Back to Archived Journals » International Journal of Clinical Transfusion Medicine » Volume 5
A global survey of clinicians' awareness, accessibility, utilization of e-continuous education, and quality of clinical blood use: policy considerations
Authors Smit Sibinga CT ![]() , Oladejo MA, Adejumo OH, Eichbaum Q, Kumagawa M
, Oladejo MA, Adejumo OH, Eichbaum Q, Kumagawa M ![]() , Kino S, Zolfaghari S, Wendel S, Rasovic G, Erdenebayar N, Makhmudova M, Mpuntsha L
, Kino S, Zolfaghari S, Wendel S, Rasovic G, Erdenebayar N, Makhmudova M, Mpuntsha L ![]() , Ingram C, Karabaev BB, Kajja I, Sanji ZMH, Satti MM
, Ingram C, Karabaev BB, Kajja I, Sanji ZMH, Satti MM
Received 3 March 2017
Accepted for publication 29 May 2017
Published 13 July 2017 Volume 2017:5 Pages 69—82
DOI https://doi.org/10.2147/IJCTM.S136047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Dora N Mbanya
Cees Th Smit Sibinga,1 Maruff A Oladejo,2 Olamide Hakeem Adejumo,3 Quentin Eichbaum,4 Midori Kumagawa,5 Shuichi Kino,5 Sima Zolfaghari,6 Silvano Wendel,7 Gordana Rasovic,8 Namjil Erdenebayar,9 Maya Makhmudova,10 Loyiso Mpuntsha,11 Charlotte Ingram,11 Bakyt B Kharabaev,12 Isaac Kajja,13 Zainab Mukhtar Hussain Sanji,14 Maria M M Satti15
1IQM Consulting for International Development of Quality Management in Transfusion Medicine, University of Groningen, Groningen, the Netherlands; 2Department of Educational Management, University of Lagos, Lagos, 3Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria; 4Department of Pathology, Microbiology and Immunology, Vanderbilt University Medical Center, Nashville, TN, USA; 5Japanese Red Cross Hokkaido Block Blood Center, Japan; 6IBTO, Tehran, Iran; 7Blood Bank, Hospital Sirio Libanês, Sao Paulo, Brazil; 8Montenegro National Blood Transfusion Center, Podgorica, Montenegro; 9National Center for Transfusion Medicine, Ulaanbaatar, Mongolia; 10Consultant IQM Consulting, Tashkent, Uzbekistan; 11South Africa National Blood Transfusion Service, Johannesburg, South Africa; 12National Blood Transfusion Service, Bishkek, Kyrgyzstan; 13Department of Orthopedics, Mulago Hospital, Makerere University, Uganda; 14Consultant, Dow University of Health Sciences, Karachi, Pakistan; 15National Blood Transfusion Service, Khartoum, Sudan
Introduction: Clinical use of blood has shown the least developed part in the vein-to-vein transfusion chain. This global study was carried out in order to investigate the level of awareness, accessibility and utilization of continuous e-learning and education, and quality of blood use among blood prescribing clinicians and nurses.
Approach: Descriptive ex post facto survey design.
Methods: A total of 264 purposively selected blood prescribing clinicians and nurses from the four Human Development Index (HDI) groups of countries (low, medium, high, and very high) participated in this study. Three research questions were answered, while seven null hypotheses were tested at 0.05 level of significance. Descriptive statistical tools (frequency counts and percentage) were used to analyze demographic backgrounds; inferential statistics – Pearson product-moment correlation coefficient (PPMCC) and analysis of variance (ANOVA) were used to analyze hypotheses.
Results: Quality of clinical blood use was positively and significantly correlated with the level of awareness (r=0.137; p=0.03; df=262) and accessibility (r=0.184; p=0.01; df=262) to e-continuous learning among clinicians/nurses. There was a significant difference in the levels of awareness (F[3,260]=53.942, p=0.01), accessibility (F[3,260]=38.582, p=0.01), and utilization (F[3,260]=24.858, p=0.01) of continuous e-learning and education among clinicians/nurses based on HDI grouping, particularly between very high and low HDI. Furthermore, there was a significant difference in the levels of accessibility (F[6,257]=6.444, p=0.01) and utilization (F[6,257]=13.704, p=0.01) of continuous e-learning and education among clinicians based on clinical specialty/department and a significant difference in the quality of clinical blood use based on clinical specialty/department (F[6,257]=9.677, p=0.01).
Conclusion and recommendations: The higher the HDI level the better is the awareness, accessibility, and utilization of continuous education, both through e-learning and conventional in teaching curricula. This has an immediate impact on the quality of clinical care and in particular on supportive hemotherapy and the development of patient blood management systems.
Keywords: continuous E-learning and education programs, awareness, accessibility, utilization, blood prescribing clinicians/nurses, Human Development Index, quality management, clinical blood use, patient blood management
Introduction
Since World Health Organization (WHO) in 1975 published its first recommendations on the utilization and supply of human blood and blood products (WHA28.72), education has been an essential part of the approach. Following the HIV/AIDS outbreak in the early 1980s, the Global Blood Safety Initiative (GBSI) was initiated. Two WHO meetings were held in 1991 on education in transfusion medicine,1,2 as part of the WHO GBSI:
- Informal consultation on assessment of training needs in transfusion medicine,
- Informal consultation on collaboration in training in transfusion medicine.
Core constraints in education (teaching and training) leading to a serious shortage of competent manpower in blood transfusion were identified and a strategy to overcome these was proposed in line with the global initiative for programs to combat HIV/AIDS. Since then, many existing and new endeavors have been undertaken all around the world with and without (sustainable) support from education authorities and financial donors. However, there has not been a structured coordination or a continuous inventory of these initiatives.
WHO has developed a series of Distance Learning Materials (DLM),3 which continue to be used and extended. At the turn of the century, the WHO Quality Management Training (QMT) program4 was created and implemented on a global level, although not all objectives could be realized due to shortage of funds, time and experienced facilitators. Council of Europe (CoE) has also initiated a series of training courses focused on development of safe, efficacious, and sustainable national blood supply and transfusion systems.5
There are many more such initiatives both from professional and from public organizations in various parts of the world. In 1991, it was recognized that absence of a workable definition of transfusion medicine not only caused confusion but also generated misunderstanding and divergent views on what this field of science and practice really should encompass. It was therefore decided to create such a definition by consensus and use it as a major prerequisite for strategy development.2 This definition reads
Transfusion medicine deals with that part of the health care system which undertakes the appropriate provision and use of human blood resources. It provides the essential scientific and clinical information for transfusion practice, and the link between the blood donor’s altruistic donation and the patient.
During a plenary session of the fourth meeting (2003) of the WHO-convened forum Global Collaboration for Blood Safety (GCBS), international organizations working for global blood safety also reiterated the need for collaboration in education (teaching and training) in transfusion medicine.6 At a WHO Informal Consultation to Develop a Global Strategy on Education and Training in Blood Transfusion October 2004, one of the objectives was the initiation of the development of a strategy to promote and support integration of education in transfusion medicine and science into existing curricula in schools of medicine, nursing, and medical laboratory technology.7
Particularly important is sustained Government commitment to develop national policies for education (teaching and training) within the national blood policy, a legislative framework advocating training for all staff associated with blood transfusion (procurement and clinical use) and adequate budget allocation for teaching and training. Within the European Union (EU), this has now been formalized through the EU Directive 2002/98.8
Apart from local/national education (teaching and training) materials, WHO, International Red Cross (IRC), CoE, and other international organizations have developed teaching and training materials for the various elements of transfusion medicine. Most of these materials are kept up-to-date and made available to those interested and involved in education and training. American Association of Blood Banks (AABB) has developed a series of teaching and training materials that are widely used outside the membership.9 These materials range from basic to advanced and cover a sliding scale of development in transfusion medicine (vein-to-vein), theoretical as well as practical.
Many of these available materials are designed using a distance learning principle. A growing number has advanced into a more interactive e-learning principle. However, most of these materials are supportive (such as the rapid growing availability of apps) rather than integrated elements of formal curricula. There is a need to assess the existing “market” of electronic education (teaching and training) materials available including language accessibility and economic affordability and create a virtual library to support global, regional, and national education in the field of transfusion medicine. This is particularly important for prescribing and practising blood transfusion at the bedside – clinicians and nurses.
Review of related literature
Although education including e-education is one of the most crucial quality system essentials, so far the need has been grossly underestimated especially in the clinical use of blood. Over the past decade, e-learning materials have been developed by some of the more advanced national blood transfusion services such as the British National Blood and Tissue Service, the Irish, Australian, and Canadian (ON) blood transfusion services. The materials have been posted on the respective web sites and are not all publicly accessible. In the USA, some initiatives have also been developed, e.g., Blood Systems and Harvard Medical School. EU, through its Optimal Blood Use project, is developing materials and courses, but these are not yet operational. Blood transfusion societies in Europe and North America have also developed e-learning materials and courses focused on clinical use of blood. Examples are the British Blood Transfusion Society (BBTS),10 AABB, and Australian Red Cross Blood Transfusion Service.11
State of transfusion medicine in developed and developing nations
In a recent publication, Smit Sibinga and Pitman12 gave a broad overview of the various states of development of transfusion medicine. The focus is on how to bridge the existing knowledge gaps. Observations in various countries in different parts of the world have demonstrated the need for adequate and competent human capacity development and retention. A state of development in transfusion medicine, vein-to-vein, is not in the first place dependent on upgraded equipment, technologies, and methodologies but on the accessibility of education (teaching and training) – a competent human capacity. Globally, clinicians prioritize clinical work and extra time away would be a serious imposition. However, the need for education in clinical use of blood (in-hospital transfusion chain) is not only restricted to low and medium Human Development Index (HDI) countries but stretches well into high and even very high HDI countries.
Continuous E-learning and education programs in blood transfusion
Programs offered can be divided into two categories – tools and courses. Tools comprise a diversity of guidelines and instructive e-documents as well as apps for consultation of, e.g., literature. EU strives to develop a series of tools to support clinicians and blood bank professionals in the development of a common quality and quality management system. The main tool is a Manual with guidelines and resources to begin the development of a quality system for the clinical transfusion process.13 Aim is to improve safety and efficacy of the clinical transfusion process and promote rational use of blood products across the EU through sharing of information and best practices.
Courses are largely interactive and modular with inbuilt e-tests. Aims are to improve patient care, reduce risk, and become competent practitioners through learning about safe transfusion practice. Online recording and assessment systems (ORAS) have been designed to allow participants to record their scores on completion of a module assessment and even print a certificate as evidence of theoretical (knowledge) and/or clinical competence. Such ORAS also allows authorized personnel of clinical care institutions to issue reports from the system that show usage, assessment and modules completed by clinical specialty, staff group, or different grades. The Australian BloodSafe e-learning program (eLearning Australia14) focuses on transfusion practice and patient blood management education with five courses – 1) clinical transfusion practice, 2) collecting blood specimens, 3) transporting blood, 4) postpartum hemorrhage, and 5) iron deficiency anemia.
The eLearning Australia clinical transfusion practice course consists of five e-learning modules: 1) risks and benefits – decision to transfuse, risks, benefits, and informed consent; 2) pretransfusion samples – importance of patient identification and specimen labeling; 3) picking up blood – transporting and storage of blood (in-hospital cold chain); 4) administering blood; and 5) monitoring and reactions – recognizing and responding to acute adverse events. The US Blood Systems e-Learning Center promotes continuous education through a tracking system of self-study courses on blood banking (six courses) and compliance (three courses). Each course has a posttest and evaluation leading to PACE (PACE is a registered trademark of the American Society for Clinical Laboratory Science) credits.15
Government expenditure on continuous education programs for clinicians
Within the EU, the Directive (Law) 2002/988 and its related EC Directive 2005/6216 require from the Member States that personnel in blood establishments and hospitals shall be continuously trained and assessed to be competent in their tasks. The British National Health Service and the Australian Department of Health have developed national e-learning programs for education and continuous education of those involved in both procurement and clinical use of blood.
Job performance and working conditions of clinicians in selected countries
Job performance and working conditions of clinicians in the various countries are diverse. Hospitals usually lack a defined blood policy and have not yet developed a hospital quality and quality management system with proper documentation to allow more detailed traceability. Hospital Transfusion Committees are not a common phenomenon in most low, medium, and high HDI countries and even the very high HDI countries do not all have reached the state of development in clinical blood transfusion as advocated by WHO. The overwhelming effect of the different economic resources, sophistication, and level of education play an important role. Key is the widely existing knowledge gap.12,17
Clinicians’ awareness of continuous e-learning and education programs
Continuous education programs are widely implemented, as most countries practice a professional competence evaluation system for health care workers. However, e-learning and e-tools have not yet gained a wide interest and application. In those areas where e-learning and continuous education programs have been instituted, there is awareness based on the mandatory demonstration that CME/CPD credits have been gained. However, this relates only to those countries where such education opportunities are formally offered. Even then, the scope of awareness may differ, largely driven by the professional license system. Whether awareness of the wealth of professional information in the e-learning materials is fully present needs to be investigated.
Clinicians’ accessibility to continuous e-learning and education programs
Accessibility to e-learning and continuous education depend on a number of factors such as availability, accessibility of a guaranteed functional internet, degree of computer literacy, ease of access of a program (user friendliness), and cultural acceptance of social media as a routing to access. These are aspects that need to be investigated. Little is known, however, Smit Sibinga presented at the ECEL 2011 information on accessibility to e-learning over a 5-year period of observation and experience with a postgraduate master course on management of transfusion medicine (MMTM).18
Clinicians’ utilization of continuous e-learning and education programs
There is little information available on the utilization of e-learning in clinical transfusion practice. In countries with developed health care and transfusion systems as well as established continuous professional education programs mandatory for licensing of professional practice in the health care, continuous education programs are used. However, they are largely based on group meetings and congresses, rather than on individual learning and upgrading of knowledge. Programs and courses or other professional/scientific events may have been identified and granted awarding of credits, provided they document and report to the granting organization such as the American Society for Clinical Laboratory Science. This needs to be investigated.
Theoretical framework
In blood transfusion, the clinical care is both starting point and end point of the vein-to-vein transfusion chain. Education (teaching and training) is fundamental to every aspect of blood transfusion safety and efficacy. This implicates a thorough and evidence-based knowledge and competence of those involves – prescribing/treating clinicians and nursing staff. Unfortunately, transfusion medicine is still the Cinderella of both clinical practice and medical science. As a result a knowledge gap is created and sustained due to insufficient and mostly inadequate availability and accessibility of relevant knowledge and related training to acquire the necessary skills.
The programs have to be designed to assist practitioners involved in the clinical transfusion process to provide and maintain consistently high standards of care. Today, there is a growing existence of e-learning tools and courses that interactively could contribute to the development of the desired high quality and efficacy of care, in particular in the application of supportive hemotherapy. Online learning packages, with accompanying knowledge assessments, increasingly are being offered to be completed in order to gain and maintain adequate knowledge necessary for best bedside practice. These may be ordered in increasing levels of perception, e.g.,
Level 1: safe transfusion practice, aimed at all staff groups involved in administration of blood and blood products, including medical and nursing staff, operating department practitioners, clinical support workers, and porters.
Level 2: blood product use, could focus on the constituents of blood products and plasma-derived medicinal products (PDMPs) and summarize the indications for use, therapeutic risks and benefits, and management of adverse events. It should be designed for practitioners who regularly prescribe and use blood and blood products in their day-to-day practice.
Level 3: appropriate blood use should be designed especially for doctors and nurses who are regularly involved in the management of patients requiring transfusion support (patient blood management [PBM]).19–22 This level could consist of scenarios dealing with transfusion management of a patient, e.g., experiencing a massive hemorrhage or severe malaria anemia. The patient scenarios would address issues such as the use of transfusion guidelines and triggers, informed consent, and alternatives to allogeneic transfusion and could be supported by a number of work apps.
These programs will appeal to anyone involved in blood transfusion or who is interested in safe and efficacious transfusion practice. Our focus, however, was on the ultimate responsible clinician and nursing staff at the bedside providing the care. Some of the challenges that may have to be overcome to provide effective training and assessment for hospital staff are:
- the large number of individuals and range of different employment groups who have some involvement in the clinical transfusion process;
- rapid turnover of staff (e.g., due to training requirements for clinical staff/residents);
- working patterns – shift work, part time work;
- multiple employers – e.g., agencies providing nurses and doctors, external contractors for support services;
- language differences;
- differences in education, training, and details of practice experience of personnel from different parts of the world.
It is important to comply with national requirements for education (teaching and training) of staff involved in blood transfusion. Although every country will have different access to resources and facilities, there are a number of essential steps to consider when implementing an education program in clinical transfusion (Figure 1).
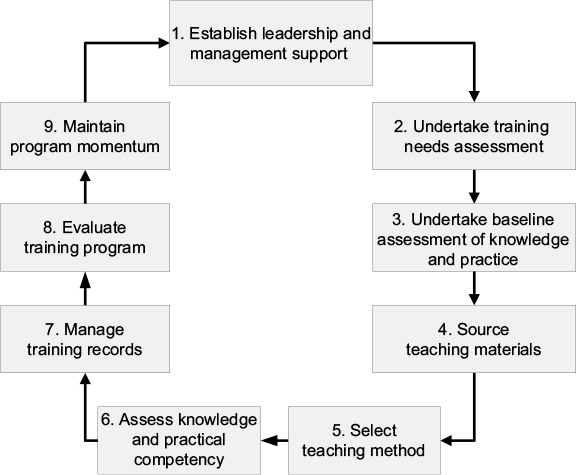 | Figure 1 Example of the steps for implementing an e-based education program. |
The development of, e.g., descriptions, guidelines, and Standard Operating Procedures is insufficient to alter and improve clinical practice. They are integral elements of a quality and quality management system that first has to be designed, based on the five key quality system essentials:
- organization and management (governance and structure),
- standards and guidelines (reference cadre),
- documentation (traceability, evidence),
- education (teaching and training, competence),
- assessment (monitoring and evaluation, continued improvement).
Study expectation was to gain a better insight in awareness, accessibility, and utilization of current e-learning tools and programs focused on clinical use of blood and blood products. That might identify existing gaps and allow the consideration of policy and strategies on how to improve in any given situation.
Appraisal of the reviewed literature
There is little peer reviewed literature on awareness, accessibility, and utilization of e-learning tools and programs for clinical prescribers of blood transfusion. The availability is in the accessibility of programs and tools designed by a limited number of organizations, exclusively coming from the very high HDI (VH-HDI) part of the world.
Given the value of e-learning today and for the future of transfusion medicine, the study might contribute to a needs assessment for a wider introduction of e-learning in clinical blood transfusion. This certainly will contribute to a more progressive development of improved patient care, reduction of transfusion related risks, and safe and efficacious clinical transfusion practice.
Statement of the problem
An important observation is the relatively extensive emphasis on the technical or operational procurement part of the transfusion chain – collection, processing, testing, storage, and distribution (cold chain), with limited emphasis on the in-hospital part of the chain that should lead to rational use of blood and blood products:
- indication setting and decision making, ordering and sample collection, and informed consent at the bedside;
- selection of blood and blood products and compatibility testing at the transfusion laboratory;
- patient and product identification, preparation (vital signs, giving set, and iv fluids), ultimate transfusion practice with appropriate monitoring and evaluation (hemovigilance) at the bedside.
In many parts of the world, blood prescribing clinicians are still not really aware of the values and risks of supportive hemotherapy. Blood transfusion as a transplant needs a thorough knowledge and experience to come to rational use as advocated by WHO.23 Blood transfusion is an integral part of the health care and therefore an essential part of patient care. When used correctly, it may improve health and save lives. However, blood transfusion carries a potential risk of acute and delayed complications and transfusion transmitted infections (TTIs). It should be prescribed only to treat conditions associated with significant morbidity or mortality that cannot be prevented or managed effectively by other means or available alternatives.
The effective implementation of national policy and guidelines requires education in clinical use of blood and safe clinical transfusion procedures for clinicians, nurses, blood bank staff, and other personnel involved. Besides undergraduate and postgraduate programs, this should include in-service teaching and training focused on the development of professional competence for clinicians, nurses, blood transfusion service, and hospital blood bank staff. An important element should be continuing medical/professional education and development (CME/CPD).
In both areas, e-learning has been introduced and is being applied increasingly. However, there are considerable lacuna’s which need to be further identified and analyzed. The national blood program as recommended by WHO24 has the responsibility to ensure that blood and blood products provided for clinical use are safe, adequate to meet demands, clinically effective, and produced consistently to appropriate standards, as well as a timely education (teaching and training) structure.
While responsibility for the decision to transfuse ultimately rests with individual treating and prescribing clinicians, consistently effective clinical transfusion practice cannot be achieved unless there is a well-organized, nationally coordinated blood transfusion service to ensure availability of and access to safe blood and blood products and transfusion guidelines. These should represent a consensus by knowledgeable clinical specialists, the blood transfusion service, pharmacists, and professional bodies on the most effective (evidence based) treatments for specific conditions. They should be practical, comprehensive, and relevant to local conditions to overcome the main problem: a continuing knowledge gap that seems to exist in all four level of the HDI.25
Study objectives
The broad objective of the study was to investigate the level of awareness, accessibility, and utilization of e-learning and continuous education programs on the quality and efficacy of clinical blood use by the blood prescribing clinicians and nursing staff:
- determine the relationship between the level of awareness, the level of accessibility and the level of utilization of continuous e-learning and education, and the quality and efficacy of clinical blood use;
- find out the differences among prescribing clinicians and nurses between the level of awareness, the level of accessibility, and the level of utilization of continuous e-learning and education, and the HDI.
- examine the difference among prescribing clinicians and nurses between the level of awareness, the level of accessibility, and the level of utilization of continuous e-learning and education, and clinical specialty/department.
Scope of the study
The study was carried out as an international comparative research among countries of different HDI state of development and in different parts of the world. Target groups were blood prescribing clinicians and nurses involved in bedside practice of blood transfusion. Both referral/general and specialized hospitals were approached to cooperate with a questionnaire completed by prescribing clinicians and residents, as well as nursing staff involved in the bedside transfusion practice. The outcome might lead to e-education (teaching and training) policy considerations and recommendations to improve quality and efficacy of blood transfusion (supportive hemotherapy) as an integral part of the clinical health care.
Research questions:
- What is the relationship between the level of awareness of continuous e-learning and education on the quality and efficacy of clinical blood use?
- What is the relationship between the level of accessibility of continuous e-learning and education on the quality and efficacy of clinical blood use?
- What is the relationship between the level of utilization of continuous e-learning and education on the quality and efficacy of clinical blood use?
Hypotheses
The following hypotheses were formulated to guide the study:
Relation to HDI:
H1 – There are no differences among the prescribing clinicians and nurses between the level of awareness of continuous e-learning and education, and HDI.
H2 – There are no differences among the prescribing clinicians and nurses between the level of accessibility of continuous e-learning and education and with different HDI.
H3 – There are no differences among the prescribing clinicians and nurses between the level of utilization of continuous e-learning and education and with different HDI.
Relation to clinical specialty/department:
H4 – There are no differences among the prescribing clinicians and nurses between the level of awareness of continuous e-learning and education, and clinical specialty/department.
H5 – There are no differences among the prescribing clinicians and nurses between the level of accessibility to continuous e-learning and education, and clinical specialty/department.
H6 – There are no differences among the prescribing clinicians and nurses between the level of utilization of continuous e-learning and education, and clinical specialty/department.
H7 – There are no differences among the prescribing clinicians and nurses between the quality of clinical use of blood, and clinical specialty/department.
Significance of the study
Education (teaching and training) is an essential quality element4,12 to create and maintain competence – the perfect match of knowledge and skills. Most traditional types of offering knowledge (teaching) and skills (training) are either personal or group performances and are based on a direct or indirect contact with a teacher – class room, apprentice, on site, or external courses of any type. These postgraduate approaches force students to leave work and often privilege those selected to be exposed to knowledge and practical skills oriented training.26 The study will provide needs assessment important for policy considerations.
E-learning offers the opportunity to individualize and reach students where ever present. E-learning does not require time off work and offers flexibility in necessary exposure – tailor made and fit for purpose. Introduction and accessibility of e-learning modules with e-testing of what was learned provides a great opportunity to improve on evidence- and knowledge-based clinical practice, as well as fast and focused consulting of available literature through dedicated apps. Additionally, the study may disclose knowledge and related skills gaps that can be analyzed and filled.
Methodology
Research design
The cross-sectional observational research design was descriptive-comparative and ex post facto in nature. This research design is appropriate for a study of this nature, considering the fact that data had to be collected across the selected countries to be able to describe the existing situation in each of these countries. It was also ex post facto due to the fact that none of the study variables could be manipulated because they are already in existence. A definition of ex post facto study has been described by Kerlinger.27
Study population
Participants were blood prescribing clinicians and nurses involved in the bedside practice of blood transfusion in representative referral/general and special hospitals.
The design of the questionnaire was anonymous; there was no possibility to identify individual hospitals, clinicians, or nurses. It was therefore decided that a consent from a research/medical ethical body was not needed. A simple request for collaboration could suffice as no patient data were involved.
Sample and sampling techniques
For statistical reasons, a minimum of eight countries of different HDI across the world (two from each of the four HDI categories) was selected through simple random sampling technique. Disproportionate stratified random sampling technique was used to select three referral/general and two specialized hospitals from each country. From each hospital, five blood prescribing clinicians and five nurses (regularly involved in bedside transfusion practice) were selected. This gave a statistical minimum total number of 50 participants from each country.
For each of the eight countries, a Coordinator was selected through the existing transfusion medicine network of the key investigators. The Coordinators were directly responsible for the introduction, sampling, and implementation (distribution and collection of the questionnaires) in their respective country and communicated with the key investigators.
Study variables
The independent variables in this study were the levels of awareness, accessibility, and utilization of continuous e-learning and education, while the dependent variable was the expressed effect on quality and efficacy of clinical care.
Instrumentation
A four-part survey questionnaire was developed based on a review of relevant literature (Figure S1). Each part utilizes a Likert-type scale to elicit responses from blood prescribing clinicians and nurses on the levels of awareness, accessibility, and utilization of e-learning and continuous education programs in transfusion medicine. For the levels of awareness and accessibility, there are four possible responses – strongly agree (SA), agree (A), disagree (D), and strongly disagree (SD). For the level of utilization, the four possible responses are – most like me (MLM), like me (LM), least like me (LLM), and not like me (NLM), where me=continued medical education and e-learning.
Each of these responses is numerically coded for analysis, thus, SA=4, A=3, D=2 and SD=1, and MLM=4, LM=3, LLM = 2, and NLM =1.
Validation of the instrument (validity and reliability)
All items in the instrument were drawn after extensive literature search. Several measures have been explored to insure validity and reliability of the research instrument. Validity of the instrument was examined by a panel of selected experts who are members of the research team. Each panelist did examine the instrument for content, clarity, and appropriateness to determine the proper structuring, adequacy, and contents validity of each item in the instrument and to ensure that the instrument measures what it was actually expected to measure.
In order to ensure the reliability of the instrument, a pilot study was carried out on some clinicians who were not included in the real study. These clinicians did share similar characteristics with the subjects of the study. Cronbach’s coefficient statistical procedure28 was computed based on responses with a view to arriving at the alpha values, which helped to determine the internal consistency and item-by-item reliability.29
Procedure for administration of the instrument
The coordinators did approach the Chief Medical Directors of the referral/general and specialized hospitals to be included in the study with a letter of introduction and solicited for their cooperation and assistance. Also, the coordinators did employ services of some postgraduate medical students as research assistants who were contacted during the pilot study. They were given orientation on how to handle the administration of the questionnaires. An electronic copy of the questionnaire was sent to each coordinator of the selected countries. The questionnaires were administered to blood prescribing clinicians and nurses preferably electronically or otherwise as a hard copy. Respondents were requested to complete the questionnaire within a week. The coordinator did collect the completed questionnaires and forwarded them to the key investigators. Only appropriately and completely filled questionnaires were used for data analysis.
Methods of data analysis
This research involved making careful descriptions of an educational phenomenon, which within the context of this study are continuous e-learning and education. Descriptive statistics, such as mean and standard deviations, were adopted in the analysis of levels of awareness, accessibility, and utilization of continuous e-learning and education programs among the blood prescribing clinicians and nurses. Descriptive statistics were equally used to analyze the demographical data of the participants. The descriptive part of the research provided descriptions in the form of statistics such as frequencies, ranking, means, and percentages.
Since the first three research questions had to do with relationship, Pearson product-moment correlation coefficient (PPMCC)30 was used to answer these questions. For the causal comparative part of the research, the blood-prescribing clinicians and nurses were categorized into four groups based on the HDI. The groups consisted of blood-prescribing clinicians and nurses in very high HDI, high HDI, medium HDI, and low HDI. Comparisons were then made on the levels of awareness, accessibility, and utilization of continuous e-learning and education.
In view of the comparisons earlier, the analysis of variance (ANOVA),31 for testing for significant differences between the means of two or more groups, was used to test the seven hypotheses at ≤0.05 level of significance.
Results
Participating countries
To allow the calculated statistical minimum of two countries per HDI group, four countries in each group with a geographical spread over the continents were invited: VH-HDI – Australia, Canada, Japan, USA; H-HDI – Brazil, Iran, Malaysia, Montenegro; M-HDI – Kyrgyzstan, Mongolia, South Africa, Uzbekistan; L-HDI – Nigeria, Pakistan, Sudan, Uganda.
Although initially all countries responded positively, some were not able to organize the set up – selection of hospitals, motivation of a contact person, clinicians and nurses, distribution of the questionnaires, and instruction on how to complete.
Countries that managed to participate with at least one hospital, were: VH-HDI (6) – Japan (5), USA (1); H-HDI (14) – Brazil (4), Iran (5), Montenegro (5); M-HDI (20) – Kyrgyzstan (5), Mongolia (5), South Africa (5), Uzbekistan (5); L-HDI (20) – Nigeria (5), Pakistan (5), Sudan (5), Uganda (5).
It was decided to include all responses, because they all met the criteria of completeness for evaluation.
Sociodemographic background
Responses of in total 264 clinicians and nurses and 60 hospitals from the 13 countries were evaluated; 164 from referral/general hospitals and 100 from specialized clinics, 102 males and 162 females. Years of experience of the clinicians and nurses involved varied from 1–10 years (100) to 31–40 years (33). There were 77 L-HDI, 91 M-HDI, 48 H-HDI, and 48 VH-HDI respondents involved. The spread over the different blood consuming clinical specialties/departments is presented in Table S1.
Research questions
The answers to the three main research questions, following a general evaluation (n=264), were:
- What is the relationship between the level of awareness of continuous e-learning and education on the quality and efficacy of clinical blood use?
There was a weak though significantly positive relationship (p=0.026, r=0.137, df=262) between level of awareness of continuous e-learning/education (mean 31.48; sd 5.360) among participating clinicians and nurses and quality and efficacy of clinical use of blood (mean 27.10; sd 4.944) in the hospitals involved, irrespective of the HDI of the participating country (Table S2).
- What is the relationship between the level of accessibility of continuous e-learning and education on the quality and efficacy of clinical blood use?
There was a highly significant positive relationship (p=0.003, r=0.184, df=262) between accessibility to continuous e-learning and education (mean 26.34; sd 3.863) and quality and efficacy of clinical use of blood (mean 27.10; sd 4.944) in the hospitals involved, irrespective of the HDI of the participating country (Table S3).
- What is the relationship between the level of utilization of continuous e-learning and education on the quality and efficacy of clinical blood use?
Although weak, there was no significant relationship (p=0.357, r=0.057, df=262) between level of utilization of continuous e-learning and education (mean 33.27; sd 6.250) and quality and efficacy of clinical use of blood (mean 27.10; sd 4.944) in the hospitals involved, irrespective of the HDI of the participating country (Table S4).
Hypotheses
Seven hypotheses were formulated, three in relation to the country level of HDI (very high, high, medium, and low) and four in relation to the different blood consuming clinical specialties/departments (Pediatrics, Gynecology/Obstetrics, Surgery, Traumatology, Internal Medicine, Hemato-oncology, and other specialties/departments) in the participating hospitals.
HDI and level of awareness, accessibility, and utilization
Hypothesis 1 – H0=There are no differences among the prescribing clinicians and nurses between the level of awareness of continuous e-learning and education, and the human development index (HDI).
ANOVA in level of awareness between the four HDI groups (Table S5) showed an overall significant difference at p=0.000 with F=53.942. To ascertain where the significant differences were, a post hoc test was done using the Scheffe post hoc criterion for significance32 (Table S6). Level of awareness of continuous e-learning and education among clinicians and nurses in the L-HDI countries is significantly lower compared with those in the medium, high, and very high HDI countries (p=0.000). Level of awareness of those in the medium HDI countries showed no difference compared with those in the high and very high HDI countries (p=0.783 and 0.367, respectively). Level of awareness of participating clinicians and nurses in the high and very high HDI countries showed a significantly higher level compared with the medium and low HDI countries (p=0.000); there was no difference between those in the high and very high countries (p=0.935).
The H0 hypothesis on awareness was rejected.
Hypothesis 2 – H0=There are no differences among the prescribing clinicians and nurses between the level of accessibility of continuous e-learning and education, and the human development index (HDI).
ANOVA in level of accessibility between the four HDI groups (Table S7) showed an overall significant difference at p=0.000 with F=38.582. To ascertain where the significant differences were, a post hoc test was done using the Scheffe post hoc criterion for significance (Table S8). Level of awareness of continuous e-learning/education among clinicians and nurses in the L-HDI countries is significantly lower compared with those in the high and very high HDI countries (p=0.000), but did not show a significant difference with those in the medium HDI countries (p=0.905). Similarly level of awareness of those in the medium HDI countries was significantly lower compared with those in the high and very high HDI countries (p=0.000). The level of awareness of participating clinicians and nurses in the high and very high HDI countries showed a significantly higher level compared with the medium and low HDI countries (p=0.000); there was no difference between those in the high and very high countries (p=0.867).
The H0 hypothesis on accessibility was rejected.
Hypothesis 3 – H0=There are no differences among the prescribing clinicians and nurses between the level of utilization of continuous e-learning and education, and the human development index (HDI).
ANOVA in level of utilization between the four HDI groups (Table S9) showed an overall significant difference at p=0.000 with F=38.858. To ascertain where the significant differences were, a post hoc test was done using the Scheffe post hoc criterion for significance (Table S10). Level of awareness of continuous e-learning/education among clinicians and nurses in the L-HDI countries is significantly lower compared with those in the medium and high HDI countries (p=0.000), but surprisingly did not show a significant difference with those in the very high HDI countries (p=0.658). Level of awareness of those in the medium HDI countries was significantly lower compared with those in the very high HDI countries (p=0.000) but did not show a difference with those in the high HDI countries (p=0.205). Level of awareness of participating clinicians and nurses in the high HDI countries showed a significantly higher level compared with the very high HDI countries (p=0.000).
The H0 hypothesis on utilization was rejected.
Clinical specialty/department and level of awareness, accessibility, and utilization
Hypothesis 4 – H0=There are no differences among the prescribing clinicians and nurses between the level of awareness of continuous e-learning and education, and clinical specialty/department.
An ANOVA was run to determine a significant difference in level of awareness to continuous e-learning and education based on clinical specialty/department (Table S11). There was no significant difference in level of awareness of e-continuous learning (F[6,257]=3.525, p=0.052) among clinicians and nurses based on specialty/department. There was no need for post hoc testing since the F-value is not significant.
The H0 hypothesis on awareness was accepted.
Hypothesis 5 – H0=There are no differences among the prescribing clinicians and nurses between the level of accessibility to continuous e-learning and education, and clinical specialty/department.
An ANOVA was done to determine a significant difference in level of accessibility to continuous e-learning and education based on clinical specialty/department (Table S12). There was significant difference in level of accessibility to e-continuous learning (F[6,257]=6.444, p=0.000) based on clinical specialty/department. To ascertain where the significant difference was, a post hoc test was done using the Scheffe post hoc criterion for significance as shown in Table S13. Mean difference in level of accessibility to continuous e-learning and education among clinicians and nurses based on clinical specialty/department was significant between Gynecology/Obstetrics and others (p<0.05), Traumatology and others (p=0.05) as well as between Hemato-oncology and Gynecology/Obstetrics (p=0.05), respectively.
The H0 hypothesis on level of accessibility was rejected.
Hypothesis 6 – H0=There are no differences among the prescribing clinicians and nurses between the level of utilization of continuous e-learning and education, and clinical specialty/department.
An ANOVA was done to determine a significant difference in level of utilization of continuous e-learning and education based on clinical specialty/department (Table S14). There was significant difference in the level of utilization to e-continuous learning (F[6,257]=13.704, p=0.000) based on clinical specialty/department. However, in order to ascertain where the significant difference was, a post hoc test was done using the Scheffe post hoc criterion for significance as shown in Table S15. Mean difference in level of utilization of continuous e-learning and education by clinicians and nurses based on clinical specialty/department was significant between Gynecology/Obstetrics and Pediatrics (p<0.05), Gynecology/Obstetrics and Surgery (p=0.05), Gynecology/Obstetrics and Hemato-oncology (p=0.05) and Gynecology/Obstetrics and Internal Medicine (p=0.05), Hemato-oncology and others (p=0.05), Internal Medicine, and others (p=0.05) respectively.
The H0 hypothesis on level of utilization was rejected.
Hypothesis 7 – H0=There are no differences among the prescribing clinicians and nurses between the quality of clinical use of blood and clinical specialty/department.
An ANOVA was done to determine a significant difference in quality of clinical blood use among blood prescribing clinicians based on clinical specialty/department (Table S16). There was significant difference in quality of clinical blood use (F[6,257]=9.677, p=0.000) based on clinical specialty/department. To ascertain where the significant difference was, a post hoc test was done using the Scheffe post hoc criterion for significance as shown in Table S17. Mean difference in quality of clinical blood use among prescribing clinicians and nurses based on clinical specialty/department was significant between Pediatrics and others (p<0.05), Hemato-oncology and others (p<0.05), and Surgery and others (p<0.05).
The H0 hypothesis on quality was rejected.
Discussion
All over the world, the clinical interface and in-hospital transfusion practice are still the weakest link in the vein-to-vein transfusion chain. Since the mystery of incompatibility was unveiled by Landsteiner,33 attention was driven away from the direct patient treatment into immunohematology and in particular blood group serology as the major key to blood safety. With the recognition of transmissibility of infectious agents by blood, starting with syphilis in the 1940s, followed by Malaria, Hepatitis B, and non-A, B or C, and in the early 1980s HIV and HTLV, and prions in the 1990s, many more have emerged.34 That initiated an epoque with a focus on laboratory detection and technical quality control and assumed inactivation of these infectious agents driven by the hypothetic paradigm of zero-risk. During the past decades, more focused attention for the bedside aspects of transfusion medicine has started to develop as reflected in the publication of textbooks on clinical practice of blood transfusion and the development of specific teaching material such as the WHO DLM on clinical use of blood3,35–39 published in different languages, and the series of proceedings (since 1980) of the Groningen Symposia on Blood Transfusion published (Martinus Nijhoff, Kluwer Academic Publishers, and Springer) between 1980 and 2004 in the series Developments in Hematology and Immunology.40 These symposia always concluded with a session on the clinical application of the highlighted theme. The obvious reason was in the globally observed and experienced knowledge gap in the peer group of prescribing clinicians and transfusion involved nursing staff. Despite the fact that over these decades, an increasing volume of printed and e-learning education material has been published and offered, and a rapidly spreading dogma on patient blood management is occurring, key weaknesses still are awareness, accessibility, and utilization of the material. This is reflected in the outcome of the survey, with differences between the clinical transfusion practitioners in the various HDI clusters of countries.
The three research questions resulted in a positive, weak, but significant relationship between level of awareness of, accessibility to, and utilization of continuous e-learning and education among blood prescribing clinicians and the quality of clinical use of blood in the selected countries.
The more specific hypotheses of our study showed:
- A significant difference in level of awareness of, continuous e-learning and education among blood prescribing clinicians based on HDI. Level of awareness of e-continuous learning among blood prescribing clinicians is significant between L-HDI and each of M-HDI, H-HDI, and VH-HDI.
- A significant difference in level of accessibility to continuous e-learning and education based on HDI. Mean difference in level of accessibility to e-continuous learning among blood prescribing clinicians is significant in the selected countries except between L-HDI and M-HDI, as well as between H-HDI and VH-HDI, respectively.
- A significant difference in level of utilization of continuous e-learning and education based on HDI. Mean difference in level of utilization of e-continuous learning is significant among the selected countries except between L-HDI and VH-HDI, as well as between M-HDI and H-HDI, respectively.
- There was no significant difference in level of awareness of continuous e-learning and education among blood prescribing clinicians solely based on specialty/department.
- However, there was a significant difference in level of accessibility to continuous e-learning and education based on clinical specialty/department. Mean difference in level of accessibility to continuous e-learning and education among blood prescribing clinicians based on clinical specialty/department is significant, but weak between Gynecology/Obstetrics and others, Traumatology and others as well as between Hemato-oncology and Gynecology/Obstetrics, respectively.
- There is also a significant difference in level of utilization of continuous e-learning and education based on clinical specialty/department. Mean difference in level of utilization of continuous e-learning and education by blood prescribing clinicians based on clinical specialty/department is significant, but weak between Gynecology/Obstetrics and Pediatrics, Gynecology/Obstetrics and Surgery Gynecology/Obstetrics and Hemato-oncology and Gynecology/Obstetrics and Internal Medicine, Hemato-oncology and others, Internal Medicine and others, respectively.
- A significant difference in quality of clinical use of blood based on clinical specialty/department. Mean difference in quality of clinical blood use among blood prescribing clinicians based on clinical specialty/department is significant, but weak between Pediatrics and others, Hemato-oncology and others, and Surgery and others, respectively.
These results reflect the difficulties in the less developed part of the world, in particular the low HDI countries, in basic academic education and postgraduate clinical specialization with respect to availability and access to continuous e-learning and education are still problematic. Acquiring and perceiving an adequate clinical transfusion medicine knowledge base, and practical utilization and maintaining of what has been learned to secure quality of clinical care in blood transfusion remains a major concern.
Limitations
However, the study has its limitations in the overall number of participating countries, and the restriction of participation; VH and H-HDI group response was not optimal (VH-HDI with two countries, H-HDI with three countries, and, respectively, 6 and 14 hospitals). Some countries did not manage to include the statistical calculated number of hospitals needed, and prescribing clinicians and nurses involved. There was significantly more interest and enthusiasm among the medium and low-HDI participants in collaboration and coordination to collect the information needed. Nevertheless, a substantial data base was collected to allow a reasonably accurate picture of the current situation with respect to awareness, accessibility, and utilization of continuous e-learning and education in clinical use of blood and blood products (hemotherapy) and the value of quality in patient blood management as an integral part of health care in the different specialties.
Conclusion
The higher the HDI level the better is the awareness, accessibility, and utilization of continuous education, both through e-learning and conventional in teaching curricula. This has an immediate impact on the quality of clinical care and in particular on supportive hemotherapy and the development of patient blood management systems. There is a better awareness among clinicians routinely prescribing blood compared with others involved only incidentally in blood transfusion.
Accessibility of e-learning depends highly on the presence of a sustained societal infrastructure which is less guaranteed in the low and medium HDI countries; reliable power supply, maintenance of hardware tools, and updated software programs, together with the necessary knowledge and skills of e-technology are prominent factors.18
Recommendations for policy consideration
Policy makers at higher education level are urged to realize that continuous e-learning and education are a sine qua non to effective and quality clinical use of blood and related health care.41
- Starting at undergraduate medical and nursing schools and continuing at postgraduate vocational medical specialization institutes, principles of clinical transfusion practice should be comprehensively included through appropriate and timely curricula.
- When practicing blood transfusion, continuous e-learning and education is paramount to maintain a high level of academic knowledge of transfusion medicine and related patient blood management principles to guarantee quality care.
- Creation of a technical climate to guarantee access to e-learning courses and materials.
- Stimulation of national and international exchange of e-learning programs focused on continuing education.
- Creation of an e-learning mentoring network through professional societies, associations, and education institutes.
- It is also recommended that clinicians should endeavor to update and maintain their knowledge and practice through e-continuous learning as a form of policy and related strategy.
Acknowledgments
The authors wish to acknowledge the contribution of all participating clinicians and nurses for their time and commitment completing the survey questionnaire. The Department of Educational Management, University of Lagos, Akoka-Yaba, Lagos, Nigeria, is thanked for her support and statistical analysis of the data collected.
Author contributions
Cees Th Smit Sibinga and Maruff A Oladejo contributed to the design of the study, the implementation, coordination, data management, and the writing of the manuscript. Olamide Hakeem Adejumo, Quentin Eichbaum, Midori Kumagawa, Shuichi Kino, Sima Zolfaghari, Silvano Wendel, Gordana Rasovic, Namjil Erdenebayar, Maya Makhmudova, Loyiso Mpuntsha, Charlotte Ingram, Bakyt B Kharabaev, Isaac Kajja, Zainab Sanji, and Maria M M Satti contributed to selection of participants, collection of data (questionnaires), and coediting of the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
WHO. Report of the Global Blood Safety Initiative (GBSI) Informal Consultation on “Assessment of Training Needs in Transfusion Medicine”, WHO LBS/92.6, 1992. Geneva: WHO; 1992. | ||
WHO. Report of the Global Blood Safety Initiative (GBSI) Informal Consultation on “Collaboration in Training in Transfusion Medicine”, WHO LBS/92.7, 1992. Geneva: WHO; 1992. | ||
WHO [homepage on the Internet]. WHO Distance Learning Material, Accessible through Education and Training in Blood Transfusion Safety. Available from: www.who.int/bloodsafety/publications/en/index.html. Accessed May 31, 2017. | ||
WHO. Quality Management for Blood Transfusion Services. Facilitator’s Toolkit (CD-ROM). WHO/EHT/04.13, 2004. Geneva: WHO; 2004. | ||
Council of Europe EDQM [webpage on the Internet]. Reports. Available from: https://www.edqm.eu/en/blood-transfusion-reports-70.html. Accessed May 31, 2017. | ||
WHO. Report of the Fifth General Meeting of the Global Collaboration for Blood Safety; 2003. Available from: http://www.who.int/bloodsafety/publications/en/GCBS_Report_DEC2003.pdf?ua=1. Accessed May 31, 2017. | ||
WHO. Report of the Fifth General Meeting of the Global Collaboration for Blood Safety; 2004. Available from: http://www.who.int/bloodsafety/GCBS_Report_NOV_2004.pdf?ua=1. Accessed May 31, 2017. | ||
Directive 2002/98/EC of the European Parliament and the Council of 27 January 2003, setting standards of quality and safety for the collection, testing, processing, storage and distribution of human blood and blood components and amending Directive 2001/83/EC. OJ L33. 8.2.2003:30-40. | ||
AABB [homepage on the Internet]. Available from: http://www.aabb.org/development/education/Pages/default.aspx. Accessed May 31, 2017. | ||
BBTS [homepage on the Internet]. Available from: http://www.bbts.org.uk/education. Accessed May 31, 2017. | ||
Australian Red Cross Blood Service. Online learning. Available from: https://transfusion.com.au/education. Accessed May 31, 2017. | ||
Smit Sibinga CTh, Pitman JP. Transmission of HIV through blood – how to bridge the knowledge gap. In: Nancy D, editor. HIV and AIDS – Updates on Biology, Immunology, Epidemiology and Treatment Strategies. (Chap. 23). Rijeka: InTech; 2011:583–618. ISBN: 978-953-307-665-2. | ||
EuBis [homepage on the Internet]. Available from: www.eubis-europe.eu/objectives.ph. Accessed May 31, 2017. | ||
BloodSafe elearning Australia [homepage on the Internet]. Available from: https://bloodsafelearning.org.au/our-courses/. Accessed May 31, 2017. | ||
Blood Systems [homepage on the Internet]. Available from: http://www.bloodsystemseducation.org/. Accessed May 31, 2017. | ||
EUR-Lex.europa.eu. Commission Directive 2005/62/EC of 30 September 2005 implementing Directive 2002/98/EC of the European Parliament and of the Council as regards Community standards and specifications relating to a quality system for blood establishments. Available from: http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2005:256:0041:0048:EN:PDF. Accessed May 31, 2017. | ||
Smit Sibinga CTh, Oladejo MA. Bridging the knowledge gap in management and operations of transfusion medicine: planning, policy and leadership. J Cases Inform Technol. 2013;15:69–82. | ||
Smit Sibinga CTh. Post-academic masters course in management of transfusion medicine: why the difference in access to the e-learning between countries? In: Greener S, Rospigliosi A, editors. In: Proceedings 10th ECEL. Brighton, UK: Academic Publishing Limited; Reading UK; 2011:776–779. | ||
Murphy MF, Saxena S, Smit Sibinga CTh. Patient safety and quality management at the clinical interface. In: Smit Sibinga CTh, editor. Quality Management in Transfusion Medicine. Hauppage, NY, USA: Nova Science Publ. Inc.; 2013:283–314. | ||
AABB. Building a Better Patient Blood Management Program. Identifying Tools, Solving Problems and Promoting Patient Safety. Bethesda, MD: AABB Press; 2015. | ||
Frank SM, Waters JH, editors. Patient Blood Management: Multidisciplinary Approaches to Optimize Care. Bethesda, MD: AABB Press; 2016. | ||
Eichbaum Q, Murphy M, Liu Y, et al. Patient blood management: an international perspective. Anesth Analg. 2016;123(6):1574–1581. | ||
AABB [webpage on the Internet]. Education. Available from: http://www.aabb.org/development/education/Pages/default.aspx. Accessed May 31, 2017. | ||
WHO. The Clinical Use of Blood, Aide Mémoire for National Health Programs. WHO/EHT/04.07. Geneva: WHO; 2004. | ||
WHO. Aide Mémoire on National Blood Programme. Geneva: WHO; 2002. | ||
UNDP [webpage on the Internet]. Human Development Index (HDI). Available from: http://hdr.undp.org/en/content/human-development-index-hdi. Accessed May 31, 2017. | ||
Kerlinger FNH. Foundation of Behavioural Research. New York, NY: Holt, Rinehart and Winston; 1992. | ||
Cronbach LJ, editor. Essentials of Psychological Testing. New York, NY: Harper & Row; 1990. | ||
Borg WR, Gall JP, Gall MD. Educational Research: An Introduction. 6th ed. White Plains, NY, USA: Longman Publishers; 1996. | ||
Leard Statistics [webpage on the Internet]. Pearson Product-Moment Correlation. Available from: https://statistics.laerd.com/statistical-guides/pearson-correlation-coefficient-statistical-guide.php. Accessed May 31, 2017. | ||
Leard Statistics [webpage on the Internet]. One-way ANOVA. Available from: https://statistics.laerd.com/statistical-guides/one-way-anova-statistical-guide.php. Accessed May 31, 2017. | ||
Statisticshowto [webpage on the Internet]. Post-Hoc Definition and Types of Post Hoc Tests. Available from: http://www.statisticshowto.com/post-hoc/#PHscheffes. Accessed May 31, 2017. | ||
Landsteiner K. Uber Agglutinationsverscheinungen normalen menschlichen Blutes [Normal human agglutination blood disorders]. Wien Klin Wochenschr. 1901;14:1132. German. | ||
Smit Sibinga CTh, Dodd RY, editors. Transmissible Diseases and Blood Transfusion. Dordrecht, Boston, London: Kluwer Academic Publ; 2002. | ||
Aide Mémoire for National Health Programmes. The Clinical Use of Blood. WHO/EHT/04.07. Geneva: World Health Organization; 2003. | ||
Aide Mémoire for National Health Authorities and Hospital Management. Clinical Transfusion Process and Patient Safety. WHO/EHT/10.05. Geneva: World Health Organization; 2010. | ||
WHO. Developing a National Policy and Guidelines on the Clinical Use of Blood. Recommendations. WHO/BTC/BTS/01.3. Geneva: World Health Organization; 2001. | ||
WHO. The Clinical Use of Blood in Medicine, Obstetrics, Paediatrics, Surgery & Anaesthesia, Trauma & Burns. DL Module. Geneva: WHO; 2002. | ||
WHO. The Clinical Use of Blood. Handbook. Geneva: WHO; 2002. | ||
Springer [webpage on the Internet]. Oncology & Hematology. Available from: http://www.springer.com/gp/medicine/oncology-hematology. Accessed May 31, 2017. | ||
Oladejo MA, Smit Sibinga CTh. Policy implications of bridging the clinical transfusion medicine gap through e-learning. In: Belthuis, Hans, editors. In: Proceedings 12th ECEL 2012. Vol. 4. Reading, England; ACI; 2012:638–640. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.