Back to Journals » Patient Preference and Adherence » Volume 19
A Gamification mHealth Intervention to Enhance Adherence to Personalized Exercise for Older Adults with Chronic Diseases: A Randomized Controlled Trial Protocol
Authors Zhang G ![]() , Xia Y, Li X
, Xia Y, Li X ![]() , Zhang Y, Xu X, Sun T
, Zhang Y, Xu X, Sun T
Received 16 June 2025
Accepted for publication 6 October 2025
Published 11 October 2025 Volume 2025:19 Pages 3145—3157
DOI https://doi.org/10.2147/PPA.S547361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Guoli Zhang,1 Yuxin Xia,1 Xuelei Li,1 Yun Zhang,1 Xuejie Xu,1 Ting Sun1,2
1School of Nursing, Bengbu Medical University, Bengbu, Anhui, People’s Republic of China; 2Joint Research Center for Regional Diseases of IHM, Bengbu Medical University, Bengbu, Anhui, People’s Republic of China
Correspondence: Ting Sun, School of Nursing, Bengbu Medical University, Bengbu, Anhui, People’s Republic of China, Tel +86 18005529759, Email [email protected]
Background: Despite proven benefits, intelligent personalized exercise prescription (IPEP) adherence remains low in middle-aged and older adults with chronic diseases (MOACD). Research evidence suggests that mobile health (mHealth)-based gamification interventions can improve participation in physical activity; however, their effects on adherence to IPEP remain unclear. Moreover, most studies report that adherence often declines rapidly once gamification interventions end, and no effective strategies have been proposed to address this issue. This study embeds the Octalysis gamification framework into a smartphone-based app to investigate the effects of an mHealth-based gamification intervention on adherence to IPEP among MOACD, as well as on related physical and psychological outcomes. Additionally, the study examines whether combining gamification interventions with health education can help sustain adherence after the intervention concludes.
Methods: We propose a double-center, single-blind, three-arm randomized controlled trial. We will recruit 132 MOACD who will participate in dyads (66 pairs). Participants will be randomly assigned to three groups: a non-gamification group, a gamification group, or a health education plus gamification group. The intervention will last for 12 weeks, followed by a 12-week follow-up period. The primary outcome is adherence to IPEP, defined as the proportion of days on which participants completed their prescribed exercise tasks at 12 and 24 weeks. Secondary outcomes include biomedical risk factors, sedentary behavior, sleep quality, self-efficacy, intrinsic motivation, patient satisfaction, and the acceptability of the intervention.
Conclusion: This trial employs the Octalysis gamification framework to design an intervention aimed at enhancing adherence to the IPEP. The findings may inform the development of scalable digital interventions to promote physical activity and long-term adherence among MOACD.
Keywords: smartphone app, gamification design, low adherence, Octalysis gamification framework, self-efficacy, intrinsic motivation
Introduction
The global burden of chronic diseases is steadily rising, presenting unprecedented challenges to public health systems.1 According to reports from the World Health Organization, chronic diseases accounted for 38% of global deaths in 2021.2 Physical inactivity is recognized as a major modifiable risk factor for numerous chronic conditions, including cardiovascular disease and type 2 diabetes.3 Exercise prescriptions, as the cornerstone of non-pharmacological interventions,4 have demonstrated significant efficacy in glycemic control, blood pressure reduction, and physical function improvement.5–8 Recent advances in artificial intelligence (AI) and big data analytics have facilitated the development of intelligent personalized exercise prescription (IPEP). For example, Sun et al developed a cloud platform-based electronic health promotion system that provides tailored exercise prescriptions for older adults.9 Similarly, Tan et al and Gao et al employed AI and machine learning techniques to develop intelligent exercise prescription systems for alleviating psychiatric symptoms in mental health patients and for preventing cardiovascular disease in cancer patients, respectively.10,11 These systems not only retain the effectiveness of traditional exercise prescriptions but also reduce associated safety risks.9,12 However, compared to the low adherence to traditional exercise prescriptions,13,14 IPEP also faces similar issues.9 This scientific and personalized transformation appears to be insufficient for fostering sustained engagement, thereby hindering the full realization of the maximum potential of IPEP. Therefore, there is an urgent need for effective interventions to enhance adherence to IPEP.
Mobile health (mHealth)-based gamification represents a promising approach to addressing behavioral adherence challenges. It involves applying game design elements (such as badges, progress bars, and leaderboards) in non-game contexts (such as education, management, and healthcare) to enhance user engagement.15 Compared to other behavioral interventions like financial incentives or motivational interviewing, gamification offers a particularly scalable and engaging approach for delivery via digital platforms, making it well-suited for mHealth applications.16,17 Several reviews have shown that gamification elements can create a game-like experience that influences user behavior and motivation, thereby promoting physical activity.18–20 However, the impact of gamification on adherence to IPEP remains unclear. Meanwhile, numerous studies have reported that while gamification interventions may produce immediate advantages, user adherence frequently diminishes swiftly to baseline levels following the conclusion of the intervention.21–23 Some researchers attribute this decline to the use of extrinsic motivators in gamification, such as point systems, which may undermine users’ intrinsic motivation to exercise.24 Despite this being a widely recognized issue, few studies have prospectively proposed or tested solutions, as the research focus has predominantly been on immediate, in-intervention effects rather than long-term sustainability. Notably, health education, as a cognitive intervention strategy, may be able to compensate for this deficiency. According to self-determination theory (SDT), when individuals comprehend the intrinsic value of a behavior (such as the role of exercise in preventing and managing certain diseases), their intrinsic motivation to engage in that behavior is strengthened.25 Thus, we hypothesize that integrating health education could mitigate the negative effects of gamification by strengthening intrinsic motivation, although experimental evidence supporting this combined approach remains limited. It is important to acknowledge, however, that introducing mHealth and gamification to older adults presents unique challenges. Potential barriers related to digital literacy, smartphone accessibility, and technology acceptance in this population must be considered when designing and implementing such interventions.
Current gamification strategies aimed at promoting physical activity primarily rely on traditional behavior change theories, with few studies applying gamification-specific theories or frameworks.20 Octalysis, an emerging gamification framework, comprises eight core drives.26 It proposes that motivation can only be triggered—and behavior change facilitated—when users experience these core drives. Although gamification designs based on this framework have been applied in educational settings and are gaining popularity, they have not yet been used to promote physical activity or improve exercise adherence.27,28 Therefore, we developed a mobile application named “Xiyou Sports” based on the Octalysis framework to address this research gap. To our knowledge, this will be the first study to apply the Octalysis framework to enhance IPEP adherence in chronic disease management. Furthermore, the intervention adopts a dyad-based (team) design, which is rooted in the Octalysis core drives of “Social Influence and Relatedness” and “Loss and Avoidance”. This approach operationalizes the well-established principles of cooperation and accountability, which are known to be powerful motivators for health behavior change.29 We hypothesize that, compared to the non-gamification group, participants in the gamification group will exhibit higher adherence to IPEP. A secondary hypothesis is that incorporating health education may help counteract the negative effects of extrinsic motivators in gamification by enhancing intrinsic motivation, thereby sustaining adherence during the follow-up period. This study will provide critical insights for developing effective, scalable, and potentially cost-effective digital interventions to promote sustained physical activity.
Methods
Study Design
This is a double-center, single-blind, three-arm randomized controlled trial comprising a 2-week baseline phase, a 12-week intervention phase, and a 12-week follow-up phase. The study aims to evaluate the effects of an mHealth-based gamification intervention on adherence to IPEP, biomedical risk factors, sedentary behavior, sleep quality, self-efficacy, and intrinsic motivation. In addition, it examines the impact of integrating health education with gamification intervention on adherence to IPEP during the follow-up period.
Prior to the intervention, 132 eligible middle-aged and older adults with chronic diseases will be recruited from two community health service centers. All participants will undergo a two-week baseline assessment of adherence to their IPEP. During this period, researchers will provide each participant with an IPEP and instruct them to follow it daily. Participants will also be informed that they must report their daily exercise completion status via WeChat by 8:00 PM each day. Researchers will record the task completion rate as a measure of baseline adherence. After the baseline phase, participants will be stratified by adherence level (low, medium, or high) and randomly assigned in a 1:1:1 ratio to one of three groups: non-gamification, gamification, or health education plus gamification. Given the intervention’s team-based design, each participant will be required to invite an eligible friend or family member to form a two-person team before enrollment. Each team will serve as the minimum unit for stratification and randomization. Following group allocation, all participants will be invited to their respective community health service centers to install the “Xiyou Sports” app under researcher supervision and complete registration and training on app features. Meanwhile, data collectors will use paper questionnaires to gather baseline information from participants and inform them of the specific dates for the 12-week and 24-week follow-ups. If participants are unable to attend the follow-ups on time due to special circumstances, they may contact the researchers in advance to reschedule. This study protocol has been reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2025 statement.30 Figure 1 presents a flowchart of the study design.
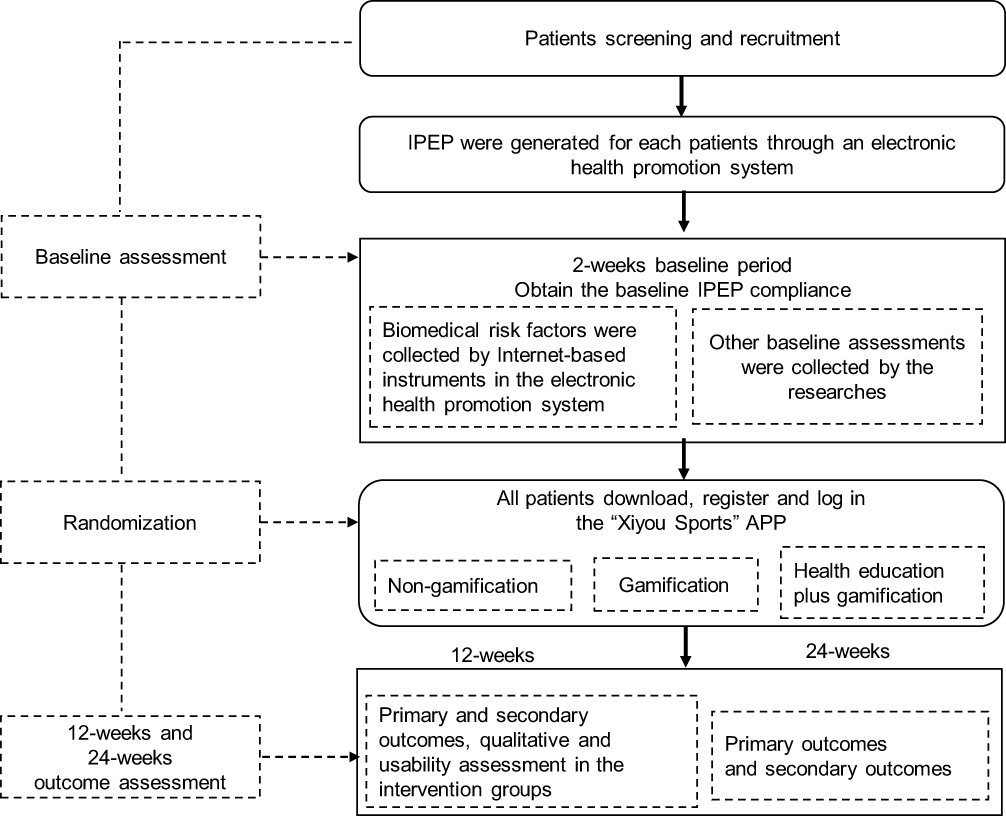 |
Figure 1 Flowchart of the study design. Abbreviation: IPEP, intelligent personalized exercise prescription. |
The IPEP used in this study is based on an electronic health promotion system deployed in community health service centers. This system consists of four components: (1) a registration system, (2) internet-based questionnaires, (3) internet-connected instruments, and (4) a cloud platform. Before generating an IPEP, users must complete real-name registration within the system. They then fill out a series of online questionnaires to collect data on health-related lifestyle factors, chronic disease history, and family medical history. Subsequently, users undergo assessments using internet-based instruments that measure body composition, cardiovascular function, and related metrics. Finally, all data are uploaded to the cloud platform, which integrates and analyzes the information to generate a personalized exercise prescription. Further details about the electronic health promotion system can be found in previous studies.9,31
Eligibility and Recruitment
The inclusion criteria were as follows: (1) middle-aged or older adults (aged ≥45 years) diagnosed by a medical institution with at least one common chronic condition (eg, hypertension, coronary heart disease, or diabetes); (2) ability to invite a relative or friend who also meets criterion (1) to form a two-person team for participation; (3) ownership of an Android smartphone and sufficient proficiency in using mobile applications (eg, taking photos); (4) adequate cognitive and communication abilities; and (5) sufficient physical mobility to perform routine exercise. The exclusion criteria were (1) presence of neurological disorders affecting motor function; (2) implantation of a pacemaker; (3) a history of epilepsy, or serious primary diseases of the heart, liver, kidneys, or metabolic system that make exercise unsuitable; and (4) participation in other clinical studies.
Participants were recruited from two community health service centers in Anhui Province through telephone invitations from researchers or verbal invitations from local healthcare staff. To encourage community residents to participate, free health checkups and assessments were provided to all community residents who attended. For individuals meeting the eligibility criteria, the study details were explained, and those who agreed to participate signed an informed consent form. It will be clearly communicated to participants that they have the right to withdraw their consent and discontinue participation at any time, for any reason, without penalty. Participants can initiate withdrawal by contacting a member of the research staff via phone. Furthermore, the research team will monitor adherence via the backend management system. If a participant is observed to be inactive for a full week, a researcher will contact them by phone to offer a reminder and inquire if they wish to continue or formally withdraw.
Specific consent for the daily photo uploads will be a key component of the informed consent process. It will be explicitly stated that: (1) the sole purpose of the photos is to verify daily exercise completion; (2) to protect privacy, participants will be instructed not to include their faces or any other identifiable features in the photos; (3) the images will be stored on the secure app backend, with access restricted to the principal investigator and designated data managers; and (4) all photos will be permanently deleted at the end of the study’s data retention period.
Sample Size Calculation
The primary outcome indicator, exercise adherence, is selected as the calculation standard. Following the definition by Patel et al, exercise adherence was defined as the proportion of days on which participants completed their prescribed exercise tasks.21 A previous study reported an effect size (Cohen’s d) of 0.79 for similar interventions.29 Based on this, and using a two-sided α of 0.025 and a power of 0.80, the required sample size was calculated with PASS version 21.0.3 (two-sample means comparison) to be 32 participants per group (N = 96). Since the intervention was delivered in pairs (mostly among family members), the observations were no longer statistically independent. Therefore, the sample size was adjusted using the formula Na = N × [1 + (m − 1) × ICC]. The intraclass correlation coefficient (ICC) was estimated to be 0.24. In the absence of pilot data for the present study, this value was selected from a published study that used a methodologically similar, family-based cluster design, providing a reasonable and evidence-based estimate for the calculation.29 Based on this ICC, the adjusted sample size (Na) was 119. Finally, accounting for an anticipated 10% loss to follow-up, the final sample size was set at 132, with 44 participants per group (22 pairs).
Randomization, Blinding and Concealed Allocation
Participants were stratified based on their baseline adherence to the IPEP. During the two-week baseline period, each team of two participants was categorized into one of three strata according to the total number of days they completed the prescribed exercises: ≤9 days, 10–19 days, or ≥20 days. An independent research assistant, not involved in the study, generated randomization lists within each stratum using SPSS software. Teams were then randomly assigned to one of three groups in a 1:1:1 ratio. Randomization codes and group assignments were concealed in sealed, opaque envelopes and provided to the intervention team only after the completion of baseline assessments. Throughout the trial, both data collectors and analysts remained blinded to the allocation.
Intervention
All participants downloaded the same version of the app via a unified download link. The intervention was managed through the backend management system. This centralized server-side application defines the data flow, receiving data from the mobile app via a secure application programming interface for management in a relational database. The system provides a web-based administrative interface for researchers, which includes an auditing trail to track data modifications. For data quality control, the principal investigator will conduct regular checks of the collected data via this interface.
Through this system, the research team was able to configure different settings for each of the three groups: (1) Gamification group: default settings applied; (2) Non-gamification group: the “gamification” option in the corresponding participant management end was turned off to hide all gamification designs; (3) Health education plus gamification group: the “health education” option in the corresponding participant management end was turned on to add the health education section. Furthermore, the backend management system also allows the research team to monitor participants’ adherence data in real-time, manage the scheduled delivery of health education materials, and collect in-app feedback on the intervention.
Gamification Group
Participants in the gamification group received an intervention based on the Octalysis framework. Researchers designed the IPEP as a series of exercise tasks, and all gamification designs were implemented to encourage task completion. Five core drives (Epic Meaning and Calling, Development and Accomplishment, Empowerment of Creativity and Feedback, Social Influence and Relatedness, and Loss and Avoidance) were integrated into the intervention. These specific drives were selected because they align with key constructs from established behavioral theories such as SDT. For instance, the core drives of “Development and Accomplishment” and “Empowerment of Creativity and Feedback” are practical mechanisms designed to foster users’ sense of competence and autonomy, which are core tenets of SDT for enhancing intrinsic motivation.25 Figure 2 displays the English-translated version of the original Chinese app interface.
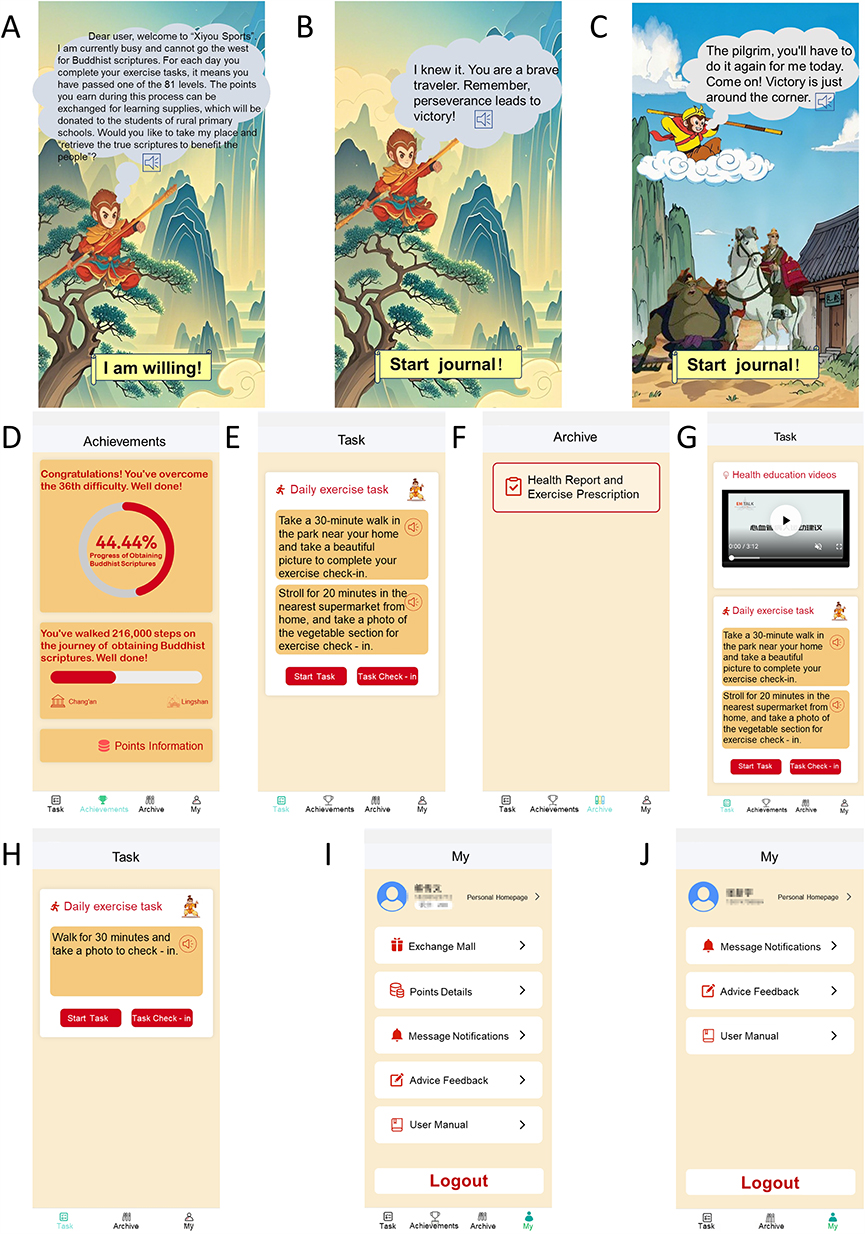 |
Figure 2 The English-translated version of the original Chinese app interface. (A and B) Interaction interface with Sun Wukong for participants in the two intervention groups during their first login; (C) Interaction interface with Sun Wukong for participants in the two intervention groups during subsequent logins; (D) “Achievements” interface for participants in the two intervention groups; (E) “Task” interface for participants in the gamification group; (F) “Archive” interface for participants in three groups; (G) “Task” interface for participants in the health education plus gamification group; (H) “Task” interface for participants in the non-gamification group; (I) “My” interface for participants in the two intervention groups; (J) “My” interface for participants in the non-gamification group. |
First, the theme of “Xiyou Sports” is based on the classic Chinese mythological tale Journey to the West, which is widely known across China. Upon their first login, participants received a virtual invitation from Sun Wukong (the protagonist of Journey to the west) to take his place in traveling westward to retrieve Buddhist scriptures. They are told that completing a day’s exercise task is equivalent to passing one of the trials in the journey (in the myth, 81 trials must be passed to obtain the true scriptures). In parallel, during this process, the points earned by participants can be exchanged for school supplies in the app to be donated to students in rural primary schools (echoing the mythological story where the scriptures are brought back to benefit the people) (Figures 2A and B). On each subsequent logon, patients received encouragement from the Sun Wukong (Figure 2C). This kind of virtual mission and public welfare linkage design,32–34 which can supply users a sense of “Epic Meaning and Calling”, has been proven to promote physical activity.
Secondly, participants received real-time feedback on their progress toward obtaining Buddhist scriptures (days to complete exercise tasks) and total step count through visual progress circles or bars (Figure 2D). Such performance feedback fosters a sense of “Development and Accomplishment”. A post-intervention interview study involving older adults found that performance feedback was a key motivator for engaging in physical activity.24
Third, the IPEP includes two types of exercises: aerobic exercise and strength training. For example, a weekly prescription might include at least 200 minutes of moderate-intensity aerobic exercise (such as normal-speed walking or light square dancing) and at least 48 repetitions of strength exercises (such as wall push-ups or chair-assisted leg extensions). Two rehabilitation physicians from the research team and the first author collaboratively assigned four specific exercise tasks to each participant via the backend management system (eg, “Take a 30-minute walk in the park near your home and take a beautiful picture to complete your exercise check-in”). These tasks were based on the recommended type and volume of exercise from the IPEP, as well as the participant’s preferred exercise environment. Each day, the app randomly presented two of the four tasks for the participant to choose from (Figure 2E). Upon task completion, the visual progress circle reflecting the number of completed exercise days was updated in real time. Empowering participants with the autonomy to choose their tasks and providing immediate feedback supports the core drive of “Empowerment of Creativity and Feedback”. Moreover, translating general system-recommended tasks into more specific ones is consistent with goal-setting theory, which emphasizes that clear and challenging goals lead to better performance than vague or simplistic ones.35 Meanwhile, the user’s health report and the exercise prescription generated by the system were presented in the “archive” interface (Figure 2F).
Finally, participants were required to form teams of two with a relative or friend. Each Monday, every participant received 140 points (20 points per day: 10 points for completing their own exercise task and 10 points for both teammates completing their tasks). If a participant completed their task and their teammate also completed theirs, no points were deducted. If a participant completed their task but their teammate did not, 10 points were deducted. If a participant did not complete the task, 20 points were deducted. This point deduction design capitalizes on the principle that people are often more motivated by losses than by gains,22,36 and it can prompt participants to develop a core drive for “Loss and Avoidance”. At the same time, the intervention strengthens social accountability by having two patients with pre-existing social relationships team up and making their scores interdependent. Participants are more likely to engage in physical activity to avoid negatively impacting their teammates, aligning with the core drive of “Social Influence and Relatedness”.
Health Education Plus Gamification Group
In this group, health education content was added in addition to the gamification intervention, and this component was delivered through educational videos (Figure 2G). Participants could only unlock the button for the daily exercise task after watching the entire educational video and answering a question at the end. Only then were they permitted to carry out the exercise tasks and submit a photo as a check-in.
Non-Gamification Group
Participants in the non-gamified group did not receive any gamification intervention. The daily exercise tasks displayed in the app interface were directly generated by the exercise prescription generation system without any modifications or manual adjustments by the researchers (Figure 2H). Compared to the “My” interface of the two intervention groups (Figure 2I), the “My” interface of this group did not include the exchange mall and points details sections (Figure 2J).
The “Xiyou Sports” Mobile Application
The “Xiyou Sports” mobile application was custom-developed for this research by three members of the in-house study team, and the ownership of the application resides with Bengbu Medical University. As a non-commercial research tool, the app has a proprietary license and is not available for public use or download. It was provided to participants free of charge, with low development and maintenance costs.
Outcome Measures and Data Collection
After 12 weeks of intervention, the app will automatically remind each patient to complete the outcome assessment. Researchers will use WeChat to remind patients to complete the same assessment at 24 weeks. For patients who do not respond on time, researchers will follow up by phone to inquire about the reasons. We will report the number and reasons for lost to follow-up patients.
Table 1 summarizes the study outcome measures. The primary outcome is the adherence of patients to the IPEP, defined as the proportion of days the prescribed exercise tasks were completed out of the total intervention days. During the intervention period, the number of days the exercise tasks were completed was collected through the backend management system (patients uploading photos consistent with the selected tasks were considered as having completed the daily exercise task). During the baseline and follow-up periods, task completion was self-reported by patients via WeChat. To improve the accuracy of self-reported adherence data during the baseline and follow-up periods, a specific verification procedure will be implemented. Each day, a trained researcher will review the daily step count for each participant from the previous day, as measured by their smartphone’s accelerometer and collected via the app. If a participant reported completing a walking task (eg, a 25-minute walk) but their step count for that day was below a predefined plausibility threshold (eg, <1000 steps), that day’s task will be re-coded as incomplete for the final analysis. Secondary outcomes included biomedical risk factors (such as body weight, resting heart rate, systolic blood pressure, diastolic blood pressure, body mass index, subendocardial viability ratio, and brachial-ankle pulse wave velocity), sedentary behavior, sleep quality, self-efficacy, and intrinsic motivation. Except for the collection of biomedical risk factors using instruments and equipment in the electronic health promotion system, all other data were collected through paper-based questionnaires (baseline, 12 weeks, 24 weeks). In addition, at the end of the 12-week intervention, the System Usability Scale was administered to patients in both intervention groups to evaluate usability.37 We will also conduct semi-structured interviews with some of the patients in both intervention groups to understand their satisfaction and the acceptability of the intervention.
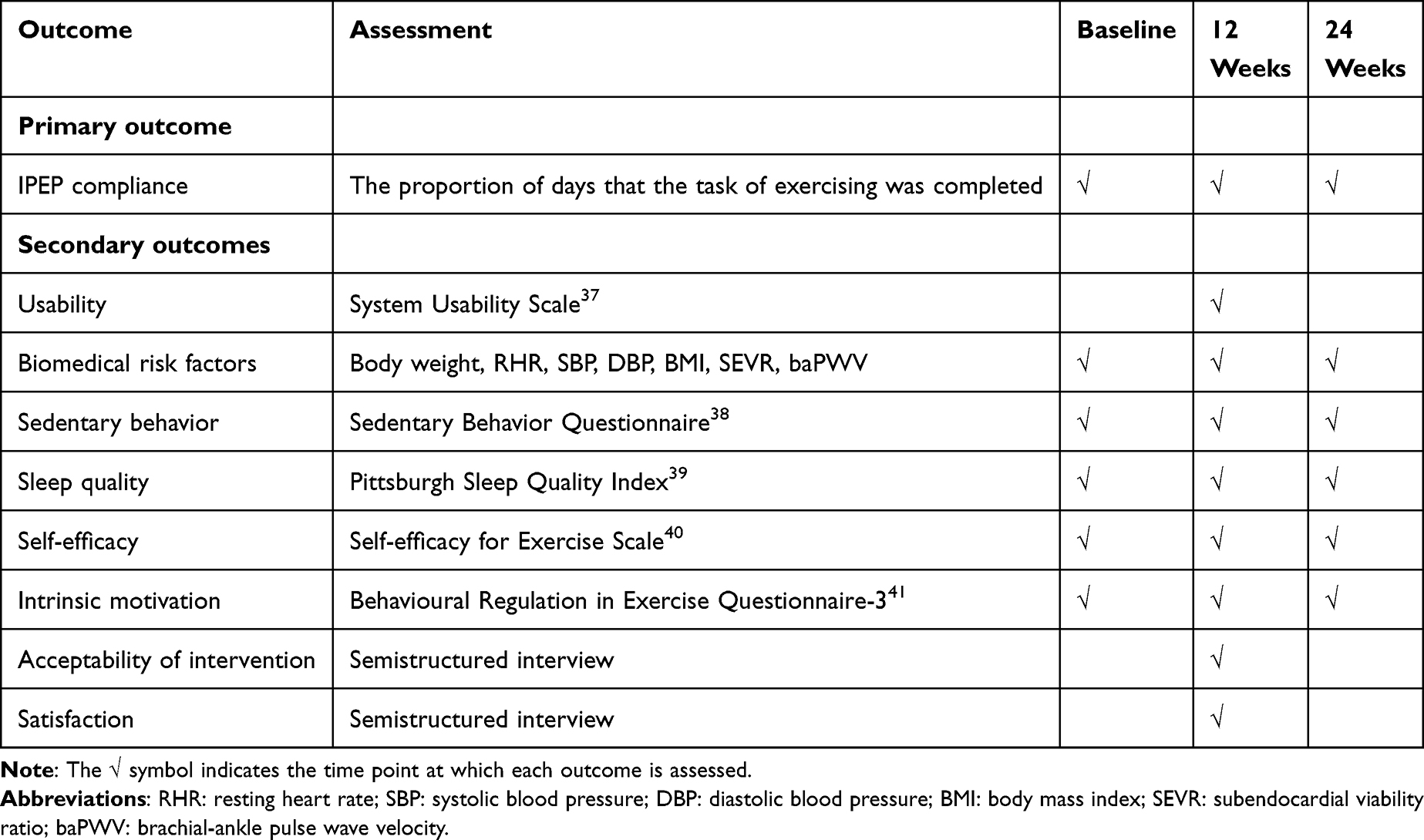 |
Table 1 Assessment Time Points for Primary and Secondary Outcomes |
A proactive adverse event monitoring procedure will be implemented throughout the entire 26-week study period. During their daily exercise report (via the app during the intervention and via WeChat during baseline and follow-up), participants will be required to answer the question “How did you feel after exercising today?” by selecting one of three options (“Normal, completed exercise smoothly”, “Slightly strenuous but no discomfort”, or “Discomfort occurred”). The research team will monitor these responses. If a participant report “Discomfort”, a researcher will contact them by phone the next day to assess the situation. Based on this assessment, the event will be documented and, if necessary, the participant’s exercise prescription will be adjusted. All significant adverse events will be reported to the ethics committee as required.
Statistical Analysis and Data Management
We will perform statistical analyses using SPSS version 25.0 (IBM, Armonk, NY, USA). Baseline differences among the three groups will be compared using one-way ANOVA, non-parametric tests, or chi-square tests. The primary analysis will be conducted based on the intention-to-treat principle, including all randomized participants in the analysis in the group to which they were originally assigned. Additionally, a per-protocol analysis will be conducted as a sensitivity analysis, including only participants who demonstrated a predefined level of adherence (eg, completing at least 70% of the prescribed exercise sessions). Missing data will be handled using multiple imputation. Generalized estimating equation (GEE) models will be employed to compare outcome measures between groups (non-gamification vs gamification; gamification vs gamification plus health education). The model will assume an autoregressive (AR1) correlation structure and will be adjusted for key baseline covariates, including age, sex, primary chronic disease diagnosis, and baseline IPEP adherence levels. A two-sided p-value of <0.05 will be considered statistically significant. The Bonferroni method will be applied to adjust for multiple comparisons.
In this study, all paper-based and WeChat-collected data will be promptly entered into a central electronic database by trained research staff. This database will then be merged with the electronically captured data (from the app’s backend and the electronic health promotion system) to create the consolidated digital dataset used for analysis.
To protect participant confidentiality, all data within this consolidated dataset will be pseudonymized. Personal identifiers (such as names and contact information) will be stored separately from the research data in an encrypted file, linked only by a unique study ID. The consolidated digital dataset will be stored and encrypted on a secure, password-protected server at Bengbu Medical University. The original paper-based questionnaires will be stored securely in a locked file cabinet within a locked office. Access to identifiable data will be restricted to the principal investigator and designated data managers, while other researchers will only work with the de-identified dataset. All study data will be securely retained for five years after study completion, after which all identifiable records will be permanently deleted.
Potential Bias and Mitigation Strategies
This study has several potential sources of bias. First, although the non-gamification group will use the same version of the app with gamification features disabled via the backend to minimize inter-group differences, participants can likely infer their group allocation. This impossibility of blinding participants is a key limitation that may introduce performance bias, where knowledge of group assignment could systematically influence participants’ adherence behaviors. Second, while daily self-reporting minimizes the risk of recall bias, our reliance on this method remains subject to information bias, specifically social desirability bias. Third, the inclusion criteria, such as the requirement for an Android smartphone and the ability to recruit a partner, may introduce selection bias and limit the generalizability of our findings. Finally, as the trial is conducted in community settings, there is a potential risk of contamination (such as information sharing) between intervention groups.
Further reflection on the ethical dimensions of these design choices is warranted. Regarding the inclusion criteria identified above as a source of selection bias, the requirement for an Android smartphone and a certain level of digital literacy was justified by the current development stage of our research platform. Similarly, the dyad-based partner requirement is a core component for testing the cooperation and accountability mechanism; we mitigated the risk of social pressure by strongly emphasizing the voluntary nature of participation for both individuals during the consent process. Finally, the charity-linked incentive was intentionally designed to be a modest, pro-social motivator to appeal to altruism, rather than a coercive financial reward, thereby minimizing the risk of undue influence.
To mitigate these potential biases, several strategies will be implemented. To begin, all outcome assessors and data analysts will be blinded. To minimize performance bias, the research staff will provide an equal level of attention to all groups. To reduce information bias, we will emphasize to all participants that their data is confidential and that there are no “right” or “wrong” answers to promote honest reporting. To minimize contamination risk, all participants will be kindly requested during the onboarding process not to discuss the specific features of their app with others until the study is complete.
Patient and Public Involvement
Patient and public involvement (PPI) plays a crucial role in this study. Before designing the app, the research team interviewed middle-aged and older adults with chronic diseases who had used IPEP but had low adherence. They expressed a willingness to accept supervision and incentives from the APP to improve their adherence. During the app development phase, we also conducted focus group interviews with patients to understand their needs and preferences regarding the APP’s functions. In the pilot study, patients were invited to provide reasonable suggestions on the study design and outcome measurements.
Discussion
This study employed the Octalysis gamification framework to design an intervention aimed at improving adherence to the IPEP among middle-aged and older adults with chronic diseases. Despite the strong scientific basis and individualized adaptability of IPEP, poor adherence remains a significant challenge in real-world application.9 Previous research suggests that gamification interventions hold promise in promoting physical activity.20 However, most existing studies design gamification interventions primarily based on behavior change theories, often resulting in the use of solely simple external incentive mechanisms. In contrast, this study adopts a game design perspective to inform the development of its gamification components.
This study is the first to apply the Octalysis gamification framework to promote physical activity, aiming to stimulate patients’ behavioral motivation through multiple dimensions, including task meaning construction, empowerment of task choice, and timely progress feedback. The framework allows for a balanced integration of extrinsic and intrinsic motivators, thereby enhancing both the initiative and sustainability of patient engagement. Additionally, traditional Chinese mythological stories and public welfare linkage mechanisms were incorporated into the design to foster emotional resonance and a sense of social value, thereby improving patient adherence.
It is worth noting that one study points out that excessive reliance on external incentives in gamified interventions may undermine individuals’ intrinsic motivation to engage in exercise, leading to a rapid decline in adherence once the intervention ends.24 To address this issue, one of the intervention groups in the present study was supplemented with health education, attempting to enhance patients’ cognitive understanding of the deeper value of exercise in chronic disease management, thereby fostering greater autonomy and intrinsic motivation. Theoretically, gamification provides the initial “push” needed to trigger behavior, while health education offers a “pull” through cognitive reinforcement to sustain it. This combination may help mitigate the decline in adherence commonly observed after the conclusion of such interventions.
This study has several limitations that should be acknowledged. First, adherence data during both the baseline and follow-up periods mainly relied on self-reports, which may be subject to information bias despite partial verification using step counts. Second, the study’s generalizability is constrained by several factors. The inclusion criteria (requiring an Android smartphone, a certain level of digital literacy, and the ability to recruit a partner) may introduce selection bias and limit the applicability of our findings to the broader older adult population. Moreover, the intervention’s narrative elements are rooted in a Chinese cultural context, and the team-based design may be more effective in collectivistic cultures; its effectiveness in other cultural settings would require further investigation. Finally, while a primary objective of this study is to formally test the sustainability of exercise behavior during a 12-week follow-up after the app-based intervention has concluded, the even longer-term persistence of this behavior (at 6 months or 1 year) lies beyond the scope of this trial and remains a critical question for future research.
Overall, this study developed and evaluated an innovative mHealth intervention model. The findings provide both theoretical foundations and practical insights for promoting IPEP within community-based chronic disease management.
Conclusion
This article outlines the rationale, objectives, and design of a forthcoming study aimed at evaluating the effects of gamification on adherence to IPEP and exploring whether integrating health education with gamification enhances the long-term maintenance of exercise adherence. Notably, this represents the first application of the Octalysis framework to promote physical activity. Should the intervention prove effective, its design could serve as a scalable model for community-based digital interventions aimed at tackling the significant public health challenge of poor exercise adherence. However, the potential findings of this study should be considered in light of its limitations to external validity, including the specific technological (Android-only), cultural (Chinese context), and social (dyad-based) context. Future work should focus on adapting and validating this intervention model for broader populations across diverse platforms and cultural settings. The trial is expected to be completed by November 16, 2025.
Abbreviations
AI, artificial intelligence; IPEP, intelligent personalized exercise prescription; mhealth, mobile health; SDT, self-determination theory; ICC, intraclass correlation coefficient; GEE, generalized estimating equation; PPI, patient and public involvement; RHR, resting heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; SEVR, subendocardial viability ratio; baPWV, brachial-ankle pulse wave velocity.
Data Sharing Statement
De-identified individual participant data that underlie the results reported in the final publication will be made available upon reasonable request to the corresponding author.
Ethics Approval and Informed Consent
The trial will be conducted in compliance with the Declaration of Helsinki. This study was approved by the Ethics Committee of Bengbu Medical University on April 10, 2025 (2025-172), and pre-registered in the Chinese Clinical Trial Registry (ChiCTR2500102132). All participants provided written informed consent. The results of this trial will be disseminated through publications in peer-reviewed journals and presentations at academic conferences.
Acknowledgments
The authors would like to thank the valuable contribution made by the patients and public representatives during the gamification intervention development.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Joint Research Center for Regional Diseases of IHM (2024bydjk003), the Anhui Provincial Department of Education (2024AH040340, 2022lhpysfjd063) and the Research Innovation Project for Graduate Students of Bengbu Medical University 2024 (Byycx24074). The funding sources played no role in the study design, interpretation, report writing, or the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
2. World Health Organization. The top 10 causes of death; 2024. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/the-top-10-causes-of-death.
3. World Health Organization. Noncommunicable diseases; 2024. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/noncommunicable-diseases.
4. Izquierdo M, Merchant RA, Morley JE, et al. International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging. 2021;25(7):824–853. doi:10.1007/s12603-021-1665-8
5. Lewis C, Rafi E, Dobbs B, Barton T, Hatipoglu B, Malin SK. Tailoring exercise prescription for effective diabetes glucose management. J Clin Endocrinol Metab. 2025;110(Supplement_2):S118–S130. doi:10.1210/clinem/dgae908
6. Bellini A, Scotto Di Palumbo A, Nicolò A, Bazzucchi I, Sacchetti M. Exercise prescription for postprandial glycemic management. Nutrients. 2024;16(8):1170. doi:10.3390/nu16081170
7. Edwards JJ, Deenmamode AHP, Griffiths M, et al. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br J Sports Med. 2023;57(20):1317–1326. doi:10.1136/bjsports-2022-106503
8. Hanssen H, Boardman H, Deiseroth A, et al. Personalized exercise prescription in the prevention and treatment of arterial hypertension: a consensus document from the European association of preventive cardiology (EAPC) and the ESC council on hypertension. Eur J Prev Cardiol. 2022;29(1):205–215. doi:10.1093/eurjpc/zwaa141
9. Sun T, Xu Y, Xie H, Ma Z, Wang Y. Intelligent personalized exercise prescription based on an eHealth promotion system to improve health outcomes of middle-aged and older adult community dwellers: pretest-posttest study. J. Med Internet Res. 2021;23(5):e28221. doi:10.2196/28221
10. Tan M, Xiao Y, Jing F, et al. Evaluating machine learning-enabled and multimodal data-driven exercise prescriptions for mental health: a randomized controlled trial protocol. Front Psychiatry. 2024;15:1352420. doi:10.3389/fpsyt.2024.1352420
11. Gao T, Ren H, He S, et al. Development of an interpretable machine learning-based intelligent system of exercise prescription for cardio-oncology preventive care: a study protocol. Front Cardiovasc Med. 2023;9:1091885. doi:10.3389/fcvm.2022.1091885
12. Lin CC, Lin YS, Yeh CH, Huang CC, Kuo LC, Su FC. An exergame-integrated Iot-based ergometer system delivers personalized training programs for older adults and enhances physical fitness: a pilot randomized controlled trial. Gerontology. 2023;69(6):768–782. doi:10.1159/000526951
13. Bullard T, Ji M, An R, Trinh L, Mackenzie M, Mullen SP. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: cancer, cardiovascular disease, and diabetes. BMC Public Health. 2019;19(1):636. doi:10.1186/s12889-019-6877-z
14. Husebø AM, Dyrstad SM, Søreide JA, Bru E. Predicting exercise adherence in cancer patients and survivors: a systematic review and meta-analysis of motivational and behavioural factors. J Clin Nurs. 2013;22(1–2):4–21. doi:10.1111/j.1365-2702.2012.04322.x
15. Sebastian D, Dan D, Rilla K, Lennart N. From game design elements to gamefulness: defining “gamification”. In:
16. Salmani B, Prapavessis H, Vanderloo LM, Mitchell MS. Financial incentives for physical activity in adults: systematic review and meta-analysis update. Prev Med. 2025;192:108237. doi:10.1016/j.ypmed.2025.108237
17. Nuss K, Moore K, Nelson T, Li K. Effects of motivational interviewing and wearable fitness trackers on motivation and physical activity: a systematic review. Am J Health Promot. 2021;35(2):226–235. doi:10.1177/0890117120939030
18. Mazeas A, Duclos M, Pereira B, Chalabaev A. Evaluating the effectiveness of gamification on physical activity: systematic review and meta-analysis of randomized controlled trials. J. Med Internet Res. 2022;24(1):e26779. doi:10.2196/26779
19. Nishi SK, Kavanagh ME, Ramboanga K, et al. Effect of digital health applications with or without gamification on physical activity and cardiometabolic risk factors: a systematic review and meta-analysis of randomized controlled trials. EClinicalMedicine. 2024;76:102798. doi:10.1016/j.eclinm.2024.102798
20. Xu L, Shi H, Shen M, et al. The effects of mHealth-based gamification interventions on participation in physical activity: systematic review. JMIR Mhealth Uhealth. 2022;10(2):e27794. doi:10.2196/27794
21. Patel MS, Small DS, Harrison JD, et al. Effectiveness of behaviorally designed gamification interventions with social incentives for increasing physical activity among overweight and obese adults across the United States: the STEP UP randomized clinical trial. JAMA Intern Med. 2019;179(12):1624–1632. doi:10.1001/jamainternmed.2019.3505
22. Xu L, Tong Q, Zhang X, et al. Smartphone-based gamification intervention to increase physical activity participation among patients with coronary heart disease: a randomized controlled trial. J Telemed Telecare. 2024;30(9):1425–1436. doi:10.1177/1357633X221150943
23. Friedman DN, Lavery JA, Moskowitz CS, et al. Feasibility and acceptability of a parent-child intervention to improve step count in childhood cancer survivors exposed to cardiotoxic therapy: the STEP UP for FAMILIES study. Pediatr Blood Cancer. 2024;71(12):e31320. doi:10.1002/pbc.31320
24. Tabak M, de Vette F, van Dijk H, Vollenbroek-Hutten M. A game-based, physical activity coaching application for older adults: design approach and user experience in daily Life. Games Health J. 2020;9(3):215–226. doi:10.1089/g4h.2018.0163
25. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037/0003-066X.55.1.68
26. Chou Y-K. Actionable Gamification: Beyond Points, Badges, and Leaderboards. Birmingham: Packt Publishing Ltd; 2019.
27. Tang HJ, Moser DK, Tang HJ, Lin CH, Hu FW. A game-based multimedia application to improve the ability of clinical nurses to perform geriatric care: a randomized controlled trial. Nurse Educ Today. 2024;139:106253. doi:10.1016/j.nedt.2024.106253
28. Mohanty S, Christopher B,P. A bibliometric analysis of the use of the gamification Octalysis framework in training: evidence from Web of Science. Humanit Soc Sci Commun. 2023;10:836. doi:10.1057/s41599-023-02243-3
29. Patel MS, Benjamin EJ, Volpp KG, et al. Effect of a game-based intervention designed to enhance social incentives to increase physical activity among families: the BE FIT randomized clinical trial. JAMA Intern Med. 2017;177(11):1586–1593. doi:10.1001/jamainternmed.2017.3458
30. Chan AW, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomised trials. BMJ. 2025;389:e081477. doi:10.1136/bmj-2024-081477
31. Xu X, Zhang G, Xia Y, et al. Influencing factors and implementation pathways of adherence behavior in Intelligent personalized exercise prescription: qualitative study. JMIR Mhealth Uhealth. 2024;12:e59610. doi:10.2196/59610
32. Direito A, Jiang Y, Whittaker R, Maddison R. Apps for improving FITness and increasing physical activity among young people: the AIMFIT pragmatic randomized controlled trial. J Med Internet Res. 2015;17(8):e210. doi:10.2196/jmir.4568
33. Fuemmeler BF, Holzwarth E, Sheng Y, et al. Mila Blooms: a mobile phone application and behavioral intervention for promoting physical activity and a healthy diet among adolescent survivors of childhood cancer. Games Health J. 2020;9(4):279–289. doi:10.1089/g4h.2019.0060
34. Mamede A, Noordzij G, Jongerling J, Snijders M, Schop-Etman A, Denktas S. Combining web-based gamification and physical nudges with an App (MoveMore) to promote walking breaks and reduce sedentary behavior of office workers: field study. J Med Internet Res. 2021;23(4):e19875. doi:10.2196/19875
35. Locke EA, Latham GP. The development of goal setting theory: a half century retrospective. Motivation Science. 2019;5(2):93–105. doi:10.1037/mot0000127
36. Kahneman D, Tversky A. Prospect theory: an analysis of decision under risk. Econometrica. 1979;47(2):263–291. doi:10.2307/1914185
37. Brooke J, et al. SUS: a “quick and dirty” usability scale. In: Jordan PW, Thomas B, Weerdmeester BA, editors. Usability Evaluation in Industry. London: Taylor & Francis; 1996:6.
38. Gardiner PA, Clark BK, Healy GN, Eakin EG, Winkler EA, Owen N. Measuring older adults’ sedentary time: reliability, validity, and responsiveness. Med Sci Sports Exerc. 2011;43(11):2127–2133. doi:10.1249/MSS.0b013e31821b94f7
39. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
40. Lee LL, Perng SJ, Ho CC, Hsu HM, Lau SC, Arthur A. A preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adults. Int J Nurs Stud. 2009;46(2):230–238. doi:10.1016/j.ijnurstu.2008.09.003
41. Markland D, Tobin V. A modification to the behavioural regulation in exercise questionnaire to include an assessment of amotivation. J Sport Exerc Psychol. 2004;26(2):191–196. doi:10.1123/jsep.26.2.191
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.