Back to Journals » Advances in Medical Education and Practice » Volume 16
A Multimodal Approach to Education at a Rural Midwestern Physical Therapy Program, Including Community Partnerships, Increases Student Confidence in Providing Acute Care
Authors Kopka RM ![]() , Beck E
, Beck E ![]() , Thompson MP
, Thompson MP
Received 7 June 2025
Accepted for publication 11 October 2025
Published 29 October 2025 Volume 2025:16 Pages 1981—1987
DOI https://doi.org/10.2147/AMEP.S542835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Rochelle M Kopka,* Emma Beck,* McKenze Primrose Thompson*
Department of Physical Therapy, Central Michigan University, Mount Pleasant, MI, 48859, USA
*These authors contributed equally to this work
Correspondence: Rochelle M Kopka, Department of Physical Therapy, Central Michigan University, 1238 Health Professions Bldg, Mount Pleasant, MI, 48859, USA, Tel +1-989-751-5950, Email [email protected]
Introduction: Incorporating various components into education, as part of the physical therapy curriculum, has increased students’ confidence levels. Examples include lecture, lab, simulation, and community outreach. Research on simulation is strong; however, there is a lack of evidence on utilizing community outreach in conjunction with the integration of interprofessional educational (IPE) simulations to improve student preparation and confidence levels. This study aimed to evaluate how a multimodal educational approach, including community partnerships, influences doctor of physical therapy (DPT) students’ confidence in acute care settings.
Methods: Using a descriptive phenomenological study design, seven participants male (n=2) and female (n=5) from a Commission on Accreditation in Physical Therapy Education (CAPTE) approved DPT program completed a focus group interview, encouraging reflection on self-confidence, experiences, and perceptions before and after their acute care clinical rotation, following their exposure to a multimodal educational approach that included lectures, laboratories, simulations, and community partnerships.
Results: Students reported increased confidence following exposure to a multimodal approach to physical therapy curriculum, which included lecture activities, laboratory activities, community partnerships, and IPE simulation. Three main themes emerged: confidence levels, perception of preparedness, and pre- and post-biases of acute care clinical rotation. All participants reported they would feel confident in accepting a position as an acute care physical therapist.
Conclusion: Multimodal curricula have been shown to increase student confidence, communication skills, and preparedness before clinical rotations, yet there is little evidence to suggest additional benefits from participation in community outreach or the structure of the acute-care curriculum for physical therapy students. This study provides guidance for physical therapy programs and further benefits the future of healthcare by improving the acute care curriculum for physical therapy students.
Keywords: acute care curriculum, multimodal educational approach, physical therapy education, student perception
Introduction
Acute care is a diverse, fast-paced, and constantly changing healthcare environment that requires highly trained clinicians in various healthcare roles to ensure patient safety and progress toward improvement. To ensure competence within the acute care setting, it has been shown that skills such as the collection and analysis of medical information, application of physical therapy knowledge, and the ability to provide information to the patient are highly valued when within the acute care setting.1 To meet this criterion, an intensive didactic curriculum, community outreach opportunities, and integration of interprofessional educational (IPE) simulations have gained popularity within doctoral healthcare professions, specifically physical therapy. Interprofessional education is operationally defined as the collaboration of two or more disciplines eliciting observable and measurable outcomes.2
Over the years, multimodal curricula have been integrated into Doctor of Physical Therapy (DPT) programs to improve the confidence and readiness of students entering acute-care clinical rotations.3 A multimodal approach to education integrates multiple modes of teaching content into a curriculum, allowing students to grasp information through various learning styles. Multimodal education is operationally defined as an educational approach that systematically incorporates multiple sensory and communication modalities simultaneously or sequentially to facilitate and enhance the learning process.4 Examples may include lectures, laboratory activities, IPE simulations, and community partnerships that provide students with the opportunity to apply their knowledge and skills in patient interactions. IPE simulations have been utilized to improve confidence and allow students to apply the didactic knowledge and skills needed to be efficient in acute care scenarios. The use of IPE simulations has been shown to improve physical therapy students’ perceptions and confidence prior to entering an acute care setting.5 Improvements were demonstrated in technical, behavioral, and cognitive performance. IPE simulations have also been shown to improve confidence and proficiency when assessing pulmonary status, utilizing intensive care unit (ICU) equipment to assess a patient’s status, and recognizing appropriate procedures in life-threatening situations. Overall, 98% of the students strongly agreed on incorporating more IPE simulations and making the acute care IPE simulation a permanent requirement of the curriculum to gain more acute care experience.3
Another important component of a multimodal curriculum is communication within the physical therapy profession. Research has shown that empathy and understanding of medical professionals have improved patient outcomes and delivery of care.6 Utilizing IPE simulations and community outreach opportunities increases students’ confidence and communication skills. Efficient communication skills increase patient compliance, create a safe environment for patients, and promote open communication between patients and clinicians.6
Community partnerships and volunteer experiences are essential components of the DPT curriculum for many programs in the country. Through outpatient experiences, students can increase their patient exposure and improve their skills. Research has shown that student engagement in volunteer services for outpatient populations results in increased confidence in patient communication following engagement.7 Further research provides similar themes and has shown that simulation of patient treatment increases student confidence in clinical reasoning and patient-centered communication throughout the stresses of unexpected situations.8
While the literature shows the effectiveness of a multimodal curriculum in increasing student confidence, communication skills, and preparedness before clinical rotations in an acute setting, there is little evidence to suggest additional benefits from participation in community outreach or the structure of the acute care curriculum for physical therapy students. In addition, no formal study has been conducted to analyze the effectiveness of a multimodal curriculum in an accredited DPT program by the Commission on Accreditation in Physical Therapy Education (CAPTE), focusing on all components of multimodal educational curricula within the acute care curriculum. This study aimed to evaluate a multimodal educational approach, including community partnerships, by assessing student confidence within the acute care curriculum at a rural Midwestern university in the United States, and to determine the influence of this approach on DPT students’ confidence in acute care settings.
Methods
Design
Using a descriptive phenomenological approach, seven physical therapy students (two males and five females) voluntarily participated in an interview focus group to elicit rich first-person accounts grounded in their perceptions and experiences in their acute care clinical rotation. This approach was selected to elicit rich, first-person accounts grounded in participants’ own perceptions. A small sample size was deemed appropriate for a focus group to achieve saturation and capture personal experiences. Participants were entry-level graduate students from a rural Midwestern doctoral physical therapy program in the United States who had completed their didactic learning and acute-care clinical rotation.
Ethical Considerations and Informed Consent
All procedures were reviewed and approved by the Central Michigan University Institutional Review Board Committee (study number 2022–1410). All procedures were in accordance with the 1964 Declaration of Helsinki. Informed consent was collected from all participants prior to data collection, including consent for publication of participant identifiers.
Previous Presentation
This paper’s abstract was presented as a poster presentation at the 7th Annual Herbert H. and Grace A. Dow College of Health Professions Research Symposium. The poster’s abstract was published in ‘Poster Abstracts’ in the symposium booklet. Hyperlink: Research Symposium Abstract Booklet.
Data Collection
Data collection and analysis followed Colaizzi’s seven-step process for descriptive phenomenology.9 In-depth, semi-structured interviews (Table 1) were conducted, utilizing a focus group-based open discussion with prompts by researchers to identify DPT students’ perceptions of the multimodal curriculum that utilized lectures, laboratories, IPE experiences, and community outreach in preparation for their acute-care clinical rotation. Interviews were conducted to gain students’ perspectives, and questions were developed based on literature and clinical expertise and were pilot-tested prior to use. Interviews were conducted via an encrypted audiovisual platform. The researchers facilitated the focus group using open-ended questions, working through prompted discussion points, and facilitating participants to elaborate on their responses for roughly an hour time span. Each participant was assigned a random number and asked to verbally state their assigned number before giving input during the focus group to keep track of each participant’s response and maintain confidentiality. Saturation was deemed achieved when responses did not elicit new or thematic information. Data was then transcribed verbatim into a password-protected, encrypted drive for further analysis.
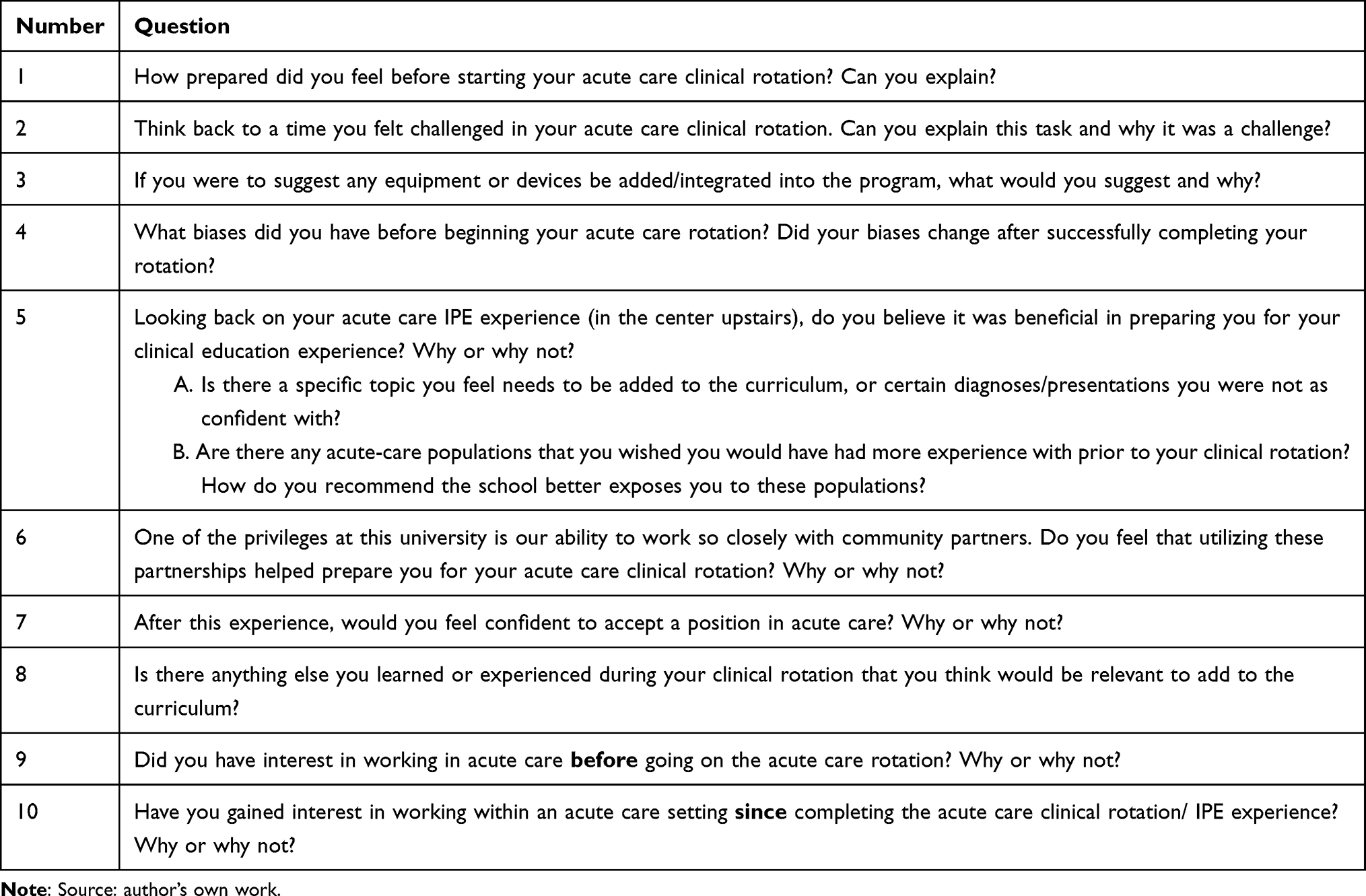 |
Table 1 Semi-Structured Interview |
Data Analysis and Trustworthiness
Following a phenomenological research paradigm to understand participants’ experiences, data analysis focused on identifying the facilitators and inhibitors of the proposed themes. Conventional content analysis is performed by counting the occurrences of words, phrases, or themes within the transcribed text. To promote credibility, the three researchers independently reviewed and coded transcripts. They then met to resolve discrepancies and refine the codebook collaboratively. Trustworthiness was further enhanced by maintaining audit trials and conducting member checks. The final codebook includes definitions of parent codes, representative quotes, and transcript references. In addition, the observation of each participant’s gestures and tone of voice was used to further analyze the data.
Results
The analyses revealed three themes: (1) confidence levels entering acute-care rotation, (2) perception of preparedness for acute-care clinical rotation, and (3) pre- and post-biases of acute care settings.
Theme 1: Confidence Levels Entering Acute Care Rotation
Qualitative analysis demonstrated that students felt moderately confident about being successful in their acute-care clinical rotation, based on an average score of 5/10 on a visual analog scale, with a 0 meaning “no confidence” and a 10 meaning “maximum confidence”. Participant 4 specifically stated that “having more of those (simulations) would have been even more helpful”.
When speaking about confidence in the participants, the majority stated that the institution’s pro-bono clinic was crucial in shaping their confidence levels. Participants mentioned that treating patients in the pro-bono clinic was a “confidence booster” that helped them create a better patient-centered language. In addition to treating patients in the pro-bono clinic, the participants were exposed to a community-based exercise class, which was an opportunity for students to have patient exposure once a week. Participant 6 stated, “… I would have been nervous to treat neuro (neurological diagnoses) if I didn’t do the exercise class often”. Although the community-based exercise class is not centered on the acute care curriculum, it does provide exposure to low-mobility community partners, which participants felt was beneficial in preparing them for their acute care rotation.
Theme 2: Perception of Preparedness for Acute Care Clinical Rotation
Almost all the students had similar perceptions of preparedness, stating that they felt moderately prepared. All participants stated that the complexity of IPE simulations and laboratory experience needed to be more complex to better simulate an acute care environment. All participants mentioned the incorporation of varying levels of complexity, such as the addition of multiple lines and assistive devices, varying levels of complexity in discharge planning, varying levels of personalities as acted out by volunteer patients in the IPE center, and varying levels of emergency scenarios.
Chest tubes, which were the hardest for me. the volume, the coloration, they can get dislodged in their thorax. use of more high-risk lines or equipment and simulate that rather than a catheter or IV because those are not life or death. (Participant 6).
Oxygen tanks. it is just something else that either you have to attach to the IV pole, carry with you, or figure out something to do with it. (Participants 1 and 2).
Incorporation of more lines in general in the IPE center. we dealt with a lot of catheters and nasal cannulas. (Participant 5)
In addition, many participants noted that increasing the complexity of discharge planning by continuously adding varying levels of the patient’s diagnosis, home life, and support system to accurately select the correct placement and increase the complexity of volunteer patient interactions in the IPE center would improve their perception of preparation for going into their acute care clinical rotation.
Discharge planning. we made all the recommendations and that was something I struggled with. just putting that together for a patient and figuring it out. (Participant 2).
Overall, the discharge planning could be a classroom discussion with case scenarios, continuously adding spin-off scenarios, and evaluating how those changes things for the patient. I think that it would be very helpful to talk through those scenarios. (Participant 3)
I think having the discharge plan conversation with the patients would be beneficial to practice and explaining to them the reason they are being discharged to the setting we recommended as PT’s and what that means for them. (Participant 1)
I had a patient that didn’t want to work with me, and he didn’t want me coming into his room to do exercises. having the standardized patients in the IPE center ‘Freak out’ on us students would have been helpful
Finally, many students felt that an introduction to emergency scenarios would have improved their perception of preparation for their acute-care clinical rotation.
I really struggled on room arrangement. knowing how to set up the room for the worst possible disaster. (Participant 3)
More emphasis on who you’re expecting to come help, positioning of the patient, and taking vitals immediately. for a patient having a seizure. that was a huge learning experience for me. (Participant 6).
Theme 3: Pre- and Post-Biases of Acute Care Setting
Biases are known to influence perception. Preconceived biases regarding acute-care clinical rotations can alter perceptions of experience. Multiple participants reflected on their biases towards being acute-care physical therapists. Multiple participants reported ‘not feeling valued’ (Participants 6, 4, and 1). Participant 2 further explained that working in acute care “did not feel like it was the most skilled regarding our position”. However, reflecting on their experiences, most of the participants retracted their original statements. Participant 2 stated that they “enjoyed it more than expected”, and many other participants agreed. Many participants did not have prior hospital exposure, which was reported to shape their confidence levels before starting their acute-care clinical rotation. Participant 3 stated that they “did not have any experience in the hospital”, which was part of the reason they were unsure about the setting. Participants stated that their acute care bias prior to their clinical rotations was a result of their prior exposure levels. Participant 2 stated that they were not sure if they “had enough exposure” to acute care, and they “did not know what to expect”.
At the end of the focus group, all participants stated that they would feel confident in accepting a position as an acute-care physical therapist. They credited their confidence to both their clinical rotation and the learning experiences they had experienced during their didactic education. Many indicated that their multi-modal education and patient exposure were beneficial to them in having successful acute care clinical rotation.
It is anticipated that students’ personal biases towards acute care prior to entering an accredited DPT program could play a role in their perception of and confidence in an acute care environment. A willingness to engage in extracurriculars or community partnerships could negatively impact students’ preparedness and confidence in their acute-care clinical rotation. In addition, many community partnerships occur outside the DPT curricula. Students may struggle to find additional time to engage in these activities because of the didactic demands of their doctoral programs.
Discussion
This study assessed the perceptions, experiences, and confidence of DPT students in their acute care clinical rotations following a multimodal approach to the acute care curriculum at a rural Midwestern university in the United States. Qualitative data collected from each participant through an open-ended focus group interview provided evidence of the effectiveness of the multimodal approach to education in the DPT program, evaluating the use of lectures, laboratories, simulations, and community partnerships to provide the tools needed to be confident and competent physical therapists in an acute care setting. This study showed that a multimodal approach to education increased the confidence levels of DPT students.
Student interaction with other healthcare professionals can also play a role in patient safety, ensuring interprofessional teams can communicate effectively.10 However, limited evidence has focused on the theme of simulation regarding the multimodal education strategy. Exploration of the theme of student preparedness and perceptions within the focus group process may be attributed to students’ exposure to the IPE center. Increased time within the IPE center may facilitate a student’s perception of their readiness when entering their acute care rotation in terms of treating patients, ensuring patient safety, and managing a complex environment. Literature reports that an acute-care IPE experience is a positive experience for DPT students.11,12 Although the literature has been positive regarding IPE experiences, limited evidence has evaluated program preparation, lacking research on community partnerships and other classroom experiences to prepare DPT students for a successful acute-care experience. The theme of community partnerships within the focus group highlights how involvement outside the DPT curriculum facilitates students’ confidence, preparedness, and communication skills by allowing them to work among diverse populations. However, it may be challenging for DPT programs to implement community partnerships and/or increased IPE time due to limitations in resources, geographical location, and access to an IPE simulation center.
The results of this study provide new evidence and student perceptions of a multimodal educational approach in a DPT acute care curriculum. Increasing DPT students’ confidence, communication, and critical thinking skills can positively impact patient safety.13 The transition to real-life clinical experience can be a challenge for students, and prior studies have been conducted discussing the dangers of a lack of clinical experience and confidence, and how it affects the ability of new graduates to safely practice within their field.14
Limitations
Sample Characteristics and Transferability
The sample was relatively homogeneous in terms of age, education level, and socioeconomic background. Although sex diversity was achieved, the small sample size and single-institution design limited transferability. Future research should consider multiple geographical regions and educational institutions.
Methodological Scope
Although a focus group elicits sharing from various perspectives and offers insight, participants may not have gleaned from an individual interview. The addition of in-depth individual interviews to future studies may provoke further contextual insights. Subsequent studies may benefit from mixed-methods or ethnographic approaches that further integrate environmental and cultural perspectives.
Conclusion
Qualitative information obtained from DPT students regarding their confidence in following a multimodal educational experience at this institution could enhance the future of healthcare. Physical therapists involved in acute care settings require clinical reasoning in complex and ever-changing environments. Providing physical therapy services in an acute care setting must also include heightened observation and assessment of patient safety due to the increased complexity of patient care. Student confidence in their abilities is a requirement for success in a fast-paced environment. Using student responses regarding their confidence in their acute care experience, researchers can help refine the acute care curriculum and provide physical therapy educators with more information on how best to prepare students for an acute care setting. With increased levels of confidence and experience prior to acute-care clinical rotation, students can safely and confidently care for complex patients.
Physical therapy programs are expected to use different strategies to allow students to apply critical thinking skills in real-world applications. By examining the effectiveness of the multimodal educational approach, this research can enhance the future of healthcare and build student confidence in real-world applications of their didactic knowledge.
Funding
No author has any financial interests or received any financial benefit from this research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Masley PM, Havrilko C-L, Mahnensmith MR, Aubert M, Jette DU. Physical therapist practice in the acute care setting: a qualitative study. Phys Ther. 2011;91(6):906–919. doi:10.2522/ptj.20100296
2. Lahey T, Ogrinc G, Fall L, Reeves S, Simons R. Wiley “Chip” Souba, Chapter 13 - the Compelling Need for Education Reform: A Futurist’s View of Health Professions Education. In: Wartman SA, Editors. The Transformation of Academic Health Centers, Academic Press; 2015:121–133. doi:10.1016/B978-0-12-800762-4.00013-X
3. Silberman NJ, Litwin B, Panzarella KJ, Fernandez-Fernandez A. High fidelity human simulation improves physical therapist student self-efficacy for acute care clinical practice. J Phys Ther Educ. 2016;30(1):14–24. doi:10.1097/00001416-201630010-00003
4. Fitzgerald C. What is multimodal learning? Available from: https://www.oakinnovation.com/blog/free-instructional-design-skills/what-is-multimodallearning#:~:text=Multimodal%20learning%20is%20an%20educational,a%20broader%20range%20of%20learners.
5. Shoemaker MJ, Riemersma L, Perkins R. Use of high fidelity human simulation to teach physical therapist decision-making skills for the intensive care setting. Cardiopulmonary Phys Ther J. 2009;20(1):13–18. doi:10.1097/01823246-200920010-00003
6. Archer E, Meyer IS. Applying empathic communication skills in clinical practice: Medical students’ experiences. South Afr Fam Pract. 2021;63(1). doi:10.4102/safp.v63i1.5244
7. Arena SK, Heeg S, Lewis A, Matero E. Doctor of physical therapy students’ perceptions of engagement in service learning with scouts: a descriptive study. Pediatric Phys Ther. 2022;34(2):239–244. doi:10.1097/pep.0000000000000871
8. Coss D, Chapman D, Fleming J. Providing occupational and physical therapy services in a free community-based interprofessional primary care clinic. J Interprof Care. 2021;35(sup1):26–32. doi:10.1080/13561820.2021.1981261
9. Phillips-Pula L, Strunk J, Pickler RH. Understanding phenomenological approaches to data analysis. J Pediatr Health Care. 2011;25(1):67–71. doi:10.1016/j.pedhc.2010.09.004
10. Jung H, Park KH, Min YH, Ji E. The effectiveness of interprofessional education programs for medical, nursing, and pharmacy students. Kor J Med Educ. 2020;32(2):131–142. doi:10.3946/kjme.2020.161
11. Dalwood N, Maloney S, Cox N, Morgan P. Preparing physiotherapy students for clinical placement. Simulation Healthcare. 2018;13(3):181–187. doi:10.1097/sih.0000000000000276
12. Reubenson A, Elkins MR. Clinical education of physiotherapy students. J Physiother. 2022;68(3):153–155. doi:10.1016/j.jphys.2022.05.012
13. Omura M, Maguire J, Levett-Jones T, Stone TE. The effectiveness of assertiveness communication training programs for healthcare professionals and students: a systematic review. Int J Nurs Stud. 2017;76:120–128. doi:10.1016/j.ijnurstu.2017.09.001
14. Murray M, Sundin D, Cope V. New graduate nurses’ understanding and attitudes about patient safety upon transition to practice. J Clin Nurs. 2019;28(13–14):2543–2552. doi:10.1111/jocn.14839
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.