Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
A Mixed-Method Study of Medication-Related Burden Among Multi-Drug Resistant Tuberculosis Patients in West Java, Indonesia
Authors Ausi Y, Yunivita V, Santoso P ![]() , Sunjaya DK
, Sunjaya DK ![]() , Barliana MI
, Barliana MI ![]() , Ruslami R
, Ruslami R
Received 15 June 2024
Accepted for publication 11 September 2024
Published 24 September 2024 Volume 2024:16 Pages 707—719
DOI https://doi.org/10.2147/CEOR.S473768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Yudisia Ausi,1 Vycke Yunivita,2 Prayudi Santoso,3,4 Deni Kurniadi Sunjaya,5 Melisa Intan Barliana,1,6 Rovina Ruslami2
1Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Division of Pharmacology and Therapy, Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Division of Pulmonary and Critical Care, Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 5Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 6Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Melisa Intan Barliana, Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Bandung Sumedang KM 21, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Background: Multidrug-resistant tuberculosis presents a challenging obstacle in global TB control. It necessitates complex and long-term therapy, which can potentially lead to medication-related burdens that may ultimately reduce therapy adherence and quality of life.
Purpose: This study aimed to gain a deep understanding of the medication-related burdens experienced by multidrug-resistant tuberculosis patients.
Methods: The study was conducted using a convergent mixed-method approach involving MDR-TB patients and their caregivers. Qualitative data were collected through semi-structured in-depth interviews, while quantitative data were gathered using the validated Living with Medicine Questionnaire 3. In the quantitative part, associations between patients’ characteristics and burden levels were analysed using bivariate and multivariate analyses.
Results: Seventy-four participants were involved in the study, with 71 of them completing the questionnaire and 36 participating in interviews. The qualitative results revealed the subjectivity of medication-related burden perception, which could not be fully captured by the quantitative method. Four themes of medication-related burdens emerged: personal beliefs, regimen burdens, socioeconomic burdens, and healthcare burdens. The quantitative results provided a generalized representation of the population. Age and side effects were found to be significantly associated with higher burden levels, with those aged 18– 30 having an odds ratio (OR) of 7.303 (95% CI: 1.045– 51.034), and those aged 31– 40 having an OR of 6.53 (95% CI: 1.077– 39.607). Additionally, experiencing side effects had a substantial impact, with an OR of 46.602 (95% CI: 2.825– 768.894). Both sets of results are valuable for designing patient-centered care.
Conclusion: MDR-TB therapy imposes a significant burden, particularly regarding the characteristics of regimen. By understanding this burden, healthcare professionals can help improve the quality of life for these patients.
Keywords: mixed method, in-depth interview, living with medicine questionnaire
Introduction
Tuberculosis (TB) remains a global health problem, especially in lower- and middle-income countries. In 2023, Indonesia had the second-highest prevalence of TB in the world.1 This infectious disease requires patients to take several medicines over a long period. Moreover, in multidrug-resistant (MDR) conditions, the patient must take multiple medications for an even longer duration of treatment. The treatment duration should be 9–11 months for a short-term regimen and usually 18–20 months for a long-term regimen (LTR).2
The chronic condition is quite challenging due to the need for self-management regarding the treatment and the illness itself. Although the use of medicine is the main intervention in MDR-TB treatment, it helps in relieving the symptoms; prolonged medication often comes with several consequences that require extra time, effort, and finances for patients.3–5 These challenges can be unbearable for several patients and are perceived as a burden. The medication-related burden may affect how patients perceive the need for medicine, regardless of other factors such as background and clinical condition, which are related to day-to-day difficulties.4,6 Medication-related burden is a complex phenomenon that involves different components and elements interacting with each other.7 It could lead to treatment non-adherence and affect the quality of life.6 Meanwhile, adherence to TB treatment is critical in achieving success, controlling disease spread, and minimizing the aggravation of drug resistance.8
Since medication-related burdens threaten treatment success and well-being, it is essential to evaluate the perception of patients regarding their own experiences and treatment outcomes.4 This study aimed to deeply understand the medication-related burden in MDR-TB patients by combining qualitative and quantitative methods (mixed methods). The quantitative section used a validated questionnaire to measure medication-related burden as the impact of long-term treatment. The qualitative section (in-depth interviews) captured a broader and deeper narrative of medication-related burdens, which cannot be fully described with a quantitative study.9,10 This research is expected to improve MDR-TB patient care and help patients connect treatment routines with the expectations of their daily life.11
Materials and Methods
Study Setting and Population
Participants were recruited from the MDR-TB clinic of Hasan Sadikin General Hospital, a tertiary referral hospital in West Java, Indonesia. All participants or their guardians gave written informed consent to participate in this research before data collection process (either for interview or filling questionnaire, or both). Patients were attending the hospital for monthly follow-ups between February and March 2021. The following were the inclusion criteria for qualitative and quantitative study participants: (1) Patients diagnosed with MDR-TB, (2) aged above 18 years old, (3) completed the first months of therapy, and (4) had no treatment interruptions (missed monthly-scheduled follow-ups) in the current regimen. Seventy-four patients participated in this study. Among them, 71 completed the questionnaire for the quantitative study. A one-month total sampling technique was used for quantitative data collection. For the qualitative section, data reached saturation after 36 patients were interviewed to explore the burden related to long-term medication use. Twenty-seven patients were interviewed privately, while others were accompanied by their caregivers due to communication difficulties caused by their health conditions.
Qualitative Data Collection and Analysis
Prior to participant recruitment, a key informant interview was conducted with an internist who is an expert in TB care, to gather preliminary information about the medication-related burden in MDR-TB patients. The in-depth interview guide was developed from a previous study on issues regarding long-term medicines by Krska et al, 201312,13 and adjusted to the local context based on the information from the key informant.
Semi-structured in-depth interviews were then conducted with patients and/or their caregivers to understand their experiences, beliefs, and perceptions of the burden associated with MDR-TB treatment and how they deal with it. The interviews were conducted by a research member who was trained in qualitative methods. Participants were recruited until data saturation was reached, with a total of 36 participants. The interviews lasted for 15–20 minutes in Bahasa Indonesia, and the audio was digitally recorded. The recordings were transcribed verbatim, and the transcript data were managed using NVivo12 software for thematic analysis.
Quantitative Data Collection and Analysis
The medication-related burden was quantitatively measured using the Living with Medicine Questionnaire version 3 (LMQ-3), developed by Katusiime et al, 2018.14 The LMQ-3 consists of 41 items and covers eight domains (1) interference with day-to-day life (6 items); (2) patient-doctor relationships (5 items); (3) perceived effectiveness (6 items); (4) general concern about medicine (7 items); (5) side effect burden (4 items); (6) practical difficulties (7 items); (7) cost-related burden (3 items); (8) autonomy over medicine (3 items). The LMQ-3 scores were transformed from ordinal data to numeric data (person measure/logit) using Winsteps software and classified into lower and higher burdens based on the mean and standard deviation values. Higher person measure reflected higher medication-related burden. Sociodemographic and clinical characteristics were also collected from patient forms and medical records. Patients’ characteristics data were presented as n (%). The association between patients’ characteristics and medication-related burden was analysed using chi-square for bivariate analysis and binary logistic regression for multivariate analysis, with SPSS v.25 (α = 0.05, CI 95%).
Results
Seventy-one patients agreed to fill out the questionnaire, and 36 agreed to be the informant of the interview.
Qualitative Result
Four themes of medication-related burdens have been identified from in-depth interviews with 36 participants, namely: personal beliefs, regimen burdens, socioeconomic burdens, and healthcare burdens (Table 1).
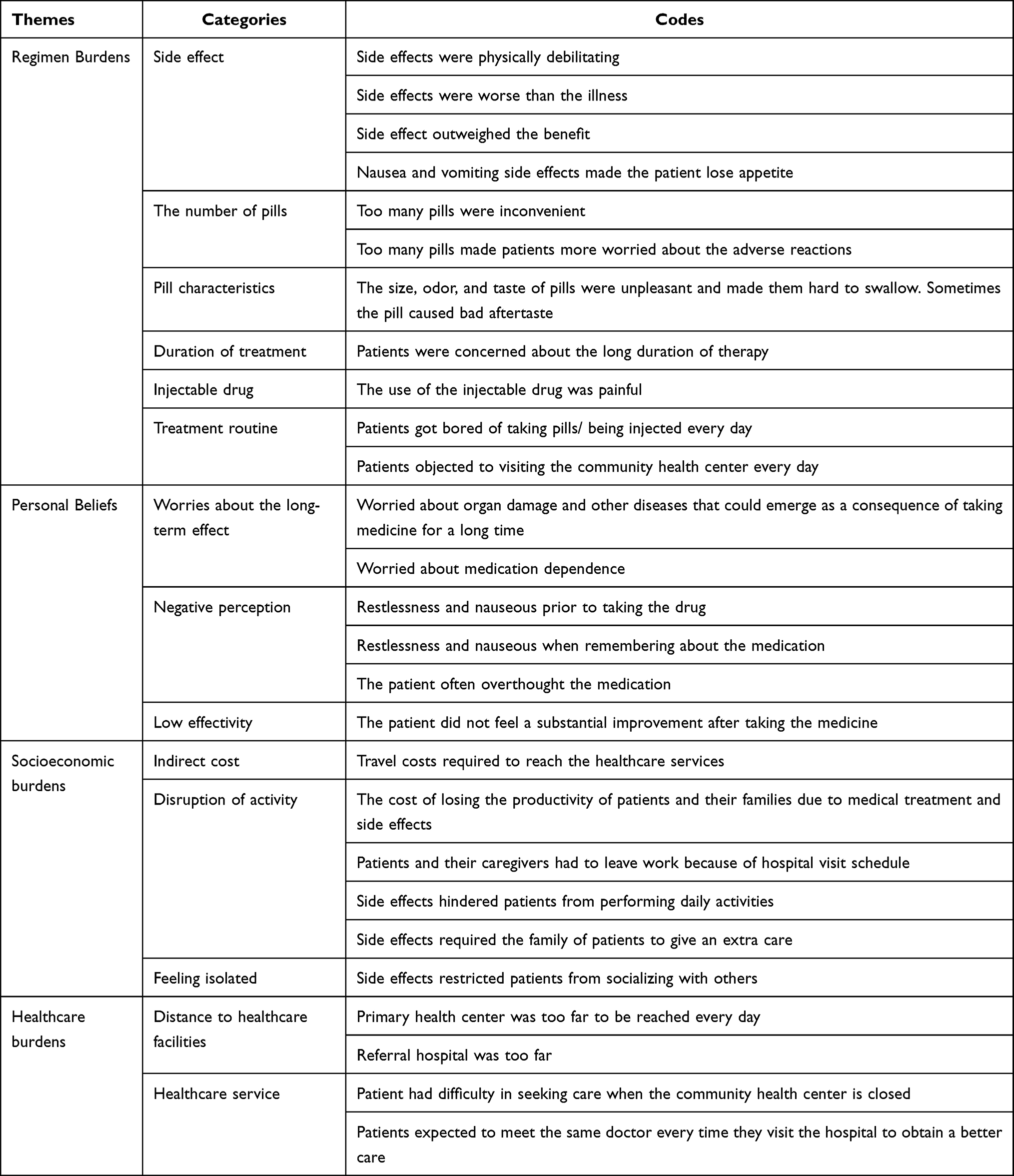 |
Table 1 Result of Thematic Analysis in Medication-Related Burden Among MDR-TB Patients |
Regimen Burden
MDR-TB treatment leads to several regimen-related concerns. In terms of physical characteristics, the taste of the pill was very bitter, the size was too big, and the odor was very strong. Moreover, patients had to take a large number of pills with all these distinct characteristics every day, for a long time. However, the main concern about the regimen is mainly side effects. The inevitable consequence of therapy interrupts day-to-day life. Some patients perceived the symptoms as terrible and not worth the benefit or even worse than the illness itself. The worst side effect period was during the first three months of therapy.
The side effect outweighs the benefit. That is the truth (a female patient)
I was so sad. Medicine made her get worse instead of getting better (a male family member of the patient)
Manifestation of side effects varied from mild to debilitating effects. Nausea, vomiting, and lethargy were the most complained about side effects that interrupted daily activities. Other side effects included loss of appetite, abdominal pain, dizziness, tingling, and numbness in limbs, myalgia, arthralgia, dry, and scaly skin, hearing impairment, blurred vision, palpitations, restlessness, irritability, and hallucinations. Some patients claimed they lost consciousness for several hours after taking the medicine.
This medication is very terrible. He (pointing to someone) said that it feels like more than taking the drugs (psychotropics). That is true, just like being drunk, slurring. (a male patient)
I cried and said to the nurse, ‘I cannot do this. How come a person has to be injected every day with this kind of side effect? I’m dying, I’m going crazy’. (a female patient)
The worry about worse consequences made the patient seek alternative therapy.
One day, I looked for alternative medicine. The therapist said, ‘You better not take medicine anymore because we have another treatment’. We (my husband and I) decided to stop the medicine. We thought we had already got over it. But when I arrived home at night, I had a cough again. My husband was worried and said, ‘You’d better continue to take the medicine again’ (a female patient)
Personal Beliefs
Bad experiences with taking medicine resulted in negative perceptions of their medication. These perceptions in the patient’s mind guided their thoughts, feelings, or behavior. For example, when the time to take medicine was approaching, the patient felt the side effects symptoms, such as nausea, or nervousness. Other patients experienced similar sensations just by looking at something that reminded them of taking medicine.
I just told my son, ‘Do you want to take your medicine here right now?’ And then he suddenly vomited. (father of a patient)
Regardless of their personal experiences, some patients believed that medicine is a chemical that may cause long-term effects and dependence. This belief results in a hesitancy to continue therapy.
A worry does exist. If we take the medication and have certain diseases in our body, such as high uric acid and stomach disorders, it will come up. Our heart, kidney, and stomach will also be triggered. Those are what I am worrying about. (a male patient)
Two patients perceived the medicine to have low effectiveness. This perception of low effectiveness made the patients feel unsatisfied with the therapy.
Socioeconomic Burden
MDR-TB patients should have a daily visit to the community health center for Directly Observed Therapy and a monthly visit to a tertiary referral hospital for clinical follow-up. This induced three social and economic-related issues. First, although the direct medical costs are covered by health insurance, the indirect costs, such as travel expenses, may become a barrier for them in accessing healthcare facilities.
Last night, I had no money to afford the travel cost to get here. Yesterday, I tried to look for a loan, but no one could help me. This morning, I asked somebody else about it, and praise God, finally, I received a loan. (a male patient)
In the social context, side effects also cause a loss of productivity and a lack of socializing.
In the beginning (of therapy), (my husband) usually sleeps after taking medicine, gets some rest, and cannot do regular activities (a woman family member of the patient)
I rarely meet up with my friends because it is difficult to find the right time. I feel unwell after taking medicine. (a female patient)
Healthcare Burden
There were two concerns of patients related to healthcare: the distance to seek healthcare and daily visits to community health centers or hospitals. In addition, in terms of service, patients expected to have the same doctor for their monthly follow-ups. A patient also said that he was upset with the community health center service because he found it difficult to get spare medicine when the community health center was closed.
Last day, I was very upset with the healthcare service in the community health center. On that day, the pill was not taken properly due to vomiting, so I went to the community health center which was closed, and asked, the security officer whether I could get any spare medicine. The security officer said, ‘Today is a day off; it would be better to come here again tomorrow.’ Then, I answered, ‘No! The dose must not be skipped. Missing one dose will make the therapy restart. The pills are supposed to be ready.’ (a male family member of the patient)
Each burden category was an inseparable part of the other burdens. One perceived barrier may induce or exacerbate other problems. Figure 1 represents the interaction among the types of burdens in this study.
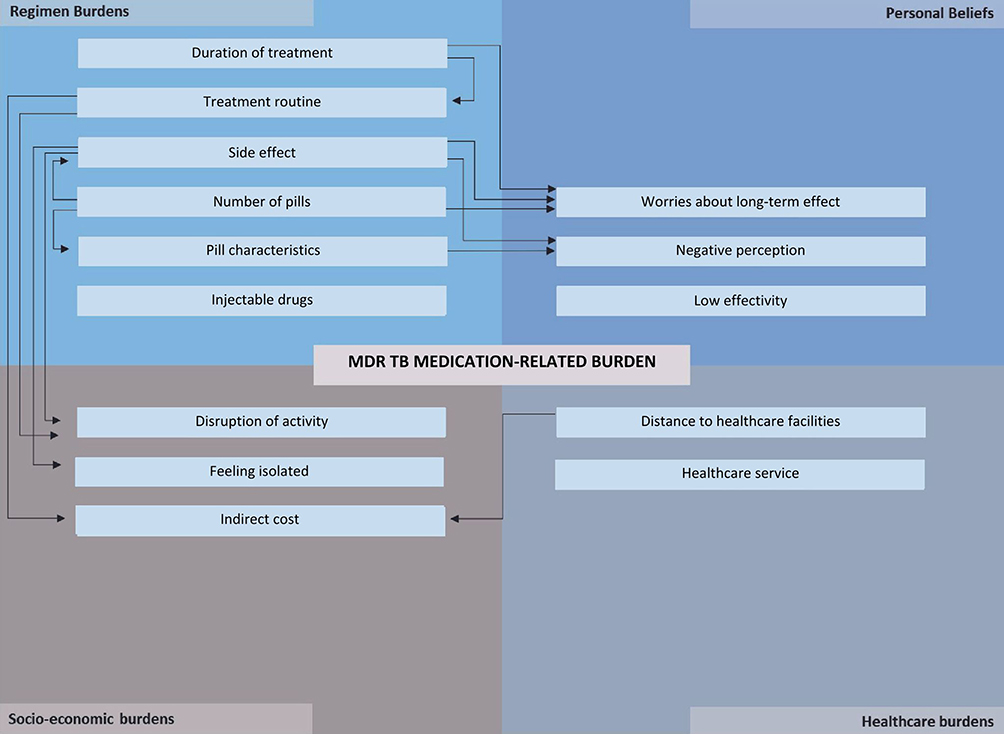 |
Figure 1 TB medication-related burdens. Abbreviation: TB, Tuberculosis. Notes: The arrow (→) means one burden worsens another burden. |
Quantitative Result
Seventy-one patients were included in this study. They were mainly male, at a productive age (below 40 years old), had income below the regional minimum wage, had lower educational backgrounds, and had family members as their caregivers. More than half of the patients received short-term regimens with various durations of treatment. Nine out of 10 patients experienced at least one side effect. The details of patients’ characteristics can be seen in Table 2.
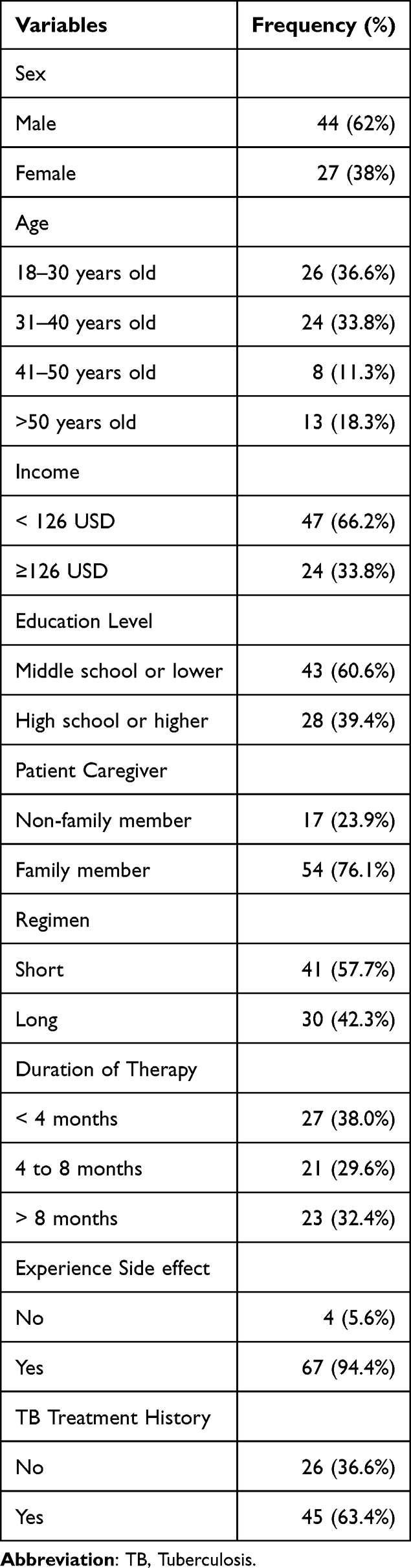 |
Table 2 Sociodemographic and Clinical Characteristics of Patients |
Based on LMQ-3 response result, the mean value for person measure is −0.28 ± 0.52 (see Table 3). Among 71 patients, 58 (81.7%) had person measure above −0.8, which were considered to have a higher medication-related burden (Table 4). This study observed associations between higher levels of burden and younger age: 18–30 years (OR 7.303, 95% CI: 1.045–51.034) and 31–40 years (OR 6.53, 95% CI: 1.077–39.607). The study also found an association between higher levels of burden and experienced side effects (OR 46.602, 95% CI: 2.825–768.894) as shown in Table 5.
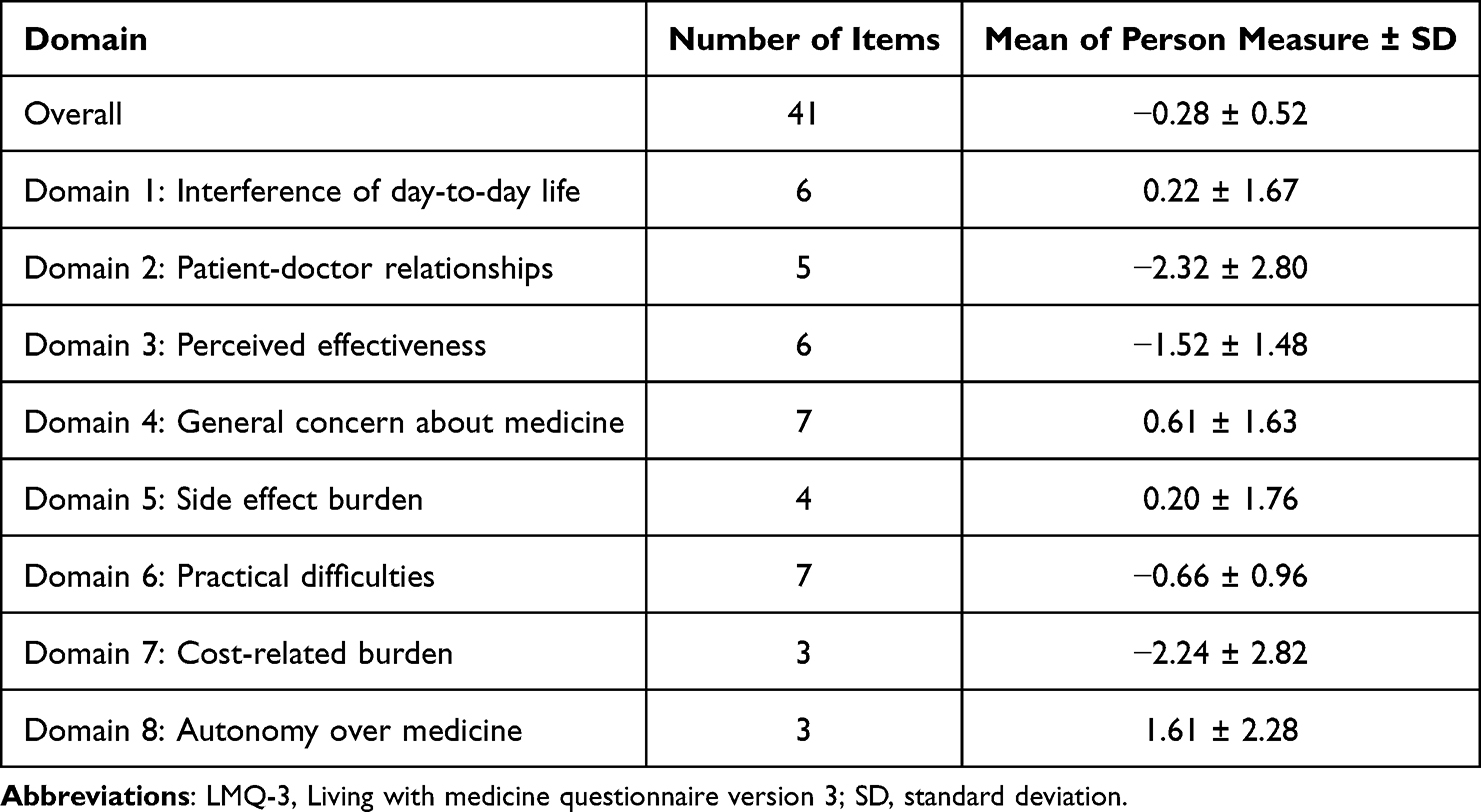 |
Table 3 Descriptive Statistics of LMQ-3 Result Person Measure |
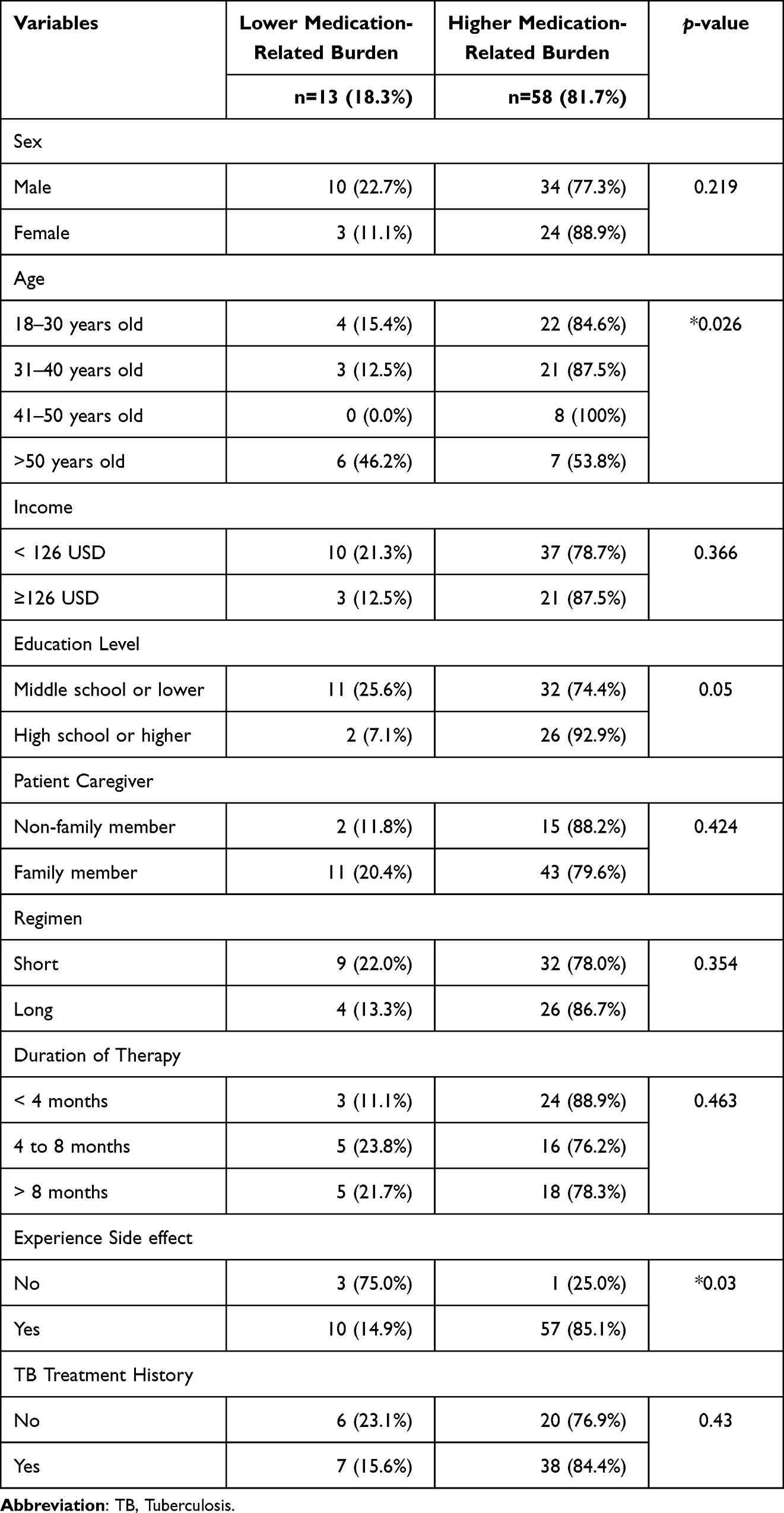 |
Table 4 Result of Bivariate Analysis Between Level of Medication-Related Burden with Sociodemographic and Clinical Characteristics Using Chi Square |
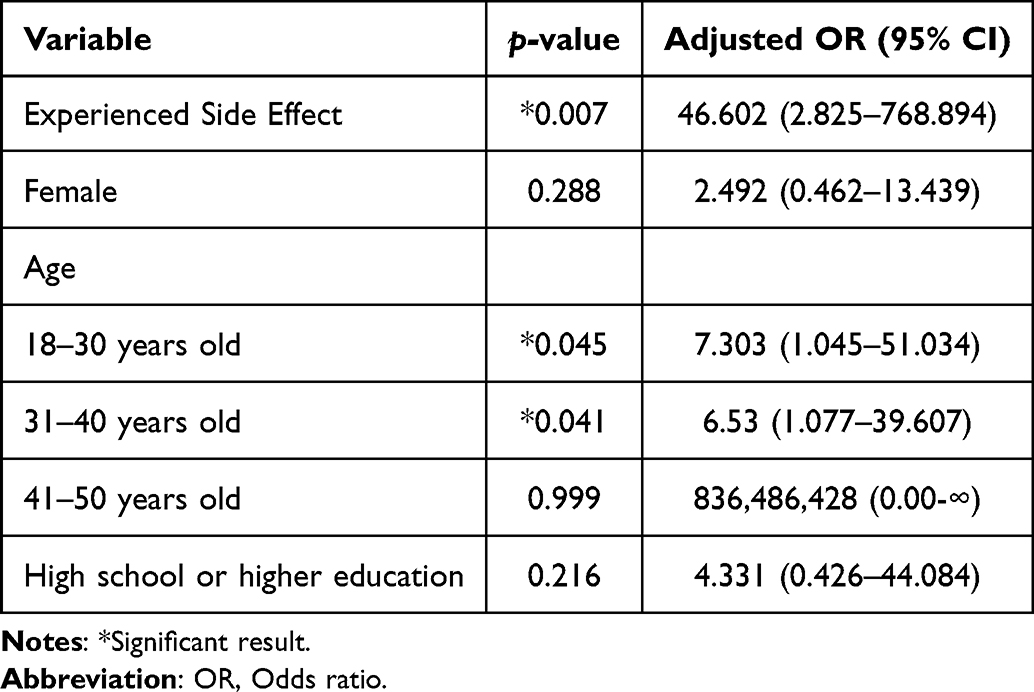 |
Table 5 Result of Multivariate Analysis Between Level of Medication-Related Burden and Sociodemographic and Clinical Characteristics Using Binary Logistic Regression |
Among the 8 domains in LMQ-3, domain 2 (patient-doctor relationships) had the lowest mean of person measure (see Table 3; Figure 2). This implies that the relationship with healthcare professionals induced a minimum burden compared with other domains. In contrast, domain 8 (lack of autonomy over medicine) had the highest mean of person measure, implying that a lack of autonomy toward medicine use was perceived as the most burdensome issue.
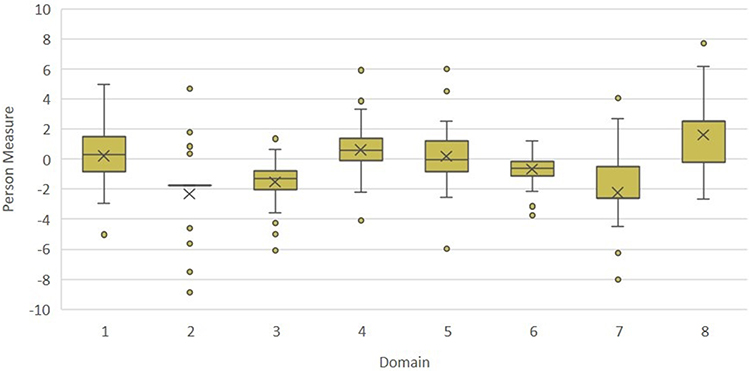 |
Figure 2 Person measure of medication-related burden which is assessed using Living with Medicine Questionnaire-3 (LMQ-3). Notes: outlier; Domain 1: Interference of day-to-day life; Domain 2: Patient-doctor relationships; Domain 3: Perceived effectiveness; Domain 4: General concern about medicine; Domain 5: Side effect burden; Domain 6: Practical difficulties; Domain 7: Cost-related burden; Domain 8: Autonomy over medicine. |
Discussion
This study found that medication induces multidimensional responses that are subjectively perceived by each patient. One issue may lead to or aggravate other issues. This corresponds with previous studies which suggest that medication-related burden is a complex phenomenon that involves different components and elements interacting with each other.7,15 The qualitative study helps in understanding the different components of patient concern and enables the caregiver to identify the personal burden to make a better approach. In contrast, more generalized issues can be better described with the quantitative method, which is valuable in formulating policies related to patient-centered care. Both methods contribute to identifying any burdens that may interrupt optimal health outcomes.16
The treatment regimen was perceived as the most dominant burden, related to the characteristics of the medicine package and the rules of MDR-TB therapy, which were complex, and strict. Similarly, autonomy over medicine domain showed the highest mean measure, which indicated there were an issue about patient’s control of medicine dose and schedule that affects patients overall. One of the most complained-about problems was side effects. Not surprisingly, the presence of side effects also showed a significant association with the severity of medication-related burden in quantitative analysis. It is known that the MDR-TB regimen causes various side effects, ranging from mild to those that cause disability and threaten life.17,18 Consequently, patients lost their daily functionality and social interaction. The results of this study correspond with a previous study that found adverse reactions or side effects of drug-resistant TB medications are associated with the quality of life of patients.19,20 For example, vomiting, as one of the most frequent side effects, not only caused discomfort but also potentially reduced the drug dose taken by the patients.
Personal belief represents individual internal factors. Treatment expectation depends on treatment experiences,21,22 verbal suggestions,22 and the learning process.22,23 This study shows that the experience of treatment constructs specific ideas about the medication. These ideas might generate a belief that controls their reaction toward therapy. For example, side effects may emerge before taking medicine, which are called anticipatory symptoms. The symptoms of side effects sometimes also occur when patients think about taking medication, which is called associative symptoms. Restlessness and feeling of distress sometimes arise before taking drugs and are called behavioral symptoms.24 However, these anticipatory, associative, and behavioral symptoms are not clinically evident. Yet, they are burdensome and make patients avoid therapy.25
A solid cultural factor also contributed to how patients avoid undesirable effects. Some people tried to seek another option of therapy instead of conventional medicine. Alternative therapy and traditional remedies are popular in Indonesia. People believe that conventional synthetic medicine treatment causes more side effects and leads to drug dependence than alternative therapy or traditional medications.9
Socioeconomic burdens represented workloads regarding their economic condition and social functioning. TB medication side effects made patients feel isolated due to the decline in their social function.26 In terms of finances, patients found constraints because they still had to pay several indirect costs in addition to medical expenses covered by national health insurance. Besides, patients are more likely to suffer income loss in this condition. This gap results in a substantial financial burden on the patient. The quantitative finding showed an association between age and burden level. It may be because different age groups perceive diverse perceptions of health.27,28 The burden of illness and medicine in MDR-TB also resulted in economic and social dependence. Consequently, the family also experiences the caregiver burden of MDR-TB therapy.
Healthcare-related burdens arise from frequent visits to healthcare facilities. Patients expect convenient and accessible services. This finding implies that the role of healthcare professionals matters a lot, either in providing appropriate treatment or in giving emotional support to patients.
Healthcare professionals are supposed to provide responsive care and respect patients as whole persons with multidimensional needs and values.29,30 A pharmacist is a healthcare professional with extensive knowledge and skills in clinical medication management.31 Since medicine use seems to be one of the major concerns of tuberculosis, pharmacists hold the potential to contribute to overcoming the medication-related burden.32–34 Intensive monitoring, counseling, and education about the disease, appropriate drug use, management of side effects, and medication therapy reviews are needed.34–37 These measures may increase self-efficacy and awareness of the severity and susceptibility of diseases. Information about side effects should be communicated with positive framing, by avoiding negative verbal suggestions.38
The ability of patients to bear workloads depended on their perception. The health belief model (HBM) explains the reasons for patients’ health behaviors that primarily arise from their health perceptions.36 When the perceived benefits outweigh the burdens, patients will continue adhering to treatment regardless of the burdens. In addition, the HBM explains that awareness about the risk of severity and susceptibility to diseases, self-efficacy, and specific cues that trigger better health behavior also matter.39,40 Therefore, assistance from a healthcare professional is recommended by providing patient-centered care, educational support, and psychological intervention.41 Psychological interventions, such as cognitive-behavioral therapy, were also recommended as non-pharmacological interventions.42 There are three domains as modifiable targets of psychological intervention: (1) knowledge, beliefs, and related cognitive constructs; (2) emotional distress and well-being; and (3) behavioral skills and coping.43
Moreover, patients also need support from family and the community. The family, as caregivers, supervises medication, and encourages patients. Peers and the TB survivor community may also provide support.44,45 This approach may create a sentimental attachment and give hope to patients. Finally, financial support from the government may be a solution to relieving the burden, especially in low-, and middle-income countries.
Limitations of this study were as follows: (1) The one-month total sampling technique, while time saving, may limit the generalizability of the data, and (2) there was no comparison of drug-sensitive TB (DS TB) patients to confirm the severity of burden in MDR-TB care. Further research is required to analyse and provide a more comprehensive understanding of the condition of MDR-TB patients compared to DS TB patients.
Conclusion
In qualitative section, side effect was identified as the major concern of the treatment. Similarly, in quantitative section, presence of side effect and younger age were associated with higher burden. Based on joint analysis, regimen-related burden was inferred as the most common issue observed in MDR-TB patients. By understanding perspective of patient, healthcare professionals are expected to provide tailored care to alleviate burdens. The findings about the burden of medication side effects also highlight the necessity for more tolerable MDR-TB medication. An extensive quantitative study over extended period will enable more findings.
Ethical Clearance
Procedure of this study has been approved by Research Ethics Committee of Universitas Padjadjaran, Bandung with approval number 20/UN6.KEP/EC/2021. This research conformed to ethical principles for research involving human subjects based on Declaration of Helsinki, include respect for persons, principle of beneficence, and principle of justice. Participant gave informed consent for data collection, questionnaire filling (for quantitative study participants), audio recording (for qualitative study participants), and publication of their response (including anonymized quote).
Acknowledgments
The authors appreciate the valuable contribution from staffs of MDR-TB Clinic of Hasan Sadikin General Hospital, Bandung, West Java, Indonesia in supporting this research.
Funding
This work was partially funded by USAID in Partnerships for Enhanced Engagement in Research (PEER) Program for MIB (Federal Award Identification Number [FAIN]: AID-OAA-A-11-00012) and Grant-in Aids from Universitas Padjadjaran (Academic Leadership Grant, grant number: 3855/UN.C/LT/2019) for RR.
Disclosure
The authors report no competing interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2023; 2023.
2. World Health Organization. Global Tuberculosis Report 2020. World Health Organization; 2020.
3. Gallacher K, May CR, Montori VM, Mair FS. Understanding patients’ experiences of treatment burden in chronic heart failure using normalization process theory. Ann Fam Med. 2011;9(3):200–204. doi:10.1017/S1359135513000031
4. Katusiime B, Corlett S, Reeve J, Krska J. Measuring medicine-related experiences from the patient perspective: a systematic review. Patient Relat Outcome Meas. 2016;7:157–171. doi:10.2147/prom.s102198
5. Sav A, King MA, Whitty JA, et al. Burden of treatment for chronic illness: a concept analysis and review of the literature. Health Expectations. 2015;18(3):312–324. doi:10.1111/hex.12046
6. Ausi Y, Santoso P, Sunjaya DK, Barliana MI. Between curing and torturing: burden of adverse reaction in drug-resistant tuberculosis therapy. Patient Prefer Adherence. 2021;15:2597–2607. doi:10.2147/PPA.S333111
7. Rosbach M, Andersen JS. Patient-experienced burden of treatment in patients with multimorbidity – a systematic review of qualitative data. PLoS One. 2017;12(6):1–18. doi:10.1371/journal.pone.0179916
8. World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care. World Health Organization (WHO); 2017.
9. Widayanti AW, Green JA, Heydon S, Norris P. Health-seeking behavior of people in Indonesia: a narrative review. J Epidemiol Glob Health. 2020;10(1):6. doi:10.2991/JEGH.K.200102.001
10. Creswell J, Clark P. Designing and Conducting Mixed Methods Research. VI. Sage; 2007.
11. Daundasekara SS, Arlinghaus KR, Johnston CA. Quality of life: the primary goal of lifestyle intervention. Am J Lifestyle Med. 2020;14(3):267–270. doi:10.1177/1559827620907309
12. Krska J, Morecroft CW, Poole H, Rowe PH. Issues potentially affecting quality of life arising from long-term medicines use: a qualitative study. Int J Clin Pharm. 2013;35(6):1161–1169. doi:10.1007/s11096-013-9841-5
13. Krska J, Katusiime B, Corlett SA. Validation of an instrument to measure patients’ experiences of medicine use: the living with medicines questionnaire. Patient Prefer Adherence. 2017;11:671–679. doi:10.2147/PPA.S126647
14. Katusiime B, Corlett S, Krska J. Development and validation of a revised instrument to measure burden of long-term medicines use: the living with medicines questionnaire version 3. Patient Relat Outcome Meas. 2018;9:155–168. doi:10.2147/prom.s151143
15. Mohammed MA, Moles RJ, Chen TF. Medication-related burden and patients’ lived experience with medicine: a systematic review and metasynthesis of qualitative studies. BMJ Open. 2016;6(2):e010035. doi:10.1136/bmjopen-2015-010035
16. Awad A, Alhadab A, Albassam A. Medication-related burden and medication adherence among geriatric patients in Kuwait: a cross-sectional study. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.01296
17. Schnippel K, Firnhaber C, Berhanu R, Page-Shipp L, Sinanovic E. Adverse drug reactions during drug-resistant TB treatment in high HIV prevalence settings: a systematic review and meta-analysis. J Antimicrob Chemother. 2017;72(7):1871–1879. doi:10.1093/jac/dkx107
18. Schnippel K, Berhanu RH, Black A, et al. Severe adverse events during second-line tuberculosis treatment in the context of high HIV co-infection in South Africa: a retrospective cohort study. BMC Infect Dis. 2016;16(1):1–10. doi:10.1186/s12879-016-1933-0
19. Sineke T, Evans D, Schnippel K, et al. The impact of adverse events on health-related quality of life among patients receiving treatment for drug-resistant tuberculosis in Johannesburg, South Africa. Health Qual Life Outcom. 2019;17(1). doi:10.1186/S12955-019-1155-4
20. Valadares RMC, Carvalho WS, de Miranda SS. Association of adverse drug reaction to anti-tuberculosis medication with quality of life in patients in a tertiary referral hospital. Rev Soc Bras Med Trop. 2019;53. doi:10.1590/0037-8682-0207-2019
21. Finniss DG, Kaptchuk TJ, Miller F, Benedetti F. Biological, clinical, and ethical advances of placebo effects. Lancet. 2010;375(9715):686–695. doi:10.1016/S0140-6736(09)61706-2
22. Webster RK, Weinman J, James Rubin G. A systematic review of factors that contribute to nocebo effects. Health Psychol. 2016;35(12):1334–1355. doi:10.1037/hea0000416
23. Faasse K, Petrie KJ. The nocebo effect: patient expectations and medication side effects. Postgrad Med J. 2013;89(1055):540–546. doi:10.1136/postgradmedj-2012-131730
24. Amaral JM, Brito MJM, Kakehasi AM. High frequency of methotrexate intolerance in longstanding rheumatoid arthritis: using the methotrexate intolerance severity score (MISS). Adv Rheumatol. 2020;60(1). doi:10.1186/s42358-020-00145-5
25. Bulatovic M, Heijstek MW, Verkaaik, M et al. High prevalence of methotrexate intolerance in juvenile idiopathic arthritis: development and validation of a methotrexate intolerance severity score. Arthritis Rheum. 2011,07;63(7):2007–2013. doi:10.1002/art.30367
26. Roba AA, Dasa TT, Weldegebreal F, et al. Tuberculosis patients are physically challenged and socially isolated: a mixed methods case-control study of health related quality of life in eastern Ethiopia. PLoS One. 2018;13(10):1–14. doi:10.1371/journal.pone.0204697
27. Silva AF, Cancela JM, Mollinedo I, Camões M, Bezerra P. The relationship between health perception and health predictors among the elderly across European countries. Int J Environ Res Public Health. 2021;18(8):4053. doi:10.3390/ijerph18084053
28. Sunjaya DK, Paskaria C, Pramayanti M, Herawati DMD, Parwati I. The magnitude of anxiety and depressive symptoms among tuberculosis patients in community health centers setting during the peak of COVID-19 pandemic. J Multidiscip Healthc. 2022;15:755–764. doi:10.2147/JMDH.S359530
29. Epstein RM, Street RL. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100. doi:10.1370/AFM.1239
30. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. 2019;19(1):1–9. doi:10.1186/S12913-018-3818-Y/TABLES/5
31. Jacobi J. Clinical pharmacists: practitioners who are essential members of your clinical care team. Med Clin Condes. 2016;27(5):571–577.
32. Karuniawati H, Putra ON, Wikantyasning ER. Impact of pharmacist counseling and leaflet on the adherence of pulmonary tuberculosis patients in lungs hospital in Indonesia. Indian J Tuberc. 2019;66(3):364–369. doi:10.1016/j.ijtb.2019.02.015
33. Miller R, Goodman C. Quality of tuberculosis care by pharmacies in low- and middle-income countries: gaps and opportunities. J Clin Tuberc Other Mycobact Dis. 2020;18. doi:10.1016/j.jctube.2019.100135
34. Wong YJ, Ng KY, Lee SWH. Community pharmacists-led interventions in tuberculosis care: a systematic review. Res Social Adm Pharm. 2022;19(1):5–15. doi:10.1016/J.SAPHARM.2022.09.001
35. Sanchez-Padilla E, Marquer C, Kalon S, et al. Reasons for defaulting from drug-resistant tuberculosis treatment in Armenia: a quantitative and qualitative study. Int J Tuberc Lung Dis. 2014;18(2):160–167. doi:10.5588/ijtld.13.0369
36. Tola HH, Karimi M, Yekaninejad MS. Effects of sociodemographic characteristics and patients’ health beliefs on tuberculosis treatment adherence in Ethiopia: a structural equation modelling approach. Infect Dis Poverty. 2017;6(1):1–10. doi:10.1186/s40249-017-0380-5
37. Toni J, Lipovec NC, Sorli PS, Kosnik M. Pharmacist’s role in the treatment of patients with tuberculosis ñ our positive experience. Eur J Hosp Pharm. 2012;19(2):250. doi:10.1136/EJHPHARM-2012-000074.433
38. Wilhelm M, Rief W, Doering BK. Decreasing the burden of side effects through positive message framing: an experimental proof-of-concept study. Int J Behav Med. 2018;25(4):381–389. doi:10.1007/S12529-018-9726-Z
39. Gebremariam RB, Wolde M, Beyene A. Determinants of adherence to anti-TB treatment and associated factors among adult TB patients in Gondar city administration, Northwest, Ethiopia: based on health belief model perspective. J Health Popul Nutr. 2021;40(1):1–10. doi:10.1186/S41043-021-00275-6/TABLES/3
40. Parwati NM, Bakta IM, Januraga PP, Wirawan IMA. A health belief model-based motivational interviewing for medication adherence and treatment success in pulmonary tuberculosis patients. Int J Environ Res Public Health. 2021;18(24):13238. doi:10.3390/ijerph182413238
41. Tola HH, Shojaeizadeh D, Tol A, et al. Psychological and educational intervention to improve tuberculosis treatment adherence in Ethiopia based on health belief model: a cluster randomized control trial. PLoS One. 2016;11(5):1–15. doi:10.1371/journal.pone.0155147
42. Zuo X, Dong Z, Zhang P, et al. Cognitive-behavioral therapy on psychological stress and quality of life in subjects with pulmonary tuberculosis: a community-based cluster randomized controlled trial. BMC Public Health. 2022;22(1). doi:10.1186/s12889-022-14631-6
43. Gonzalez JS, Tanenbaum ML, Commissariat PV. Psychosocial factors in medication adherence and diabetes self-management: implications for research and practice. American Psychologist. 2016;71(7):539–551. doi:10.1037/a0040388
44. Bastard M, Sanchez-padilla E, Hewison C, et al. Effects of treatment interruption patterns on treatment success among patients with multidrug-resistant tuberculosis in Armenia and Abkhazia. J Infect Dis. 2015;211(10):1607–1615. doi:10.1093/infdis/jiu551
45. Deshmukh RD, Dhande DJ, Sachdeva KS, Sreenivas AN, Kumar AMV, Parmar M. Social support a key factor for adherence to multidrug-resistant tuberculosis treatment. Indian J Tuberc. 2018;65(1):41–47. doi:10.1016/j.ijtb.2017.05.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.