Back to Journals » Infection and Drug Resistance » Volume 19
A Diagnostic Accuracy Study of Combined OMP22-PCR and SAT for Brucellosis in Xinjiang, China
Authors Yun M, Chen J, Zhou Y, Wei C, Zhang K, Zhang C, Zhu C ![]() , Xie S
, Xie S
Received 10 November 2025
Accepted for publication 27 January 2026
Published 2 February 2026 Volume 2026:19 575518
DOI https://doi.org/10.2147/IDR.S575518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Minghui Yun,1,2,* Jing Chen,3,4,* Yang Zhou,1,2,* Chao Wei,1,2 Kaiting Zhang,1,2 Chanjuan Zhang,1,2 Chuanlong Zhu,5 Songsong Xie1,2
1NHC Key Laboratory of Prevention and Treatment of Central Asia High Incidence Diseases(Co-Construction), The First Affiliated Hospital of Shihezi University, The Clinical Research Center for Infectious Diseases of Xinjiang Production and Construction Corps, Shihezi, 832099, People’s Republic of China; 2State Key Laboratory for Diagnosis and Treatment of Severe Zoonotic Infectious Diseases, Wuhan, 430000, People’s Republic of China; 3Nanjing Medical University, Nanjing, 210000, People’s Republic of China; 4The Second People’ s Hospital of Yining, Yining, Xinjiang, 835000, People’s Republic of China; 5Department of Infectious Diseases, the First Affiliated Hospital with Nanjing Medical University, Nanjing, 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Songsong Xie, Email [email protected] Chuanlong Zhu, Email [email protected]
Background: The standard tube agglutination test (SAT) is a cornerstone for brucellosis diagnosis but has inherent limitations, including false negatives in early and chronic infections and false positives due to cross-reactivity. To overcome these drawbacks, molecular detection targeting the highly conserved Brucella outer membrane protein 22 (OMP22) gene presents a promising solution. This study aimed to evaluate the diagnostic value of OMP22-PCR and its efficacy when combined with SAT.
Methods: From January 2023 to May 2024, serum samples from 62 culture-confirmed brucellosis patients and 25 controls were analyzed using OMP22-PCR and SAT. Diagnostic performance was compared, discordant results were analyzed, and OMP22 detection was extended to 20 clinical isolates, 20 urine samples, and 2 cerebrospinal fluid (CSF) samples.
Results: OMP22-PCR demonstrated a sensitivity of 93.5% and specificity of 92.0%, which was comparable to SAT (96.8% and 88.0%, respectively; both P > 0.05). Crucially, the combined detection approach achieved a significantly higher specificity of 100% and a positive predictive value of 100%, and a significantly larger area under the ROC curve (AUC) than either test alone (P < 0.05), all while maintaining a high sensitivity of 96.8%. Analysis of discordant samples revealed their complementary nature: SAT-positive/OMP22-PCR-negative samples were primarily from chronic-stage patients, whereas SAT-negative/OMP22-PCR-positive samples were from early-stage patients. Furthermore, OMP22 was detected in all clinical isolates (100%), 70.0% of urine samples, and both CSF samples (100%).
Conclusion: The combination of OMP22-PCR and SAT effectively compensates for the limitations of each method alone, significantly enhancing diagnostic accuracy. The strong performance of OMP22-PCR in non-blood samples further underscores its value as a complementary tool, thereby supporting the development of more comprehensive diagnostic strategies for brucellosis.
Keywords: brucellosis, OMP22, PCR, standard tube agglutination test, diagnostic efficacy
Introduction
Brucellosis, also known as Malta fever or undulant fever, is a global zoonotic disease caused by bacteria of the genus Brucella. It poses a significant public health challenge, with recent models estimating the global annual incidence to be approximately 1.6 to 2.1 million cases.1,2 The disease burden is particularly high in regions with extensive livestock husbandry, including the Mediterranean, Middle East, Central Asia, and parts of Latin America.3,4 In China, the incidence has markedly increased in recent years, with reported cases rising from 45,046 in 2019 to 70,439 in 2023, and the incidence rate increasing from 3.25 to 4.99 per 100,000 population.5 The infection is typically acquired through direct contact with infected animals (eg, cattle, sheep, goats), consumption of unpasteurized dairy products, or inhalation of contaminated aerosols. Occupations such as farming, veterinary medicine, and slaughterhouse work are therefore at highest risk, which explains the male predominance commonly observed in epidemiological studies.6,7 A major clinical hurdle is its non-specific and protean symptomatology. Patients often present with irregular fever, fatigue, profuse sweating, and arthralgia, which frequently leads to misdiagnosis or delayed treatment.8 Furthermore, brucellosis can affect almost any organ system, leading to severe complications such as osteoarticular involvement (eg, spondylitis, sacroiliitis), hepatosplenomegaly, endocarditis, and neurological manifestations (neurobrucellosis).9 Consequently, achieving an early, rapid, and accurate diagnosis is essential for the effective treatment of brucellosis.
The current diagnostic landscape for brucellosis presents considerable limitations. While blood culture is regarded as the “gold standard”, its utility is constrained by a prolonged culture cycle, biosafety risks, and variable sensitivity, particularly in the acute phase (ranging from 15% to 70%).10 Serological methods are thus the cornerstone of routine diagnosis. The standard tube agglutination test (SAT) is widely used but is inherently limited by its dependence on the host’ s antibody response. This reliance renders it susceptible to false negatives during the early antibody window period, in immunocompromised patients, and in chronic stages when antibody titers decline.11,12 Other rapid serological assays, such as the Rose Bengal plate agglutination test (RBT) and various enzyme-linked immunosorbent assays (ELISA), are commonly used for screening but share the fundamental limitations of SAT: they are indirect tests that cannot reliably distinguish between active infection and past exposure, and they are prone to cross-reactivity with other Gram-negative bacteria (eg, Yersinia enterocolitica O:9, Escherichia coli O:157), potentially leading to false-positive results.13 Furthermore, these methods cannot be reliably applied to non-blood samples. These shortcomings underscore the urgent need for diagnostic methods that directly target the pathogen.
Molecular biology techniques like PCR can directly detect Brucella DNA and offer a promising alternative to overcome the limitations of serology. PCR demonstrates advantages for diagnosing early and late infections and is highly applicable to non-blood sample types. Among various genetic targets, the Brucella outer membrane protein OMP22 gene stands out as an ideal candidate due to its high conservation and species specificity.14 The OMP22 sequence is stable across different Brucella species and biovars, ensuring broad coverage of common and highly pathogenic strains. This stability minimizes the chance of missed detection due to strain variability and, in parallel, confers high specificity with low cross-reactivity against common Gram-negative bacteria, thereby reducing the risk of false-positive results.12 Based on this rationale, the present study was designed with the following objectives: to systematically evaluate the diagnostic value of OMP22-PCR for brucellosis, to compare its efficacy with the conventional SAT, and crucially, to explore the potential synergistic improvement in diagnostic accuracy achieved by their combined use. Moreover, we aimed to extend the application of OMP22-PCR beyond serum by evaluating its detection capability in clinical isolates, urine, and cerebrospinal fluid (CSF), thereby assessing its potential as a comprehensive diagnostic tool. This extended application was prompted by our prior success in concurrently detecting the OMP22 gene in the CSF, blood, and urine of a neurobrucellosis patient, which facilitated a definitive diagnosis in a complex clinical case.15 Building upon that preliminary finding, this study provides a systematic scientific basis for optimizing diagnostic strategies for brucellosis.
Materials and Methods
Study Subjects and Sample Collection
Samples of various types from patients suspected of having brucellosis and from control patients at the Department of Infectious Diseases, the First Affiliated Hospital of Shihezi University, were collected from January 2023 to May 2024. The sample types included serum, urine, CSF, and blood culture-positive isolates. Prior to being sent to the research laboratory for subsequent DNA extraction, the blood culture-positive isolates were inactivated by the clinical laboratory. This research was approved by the Ethics Committee of The First Affiliated Hospital of Shihezi University (Approval number: KJ2020-034-01), and all enrolled patients provided written informed consent.
Serum Samples and Grouping
Brucellosis Group
A total of sixty-two patients who were initially diagnosed with brucellosis were enrolled in the study. The diagnosis and staging of the disease adhered to the Chinese Health Industry Standard “Diagnosis for Brucellosis” (WS 269–2019).16 The diagnosis was based on the following criteria: 1) a clear epidemiological history, such as contact with infected livestock (eg, cattle and sheep) or consumption of undercooked meat and dairy products; 2) the presence of typical clinical manifestations, including fever, profuse sweating, fatigue, and arthralgia; and 3) a SAT titer of ≥1:100 (++) and/or a positive blood culture. The specific staging criteria were defined as follows: a disease course of less than 3 months indicated the acute stage, 3 to 6 months indicated the subacute stage, and more than 6 months indicated the chronic stage. Notably, none of the patients had received standardized antimicrobial therapy before enrollment.
Control Group
This group consisted of 25 subjects: 15 healthy volunteers from the health examination center (no brucellosis epidemiological history, symptoms, or SAT positivity), and 10 disease controls presenting with brucellosis-like symptoms, including acute respiratory infections (n=3), rheumatic fever (n=4), and tuberculosis (n=3). All controls tested negative for SAT, and the disease controls were definitively diagnosed with their respective conditions.
Sample Collection and Processing
Serum
From each subject, 3 mL of venous blood was collected in coagulation-promoting tubes. The samples were centrifuged at 3000 r/min for 5 minutes, and the supernatant serum was aliquoted and stored at −80°C until analysis.
Clinical Isolates
Brucella melitensis standard strain 16M served as the positive reference strain, while Escherichia coli was utilized as the negative control. Furthermore, clinical isolates from 20 patients with positive blood cultures were examined. These isolates were obtained as part of the routine hospital diagnostic procedure and were subsequently utilized for research purposes in this study. All bacterial strains were inactivated by the clinical laboratory prior to DNA extraction to ensure biosafety.
Non-Blood Samples
To evaluate the expanded application of OMP22-PCR, clean-catch midstream urine samples were prospectively collected from 20 brucellosis patients. CSF samples were also collected from 2 patients exhibiting severe neurological symptoms suggestive of neurobrucellosis. All body fluid samples were centrifuged at 3000 rpm for 10 minutes to pellet cells and debris for subsequent DNA extraction.
Standard Tube Agglutination Test (SAT)
The SAT was performed strictly in accordance with the Chinese Health Industry Standard “Diagnosis for Brucellosis” (WS 269–2019).16 Serum samples were reacted with Brucella antigen, and a titer of ≥1:100 was deemed positive.
Molecular Detection by OMP22-PCR
Genomic DNA Extraction
All samples, including serum, inactivated bacterial suspension, urine, and CSF pellets, were extracted uniformly using the TIANamp Blood/Cell/Tissue Genomic DNA Extraction Kit (Tiangen Biotech, Beijing), strictly adhering to the manufacturer’s instructions. The bacterial suspensions were thoroughly inactivated prior to extraction to ensure biosafety. Additionally, a negative control, utilizing sterile water in place of the sample, was included in each extraction batch and subjected to PCR amplification concurrently with the test samples.
PCR Amplification
The OMP22 gene was amplified using the following specific primers, selected based on its high conservation and specificity within the Brucella genus:17
Forward: 5’-TGATGGGAGGGACCGACTA-3’
Reverse: 5’-TGGTTCTTCAGGTTGTTACGC-3’
(Synthesized by Xinjiang Youkang Biotechnology Co., Ltd).
Reaction System and Conditions
The PCR reaction was carried out in a total volume of 10 μL, containing 5 μL of 2×PCR Mix, 1 μL of DNA template, 0.3 μL of each primer (10 μM), and 3.4 μL of deionized water. The thermal cycling conditions were as follows: initial denaturation at 95°C for 5 minutes; 35 cycles of denaturation at 94°C for 40 seconds, annealing at 55°C for 40 seconds, and extension at 72°C for 40 seconds; followed by a final extension at 72°C for 8 minutes.
Result Analysis
The PCR products were separated by 1.5% agarose gel electrophoresis and visualized under UV light. The presence of a clear, specific band at 525 bp was judged as a positive result.
Combined Detection Strategy
A sample was considered positive by the combined detection strategy if it tested positive by either the SAT or the OMP22-PCR assay. This approach inherently combines the results from both tests, classifying samples with any positive result (SAT+/PCR+, SAT+/PCR-, or SAT-/PCR+) as positive for brucellosis in order to maximize sensitivity.
Statistical Analysis
All statistical analyses were performed using SPSS Statistics version 25.0 (IBM Corp., USA). Using blood culture positivity as the reference standard, 2×2 contingency tables were constructed to calculate the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy for OMP22-PCR and SAT. McNemar’s test was used to compare the sensitivities and specificities of the two methods. The agreement between OMP22-PCR and SAT results was assessed using the Kappa statistic. A Receiver Operating Characteristic (ROC) curve was plotted, and the DeLong test was utilized to compare the areas under the curve (AUC). A two-tailed p-value of < 0.05 was considered statistically significant. The de-identified individual participant data that underlie the diagnostic accuracy calculations, along with the extended clinical dataset, are available in Supplementary Datasets S1.
Results
Basic Characteristics of the Study Subjects
A total of 87 subjects were enrolled in the study, comprising 62 patients initially diagnosed with brucellosis (case group) and 25 control subjects (control group). According to the WS 269–2019 standard for disease staging, among the 62 brucellosis patients, 38 (61.3%) were classified in the acute stage, 16 (25.8%) in the subacute stage, and 8 (12.9%) in the chronic stage (Table 1). There were no statistically significant differences in age and gender distribution between the case and control groups (P > 0.05), indicating that the demographic characteristics of the two groups were comparable. Male patients predominated in the case group (74.2%), which is consistent with the epidemiological observation that brucellosis is more prevalent among individuals engaged in animal husbandry, slaughtering, and related occupations.18 A consolidated overview of clinical stages and corresponding laboratory test results for all 62 brucellosis patients is provided in Supplementary Table S7.
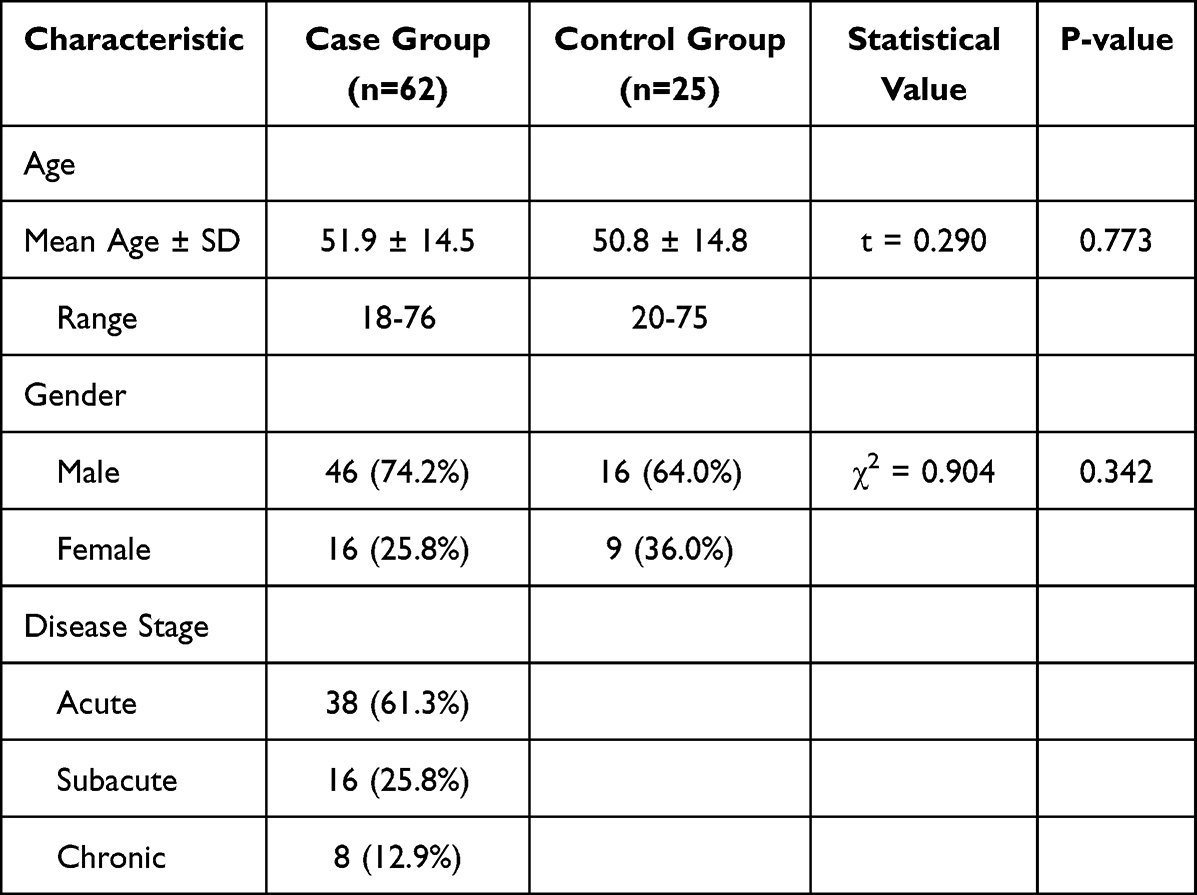 |
Table 1 Comparison of Basic Characteristics Between the Brucellosis Case Group and the Control Group |
Diagnostic Performance and Consistency Between SAT and OMP22-PCR in Serum
We first evaluated the diagnostic performance of SAT and OMP22-PCR in serum samples using blood culture as the reference standard. SAT detection revealed that 60 out of 62 confirmed cases (96.8%) tested positive, while 22 out of 25 controls (88.0%) tested negative, yielding a sensitivity of 96.8% and a specificity of 88.0% (Supplementary Table S1). The most prevalent titer was 1:200 (Supplementary Table S3). In parallel, OMP22-PCR demonstrated a comparable performance, with a positive detection rate of 93.5% (58/62) in the case group and a specificity of 92.0% (23/25) in the control group (Supplementary Table S2). A representative electrophoretogram of OMP22-PCR detection in partial serum samples is shown in Supplementary Figure S1, confirming the specific amplification of the 525-bp target fragment. There were no statistically significant differences in either sensitivity or specificity between the two methods (both P > 0.05).
Subsequently, we assessed the consistency between these two assays. The Kappa test demonstrated a substantial agreement between the two methodologies, with a Kappa value of 0.70 (P < 0.001). However, a detailed analysis of discordant results revealed their complementary nature. Out of the 87 samples analyzed, 11 exhibited discordant results (12.6%). Specifically, 7 samples were SAT-positive yet OMP22-PCR-negative, while 4 samples were SAT-negative but OMP22-PCR-positive. Notably, this comprised 7 samples from the case group (4 SAT-positive/OMP22-PCR-negative and 3 SAT-negative/OMP22-PCR-positive) and 4 samples from the control group (3 SAT-positive/OMP22-PCR-negative and 1 SAT-negative/OMP22-PCR-positive) (Supplementary Table S4).
To further understand the clinical relevance of these discordant results, we analyzed the clinical stages and SAT titers of the involved case group samples. The four SAT-positive/OMP22-PCR-negative cases were predominantly from the chronic stage (3/4, 75%), characterized by persistent symptoms but potentially low or localized bacterial loads. Conversely, the three SAT-negative/OMP22-PCR-positive cases were all from the acute stage (3/3, 100%), with disease durations of less than 2 weeks and low or borderline SAT titers (1:100), highlighting the value of molecular detection during the serological window period. Among the 4 discordant samples from the control group, the 3 SAT-positive/OMP22-PCR-negative samples had low SAT titers (ranging from 1:100 to 1:200). The single SAT-negative/OMP22-PCR-positive sample was from a healthy volunteer with no clinical or epidemiological evidence of brucellosis.
Superior Diagnostic Efficacy of the Combined Detection Approach
Given the complementary patterns observed in discordant samples, we further evaluated a combined detection strategy where a sample was considered positive if either SAT or OMP22-PCR was positive. This approach yielded a sensitivity of 96.8% and, critically, achieved a perfect specificity of 100.0%, along with a positive predictive value (PPV) of 100.0% and an overall accuracy of 97.7% (Supplementary Table S5).
To comprehensively compare the diagnostic efficacy, we plotted the ROC curves and calculated the AUCs (Figure 1). The AUC values for OMP22-PCR, SAT, and the combined detection method were 0.928, 0.921, and 0.981, respectively. Importantly, pairwise comparisons using the DeLong test revealed that the AUC for the combined diagnostic method was significantly higher than that of the SAT (Z = 2.132, P = 0.033) and the OMP22-PCR (Z = 2.045, P = 0.041). These results statistically confirm the superior overall diagnostic performance of the combined approach. In contrast, no statistically significant difference was observed between the AUCs of SAT and OMP22-PCR (Z = 0.815, P = 0.415).
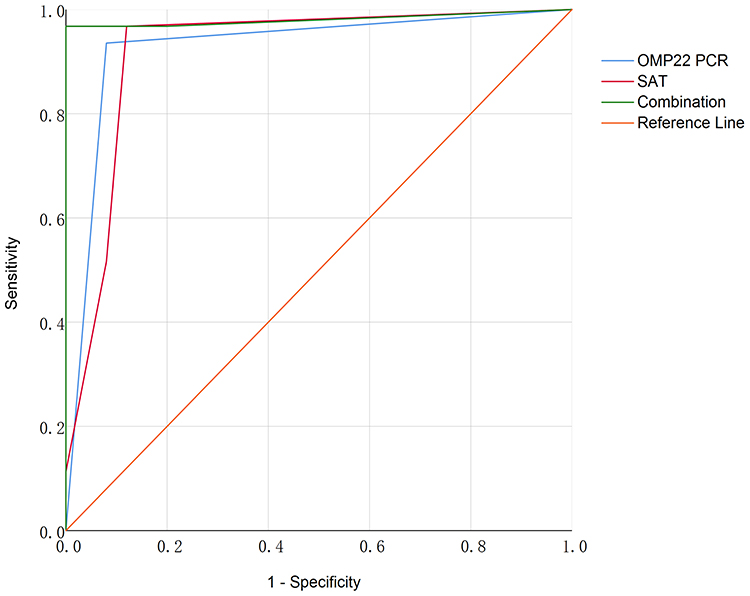 |
Figure 1 ROC curves of OMP22-PCR, SAT and combined detection for the diagnosis of brucellosis. |
OMP22-PCR Detection in Clinical Isolates
To verify the effectiveness of OMP22-PCR in detecting genomic DNA from clinical strains in this study, genomic DNA from clinical isolates corresponding to 20 blood culture-positive patients was tested. All strains were completely inactivated prior to DNA extraction. The DNA from all clinical isolates (20/20) exhibited single, bright, specific bands at 525 bp, resulting in a positive detection rate of 100%, which was fully consistent with the blood culture results. A representative electrophoretogram is presented in Supplementary Figure S2.
OMP22-PCR Detection Results in Non-Blood Samples
Finally, we explored the applicability of OMP22-PCR beyond blood and isolates by testing non-blood clinical samples. OMP22-PCR successfully detected Brucella DNA in 14 of 20 urine samples from confirmed patients, yielding a positivity rate of 70.0% (14/20). Additionally, CSF samples from two patients exhibiting severe neurological symptoms were both positive (2/2, 100%), providing molecular evidence for neurobrucellosis (Supplementary Figure S3).
The detection rates varied across sample types, with blood yielding the highest positivity (93.5%), followed by urine (70.0%). This gradient likely reflects differences in bacterial load and distribution in body fluids during infection. A comparative summary is provided in Supplementary Table S6.
Discussion
Brucellosis, a widely prevalent zoonosis, necessitates early and accurate diagnosis for effective clinical treatment and public health prevention and control. Our study systematically evaluated a molecular approach targeting the Brucella OMP22 gene and its integration with conventional serology. The principal finding of this study is that while OMP22-PCR exhibits diagnostic efficacy comparable to the standard SAT, its combined use creates a synergistic effect that significantly enhances overall diagnostic accuracy. This conclusion is strongly supported by the superior AUC of the combined method and its achievement of 100% specificity.
The complementary value of the two assays is critically illuminated by the analysis of discordant samples. In our cohort, the SAT-positive/OMP22-PCR-negative pattern was primarily identified in patients with chronic infections. This finding is consistent with the established pathogenesis of chronic brucellosis, where the pathogen may be sequestered within the reticuloendothelial system, leading to low-level or intermittent bacteremia below the detection limit of PCR,19 while specific IgG antibodies detectable by SAT can persist for an extended period.20 This scenario highlights a key limitation of serology in differentiating active localized infection from past exposure. Conversely, the SAT-negative/OMP22-PCR-positive pattern was associated with early-stage disease. This pattern underscores the unique advantage of direct pathogen DNA detection in overcoming the limitations of SAT during the serological window period or in cases potentially affected by the prozone phenomenon, thereby facilitating earlier diagnosis.21
The discordant results in the control group further inform the specific limitations of each test. The SAT-positive/OMP22-PCR-negative pattern observed in three disease controls (with low titers) is consistent with the known potential for cross-reactivity in serological assays or, in endemic regions, with the presence of residual antibodies from a past infection.22 On the other hand, the single OMP22-PCR-positive/SAT-negative result in a healthy control, in the absence of any clinical evidence of infection, likely represents a false positive, potentially due to minute contamination. This isolated finding underscores the necessity of rigorous laboratory controls and the interpretation of PCR results within the full clinical context. Crucially, the combined detection strategy effectively mitigated the impact of these individual test limitations, as evidenced by the achievement of 100% specificity.
The diagnostic challenges we aimed to address are not unique to our setting but are a global concern in brucellosis-endemic countries. Similar studies from diverse regions have underscored the limitations of relying on a single test. For instance, research from Peru and Egypt has highlighted the persistent issue of serological cross-reactivity and the value of molecular confirmation, particularly in chronic or complicated cases.23,24 In the Middle East, evaluations of combined serological and molecular approaches have similarly pointed towards improved accuracy, echoing our findings on the synergy between direct pathogen detection and antibody assays.25,26 The clinical significance of these findings lies in the formulation of a more robust diagnostic strategy. We propose a practical, tiered diagnostic algorithm: initial screening with SAT, supplemented by mandatory OMP22-PCR testing for SAT-negative patients with a high clinical index of suspicion for early infection or immunosuppression, as well as for suspected chronic and extrapolated cases. This approach leverages the efficiency of SAT for routine screening while systematically addressing its blind spots, thereby minimizing missed diagnoses.
Beyond serum diagnostics, our study successfully expands the application of OMP22-PCR to non-blood samples, unlocking new potential for diagnosing complicated brucellosis. The detection of Brucella DNA in 70.0% of urine samples, while lower than in blood, establishes OMP22-PCR as a promising non-invasive tool for investigating genitourinary involvement. The lower detection rate in urine compared to blood may be attributed to intermittent bacterial shedding, lower bacterial loads in the urinary tract, or potential degradation of DNA during sample processing and storage.27 More significantly, the 100% positivity rate in CSF samples from patients with neurobrucellosis represents a major step forward. Serological tests on CSF are often hampered by low antibody titers and a lack of standardization.28 OMP22-PCR, by directly targeting pathogen nucleic acids at the site of infection, effectively circumvents these limitations and offers a reliable means to confirm this severe complication. Our present findings are strongly supported by a previous case report, where OMP22-PCR successfully detected Brucella DNA in the CSF of a neurobrucellosis patient presenting with ischemic stroke, enabling a critical etiological diagnosis.15
The diagnostic reliability of the OMP22-PCR assay is firmly rooted in the molecular characteristics of its target. The high conservation of the OMP22 gene across Brucella species provides a solid genetic foundation for its stability and broad detection coverage.29 This places it among several genetic targets commonly used for Brucella detection, each with distinct advantages. Multi-copy insertion sequences like IS711 offer high sensitivity but may cross-react with phylogenetically close bacteria, while the single-copy BCSP31 gene is highly specific and widely adopted as a standard target.30,31 Other outer membrane protein genes (eg, omp2, omp31) and the 16S rRNA gene are also used, but variability or conservation across broader bacterial genera can sometimes affect specificity or discriminatory power.32 Our selection of OMP22 was strategic, aiming to combine the broad coverage ensured by its conservation within the genus with the high specificity conferred by its status as a single-copy outer membrane protein gene, thereby minimizing false positives. This rationale is supported by studies from other endemic regions, such as Iran and Turkey, which have also reported successful use of conserved single-copy gene targets for reliable PCR-based diagnosis.33 This was unequivocally validated by our experimental data, which showed a 100% detection rate without non-specific amplification across all 20 clinical isolates. This high specificity also underlies the method’s low cross-reactivity with common Gram-negative bacteria, effectively reducing the risk of false positives that can plague serological assays.
Despite the promising results, our study has limitations that must be acknowledged. First, the sample size is limited, particularly with only two CSF samples, necessitating validation with larger cohorts. Second, all detections were conducted using conventional PCR; future research could employ quantitative PCR (qPCR) technology to enhance sensitivity and facilitate dynamic monitoring of pathogen loads. Additionally, this is a single-center study; future multi-center collaborations could help verify the generalizability of these conclusions.
Conclusions
In conclusion, OMP22-PCR is a reliable molecular diagnostic method with efficacy comparable to that of SAT. Its value lies not only in effectively addressing the deficiencies of SAT in diagnosing early infections and chronic stages but also in its ability to overcome the limitations of serological testing by extending to non-blood samples such as urine and CSF. This method provides a new direction for the early diagnosis and precise prevention and control of brucellosis, particularly in cases of extrapolated infections, and is expected to contribute to the establishment of a more comprehensive diagnostic system.
Ethical Approval and Consent to Participate
This study was reviewed and approved by the ethics committee of the First Affiliated Hospital of Shihezi University (Approval number: KJ2020-034-01). This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The author would like to thank all the colleagues who contributed to the sample collection and sample preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the “Tianshan Talent” High-level Talents Project in the Field of Medicine and Health under the Third Batch of the “2+5” Key Talent Program (TSYC202401B078); Multicenter, Bidirectional Cohort Study on Anti-Infective Regimens for Brucellosis and Brucellosis Complicated by Osteoarthritis (2025DLYJ07); Tianshan Young Talent Scientific and Technological Innovation Team: Innovative Team for Research on Prevention and Treatment of High-incidence Diseases in Central Asia (2023TSYCTD0020); State Key Laboratory for Diagnosis and Treatment of Severe Zoonotic Infectious Diseases (2024KF10006); Development and Clinical Implementation of an Integrated Traditional Chinese-Western Medicine Protocol for Human Brucellosis in the Xinjiang Production and Construction Corps Region (2023AB018-14); Study on Early Diagnosis, Treatment Strategies and Evaluation of Brucellosis (2022B03013-5).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Khalid HM. Seroprevalence and associated risk factors of brucellosis among human population in duhok city, Iraq. Infect Drug Resist. 2023;16:2805–10. doi:10.2147/IDR.S407263
2. Laine CG, Johnson VE, Scott HM, Arenas-Gamboa AM. Malaria misdiagnosis substantially contributes to the underestimation of global human brucellosis incidence. BMC Public Health. 2025;25(1):1425. doi:10.1186/s12889-025-22665-9
3. Kydyshov K, Usenbaev N, Sharshenbekov A, et al. Brucellosis in humans and animals in Kyrgyzstan. Microorganisms. 2022;10(7):1293. doi:10.3390/microorganisms10071293
4. Facciolà A, Palamara MAR, D’Andrea G, et al. Brucellosis is a public health problem in southern Italy: burden and epidemiological trend of human and animal disease. J Infect Public HEALTH. 2018;11(6):861–866. doi:10.1016/j.jiph.2018.07.007
5. Liu Z, Shi Y, Xue C, Yuan M, Li Z, Zheng C. Epidemiological and spatiotemporal clustering analysis of human brucellosis - China, 2019-2023. China CDC Wkly. 2025;7(4):130–136. doi:10.46234/ccdcw2025.020
6. Tulu D. Bovine brucellosis: epidemiology, public health implications, and status of brucellosis in Ethiopia. Vet Med. 2022;13:21–30. doi:10.2147/VMRR.S347337
7. Ali S, Saeed U, Rizwan M, et al. Serosurvey and risk factors associated with brucella infection in high risk occupations from district lahore and kasur of Punjab, Pakistan. Pathog. 2021;10(5):620. doi:10.3390/pathogens10050620
8. Wang W, Wang Z, Jia K, Tang J, Wang L. Clinical and laboratory characteristics of childhood brucellosis in high-risk area of western China. Jpn J Infect Dis. 2022;75(2):127–132. doi:10.7883/yoken.JJID.2021.388
9. Ta N, Mi J, Li X, et al. Epidemiological characteristics and clinical manifestations of brucellosis and Q fever among humans from northeastern inner Mongolia. Infect Drug Resist. 2022;15:6501–6513. doi:10.2147/IDR.S381370
10. Sümer Ş, Aktuğ Demir N, Demir LS, Fındık D, Kölgelier S, Ural O. serum neutrophil gelatinase-associated lipocalin levels in acute brucellosis and brucellar spondylodiscitis. Mikrobiyol Bul. 2022;56(1):1–10. doi:10.5578/mb.20229901
11. Camacho-Martínez JC, Rios-Lugo MJ, Gaytán-Hernández D, Hernández-Mendoza H. Comparison of a brucella enzyme immunoassay and the standard agglutination with 2-mercaptoethanol test in the diagnosis and monitoring of brucellosis in Mexican patients. Clin Lab. 2020;66(9). doi:10.7754/Clin.Lab.2020.190932
12. Yao M, Guo X, Wu X, Bai Q, Sun M, Yin D. Evaluation of the combined use of major outer membrane proteins in the serodiagnosis of brucellosis. Infect Drug Resist. 2022;15:4093–4100. doi:10.2147/IDR.S372411
13. O’Grady D, Kenny K, Power S, Egan J, Ryan F. Detection of yersinia enterocolitica serotype O:9 in the faeces of cattle with false positive reactions in serological tests for brucellosis in Ireland. Vet J. 2016;216:133–135. doi:10.1016/j.tvjl.2016.07.016
14. Bai Q, Li H, Wu X, Shao J, Sun M, Yin D. Comparative analysis of the main outer membrane proteins of Brucella in the diagnosis of brucellosis. Biochem Biophys Res Commun. 2021;560:126–131. doi:10.1016/j.bbrc.2021.04.127
15. Zhou Y, Yun M, Han X, et al. Ischemic stroke as a rare manifestation of neurobrucellosis: a case report. Infect Drug Resist. 2025;18:4329–4335. doi:10.2147/IDR.S544038
16. National Health Commission of the People’s Republic of China. Diagnosis for Brucellosis: WS 269-2019. Beijing: China Standards Press; 2019.
17. Wang Q, Zhao S, Wureli H, et al. Brucella melitensis and B. abortus in eggs, larvae and engorged females of dermacentor marginatus. Ticks Tick-Borne Dis. 2018;9(4):1045–1048. doi:10.1016/j.ttbdis.2018.03.021
18. Modak D, Biswas S, Mondal A, et al. Seroprevalence of brucellosis among animal handlers in West Bengal, India: an occupational health study. AIMS Microbiol. 2024;10(1):1–11. doi:10.3934/microbiol.2024001
19. Vishnu US, Sankarasubramanian J, Gunasekaran P, Rajendhran J. Identification of potential antigens from non-classically secreted proteins and designing novel multitope peptide vaccine candidate against brucella melitensis through reverse vaccinology and immunoinformatics approach. Infect Genet Evol J Mol Epidemiol Evol Genet Infect Dis. 2017;55:151–158. doi:10.1016/j.meegid.2017.09.015
20. Wang H, Liu H, Zhang Q, et al. Natural history of and dynamic changes in clinical manifestation, serology, and treatment of brucellosis, China. Emerg Infect Dis. 2022;28(7):1460–1465. doi:10.3201/eid2807.211766
21. Pourmontaseri H, Rismani M, Karami B, Montaseri Z, Azmi A, Hooshmandi S. A rare case report of neuro-brucellosis with concurrence of depression, visual impairment, bilateral sensorineural hearing loss, and paraplegia. PLoS NeglTrop Dis. 2025;19(7):e0012824. doi:10.1371/journal.pntd.0012824
22. Copur B, Pasa O. The role of the serum tube agglutination test in the monitoring of human brucellosis: evaluation of post-treatment SAT titers. Rev Assoc Med Bras. 2022;68(9):1234–1239. doi:10.1590/1806-9282.20220269
23. Wernery U. Camelid brucellosis: a review. Rev Sci Tech. 2014;33(3):839–857. doi:10.20506/rst.33.3.2322
24. Dal T, Kara SS, Cikman A, et al. Comparison of multiplex real-time polymerase chain reaction with serological tests and culture for diagnosing human brucellosis. J Infect Public HEALTH. 2019;12(3):337–342. doi:10.1016/j.jiph.2018.11.008
25. Suleiman JM, Kandori AH, Saed OAS. Serological, molecular, and clinical diagnosis of caprine brucellosis in tikrit, Iraq. OPEN Vet J. 2025;15(10):5230–5237. doi:10.5455/OVJ.2025.v15.i10.39
26. Freire ML, Machado de Assis TS, Silva SN, Cota G. Diagnosis of human brucellosis: systematic review and meta-analysis. PLoS NeglTrop Dis. 2024;18(3):e0012030. doi:10.1371/journal.pntd.0012030
27. Pal D, Boby N, Kumar S, et al. Visual detection of brucella in bovine biological samples using DNA-activated gold nanoparticles. PLoS One. 2017;12(7):e0180919. doi:10.1371/journal.pone.0180919
28. Zhuang W, He T, Tuerheng J, et al. Neurobrucellosis: laboratory features, clinical characteristics, antibiotic treatment, and clinical outcomes of 21 patients. BMC Infect Dis. 2024;24(1):485. doi:10.1186/s12879-024-09308-x
29. Wu Q, Yuan L, Guo X, Sun M, Yao M, Yin D. Study on antigenic protein Omp2b in combination with Omp31 and BP26 for serological detection of human brucellosis. J Microbiol Methods. 2023;205:106663. doi:10.1016/j.mimet.2022.106663
30. Wang H, Yang H, Yang J, et al. Establishment of a 23S rRNA assay for brucella and its application in evaluating bacterial growth status. Vet Res Commun. 2025;49(2):110. doi:10.1007/s11259-025-10676-1
31. Chang J, Wang N, Zhan JP, et al. A recombinase polymerase amplification-SYBR Green I assay for the rapid and visual detection of Brucella. Folia Microbiol. 2024;69(4):767–774. doi:10.1007/s12223-023-01115-2
32. Madan A, Kumaresan G, Rekha B, et al. Serological and molecular study on caprine brucellosis in Puducherry (India) and its public health significance. Vet Ital. 2024;60(3). doi:10.12834/VetIt.3201.25494.2
33. Chen Z, Zhu Y, Sha T, et al. Design of a new multi-epitope vaccine against Brucella based on T and B cell epitopes using bioinformatics methods. Epidemiol Infect. 2021:149e136. doi:10.1017/S0950268821001229.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.