Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
A Hierarchical Management Model Based on the Multidisciplinary Team Concept for Pre-Hospitalized Patients Undergoing Ophthalmic Day Surgery
Authors Zhao YH, Dai C, Ouyang P, Xi WQ
Received 1 August 2025
Accepted for publication 20 November 2025
Published 1 December 2025 Volume 2025:18 Pages 7839—7846
DOI https://doi.org/10.2147/JMDH.S557667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Yan-Hua Zhao,1 Can Dai,2 Ping Ouyang,2 Wen-Qun Xi3
1Pre-Hospitalization Management Center, Shenzhen Eye Hospital, Shenzhen Eye Center, Southern Medical University, Shenzhen, Guangdong, 518040, People’s Republic of China; 2Nursing Department, Shenzhen Eye Hospital, Shenzhen Eye Center, Southern Medical University, Shenzhen, Guangdong, 518040, People’s Republic of China; 3Cataract Department, Shenzhen Eye Hospital, Shenzhen Eye Center, Southern Medical University, Shenzhen, Guangdong, 518040, People’s Republic of China
Correspondence: Wen-Qun Xi, Cataract Department, Shenzhen Eye Hospital, Shenzhen Eye Center, Southern Medical University, No. 18 of Zetian Road, Futian District, Shenzhen, Guangdong, 518040, People’s Republic of China, Tel +86 13424373287, Fax +86 0755-23959563, Email [email protected]
Objective: The aim of this study is to evaluate the effectiveness of a hierarchical management model based on the multidisciplinary team (MDT) concept in managing pre-hospitalized patients undergoing ophthalmic day surgery.
Methods: A cohort of 6178 patients who underwent elective ophthalmic day surgery between October and December 2022 prior to the implementation of the revised pre-hospitalization service model were selected as the control group, while 8,788 patients who underwent elective ophthalmic day surgery between October and December 2023 following the implementation of the new hierarchical management model for pre-hospitalized patients were included as the observation group. The conventional admission process for surgical patients was adopted in the control group, whereas the new MDT-based hierarchical management model for pre-hospitalized patients was implemented in the observation group. This innovative model encompassed three components: pre-hospitalization information management, a structured preoperative evaluation system, and hierarchical preoperative nursing management. The rates of day-of-surgery cancellations and hospitalization cancellations, as well as satisfaction levels among patients who had elective ophthalmic day surgery, were compared between the two groups.
Results: The rates of day-of-surgery cancellations and hospitalization cancellations in ophthalmic day surgery among patients in the observation group were significantly lower, while patient satisfaction was significantly higher compared to the control group (p < 0.05).
Conclusion: The implementation of an MDT-based hierarchical management model for pre-hospitalized patients proved effective in facilitating a closed-loop system for preoperative safety management during the perioperative period of ophthalmic day surgery, reducing the rates of day-of-surgery cancellations, improving patient satisfaction, and ensuring the efficient and safe conduct of ophthalmic day surgery procedures.
Keywords: day surgery, day-of-surgery cancellation rates, nursing hierarchical management, preoperative evaluation model
Introduction
Ophthalmology is considered one of the most suitable specialties for day surgery.1 The implementation of day surgery has led to a shift from the traditional surgical management model and has contributed considerably to improving the efficiency of resource utilization in medical institutions, reducing healthcare costs,2 and resolving challenges related to accessibility and affordability of medical treatment. However, ensuring the quality and safety of day surgery remains a key concern, as rigorous management is necessary to address the rapid turnover of procedures, shortened hospital stays, and increased safety risks in day surgery.
The need for precise management throughout the entire ophthalmic day surgery process has been emphasized in the Draft for Comments on the Implementation Rules for Guangdong Specialized Hospitals (Ophthalmology Specialty) in the Standard of Review for Tertiary Hospitals (2020 Edition) as well as the Expert Consensus on the Management of Ophthalmic Day Surgery in China.3 However, multiple safety risks exist during the period between patient registration for pre-hospitalization and formal hospital admission. Safety management—which involves management measures designed to effectively control various risk factors to safeguard the physical and mental health of patients—is the core focus of pre-hospitalization protocols.
At present, optimizing the processes and implementation of pre-hospitalization models has been the focus of research, while studies on the safety management of patients before admission remain limited. In an effort to refine pre-hospitalization management for surgical patients, based on preliminary research and expert evaluations, a structured management process was established in the medical institution where the study was conducted. Following nearly two years of implementation, a distinct pre-hospitalization management model has been developed. Given that hospitalized surgical patients require comprehensive preoperative evaluation4 and a hierarchical management model based on the multidisciplinary team (MDT) concept for pre-hospitalized patients was incorporated into the management of ophthalmic day surgery patients, and an analysis of this model is presented in the sections below.
Participants and Methods
Study Participants
A total of 6,178 patients who underwent elective ophthalmic day surgery between October and December 2022 prior to the implementation of the revised pre-hospitalization service model in the hospital were selected as the control group, while 8,788 patients who underwent elective ophthalmic day surgery between October and December 2023 after the new hierarchical management model was implemented for pre-hospitalized patients were included in the observation group.
Inclusion criteria: Patients covered by medical insurance for employees or urban and rural residents within the province and those who had undergone preliminary assessment by an ophthalmologist at the outpatient clinic to determine the presence of any internal medical emergencies, acute disease exacerbations, or other contraindications. Only patients in stable health condition meeting the indications for ophthalmic elective day surgery were included in the study.
Intervention Methods
Intervention Methods for Patients in the Control Group
The conventional hospitalization process was followed for patients in the control group. Patients undergoing elective surgery were initially screened in an outpatient clinic, and their day surgery information was manually recorded. Patients were instructed to complete the preoperative examinations and preparations and were provided with relevant details of the procedure, including the scheduled time of surgery, surgical approach, anesthesia method, and so on. On the day of admission, consultations with physicians in the internal medicine departments were organized based on the results of the preoperative examinations, and ophthalmic day surgery was performed in accordance with the recommendations provided by the internal medicine specialists.
Intervention Methods for Patients in the Observation Group
The establishment of a pre-hospitalization center was planned, with designated personnel assigned to oversee the pre-hospitalization management for ophthalmic day surgery patients. The implementation process was structured around three aspects: integration of patients into a pre-hospitalization information management system, development of an innovative preoperative evaluation model, and implementation of a preoperative hierarchical management approach. Additionally, preoperative medical information pertaining to the patient was digitally shared with the ward and surgical teams, facilitating a closed-loop system for preoperative safety management throughout the perioperative period of ophthalmic day surgery. This approach was designed to enhance the safety and efficient conduct of ophthalmic day surgery procedures.
Closed-Loop Intelligent Pre-Hospitalization Information System for Ophthalmic Day Surgery Patients
At present, most hospitals in China have established comprehensive information systems such as the Hospital Information System (HIS), Laboratory Information System (LIS), Radiology Information System (RIS), and Picture Archiving and Communication System (PACS), among others. However, it has been found in clinical practice that there are often inconsistencies in surgical nomenclature, where multiple names exist for the same surgical procedure, and variations in interpretation are observed even among specialists within the same field. These discrepancies not only create challenges in surgical data analysis and statistical reporting but also greatly reduce the efficiency of information management. This necessitates the establishment of a standardized and robust surgical management information system.
At the Shenzhen Eye Hospital, a pre-hospitalization management information system was independently developed based on the existing HIS framework. The construction of the pre-hospitalization information system was vigorous, integrating multiple functions such as registration and inquiry, closed-loop management of abnormal findings in examinations and laboratory investigations, pre-hospital education, pre-writing of medical records, lens booking, submission of surgical applications, and automated text message notifications. The incorporation of patients as well into the pre-hospitalization information management system was designed to facilitate the precision of pre-hospitalization management.
The hospital-wide information network was organized to enable convenient access to patient records, addressing previous challenges associated with manual data entry, which often resulted in missing patient information, low efficiency, and an inability to share data effectively. Information technology was incorporated not only to simplify the process of scheduling day surgery but also to enhance operation efficiency and support the hospital’s strategic expansion of ophthalmic day surgery services. In addition, the implementation of this digital platform was aimed at enabling time-based admission for ophthalmic day surgery patients, thereby reducing hospital waiting times and improving the overall medical experience for patients.
Establishment of a Preoperative Risk Assessment System for Pre-Hospitalized Patients
Development of a Standardized Preoperative Management System
The expansion of ophthalmic day surgery in the hospital has resulted in a notable increase in the proportion of grade 3/4 surgeries and same-day surgeries. A considerable proportion of patients opting for such surgeries is elderly or those with multiple comorbidities. However, the absence of a standardized preoperative management system resulted in inconsistent preoperative procedures. No uniform pre-hospitalization process or preoperative assessment tools meant inadequate communication between medical staff and reliance on the subjective clinical judgment of physicians for preoperative evaluations. The use of a single-dimensional quality assessment method, along with insufficient objectivity and comprehensiveness, further contributed to a high rate of missed appointments for ophthalmic day surgery. To address these challenges, a standardized and systematic preoperative management system as developed to improve the uniformity of ophthalmic day surgery management.
Formulation of Consistent Preoperative Evaluation Standards and the Surgical Risk Threshold
In a significant departure from the traditional management concept of the hospital, a tripartite linkage risk assessment model under the MDT framework was established to ensure comprehensive preoperative risk screening throughout the perioperative period. This model involved collaboration among physicians, nurses, and anesthesiologists, incorporating multidisciplinary and multi-team coordination, multiple interventional modalities, and a dynamic approach to preoperative management of ophthalmic day surgery patients. The entire perioperative risk screening process was thereby optimized.
By integrating relevant concepts from the American Society of Anesthesiologists (ASA) classification5 and comprehensive geriatric assessment, an evaluation framework addressing eight major physiological systems and multiple drug management factors was established. This results in the development of a standardized “Preoperative Evaluation Standard for the Internal Medicine Department” for perioperative risk management and control. Patients’ tolerance to anesthesia and surgery, as well as associated risks, were systematically and objectively evaluated.
The pre-hospitalization phase for patients undergoing ophthalmic day surgery was designated as a critical evaluation point. Key surgical risk factors, including preoperative blood pressure, blood glucose, serum creatinine levels, grade of surgery, and duration of surgery, were incorporated into the pre-hospitalization management framework. Additionally, the concept of surgical risk thresholds (risk alert values) was introduced. Standardized “Pre-Hospitalization Criteria” and “Operability Standards” for ophthalmic day surgery in the hospital were established to guide the completion of patients’ preoperative preparations and determine whether further examinations, medication adjustments, or postponement of surgery were necessary.
These standardized criteria provided an evidence-based framework for patients and doctors to decide the timing of surgery, ensuring that surgeries exceeding the predefined risk threshold were postponed to allow for necessary interventions and risk control measures. Conversely, procedures within the acceptable risk range were conducted as scheduled, allowing patients to receive timely surgical treatment without an increased risk of postoperative complications. This approach mitigates the risks associated with subjective clinical judgment, thereby reducing instances of both over-treatment and under-treatment potentially caused by errors in physicians’ subjective judgments.
Hierarchical Management and Nursing Model for Pre-Hospitalized Patients
Hierarchical pre-hospitalization management for ophthalmic day surgery patients based on their preoperative risk assessment levels was implemented at the pre-hospitalization management center of the hospital. Patients classified as low-risk patients were those considered to have stable conditions and deemed suitable for surgery. Medium-risk patients were those that presented a higher surgical risk requiring enhanced monitoring and a cautious approach toward surgical intervention. High-risk patients were those that faced an extremely high surgical risk, and postponement of surgery was recommended.
For low- and medium-risk patients, routine pre-hospitalization procedures were followed, including pre-operative guidance and preparation for ophthalmic day surgery. Instructions were provided to patients regarding preoperative medication, information, bowel preparation (such as fasting and fluid restriction), and dietary adjustments to minimize patients’ anxiety and facilitate the smooth conduct of day surgery. For patients categorized as high risk in the preoperative assessment, an “online continuation service” provided by the pre-hospitalization center was implemented to respond to patients’ queries related to medical conditions and so on. The aim of this approach—with emphasis on “enhanced information exchange and reduced patient travel”—was to resolve pre-hospital concerns through a single hospital visit.
High-risk patients often require re-evaluation of abnormal blood test results. To prevent unnecessary re-examinations or omission of required tests, a “Notice of Normalization and Standardization of Abnormal Tests” was issued to the patient from the pre-hospitalization center, where normal indicators were explicitly marked, facilitating patients to understand the required re-evaluations. Additionally, individualized information and guidance were provided based on specific abnormal findings, such as blood pressure, blood sugar, electrolyte imbalances, and other conditions. Medication adjustments, dietary recommendations, and lifestyle modifications were suggested accordingly. Patient follow-up, monitoring, and feedback were conducted through the “pre-hospitalization center enterprise WeChat group” to improve adherence and patient satisfaction.
For patients whose surgical eligibility was temporarily affected by abnormal laboratory results, regular follow-up calls were conducted to track the patient’s re-evaluation status. Integration with the hospital’s information system allowed seamless communication with the primary surgeon via the updated appointment system, ensuring appropriate adjustments to the treatment plan. This process facilitated the closed-loop management of high-risk patients, enhancing the safety and efficiency of ophthalmic day surgery procedures.
Evaluation Indicators
The day-of-surgery cancellation rates, hospitalization cancellation rates, and patient satisfaction in ophthalmic day surgery were compared between the two groups of patients.
Statistical Analysis
Excel 2019 and SPSS 26.0 software were used for data analysis. Normally distributed quantitative data were expressed as the mean ± standard deviation (x ± s), and the t-test was used for comparisons between groups. Qualitative data were expressed in terms of number of cases (frequency) and percentage (%). A difference was considered statistically significant if the p-value was <0.05.
Results
Comparison of Same-Day Cancellation and Discharge Rates Between the Two Groups
In the observation group, a total of 8,788 day surgeries were scheduled, of which 117 cases (1.33%) were canceled on the day of surgery, and 32 patients (0.36%) withdrew from the hospitalization process. In the control group, 6,178 day surgeries were scheduled, with 266 cases (4.31%) canceled on the day of surgery and 40 patients (0.65%) withdrawing from hospitalization. The differences between the two groups in terms of same-day surgery cancellation rate (χ2 = 128.692, p < 0.001) and day surgery discharge withdrawal rate (χ2 = 6.082, p = 0.014) were statistically significant. Detailed results are shown in Table 1.
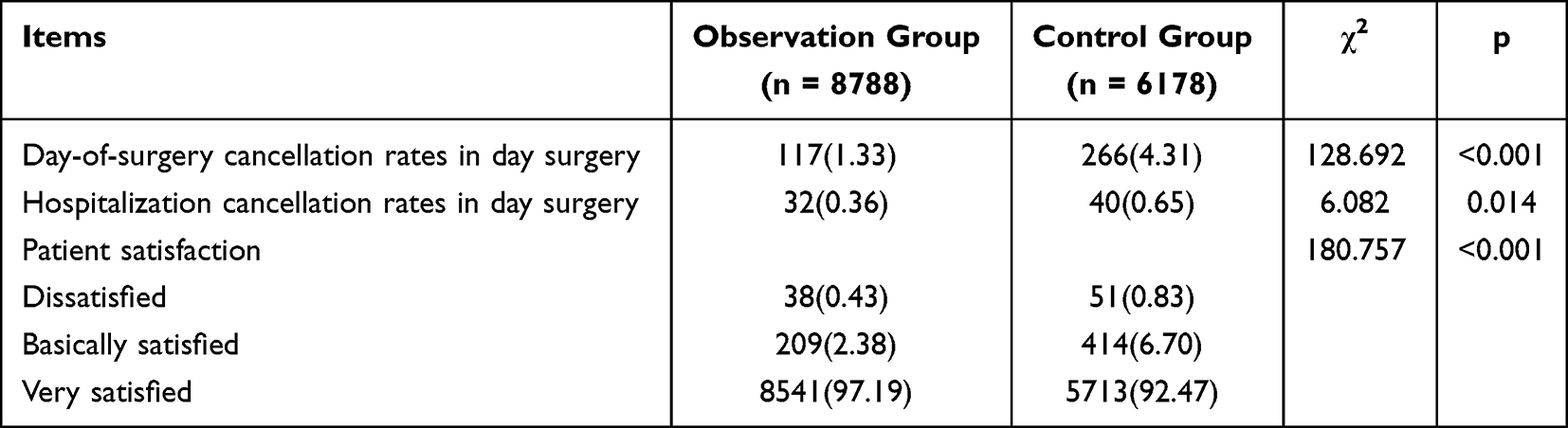 |
Table 1 Comparison of the Day-of-Surgery Cancellation Rates, Hospitalization Cancellation Rates, and Patient Satisfaction in Day Surgery Between the Two Groups |
Comparison of Satisfaction Between the Two Groups
In the observation group, 8,541 patients (97.19%) were very satisfied, 209 (2.38%) were basically satisfied, and 38 (0.43%) were dissatisfied. In the control group, 5,713 patients (92.47%) were very satisfied, 414 (6.70%) were basically satisfied, and 51 (0.83%) were dissatisfied. The difference in satisfaction between the two groups was statistically significant (χ2 = 180.757, p < 0.001).
Discussion
Advantages of the New MDT-Based Hierarchical Management Model
In routine pre-admission management model, nurses manually registered patients’ day-surgery information at the nurse clinic, provided basic preoperative instructions, and informed patients of relevant surgical requirements. Patients were then admitted for surgery as scheduled. In contrast, the MDT-based hierarchical nursing management model applied in this study was an innovative approach that integrated the MDT concept, comprising anesthesiologists, internists, nurses, and hospital administrators, into pre-admission care. A standardized preoperative assessment system was established, supported by a hospital-wide information platform enabling real-time patient monitoring and coordination across departments. During pre-admission, the MDT team performed a comprehensive evaluation of each patient’s ocular and systemic conditions, and stratified them according to disease severity and treatment needs. Based on the stratified risk assessment, pre-admission nurses played an expanded role by providing targeted examination guidance, personalized health education, follow-up management, and coordination of further medical services such as bed allocation and surgical scheduling once surgical criteria were met. In the conventional model, insufficient preoperative preparation or unrecognized comorbidities often led to surgery delays or cancellations, increasing perioperative risk. The MDT-based hierarchical nursing model, supported by information technology, overcomes disciplinary barriers, enhances multidisciplinary collaboration efficiency, enables nurses to conduct more precise risk-based management, and optimizes the allocation of medical resources.
Implementation of the New MDT-Based Hierarchical Management Model Improved Medical Resource Utilization Efficiency
The new MDT-based hierarchical management model for pre-hospitalized patients was found to improve the efficiency of medical resource utilization. The quality and efficiency of medical services are increasingly recognized as key indicators of surgical patient satisfaction.6 Hospitals that consistently provide high-quality care while maintaining cost-effectiveness and patient satisfaction are better positioned for long-term operational sustainability. A key result in this study was that the time from admission to surgery was significantly shorter in the observation group, which was similar to the results of Mei and Kaizhu.7
In the traditional mode, consultation with internal medicine departments typically occurs after hospitalization for patients undergoing ophthalmic day surgery. Consequently, if patients are deemed temporarily unsuitable for surgery after the medical or pre-anesthetic evaluation, their surgery may be delayed or canceled, thereby extending their hospital stay. Furthermore, same-day surgery cancellations not only waste operating room resources but also impose emotional distress and financial burdens on patients and families.8,9
Implementation of the MDT-Based Preoperative Evaluation System Reduced the Day-of-Surgery Cancellation Rates in Ophthalmic Day Surgery
Prolonged waiting times for hospital beds and surgeries in general hospitals have been a major source of patient dissatisfaction, often leading to doctor-patient conflicts and negatively affecting the overall medical experience.10 To address this issue, the scope of pre-inpatient and outpatient services was proactively expanded in the hospital, and a preoperative risk assessment model for pre-hospitalized patients based on the concept of MDT was developed.
The tripartite linkage risk assessment model incorporating physicians, nurses, and anesthesiologists ensured clearly defined roles and responsibilities, reduced redundant assessments, and improved comprehensive preoperative evaluations. This model enabled dynamical patient tracking and timely transmission of preoperative examination results to physicians, thereby strengthening the perioperative risk screening process. This systematic approach thus promoted pre-hospital safety management in ophthalmic day surgery while also serving as an important indicator of high-standard medical care.
In the new model, the preoperative consultation with internal medicine specialists from the post-admission phase (as practiced in the traditional hospitalization model) was shifted to the pre-hospitalization outpatient stage. This strategy not only alleviated patient anxiety but also effectively shortened preoperative waiting times, reduced the day-of-surgery cancellation rates in ophthalmic day surgery, and improved the overall medical experience of patients. Additionally, the enhanced efficiency of ophthalmic day surgery led to optimized hospital bed utilization, benefiting both patients and healthcare providers. In this study, patient satisfaction in the observation group reached 99.57%, aligning with the results reported by Yang et al.11
Implementation of the MDT-Based Hierarchical Management Model Reduced Hospitalization Cancellation Rates in Ophthalmic Day Surgery
The innovative hierarchical management model for pre-hospitalized patients based on the concept of MDT was introduced in the institution in alignment with safety management requirements. In this model, patients were classified and managed according to their risk assessment levels, focusing on high-risk populations, thereby ensuring the quality and safety of medical services.
Risk assessment and hierarchical management represent essential components of modern clinical nursing management.12 Unlike traditional reactive nursing approaches, which primarily involve “firefighting” through post-event remedial nursing interventions, proactive patient care was emphasized in this model. By stratifying patients based on risk levels, individualized nursing interventions were implemented, enabling targeted and predictive nursing measures. This approach facilitated early detection, screening, and treatment, ensuring safety and optimal patient outcomes.
In addition, the expansion of the “online pre-hospitalization continuation service” for high-risk patients in ophthalmic day surgery established a closed-loop management system for abnormal laboratory indicators and significantly reduced hospitalization cancellation rates. By prioritizing “more information transmission and fewer hospital visits”, patient inconvenience was minimized in this model, reducing unnecessary hospital visits while improving the overall medical experience.
These improvements helped to achieve the standardization of quality and safety management in ophthalmic day surgery nursing, while promoting the rationalization of medical and health resource utilization in the hospital and ensuring the systematic and orderly implementation of ophthalmic day surgery services.
Future Directions
In recent years, day surgery programs have been widely implemented, with missed rates of day surgery reported in the range of 2.28% to 11.51% in the literature in China and elsewhere.13 A high no-show rate in day surgery not only compromises the patient’s medical experience but also presents considerable challenges to the efficient operation of hospitals. At present, perioperative safety management has been enhanced in most hospitals in China, but due to variations in digital infrastructure and non-standardized processes, the effective implementation of perioperative management systems remains a challenge in many hospitals. Moving forward, leveraging information technology to optimize perioperative management, enhance operational efficiency, minimize no-show rates, and reduce unplanned surgeries will be key areas for further research and development. A more comprehensive and standardized approach to digital perioperative management is essential to improving the safety, efficiency, and overall success of ophthalmic day surgery programs.
In the future, artificial intelligence (AI) is expected to play an increasingly pivotal role in supporting multidisciplinary perioperative management. AI-driven systems can enhance predictive analytics for surgical risk assessment, optimize patient scheduling, and improve the allocation of medical resources, further strengthening the MDT-based model proposed in this study. In ophthalmic surgery, AI applications have shown promise in diagnostic imaging, surgical planning, and postoperative monitoring, enabling more accurate and personalized care.14 Similarly, in dentistry, AI has demonstrated significant value in radiologic interpretation and implant planning, improving clinical precision and patient safety.15 The integration of AI technologies into perioperative information systems could therefore facilitate real-time data analysis, streamline workflows, and promote more efficient, patient-centered care across medical disciplines.
Conclusion
This study developed a closed-loop safety management system for ophthalmic day surgery using a multidisciplinary, stratified management approach for patients before admission. The model improved the quality and safety of day surgery and may serve as a reference for other hospitals to enhance their management processes. Future studies could test this model in other medical fields and explore the use of AI technologies to support automated and personalized risk assessment, further improving day surgery safety and efficiency.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Shenzhen Eye Hospital. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
No external funding was received to conduct this study.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Haihan D, Changfei Z, Hengli L, Ning T, Lezhen Z, Hui L. The development of day surgery in China and the effectiveness and reflection of day surgery in ophthalmology-specialized hospitals. Cost Eff Resour Alloc. 2024;22(1):47. doi:10.1186/s12962-024-00558-9
2. Kuuskeri M, Suorsa ET, Luukkaala TH, Palve JS. Day surgery in reduction mammaplasty - saving money or increasing complications? J Plast Reconstr Aesthet Surg. 2023;76:174–179. doi:10.1016/j.bjps.2022.10.027
3. Ji W, Liu YP, Dai W. Current developments and future perspectives of ambulatory surgery in China. Chin J Pract Surg. 2020;40(2):
4. Tsai HW, Huang SW, Hung YL, Hsu YS, Huang CC. Use of the smart lean method to conduct high-quality integrated perioperative management prior to hospitalization. Int J Environ Res Public Health. 2021;18(24):13391. doi:10.3390/ijerph182413391
5. Bartha E, Ahlstrand R, Bell M, et al. ASA classification and surgical severity grading used to identify a high-risk population, a multicenter prospective cohort study in Swedish tertiary hospitals. Acta Anaesthesiol Scand. 2021;65(9):1168–1177. doi:10.1111/aas.13932
6. Wang SY. Influence of information system on operating efficiency and work quality of operation room. Med Society. 2019;32(1):72–74. doi:10.13723/j.yxysh.2019.01.016
7. Zheng M, Chen KZ. Practice and optimization of pre-hospitalization management mode in a tertiary hospital. Hosp Manag Forum. 2020;37(8):21–22. doi:10.3969/j.issn.1671-9069.2020.08.006
8. Kaddoum R, Fadlallah R, Hitti E, El-Jardali F, El Eid G. Causes of cancellations on the day of surgery at a tertiary teaching hospital. BMC Health Serv Res. 2016;16(1):259. doi:10.1186/s12913-016-1475-6
9. Solak AK, Pandza H, Beciragic E, Husic A, Tursunovic I, Djozic H. Elective case cancellation on the day of surgery at a general hospital in sarajevo: causes and possible solutions. Mater Sociomed. 2019;31(1):49–52. doi:10.5455/msm.2019.31.49-52
10. Zhang H, Shi L, Yang J, Sun G. Efficiency and equity of bed utilization in China’s health institutions: based on the rank-sum ratio method. Int J Equity Health. 2023;22(1):177. doi:10.1186/s12939-023-01986-4
11. Yang J, Zhou L, Liu Y, He XY. Construction and optimization of one-stop pre-hospitalization preparation center for “medical steward”. Chin Hosp. 2023;27(3):66–68. doi:10.19660/j.issn.1671-0592.2023.03.18
12. Xiaoyu L, Jinxue L, Fengqiong J, Yan Z, Qiaohua Y. Development and application of nursing risk management evaluation system. Stud Health Technol Inform. 2021;284:414–420. doi:10.3233/SHTI210761
13. Gaucher S, Boutron I, Marchand-Maillet F, Baron G, Douard R, Béthoux JP, AMBUPROG Group Investigators. Assessment of a standardized pre-operative telephone checklist designed to avoid late cancellation of ambulatory surgery: the ambuprog multicenter randomized controlled trial. PLoS One. 2016;11(2):e0147194. doi:10.1371/journal.pone.0147194
14. Nuliqiman M, Xu M, Sun Y, et al. Artificial intelligence in ophthalmic surgery: current applications and expectations. Clin Ophthalmol. 2023;17:3499–3511. doi:10.2147/OPTH.S438127
15. Macrì M, D’Albis V, D’Albis G, et al. The role and applications of artificial intelligence in dental implant planning: a systematic review. Bioengineering. 2024;11(8):778. doi:10.3390/bioengineering11080778
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.