Back to Journals » OncoTargets and Therapy » Volume 15
A Multidisciplinary Approach to the Management of Fibrolamellar Carcinoma: Current Perspectives and Future Prospects
Authors Polychronidis G, Murtha-Lemekhova A, Fuchs J ![]() , Karathanasi E, Hoffmann K
, Karathanasi E, Hoffmann K
Received 22 February 2022
Accepted for publication 8 June 2022
Published 3 October 2022 Volume 2022:15 Pages 1095—1103
DOI https://doi.org/10.2147/OTT.S296127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Georgios Polychronidis,1,* Anastasia Murtha-Lemekhova,1,* Juri Fuchs,1 Evdokia Karathanasi,2 Katrin Hoffmann1
1Department of General, Visceral and Transplant Surgery, Heidelberg University Hospital, Heidelberg, 69120, Germany; 2Post-Graduate Program “Human Genetics- Genetic Counseling”, Faculty of Medicine, University of Thessaly, Larisa, Greece
*These authors contributed equally to this work
Correspondence: Katrin Hoffmann, Department of General, Visceral and Transplant Surgery, Heidelberg University Hospital, Im Neuenheimer Feld 420, Heidelberg, 69120, Germany, Email [email protected]
Abstract: Fibrolamellar carcinoma (FLC) is a rare primary liver tumor affecting predominantly younger and otherwise healthy patients. Typically, FLC presents with advanced disease due to the paucity of typical symptoms and no history of underlying liver disease. Depending on tumor characteristics and the patient’s general condition, surgical treatment is the most promising treatment modality. Aggressive resection and liver transplantation have been utilized and are presently indispensable curative treatment options. Under certain circumstances surgical resection is also possible for metachronous metastases or local recurrence. Recent tumor biology discoveries have contributed to improved diagnostic specificity and systemic treatment options.
Keywords: hepatocellular carcinoma, fibrolamellar carcinoma, tumor recurrence, liver resection, surgery, transarterial radioembolization
Background
Fibrolamellar carcinoma (FLC) is a rare liver cell carcinoma which is not associated with cirrhosis or chronic hepatitis and is more common in younger ages (adolescents and young adults), with an estimated age-adjusted incidence rate of 0.02 per 100,000 in the United States.1 Originally described in 1956, it derives its name from its presentation ie, abundant fibrosis which is organized in characteristic lamellar bands.2,3 In the majority of the literature there is a slightly higher incidence among women and no specific race or geographical region related imbalance in incidence.4–6 No environmental exposures or toxins such as aflatoxin have been directly associated with FLC and neither have alcohol use, iron overload or other factors that contribute to conventional hepatocellular carcinomas. This is substantiated by the fact that the liver tissue surrounding the tumors seldom demonstrates any pathological findings.7,8
Clinical Findings
FLC lacks early or specific signs. A wide range of symptoms has been described, ranging from abdominal pain and distention, to more general symptoms such as malaise and weight loss.9 The most common symptom is a palpable mass or abdominal pain; however, FLC lesions are most often detected by chance during examinations for other clinical conditions.9 An array of other symptoms has been described spanning from gynecomastia to refractory hyperammonemic encephalopathy, to fulminant liver failure.9–13 Paraneoplastic symptoms are rarely described and not fully understood. A previous study has suggested that molecular pathogenesis resulting in overexpression of Aurora Kinase A may cause a urea cycle dysregulation, through upregulation of ornithine decarboxylase, which ultimately leads to excessive ornithine consumption and hyperammonemia.14 Gynecomastia may result from overexpression of aromatase P450 within the tumor cells, which catalyzes conversion of steroids to estrogens, thus leading to severely elevated levels of estrone and estradiol.12,15 As for markers, AFP is often normal or only slightly increased.9
Radiology
FLC habitually presents as a large single mass. Due to radiomorphological similarities to focal nodular hyperplasia (FNH), as both frequently present with a central scar, a misdiagnosis is possible. In fact, an association has often been reported between FNH and FLC, with some patients presenting with FLC and a history of surveillance for FNH and some presenting with both lesions simultaneously.16,17 FNH has previously been suspected to be a precursor of FLC but current evidence does not imply causality.18 FLC may first be viewed on an ultrasound as an incidental finding. Sonographic features are nonspecific, and a sonographer may merely see a heterogeneous echogenic lesion with echogenic center correlating to the central scar.19
Gadolinium-enhanced MRI is the preferred imaging modality for FLC. A central hypointensity on T2-weighted images correlates to the fibrous central scar and is a feature that can help distinguish between FLC and FNH, as the latter is frequently T2 hyperintense.19 Additionally, FLC may display T1 hypointensity, T2-hyperintensity, inhomogeneous arterial phase enhancement, hepatobiliary phase hypointensity, which may also help distinguish FLC from FNH, as well as high signal intensity on diffusion weighted imaging.19,20 On a contrast-enhanced CT, a FLC can exhibit lobulated margins. Without enhancement, FLC is hypoattenuating, while enhanced images show a heterogeneous hyperattenuation. A large central scar is a frequent feature in CT scans as well, albeit with low specificity. Oftentimes, calcifications within FLC can be seen, a feature infrequently encountered in FNH. Generally, as FLC frequently exhibits more aggressive features, such as vascular invasion, biliary obstruction, lymph node enlargement and distant metastases, those features may not only help differentiate the lesion from benign diagnoses, but also have a prognostic significance.20 In all, FLC should be considered in patients with suspected benign lesions other than FNH. Hemangioma exhibits a centripetal enhancement during the delayed phase, which has not been reported in FLC.19 Hepatic adenomas have a homogeneous hypervascularized enhancement.19
Pathophysiology
After sequencing FLC tumors, Honeyman et al demonstrated a deletion in chromosome 19 which leads to a combination of the subunits of the heat shock protein and the protein kinase A (PKA) into the DNABJ1-PRKACA.21,22 The transcription of this DNAJ–PKAc chimeric protein is expressed exclusively in FLC, in what has been shown to be a somatic mutation.21,23 The chimera can subsequently be separated into specific subcellular locations by fusion into the A-Kinase Anchoring Protein (AKAP) signaling complexes.24,25 Attributed to the DNAJ part, the protein interacts with the chaperonin heat shock protein 70 (Hsp70).26 The latter causes protein folding which could account for the high levels of DNAJ-PKAc compared to wildtype PKA in FLC tumors. Of note, although PKA is not classified as an oncogene, the subunit PKAc has been detected in the serum of various carcinomas.27 Recent advances in the understanding of the formation of this chimeric protein have led to the hypothesis that its chaperonin binding properties could facilitate oncogenesis while transforming the Protein Kinase A into a protein with tumorigenic potential.26
Pathology
Until now, no specific serum biomarkers have been detected. Contrary to conventional hepatocellular carcinomas, AFP is elevated in less than 5% of FLC patients, while there have been reports of elevated vitamin B12 binding capacity.28–30 The most common immune-histochemistry markers of the tumor cells are CD 68 and Cytokeratin 7.29,31,32 Although FLC has distinctive histologic and clinical features, hepatocellular carcinomas are often misidentified as FLC creating misconceptions on survival and recurrence rates. Some authors have reported RASSF1 methylation as grounds for this and showed distinctly different prognosis for mixed FLC tumors in retrospective studies.33 This misclassification could account for the discrepancies in patient ages reported in original studies and the SEER database analyses where a higher proportion of patients older than 50 years of age are commonly described.1,4,34–38 After the discovery of the DNAJB1–PRKACA chimera, FISH DNAJB1–PRKACA has been introduced as a diagnostic technique increasing specificity to almost 100% but has not yet been introduced to routine practice.31,39
Staging
Due to the differences in categorization and its rarity, there is no specific FLC classification and tumors are classified according to the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC) classification for hepatocellular carcinoma (Table 1).40 In the available reports the tumor stage was most often T1, comprising 42%, but vascular invasion is frequent in the tumor, thus T2 (13%) and T3 (28%) are also prevalent at diagnosis.34 T4 has been reported in approximately 8% of cases. Unknown stage at presentation was reported in 9% of cases, as reported by a recent SEER database analysis.34 Most FLC are diagnosed at an advanced stage, with AJCC stage III and IV amounting to 70–80% due to frequent lymph node and major blood vessels’ involvements.41
 |
Table 1 Staging According to the AJCC/UICC 8th Edition |
Surgical Treatment
Primary Resection and Liver Transplantation
The majority of FLC patients present with large tumors, often larger than 10cm.42,43 Notwithstanding, complete surgical resection is feasible mainly due to young age and the lack of cirrhosis, reaching rates up to 73% in adult and 84% in pediatric patients.28,44 Achieving negative resection margins is a cardinal priority, hence the majority of patients require a hemi-hepatectomy or trisectionectomy.45 Major resections are reported more often in smaller case series, such as in the study by Wahab et al with 90% of patients treated as such.46 Curative intent resections achieve R0 resection rates from 81% (reported by Darcy et al in pediatric patients) up to 96% (McDonald et al, National Cancer Database), although there is a notable selection bias and omission of missing data in such estimates.6,44,47 In very selected cases, palliative surgical tumor reduction can be performed in order to alleviate symptoms such as hyperammonemic encephalopathy but this is absolutely not standard.48
Resection is a factor greatly influencing the prognosis, with 5-year survival rates reaching up to 86% for stage I patients.43 Mavros et al reported of a 0% 5-year survival rate among patients who received chemotherapy (including palliative), intra-arterial therapy or other treatment instead.49 Generally, the reported 5-year overall survival (OS) for resection varies widely in the literature between 26–76% and with 5-year recurrence-free survival (RFS) and as low as 18%, spanning from 14 to 87 months44,50–53 (Table 2). Negative resection margins have been associated with better OS in young adults and adolescents where the 5-year OS of those who underwent complete resection was 51.6% versus 42.6% for R1/R2 and improved long-term overall survival was associated with R0 resection. This association was not present in other monocentric studies or database analyses.42
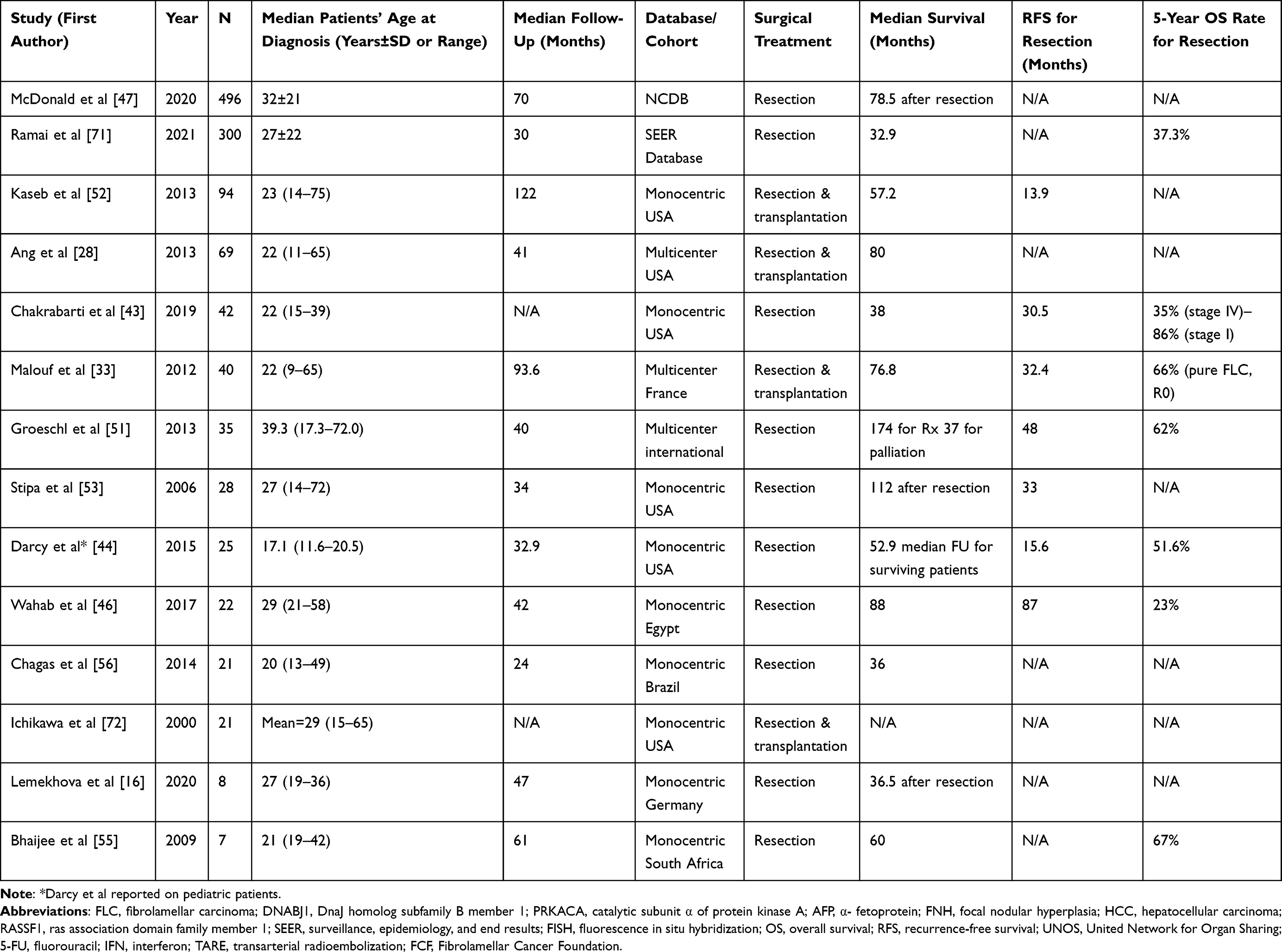 |
Table 2 Studies Reporting Surgical Treatment Outcomes (for Data Used Repeatedly, Such as the SEER Database, the Largest Sample Size Has Been Used) |
A number of other prognostic factors with variable significance have been described for FLC. Unfavorable factors include vascular and lymph-node invasion, tumor multiplicity and metastases at baseline.34,35,49,52 Furthermore, young age has been shown to positively influence survival, especially in the SEER database analyses, while risk estimates on sex are either insignificant or in favor of advantageous prognosis for female patients.
Liver transplantation is not a common therapeutic strategy for FLC on organizational grounds such as the need for specialized centers and lack of grafts in some regions but also due to the existence of nodal infiltration. When possible, transplantation has shown comparable OS to surgical resection treatment or at least far better OS than systemic therapy alone.50 Recent data from the UNOS registry showed a 48% 5-year OS for FLC but comparable 1-year and 3-year OS to HCC (77% and 68% for HCC vs 80% and 48% for FLC).54
Surgery for Recurrence
Recurrent disease is observed in the majority of patients after curative resection irrespective of resection margins, with a reported rate spanning from 50–80% for most reported studies and up to 100% in smaller monocentric analyses.6,16,42,55 Longer recurrence-free survival has been associated with younger age and lack of vascular invasion as well as lack of extrahepatic disease.42,51,56 While the most common sites of recurrence are the intraabdominal lymph nodes and the liver, FLC recurrence in terms of systemic disease is also diagnosed in the lungs and bones, with cases of peritoneal carcinomatosis or even duodenal recurrence.49,57–59 Malouf et al reported a 100% extrahepatic recurrence for pure FLC patients, with some also presenting with intrahepatic metachronous metastases.33 Repeated resection of recurrent FLC or metachronous metastases has been shown to effect survival, albeit the effect is less evident compared to surgery for primary tumors. Yamashita et al reported a median overall survival of 122 months for aggressive recurrent disease resection compared to 37 months with non-surgical therapies for recurrence; while, with a multimodal approach, Maniaci et al achieved a 112-month median OS and 48% 5-year OS in a 10-patient series.42,59 In another series, only intrahepatic recurrence was present, with a 61% rate and mean time to recurrence of 37 months.53 Metachronous metastasectomy was possible for all patients who had recurrence with an OS of 26 months as a result.53 Similarly, Kaseb et al reported a median OS of 145 months after re-resection for recurrence in contrast with 35 months OS for non-surgical treatment.52 These results demonstrate that very favorable outcomes can be achieved with close follow-up, timely resection, and careful patient selection. Therefore, all cases with recurrent FLC should be presented to a multi-disciplinary tumor-board and to specialized HBP surgeons.
Non-Surgical Treatment
To date there are no standard systemic therapies for FLC, and surgery remains the mainstream therapy.16 Non-surgical treatment shows worst overall survival, with 5-year overall survival estimated at 0%.49 Generally, chemotherapy in combination with surgery showed overall worse survival than surgery alone, potentially due to confounders and comparatively progressed disease.34 Utilization of interventional radiological methods has only been reported sporadically and their safety and efficacy remain to be evaluated.
Chemotherapy
Administration of chemotherapy is controversial in FLC and utilized on a case-to-case basis. For patients who present with unresectable disease (approximately 20–25%), a median survival can be estimated at 12 months.45 With chemotherapy, overall survival can be extended to 20.6 months.52
Notably, chemotherapy regimens are extremely variable. Sorafenib, a first-line therapeutic agent for HCC, has been used with inconsistent results: while some patients achieved stable disease, median survival did not surpass 10 months.43 Recently, it has been shown that the DNAJB1–PRKACA chimeric transcript can be detected in 100% of FLCs. This transcript leads to overexpression of Aurora kinase A, thus a selective Aurora kinase A inhibitor, ENMD-2076, has been evaluated in a Phase II multicenter open-label trial.60 Of 35 patients, only 1 (3%) had a partial response and 20 (57%) had stable disease, while overall survival was 19 months. As immunotherapy has been gaining popularity in HCC treatment as well, triple immunochemotherapy with 5-fluorouracil, interferon, and nivolumab was applied in patients with unresectable, metastatic, or relapsed FLC.61 Fifty percent partially responded to therapy, while 93% had either a partial response or stable disease. After 26 months over 90% of patients were still alive.61 In a pediatric cohort, platinum-based chemotherapy has shown to lead to a partial response in 31% of patients; however, 3-year overall survival was only 22%.62 Programmed cell death ligand-1 (PD-L1) is expressed on FLC tumor cells in approximately 63% and ca. 70% of patients exhibit PD-L1 positive tumor infiltrating lymphocytes and tumor-associated macrophages.63 So far, PD-L1 therapy has singularly been described in a patient who responded well to the treatment but without long-term results.43 At the moment there is one clinical trial recruiting patients for a DNAJB1-PRKACA Fusion Kinase Peptide Vaccine Combined with Nivolumab and Ipilimumab and one trial for Pembrolizumab in pediatric patients.23,64 Generally, chemotherapy in combination with surgery showed overall worse survival than surgery alone. From our point of view, this might be due to an already advanced tumor stage at time point of surgery necessitating (neo-) adjuvant treatment.
Neoadjuvant Treatment
Neoadjuvant chemotherapy for FLC is not habitually utilized and only reported sporadically. The regimens vary between sorafenib, sirolimus, 5-FU, Cisplatin, doxorubicin, carboplatin, bevacizumab, capecitabine, IFN, oxaliplatin, and often in various combinations. A report of ten patients with various regimes of neoadjuvant therapy showed a median survival of 60 months, which is marginally better than the survival after resection without neoadjuvant therapy according to a SEER database analysis.34,52 Oxaliplatin and gemcitabine have also been tried in one patient with a 16-cm FLC with extensive vascular invasion; the radiological response was favorable, with tumor reduction size to 8.5 cm. A follow-up of 14 months after resection was uneventful.65 Overall, the evidence for neoadjuvant treatment is very low and patient numbers too small for a clear recommendation. Each case should be discussed individually by a tumor-board.
Adjuvant Treatment
Surgery with adjuvant therapy showed a median survival of 110.5 months.34,52 However, evaluated chemotherapy regimens are heterogeneous, with most patients receiving interferon in addition to 5-fluorouracil and/or platin-based agents.52,59 Also, here individual treatment strategies can be discussed since clear standards and data are missing.
Interventional Radiology
Interventional radiology has recently gained popularity, yet it remains highly unexplored in rare liver lesions. Hepatic chemoembolization in a patient has shown good clinical and laboratory response, although diameter remained unchanged after repeated chemoembolization and the patient developed new lesions two years after initial treatment.66 Tumor embolization with lipiodol in otherwise unresectable disease led to overall survival of 38 months in one patient.55 Transcatheter oily chemoembolization was utilized in three patients. After several courses every 4 months, two patients displayed a decrease in tumor size and good tolerability, so that hepatic resection was feasible.67 Transarterial radioembolization (TARE) with Yttrium-90 has been introduced as a potential bridging therapy to hepatectomy or transplantation for HCC. Thus far it has been tried in two pediatric patients with unresectable FLC, both of which could be resected afterwards and had survived the follow-up of 12 months.68 These studies demonstrate that multimodal therapy needs further development and consistency as more and more patients may be treated with curative intent.
Conclusion
Fibrolamellar carcinoma is a rare, highly malignant liver lesion; however, if managed surgically, a favorable long-term result can be obtained. A multimodal approach has achieved resectability in a few otherwise unresectable patients and should be evaluated further in multicenter trials with adequate follow-up.
As DNAJ–PKAc is in essence a hallmark of FLC, its use as a primary diagnostic marker in specific populations should be established after further evidence has been generated in order to speed up therapy. Presentation at a multi-disciplinary tumor-board and to specialized HBP surgeons is absolutely mandatory to offer patients the best individual treatment. Advancements in systemic therapy can further support current surgical management to achieve better outcomes for patients with recurrent disease. Overall, clinical trials are important to gain more information and patient data should be summarized in an international registry such as Fibroregistry.org to create a collaborative research community amongst multiple academic specialties.69 Patients’ organizations such as the Fibrolamellar Cancer Foundation (FCF) can be counseled since they support the search for the right specialist and improve awareness and education amongst patients with fibrolamellar carcinoma.70
Acknowledgment
The authors would like to thank Mr. Nicholas J. Murtha for the language review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. El-Serag HB, Davila JA. Is fibrolamellar carcinoma different from hepatocellular carcinoma? A US population-based study. Hepatology. 2004;39(3):798–803. doi:10.1002/hep.20096
2. Craig JR, Peters RL, Edmondson HA, et al. Fibrolamellar carcinoma of the liver: a tumor of adolescents and young adults with distinctive clinico-pathologic features. Cancer. 1980;46(2):372–379. doi:10.1002/1097-0142(19800715)46:2<372::AID-CNCR2820460227>3.0.CO;2-S
3. Edmondson HA. Differential diagnosis of tumors and tumor-like lesions of liver in infancy and childhood. AMA J Dis Child. 1956;91(2):168–186. doi:10.1001/archpedi.1956.02060020170015
4. Eggert T, McGlynn KA, Duffy A, et al. Fibrolamellar hepatocellular carcinoma in the USA, 2000–2010: a detailed report on frequency, treatment and outcome based on the surveillance, epidemiology, and end results database. United Eur Gastroenterol J. 2013;1(5):351–357. doi:10.1177/2050640613501507
5. Lalazar G, Simon SM. Fibrolamellar carcinoma: recent advances and unresolved questions on the molecular mechanisms. Semin Liver Dis. 2018;38(1):51–59. doi:10.1055/s-0037-1621710
6. Assi HA, Mukherjee S, Machiorlatti M, et al. Predictors of outcome in patients with fibrolamellar carcinoma: analysis of the national cancer database. Anticancer Res. 2020;40(2):847–855. doi:10.21873/anticanres.14017
7. Graham RP, Craig JR, Jin L, et al. Environmental exposures as a risk factor for fibrolamellar carcinoma. Mod Pathol. 2017;30(6):892–896. doi:10.1038/modpathol.2017.7
8. Klein WM, Molmenti EP, Colombani PM, et al. Primary liver carcinoma arising in people younger than 30 years. Am J Clin Pathol. 2005;124(4):512–518. doi:10.1309/TT0R7KAL32228E99
9. Smith M, Tomboc PJ, Markovich B. Fibrolamellar hepatocellular carcinoma. In: StatPearls [Internet]. StatPearls Publishing; 2021.
10. Kastenhuber ER, Lalazar G, Houlihan SL, et al. DNAJB1–PRKACA fusion kinase interacts with β-catenin and the liver regenerative response to drive fibrolamellar hepatocellular carcinoma. Proc Natl Acad Sci USA. 2017;114(50):13076–13084. doi:10.1073/pnas.1716483114
11. Simon EP, Freije CA, Farber BA, et al. Transcriptomic characterization of fibrolamellar hepatocellular carcinoma. Proc Natl Acad Sci USA. 2015;112(44):E5916–E5925. doi:10.1073/pnas.1424894112
12. Mccloskey JJ, Germain-Lee EL, Perman JA, et al. Gynecomastia as a presenting sign of fibrolamellar carcinoma of the liver. Pediatrics. 1988;82(3):379–382. doi:10.1542/peds.82.3.379
13. Athanasakis E, Mouloudi E, Prinianakis G, et al. Metastatic liver disease and fulminant hepatic failure: presentation of a case and review of the literature. Eur J Gastroenterol Hepatol. 2003;15(11):1235–1240. doi:10.1097/00042737-200311000-00014
14. Surjan RC, Dos Santos ES, Basseres T, et al. A proposed physiopathological pathway to hyperammonemic encephalopathy in a non-cirrhotic patient with fibrolamellar hepatocellular carcinoma without ornithine transcarbamylase (OTC) mutation. Am J Case Rep. 2017;18:234. doi:10.12659/AJCR.901682
15. Agarwal VR, Takayama K, Van Wyk JJ, et al. Molecular basis of severe gynecomastia associated with aromatase expression in a fibrolamellar hepatocellular carcinoma. J Clin Endocrinol Metab. 1998;83(5):1797–1800.
16. Lemekhova A, Hornuss D, Polychronidis G, et al. Clinical features and surgical outcomes of fibrolamellar hepatocellular carcinoma: retrospective analysis of a single-center experience. World J Surg Oncol. 2020;18(1):93. doi:10.1186/s12957-020-01855-2
17. Saxena R, Humphreys S, Williams R, et al. Nodular hyperplasia surrounding fibrolamellar carcinoma: a zone of arterialized liver parenchyma. Histopathology. 1994;25(3):275–278. doi:10.1111/j.1365-2559.1994.tb01328.x
18. Vecchio FM, Fabiano A, Ghirlanda G, et al. Fibrolamellar carcinoma of the liver: the malignant counterpart of focal nodular hyperplasia with oncocytic change. Am J Clin Pathol. 1984;81(4):521–526. doi:10.1093/ajcp/81.4.521
19. Ganeshan D, Szklaruk J, Kundra V, et al. Imaging features of fibrolamellar hepatocellular carcinoma. Am J Roentgenol. 2014;202(3):544–552. doi:10.2214/AJR.13.11117
20. Yoon JK, Lee J, Jeong WK, et al. MRI features of histologic subtypes of hepatocellular carcinoma: correlation with histologic, genetic, and molecular biologic classification. Eur Radiol;2022. 1–15. doi:10.1007/s00330-021-08094-3
21. Honeyman JN, Simon EP, Robine N, et al. Detection of a recurrent DNAJB1-PRKACA chimeric transcript in fibrolamellar hepatocellular carcinoma. Science. 2014;343(6174):1010–1014. doi:10.1126/science.1249484
22. Xu L, Hazard FK, Zmoos A-F, et al. Genomic analysis of fibrolamellar hepatocellular carcinoma. Hum Mol Genet. 2015;24(1):50–63. doi:10.1093/hmg/ddu418
23. O’Neill AF, Church AJ, Perez-Atayde AR, et al. Fibrolamellar carcinoma: an entity all its own. Curr Probl Cancer. 2021;45(4):100770. doi:10.1016/j.currproblcancer.2021.100770
24. Riggle KM, Riehle KJ, Kenerson HL, et al. Enhanced cAMP-stimulated protein kinase A activity in human fibrolamellar hepatocellular carcinoma. Pediatr Res. 2016;80(1):110–118. doi:10.1038/pr.2016.36
25. Langeberg LK, Scott JD. Signalling scaffolds and local organization of cellular behaviour. Nat Rev Mol Cell Biol. 2015;16(4):232–244. doi:10.1038/nrm3966
26. Turnham RE, Smith FD, Kenerson HL, et al. An acquired scaffolding function of the DNAJ-PKAc fusion contributes to oncogenic signaling in fibrolamellar carcinoma. Elife. 2019;8. doi:10.7554/eLife.44187
27. Porter SE, Dwyer-Nield LD, Malkinson AM. Regulation of lung epithelial cell morphology by cAMP-dependent protein kinase type I isozyme. Am J Physiol Lung Cell Mol Physiol. 2001;280(6):L1282–L1289. doi:10.1152/ajplung.2001.280.6.L1282
28. Ang CS, Kelley RK, Choti MA, et al. Clinicopathologic characteristics and survival outcomes of patients with fibrolamellar carcinoma: data from the fibrolamellar carcinoma consortium. Gastrointest Cancer Res. 2013;6(1):3–9.
29. Graham RP, Torbenson MS. Fibrolamellar carcinoma: a histologically unique tumor with unique molecular findings. Semin Diagn Pathol. 2017;34(2):146–152. doi:10.1053/j.semdp.2016.12.010
30. Kanai T, Takabayashi T, Kawano Y, et al. A case of postoperative recurrence of fibrolamellar hepatocellular carcinoma with increased vitamin B12 binding capacity in a young Japanese female. Jpn J Clin Oncol. 2004;34(6):346–351. doi:10.1093/jjco/hyh050
31. Graham RP, Yeh MM, Lam-Himlin D, et al. Molecular testing for the clinical diagnosis of fibrolamellar carcinoma. Mod Pathol. 2018;31(1):141–149. doi:10.1038/modpathol.2017.103
32. Van Eyken P, Sciot R, Brock P, et al. Abundant expression of cytokeratin 7 in fibrolamellar carcinoma of the liver. Histopathology. 1990;17(2):101–107. doi:10.1111/j.1365-2559.1990.tb00679.x
33. Malouf GG, Brugières L, Le Deley M-C, et al. Pure and mixed fibrolamellar hepatocellular carcinomas differ in natural history and prognosis after complete surgical resection. Cancer. 2012;118(20):4981–4990. doi:10.1002/cncr.27520
34. Polychronidis G, Feng J, Murtha-Lemekhova A, et al. Factors influencing overall survival for patients with fibrolamellar hepatocellular carcinoma: analysis of the surveillance, epidemiology, and end results database. Int J Gen Med. 2022;15:393–406. doi:10.2147/IJGM.S338066
35. Ziogas IA, Ye F, Zhao Z, et al. Population-based analysis of hepatocellular carcinoma in children: identifying optimal surgical treatment. J Am Coll Surg. 2020;230(6):1035–1044.e3. doi:10.1016/j.jamcollsurg.2020.03.024
36. Mayo SC, Mavros MN, Nathan H, et al. Treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma: a national perspective. J Am Coll Surg. 2014;218(2):196–205. doi:10.1016/j.jamcollsurg.2013.10.011
37. Allan BJ, Wang B, Davis JS, et al. A review of 218 pediatric cases of hepatocellular carcinoma. J Pediatr Surg. 2014;49(1):
38. McAteer JP, Goldin AB, Healey PJ, et al. Hepatocellular carcinoma in children: epidemiology and the impact of regional lymphadenectomy on surgical outcomes. J Pediatr Surg. 2013;48(11):2194–2201. doi:10.1016/j.jpedsurg.2013.05.007
39. Cornella H, Alsinet C, Sayols S, et al. Unique genomic profile of fibrolamellar hepatocellular carcinoma. Gastroenterology. 2015;148(4):806–18.e10. doi:10.1053/j.gastro.2014.12.028
40. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
41. Chaudhari VA, Khobragade K, Bhandare M, et al. Management of fibrolamellar hepatocellular carcinoma. Chin Clin Oncol. 2018;7(5):5. doi:10.21037/cco.2018.08.08
42. Yamashita S, Vauthey J-N, Kaseb AO, et al. Prognosis of fibrolamellar carcinoma compared to non-cirrhotic conventional hepatocellular carcinoma. J Gastrointest Surg. 2016;20(10):1725–1731. doi:10.1007/s11605-016-3216-x
43. Chakrabarti S, Tella SH, Kommalapati A, et al. Clinicopathological features and outcomes of fibrolamellar hepatocellular carcinoma. J Gastrointest Oncol. 2019;10(3):554–561. doi:10.21037/jgo.2019.01.35
44. Darcy DG, Malek MM, Kobos R, et al. Prognostic factors in fibrolamellar hepatocellular carcinoma in young people. J Pediatr Surg. 2015;50(1):153–156. doi:10.1016/j.jpedsurg.2014.10.039
45. Kassahun WT. Contemporary management of fibrolamellar hepatocellular carcinoma: diagnosis, treatment, outcome, prognostic factors, and recent developments. World J Surg Oncol. 2016;14(1):151. doi:10.1186/s12957-016-0903-8
46. Wahab MA, El Hanafy E, El Nakeeb A, et al. Clinicopathological features and surgical outcome of patients with fibrolamellar hepatocellular carcinoma (experience with 22 patients over a 15-year period). World J Gastrointest Surg. 2017;9(2):61–67. doi:10.4240/wjgs.v9.i2.61
47. McDonald JD, Gupta S, Shindorf ML, et al. Elevated serum α-fetoprotein is associated with abbreviated survival for patients with fibrolamellar hepatocellular carcinoma who undergo a curative resection. Ann Surg Oncol. 2020;27(6):1900–1905. doi:10.1245/s10434-019-08178-x
48. Solipuram V, Baretti M, Kim AY, et al. Surgical debulking for refractory hyperammonemic encephalopathy in fibrolamellar hepatocellular carcinoma. Hepatology. 2021;74(5):2899–2901. doi:10.1002/hep.31998
49. Mavros MN, Mayo SC, Hyder O, et al. A systematic review: treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma. J Am Coll Surg. 2012;215(6):820–830. doi:10.1016/j.jamcollsurg.2012.08.001
50. El-Gazzaz G, Wong W, El-Hadary MK, et al. Outcome of liver resection and transplantation for fibrolamellar hepatocellular carcinoma. Transpl Int. 2000;13 Suppl 1:S406–S409. doi:10.1111/j.1432-2277.2000.tb02071.x
51. Groeschl RT, Miura JT, Wong RK, et al. Multi-institutional analysis of recurrence and survival after hepatectomy for fibrolamellar carcinoma. J Surg Oncol. 2014;110(4):412–415. doi:10.1002/jso.23658
52. Kaseb AO, Shama M, Sahin IH, et al. Prognostic indicators and treatment outcome in 94 cases of fibrolamellar hepatocellular carcinoma. Oncology. 2013;85(4):197–203. doi:10.1159/000354698
53. Stipa F, Yoon SS, Liau KH, et al. Outcome of patients with fibrolamellar hepatocellular carcinoma. Cancer. 2006;106(6):1331–1338. doi:10.1002/cncr.21703
54. Atienza LG, Berger J, Mei X, et al. Liver transplantation for fibrolamellar hepatocellular carcinoma: a national perspective. J Surg Oncol. 2017;115(3):319–323. doi:10.1002/jso.24515
55. Bhaijee F, Locketz ML, Krige JE. Fibrolamellar hepatocellular carcinoma at a tertiary centre in South Africa: a case series. South Afr J Surg. 2009;47(4):108–111.
56. Chagas AL, Kikuchi L, Herman P, et al. Clinical and pathological evaluation of fibrolamellar hepatocellular carcinoma: a single center study of 21 cases. Clinics. 2015;70(3):207–213. doi:10.6061/clinics/2015(03)10
57. Díaz Hernández HA, Gómez Ruiz IA, Torre A. Duodenal recurrence of fibrolamellar carcinoma 12 years after partial hepatectomy and adjuvant chemotherapy. ACG Case Rep J. 2016;3(4):e160. doi:10.14309/crj.2016.133
58. Kyziridis D, Kalakonas A, Zarambouka K, et al. Cytoreductive surgery and HIPEC for recurrent fibrolamellar hepatocellular carcinoma with peritoneal carcinomatosis. J Gastrointest Cancer. 2020;51(1):300–303. doi:10.1007/s12029-019-00236-7
59. Maniaci V, Davidson BR, Rolles K, et al. Fibrolamellar hepatocellular carcinoma–Prolonged survival with multimodality therapy. Eur J Surg Oncol. 2009;35(6):617–621. doi:10.1016/j.ejso.2008.12.009
60. Abou-Alfa GK, Mayer R, Venook AP, et al. Phase II multicenter, open-label study of oral ENMD-2076 for the treatment of patients with advanced fibrolamellar carcinoma. Oncologist. 2020;25(12):e1837–e1845. doi:10.1634/theoncologist.2020-0093
61. Gottlieb S, O’Grady C, Gliksberg A, et al. Early experiences with triple immunochemotherapy in adolescents and young adults with high-risk fibrolamellar carcinoma. Oncology. 2021;99(5):310–317. doi:10.1159/000513358
62. Weeda VB, Murawski M, McCabe AJ, et al. Fibrolamellar variant of hepatocellular carcinoma does not have a better survival than conventional hepatocellular carcinoma–results and treatment recommendations from the Childhood Liver Tumour Strategy Group (SIOPEL) experience. Eur J Cancer. 2013;49(12):2698–2704. doi:10.1016/j.ejca.2013.04.012
63. Kim AK, Gani F, Layman AJ, et al. Multiple immune-suppressive mechanisms in fibrolamellar carcinoma. Cancer Immunol Res. 2019;7(5):805–812. doi:10.1158/2326-6066.CIR-18-0499
64. Clinicaltrials.gov. Currently recruiting trials for FLC treatment; 2022. Available from: https://clinicaltrials.gov/ct2/results?cond=Fibrolamellar+Carcinoma&Search=Apply&recrs=b&recrs=a&recrs=f&recrs=d&age_v=&gndr=&type=&rslt=.
65. Fonseca GM, Varella AD, Coelho FF, et al. Downstaging and resection after neoadjuvant therapy for fibrolamellar hepatocellular carcinoma. World J Gastrointest Surg. 2014;6(6):107–111. doi:10.4240/wjgs.v6.i6.107
66. Semelka RC, Worawattanakul S, Mauro MA, et al. Malignant hepatic tumors: changes on MRI after hepatic arterial chemoembolization – preliminary findings. J Magn Reson Imaging. 1998;8(1):48–56. doi:10.1002/jmri.1880080113
67. Soyer P, Roche A, Rougier P, et al.Carcinome hépatocellulaire fibrolamellaire non résécable: évolution de 4 cas traités par chimiothérapie intra-artérielle [Nonresectable fibrolamellar hepatocellular carcinoma: outcome of 4 cases treated by intra-arterial chemotherapy]. J Belge Radiol. 1992;75(6):463–468. French.
68. Whitlock RS, Loo C, Patel K, et al. Transarterial radioembolization treatment as a bridge to surgical resection in pediatric hepatocellular carcinoma. J Pediatr Hematol Oncol. 2021;43(8):e1181–e1185. doi:10.1097/MPH.0000000000002089
69. The Fibro Registry. Available from: https://fibroregistry.org/ [homepage].
70. Fibrolamellar Cancer 1 Foundation. Fibrolamellar cancer foundation [homepage]. Available from: http://fibrofoundation.org/.
71. Ramai D, Ofosu A, Lai JK, Gao ZH, Adler DG. Fibrolamellar Hepatocellular Carcinoma: A Population-Based Observational Study. Dig Dis Sci. 2021;66(1):308-314. doi:10.1007/s10620-020-06135-3
72. Ichikawa T, Federle MP, Grazioli L, Marsh W. Fibrolamellar Hepatocellular Carcinoma: Pre- and Posttherapy Evaluation with CT and MR Imaging. Radiology. 2000;217(1):145-151. doi:10.1148/radiology.217.1.r00se46145
73. Amin MB, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York: Springer Cham; 2017.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.