Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
A Modified Expandable Headgear-Activator for Combined Adenotonsillar Hypertrophy and Bimaxillary Constriction: Insights from a 9-Year Follow-Up
Authors Qiu T, Sun M ![]() , Luo Y, Fang T, Liu X
, Luo Y, Fang T, Liu X
Received 22 March 2026
Accepted for publication 23 May 2026
Published 9 June 2026 Volume 2026:18 610362
DOI https://doi.org/10.2147/CCIDE.S610362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Tao Qiu,* Mouyuan Sun,* Yaxian Luo,* Tinglu Fang, Xiangtao Liu
Stomatology Hospital, School of Stomatology, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
*These authors contribute equally to this work
Correspondence: Mouyuan Sun, Stomatology Hospital, School of Stomatology, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected] Xiangtao Liu, Stomatology Hospital, School of Stomatology, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Abstract: This report describes the successful long-term, non-extraction orthodontic management of an adolescent with high-angle skeletal Class II malocclusion, bimaxillary constriction, lip incompetence, and chronic mouth breathing with adenotonsillar hypertrophy. Treatment initiated at CVMS II employed a patented headgear-activator appliance to achieve concurrent vertical control, mandibular advancement, and arch expansion, followed by fixed therapy. Five-year clinical follow-up with cephalometric evaluation at the end of active treatment confirmed significant skeletal correction, with the ANB angle reducing from 4.4° to 3.0°, while vertical dimensions remained stable (SN-MP: 41.8° to 41.3°; FH-MP: 34.3° to 32.2°). Transverse expansion resolved the posterior crossbite, transforming constricted arches into harmonious ovoid forms. Lip seal and a straight facial profile were achieved without surgical airway intervention. These outcomes suggest that early functional orthopedic treatment emphasizing three-dimensional control prior to fixed therapy can yield stable skeletal, occlusal, and aesthetic results while circumventing extractions. The prolonged soft tissue adaptation observed further underscores the necessity of extended follow-up for accurate assessment of orthopedic stability.
Keywords: modified headgear-activator appliance, class II malocclusion, high-angle, mouth breathing, bimaxillary constriction, growth modification
Introduction
Skeletal Class II malocclusion represents a prevalent dentofacial anomaly with a multifactorial etiology encompassing both genetic and environmental determinants.1 Among Asian pediatric and adolescent populations, malocclusion affects approximately 48% of individuals, with over half classified as Class II.2 This condition typically manifests as maxillary prognathism, mandibular retrognathism with posterior rotation, or a combination thereof, frequently accompanied by proclined anterior teeth that compromise dental aesthetics and elevate trauma risk.3 Management strategies range from functional orthopedics and compensatory fixed mechanics to combined orthodontic-surgical interventions.4
Maxillary arch constriction, frequently arising from chronic mouth breathing with adenotonsillar hypertrophy, can induce clockwise rotation of the mandible. This rotational pattern contributes to a high-angle facial configuration clinically recognized as long-face syndrome. Accordingly, high-angle skeletal Class II malocclusion is often associated with respiratory compromise, presenting clinically with chin retrusion, an elongated facial profile, and dentoalveolar narrowing.5 Affected individuals typically demonstrate a shortened mandibular ramus, reduced mandibular body length, insufficient posterior occlusion, compromised masticatory function, and concurrent airway impairment.
The modified headgear‑activator appliance proffers the dual biomechanical prerogative of simultaneous maxillary growth attenuation and mandibular protraction.6 In contradistinction to its conventional counterpart, this refined design transposes the J‑hook anchorage unit into closer anatomical alignment with the center of resistance of the maxillary anterior complex. Such biomechanical refinement affords augmented dominion over the anterior vertical dimension whilst expediting counterclockwise mandibular reorientation. Concomitantly, the fully integrated J‑hook assembly supplants the cumbersome extraoral superstructure, substantially ameliorating perioral soft tissue compression during nocturnal wear and thereby potentiating longitudinal therapeutic adherence. Despite ongoing debate regarding its optimal timing, the pubertal growth spurt is widely regarded as a favorable window for orthopedic intervention.7 The traditional Activator remains a fundamental orthopedic device, valued for its simplicity, cost-effectiveness, and well-documented biological effects.8
The J-hook headgear, an integral component of the Tweed-Merrifield technique, serves to intrude and retract maxillary incisors while concurrently stabilizing maxillary molars. This appliance is particularly indicated for high-angle Class II cases presenting with excessive incisor display, lip incompetence, and deep overbite.9 By integrating anterior vertical control, it enables precise management of the anterior vertical dimension, facilitates counterclockwise mandibular rotation, and allows for accurate control of facial height.
This report documents the long-term management of a mouth-breathing patient with bimaxillary constriction utilizing a patented headgear-activator appliance. It elucidates the therapeutic mechanism of this modified expansion-type device and presents comprehensive nine-year outcomes. These findings suggest that timely early orthodontic intervention may potentially obviate or simplify the complexity of comprehensive treatment for patients with skeletal malocclusion, while underscoring the necessity of prolonged follow-up for assessing orthopedic stability.
Case Report
A 9-year-old Chinese male presented with protruding maxillary anterior teeth. Extraoral assessment (Figure 1A) revealed classic features associated with mouth breathing, including increased lower anterior facial height, lip incompetence with excessive gingival display, allergic shiners, and a convex profile with everted lips. Intraoral examination (Figure 1B) demonstrated a permanent dentition with unerupted second molars, deep overjet and overbite, Class I canine and molar relationships, and enlarged tonsils. Analysis of study models confirmed bimaxillary transverse deficiency, characterized by triangular arch forms.
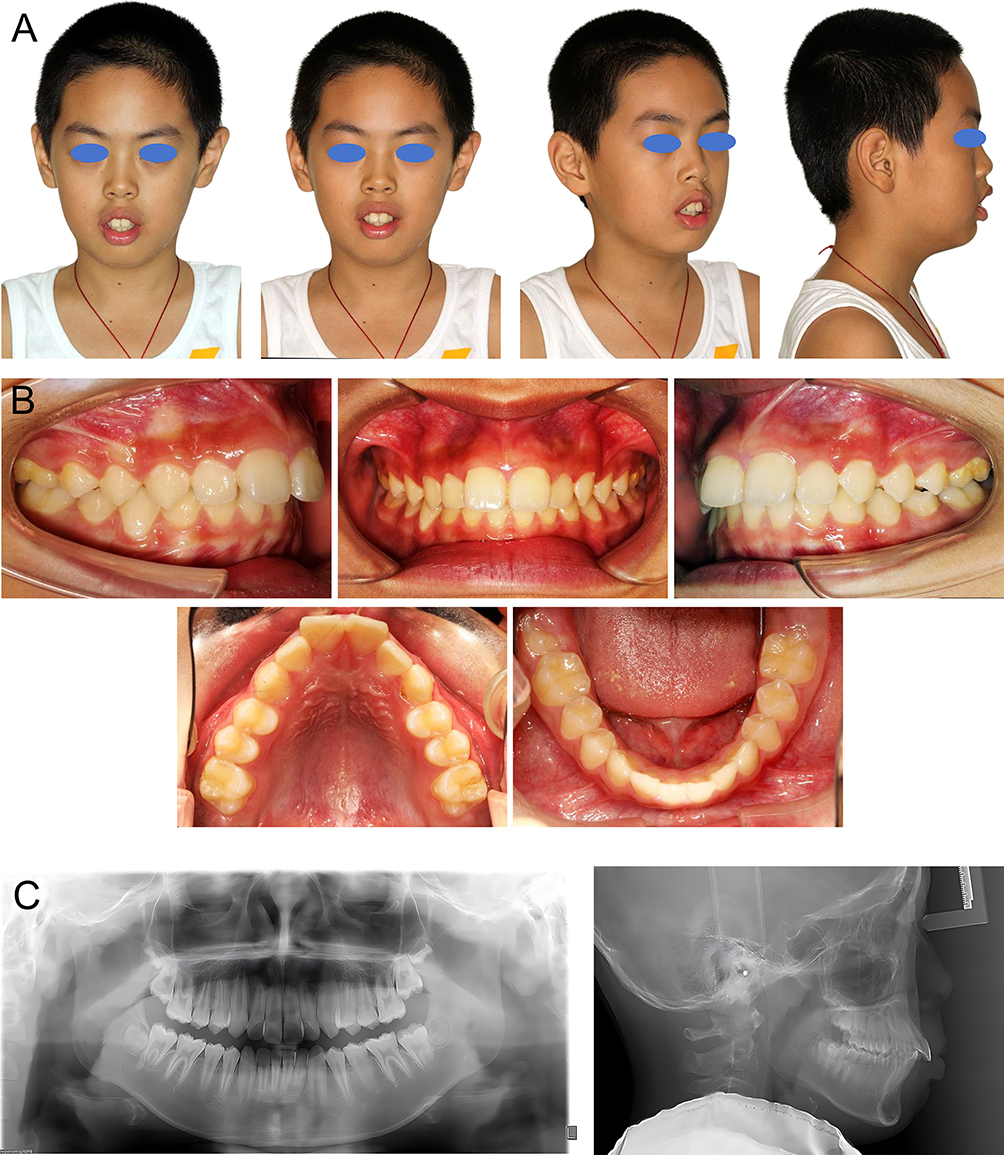 |
Figure 1 Extraoral & intraoral with radiographic examinations at pre-treatment stage. (A) Extraoral photographs. (B) Intraoral photographs. (C) Panoramic and Lateral Cephalometric Radiographs. |
Cephalometric analysis (Figure 1C and Table 1) confirmed a skeletal Class II relationship (ANB = 4.4°) accompanied by a high-angle mandibular plane (SN-MP = 41.8°). Soft-tissue evaluation demonstrated lip protrusion beyond the E-line. Airway assessment revealed adenotonsillar hypertrophy. Cervical vertebral maturation corresponded to CVMS II, indicating pre-peak growth potential.
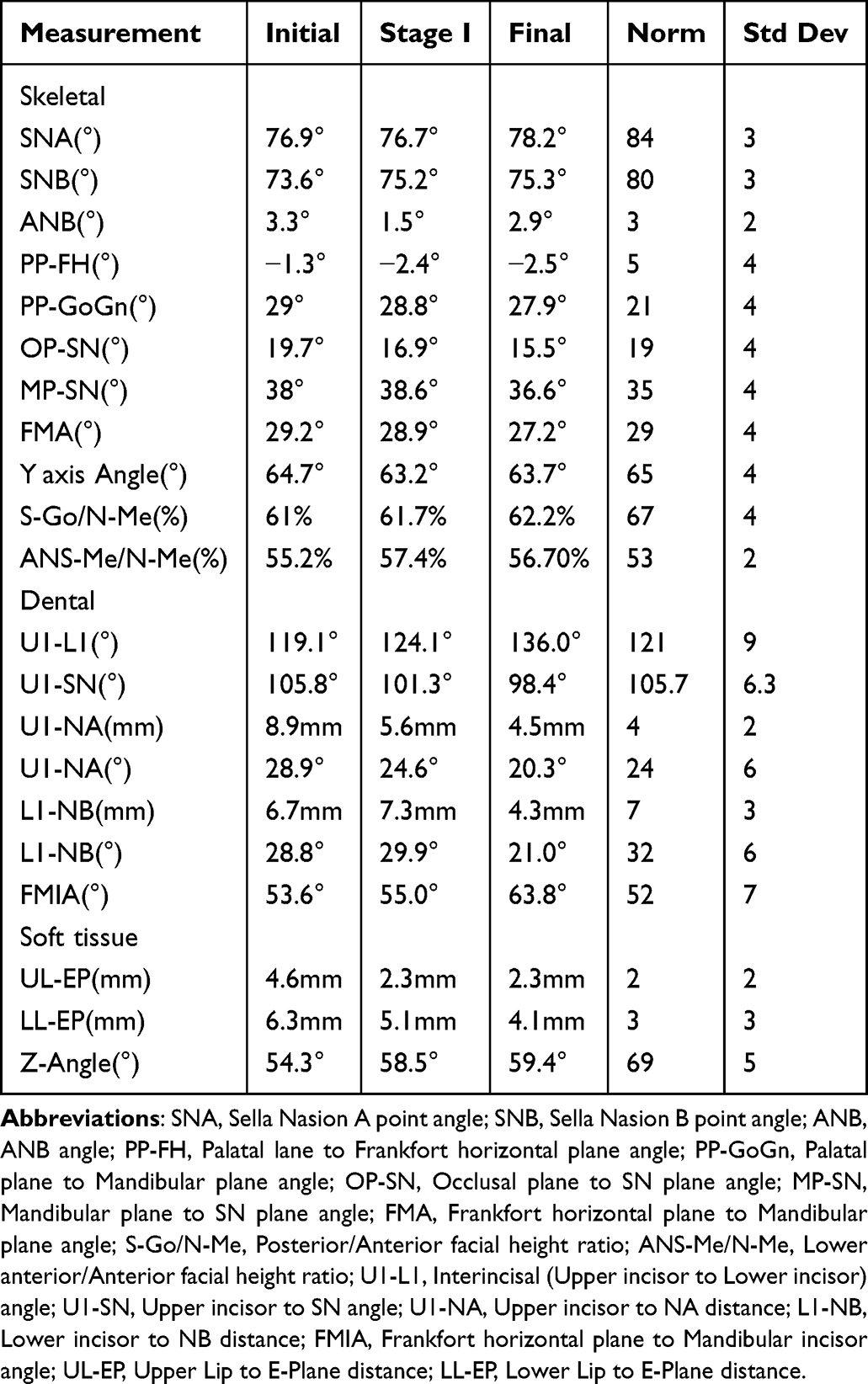 |
Table 1 Cephalometric Values of Pre-Treatment, Stage I and Post-Treatment |
The primary diagnoses included mandibular retrognathia, constricted maxillary and mandibular arches, and adenotonsillar hypertrophy. Treatment objectives were threefold: to advance the mandible with concomitant vertical control using a headgear-activator appliance, to achieve simultaneous arch expansion, and to monitor airway status throughout treatment.
Phase I orthodontic intervention deployed a modified expansion‑type activator amalgamated with high‑pull headgear and strategically positioned J‑hook assemblies (Figure 2A and B). Distinct from the conventional headgear‑activator paradigm, the J‑hook attachments were transposed to a mesial orientation relative to the maxillary canines (Figure 2D). This bespoke anchorage configuration propels the resultant force vector into intimate anatomical congruity with the center of resistance of the maxillary anterior complex, thereby conferring enhanced autonomy and precision in governing the anterior vertical dimension whilst expediting counterclockwise mandibular rotation. A midpalatal expansion screw was integrated to orchestrate harmonious transverse development (Figure 2D). High‑pull traction was channeled through the maxillary center of resistance to optimize vertical governance (Figure 2C).
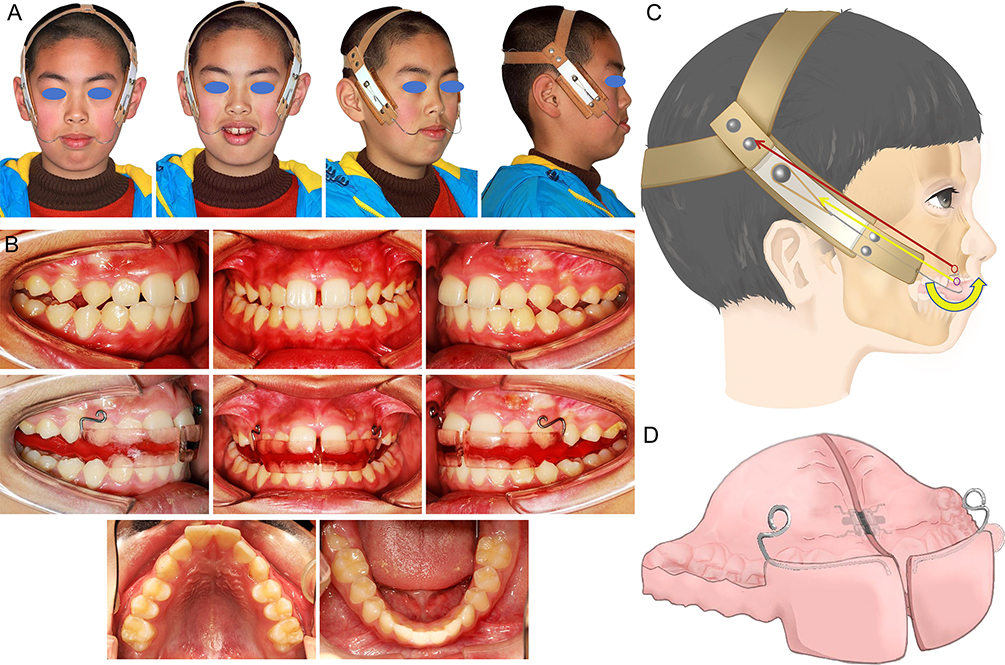 |
Figure 2 Extraoral and intraoral examinations in phaseItreatment. (A) Extraoral photographs. (B) Intraoral photographs. (C) Schematic Diagram of the Modified Expansion-Type Activator in Place. The purple circle represents the center of resistance of the upper dentition, and the red circle represents the center of resistance of the maxilla. The headgear J-hook applies force closer to the center of resistance of the maxilla, generating a translational force (red arrow). This results in a counterclockwise rotation combined with intrusion and retraction force on the upper dentition (yellow arrow). (D) Schematic Diagram of the Modified Expansion-Type Activator. |
The comprehensive therapeutic protocol synergistically amalgamated rapid maxillary expansion, mandibular advancement, and incisor intrusion with en masse retraction, applying 500 g of force per side. Notably, the fully integrated J‑hook architecture supplants the voluminous extraoral superstructure emblematic of traditional facebow designs, substantially attenuating perioral soft tissue compression during nocturnal wear and thereby potentiating sustained therapeutic adherence. A minimum daily wearing duration of 12 hours was mandated across a 12‑month treatment horizon.
Phase I treatment yielded notable clinical improvements, including enhanced lip competence and a more balanced facial profile (Figure 3A). Dental examination revealed a midline diastema and an anterior edge-to-edge relationship with residual posterior crossbite (Figure 3B), although transverse dimensions showed measurable improvement. Cephalometric assessment (Figure 3C and Table 1) demonstrated skeletal correction, with the ANB angle reducing from 4.4° to 1.9°. The mandibular plane angle remained stable (SN-MP: 41.8° to 41.6°). Maxillary incisors exhibited moderate retraction and intrusion, while mandibular incisor inclination was maintained.
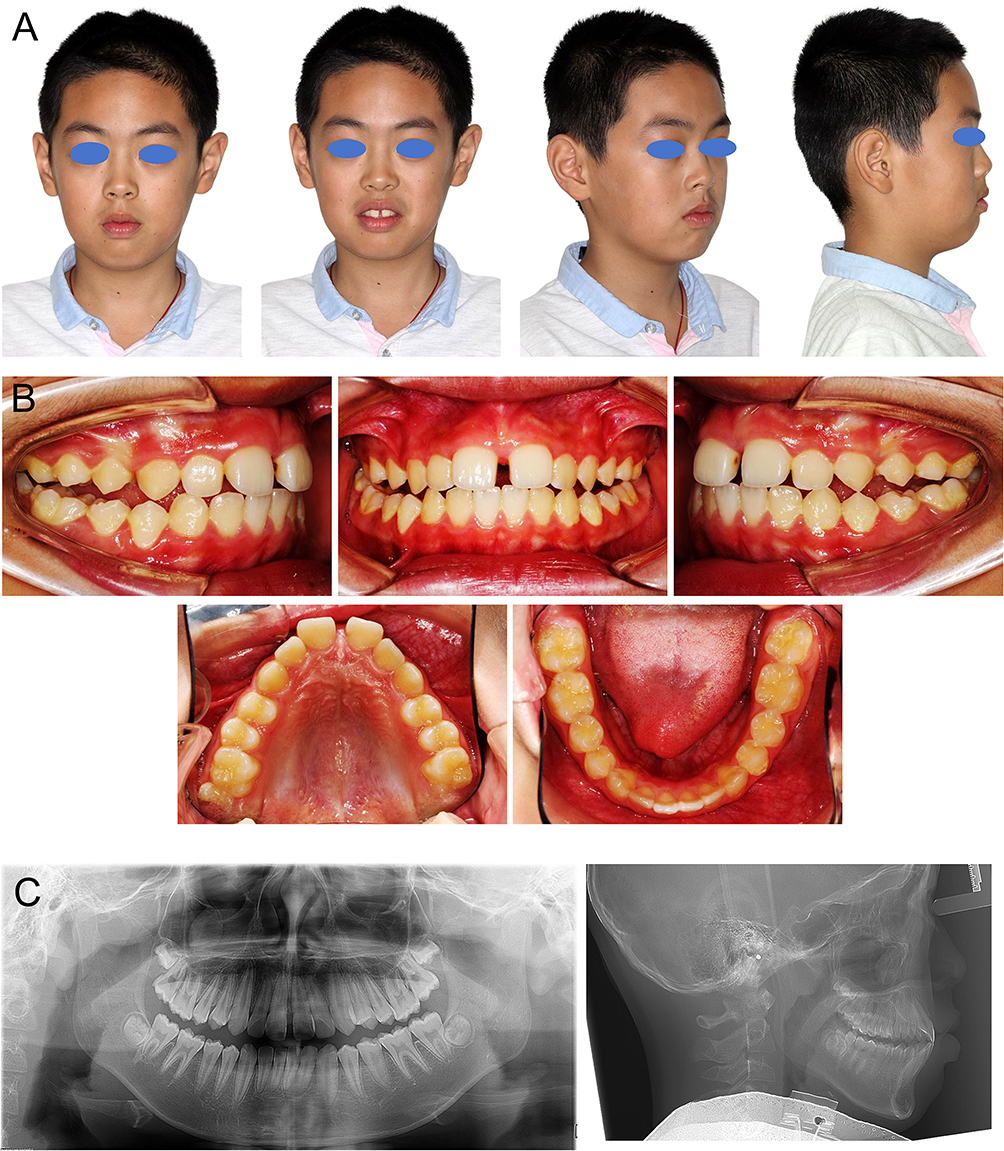 |
Figure 3 Extraoral & intraoral with radiographic examinations after phaseItreatment. (A) Extraoral photographs. (B) Intraoral photographs. (C) Panoramic and Lateral Cephalometric Radiographs. |
With residual growth potential confirmed (remaining at CVMS II) and skeletal correction achieved, Phase II treatment employed non-extraction fixed appliances (Figure 4A and B). Interarch elastics were utilized to correct the residual posterior crossbite, level the occlusal plane, and facilitate mild incisor retraction. Final records (Figure 5A–C) demonstrated Class I canine and molar relationships, normalized overjet and overbite, and well-aligned ovoid arch forms. Cephalometric assessment (Figures 3C, 5C, 6 and Table 1) confirmed a stable skeletal Class I relationship (ANB = 3.0°) with maintained vertical control (SN-MP = 41.3°). The soft-tissue profile exhibited marked improvement.
 |
Figure 4 Extraoral and intraoral examinations in phaseIItreatment. (A) Extraoral photographs. (B) Intraoral photographs. |
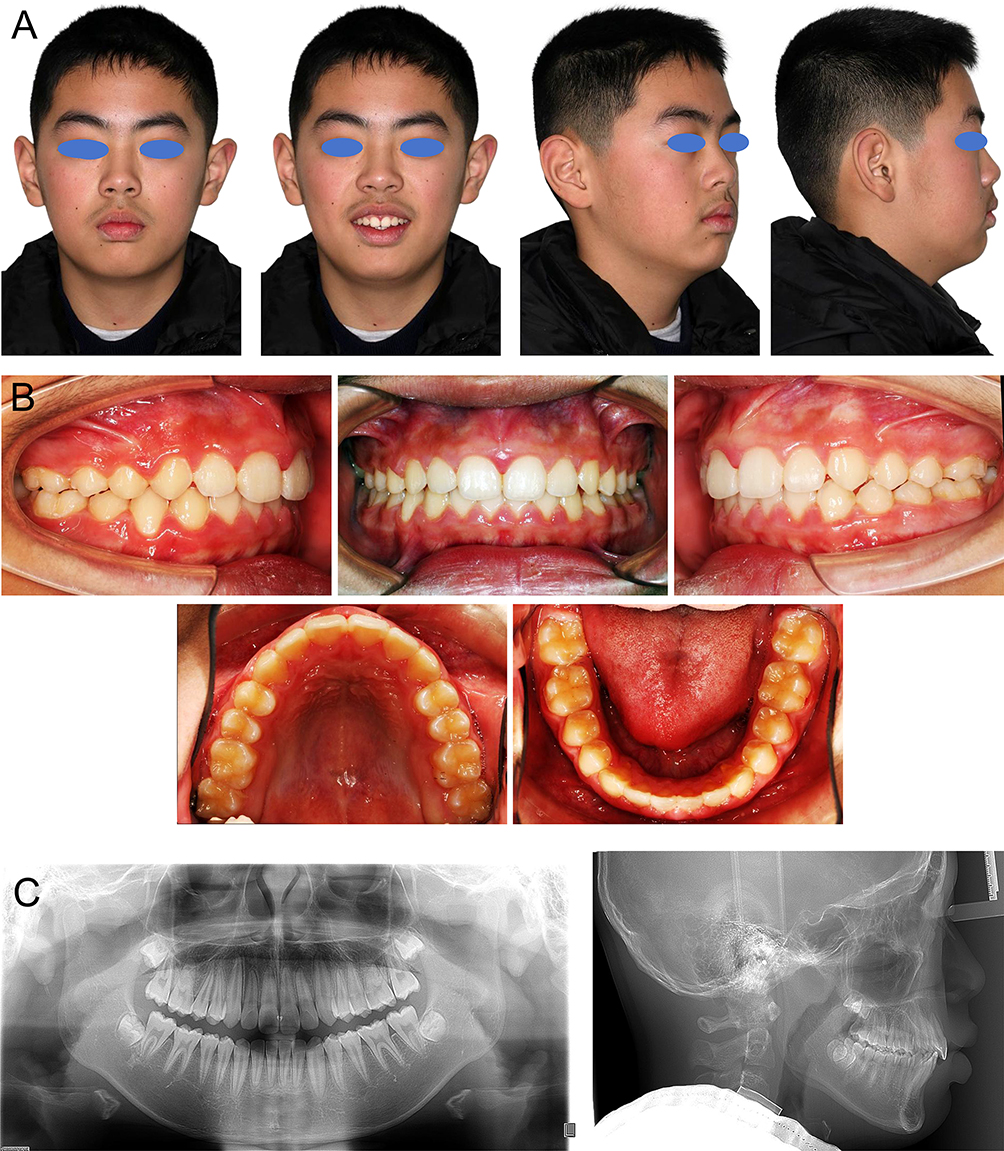 |
Figure 5 Extraoral & intraoral with radiographic examinations after phaseIItreatment. (A) Extraoral photographs. (B) Intraoral photographs. (C) Panoramic and Lateral Cephalometric Radiographs. |
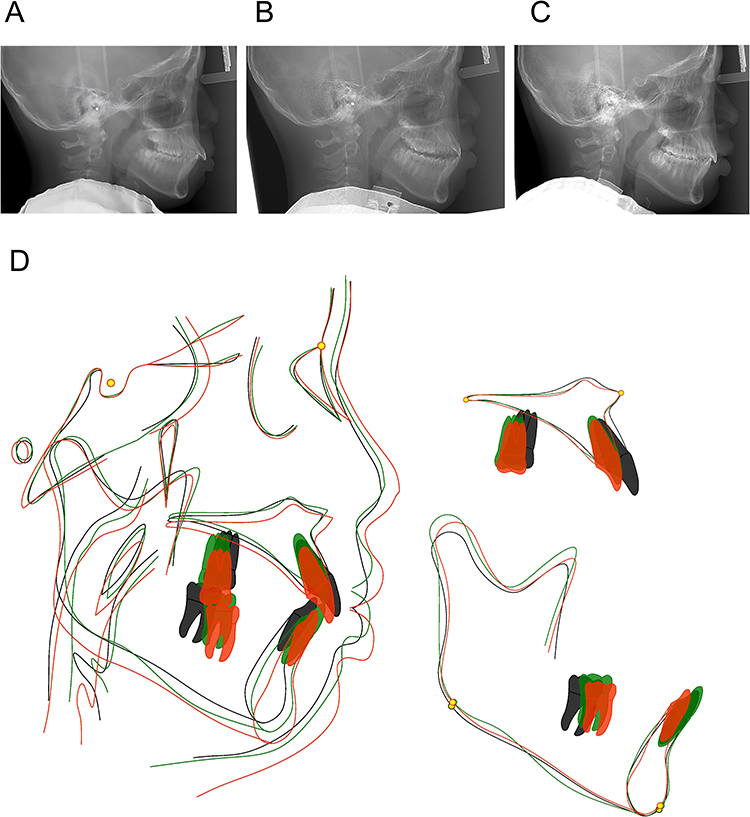 |
Figure 6 Lateral cephalograms and Cephalometric tracing of pre- and post-treatment and Stage along with superimpositions. (A) Lateral cephalogram at pre-treatment. (B) Lateral cephalogram after PhaseItreatment. (C) Lateral cephalogram at post-treatment. (D) Cephalometric tracing of pre-(black line) and post-treatment (red line) and StageI (green line) along with superimpositions. |
Retention was accomplished using a clear thermoplastic retainer. Follow-up assessments at five years (Figure 7) and nine years (Figure 8) revealed progressive soft tissue refinement and maintenance of a stable, straight facial profile.
 |
Figure 7 Extraoral and intraoral examinations in 5 year follow. (A) Extraoral photographs. (B) Intraoral photographs. |
 |
Figure 8 Extraoral and intraoral examinations in 9 year follow. (A) Extraoral photographs. (B) Intraoral photographs. |
Discussion
Globally prevalent, Angle Class II malocclusion arises from multifactorial etiology, including genetics and environmental determinants like harmful oral habits.7 Chronic mouth breathing, frequently secondary to adenotonsillar hypertrophy, exerts a profound influence on craniofacial development,10 contributing to long-face syndrome characterized by a hyperdivergent pattern, maxillary constriction, and lip incompetence.11 This case exemplifies the direct pathological association between airway compromise and the development of high-angle skeletal Class II malocclusion with bimaxillary constriction. Accordingly, early interdisciplinary management incorporating ENT assessment assumes critical importance.12
Managing high-angle Class II malocclusions necessitates sophisticated biomechanical control to restrain vertical growth while simultaneously improving sagittal relationships.13,14 The primary therapeutic objectives encompass vertical dimension control, prevention of clockwise mandibular rotation, and sagittal correction. This case illustrates how a modified expansion-type headgear-activator achieved these goals in a growing patient, effectively addressing the skeletal discrepancy prior to definitive alignment.
The biomechanical rationale for this approach rests on established principles.10,15 It is well recognized that a steep occlusal plane and excessive vertical development are associated with mandibular retrusion. Anterior tooth intrusion creates space that facilitates counterclockwise mandibular rotation.16 The modified appliance integrates high-pull headgear with J-hooks to intrude and retract the maxillary incisors, thereby counteracting clockwise tipping while also promoting mandibular incisor intrusion. Since the J-hook force line passes through the maxillary center of resistance, it additionally restrains maxillary growth (Figure 2C), a mechanism supported by the observed SNA changes following Phase I treatment.
Cephalometric analysis validated the therapeutic efficacy of this approach. The reduced SN-MP and FH-MP angles confirmed effective mandibular plane control,17–19 while anterior segment intrusion contributed to decreased occlusal plane steepness. Concurrent mandibular advancement improved the sagittal relationship, as evidenced by the reduction in ANB angle to a stable skeletal Class I configuration, all achieved without extractions.
Management of perioral muscle dysfunction constitutes an integral component of comprehensive orthodontic treatment.20 The active lip seal induced by the appliance may serve as a form of adjunctive myofunctional therapy. The progressive improvement in lip competence and facial profile observed over nine years underscores that soft-tissue adaptation in chronic mouth breathers follows the establishment of skeletal and dental harmony. This finding cautions against premature extraction-based profile correction before soft tissue adaptation is complete.
In summary, this report demonstrates that a modified functional orthopedic approach emphasizing three-dimensional control across sagittal, vertical, and transverse dimensions can effectively manage complex high-angle Class II malocclusions. The stable long-term outcomes achieved without extractions underscore the value of growth-modifying intervention and comprehensive retention protocols. Crucially, this therapeutic strategy necessitates interdisciplinary collaboration with ENT specialists to address airway patency, thereby promoting stable dentofacial health and minimizing relapse risk associated with persistent mouth breathing.
The present study acknowledges salient methodological limitations. The unavailability of cone‑beam computed tomography and polysomnographic datasets renders any extrapolations concerning airway dimensional modulation inherently conjectural. Although formal otolaryngological consultation was prompted, the absence of documented longitudinal follow‑up circumscribes definitive causal inference. These observations must therefore be interpreted with requisite circumspection, strictly as a solitary clinical vignette. The modified appliance undoubtedly presents a clinically pragmatic therapeutic alternative; nonetheless, its differential efficacy across discrete pharyngeal segments mandates rigorous substantiation through future multidisciplinary inquiries incorporating standardized volumetric imaging modalities.
Conclusion
This case demonstrates that early intervention during the late mixed or early permanent dentition, when substantial growth potential remains, is of critical importance for growing patients with hyperdivergent skeletal Class II malocclusion. A modified expansion-type Activator successfully addressed the sagittal discrepancy, transverse constriction, and vertical dimension without resorting to extractions or surgery, achieving stable skeletal, occlusal, and aesthetic outcomes over a nine-year period. This solitary clinical vignette, while illuminating the nascent therapeutic potential of the modified appliance, concomitantly demarcates salient trajectories for future scholarly pursuit. Notwithstanding its biomechanical efficacy, it is clinically imperative to underscore that this modified device functions as a removable orthodontic appliance. Consequently, the therapeutic outcome is inextricably contingent upon patient compliance; meticulous patient education and stringent monitoring protocols are therefore indispensable to ensure consistent wear and to actualize the observed skeletal modifications. Subsequent investigations integrating cone‑beam computed tomography and polysomnographic paradigms are imperative to rigorously quantify the differential morphometric impact upon nasopharyngeal and oropharyngeal airway compartments. The codification of a standardized multidisciplinary protocol, one that mandates comprehensive otolaryngological appraisal antecedent to orthodontic intervention, will prove indispensable for deciphering the intricate reciprocity between airway patency restoration and skeletal architectural correction. Large‑scale comparative trials are ultimately requisite to substantiate the generalized translational validity of this refined functional orthopedic approach.
Data Sharing Statement
Raw data supporting the findings of this manuscript are available upon request from Prof. Xiangtao Liu (Email: [email protected]), the designated corresponding author responsible for data sharing.
Ethics Approval and Consent to Participate
This work was reviewed and approved by the Ethics Committee of the Stomatology Hospital of Zhejiang University School of Medicine (No.2026-03-281). The study protocol followed the Declaration of Helsinki ethical standards for research involving human subjects. Informed consent was obtained from the patient and his guardian.
Consent for Publication
Written informed consent was obtained from the patient and his mother for the publication of this case report, including all accompanying images, clinical details, and identifiable data. The consent form explicitly permits the use of facial photographs, radiographic images, and clinical records contained in this manuscript. This process adhered to CARE guidelines in order to ensure all key details about the case are reported.
Acknowledgment
We sincerely thank the patients and their families for their long-term support and cooperation throughout this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82501180), Zhejiang Provincial Natural Science Foundation of China (LQN25H140004), Zhejiang Province Traditional Chinese Medicine Science and Technology Plan Project (2026ZL0078), China Oral Health Foundation (C2024-002), and Zhejiang Provincial Medical and Health Science and Technology Plan (2025KY942).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ding L, Chen R, Liu J, et al. The effect of functional mandibular advancement for adolescent patients with skeletal class II malocclusion on the TMJ: a systematic review and meta-analysis. BMC Oral Health. 2022;22:51. doi:10.1186/s12903-022-02075-8
2. Atasever Işler AA, Hezenci Y, Bulut M. Prevalence of orthodontic malocclusion in children aged 10–12: an epidemiological study. BMC Oral Health. 2025;25:249. doi:10.1186/s12903-025-05650-x
3. Alsaggaf DH, Afify AR, Zawawi KH, et al. Factors influencing the orthodontic treatment plan in Class II malocclusion. Am J Orthod Dentofacial Orthop. 2022;161:829–837.e821. doi:10.1016/j.ajodo.2021.01.034
4. Kaje R, Rashme R, Manimegalan P, et al. Assessing the efficacy of early versus late orthodontic intervention in the management of class II malocclusion: a comparative analysis. J Pharm Bioallied Sci. 2024;16:S2691–12. doi:10.4103/jpbs.jpbs_370_24
5. Thomas J, Kannan A, Kailasam V. Morphological dimension of the permanent dentition in various malocclusion: a systematic review and meta-analysis. BMC Oral Health. 2025;25:857. doi:10.1186/s12903-025-06203-y
6. Altenburger E, Ingervall B. The initial effects of the treatment of Class II, division 1 malocclusions with the van Beek activator compared with the effects of the Herren activator and an activator-headgear combination. Eur J Orthod. 1998;20:389–397. doi:10.1093/ejo/20.4.389
7. Giuntini V, McNamara JA, Franchi L. Treatment of class II malocclusion in the growing patient: early or late? Semin Orthodont. 2023;29:183–188. doi:10.1053/j.sodo.2023.04.008
8. De Oliveira Firmino JBM, França e Silva KK, Ribeiro Vasconcelos G, et al. 388 - Rapid maxillary expansion assisted by mini-implants in an adult with severe atresia: report of two sequent expansions. J World Fed Orthod. 2025;14:526. doi:10.1016/j.ejwf.2025.07.392
9. Amm E, Maalouf L, Mansour M, et al. Three-dimensional printed J-hook headgear: bridging traditional and contemporary orthodontic practices. AJO-DO Clin Companion. 2025;5:369–373. doi:10.1016/j.xaor.2025.05.006
10. Kim K-A, Kim S-J, Yoon A. Craniofacial anatomical determinants of pediatric sleep-disordered breathing: a comprehensive review. J Prosthodontics. 2025;34:26–34. doi:10.1111/jopr.13984
11. Dogra S, Kouznetsova VL, Kesari S, et al. Development of a miRNA-based deep learning model for autism spectrum disorder diagnosis. Adv Tech Neurosci. 2025;2:72–76.
12. Liu Y, Chen W, Wei Y, et al. The effect of orthodontic vertical control on the changes in the upper airway size and tongue and hyoid position in adult patients with hyperdivergent skeletal class II. BMC Oral Health. 2022;22:532. doi:10.1186/s12903-022-02580-w
13. Knigge RP, Hardin AM, Middleton KM, et al. Craniofacial growth and morphology among intersecting clinical categories. Anat Record. 2022;305:2175–2206. doi:10.1002/ar.24870
14. Lin R, Guo Y, Jiang W, et al. Advanced technologies for the study of neuronal cross-organ regulation: a narrative review. Adv Tech Neurosci. 2024;1:166–176.
15. Piełunowicz M, Kotuła J, Kotuła K, et al. Effects of rapid maxillary expansion and functional orthodontic treatment in children with sleep disordered breathing: a systematic review. BMC Oral Health. 2025;25:1059. doi:10.1186/s12903-025-06348-w
16. Wang Y, Zhou Y, Zhang J, et al. Long-term stability of counterclockwise mandibular rotation by miniscrew-assisted maxillary intrusion in adult patients with skeletal Class II high-angle malocclusion: a 10-year follow-up of 2 patients. AJO-DO Clin Companion. 2022;2:601–617. doi:10.1016/j.xaor.2022.08.002
17. Kerbrat A, Rivals I, Rouch P, et al. Specific postural alignment alterations due to long-face deformity in patients with maxillo-mandibular deformities. J Stomatol Oral Maxillofac Surg. 2025;126:102200. doi:10.1016/j.jormas.2024.102200
18. Guo Y-N, Cui S-J, Liu Y, et al. Quantitative evaluation of vertical control in orthodontic camouflage treatment for skeletal class II with hyperdivergent facial type. Head Face Med. 2024;20:31. doi:10.1186/s13005-024-00432-2
19. Maryenko NI. Applications of fractal analysis techniques in magnetic resonance imaging and computed tomography for stroke diagnosis and stroke-related brain damage: a narrative review. Adv Tech Neurosci. 2024;1:105–122.
20. Kui A, Bereanu A, Condor AM, et al. Craniocervical posture and malocclusion: a comprehensive literature review of interdisciplinary insights and implications. Medicina. 2024;60:2106. doi:10.3390/medicina60122106
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.