Back to Archived Journals » Clinical Audit » Volume 12
A Minor Eye Conditions Pilot Delivered by Community Optometrists
Received 13 December 2019
Accepted for publication 20 February 2020
Published 9 March 2020 Volume 2020:12 Pages 1—9
DOI https://doi.org/10.2147/CA.S242091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zoka Milan
David Hill,1 Inderaj Hanspal2
1Suffolk Local Optical Committee, Newmarket, UK; 2Department of Ophthalmology, West Suffolk Hospital, Bury St Edmunds, UK
Correspondence: David Hill Email [email protected]
Purpose: To determine the viability of an optometry-led community eye care scheme.
Methods: Pilot study. Assessment of examination reports and patient feedback collected from six community optometry practices in West Suffolk over a 3-month period. A patient satisfaction questionnaire was given to each patient using the service. The entry route, outcomes and appropriateness of referrals to secondary care were assessed.
Results: A total of 299 patients accessed the scheme. The optometrist managed eighty-one per cent of cases without a referral. 16% were referred to ophthalmology secondary care, of which 79% were deemed appropriate. The most frequently presenting conditions were related to the anterior eye (70%). 23% presented with recent onset flashes or floaters. Antibiotics were recommended in 7% of cases and lubricants in 30%. Patient satisfaction information was available for 75% of episodes. All agreed it was convenient to be seen in their local community, 95% were very confident in the optometrist, and 95% rated overall satisfaction as excellent.
Conclusion: A community eye care scheme can benefit the patient, the NHS and the optometrist. Not only are financial savings likely to be made, but secondary care capacity is also increased. Several of the NHS key drivers; including the time to care and care closer to home are met.
Keywords: optometrist, eye care, MECS, primary care
Introduction
In the UK, optometrists provide routine sight testing either privately or free for those eligible through General Ophthalmic Services (GOS). Over the last decade, numerous enhanced optometric schemes (EOS) have been commissioned with the primary aim of reducing the burden on secondary care, general practice (GP) and accident and emergency departments. The need has been driven by the critical situation some ophthalmology departments find themselves in. This is a result of the ageing demographic and increased number of chronic conditions requiring ongoing care.1,2 These schemes, most commonly referred to as MECS (minor eye conditions scheme) have been facilitated by changes in the optician’s act. The refinements to the act allow optometrists to manage patients with an ocular disease rather than having to refer.3 The current insufficiency in the number of ophthalmologists and increasing use of technology in ophthalmology means re-thinking of working practices is needed to prevent avoidable sight loss from delayed care.1,4 Just under two million referrals were received by ophthalmology in the year 2016/17,5 with three out of ten referrals being discharged at the first visit.6 GOS is designed for routine eye examinations and refractive problems. It is not appropriate for many eye problems such as a red or painful eye.7 An EOS provides a focused NHS funded appointment where the presenting problem can be thoroughly investigated and then managed. Management may include treatment or referral to the patient’s GP or ophthalmology. It has been shown referrals following an EOS appointment are of a higher quality8,9 facilitating appropriate triage in terms of clinic allocation and urgency in secondary care.
Despite the number of EOS schemes that have been commissioned reports of the various outcomes are few. This pilot study aimed to determine the types of conditions that would present, the number of patients retained in primary care, and patient opinion about being seen in the community. The pilot was a joint enterprise between West Suffolk clinical commissioning group (CCG), West Suffolk Hospital Trust and Suffolk Local Optometric Committee (LOC).
Methods
The pilot ran for three months from December 2018 using the 100-day methodology. This method is described elsewhere;4,10 but briefly, the aim is to provide a route to rapid change with tangible benefits utilising an approach which is good enough. After a short period of planning the service is launched with regular review before stopping after 100 days. At this point, the data is analysed, the outcomes assessed against the objectives, before deciding whether to continue the service. This approach has been used in several medical specialities.11–13 Six optometry practices within West Suffolk CCG participated. All the practitioners had expressed an interest in enhanced services and were known to the overseeing ophthalmologist. The optometrists met to discuss the protocol, which was based on the local optometric committee support unit (LOCSU) MECS pathway.14 The optometrists had previously completed the Welsh Optometric Postgraduate Education Centre (WOPEC) MECS training. This consists of distance learning modules and a practical examination.
Patients accessed the scheme by one of four routes: GP referral, care navigator signposting, pharmacy signposting or walk-in (direct access). The GP practices in the CCG area were informed about the pilot through CCG communications or by one of the pilot optometrists. A leaflet explaining the scheme was supplied to GP practices and several pharmacies in the area. At the first contact, the pilot practice completed a triage form to determine the suitability for a MECS appointment and the urgency they needed to be seen. The urgency was either within 24 hrs or 7 days. If the practice could not offer an appointment in an appropriate time frame, the practice would contact one of the other pilot practices. For those patients seen in the pilot, a report was completed in addition to the patient record. The report included patient demographic information (age and gender), triage information, presenting symptoms, tests conducted, and management. Management included treatment by the optometrist and referral either to ophthalmology or to the patients GP. The completed report was sent to the patients GP and an anonymised copy to the local optometric committee for audit purposes. On the advice of the association of optometrists (AOP), only the tests appropriate for the presenting problem were performed rather than a full sight test routine. It was made clear to the patient the EOS appointment was not a replacement for a sight test. The appropriateness of referrals to the hospital eye service (HES) was assessed by an ophthalmologist (IH) and optometrist (DH). A referral was considered inappropriate if the patient was discharged at the first visit with no treatment, and the ophthalmologist found no other reason warranting the referral. Others have considered the referral appropriateness in terms of the urgency.21 The HES outcome was checked for each referral received by the hospital and compared to the provisional diagnosis recorded by the optometrist. Patient satisfaction was assessed through a short questionnaire. This was completed before the patient left the practice. The questionnaire consisted of seven questions and a free text box. The reports were assessed by one of the pilot optometrists with the measures being entered into an excel spreadsheet (Microsoft, Washington, USA) for analysis.
No formal ethical approvals were required with this being a service evaluation pilot in collaboration with West Suffolk clinical commissioning group. The authors used pre-collected data that were analysed retrospectively. The audit, however, was carried out in accordance with the declaration of Helsinki. Participating optometrists gave written consent.
Results
During the study, two hundred and ninety-nine episodes were reported from the six pilot practices. The mean age was 51 years SD±22 with a range between 2 and 93 years. Sixty-one per cent (182) were female, and 39% (117) male (Figure 1). Information on ethnicity and socioeconomic status were not collected.
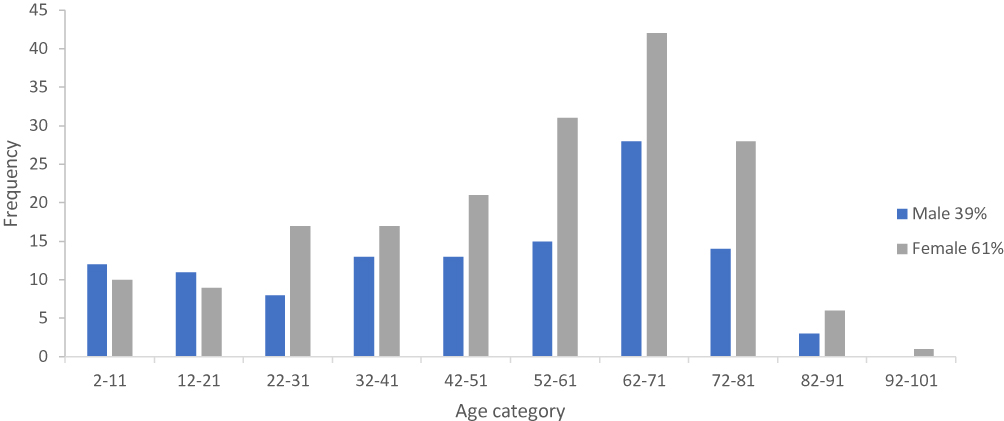 |
Figure 1 Frequency of those using the service by age category (n=299). |
Access to the Service
Four points of access were included in the pilot (Figure 2A). There was an even split between patients walking into a pilot practice and those being directed by some other healthcare worker. Sub-analysis showed the practices that engaged the local GP’s early in the pilot had a greater proportion of patients (70%) entering the scheme directed from the GP or by the practice care navigator. Each patient was triaged at the optical practice to determine the type of appointment needed, ie Full Eye Examination (Sight Test) or EOS, and the urgency. 86% of patients were seen on the day of the first contact, although only 61% were determined to need a same-day appointment (Figure 2B).
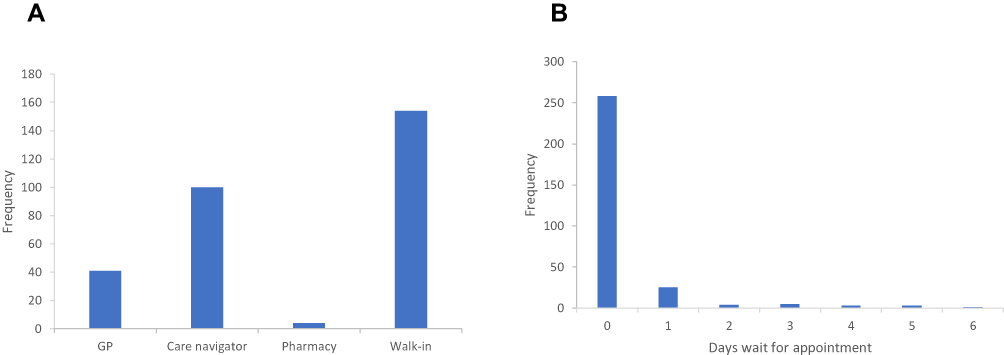 |
Figure 2 (A) Route of entry to the service. (B) shows the time between first contact and the consultation (n=299). |
Main Outcomes
One hundred and ninety-eight (66%) were seen, treated and discharged after one appointment with a further 44 (15%) being reviewed before discharge. Out of those reviewed, 78% were seen in person, and 22% reviewed by phone. Fifty-seven (19%) were referred on for further care (Figure 3A). A third of the referrals were classed as acute and sent via the on-call ophthalmologist or direct to a specialist centre (Figure 3B). Eight patients were referred to their GP.
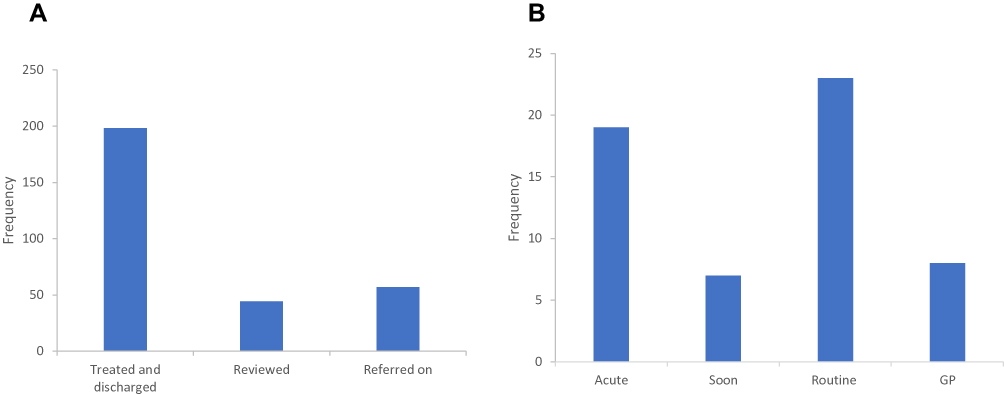 |
Figure 3 (A) shows the outcomes of the consultation (n=299). (B) shows the referral rates and pathway selected (n=57). |
A wide range of conditions, from minor to potentially sight-threatening, presented for EOS appointments. The most common presenting problems were related to the anterior eye (210 cases). Flashes and floaters accounted for 24% (70) of cases. Eight of these were reported to be visual migraine, and two were found to have macula-on retinal detachments. Several other cases with potentially sight-threatening conditions were seen; these included a case of acute angle-closure glaucoma, four cases of iritis and four corneal ulcers (Table 1).
 |
Table 1 Frequency of Conditions Presenting, Number Sent from GP Practice, Number Managed by the Optometrist and the Amount Sent to Ophthalmology |
One hundred and twelve cases (38%) were recommended eye drops. The majority (90 cases) were advised to use lubricants. Topical antibiotics were prescribed in twenty cases (7%), and one prescription for an oral antibiotic was issued. Anti-allergy drops (Sodium cromoglycate) were suggested in four cases. The GP was asked to issue an NHS prescription for the medication in 12 cases (10% of cases requiring the treatment); only one case was for a drug unavailable for entry level optometrists. In the remaining cases, the patient was directed to purchase the drops. Forty-nine patients were sent to secondary care (ophthalmology). The referral to secondary care was assessed to be appropriate in 78.7% of cases. Those classed as inappropriate were mainly cases of posterior vitreous detachment in which dilated in-direct fundus examination revelled no Schaefer’s sign or retinal tears. The patients had been counselled, and referred to secondary care for a further check, which was deemed unnecessary. The other case was dry eye-related where the optometrist had advised lubricants; however, the patient was still not satisfied. The hospital supplied lubricants and advice in this case. Where the optometrist had provided a provisional diagnosis, this agreed with the hospital diagnosis in 96% of cases. If the four cases that the optometrist marked as unknown, but the hospital assigned a diagnosis, were included the agreement was 88%.
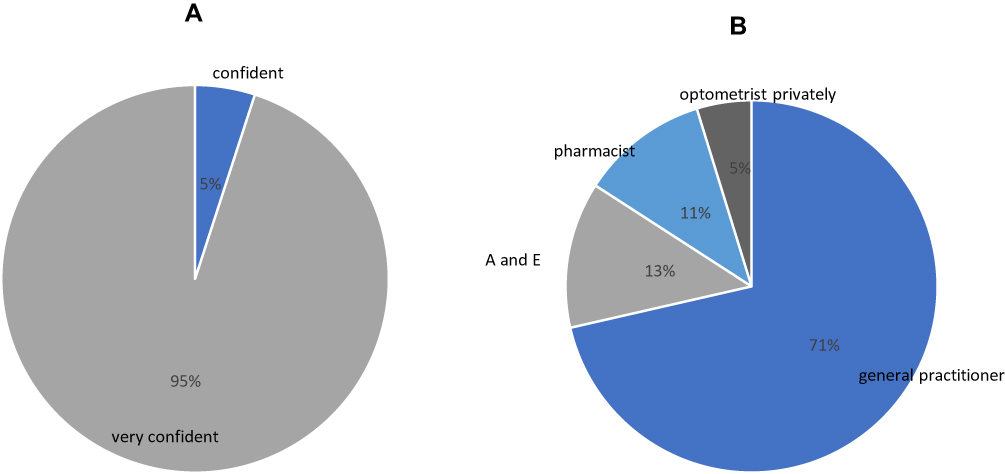 |
Figure 4 (A) shows the rating of confidence in the optometrist following the consultation. (B) shows where the patient would have sought help if the scheme were not available (n=223). |
User Feedback
Feedback was received in 223 (75%) cases. The feedback was extremely positive for all seven measures, especially in terms of the short wait times. All respondents found it convenient to be seen within their local community, with 95% rating their overall experience as excellent. When the patient’s confidence in the optometrist was assessed, 95% reported they were very confident, and the remaining 5 % scored the rating as confident (Figure 4A).
The final question enquired as to what the patient would have done if this service was not available. The majority (71%) said they would see their GP, and 13% would self-refer to A and E. No respondents said they would do nothing (Figure 4B). The pilot optometrists completed a short survey. Five out of 6 pilot optometrists stated they were a little out of their comfort zone. The time needed to see a patient varied with an average of 25 mins. Completing the report was the most onerous aspect.
Discussion
The aim of the West Suffolk community eye care pilot study was to investigate how both referrals to ophthalmology and the burden on GP time could be reduced. The types of conditions presenting and how these were managed by the optometrist was assessed, in addition to evaluation of patient feedback on being seen in the community.
Access to the Scheme
The 299 patients accessed the scheme through two main routes; either directed by some other healthcare worker or as a walk-in to the optometric practice. The Welsh PEARS (primary eyecare acute referral scheme) scheme initially was a second opinion service for patients that had been seen by the GP as an alternative to referring directly to secondary care. Subsequently, it was expanded to include a walk-in option. Most existing schemes have included the access points used in this pilot with the addition of accident and emergency and 111 signposting to the MECS practitioner. In the practices where the GP practice manager was engaged, the care navigator became the most significant source of patients. This saves GP time, in terms of appointments and time that may have been spent speaking to the on-call ophthalmologist or following up eye problems. Many anterior eye conditions require multiple appointments either to review progress or when the first remedy fails to resolve the issue. However, using the care navigator could make imposing inclusions and exclusions more complicated. Not all pilot practices felt comfortable promoting the scheme for fear of being overrun with patients; this limited our ability to assess demand fully. The patient questionnaire asked, “where would you have gone if the scheme were not available”, the GP was overwhelmingly the first choice. This agrees with a report assessing the public’s perception of the optical profession.15 It has been reported that GP’s are not always confident in dealing with eye problems and welcome the support of an expert.16,17
Demographic Information
More females accessed the scheme in all but the youngest age categories. It is known females attend routine healthcare appointments more often.18 The males in the younger groups are likely to still be under their parent’s care. MECS is appropriate for recent-onset conditions, so with men being more likely to suffer minor eye injuries,19 the female bias was unexpected. If public knowledge of MECS is increased, more men may use this source of care given the convenience in terms of location and wait time. No minimum age was specified for the pilot. The youngest seen was two years of age. Several schemes exclude those under sixteen years of age, whereas others have a lower age limit of 7 years. The eight children younger than age seven in our pilot all had anterior eye conditions and just needed advice and reassurance. Two-thirds of this young group had been signposted from the GP practice. This group may be more suited to management outside a MECS.
Main Outcomes
As a result of how the pilot practices scheduled MECS appointments, 86% of patients were seen on the day of presentation. From the triage, 61% were deemed to require a same-day appointment. As a MECS scheme is not an emergency eye care service, this would seem high. However, optometrists are known to be a cautious profession.20 The optometrist managed eighty-one per cent of presenting cases in-house. This is in concordance with other enhanced service schemes that have been audited.8,21–23 A larger pilot in Lambeth and Lewisham ran for two years with 2123 episodes in the analysis. They reported 64% were managed by the optometrist and discharged after one visit, with a further 10% being discharged following a second appointment.21 This agrees with our follow up rate. In our study, the follow up was conducted face to face (78%) or over the phone (22%). As the pilot went on, fewer patients were followed up in person. This change in behaviour may be explained firstly by the increasing confidence of the optometrist; secondly, when the patient’s complaint had resolved, they tended not to attend scheduled follow up appointments. Those followed up were mainly cases with corneal trauma.
Minor eye care schemes have been running in some parts of the country for several years. Our rates of onward referral were like previous reports.21,23 The referral rate following a sight test is stated to be approximately 3%,5 whereas most MECS have onward referral rates of around 20% (Table 2). Patients seen in a MECS are at greater risk so that a higher referral rate would be expected.8 Eight patients were referred to their GP for blood glucose tests or further investigation of migraines.
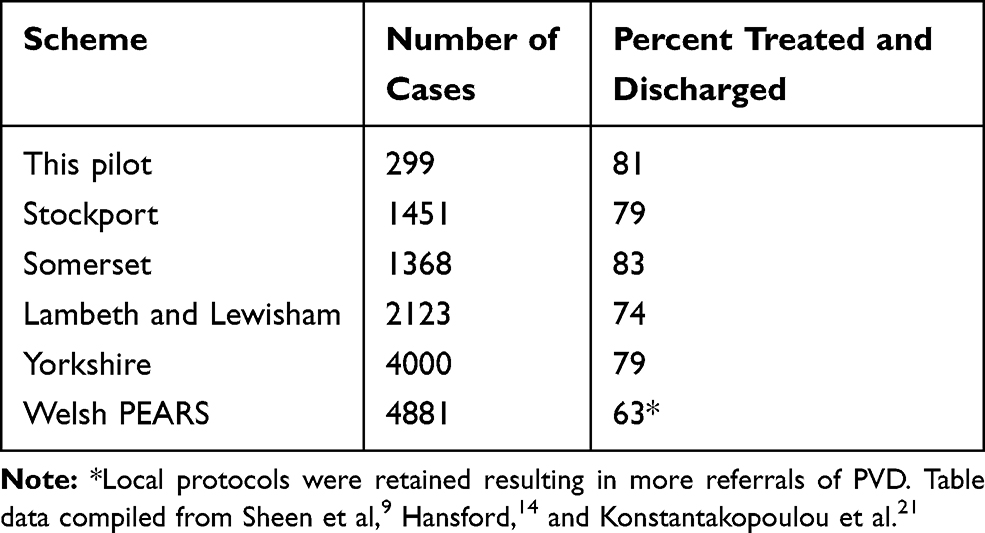 |
Table 2 Outcomes of Other Community Eye Care Scheme |
Anterior eye conditions accounted for most cases seen during the pilot. Previous referral audits have shown that ophthalmology referrals from GP’s mainly concerned the anterior eye, while those from optometrists were for conditions affecting the posterior segment.24 Due to the pilot only running during the winter months the number of allergic eye problems was low. Recent onset flashes and floaters were the presenting symptoms in seventy cases (23%) with most (68%) being managed and discharged by the optometrist. This symptom carries a risk of visual loss from retinal detachment. Most of the patients with this symptom were diagnosed as having a PVD. This symptom would appear an appropriate use of a MECS appointment. The tailored appointment allows the optometrist to focus on the key examinations, with time for counselling, to facilitate the patient’s appreciation of symptoms should a retinal tear form in subsequent weeks. When the appropriateness of onward referral was assessed, PVD resulted in all but one of the referrals classed as inappropriate. This may be a result of it being difficult to be certain there is no tear and the perceived consequences of missing a tear. Referrals of these patients with no significant risk factors or signs suggestive of a retinal tear are likely to result in wasted eye clinic time, and it may be better for these patients to be followed up in the MECS practice. No payment was made for follow up in the pilot; although, it was most likely the lack of local training and clear protocols that resulted in the optometrists referring these cases to secondary care.
Lubricants and advice were the mainstays of treatment for the 81% managed by the optometrist. Time spent educating the patient about their condition and the various non-pharmacological management options can result in a better outcome and promotes future self-care.25 It has been reported that patients are happy to receive advice and would indeed be glad to pay £22 for the advice,26 although this conflicts with a small needs assessment pilot in Yorkshire where 12% of patients declined the service due to the charge.22 Antibiotics were advised by the optometrist in 21 cases. An audit of an anterior eye scheme involving GP’s and community optometrists found the GP to prescribe antibiotics in 70% of cases, while the optometrists prescribed in 35% of cases, in a similar case mix.27 This may be due to GP practices not having the appropriate equipment to make an accurate diagnosis or patient pressure to prescribe. This behaviour by optometrists, recently reinforced by the college of optometrists,28 also fits well with the NHS England public health message to minimise antibiotic use.29 By promoting non-pharmacological advice and self-purchase of eye drops a MECS could reduce the NHS drug bill. Drug costs account for 8% of the total NHS spend. From the 113 advised to use a topical eye drop, only 12 (10%) requested an NHS funded prescription; most were happy to purchase the drops. However, it is important that groups who are entitled to NHS medicines, especially those who may struggle to pay for medications are able to access free medicines in a way that is straightforward for all parties.
User Feedback
The patient experience questionnaire was completed for two-thirds of episodes. The feedback was generally positive. Patients stated that they had been either very confident or confident in the optometrist. In a report that considered the views of several stakeholders including patients, health professional, optometrists and commissioners, all were impressed by the level of care delivered by a MECS appointment and the way it streamlined the passage to secondary care.16
The six pilot practices found the scheme well received by patients. The time spent with the patient varied with presenting symptoms; however, all agreed the average was 25 mins. This would allow MECS appointments to fit in the usual scheduling of the standard optometric practice. The main concern of the pilot optometrists was the volume, and how to accommodate this into their clinic. All reported that more practices would need to sign up to spread the workload and to ensure a consistent level of service. Several of the pilot optometrists requested local protocols covering what should be referred, and what could be reviewed in practice. Despite the points raised all the optometrists said they would be keen to be involved in a future scheme to enhance their practice offering and personal job satisfaction.
The skills to safely see patients in a MECS are core optometry competency. Our pilot feedback indicated that the optometrist felt out of their comfort zone in many cases. Participating in a scheme exposes optometrists to a greater number of acute cases which may increase experience and skill. This should result in improved optometry to the benefit of patients and the NHS. In general, most MECS use WOPEC level 1 and 2 training in addition to local consultant led presentations. We would suggest that being part of a MECS is a continual enhancement of skills and relationships with other health care providers. Follow up training should support in other areas such as governance and public health, not just clinical skills. Other healthcare workers directing patients to a MECS practice need to be educated; any training needs to be concise in view of the demands on their time.
Strengths and Weaknesses
This 100-day pilot has several strengths, including ophthalmologist collaboration and some strong GP engagement. Despite the strengths, the small numbers of patients seen by some of the practices reduce the power of comparisons between practices. The decision not to collect information on ethnicity and social class restricts our ability to confirm equal access to the service. Inequality in Suffolk is low compared to other areas of the UK.30 Some of the pilot optometrists were reluctant to promote the scheme with their local GP’s for the fear of not being able to meet the demand. A full scheme would have more practitioners spreading the workload. A quantitative assessment of cost saving was not part of the pilot although others have shown savings when a MECS scheme is active.9,21
Summary and Conclusion
An eye care scheme negates the limitation of the NHS sight test by allowing the optometrist to spend time addressing the presenting problem rather than having to carry out a list of tests to satisfy the GOS terms of service. Access to an NHS Sight Test, for those eligible, is governed by the time since the previous examination, or symptoms related to vision. This means the optometrist is not permitted to see patients presenting with red-eye, or flashes and floaters for example, unless they are due their sight test appointment. When setting inclusions and exclusions, a blanket duration of symptoms as an access criterion would seem inappropriate. Some conditions such as flashes and floaters may have less significance with longer time since onset, whereas chronicity of an eyelid lump may indicate some more sinister condition. We would suggest a tighter inclusion criterion for walk-in patients compared to those signposted from another healthcare worker. Future care, with the shift to more efficient working practices using remote consultations either by phone or other visual technology could be used to follow up patients. Many patients presenting to the scheme do not need an appointment, but only advice; many are just seeking reassurance. The extra time in a MECS appointment should be used to promote self-care for reoccurrences. The pharmacist should be used as a cost-efficient expert as the first step but being aware of the pathways if red flags are identified.
In summary, a MECS may reduce costs in terms of medic time and drug costs. It meets the aims directly through patients being kept in primary care, more patient education to promote future self-care, short time to care and being seen closer to home. There are potential benefits in terms of better referrals and a reduction in false positives referrals to ophthalmology. Patients were highly satisfied with the service.
Abbreviations
AOP, Association of optometrists; CCG, Clinical commissioning group; EOS, Enhanced optical services; GOS, General ophthalmic services; GP, General practitioner; LOC, Local optometric committee; LOCSU, Local optical committee support unit; MECS, Minor eye conditions scheme; NHS, National health service; PVD, Posterior vitreous detachment; WOPEC, Welsh optometric postgraduate education centre.
Acknowledgment
Clare Jay for her support in starting the project and obtaining funding.
Disclosure
Dr David Hill reports that funding for the patient episodes was received from the NHS but no funding was used in the analysis of the data or the writing of this paper. A potential conflict of interest is that DH is an optometrist working in a practice that may benefit should a MECS be commissioned in the area. The authors report no other conflicts of interest in this work.
References
1. The Royal College of Ophthalmologists. The way forward; 2017. Available from: https://www.rcophth.ac.uk/standards-publications-research/the-way-forward/. Accessed March 3, 2020.
2. RNIB. The State of the Nation Eye Health 2017 A Year in Review; 2017. Available from: www.rnib.org.uk.
3. Council TGO. The opticians act. Rules relating to injury or disease of the eye; 1999. Available from: http://www.legislation.gov.uk/uksi/1999/3267/contents/made.
4. Nesta. Transforming elective care services ophthalmology; 2019. Available from: https://www.england.nhs.uk/publication/transforming-elective-care-services-ophthalmology/. Accessed March 3, 2020.
5. Davey CJ, Scally AJ, Green C, Mitchell ES, Elliott DB. Factors influencing accuracy of referral and the likelihood of false positive referral by optometrists in Bradford, United Kingdom. J Optom. 2016;9(3):158–165. doi:10.1016/j.optom.2015.10.007
6. Moorfields Eye Hospital NHS Foundation Trust. Moorfields Annual Report; 2017. Available from: https://www.moorfields.nhs.uk/content/annual-report-and-accounts-2016-17.
7. Optometrists A of. Making accurate claims in England; 2014. Available from: https://www.aop.org.uk/advice-and-support/regulation/england/making-accurate-claims.
8. Arbuthnot T. PEARS scheme in Wales: results of a practice self-audit. Optom Today. 2005;22–24.
9. Sheen NJL, Fone D, Phillips CJ, Sparrow JM, Pointer JS, Wild JM. Novel optometrist-led all Wales primary eye-care services: evaluation of a prospective case series. Br J Ophthalmol. 2009;93(4):435–438. doi:10.1136/bjo.2008.144329
10. NHS-England. 100 day challenge; 2018. Available from: www.england.nhs.uk/elective-care-transformation.
11. Lincolnshire-NHS-Trust. 100 day challenge for stroke services; 2019. Available from: https://www.lincolnshirecommunityhealthservices.nhs.uk/latest-news/lincolnshire-nhs-launches-100-day-challenge-stroke-services.
12. Doncaster-NHS-Trust. Urology pathway re-design; 2018. Available from: http:/www.doncasterccg.nhs.uk/your-care/planned-care/latest-100-day-challenge.
13. Mid-Essex-CCG. 100 day challenge-preventing admissions; 2016. Available from: https://midessexccg.nhs.uk/news/200-100-day-challenge.
14. Hansford L LOCSU MECS pathway; 2015. Available from: https://www.locsu.co.uk/commissioning/pathways/minor-eye-conditions-service.
15. The General Optical Council. Public perceptions of the optical industry; 2017. Available from: https://www.optical.org/download.cfm?docid=49A2AF49-8823-40A5.
16. Baker H, Harper RA, Edgar DF, Lawrenson JG. Multi-stakeholder perspectives of locally commissioned enhanced optometric services. BMJ Open. 2016;6(10):e011934. doi:10.1136/bmjopen-2016-011934
17. Teo MAL. Improving acute eye consultations in general practice: a practical approach. BMJ Qual Improv Rep. 2014. doi:10.1136/bmjquality.u206617.w2852
18. Verbrugge LM. Sex differentials in health. Public Health Rep. 1982;97(5):417–437.
19. Macewen CJ. Eye injuries: a prospective survey of 5671 cases. Br J Ophthalmol. 1989;73:888–894. doi:10.1136/bjo.73.11.888
20. Konstantakopoulou E, Harper RA, Edgar DF, Larkin G, Janikoun S, Lawrenson JG. Clinical safety of a minor eye conditions scheme in England delivered by community optometrists. BMJ Open Ophthalmol. 2018;3(1):e000125. doi:10.1136/bmjophth-2017-000125
21. Konstantakopoulou E, Edgar DF, Harper RA, et al. Evaluation of a minor eye conditions scheme delivered by community optometrists. BMJ Open. 2016;6(8):1–7. doi:10.1136/bmjopen-2016-011832
22. Swystun AG, Davey CJ. A needs assessment for a minor eye condition service within Leeds, Bradford and Airedale, UK. BMC Health Serv Res. 2019;19. doi:10.1186/s12913-019-4448-8
23. Cottier K, Mcoptom H, As D. An audit of the Primary Eye-care Acute Referral Scheme (PEARS) within NHS Bromley Clinical Commissioning Group (CCG). Optom Pract. 2015;16(1):21–31.
24. Harrison RJ, Wild JM, Hobley AJ. Referral patterns to an ophthalmic outpatient clinic by general practitioners and ophthalmic opticians and the role of these professionals in screening for ocular disease. Br Med J. 1988;297:1162–1167. doi:10.1136/bmj.297.6657.1162
25. Patel A, Patel H. Promoting self care in the community: the evidence and why it is important. Pharm J. 2014.
26. Porteous T, Ryan M, Bond CM, Hannaford P. Preferences for self-care or professional advice for minor illness: a discrete choice experiment. Br J Gen Pract. 2006;56(533):911–917.
27. Burns DH, Edgar DF. Review of the Camden and Islington anterior segment eye disease scheme. Optom Pract. 2002;3:55–60.
28. Kathy O The antimicrobial time bomb. Acuity; November 2018. Available from: https://www.college-optometrists.org/acuity-resource/the-antimicrobial-time-bomb.html.
29. England N Antibiotic awareness resources. Available from: https://www.gov.uk/government/collections/european-antibiotic-awareness-day-resources. Accessed March 3, 2020.
30. Moore M. Suffolk demographic profile. Available from: https://www.suffolk.gov.uk/assets/council-and-democracy/our-aims-and-transformation-programmes/Suffolk-Diversity-Profile.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.