Back to Journals » Patient Preference and Adherence » Volume 17
A Mobile Application to Improve Diabetes Self-Management Using Rapid Prototyping: Iterative Co-Design Approach in Asian Settings
Authors Kwan YH, Ong ZQ ![]() , Choo DYX, Phang JK, Yoon S
, Choo DYX, Phang JK, Yoon S ![]() , Low LL
, Low LL ![]()
Received 16 August 2022
Accepted for publication 7 December 2022
Published 5 January 2023 Volume 2023:17 Pages 1—11
DOI https://doi.org/10.2147/PPA.S386456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Yu Heng Kwan,1– 4 Zhi Quan Ong,5 Dawn Yee Xi Choo,1 Jie Kie Phang,2,4 Sungwon Yoon,2,4 Lian Leng Low2,4,6– 9
1Department of Pharmacy, National University of Singapore, Singapore, Singapore; 2Health Services and Systems Research, Duke-NUS Medical School, Singapore, Singapore; 3Internal Medicine Residency, SingHealth, Singapore, Singapore; 4Centre for Population Health Research and Implementation, SingHealth Regional Health System, Singapore, Singapore; 5School of Computing, National University of Singapore, Singapore, Singapore; 6Population Health & Integrated Care Office (PHICO), Singapore General Hospital, Singapore, Singapore; 7Department of Family Medicine and Continuing Care, Singapore General Hospital, Singapore, Singapore; 8Post-Acute and Continuing Care, Outram Community Hospital, Singapore, Singapore; 9SingHealth Duke-NUS Family Medicine Academic Clinical Program, Singapore, Singapore
Correspondence: Lian Leng Low, Department of Family Medicine & Continuing Care, Singapore General Hospital, 20 College Road, Singapore, 169856, Singapore, Tel +65 63265872, Email [email protected]
Background: Diabetes is a global public health issue, causing burden on healthcare system and increasing risk of mortality. Mobile applications (apps) can be a promising approach to facilitate diabetes self-management. An increasingly utilized approach to facilitate engagement with mobile health (mHealth) technology is to involve potential users in the creation of the technology.
Objective: The aim of this study was to use co-design for type 2 diabetes mellitus (T2DM) self-management mHealth development.
Methods: Three rounds of iterative rapid prototyping panel sessions were conducted with a total of 9 T2DM participants in an Asian setting between Oct 2020 and April 2021. The participants were recruited through convenience sampling. For each round, feedback was gathered through qualitative interviews, and the feedback was used as a reference by the development team to develop and test a more refined version of the app in the next round. Transcribed semi-structured interview data was analyzed thematically using an inductive approach.
Results: Participants’ ages ranged from 40 to 69 years. Data saturation was reached, with no new themes emerging from the data. During the sessions, the participants expressed a variety of concerns and feedback on T2DM self-management using EMPOWER app and raised suggestions on the features of ideal T2DM self-management app. Important features include 1) reminders and notifications for medications, 2) Bluetooth integration with glucometers and blood pressure machines to minimize manual entry, 3) enlarged local food database including information on sugar content and recommendations for healthier options, 4) one touch for logging of routine medications and favorite foods, 5) export function for data sharing with physicians. Overall inputs concerned aspects such as user-friendliness of the app, customization possibilities, and educational content for the features in the mobile app.
Conclusion: In this study, we explored users’ opinions on a T2DM self-management mobile app using co-design approach. This study adds to the growing body of literature on co-designing behavioral mHealth interventions and can potentially guide researchers in mobile app design for other chronic conditions.
Keywords: type 2 diabetes mellitus, mHealth, mobile app
Introduction
Diabetes is a chronic disease that is rising across the globe, affecting approximately 537 million adults1,2 and accounting for 1.5 million of the total deaths globally in 2019.3 According to the National Health Survey 2019, the prevalence of self-reported diabetes, among Singapore residents aged 18 to 74 years was found to be 6.9%,4 in which the prevalence of type 2 diabetes mellitus (T2DM) among Singapore residents aged 18 to 69 years was anticipated to reach 15% by 2050.5 Diabetes can result in microvascular complications (ie, cardiovascular disease), macrovascular complications (ie, neuropathy, nephropathy, and retinopathy), and diabetes-related depression, all of which increase the risk of mortality, disability and decrease quality of life.6 Poor lifestyle habits6 and inadequate adherence to medications for diabetes were commonly observed.7–9 These behaviors could lead to inadequate glycemic control,10 contributing to the burden of diabetes such as increased medical cost and increased mortality rates.11
To effectively manage T2DM and prevent its complications, good self-management behaviors, in which patients actively involve themselves in their own care, need to be further emphasized as an essential role in complementing clinical care. Self-management interventions have been found in studies to increase medication adherence12 and to have clinically important benefits on glycemic outcomes13,14 and mental health outcomes.14 In fact, mobile applications (apps) have been utilized to deliver effective self-management support through supporting healthy lifestyle changes15–17 and encouraging medication adherence.18,19 However, low engagement with the apps may hamper users from reaping the benefits of the mobile apps.20,21 Having users to participate in the design process may result in a higher level of empowerment and engagement,22 which would assist mobile health (mHealth) apps in effectively supporting T2DM patients.23
Co-design refers to the active involvement of users in the creation of innovative products.24 By embracing users’ inputs, it can aid app designers in developing an app that better meet users’ requirements.25,26 Although co-designing has been proven to substantially improve patients’ experiences,27 increase user-friendliness and appeal of a mobile app,28 only limited studies on co-designing with users of a diabetes-related mobile app are available,29–32 which may be because co-design is still in developing stage in the area of healthcare.27 Furthermore, only limited qualitative studies on user engagement with mHealth apps have been undertaken in Asian settings.33 Previous studies have demonstrated that the effectiveness of digital interventions may be potentially influenced by culture.34,35 Among the qualitative studies that were conducted on patients’ perspectives of mHealth apps for diabetes management, the majority of them were conducted in non-Asian settings.17,36–40 In addition, our previous study has indicated the potential of nudges to promote T2DM self-management,41 and literature on digital nudging for T2DM self-management is scarce.42 Hence, this study aims to use co-design for T2DM self-management mHealth development.
Methods
Study Design
A co-design approach was used, which utilized qualitative methods in rapid prototyping process (RPP). We adopted the co-design framework suggested by Sanders & Stappers43 in this study. A rapid prototyping approach was utilised to obtain input from users to quickly create and improve the design of app prototypes.44 This approach enables developers to build, test and make revisions rapidly through feedback loops to ultimately yield a superior and functional prototype.45
Ethical approval for this study was obtained from SingHealth Centralized Institutional Review Board (CIRB Ref No.: 2019/2468). Informed consent was obtained from the participants prior to their involvement in the study.
EMPOWER App
Initial design ideas of the EMPOWER app were derived from focus group discussions (FGDs) with 29 T2DM patients and 56 healthcare professionals previously.41 These FGDs explored their interactions with mHealth apps that were available on the market, and their preferences for apps that promote healthy lifestyle behavior. The initial wireframes for the EMPOWER app were also developed in accordance with the Behavior Change Wheel46 to raise users’ awareness of how their lifestyle behaviors could affect their condition and for the app to effectively encourage action for behavior change.
Following that, the app prototype was developed and introduced in Round 1. Four features (ie, Activity Logging, Medication Plan, Report, Patient Diary) were available in the app initially. Subsequently, another 4 features (ie, Appointment Management, Gamification, Goals Setting, Educational Materials) were incorporated before Round 2. Notification feature was then added before Round 3. These features are described in Table 1.
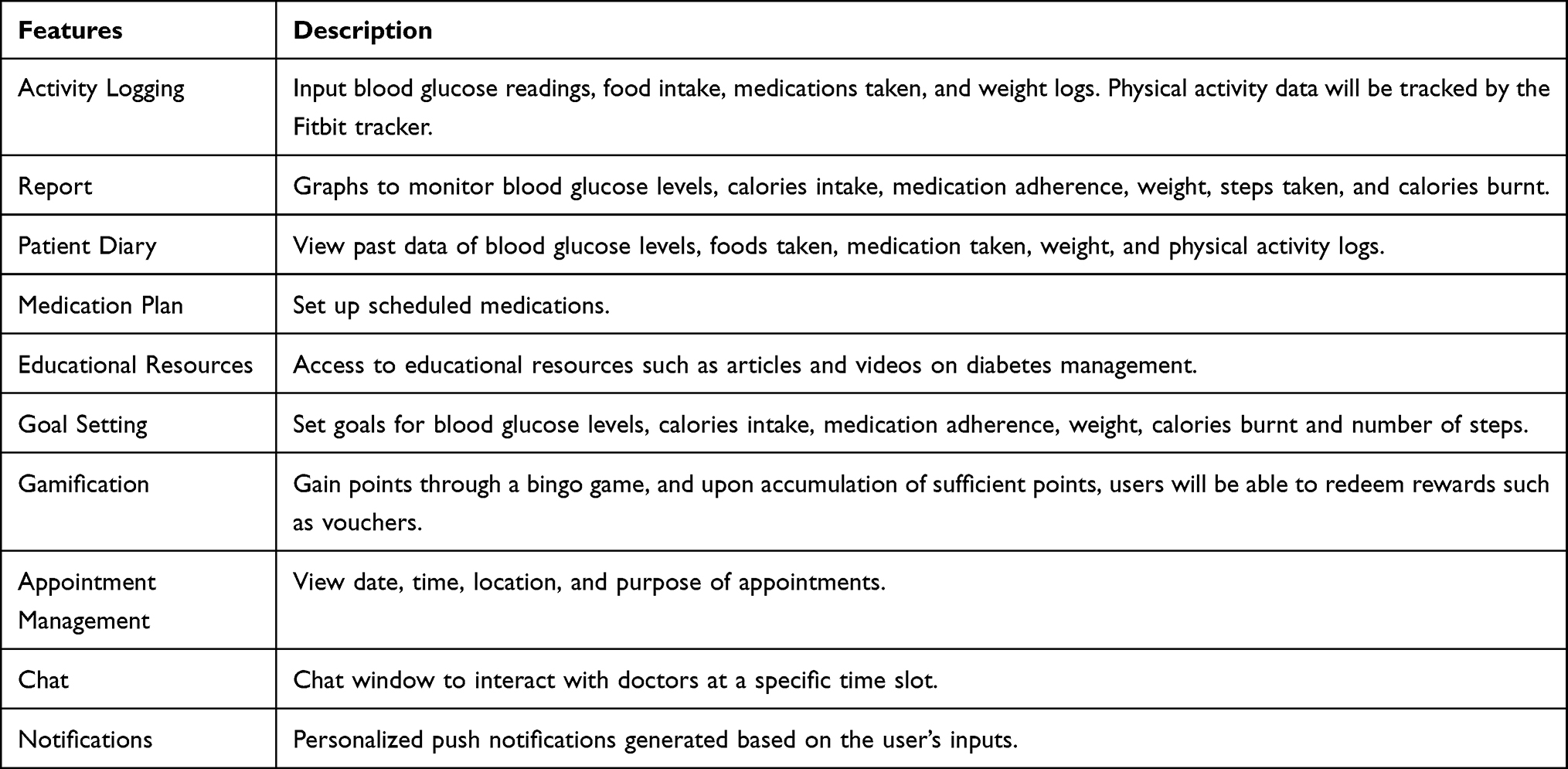 |
Table 1 EMPOWER App Features |
Participants
We recruited participants for the RPP from the original pool of participants who participated in previous studies (manuscripts under review). Eligible participants included those who were 40 years old and above and had the diagnosis of T2DM. Patients who presented diabetes-related complications or gestational diabetes were excluded. We recruited participants who were more vocal and ensured that both technologically savvy and non-technologically savvy participants were included. Out of the 9 participants who were approached, all nine participants agreed to participate in the RPP sessions. However, one participant dropped out after Round 1 as she was concerned that she was not technologically savvy enough to test the app. Due to scheduling conflicts, only 3 participants were able to participate in all 3 rounds. The number of participants who were involved in Rounds 1, 2, 3 were 7, 5, 5, respectively. Each participant was rewarded $40 per session for their participation.
Data Collection
Prior to the RPP sessions, the participants were asked to use the app. We provided 10-minute free-and-easy app testing before commencing the RPP session if any participants have not tested the app. For each RPP session, feedback was gathered which was used as a reference by the development team to develop and test a more refined version of the app in the next round. The purpose and scope of the app were refined, possible pitfalls were addressed, new updates were introduced briefly, and design features were discussed.
Three trained interviewers conducted the sessions through a video conferencing software (Zoom). The sessions were audio-recorded, and each session lasted between 75 and 110 minutes. We conducted 3 rounds of RPP sessions in total. The sessions were facilitated by using a semi-structured interview guide (Supplementary Table 1) for each round. Qualitative data was collected between 30 Oct 2020 to 27 April 2021.
Data Analysis
Qualitative data was analyzed using a thematic analysis approach using NVivo 12 Software (QSR International). An inductive approach was performed to develop codes and themes without trying to fit into an existing framework. The 6-step thematic analysis approach (familiarizing with data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, as well as producing the report) recommended by Braun and Clarke47 was used.
Results
Demographics of Participants
In total, there were 6 female participants (67%) and 3 male participants (33%) who participated in the RPP sessions. Data saturation was reached, with no new themes emerging from the data. The participants ranged in age from 40 to 69 years, with the most common age range being 60 to 70 years (56%). Further participant characteristics are summarized in Supplementary Table 2.
Prototype Development
The key themes, their definitions and quotes from participants are summarized in Supplementary Table 3 and Supplementary Table 4. The suggestions offered by participants, how the prototypes reflected the suggestions, and potential integration work are summarized in Table 2.
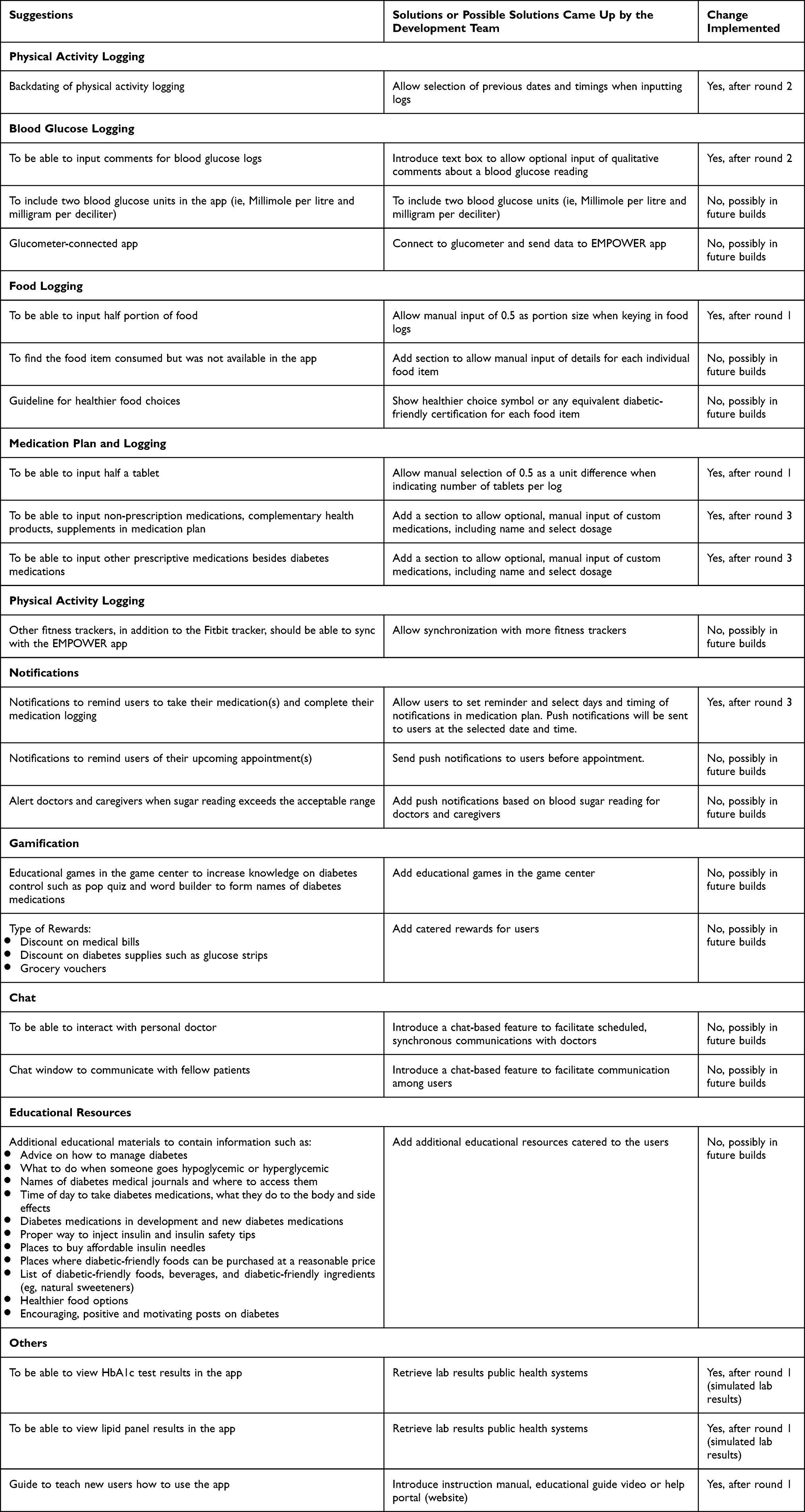 |
Table 2 Suggestions of EMPOWER App and Solutions |
App Features
Blood Glucose Logging
In Round 1, a participant pointed out that a glucometer-connected mobile app could eliminate the need for users to enter blood glucose readings manually. In addition, as blood glucose levels can be measured in two different units – millimoles per litre (mmol/L) and milligrams per decilitre (mg/dL), a participant enquired whether both units could be incorporated in the app. In Round 2, a participant who received insulin treatment stated that regular inputting of blood glucose readings helped him in titrating his insulin dose. In round 2, another participant emphasized the importance of adding comment box for blood glucose readings to understand the cause of fluctuations in blood glucose levels eg, due to consumption of “sinful food”.
Food Logging
Participants liked the availability of local food options, and the capacity to log in as many meals as they consumed throughout the day. As the EMPOWER app allowed users to view a food’s nutritional information, it could advise users to control portion sizes. In Round 2, one participant stated that the provision of carbohydrate content information aided him in meal planning. However, due to the extensive food options available in the database, selecting a food item that matched what they had consumed became more complicated. Despite the extensive food options available in the database, three participants pointed out that not all food options, such as home cooked meals, were in the database. Fortunately, the participants understood that they could select a similar option or enter the food details manually. Other suggestions raised by the participants to improve the app included providing a list of healthier options and displaying the sugar content of foods.
Medication Plan and Logging
Suggestions included allowing backdating medication logs, permitting logging of partial doses of medication, including non-diabetes medications and including complementary health products. In Rounds 1 and 2, three participants also enquired whether they could record medication by simply tapping on a button instead of typing in the medication name every time.
Physical Activity Logging
Since the physical activity logging feature required a connection to a fitness tracker, four participants hoped that a tracker would be provided to motivate their use of the app. In Round 3, two participants expressed concern that the EMPOWER app could only pair with a single brand of tracker, given that different brands of tracker wearables are available in the market.
Patient Diary
Participants mentioned that the ability to view their previous entries using the diary function is beneficial to remind them of their previous inputs.
Report and Goal Setting
All participants valued the significance of blood glucose trending and food tracking in the report section to determine whether they were on track. If they were not, it would nudge them to take the necessary steps to control their condition. If there was spike in the trend of blood glucose levels, they could find out which meal that caused it and subsequently adjust their meal intake accordingly. The participants also valued the ability of the app to export their trends for their doctor to view and better understand their situation.
As the EMPOWER app allowed users to view their progress over a period, they might experience negative or positive emotions depending on the outcome of the trend. For example, participants stated that the readings served as a reminder and encouragement to persevere and strive for their goals. However, users may become demotivated when goals were not met. In Round 3, one participant expressed that while progress that fell short of his expectations could dampen his spirits, it would remind him to keep going at a steady pace.
Notifications
Participants valued the notification feature as it would serve as a reminder to take their medications. In Rounds 1 and 2, two participants mentioned that they envisioned the app to alert their doctor or caregiver when their readings were significantly outside of the acceptable range.
Appointment Management
Although all participants found the appointment management feature useful, two participants in Round 1 voiced out that this was a duplication of function in other health apps. They would prefer an integrated app to avoid the need to use multiple apps.
Gamification
This gamification feature had received an unenthusiastic response from most participants. In Round 1, one participant that expressed his disinterest asserted that his only purpose of using this app was to manage his condition. In Rounds 2 and 3, participants mentioned that they would be enticed to play the game if the rewards included grocery vouchers, discounts on their medical bills or discounts on glucose strips. In Round 3, participants suggested including educational games to raise users’ level of diabetes knowledge.
Educational Materials
Even though the educational resources available were limited, most participants were contented with this feature. The participants mentioned that the educational resources appeared useful, informative, and reliable. However, in Rounds 1 and 2, three participants stated that they were already well informed about their condition and that the educational resources would be better suited for patients newly diagnosed with diabetes. Participants also suggested the desired information to be included in the app, including information on diabetes management, diabetes medication, insulin injection technique, diabetic-friendly foods and beverages, and places to purchase affordable diabetes supplies.
Chat
In Round 1, three participants expressed skepticism when asked about the possibility of a chatting platform with doctors, raising concerns such as whether time required to receive reply. One suggestion raised was to have a chatting platform among patients with diabetes for emotional support and sharing of information on diabetes.
General Feedback and Concerns
When asked whether they would use the EMPOWER app daily, most participants declined or expressed uncertainty about their ability to do so, citing reasons such as a busy lifestyle and data to be inputted being too repetitive. The participants also raised the concern whether app will be suitable for older patients who may not be technologically savvy. Other concerns included the risk of patient confidentiality being compromised, as well as the lack of HbA1c and lipid panel results in the EMPOWER app.
Despite these concerns, participants stated that they would like their family members and friends, including people with diabetes, those with poor diabetes control, pre-diabetics, and even non-diabetics, to use the app to monitor their blood glucose levels and overall health.
Discussion
In this study, we explored users’ opinions on utilizing the EMPOWER app for diabetes self-management through RPP to improve the design of the app. Adopting a co-design approach enabled insight into users’ perspectives and experiences with the mobile app on diabetes self-management with sufficient depth to understand their concerns. Our study also demonstrated the potential of using app notifications as nudging for patients with T2DM, which may be a useful addition to the scarce literature on digital nudging for T2DM self-management.42 The suggestions and potential solutions derived from this study may be useful for other researchers and app developers working on mHealth tools for chronic disease management. Our findings indicate that using an iterative co-design approach employing qualitative methods allows comprehensively examination of app utility, usability, and acceptability. Similar technique has been employed in other studies.48,49 Although the use of qualitative methods reflects a solid approach to ascertain usability, additional methods need to be considered when refining the app in the future research. For example, analysis of app usage data can provide useful information in terms of engagement with mobile app.50
Our findings reveal that app functionality and usability were important factors affecting the user experience of the mobile app. One consistent concern raised by participants was that effortful manual input of blood glucose, food and medication logs may hamper the use of app, which is also seen in another study.51 Throughout the 3 rounds of RPP sessions, we received feedback and suggestions to improve the mobile app. Due to the time and resource constraint for app development for the next phase of the study,52 we have only incorporated a portion of the suggestions and potential solutions derived from this study based on complexity and needs of the users. Together with other potential behavior change interventions such as health coaching53,54 and motivational interviewing,55,56 the unimplemented suggestions and solutions in this study will be considered during subsequent updates of the mobile app.
Our results highlight that the availability of relevant informative content in the mobile app is in demand and critical, which aligns with findings from other studies.16,38,40,51,57 Furthermore, as people can be exposed to misinformation through the internet, having access to reliable information on diabetes management is especially crucial.16,40,51 However, this study provides valuable insight into the potential negative impact of mHealth on psychological wellbeing. Consistent with other evidence,51 our results showed that the information presented in mobile app can have counterproductive emotional and motivational consequences. For example, users may become demotivated when goals were not met. A potential solution to mitigate negative emotional consequences from mHealth may be through developing a communication platform among the patients for social support.15,40,58–60
Similar to other studies,51,61–64 our findings also highlighted users’ concern on app privacy and the disclosure of personal records. To foster trust and ensure transparency, app developers should provide users with clear private policy outlining the key data practices, how and what kind of data will be collected, handled, and stored.61,65
This study used convenience sampling to recruit participants who were willing to participate in multiple rounds of RPP sessions which may affect the representativeness of the sample. However, even though the sample size was small, the participants varied with respect to age, gender, educational level, and employment status which may support the generalizability of the findings from this study. As some participants had not used the app prior to the sessions or had only used it briefly throughout the duration of data collection, user experience for these participants was limited. During the sessions, the interviewers made a significant effort to guide the participants through the app so that they could provide more detailed feedback on the app.
Conclusion
In this study, we explored users’ opinions on a T2DM self-management mobile app using a co-design approach. Participants provided their perspectives on the usability, functionality, and acceptability of the mobile app together with suggestions for improvement such as the importance of simplifying logging process to enhance users’ sustained engagement. Our study also highlights the value of relevant informative content in mHealth tools for diabetes management. The suggestions and potential solutions derived from this study may be useful for other researchers and app developers working on mHealth tools for chronic disease management. This study adds to the emerging literature on employing a co-design approach to design mHealth technology for T2DM self-management by incorporating user feedback and concerns in the development of mobile apps, and the study design can be adapted when designing mHealth technology for other populations.
Data Sharing Statement
The data used in this study will be made available by the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The SingHealth Centralized Institutional Review Board approved this study (Ref No: 2019/2468). We obtained informed consent from all participants prior to the commencement of the study. The participants’ informed consent included publication of anonymized responses.
Acknowledgment
We wish to thank the participants who contributed to this study.
Funding
This work was supported by the Singapore Ministry of Health’s National Innovation Challenge Grant (Ref: MOH/NIC/CDM1/2018) and Singapore Ministry of Health’s National Medical Research Council under the SingHealth Regional Health System, Population-based, Unified, Learning System for Enhanced and Sustainable (PULSES) Health Centre Grant (NMRC/CG/C027/2017_SHS). Funders were not involved in design, delivery and submission of research.
Disclosure
The authors declare that they have no other competing interests.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. World Health Organization. Diabetes; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes.
4. (Singapore) MOH. National population health survey; 2019. Available from: https://www.moh.gov.sg/resources-statistics/reports/national-population-health-survey-2018-19.
5. Phan TP, Alkema L, Tai ES, et al. Forecasting the burden of type 2 diabetes in Singapore using a demographic epidemiological model of Singapore. BMJ Open Diabetes Res Care. 2014;2(1):e000012. doi:10.1136/bmjdrc-2013-000012
6. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
7. Lin LK, Sun Y, Heng BH, Chew DEK, Chong PN. Medication adherence and glycemic control among newly diagnosed diabetes patients. BMJ Open Diabetes Res Care. 2017;5(1):e000429. doi:10.1136/bmjdrc-2017-000429
8. Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic prescriptions. J Gen Intern Med. 2010;25(4):284–290. doi:10.1007/s11606-010-1253-9
9. Chew SM, Lee JH, Lim SF, Liew MJ, Xu Y, Towle RM. Prevalence and predictors of medication non-adherence among older community-dwelling people with chronic disease in Singapore. J Adv Nurs. 2021;77(10):4069–4080. doi:10.1111/jan.14913
10. Bereda G, Bereda G. The incidence and predictors of poor glycemic control among adults with type 2 diabetes mellitus in ambulatory clinic of Mettu Karl Referral Hospital, southwestern Oromia, Ethiopia: a prospective cross sectional study. Diabetes Updates. 2021;7. doi:10.15761/DU.1000155
11. Nguyen C, Luthra R, Kuti E, Willey VJ. Assessing risk of future cardiovascular events, healthcare resource utilization and costs in patients with type 2 diabetes, prior cardiovascular disease and both. Curr Med Res Opin. 2020;36(12):1927–1938. doi:10.1080/03007995.2020.1832455
12. Li R, Liang N, Bu F, Hesketh T. The effectiveness of self-management of hypertension in adults using mobile health: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2020;8(3):e17776. doi:10.2196/17776
13. Chodosh J, Morton SC, Mojica W, et al. Meta-analysis: chronic disease self-management programs for older adults. Ann Intern Med. 2005;143(6):427–438. doi:10.7326/0003-4819-143-6-200509200-00007
14. Chai S, Yao B, Xu L, et al. The effect of diabetes self-management education on psychological status and blood glucose in newly diagnosed patients with diabetes type 2. Patient Educ Couns. 2018;101(8):1427–1432. doi:10.1016/j.pec.2018.03.020
15. Kabeza CB, Harst L, Schwarz PEH, Timpel P. A qualitative study of users’ experiences after 3 months: the first Rwandan diabetes self-management Smartphone application “Kir’App”. Ther Adv Endocrinol Metab. 2020;11:2042018820914510. doi:10.1177/2042018820914510
16. Jeffrey B, Bagala M, Creighton A, et al. Mobile phone applications and their use in the self-management of type 2 diabetes mellitus: a qualitative study among app users and non-app users. Diabetol Metab Syndr. 2019;11:84. doi:10.1186/s13098-019-0480-4
17. Du Y, Dennis B, Rhodes SL, et al. Technology-assisted self-monitoring of lifestyle behaviors and health indicators in diabetes: qualitative study. JMIR Diabetes. 2020;5(3):e21183. doi:10.2196/21183
18. Huang Z, Tan E, Lum E, Sloot P, Boehm BO, Car J. A smartphone app to improve medication adherence in patients with type 2 diabetes in Asia: feasibility randomized controlled trial. JMIR Mhealth Uhealth. 2019;7(9):e14914. doi:10.2196/14914
19. Morawski K, Ghazinouri R, Krumme A, et al. Association of a smartphone application with medication adherence and blood pressure control: the MedISAFE-BP randomized clinical trial. JAMA Intern Med. 2018;178(6):802–809. doi:10.1001/jamainternmed.2018.0447
20. Amagai S, Pila S, Kaat AJ, Nowinski CJ, Gershon RC. Challenges in participant engagement and retention using mobile health apps: literature review. J Med Internet Res. 2022;24(4):e35120. doi:10.2196/35120
21. Böhm A-K, Jensen ML, Sørensen MR, Stargardt T. Real-world evidence of user engagement with mobile health for diabetes management: longitudinal observational study. JMIR Mhealth Uhealth. 2020;8(11):e22212. doi:10.2196/22212
22. Conway N, Campbell I, Forbes P, Cunningham S, Wake D. mHealth applications for diabetes: user preference and implications for app development. Health Informatics J. 2016;22(4):1111–1120. doi:10.1177/1460458215616265
23. Whitehead L, Seaton P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: a systematic review. J Med Internet Res. 2016;18(5):e97. doi:10.2196/jmir.4883
24. Sánchez de la Guía L, Cazorla Puyuelo M, de-Miguel-Molina B. Terms and meanings of “participation” in product design: from “user involvement” to “co-design”. Design J. 2017;20(sup1):S4539–S4551. doi:10.1080/14606925.2017.1352951
25. Sanz MF, Acha BV, García MF. Co-design for people-centred care digital solutions: a literature review. Int J Integr Care. 2021;21(2). doi:10.5334/ijic.5573
26. Jackson DN, Sehgal N, Baur C. Benefits of mHealth co-design for African American and Hispanic adults: multi-method participatory research for a health information app. JMIR Form Res. 2022;6(3):e26764. doi:10.2196/26764
27. Boyd H, McKernon S, Mullin B, Old A. Improving healthcare through the use of co-design. N Z Med J. 2012;125(1357):76–87.
28. Buller DB, Berwick M, Shane J, Kane I, Lantz K, Buller MK. User-centered development of a smart phone mobile application delivering personalized real-time advice on sun protection. Transl Behav Med. 2013;3(3):326–334. doi:10.1007/s13142-013-0208-1
29. Tay BSJ, Edney SM, Brinkworth GD, et al. Co-design of a digital dietary intervention for adults at risk of type 2 diabetes. BMC Public Health. 2021;21(1):2071. doi:10.1186/s12889-021-12102-y
30. Avila-Garcia P, Nouri S, Cemballi A, Sarkar U, Lyles C, Aguilera A. Engaging users in the design of an mhealth, text message-based intervention to increase physical activity at a safety-net healthcare system. J Gen Intern Med. 2019;34(2):S212.
31. Ogrin R, Viswanathan R, Aylen T, Wallace F, Scott J, Kumar D. Co-design of an evidence-based health education diabetes foot app to prevent serious foot complications: a feasibility study. Pract Diabetes. 2018;35(6):203–209d. doi:10.1002/pdi.2197
32. Garnweidner-Holme LM, Borgen I, Garitano I, Noll J, Lukasse M. Designing and developing a mobile smartphone application for women with gestational diabetes mellitus followed-up at diabetes outpatient clinics in Norway. Healthcare. 2015;3(2):310–323. doi:10.3390/healthcare3020310
33. Vo V, Auroy L, Sarradon-Eck A. Patients’ perceptions of mHealth apps: meta-ethnographic review of qualitative studies. JMIR Mhealth Uhealth. 2019;7(7):e13817. doi:10.2196/13817
34. Liu Y, Heimgärtner R. KEEP fit worldwide: cultural adaptations of the user interface of mobile fitness apps in different language versions.
35. Sivaraman M, Fahmie TA. A systematic review of cultural adaptations in the global application of ABA-based telehealth services. J Appl Behav Anal. 2020;53(4):1838–1855. doi:10.1002/jaba.763
36. Tatara N, Årsand E, Bratteteig T, Hartvigsen G. Usage and perceptions of a mobile self-management application for people with type 2 diabetes: qualitative study of a five-month trial. Stud Health Technol Inform. 2013;192:127–131.
37. Torbjørnsen A, Ribu L, Rønnevig M, Grøttland A, Helseth S. Users’ acceptability of a mobile application for persons with type 2 diabetes: a qualitative study. BMC Health Serv Res. 2019;19(1):641. doi:10.1186/s12913-019-4486-2
38. Baptista S, Wadley G, Bird D, Oldenburg B, Speight J. User experiences with a type 2 diabetes coaching app: qualitative study. JMIR Diabetes. 2020;5(3):e16692. doi:10.2196/16692
39. Lauffenburger JC, Barlev RA, Sears ES, et al. Preferences for mHealth technology and text messaging communication in patients with type 2 diabetes: qualitative interview study. J Med Internet Res. 2021;23(6):e25958. doi:10.2196/25958
40. Jain SR, Sui Y, Ng CH, Chen ZX, Goh LH, Shorey S. Patients’ and healthcare professionals’ perspectives towards technology-assisted diabetes self-management education. A qualitative systematic review. PLoS One. 2020;15(8):e0237647. doi:10.1371/journal.pone.0237647
41. Yoon S, Ng JH, Kwan YH, Low LL. Healthcare professionals’ views of factors influencing diabetes self-management and the utility of a mHealth application and its features to support self-care. Front Endocrinol (Lausanne). 2022;13. doi:10.3389/fendo.2022.793473
42. Kwan Y, Cheng T, Yoon S, et al. A systematic review of nudge theories and strategies used to influence adult health behaviour and outcome in diabetes management. Diabetes Metab. 2020;46(6):450–460. doi:10.1016/j.diabet.2020.04.002
43. Sanders EBN, Stappers PJ. Probes, toolkits and prototypes: three approaches to making in codesigning. CoDesign. 2014;10(1):5–14. doi:10.1080/15710882.2014.888183
44. Chasanidou D, Gasparini AA, Lee E. Design thinking methods and tools for innovation.
45. Kinzie MB, Cohn WF, Julian MF, Knaus WA. A user-centered model for web site design: needs assessment, user interface design, and rapid prototyping. J Am Med Inform Assoc. 2002;9(4):320–330. doi:10.1197/jamia.M0822
46. Michie SA. The Behaviour Change Wheel: A Guide to Designing Interventions. Silverback Publishing; 2014.
47. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
48. Mrklas KJ, Barber T, Campbell-Scherer D, et al. Co-design in the development of a mobile health app for the management of knee osteoarthritis by patients and physicians: qualitative study. JMIR Mhealth Uhealth. 2020;8(7):e17893. doi:10.2196/17893
49. Martin A, Caon M, Adorni F, et al. A mobile phone intervention to improve obesity-related health behaviors of adolescents across Europe: iterative co-design and feasibility study. JMIR mHealth uHealth. 2020;8(3):e14118. doi:10.2196/14118
50. Short CE, DeSmet A, Woods C, et al. Measuring engagement in eHealth and mHealth behavior change interventions: viewpoint of methodologies. J Med Internet Res. 2018;20(11):e9397. doi:10.2196/jmir.9397
51. Dennison L, Morrison L, Conway G, Yardley L. Opportunities and challenges for smartphone applications in supporting health behavior change: qualitative study. J Med Internet Res. 2013;15(4):e86. doi:10.2196/jmir.2583
52. Kwan YH, Yoon S, Tan CS, et al. EMPOWERing patients with diabetes using profiling and targeted feedbacks delivered through smartphone app and wearable (EMPOWER): protocol for a randomized controlled trial on effectiveness and implementation. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.805856
53. Gershkowitz BD, Hillert CJ, Crotty BH. Digital coaching strategies to facilitate behavioral change in type 2 diabetes: a systematic review. J Clin Endocrinol Metab. 2021;106(4):e1513–e1520. doi:10.1210/clinem/dgaa850
54. Obro LF, Heiselberg K, Krogh PG, et al. Combining mHealth and health-coaching for improving self-management in chronic care. A scoping review. Patient Educ Couns. 2021;104(4):680–688. doi:10.1016/j.pec.2020.10.026
55. Nurmi J, Knittle K, Ginchev T, et al. Engaging users in the behavior change process with digitalized motivational interviewing and gamification: development and feasibility testing of the precious app. JMIR mHealth uHealth. 2020;8(1):e12884. doi:10.2196/12884
56. Pedamallu H, Ehrhardt MJ, Maki J, Carcone AI, Hudson MM, Waters EA. Technology-delivered adaptations of motivational interviewing for the prevention and management of chronic diseases: scoping review. J Med Internet Res. 2022;24(8):e35283. doi:10.2196/35283
57. Wiechmann W, Kwan D, Bokarius A, Toohey SL. There’s an app for that? Highlighting the difficulty in finding clinically relevant smartphone applications. West J Emerg Med. 2016;17(2):191–194. doi:10.5811/westjem.2015.12.28781
58. Revenäs Å, Opava CH, Martin C, Demmelmaier I, Keller C, Åsenlöf P. Development of a web-based and mobile app to support physical activity in individuals with rheumatoid arthritis: results from the second step of a co-design process. JMIR Res Protoc. 2015;4(1):e22. doi:10.2196/resprot.3795
59. Mugabirwe B, Flickinger T, Cox L, Ariho P, Dillingham R, Okello S. Acceptability and feasibility of a mobile health application for blood pressure monitoring in rural Uganda. JAMIA Open. 2021;4(3):ooaa068. doi:10.1093/jamiaopen/ooaa068
60. Jessen S, Mirkovic J, Ruland CM. Creating gameful design in mHealth: a participatory co-design approach. JMIR Mhealth Uhealth. 2018;6(12):e11579. doi:10.2196/11579
61. Adhikari R, Richards D, Scott KM. Security and privacy issues related to the use of mobile health apps. 2014.
62. Brandtzaeg PB, Pultier A, Moen GM. Losing control to data-hungry apps: a mixed-methods approach to mobile app privacy. Soc Sci Comput Rev. 2018;37(4):466–488. doi:10.1177/0894439318777706
63. Lupton D. Digital health now and in the future: findings from a participatory design stakeholder workshop. Digit Health. 2017;3:205520761774001. doi:10.1177/2055207617740018
64. Morrissey EC, Casey M, Glynn LG, Walsh JC, Molloy GJ. Smartphone apps for improving medication adherence in hypertension: patients’ perspectives. Patient Prefer Adherence. 2018;12:813–822. doi:10.2147/PPA.S145647
65. Albrecht U-V. Transparency of health-apps for trust and decision making. J Med Internet Res. 2013;15(12):e277–e277. doi:10.2196/jmir.2981
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.