Back to Journals » Patient Preference and Adherence » Volume 17
A Mixed Methods Assessment of Self- Management Needs and Preferences of People with Type 2 Diabetes Mellitus in China
Authors Hu L, Jin X, Li Y, Yang D ![]() , Zhang Z
, Zhang Z ![]() , He X, Chen W, Gong N
, He X, Chen W, Gong N
Received 19 October 2022
Accepted for publication 25 February 2023
Published 13 March 2023 Volume 2023:17 Pages 653—666
DOI https://doi.org/10.2147/PPA.S394003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Lei Hu,1,* Xiaoyuan Jin,2,* Yundong Li,3 Dan Yang,1 Ziqing Zhang,1 Xiaoyu He,1 Weiju Chen,1 Ni Gong1
1School of Nursing, Jinan University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Social Medicine of School of Public Health, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 3School of Ethnology and Sociology, Yunnan University, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ni Gong; Weiju Chen, School of Nursing, Jinan University, No. 601 West Huangpu Avenue, Tianhe District, Guangzhou, Guangdong, People’s Republic of China, Tel +86 15013217344;+86 18688898425, Email [email protected]; [email protected]
Background: Consistent and effective self-management is a major challenge for people with diabetes and long-term effects can be difficult to sustain despite the many interventions. Interventions often fail to take patients’ perceptions of self-management into account from their perspective. Exploring the needs preferences and the influencing factors of self-management in patients can improve the effectiveness of self-management.
Methods: This study used a mixed research approach, exploring patient needs and preferences through web crawl methods and using qualitative interviews to explore the logic of preferences. 1605 data were obtained from 4 online health communities through web crawlers. Data were coded using grounded theory to analyze self-management needs. The codes were also coded for frequency statistics and ranked to explain the self-management preferences. The second phase explained the logic of the ranked distribution of preferences through one-on-one interviews with 22 patients.
Results: This study summarized six self-management needs of people with diabetes through web crawler data, among which medication management and conflict between disease and daily life were the most important concerns of patients. The reasons why patients are particularly concerned about these two needs were explored through qualitative interviews, and it was found that patients’ concerns about medication were mainly due to the following three aspects: the effect of drugs is direct and obvious, medication use makes life less complicated, and progressive side effects. The patients’ concerns about the conflict between disease and daily life are often caused by the following three aspects: diabetes impacts social roles, disease complicates life, and reducing the impact of the disease on life.
Conclusion: The self-management needs of Chinese diabetics have six themes. Medication management, conflict between disease and daily life, diet, diabetes knowledge, blood glucose monitoring and exerciseIn order of frequency of mention and possible preference: medication management, conflict between disease and daily life were the most frequent needs, while diet, knowledge about diabetes, blood glucose monitoring and exercise were their least frequent needs.Understanding the individual’s perception and understanding of diabetes self-management and the expression of the patient’s daily life situations can guide the medical team to optimize collaboration on personalized care plans.
Keywords: type 2 diabetes, self-management, needs, preferences, person-centered care, patients’ experience
Introduction
Diabetes mellitus is a chronic disease with a high prevalence and high disability rate,1 requiring intensive, ongoing self-management2 to prevent irreversible negative health outcomes.3 Self-management of diabetes is strongly related to the quality of life.4 There is solid evidence that effective self-management of diabetes can lead to optimal blood glucose levels, improved psychosocial functioning and quality of life.5 Diabetes self-management behaviors involve engaging in recommended behavioral activities such as healthy diets, medication adherence, being proactive, monitoring, risk reduction, problem solving, and healthy coping, all of which are necessary to successfully manage the disease.6 However, consistent and effective self-management remains a great challenge for patients.7,8 More than half of people with diabetes cannot control their diet; fewer than 70% of patients take medication on time and participate in physical exercise,9 and 59.2% report that they occasionally, rarely, or never self-monitor their blood glucose.10 One out of every four patients has low compliance with diabetes management.11 As a result, many approaches have been tried in various countries to address the problems of low self-management, low adherence to treatment, and poor glycemic management. The Chinese government has focused on diabetes management through screening and healthy lifestyle promotion. However, little progress has been achieved to date.12 A nationally representative cross-sectional study by JAMA found that among Chinese adults with diabetes, 36.7% reported awareness of their condition, and 32.9% were receiving treatment. However, only 50.1% of those receiving treatment were fully controlled.13 Overall, the level of diabetes self-management in China remains at moderate and low levels.14
Studies have mainly focused on approaches to intervention and evaluation of intervention effects. Diabetes self-management education (DSME) is an established approach that constitutes a vital component of the complete treatment of diabetes.15 In DSME, a professional team supports decision making and implementation of interventions that can actively change diabetes-specific knowledge and lifestyles, and help patients overcome treatment inertia.16,17 Such interventions have been effective in improving psychosocial and clinical outcomes, increasing self-efficacy and quality of life, and reducing the risk of cardiovascular events.18–20 Empirical evidence shows that patients can control blood sugar, blood pressure, and lipids, and improve social support in the short term after self-management interventions, but long-term effects are not sustained.21,22 The initial effects of intervention gradually weaken over time, and patients do not achieve effective long-term management. Patients lie at the heart of self-management. Thus, to achieve effective disease management, we need to start by meeting the needs of individuals and understanding critical aspects of self-management from a patient perspective.
Interventions proposed in current research are based on assumptions about rational and typical human beings, often removed from their real life situations and assuming they will make optimal health choices. However, once removed from the guidance and support of intervention programs, patients often return to their original levels of self-management. Secondly, although many previous studies have focused on patients’ self-management barriers, they have mostly focused on physician-patient communication, patients’ perceptions of disease management, and the social environment.23–25 The analytical logic of previous studies on patient self-management has mostly ignored the compatibility between the ponderous and rational knowledge of illness and daily life, and the possible hindrance to management caused by desires, and trivial daily life. Thus, it is evident that research that collects extensive patient data from the real world and delves into the link between patient self-management and daily life, as well as its causes, is relatively limited. Therefore, this study is dedicated to fill this gap.
This study will use a mixed research approach to explore patients’ needs, preferences, and their underlying reasons by reducing them to life situations. Firstly, the self-management needs and preferences of people with diabetes were explored and described from the real-life situations of patients’ diabetic disease and treatment journeys through a web crawler approach. The deeper reasons for the existence of these needs and preferences of patients were then further explored through qualitative interviews.
Methods
Study Design
There is individual variability in patients’ needs and the particular demands of their daily lives. Therefore, we used a web crawler method to crawl the text contents of diabetes patients’ health consultations to doctors in online health communities, and extensively collect patients’ questions and needs arising from their daily management of diabetes. In addition, a qualitative interview method was used to conduct face-to-face interviews with patients to further understand and explore the underlying reasons for patients’ self-management needs and preferences.
The mixed methods approach included a web crawling method and qualitative interviews. The first stage involved the collection of web crawler data to categorize the needs of people with diabetes by coding the text, then the codes were subjected to frequency counts, and the patient needs were ranked according to the resulting weights to derive the patient’s self-management preferences. The subsequent phase involved qualitative interviews, building on the results of the previous web crawl to explain why the results occurred and to explore in more detail the underlying reasons for diabetes demand preferences.
Web Crawler
A Web crawler, sometimes called a spider or spiderbot and often shortened to crawler, are created to automatically extract relevant data in bulk from the vast amount of data on the Internet. It is now widely used in areas such as search engines, large-scale data mining and analysis, artificial intelligence and machine learning dataset production.26
The web crawler survey obtained 2305 crawler data from four online health communities from March 2020 to July 2020, with 1605 valid filtered items. Patients with diabetes browse the websites on the online health communities for information about doctors and then select doctors for medical consultations to obtain health information about the disease and treatment. A total of four web platforms (referred to as A, W, C, and D) were selected for this study (Appendix 1) based on multiple authorized rankings (2020 China Internet Healthcare Annual Analysis Report (updated December 25, 2020); Internet Healthcare Industry Report). The data crawled by the web crawler is in the form of a question and answer between a diabetic patient and a doctor about the word “diabetes”. The following is a example of the data crawled (Figure 1).In addition, all participants’ information is anonymized.
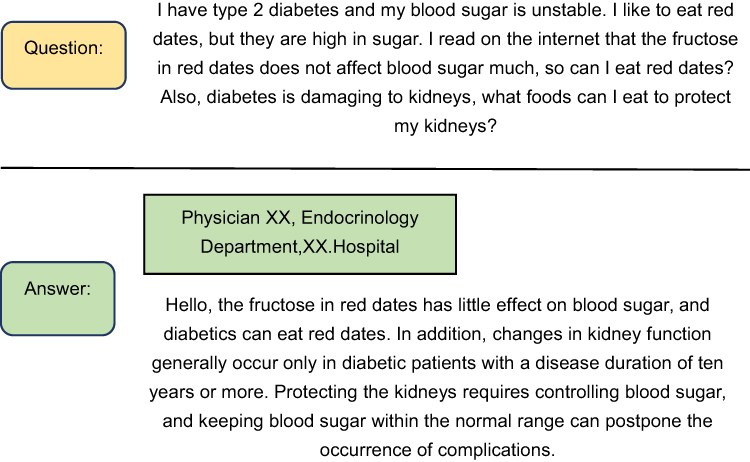 |
Figure 1 Schematic diagram of the doctor-patient conversation segment of the web crawler data. |
Methods of Data Extraction
The web crawler applied the Basic Web Crawling crawler program, written in Python. Starting with a given set of seed URLs, the web crawler fetched web pages. After a successful download, the HTML of the web page was parsed, and hyperlinks to other web pages were extracted. These links were then analyzed and added to a priority queue called the “frontier”. The web graph was then accessed through those URLs saved in the frontier. The crawler repeated this process until the frontier was empty or manually stopped.
Data Screening
The inclusion criteria for the data in this study were: online questions from patients with type 2 diabetes themselves or their family members. Exclusion criteria: 1) online questions from patients with type 1 diabetes, gestational diabetes, and special types of diabetes; 2) questions with incomplete information or unclear statements; and 3) questions with ineffective communication with physicians were excluded. Altogether, 2305 raw data items were screened to obtain a total of 1982 valid datapoints. The data were also categorized according to patients’ disease descriptions, and to ensure the quality of the classification, the researchers obtained professional clinical support from physicians. All questions were classified into three categories: 1) undiagnosed patients (374 items); 2) diagnosed people with diabetes (1560 items), and 3) patients with suspected diabetes (patients who have been diagnosed but do not believe the fact that they have the disease and repeatedly confirm it;45 items). This study focused on exploring the demand preferences for self-management among patients with confirmed type 2 diabetes. Therefore, 1605 data items were selected for this study based on questions from patients with diagnosed and suspected diabetes.
Data Analysis
The web crawler data were analyzed in two stages: firstly, the web crawler data were coded to analyze the needs of people with diabetes for self-management through grounded theory; secondly, to describe patients’ preferences for self-management through frequency statistics of the codes.We used the grounded theory approach proposed by Corbin and Straus to guide the research design,27 because the data obtained through web crawlers are fragments of doctor-patient conversations with a broad geographic scope, a wide range of periods, and a large and overly fragmented content. The coding stages included three main phases as follows: (1) open-ended coding, (2) axial coding, and (3) selective coding. The initial phase of open-ended coding was conducted by two researchers to identify, label, and conceptualize the phenomena experienced by people with diabetes by reading the crawler’s data line by line and extracting keywords and phrases. That process resulted in codes through research team meetings, respective analyses and review. Axial coding was used to discover and establish connections between conceptual classes. The researchers grouped the open-ended coding results and identified phenomena related to the self-management needs of people with diabetes through multiple meetings and reviews with the research team. During the selective coding process, the research team integrated the relationships between all extracted classes by deriving an integrated, highly abstract core class to fully explain patients’ preferences during illness and self-management.
Qualitative Interviews
Study Design and Sample
This survey was conducted at a tertiary hospital in Guangdong Province in China from November 2021 to March 2022. We conducted semi-structured interviews with 22 patients with diabetes. The inclusion criteria were patients: 1) who met the diagnostic criteria for type 2 diabetes mellitus established by the World Health Organization (WHO); 2) diagnosed with diabetes mellitus for ≥1 year; 3) with good communication skills; and 4) willing to participate in the study. Patients were excluded if they withdrew from the study before data collection was completed. Open-ended questions were asked based on patients’ disease history and self-management process, to better understand and explore the intrinsic reasons for participants’ behavioral preferences.
Procedure
Researchers trained in qualitative methods conducted face-to-face in-depth, semi-structured interviews with patients with diabetes. The interview questions focused on the needs of patients in terms of disease management in their daily lives. The questions were as follows: What life changes has diabetes brought about? (Prompts: What compromises have you made for diabetes? What is the impact of the changes brought about by the disease on your life?) What are the problems in the disease management process? (Prompts: How do you overcome difficulties? How do you seek help?) What are the essential aspects of the diabetes management process? The same investigator conducted all interviews to ensure consistency. Interviews were terminated once data saturation occurred. Interviews lasted between 30 minutes and one hour and included questions about self-management in the daily lives of people with diabetes. The interviews were conducted when the time was appropriate for the participants and live recordings were conducted after informed consent was obtained. All respondents had confirmed before the start of the interview that everything they expressed in the interview would be anonymized in the final results sharing. Interview data were transcribed within 24 hours.
Information Analysis
This study conducted data analysis through content analysis method of qualitative research.28 Two authors coded and analyzed data in parallel and independently, reading the original text repeatedly to identify initial codes, which were then created into themes related to the research questions. All team members participated in group discussions to resolve any discrepancies. Six themes and 17 sub-themes were eventually obtained. Typical quotes from participants were selected as examples to support each theme and answer the research questions.
Results
Web Crawler
The valid data from the crawling results of the 4 online health communities were 1605. We used the grounded theory to analyze the primary data. 6 themes and 25 sub-themes were analyzed regarding the questions and needs of people with diabetes arising from their illness and treatment (Table 1, more coding processes are shown in Appendix 2). The six themes were medication management needs, needs to resolve conflicts between illness and daily life, dietary management needs, knowledge needs, glucose monitoring needs, and exercise management needs. While six topics are highly relevant to the current “five horsemen” of diabetes health management——medication use, diet control, knowledge, glucose monitoring, and physical activity. There is also a result beyond the “five horses”, namely, the need to address the conflict between illness and daily life. This is a need that exists outside of the current health management and is inextricably linked to the daily lives of patients.
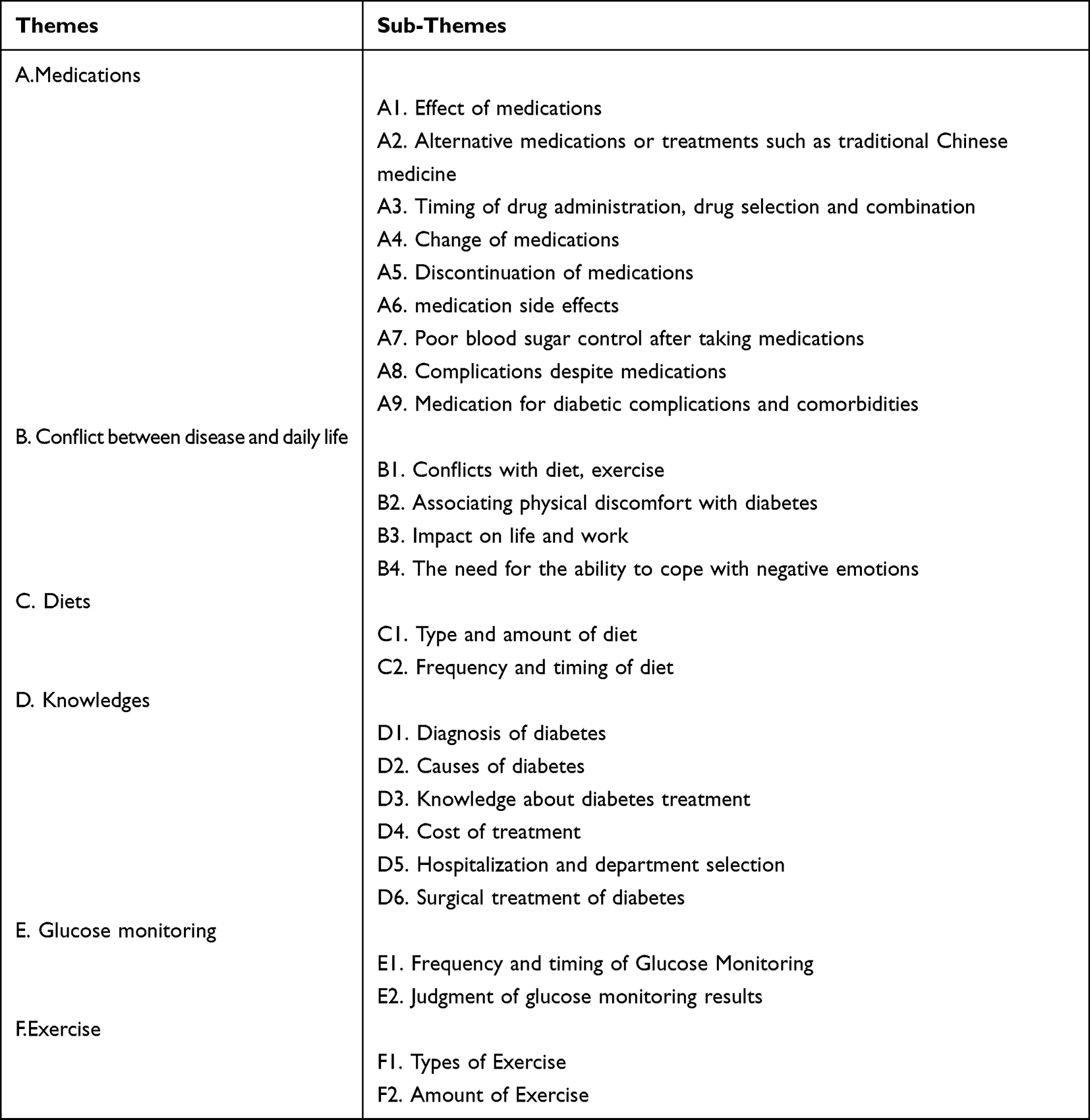 |
Table 1 Classification of Self-Management Needs of People with Diabetes Based on Web Crawler Data |
By performing frequency counts on the codes, this study found a clear preference for self-management behaviors among diabetics, with a preference for “medication management” and “resolving conflicts between disease and daily life”. In contrast, their needs for diet control, exercise, blood glucose monitoring, and knowledge are few and shallow. Overall, medication management was the most widespread patient need, with 654 medication management items out of 1605 results, accounting for 40.74% of total needs. This was followed by the conflict between disease and daily life, involving 526 items (32.77%). Diet management ranked third, containing 187 items and accounting for 11.65% of needs. Fourth was diabetes diagnosis and treatment knowledge, including 186 items (11.58%). Fifth was blood glucose management with 25 articles accounting for 1.55%, and finally, exercise management, included 20 articles (1.24%). The people with diabetes in this study had a clear preference for the choice of self-management matters as shown in the figure (Figure 2).
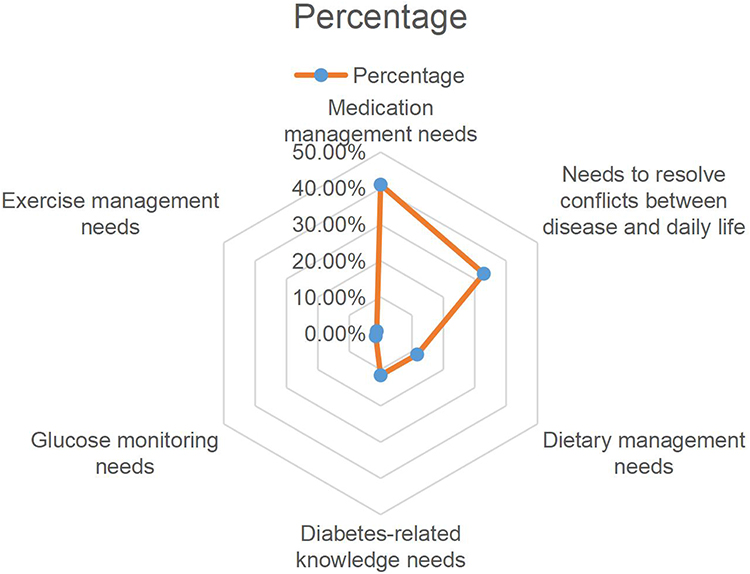 |
Figure 2 Preferences of people with diabetes for self-management. Percentage: n/N; N represents the total number of text encoding frequencies, which is 1605; n represents the number of text encoding frequencies for each self-management requirement. |
Among the dimensions of self-management, patients generally preferred medication management the most, and after medication, our new finding “the conflict between illness and daily life” became the second concern of patients.Surprisingly, diet, knowledge, exercise, and glucose monitoring – all long considered important by the medical profession – accounted for only a small percentage of overall needs. Why has this polarization developed? What is the internal logic of the phenomenon? To address these questions, we conducted face-to-face qualitative interviews with patients, seeking to summarize the intrinsic causes in the patients’ daily lives.
Qualitative Interviews
Twenty-two people with diabetes were recruited for in-depth interviews in this study, 14 (63.6%) of whom were male and 8 (36.3%) were female. The age of the participants ranged from 38 to 69 years, the duration of diabetes ranged from 2 to 24 years. Participant demographics are shown in Table 2.
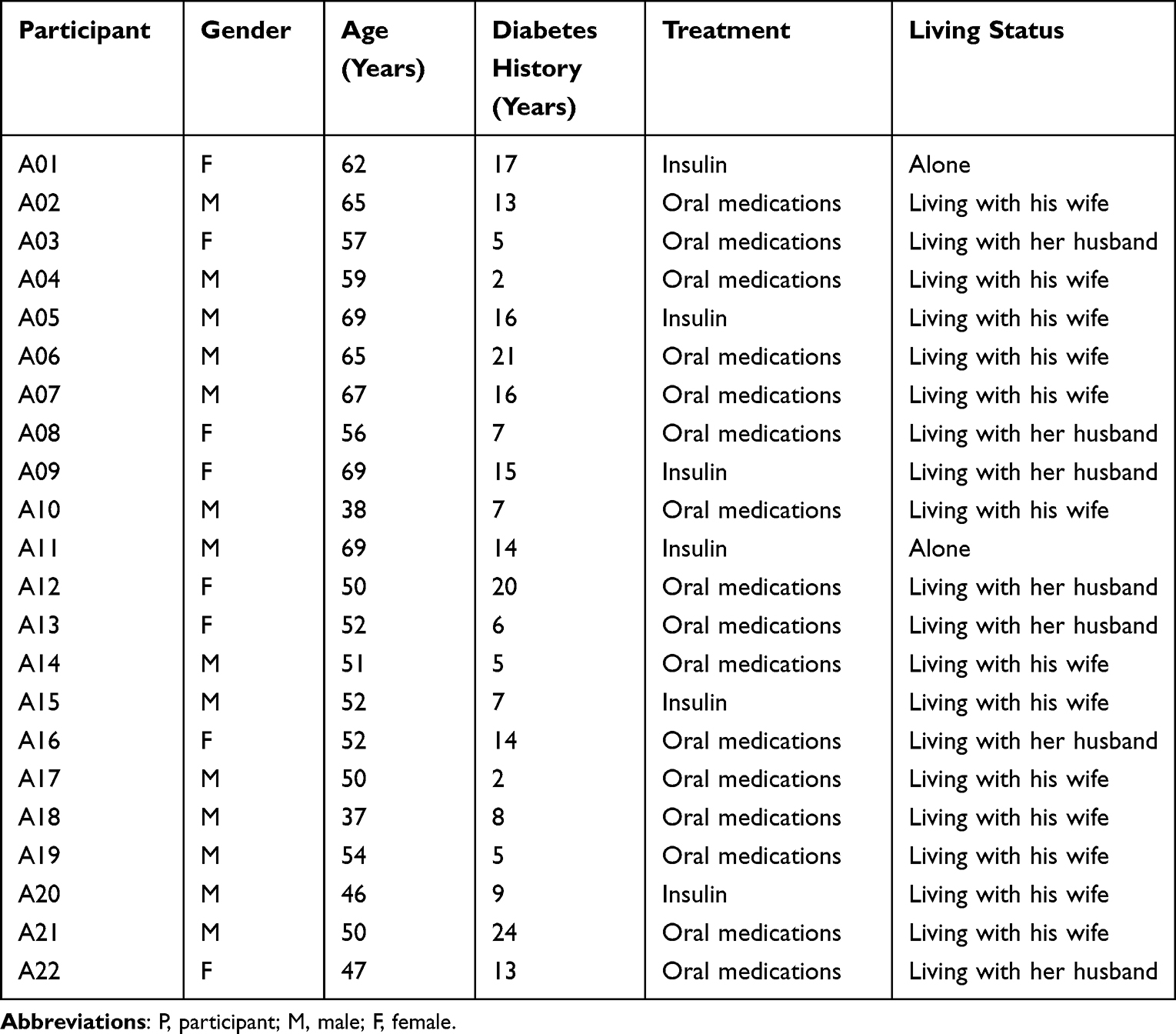 |
Table 2 Demographic Data of the Participants (n=22) |
The web crawler data indicated that patients’ demands for medication is the strongest, and the need to address the disease’s restrictions and conflicts in daily life ranks second. However, the proportion of needs related to diet, knowledge of diabetes treatment, blood glucose monitoring, and exercise was small. We further explain the reasons underlying this ranking result through qualitative interviews. This study found that patients’ concerns about medication were mainly due to the following three aspects: the effect of drugs is direct and obvious, medication use makes life less complicated, and progressive side effects. The patients’ concerns about the conflict between disease and daily life are often caused by the following three aspects: diabetes impacts social roles, disease complicates life, and reducing the impact of the disease on life. The reason for the low demand for diet, blood glucose monitoring, exercise, and knowledge about diabetes is that the patients mainly “know but don’t do”, which is manifested by misconceptions, excessive complexity, and increased burden of life.
Medications Administration
The primary concern of patients in the disease management process was medication management. The effect of medication is directly visible for patients, and it helps patients quickly control their blood sugar and relieve physical symptoms. At the same time, medication allows patients to briefly detach from the hardships associated with the lifestyle changes that have led to the need for medication. Some patients are frustrated in their search for appropriate medication, and the lack of efficacy after long-term use can cause patients to question the value of medication. Therefore, the intrinsic reasons for patient concerns about medication can be summarized as follows: the effect of the medication is directly visible; the medication makes the disease less complicated, and the ineffectiveness of the medication generates powerlessness and despair.
The Effect of Medications is Direct and Obvious
For patients, fluctuations in blood sugar can lead directly to discomfort or complications. As an immediate treatment, medication can help patients rapidly control their blood sugar.
A01:
I came here to be hospitalized in 2019 and was cured by coming here for insulin. The insulin is beneficial. The blood sugar will not be high if you take it before eating, and even if it is high, it is only a little high.
Patients find it difficult to avoid occasions such as going out and socializing in their daily lives, and they expect to control their blood sugar instantly with medication when they cannot strictly control their diet.
A18: I occasionally go out to socialize and inevitably drink. Knowing that my blood sugar will be high after socializing, I will inject insulin in advance. For example, if I usually inject 18 units, my blood sugar is normal. Then I will add six units, and that will solve the problem.
Medication Use Makes Life Less Complicated
People with diabetes are limited in many ways, and medications can briefly help remove them from this situation. Participants noted that medications ease the restrictions of going out.
A06: I chose to inject insulin later, because one of the advantages is that it is easy to control. If my blood sugar is high, I will take two more units of insulin, and if my blood sugar is low, I will take two less. Even if I go out to participate in activities, I don’t have to worry about my blood sugar.
A long-term controlled diet can lead to an increased desire for food, and the medication can briefly help patients satisfy occasional cravings while their blood sugar is stable It also relieves the patient’s psychological burden.
A05: I take insulin before I eat. I’ve experienced it myself. If I eat more at that meal, I will take more insulin. If I go out to eat a table of food, I can’t help it. After taking insulin, I dare to eat a little more.
Progressive Side Effects
In the early stages of the disease, medication can help patients with diabetes control their blood sugar and maintain their lifestyle. However, patients who do not follow the evidence-based treatment for an extended period may contribute to the progression of the disease. They may find that once-effective medication becomes less effective in regulating blood glucose and they may fail to change their medication. Even after patients are forced to change their lifestyles, the disease may progress further. Patients may feel a deep sense of powerlessness and despair in such cases.
A01: I usually take hypoglycemic drugs at home. I’ve taken everything – Metformin, Bystolic, Acarbose, Gliadin, etc. – and it doesn’t work. I’m really out of ideas.
In some patients, despite long-term medication, the disease further progresses and worsens due to various factors.
A15: My eyes are blurry now. I can’t see clearly. And there are other problems more serious than complications – problems with my personal sex life. How will I live after taking so many medications for nothing, with my blood sugar still so high and now so many problems with my body?
Conflict Between Disease and Daily Life
The chronic nature of diabetes means that many patients struggle with the long-term complexity of self-management, and the uncertainty of disease progression can keep patients living under a long-term disease haze. Medical rationality requires patients to change their previous lifestyle completely. However, patients live in the real world where medical rationality is not always perceived as relevant. Patients may feel that the disease limits every aspect of their lives, and most face conflicts and limitations in their daily lives.
Diabetes Impacts Social Roles
Patients do not want to be treated as patients, and they feel uncomfortable when they are treated differently because of their diabetes.
A09: When I eat with my friends, I cannot eat this or that, and then my friends will take special care of me when I order food. This makes me feel very uncomfortable – I am in good health. Why should I be treated as a patient?
Patients may feel ashamed of self-management of diabetes in their daily lives because of the strange looks or words of others.
A06: When taking insulin, people outside, such as neighbors, would mistakenly think I was on drugs. I felt embarrassed, so I didn’t want people to know that I was taking insulin. I was afraid that people would see it and would often sneak around and take it inside my room by myself.
Diabetes causes physical weakness, makes it difficult to cope with intense workloads, and creates a strong sense of social role deficit for patients.
A04: I support my family by working as a construction worker. It costs me money to see a doctor and pay for health insurance, and I spend more than 500 yuan every month. My mother is also diabetic. I can’t do heavy work now that I have diabetes, and if I don’t work, I can’t earn money, and if I don’t have money, I don’t have food to eat, so I really have no choice.
Disease Complicates Life
Diabetes requires patients to make radical lifestyle changes, creating a complex behavioral challenge for patients. Most patients report that diabetes places a heavy burden on their lives.
A01: I feel diabetes is easily aggravated if you ignore your diet. I usually eat in a less restrained way at home, eating more if I want to. I now realize that it is so harmful – not even one more bite of pork, and now, not even one more bite of rice.
The disease causes known or unknown physical symptoms that can cause worry and panic in patients.
A15: I feel so scared when I think of the complications of diabetes. I’m not afraid of dying, but I’m afraid of the kind of tragic death that people talk about, such as stroke, leg amputation and so on.
Diabetes tends to bring negative emotions such as irritability and anxiety to patients.
A02: After I got diabetes, I often felt that I was not in a good mood. I often whine at work, and at home. I lose my temper and want to curse. When people ask me to do things, I don’t want to do them, and I often have resistance, which I didn’t have before.
Reducing the Impact of the Disease on Life
When patients are caught in the conflict between illness and life, they make choices and adjustments based on their actual need to minimize the disruption of their lives. In our study, we found that this tendency varies, with some patients looking for a suitable alternative and others preferring to maintain their original lifestyle with the ultimate goal of restoring their lives as much as possible.
A17: Many people with diabetes say they can’t eat this or that, and they don’t dare to eat anything. Because people who eat less will lose weight quickly, I’m a little resistant to control the diet. I think this certainly means the disease is not cured but the body is collapsing, so I insist on eating everything to ensure my body is healthy before I can cure my disease.
A12: At the very beginning, I took Bactrim, a drug that made me flatulent after taking it. I was attending more events, and it was embarrassing to fart in front of so many people. I asked my doctor to change my medication, and then I took insulin. One advantage is that I can control it myself, and I can take two more units for high and two less units for low insulin levels. It was easier to control. I can do activities when I go out, and basically I can do it outside.
When patients find a balance between illness and life, or adapt to the contradictions between the two, they are able to reconcile themselves with their illness.
Self-Abandonment After Failing to Persevere
In this study, diet and knowledge of diagnosis and treatment were required less by the patients. Blood glucose and exercise management were two further topics of relatively little interest to patients, despite medical prescription requirements. The web crawler data showed that patients need less dietary management. However, interviews revealed that patients consider dietary management essential, probably because dietary management is fundamental for diabetes and there are many knowledge channels available about diet. Dietary education is widely recognized and implemented by patients so that fewer patients will search for dietary-related information online. However, most patients report that effective diet management is the most challenging aspect of diabetes.
A18: It’s not easy to control the diet. Usually, I have to ration my food. At first I only ate a bowl of rice, but then I slacked off over time, and I was often so hungry in the middle of the night that I got up to find something to eat.
Although patients strongly agree that diet management is essential for diabetes treatment, the complexity of diet management and the difficulty in maintaining it over time means patients often fail to adhere with the requirements of diet management, leading directly to poor glycemic control.
A17: Usually the family also controls me, and over time I sometimes can’t help but sneak out to restaurants to eat. I order three or four dishes, and then eat them all in one gulp, and after eating I find that my blood sugar is out of control.
In terms of blood glucose management, the pain and psychological burden of blood glucose monitoring can lead patients to believe that blood glucose management will increase their disease burden. In addition, patients may choose to ignore fluctuations in blood glucose until they cause physical discomfort.
A18: I can’t even hold a pen because my fingers are so pricked from blood glucose testing. Every day, I prick my fingers 6 or 7 times. How can I have enough fingers to prick? I’m afraid of it. I don’t want to test my blood sugar.
Regarding the reasons for the low demand for medical knowledge, patients’ limited receptivity and misconceptions about knowledge can lead to a lack of motivation to seek knowledge, and patients believe that medical knowledge has no direct impact on disease.
A03: What’s the use of knowledge? I just need to know how to take my medication, and how to control my diet. As long as I get my diet and medication right, nothing else will affect me.
Exercise management, which has a similar internal logic to blood glucose management, is more likely to be ignored by patients as they perceive that exercise will further increase their fatigue and not see immediate healing effects.
A11: I think it’s too tiring to go running every day. I’m tired easily with diabetes. I’m tired and weak, and I can’t stand it if I’m asked to go running again.
In summary, patients’ needs and preferences, as they attempt to manage diabetes, are influenced by their social environment. They typically prefer to seek treatments that can be seen to be effect and do not impact their lifestyles.
Discussion
This study used a mixed research approach to explore the self-management needs, preferences, and underlying causes of people with diabetes. Firstly, we summarized that people with diabetes have six self-management needs through the web crawler method. The two major needs, medication management and resolving conflicts between disease and daily life, accounted for 73.4% of the total, while the remaining four areas accounted for a small percentage. There is a polarization of patients’ needs. Secondly, qualitative interviews were conducted to explore the deeper reasons for the above phenomenon. This study found that, firstly, because medications can directly and visibly modulate blood glucose levels, they are the greatest hope for patients to manage their diabetes,29 echoing the result that medication management accounts for the largest proportion of web crawlers. Secondly, the management of diabetes needs to be completely embedded in the daily life of patients. Thus, balancing the disease and daily life naturally becomes the focus for patients. Third, integrated management approaches, such as diet, knowledge, blood glucose monitoring and exercise, are selectively ignored by patients, similar to the findings of a survey involving 17 countries,30 as an adverse behavioral response to the integration of the disease into daily life.
Therefore, the web crawler results indicate the self-management needs of patients with diabetes, and the qualitative interview results elucidate the behavioral mechanism of these preferences (Figure 3). Patients value medication and are concerned about the conflict between their illness and daily life. The logic is that the illness disrupts daily life but the effective medication helps them to instantly escape the negative feelings associated with changing their lifestyle while controlling the illness.31 When the disease progresses and patients have to fully comply with a combination of diet, exercise, and blood glucose monitoring, the collision between real life logic and medical rationality makes it difficult for patients. Patients seek a balance between life and disease, making trade-offs between diet, exercise, knowledge, blood glucose monitoring, and other comprehensive treatments based on their own needs and situation.
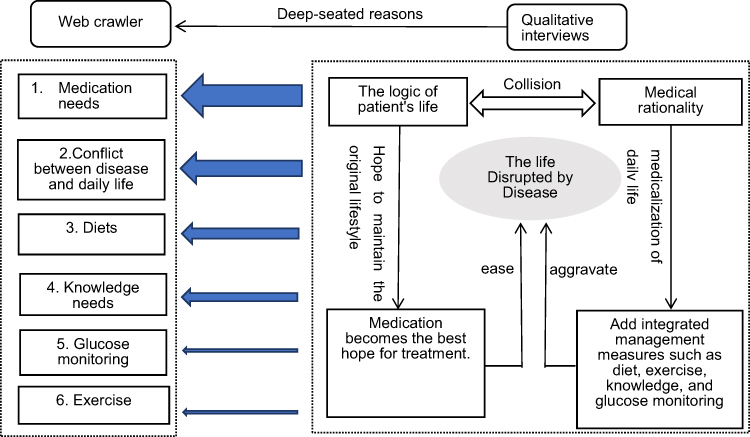 |
Figure 3 Logic diagram of data demand preferences for qualitative interviews. 1. The analysis results of the web crawler data are shown on the left side of the blue cutout in the Figure 2. The blue arrows are from wide to narrow, indicating that the patient’s needs are progressively smaller from medication needs to exercise needs. 3. To the right of the blue arrows are the analysis results of the qualitative interviews, which are used to explain the deeper reasons for the web crawler results. |
The analysis of patients’ preference logic reveals that patients – as social beings – seek a balance between the logic of life and medical rationality based on their individual feelings after the disease has disrupted life. Thus, we conclude the following:
A life out of control and a disease that is hard to solve.Patients must manage their diabetes from the moment of diagnosis. They are often required to complete several daily tasks, such as monitoring blood sugar levels and adhering to complex medical protocols32 and the volume of information may overwhelm newly-diagnosed patients.33 Diabetes is a lifelong metabolic disease that requires patients to follow a long-term diet plan, increase exercise, monitor blood sugar, and receive health education. However, long-term adjustments to daily life to control diabetes may easily lead to patients experiencing feelings of resistance and rejecting health management.34 Although most patients understand the importance of diet control, adherence to exercise, and blood sugar monitoring, it can be difficult to maintain these behaviors, and several studies have shown that patients may choose not to comply.35 In one study, almost all participants lacked regular blood glucose monitoring, and although healthcare providers always emphasized the importance of 2-hour postprandial blood glucose measurement, most patients measured fasting blood glucose and selectively forgot to measure postprandial blood glucose.23 However, the effect of drugs on blood glucose control is straightforward.24 Patients consider medication as a way to escape lifestyle changes, helping them control their blood sugar and delay disease progression without changing their lifestyle.36 Drugs are patients’ main focus for diabetes treatment, reflecting reluctance to make long-term lifestyle changes for diabetes management. When blood glucose can be effectively controlled through medication, other comprehensive management options are often dismissed by patients.
The collision of life logic and medical reason. Academic rationality expects patients to establish new body norms, and medical rationality is a set of disease coping protocols with uniform standards. This is the well-known self-management requirement of various guidelines and medical standards of care for people with diabetes. Effective management of diabetes requires radical lifestyle changes, and patients are challenged daily by a series of complex behavioral demands, including following a diet plan, engaging in appropriate exercise, and monitoring blood sugar. Patients must integrate these tasks into their routines.37 However, patients want to return to the order of their lives as much as possible before they became ill. As in this study, patients perceived serious conflicts between illness and daily life. Self-management of diabetes not only complicates daily life, but affects basic social roles because of disease stigma, making patients desperate to resolve the conflict between the disease and daily life. Patients typically prioritize “normal” life and more or less ignore diabetes. Previous research supports these findings.38 This is the logic of the patient’s life. Patients seek to minimize the impact of the disease on their lives, and this is judged by how well lifestyle changes fit in with their lives. When patients are unable to successfully integrate diabetes into their lives,37 they focus on balancing their disease with their life. Faced with the complex additional burdens of diet, exercise, and blood sugar monitoring, patients make choices based on their own conditions. These findings explain why patients rely on pharmacological control rather than comprehensive management programs – medication is relatively easy to administer, has minimal impact on daily life, causes minimal disruption, and best meets the goal of controlling the disease without altering daily life.
The critical question that remains is, therefore, how to rationally embed disease self-management into patients’ lives. Our study found that patients prefer drug control because comprehensive management is too difficult to integrate in daily life. They do not consider other control methods unimportant, but effects of medication are easily visible and help balance life and diabetes. When medications are effective, patients selectively ignore the equally important comprehensive lifestyle treatments.39 Comprehensive management through lifestyle changes together with medication is too complicated.31 Conversely, when medication is not effective, patients must resort to other means of comprehensive treatment involving behavioral changes. In addition to medication “failure”, patients may find that the complex management of their lives is chaotic, and diabetes remains poorly managed and even worsens.40 The imbalance between disease management and daily life can lead to a deep sense of despair and powerlessness in diabetes self-management. Patients do not exist in an absolutely rational medical space. Their behavior is profoundly influenced by the social and cultural space in which they live and the rules of socialization. To control the logic of their lives when their physical and social roles are disrupted by disease, patients tend to “act” as healthy individuals, accounting for the emphasis placed on resolving the conflict between illness and daily life.
Limitations and Future Directions
There are some limitations to this study. Firstly, as a qualitative study, one of its limitations is the possibility of selection bias. Secondly, the qualitative interviews in this study were conducted in a more economically developed city and may not be representative of the experiences and perspectives of all people with diabetes in China, which may affect the generalizability of the findings. Future studies should recruit more participants from different regions and different life backgrounds.
Conclusion
In conclusion, medication management, disease and daily life conflicts are the most predominant needs of Chinese people with diabetes, while diet, diabetes knowledge, blood glucose monitoring and exercise are their least common needs. Understanding the individual’s knowledge and understanding of diabetes self-management and the expression of the patient’s daily life situation can guide the health care team to optimize collaboration and develop an individualized care plan. The internal logic lies in patients’ attempts to balance the disease and the lifestyle they have developed over time to find a reasonable way to integrate diabetes into their daily lives. Therefore, understanding the individual’s perception and understanding of diabetes self-management and the expression of the patient’s daily life situations can guide the medical team to optimize collaboration on personalized care plans.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author Ni,Gong on reasonable request.
Ethics Approval
The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Jinan University (KY-2022-110), and its implementation process strictly complied with the Declaration of Helsinki. Before the interview, all participants provided informed consent after understanding their right to confidentiality, anonymity, and voluntary participation. Participants had the right to stop the interview at any time. All data were used for research purposes only and are not accessible to anyone other than the research team.
Consent to Participate
Informed consent was obtained from all subjects involved in the study. Subject Statement:The investigator explained to me the background, purpose, steps, risks, and benefits of the study (Self-Management Needs and Preferences of People with Type 2 Diabetes in China: A Mixed Methods Study), and I was given sufficient time and opportunity to ask questions. I was satisfied with the answers provided by the researcher. I know who to contact when I have questions or want further information. I have read this informed consent form and have decided to participate in this study. I understand that I can withdraw from this study at any time during the study without any reason. I was told that I would be given a copy of this informed consent form, which contains my signature.
Acknowledgments
The authors are grateful to all the involved unknown subjects.
Funding
The study was developed without funding supports.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saeedi P, Petersohn I, Salpea P. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
2. Icks A, Haastert B, Arend W. Time spent on self-management by people with diabetes: results from the population-based KORA survey in Germany. Diabet Med. 2019;36(8):970–981. doi:10.1111/dme.13832
3. Sun H, Saeedi P, Karuranga. S. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
4. Angelos K. Healthy diet and self-care activities adherence improved life-quality and type 2 diabetes mellitus management in Turkish adults. Int J Med. 2020;1:58.
5. Basevi V, Di Mario S, Morciano C, Nonino F, Magrini N. Comment on: American Diabetes Association. Standards of medical care in diabetes--2011. Diabetes Care. 2011;34(5):e53. doi:10.2337/dc11-0174
6. Tomky D, Tomky D, Cypress M. Aade position statement. Diabetes Educ. 2008;34(3):445–449. doi:10.1177/0145721708316625
7. Hinder S, Greenhalgh T. ”This does my head in”. Ethnographic study of self-management by people with diabetes. BMC Health Serv Res. 2012;12(83). doi:10.1186/1472-6963-12-83
8. Peyrot M, Burns KK, Davies M. Diabetes Attitudes Wishes and Needs 2 (DAWN2): a multinational, multi-stakeholder study of psychosocial issues in diabetes and person-centred diabetes care. Diabetes Res Clin Pract. 2013;99(2):174–184. doi:10.1016/j.diabres.2012.11.016
9. Wei W, Liu M, Gao F. A study on the current status of self-management ability of diabetes patients in communities in 3 provinces in China. Chinese health education. Chinese Health Education. 2021;37(07):602–605.
10. Ji L, Su Q, Feng B. Glycemic control and self-monitoring of blood glucose in Chinese patients with type 2 diabetes on insulin: baseline results from the COMPASS study. Diabetes Res Clin Pract. 2016;112:82–87. doi:10.1016/j.diabres.2015.08.005
11. Srulovici E, Feldman B, Reges O. Which patients with Type 2 diabetes will have greater compliance to participation in the Diabetes Conversation Map™ program? A retrospective cohort study. Diabetes Res Clin Pract. 2018;143:337–347. doi:10.1016/j.diabres.2018.07.037
12. Qi X, Xu J, Chen G. Self-management behavior and fasting plasma glucose control in patients with type 2 diabetes mellitus over 60 years old: multiple effects of social support on quality of life. Health Qual Life Outcomes. 2021;19(1):254. doi:10.1186/s12955-021-01881-y
13. Wang L, Peng W, Zhao Z. Prevalence and Treatment of Diabetes in China, 2013-2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
14. Sun X, Wang H, Fanglei X. Effect of individualized health education on self-management behavior and blood glucose control in patients with type 2 diabetes mellitus. China Nursing Management. 2015;15(02):179–182.
15. Davis J, Fischl AH, Beck J. 2022 National Standards for Diabetes Self-Management Education and Support. Diabetes Care. 2022;45(2):484–494. doi:10.2337/dc21-2396
16. DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ. 2002;325(7367):746. doi:10.1136/bmj.325.7367.746
17. Davies MJ, Heller S, Skinner TC. Effectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: cluster randomised controlled trial. BMJ. 2008;336(7642):491–495. doi:10.1136/bmj.39474.922025.BE
18. Azami G, Soh KL, Sazlina SG. Effect of a Nurse-Led Diabetes Self-Management Education Program on Glycosylated Hemoglobin among Adults with Type 2 Diabetes. J Diabetes Res. 2018;2018:4930157. doi:10.1155/2018/4930157
19. Essien O, Otu A, Umoh V. Intensive Patient Education Improves Glycaemic Control in Diabetes Compared to Conventional Education: a Randomised Controlled Trial in a Nigerian Tertiary Care Hospital. PLoS One. 2017;12(1):e0168835. doi:10.1371/journal.pone.0168835
20. Berenguera A, Molló-Inesta À, Mata-Cases M. Understanding the physical, social, and emotional experiences of people with uncontrolled Type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2016;10:2323–2332. doi:10.2147/PPA.S116173
21. Debussche X, Besançon S, Balcou-Debussche M. Structured peer-led diabetes self-management and support in a low-income country: the ST2EP randomised controlled trial in Mali. PLoS One. 2018;13(1):e0191262. doi:10.1371/journal.pone.0191262
22. Spencer MS, Kieffer EC, Sinco B. Outcomes at 18 Months From a Community Health Worker and Peer Leader Diabetes Self-Management Program for Latino Adults. Diabetes Care. 2018;41(7):1414–1422. doi:10.2337/dc17-0978
23. Peng X, Guo X, Li. H, Qualitative A, Liu C, Du Y. Exploration of Self-Management Behaviors and Influencing Factors in Patients With Type 2 Diabetes. Front Endocrinol (Lausanne). 2022;13:771293. doi:10.3389/fendo.2022.771293
24. Lv X, Yu DSF, Cao Y, Xia J. Self-care experiences of empty-nest elderly living with type 2 diabetes mellitus: a Qualitative Study From China. Front Endocrinol (Lausanne). 2021;12:745145. doi:10.3389/fendo.2021.745145
25. Tewahido D, Berhane Y. Self-care practices among diabetes patients in addis ababa: a qualitative study. PLoS One. 2017;12(1):e0169062. doi:10.1371/journal.pone.0169062
26. Velkumar K, Thendral. P, Crawler W. Web Crawler Algorithms: a Perspective. Int J Eng Adv Technol. 2020;9:203–205. doi:10.35940/ijeat.E9362.069520
27. Anselm Strauss Juliet Corbin. Basics of Qualitative Research Techniques and Procedures for Developing Grounded Theory. Los Angeles London New Delhi; 2015.
28. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
29. Al Johani KA, Kendall GE, Snider PD. Self-management practices among type 2 diabetes patients attending primary health-care centres in Medina, Saudi Arabia. East Mediterr Health J. 2015;21(9):621–628. doi:10.26719/2015.21.9.621
30. Nicolucci A, Kovacs Burns K, Holt. RI. Diabetes Attitudes, Wishes and Needs second study (DAWN2™): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet Med. 2013;30(7):767–777. doi:10.1111/dme.12245
31. Hayes RP, Bowman L, Monahan PO, Marrero DG, McHorney CA. Understanding diabetes medications from the perspective of patients with type 2 diabetes: prerequisite to medication concordance. Diabetes Educ. 2006;32(3):404–414. doi:10.1177/0145721706288182
32. DiMeglio LA, Evans-Molina C, anRichard A. Type 1 diabetes. The Lancet. 2018;391(10138):2449–2462. doi:10.1016/S0140-6736(18)31320-5
33. Winkley K, Evwierhoma C, Amiel SA, Lempp HK, Ismail K, Forbes A. Patient explanations for non-attendance at structured diabetes education sessions for newly diagnosed Type 2 diabetes: a qualitative study. Diabet Med. 2015;32(1):120–128. doi:10.1111/dme.12556
34. Holt RI, Nicolucci A, Kovacs. BK. Diabetes Attitudes, Wishes and Needs second study (DAWN2™): cross-national comparisons on barriers and resources for optimal care--healthcare professional perspective. Diabet Med. 2013;30(7):789–798. doi:10.1111/dme.12242
35. Suglo JN, Evans C. Factors influencing self-management in relation to type 2 diabetes in Africa: a qualitative systematic review. PLoS One. 2020;15(10):e0240938. doi:10.1371/journal.pone.0240938
36. Elliott AJ, Harris F, Laird SG. Patients’ beliefs on the impediments to good diabetes control: a mixed methods study of patients in general practice. Br J Gen Pract. 2016;66(653):e913–e919. doi:10.3399/bjgp16X687589
37. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1):14. doi:10.1186/2251-6581-12-14
38. Zoffmann V, Kirkevold M. Life versus disease in difficult diabetes care: conflicting perspectives disempower patients and professionals in problem solving. Qual Health Res. 2005;15(6):750–765. doi:10.1177/1049732304273888
39. Broadbent E, Donkin L, Stroh JC. Illness and treatment perceptions are associated with adherence to medications, diet, and exercise in diabetic patients. Diabetes Care. 2011;34(2):338–340. doi:10.2337/dc10-1779
40. Trout KK, McCool WF, Homko CJ. Person-centered primary care and type 2 diabetes: beyond blood glucose control. J Midwifery Womens Health. 2019;64(3):312–323. doi:10.1111/jmwh.12973
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.