriasis Foundation surverys 2003–2011. Dermatology. 2012;225(2):121–126. doi:10.1159/000342180
60. Comi G, Filippi M, Wolinsky JS. European/Canadian multicenter, double-blind, randomized, placebo-controlled study of the effects of glatiramer acetate on magnetic resonance imaging–measured disease activity and burden in patients with relapsing multiple sclerosis. European/Canadian Glatiramer Acetate Study Group. Ann Neurol. 2001;49(3):290–297.
61. Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial. Lancet. 2012;380(9856):1819–1828. doi:10.1016/S0140-6736(12)61769-3
62. Kasper LH, Reder AT. Immunomodulatory activity of interferon-beta. Ann Clin Transl Neurol. 2014;1(8):622–631. doi:10.1002/acn3.84
63. Ransohoff RM. Natalizumab for multiple sclerosis. N Engl J Med. 2007;356(25):2622–2629. doi:10.1056/NEJMct071462
64. Thomas RH, Wakefield RA. Oral disease-modifying therapies for relapsing-remitting multiple sclerosis. Am J Health Syst Pharm. 2015;72(1):25–38. doi:10.2146/ajhp150051
65. Goodkin DE, Kinkel RP, Weinstock-Guttman B, et al. A phase II study of i.v. methylprednisolone in secondary-progressive multiple sclerosis. Neurology. 1998;51(1):239–245. doi:10.1212/wnl.51.1.239
66. Gray OM, McDonnell GV, Forbes RB. A systematic review of oral methotrexate for multiple sclerosis. Mult Scler. 2006;12(4):507–510. doi:10.1191/1352458506ms1299oa
67. Weiner HL, Mackin GA, Orav EJ, Hafler DA. Intermittent cyclophosphamide pulse therapy in progressive multiple sclerosis: final report of the Northeast cooperative multiple sclerosis treatment group. Neurology. 1993;l43(5):910–918. doi:10.1212/WNL.43.5.910
68. Hartung HP, Gonsette R, Konig N, et al. Mitoxantrone in progressive multiple sclerosis: a placebo-controlled, double-blind, randomised, multicentre trial. Lancet. 2002;360(9350):2018–2025. doi:10.1016/S0140-6736(02)12023-X
69. Montalban X, Hauser A, Kappos L, et al. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2017;376:209–220. doi:10.1056/NEJMoa1606468
70. Pohlau D, Przuntek H, Sailer M, et al. Intravenous immunoglobulin in primary and secondary chronic progressive multiple sclerosis: a randomized placebo controlled multicentre study. Mult Scler J. 2007;13(9):1107–1117. doi:10.1177/1352458507078400
71. Rice GP, Filippi M, Comi G. Cladribine and progressive MS: clinical and MRI outcomes of a multicenter controlled trial. Cladribine MRI study group. Neurology. 2000;54(5):1145–1155. doi:10.1212/wnl.54.5.1145
72. Havrdova E, Belova A, Goloborodko A, et al. Activity of secukinumab, an anti-IL-17A antibody, on brain lesions in RRMS: results from a randomized, proof-of-concept study. J Neurol. 2016;263:1287–1295. doi:10.1007/s00415-016-8128-x
73. Kolbinger F, Huppertz C, Mir A, Di Padova F. IL-17A and multiple sclerosis: signaling pathways, producing cells and target cells in the central nervous system. Curr Drug Targets. 2016;17(16):1882–1893.
74. Ashtari F, Savoj MR. Effects of low dose methotrexate on relapsing-remitting multiple sclerosis in comparison to Interferon β-1α: a randomized controlled trial. J Res Med Sci. 2011;16(4):457–462.
75. Currier RD, Haerer AF, Meydrech EF. Low dose oral methotrexate treatment of multiple sclerosis: a pilot study. J Neurol Neurosurg Psychiatry. 1993;56(11):1217–1218. doi:10.1136/jnnp.56.11.1217
76. Goodkin DE, Rudick RA, VanderBrug Medendorp S, et al. Low-dose (7.5 mg) oral methotrexate reduces the rate of progression in chronic progressive multiple sclerosis. Ann Neurol. 1995;37(1):30–40. doi:10.1002/ana.410370108
77. Neumann JW, Ziegler DK. Therapeutic trial of immuno-suppressive agents in multiple sclerosis. Neurology. 1972;22:1268–1271. doi:10.1212/wnl.22.12.1268
78. Paty DW, Li DK. Interferon beta-lb is effective in relapsing-remitting multiple sclerosis. II. MRI analysis results of a multicenter, randomized, double-blind, placebo-controlled trial. 1993 [classical article]. Neurology. 2001;57(12 suppl 5):S10–S15.
79. Zhao GJ, Li DK, Wolinsky JS, et al. Clinical and magnetic resonance imaging changes correlate in a clinical trial monitoring cyclosporine therapy for multiple sclerosis. The MS Study Group. J Neuroimaging. 1997;7(1):1–7.
80. Calbresi PA, Wilterdink JL, Rogg JM, et al. An open-label trial of combination therapy with interferon beta-1a and oral methotrexate in MS. Neurology. 2002;58(2):314–317. doi:10.1212/wnl.58.2.314
81. Cargill M, Schrodi SJ, Chang M, et al. A large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genes. Am J Hum Genet. 2007;80(2):273–290. doi:10.1086/511051
82. Segal BM, Constantinescu CS, Raychaudhuri A, et al. Repeated subcutaneous injections of IL12/23 p40 neutralising antibody, ustekinumab, in patients with relapsing-remitting multiple sclerosis: a phase II, double-blind, placebo-controlled, randomised, dose-ranging study. Lancet Neurol. 2008;7(9):796–804. doi:10.1016/S1474-4422(08)70173-X
83. Kaushik SB, Lebwhol MG. Psoriasis: which therapy for which patient: psoriasis comorbidities and preferred systemic agents. Jour Amer Acad Derm. 2019;80(1):27–40. doi:10.1016/j.jaad.2018.06.057
84. TNF neutralization in MS: results of a randomized, placebo-controlled multicenter study. The lenercept multiple sclerosis study group and The University of British Columbia MS/MRI Analysis Group. Neurology. 1999;53(3):457–465.
85. Lozeron P, Denier C, Lacroix C, Adams D. Long-term course of demyelinating neuropathies occurring during tumor necrosis factor-alpha-blocker therapy. Arch Neurol. 2009;66(4):490–497. doi:10.1001/archneurol.2009.11
86. Guo H, Li B, Wang W, Zhao N, Gao H. Mesenchymal stem cells overexpressing IL-35: a novel immunosuppressive strategy and therapeutic target for inducing transplant tolerance. Stem Cell Res Ther. 2018;9(1):254. doi:10.1186/s13287-018-0988-9
87. Su LC, Liu XY, Huang AF, Xu WD. Emerging role of IL-35 in inflammatory autoimmune diseases. Autoimmune Rev. 2018;17(7):665–673. doi:10.1016/j.autrev.2018.01.017
88. Kim CH, Lim CY, Lee JH, et al. Human embryonic stem cells-derived mesenchymal stem cells reduce the symptom of psoriasis in imiquimod-induced skin model. Tissue Eng Regen Med. 2018;16(1):93–102. doi:10.1007/s13770-018-0165-3
89. Genc B, Bozan HR, Genc S, Genc K. Stem Cell Therapy for Multiple Sclerosis. Adv Exp Med Biol. Epub 2018 Jul 24. doi:10.1007/5584_2018_247
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.