Back to Journals » Clinical Interventions in Aging » Volume 21
A Mixed-Methods Study on Carers’ and Aged-Care Staff’s Perception and Appropriate Utilization of Molded Puree in Older Adults
Authors Fong R ![]() , Kwan CCY, Choi YYY, Leung MHN
, Kwan CCY, Choi YYY, Leung MHN
Received 4 May 2026
Accepted for publication 26 June 2026
Published 10 July 2026 Volume 2026:21 621981
DOI https://doi.org/10.2147/CIA.S621981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Raymond Fong,1,2 Connie CY Kwan,1,2 Yuki YY Choi,1,2 Maggie HN Leung1,2
1Department of Otorhinolaryngology, Head and Neck Surgery, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 2Institute of Human Communicative Research, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China
Correspondence: Raymond Fong, Department of Otorhinolaryngology, Head and Neck Surgery, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China, Tel +85239439602, Email [email protected]
Purpose: While molded puree is marketed as a dignified alternative to traditional texture-modified diets for older adults and patients with dementia, the clinical implications of their rapid commercialization remain under-examined. To investigate the knowledge, clinical expectations, and psychosocial drivers regarding molded puree for older adults among community carers and aged-care professionals.
Participants and Methods: This concurrent mixed-methods study recruited 164 community carers (public cohort) and 60 aged-care professionals (staff cohort) who work in non-governmental residential aged-care networks in Hong Kong SAR. Quantitative data were collected via cross-sectional surveys evaluating self-rated knowledge, swallow safety perceptions, and clinical expectations on consumption of molded puree in older adults. Qualitative data were obtained through semi-structured, in-depth interviews with a purposive sub-sample of 12 community carers to explore underlying behavioral drivers. Quantitative differences were analyzed using Mann–Whitney U and Chi-Square tests, while qualitative data underwent thematic analysis.
Results: Self-rated knowledge about molded puree was significantly lower in the public cohort compared to professional staff (p < 0.001). A puree equivalence fallacy was prevalent; 23.8% of the public believed molded puree shares the exact texture of conventional puree, and 39.3% assumed it requires no chewing. Staff were significantly more aware of biomechanical differences (65.0% disagreed with equivalence). The public held significantly higher expectations regarding improvements in feeding behaviors (50.6% agreement) and nutritional value (26.2%) compared to professionals (p< 0.05). Qualitatively, thematic analysis revealed twohigher-order themes: psychosocial motivations centered on restoringdining dignity and avoiding dietary stigma, and structural hurdlesinvolving procedural ambiguity.
Conclusion: A significant knowledge-perception gap exists between the general public and healthcare professionals. While molded puree offers substantial psychosocial benefits, the prevalence of the puree equivalence fallacy underscores a potential risk for vulnerable older adults. Clinical interventions should prioritize evidence-based swallow safety and standardized screening over aesthetic appeal.
Keywords: dysphagia, aged care, swallow safety, texture-modified diets, caregiver burden
Introduction
Texture modification is one of the commonly adopted compensatory strategies in dysphagia management, a condition highly prevalent among the aging population and those with complex medical conditions.1–3 The modification of food texture could improve the efficiency and safety of swallowing by overcoming the physiological deficits of food processing by individuals.4–6 However, texture-modified diets (TMDs) have a major shortcoming: the texture is often bland and dissimilar to the variety of food textures that patients are used to consuming, which negatively impacts appetite, oral intake amount, perceptions by patients and carers, the mealtime experience and broader quality of life.7–9 This is particularly apparent for textures on the lower end of the International Dysphagia Diet Standardisation Initiative (IDDSI) food spectrum, such as pureed and liquidized food.9,10
Over the past decade, alternative preparation techniques for puree, including molded puree and 3D printed foods, have emerged as a viable option to balance effective compensation for dysphagia with the pleasure of eating.11–13 Driven by their aesthetic appeal, these meals are specifically designed to resemble the appearance of everyday food, offering a visually pleasing alternative that aims to maintain the consumer’s appetite, dignity, and self-esteem during mealtimes.14–16 Consequently, the consumption of molded puree has increased exponentially in some regions, supported by local funding initiatives and heavy commercial promotion.17,18 These entities frequently market molded puree as an ideal supplement or a complete replacement for conventional TMDs.19,20
However, the rapid commercialization of molded puree has predominantly focused on the products themselves, emphasizing favorable and diverse food appearances, ease of purchase, and preparation methods to improve appetite.21–23 This heavy emphasis on aesthetics and practical aspects has neglected the critical clinical questions regarding molded puree indications and contraindications.24,25 Crucially, previous studies indicate that the biomechanical process of swallowing molded puree, despite being classified on the same IDDSI level, is not identical to swallowing conventional puree due to the altered rheological properties caused by hydrocolloids and gelling agents.26,27 Despite this evidence, ambiguity regarding precise safety boundaries, institutional implementation barriers, and strict protocol adherence for modified textures remains a persistent challenge.28,29 For medically vulnerable older adults, operating under unverified assumptions can be lethal; individuals who safely tolerate conventional puree may still be at risk of choking or aspiration pneumonia when consuming molded puree.30
Beyond the immediate safety risks, the overarching clinical benefits of molded puree are often over-emphasized in public discourse.31 Driven by aggressive marketing, carers of older adults may unrealistic expectations, incorrectly assuming that molded puree consumption will yield rapid improvements in feeding behaviors, overall nutritional intake, and short-term weight gain.32–34 Recent research has demonstrated that while reshaped molded puree may offer certain quality-of-life benefits for older adults, specific clinical and nutritional outcomes do not always show significant short-term improvement across all populations.35–38 If carers and professionals operate under these false assumptions, it can dangerously delay the implementation of other necessary clinical interventions and alternative dysphagia management strategies.39,40
There is a need to understand whether there are knowledge gaps and misconceptions surrounding molded puree, and address them to ensure its safe and appropriate utilization in aged care. Building upon this objective, the primary aim of this concurrent mixed-methods study is to evaluate and compare the perceptions of molded puree between the general public and healthcare professionals. Specifically, this study addresses two central research questions: What are the significant quantitative differences in knowledge and perception, clinical expectations, and perceived implementation barriers between community carers of older adults and professional aged-care staff? Qualitatively, what are the underlying psychosocial drivers and theoretical assumptions that shape carers’ perceptions of molded puree.
Methodology
Study Design
This study used a concurrent mixed-methods design,41 with a large-scale survey and structured interviews. This study used a pragmatist research paradigm. The cross-sectional survey compared the knowledge and perceptions of community members of the public and healthcare professionals. The qualitative arm utilized semi-structured, in-depth interviews to deeply explore the conceptualization and emotional drivers of community carers prior to receiving any formal education on texture-modified diets. To support comprehensive and rigorous reporting, the methodology and integration workflows of this study adhere strictly to the Good Reporting Aims for Mixed Methods Research (GRAMMS) framework.42
Participants and Setting
Participants were recruited across a regional territory in Hong Kong SAR, China, targeting two distinct cohorts to evaluate systemic and community-level differences.
Public cohort: A total of 164 community members and carers (N=164) were recruited via informational flyers or electronic messaging through local district health centers and aged care networks to complete the quantitative survey. Eligible participants were adults (>18 years old) currently providing or demonstrating an active interest in TMDs for older adults. From this cohort, a sub-sample of 12 participants (N=12) was selected to participate in the qualitative interviews.
Staff cohort: A total of 60 professional and frontline staff (N=60)—including rehabilitation assistants, healthcare workers, registered nurses, and social workers—were recruited from non-governmental aged care service providers via institutional Email or electronic messaging to complete the professional version of the quantitative survey. Eligible participants were active staff members involved in mealtime care or rehabilitation.
Data Collection Procedures
The survey instruments were designed to assess self-rated baseline knowledge (measured on a 1 to 5-star scale), and 10 questions that evaluated perceptions of swallow safety, texture equivalence, short-term clinical expectations (eg, impact on appetite and feeding behaviors), and perceived barriers to implementation, which are well-documented hurdles in aged care.28 Responses were captured using a categorical Likert-type scale (“Agree”, “Neutral”, “Disagree”, and “Don’t Know”). Additional cohort-specific questions assessed the source of information and access barriers (Public; 10 questions) and professional training needs (Staff; 1 question). The survey was conducted electronically via Microsoft Forms (Microsoft Corporation, Redmond, WA), responses were collected from participants anonymously.
Qualitative semi-structured, one-on-one interviews were conducted by trained final-year Master of Speech-Language Pathology students using a standardized interview guide (Supplementary Information 1). The participants were randomly selected from a pool of participants who expressed willingness to participate (n=20). The interview guide specifically explored five core domains: prior exposure to molded puree, assumptions regarding physical properties (appearance and texture), perceived preparation methods, assumed target populations, and expected holistic impacts across health, financial, psychological, and social dimensions. Interviews took place in private, quiet rooms at community centers. All interviews were audio-recorded and transcribed verbatim.
Data Analysis
Descriptive statistics, including frequencies and valid percentages, were calculated to summarize overall distribution trends and to analyze all questions. For 11 questions that were answered by both cohorts, data were analysed to compare statistical differences between the independent public and staff cohorts. Mann–Whitney U-test was utilized for the ordinal self-rated knowledge. For overlapping Likert-scale questions, a Chi-Square test of independence was employed to compare the distribution of responses across all four categories (Agree, Neutral, Disagree, and Do not Know).43 Cohort-specific questions were analyzed using descriptive statistics. Statistical significance was defined as p < 0.05.
The qualitative interviews were transcribed and analyzed using Braun and Clarke’s44 six-phase framework for thematic analysis to ensure rigorous and transparent data interpretation. A hybrid inductive and deductive coding approach was applied. During the initial phases (familiarization and initial coding), transcripts were analyzed line-by-line to identify preconceived layperson beliefs, cognitive frameworks, clinical misunderstandings, and emotional drivers. Deductive codes targeted known clinical issues (eg, the puree equivalence fallacy), while inductive codes captured organically emerging phenomena (eg, the concept of dining dignity and commercial susceptibility). These codes were systematically reviewed, refined, and collated into overarching definitive themes and sub-themes to contextualize and explain the behavioral drivers behind the quantitative survey data.
To establish qualitative rigor, measures were instituted to ensure data trustworthiness and researcher reflexivity. Qualitative coding and interview interpretations were conducted by investigators (CCYK, YYYC) with backgrounds in speech-language pathology. The investigators also ensured that the layperson narratives were interpreted organically from a consumer standpoint rather than strictly through an institutional lens. Credibility and dependability were supported among investigators and the progression from initial semantic codes to higher-order themes were audited by the first author (RF).
The quantitative survey data and qualitative interview findings were combined at the interpretation and reporting level following a framework of contiguous narrative integration and joint displays.45
Results
Participant Characteristics
The quantitative component of the study included a total of 224 participants, comprising 164 community members/carers (the public cohort) and 60 healthcare and aged-care professionals (the staff cohort, including rehabilitation assistants, social workers, and nurses). Details of the demographics are in Table 1. For the qualitative component, a purposive sub-sample of 12 participants from the public cohort participated in semi-structured, in-depth interviews.
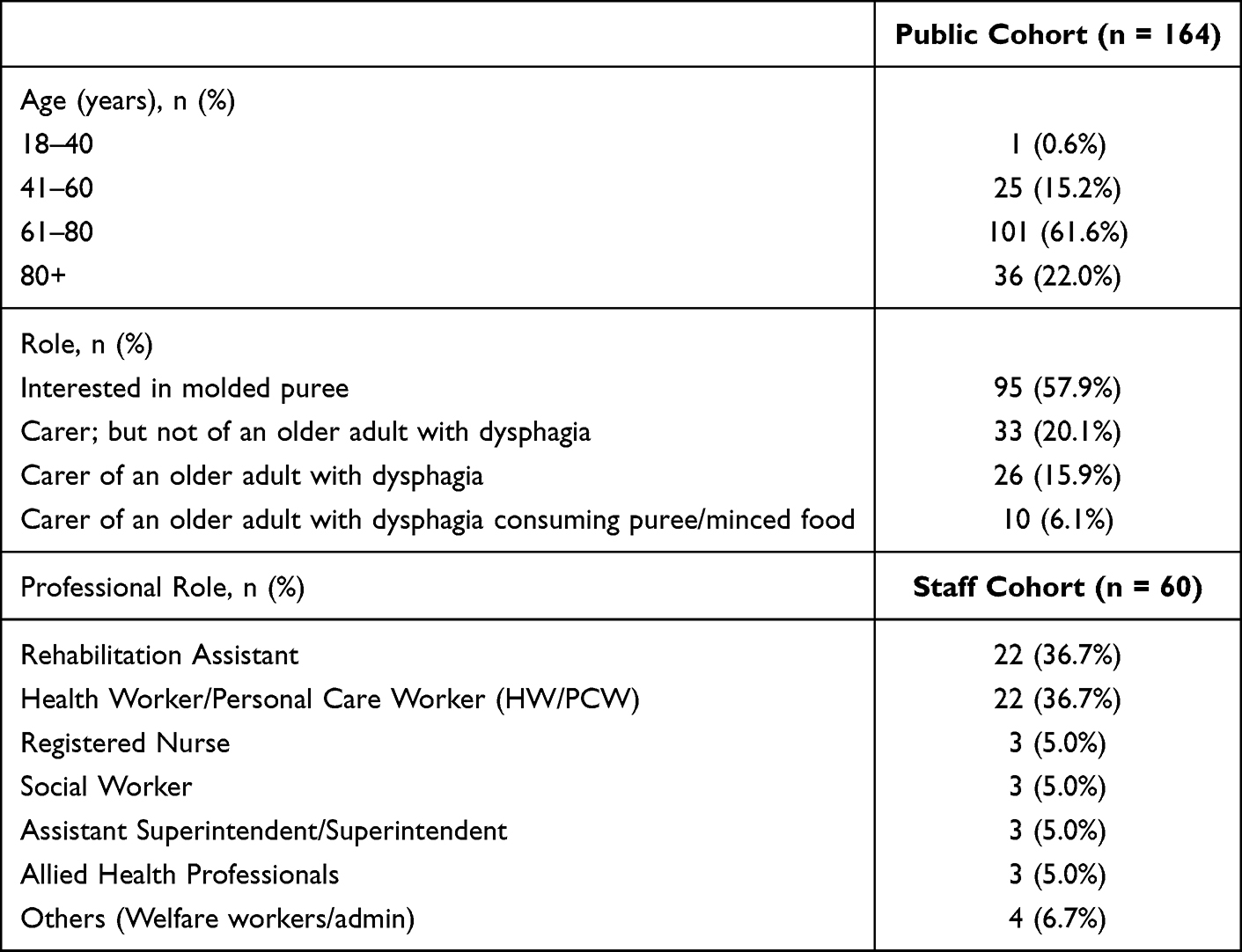 |
Table 1 Participant Demographics and Characteristics |
Quantitative Findings and Comparison Between Two Cohorts
For the self-rating of knowledge about molded puree, the public cohort reported significantly lower rating (Mean = 1.73) compared to professional aged-care staff (Mean = 3.02) (U = 1351.5, p < 0.0001). The results from the 10 questions to both cohorts are detailed in Table 2.
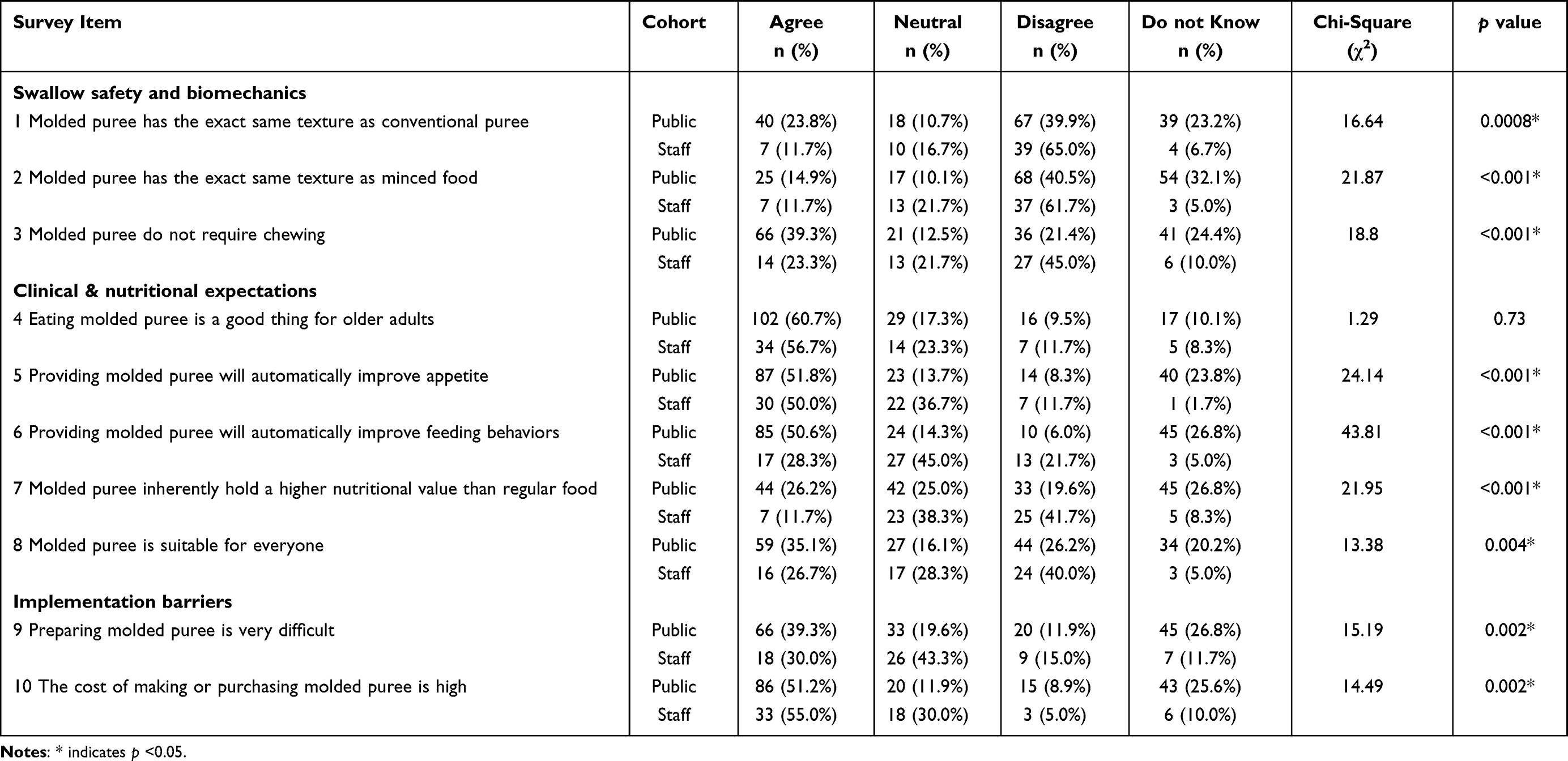 |
Table 2 Comparison of Perceptions, Clinical Expectations, and Implementation Barriers Between Public and Staff Cohorts (10 Questions) |
When asked if molded puree possess the exact same texture as conventional pureed diets, 65.0% of the staff correctly disagreed, compared to only 39.9% of the public (p < 0.05). Conversely, nearly a quarter of the public (23.8%) incorrectly agreed with the statement, and 23.2% selected “Don’t Know”. When asked if molded puree “do not require chewing,” the largest proportion of the public cohort (39.3%) incorrectly assumed they required no chewing, misjudging potential choking hazards associated with hydrocolloid-based reshaping.11,26 In contrast, the staff cohort was significantly more likely to correctly disagree (45.0%) with this assumption (p < 0.05).
For clinical expectations regarding molded puree, the public cohort held significantly different, more optimistic and short-term, clinical expectations compared to the aged-care staff. Over half of the public cohort (50.6%) believed that providing molded puree would automatically improve feeding behaviors. The staff cohort was significantly more conservative, with the majority selecting “Neutral” (45.0%) or “Disagree” (21.7%), and only 28.3% agreeing (p < 0.05). The public assumed that molded puree hold a higher nutritional value than standard regular food (26.2% agreed, 26.8% did not know). Staff members largely rejected this notion, with 41.7% disagreeing that the texture modification itself increases nutritional value (p < 0.05). While 35.1% of the public assumed molded puree is suitable for everyone, staff were significantly more aware of clinical contraindications, with 40.0% disagreeing (p < 0.05).
Community Perceptions of Molded Puree (Public Cohort Only)
Questions asked exclusively to the public cohort (N=164) focused on the factors respondents considered for choosing molded puree and the relevant access barriers. Exactly half of the public respondents (n=84, 50.0%) agreed that “taste is the most important factor” when choosing or purchasing molded puree. Furthermore, while a high percentage agreed the meals look “beautiful” (n=75, 44.6%), a large portion admitted they simply “Don’t Know” if the actual texture is ideal (n=71, 42.3%) or if the taste is excellent (n=70, 41.7%), indicating that initial aesthetic appeal heavily drives their perception. A significant portion of the public perceives access as a major hurdle. Nearly half (n=74, 44.0%) agreed that purchasing molded puree is very difficult, and the vast majority (n=134, 79.8%) reported that they have “Never” purchased them. Similarly, 77.4% (n=130) have “Never” attempted to make them at home.
Professional Training Needs (Staff Cohort Only)
Descriptive data from the staff cohort (N=60) indicated a strong demand for standardized, practical, and clinical training. When asked what they most wanted to understand deeply about molded puree (multi-selection allowed), the most frequently selected priority was “Preparation processes/procedures” (n=44, 73.3%). This was closely followed by advanced clinical applications, specifically: “How to screen and select suitable candidates for consumption” (n=43, 71.7%), “Effects and benefits” (n=37, 61.7%), “Precautions and contraindications” (n=36, 60.0%), and the “Underlying biomechanical principles” (n=33, 55.0%).
Qualitative Findings: Carer Understanding and Perceptions
The qualitative sub-sample was predominantly composed of participants aged 41–60 (n=10, 83.3%), while the remaining participants belonged to the 61–80 age bracket (n=2, 16.7%). In terms of caregiving status, 2 were caring for a person with dysphagia requiring minced/pureed food, 3 were carers of persons with dysphagia and 7 were persons interested in molded puree. The mean duration of interview was 16 minutes. A thematic analysis of the 12 transcripts was conducted to capture the baseline perceptions, knowledge gaps, and clinical expectations regarding molded puree. To enhance analytical clarity, the initial thematic codes were synthesized and grouped into two distinct higher-order themes reflecting (1) psychosocial and aesthetic motivations for adoption, and (2) structural and procedural implementation hurdles. The complete hierarchical coding architecture and corresponding transcript code origins are illustrated in Table 3.
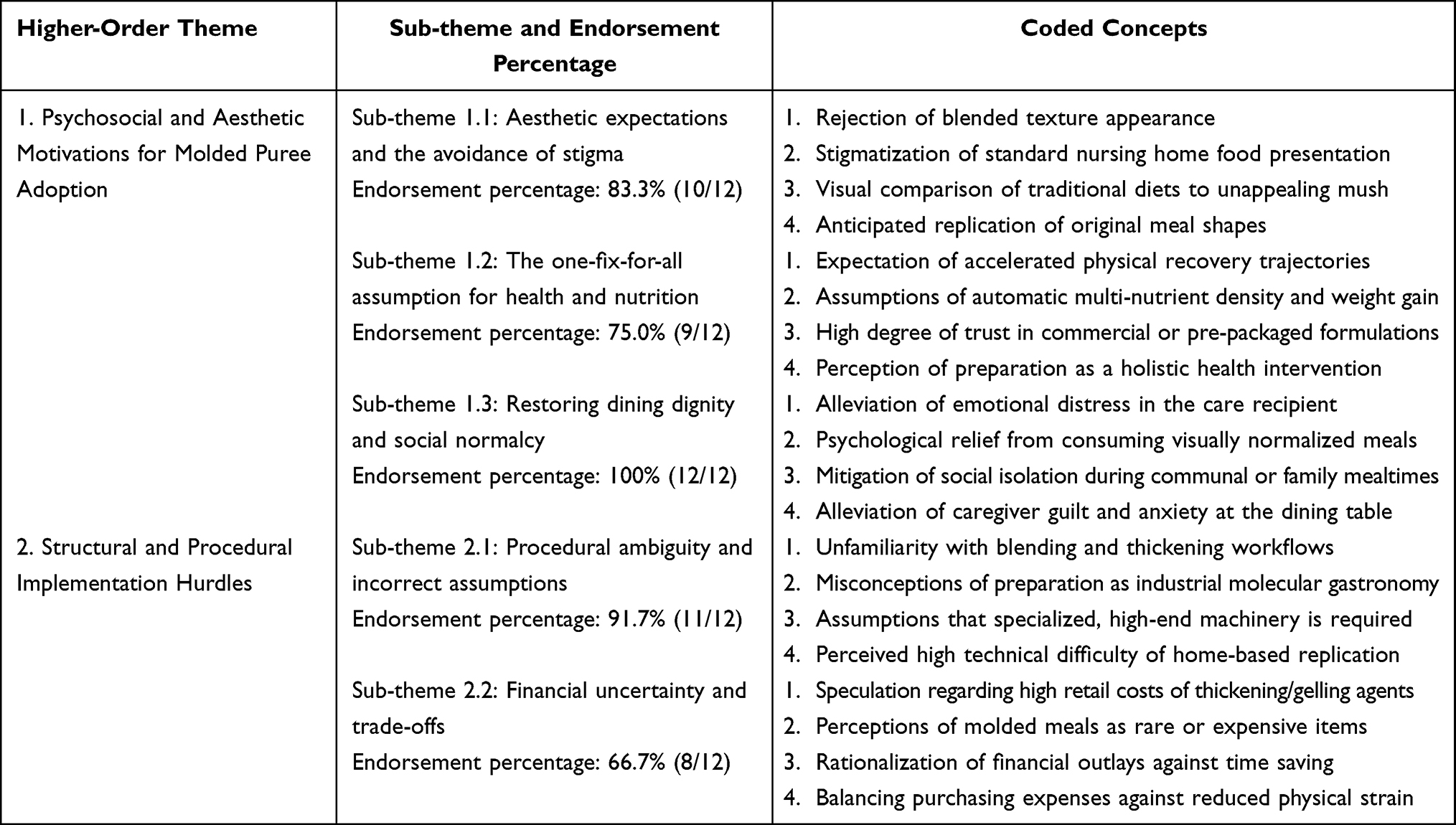 |
Table 3 Qualitative Coding Tree and Coding Frequencies |
Theme 1: Psychosocial and Aesthetic Motivations for Adoption
The higher-order theme included sub-themes of aesthetic expectations, the one-fix-for-all assumption and restoring dining dignity.
Sub-Theme 1.1: Aesthetic Expectations and the Avoidance of Stigma
While practical experience with molded puree was low, participants possessed strong preconceived views about their appearance. The primary driver for embracing molded puree was an aversion to traditional pureed diets. Participants expected molded puree to perfectly replicate the original food to spare patients from visually unappealing meals.
I think the appearance is close to what we usually eat. It doesn’t look like the mashed-up stuff in nursing homes that looks like vomit when they bring it out. (Participant1)
They will feel more respected, meaning they don’t have to eat disgusting mush. (Participant 3)
Sub-Theme 1.2: The One-Fix-for-All Assumption for Health and Nutrition
At baseline, participants held highly optimistic, generalized clinical expectations for molded puree. Because they believed the meals looked better, they automatically assumed this would translate to comprehensive nutritional healing and rapid recovery, viewing the meals as a panacea rather than a specific tool for swallow safety.
In terms of health... it can supplement multi-dimensional nutrients... for example, they won’t just be eating congee and only getting carbohydrates. (Participant 3)
They can absorb more nutrition, and they will recover faster, prolonging their life expectancy. (Participant 10)
Furthermore, some participants exhibited a trust in the commercial or institutional provision of these meals, assuming they are inherently safe and balanced without needing individualized screening:
Because molded puree is usually designed by dietitians... every meal is guaranteed to be nutritious. (Participant 2)
Sub-Theme 1.3: Restoring Dining Dignity and Social Normalcy
The psychological and social benefits of molded puree were the most intensely discussed topics. Participants believed that the aesthetic improvement of the food directly correlates to restored self-esteem, reduced depressive symptoms, and the facilitation of social integration. Carers highlighted the immense psychological burden of eating differently from others, and saw molded puree as the ultimate equalizer.14,16,46
Psychologically, they would feel relieved, like there is a solution to the health problem they are facing, so they won’t feel so different from everyone else. (Participant 4)
From a social angle, it won’t look so abrupt [when eating together at a table], like having to bring out a completely separate dish. (Participant 1)
Theme 2: Structural and Procedural Hurdles in Implementation
This higher-order theme included sub-themes of the structural limitations facing caregivers, specifically procedural ambiguity and financial uncertainty.
Sub-Theme 2.1: Procedural Ambiguity and Incorrect Assumptions
When asked how molded puree is prepared, the data revealed a profound knowledge gap. The lack of standardized education led to high procedural ambiguity. Several participants frankly admitted ignorance (“I really don’t know”, Participant 1; “I don’t know this one”, Participant 5). Those who attempted to guess conceptualized the process as highly complex, industrial, or akin to high-end culinary techniques, which contributed to the perception that they are difficult to make at home.
Is it like molecular gastronomy? Mincing it up and changing it back to look about the same. (Participant 11)
I guess maybe there are special machines, maybe compressing the food, or using a blender... or liquidifying the food. (Participant 4)
Sub-Theme 2.2: Financial Uncertainty and Trade-Offs
Perceptions regarding the financial impact of molded puree were highly speculative and mixed. Because participants lacked concrete knowledge of the preparation process or commercial availability, they struggled to estimate costs. Many assumed the meals would be expensive due to the perceived complexity of production.
Financially, I guess because molded puree isn’t very common yet. the cost of buying or making them is relatively more expensive. (Participant 8)
However, several participants rationalized these unknown costs by framing them as trade-offs against the broader burdens of caregiving, assuming that buying molded puree would ultimately save time or reduce overall caregiving expenses.
Caregiving might become a bit easier, so maybe the cost of hiring a caregiver would be lower... but buying the meals still costs money. (Participant 10)
In summary, the quantitative data demonstrated a knowledge-perception discrepancy, characterized by community misconceptions regarding texture equivalence and optimistic clinical outcomes. Concurrently, the qualitative findings showed the underlying emotional and psychosocial mechanisms driving this gap, namely an emphasis on dining dignity over safety. Together, these convergent data series highlight a need for evidence-based interventions, a concept explored in depth in the following section.
Discussion
This mixed-methods study successfully compared the baseline knowledge, expectations, and behavioral drivers regarding molded purees between community carers and healthcare professionals. The findings reveal a knowledge-perception gap, where the general public demonstrates a high susceptibility to the aesthetic appeal of molded puree while simultaneously downplaying critical swallow biomechanics. Crucially, our integrated data indicate that the profound caregiver desire to alleviate mealtime distress and restore dining dignity frequently eclipses evidence-based safety considerations.17,18
Regarding swallowing safety, the prevalence of the puree equivalence fallacy among the public is alarming.28 A significant proportion of community respondents incorrectly believed that molded puree share the exact texture as conventional puree and require no chewing. Qualitative data further revealed that carers conceptualized molded puree purely as a visual upgrade, completely devoid of biomechanical implications.31 This assumption is clinically hazardous.30 Recent endoscopic research demonstrates that molded puree, due to the hydrocolloids and gelling agents used in their reconstruction, require significantly more masticatory cycles, exhibit a longer swallow reaction time, and involve a more inferior site of swallow initiation compared to traditional puree.27 Similarly, the rheological properties of molded items differ heavily based on the specific binders used, uniquely altering bolus formation.11,26 Consequently, older adults who can safely tolerate a conventional puree may be at a heightened risk of aspiration or choking when consuming molded puree if adequate clinical screening is bypassed.2,30 The fact that professional staff were significantly more aware of these risks underscores the urgent need to redirect public discourse away from mere aesthetics and toward strict swallow safety.29
Our quantitative and qualitative data consistently demonstrated that community carers hold overly optimistic clinical expectations for molded puree.34 Driven by the assumption that transitioning to visually appealing molded puree would automatically ensure comprehensive nutritional healing, weight gain, and rapid recovery. However, the scientific literature paints a more nuanced picture.9 While molded puree can undoubtedly improve short-term feeding behaviors and intake volume, particularly in older adults with dementia, texture modification alone does not inherently increase nutritional density.33,36 In fact, systematic reviews highlight that consumers of texture-modified diets frequently exhibit compromised nutritional status and continued weight loss.9 For molded puree to actively reverse malnutrition or induce weight gain, the meals must be systematically fortified or enriched alongside reshaping.35 The public’s blind trust in the intrinsic health benefits of molded puree threatens to delay other necessary interventions, such as tailored dietetic support or oral motor rehabilitation.39,40
Despite these clinical misconceptions, the qualitative findings validate the psychosocial imperative behind molded puree.23 Carers expressed a profound aversion to traditional puree, stigmatizing them as vomit-like and acknowledging the severe psychological toll eating food in such form takes on patients.16,31 By perfectly replicating the appearance of everyday food, molded puree actively restore dining dignity, reduce depressive symptoms, and facilitate social normalcy.14,15 Importantly, this aesthetic upgrade serves a dual purpose: it not only elevates the patient’s quality of life but significantly alleviates the psychological distress, guilt, and mealtime anxiety experienced by the caregiver.32,34,46 Acknowledging this emotional driver is crucial; clinicians must not dismiss the aesthetic value of molded puree but rather leverage it to encourage dietary compliance, provided it is done safely.20,33
The study also highlights severe procedural ambiguity among the public, with many carers assuming molded puree preparation is akin to molecular gastronomy.25 This perceived complexity drives the belief that molded puree is expensive and too difficult to implement at home, creating an over-reliance on commercial providers.8,47 Conversely, the professional cohort identified a pressing need for standardized clinical training, specifically regarding how to systematically screen and select suitable candidates for these meals.24 This points to a systemic gap: while the market aggressively promotes the product, there is a distinct lack of accessible, evidence-based screening protocols for frontline staff and clear, demystified preparation guidelines for home carers.25,28
Strengths and Limitations
A key strength of this study is its concurrent mixed-methods design, which allowed for the objective quantification of clinical misconceptions while utilizing qualitative thematic analysis to uncover the profound emotional drivers behind caregiver behaviors.44 However, the study is not without limitations. The reliance on self-reported survey data may introduce response bias, and voluntary recruitment patterns mean that self-selection bias could influence both survey and interview participation rates. Also, the detailed demographical data of the public and staff cohorts were not collected. If further details such as educational background and years of experience as a staff/carer were collected, further subgroup analysis would be possible. Furthermore, because data collection was geographically bounded within urban healthcare settings in Hong Kong, the transferability and generalizability of these findings to rural regions or distinct cultural dietary models require further validation. Additionally, future studies could longitudinally evaluate whether addressing misconceptions revealed in this study could be changed via public education that translates into sustained, safe practices at home.36
Conclusion
Molded puree represent a vital advancement in aged care, offering unparalleled benefits for older adults’ dignity and carer well-being.14,23 However, their aesthetic success has overshadowed their clinical complexity.27 To prevent adverse events such as choking or insidious malnutrition, the aged-care sector must urgently bridge the knowledge gap.9,30 Stakeholders, including speech-language pathologists, dietitians, and commercial providers, must collaborate to establish rigorous screening protocols aligned with international standards and shift the public narrative.10 Molded puree is not a one-off or one-fix-for-all solution, as highlighted by the significant portion of the public who incorrectly assumed universal suitability versus the professional cohort who recognized clinical contraindications. Consequently, this preparation technique remains a highly specialized clinical tool that requires individualized, mandatory screening checklists formally integrated into aged-care operational guidelines to ensure dining dignity never compromises physiological safety.36
Data Sharing Statement
The data is available upon reasonable request to the corresponding author.
Acknowledgment
The authors would like to acknowledge the contribution by colleagues from the Methodist Center, Tung Wah Group of Hospitals and the Jockey Club Cadenza Hub.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported by the Knowledge Transfer Project Fund (KPF 2023/24) of The Chinese University of Hong Kong (Ref: PF24GWP07).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Doan TN, Ho WC, Wang LH, Chang FC, Nhu NT, Chou LW. Prevalence and methods for assessment of oropharyngeal dysphagia in older adults: a systematic review and meta-analysis. J Clin Med. 2022;11(9):2605. doi:10.3390/jcm11092605
2. Madhavan A, LaGorio LA, Crary MA, Dahl WJ, Carnaby GD. Prevalence of and risk factors for dysphagia in the community dwelling elderly: a systematic review. J Nutr Health Aging. 2016;20(8):806–12. doi:10.1007/s12603-016-0712-3
3. Rivelsrud MC, Hartelius L, Bergstrom L, Lovstad M, Speyer R. Prevalence of oropharyngeal dysphagia in adults in different healthcare settings: a systematic review and meta-analyses. Dysphagia. 2023;38(1):78–93. doi:10.1007/s00455-022-10465-x
4. Cha S, Kim WS, Kim KW, et al. Sarcopenia is an independent risk factor for dysphagia in community-dwelling older adults. Dysphagia. 2019;34(5):692–697. doi:10.1007/s00455-018-09973-6
5. Sukkar SG, Maggi N, Travalca Cupillo B, Ruggiero C. Optimizing texture modified foods for oro-pharyngeal dysphagia: a difficult but possible target? Front Nutr. 2018;5:68. doi:10.3389/fnut.2018.00068
6. Steele CM, Alsanei WA, Ayanikalath S, et al. The influence of food texture and liquid consistency modification on swallowing physiology and function: a systematic review. Dysphagia. 2015;30(1):2–26. doi:10.1007/s00455-014-9578-x
7. Blaise M. Mealtime experiences of hospitalized older patients requiring a puree consistency diet [Master’s thesis]. McGill University; 2010. https://dam-oclc.bac-lac.gc.ca/download?is_thesis=1&oclc_number=1147917394&id=2f9a2adb-4bb2-453f-bcfa-84dd55630779&fileName=Blaise_Magdalena_2009_these.pdf.
8. Ilhamto N, Anciado K, Keller HH, Duizer LM. In-house pureed food production in long-term care: perspectives of dietary staff and implications for improvement. J Nutr Gerontol Geriatr. 2014;33(3):210–228. doi:10.1080/21551197.2014.927306
9. Wu XS, Miles A, Braakhuis AJ. Texture-modified diets, nutritional status and mealtime satisfaction: a systematic review. Healthcare. 2021;9(6):624. doi:10.3390/healthcare9060624
10. Cichero JA, Lam P, Steele CM, et al. Development of International Terminology and Definitions for Texture-Modified Foods and thickened fluids used in dysphagia management: the IDDSI Framework. Dysphagia. 2017;32(2):293–314. doi:10.1007/s00455-016-9758-y
11. Dick A, Bhandari B, Dong X, Prakash S. Feasibility study of hydrocolloid incorporated 3D printed pork as dysphagia food. Food Hydrocoll. 2020;107:105940. doi:10.1016/j.foodhyd.2020.105940
12. Lorenz T, Iskandar MM, Baeghbali V, Ngadi MO, Kubow S. 3D food printing applications related to dysphagia: a narrative review. Foods. 2022;11(12):1789. doi:10.3390/foods11121789
13. Smith R, Bryant L, Hemsley B. Allied health professionals’ views on the use of 3D food printing to improve the mealtime quality of life for people with dysphagia: impact, cost, practicality, and potential. Am J Speech Lang Pathol. 2022;31(4):1868–1877. doi:10.1044/2022_AJSLP-21-00391
14. Cassens D, Johnson E, Keelan S. Enhancing taste, texture, appearance, and presentation of pureed food improved resident quality of life and weight status. Nutr Rev. 1996;54(1):S51–S54. doi:10.1111/j.1753-4887.1996.tb03790.x
15. Lam CJY, Phua QQ, Guo EY, Sia IKM. Impact of a moulded pureed diet on taste, appearance, recognisability, and overall liking among patients in an acute hospital. Front Nutr. 2023;10:1248779. doi:10.3389/fnut.2023.1248779
16. Smith R, Bryant L, Hemsley B. Perspectives of people with dysphagia and their supporters on the potential for 3D food printing to improve mealtime-related quality of life. Disabil Rehabil. 2024;19(3):1032–1040. doi:10.1080/17483107.2022.2142681
17. Keller HH, Chambers LW, Fergusson DA, et al. A mix of bulk and ready-to-use modified-texture food: impact on older adults requiring dysphagic food. Can J Aging. 2012;31(3):335–348. doi:10.1017/S0714980812000268
18. Raheem D, Carrascosa C, Ramos F, Saraiva A, Raposo A. Texture-modified food for dysphagic patients: a comprehensive review. Int J Environ Res Public Health. 2021;18(10):5125. doi:10.3390/ijerph18105125
19. Honnens de Lichtenberg Broge E, Wendin K, Bredie WL. Adapting dysphagia meals for acceptance among a broader group of older adults. J Sens Stud. 2024;39(1):e12894. doi:10.1111/joss.12894
20. Okkels SL, Saxosen M, Bügel S, Olsen A, Klausen T, Beck A. Acceptance of texture-modified in-between-meals among old adults with dysphagia. Clin Nutr ESPEN. 2018;25:126–132. doi:10.1016/j.clnesp.2018.03.119
21. Makame J, Nolden AA, Emmambux MN. Texture properties of foods targeted for individuals with limited oral processing capabilities: the elderly, dysphagia, and head and neck cancer patients. Food Funct. 2023;14(9):3949–3965. doi:10.1039/D3FO00363A
22. Miles A, Dennison K, Oad MA, Shasha L, Royal M. Consumer satisfaction of texture modified meals served in residential aged-care facilities. Int J Food Sci Nutr Res. 2019;1(1):1005.
23. Smith R, Bryant L, Reddacliff C, Hemsley B. A review of the impact of food design on the mealtimes of people with swallowing disability who require texture-modified food. Int J Food Design. 2022;7(1):7–28. doi:10.1386/ijfd_00034_1
24. Painter V, Le Couteur DG, Waite LM. Texture-modified food and fluids in dementia and residential aged care facilities. Clin Interv Aging. 2017;12:1193–1203. doi:10.2147/CIA.S140581
25. Giura L, Urtasun L, Belarra A, Ansorena D, Astiasaran I. Exploring tools for designing dysphagia-friendly foods: a review. Foods. 2021;10(6):1334. doi:10.3390/foods10061334
26. Strother H, Moss R, McSweeney MB. Comparison of 3D printed and molded carrots produced with gelatin, guar gum and xanthan gum. J Texture Stud. 2020;51(6):852–860. doi:10.1111/jtxs.12545
27. Wong MKL, Ku PKM, Tong MCF, Lee KYS, Fong R. Endoscopic and observational findings of swallowing of traditional and molded puree in healthy individuals. Dysphagia. 2023;38(5):1363–1370. doi:10.1007/s00455-023-10565-2
28. Hill C, Clapham RP, Buccheri A, Field M, Wong Shee A, Alston L. Assessing adherence and exploring barriers to provision of prescribed texture modifications for dysphagia in a residential aged care facility in rural Australia. Int J Speech Lang Pathol. 2022;24(1):67–76. doi:10.1080/17549507.2021.1953144
29. Holteng LBA, Frøiland CT, Corbett A, Testad I. Care staff perspective on use of texture modified food in care home residents with dysphagia and dementia. Ann Palliat Med. 2017;6(4):310–318.
30. Kyodo R, Kudo T, Horiuchi A, Sakamoto T, Shimizu T. Pureed diets containing a gelling agent to reduce the risk of aspiration in elderly patients with moderate to severe dysphagia: a randomized, crossover trial. Medicine. 2020;99(31):e21165. doi:10.1097/MD.0000000000021165
31. Smith R, Bryant L, Hemsley B. ‘It looks better than a bowl of mush’: views on the use of food design strategies, including 3D food printing, to improve meals for people with dysphagia. Int J Food Design. 2024;9(2):177–199. doi:10.1386/ijfd_00071_1
32. Lisiecka D, Kelly H, Jackson J. ‘This is your golden time. You enjoy it and you’ve plenty time for crying after’: how dysphagia impacts family caregivers of people with amyotrophic lateral sclerosis–A qualitative study. Palliat Med. 2020;34(8):1097–1107. doi:10.1177/0269216320932754
33. Liu W, Lee K, Suh H, Li J. Optimizing mealtime care and outcomes for people with dementia and their caregivers: a systematic review and meta-analysis of intervention studies. Alzheimers Dement. 2025;21(3):e14522. doi:10.1002/alz.14522
34. Yau KH, Mo KY-H. Navigating caregiver challenges: exploring attitudes, usage and stress in elderly texture-modified food practices in Hong Kong. Hong Kong J Social Work. 2026;1–18.
35. Germain I, Dufresne T, Gray-Donald K. A novel dysphagia diet improves the nutrient intake of institutionalized elders. J Am Diet Assoc. 2006;106(10):1614–1623. doi:10.1016/j.jada.2006.07.008
36. Lai JFC, Ng RWY, Kwan CCY, Tong MCF, Lee KYS, Fong R. A Quasi-Experimental Study on feeding behaviors and related outcomes by provision of molded puree in aged-care facilities. Folia Phoniatr Logop. 2025;1–10. doi:10.1159/000548799
37. Ott A, Senger M, Lötzbeyer T, Gefeller O, Sieber CC, Volkert D. Effects of a texture-modified, enriched, and reshaped diet on dietary intake and body weight of nursing home residents with chewing and/or swallowing problems: an enable study. J Nutr Gerontol Geriatr. 2019;38(4):361–376. doi:10.1080/21551197.2019.1628158
38. Torrence SE. Pureed Diets in a Long-Term Care Setting: Does Use of Pre-Shaped Pureed Foods Increase Consumption? Northern Illinois University; 2011.
39. Giles H, Zannidi D, Clegg ME, et al. A systematic review of the factors affecting textural perception by older adults and their association with food choice and intake. Appetite. 2025;214:108202. doi:10.1016/j.appet.2025.108202
40. Stockdell R, Amella EJ. The Edinburgh feeding evaluation in dementia scale: determining how much help people with dementia need at mealtime. Am J Nurs. 2008;108(8):46–54;quiz55. doi:10.1097/01.NAJ.0000327831.51782.8e
41. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
42. O’Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy. 2008;13(2):92–98. doi:10.1258/jhsrp.2007.007074
43. McHugh ML. The chi-square test of Independence. Biochem Med. 2013;23(2):143–149. doi:10.11613/bm.2013.018
44. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
45. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–2156. doi:10.1111/1475-6773.12117
46. Namasivayam-MacDonald AM, Shune SE. The burden of dysphagia on family caregivers of the elderly: a systematic review. Geriatrics. 2018;3(2):30. doi:10.3390/geriatrics3020030
47. Wu XS, Miles A, Braakhuis A. An evaluation of texture-modified diets compliant with the International Dysphagia Diet standardization initiative in aged-care facilities using the consolidated framework for implementation research. Dysphagia. 2022;37(5):1314–1325. doi:10.1007/s00455-021-10393-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.