Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Cross Sectional Survey-Based Study to Investigate the Availability and Utilisation of Home Nutrition Support in Saudi Arabia
Authors Zaher S ![]() , Ajabnoor SM
, Ajabnoor SM ![]()
Received 21 November 2022
Accepted for publication 5 January 2023
Published 12 January 2023 Volume 2023:16 Pages 41—50
DOI https://doi.org/10.2147/JMDH.S398569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sara Zaher,1,2 Sarah M Ajabnoor2,3
1Clinical Nutrition Department, Faculty of Applied Medical Sciences, Taibah University, Madinah, Saudi Arabia; 2National Nutrition Committee (NNC), Saudi Food and Drug Authority (Saudi FDA), Riyadh, Saudi Arabia; 3Clinical Nutrition Department, Faculty of Applied Medical Sciences, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Sara Zaher, Clinical Nutrition Department, Faculty of Applied Medical Sciences, Taibah University, P.O. Box 344, Madinah, 42353, Saudi Arabia, Email [email protected]; [email protected]
Background and Aims: Many patients require long-term nutrition support, typically in the form of home nutrition support (HNS). The availability and utilisation of HNS in Saudi Arabia is currently unknown; therefore, this study was conducted to assess the availability of HNS in Saudi hospitals and to explore factors associated with the availability of HNS in different healthcare facilities in Saudi Arabia.
Methods: A cross-sectional study was conducted among physicians, dietitians, and pharmacists working in Saudi Arabia with regular practice in nutrition support. Data was collected through self-administered web-based survey, which was distributed via social-media platforms.
Results: A total of 114 responses were received from healthcare providers involved in nutrition support across Saudi Arabia. Of the respondents, 55 (48.2%) indicated that nutrition support services were available at their facility. Regression analysis showed that other regions in Saudi Arabia had lower odds of having HNS compared with the Western region (OR=0.01; 95% CI=0.01– 0.69). The university and specialised hospitals had lower odds of having HNS compared with Ministry of Health hospitals (OR=0.11; 95% CI=0.02− 0.71, OR=0.11; 95% CI=0.02− 0.56, respectively). Hospitals with capacities of 100– 250 beds and 251– 500 had higher odds of having HNS than smaller hospitals (OR=13.17; 95% CI=1.09– 159.5, OR=3.11; 95% CI=2.04– 248.77, respectively).
Conclusion: There is lack of published reports from hospitals with implemented HNS. Therefore, it is difficult to assess the current situation of HNS programmes. Future national studies focusing on HNS are warranted as there is a rising international trend in the number of patients requiring HNS.
Keywords: home enteral nutrition, home parenteral nutrition, home nutrition support
Corrigendum for this paper has been published.
Introduction
Gastrointestinal (GI) disorders are usually associated with suboptimal nutrition due to malabsorption and other GI symptoms that limit dietary intake.1 Achieving and maintaining good nutrition is essential to managing the symptoms of GI conditions.2 Nutrition support, either enterally or parenterally, has a crucial role in maintaining or improving clinical outcomes among this group of patients.3
It has been estimated that around 41.6% of patients with inflammatory bowel disease require nutrition support.4 In addition, for most patients with severe short bowel syndrome, parenteral nutrition is considered a cornerstone of therapy.5 Generally, nutrition support, either enterally or parenterally, can be initiated and maintained successfully during hospitalisation. However, a considerable percentage of patients require long-term nutrition support, typically in the form of home nutrition support (HNS).6 This requires an extended period of monitoring by healthcare providers to avoid the associated complications. Although HNS is used for many disorders that mainly affect the GI system, however, HNS can also be indicated for other patients with conditions such as progressive neurological, failure to thrive, severe malnutrition and inborn error of metabolism.7,8
HNS is offered to patients who can receive therapy outside of an acute care setting but cannot meet their nutrient requirements by normal dietary intake.9 It is usually managed by a multidisciplinary team, typically consisting of a physician, dietician, nurse, and pharmacist.5 This team is dedicated to facilitating a safe transition from hospital to home by providing proper nutritional education for patients and their families.10 Regular monitoring of the patient’s clinical and laboratory parameters is essential to ensuring the success of an HNS plan. Bielawska at al. indicated that patients receiving HNS should be seen by a multidisciplinary nutrition team every 1–3 months at the initiation phase and the once a year when they are stable.5 Data about any established multidisciplinary team to manage patients on HNS is lacking in Saudi Arabia. However, this has been previously explored in other middle eastern countries such as Iran where they indicated that presence of multidisciplinary nutrition support team to manage patients with intestinal failure is associated with improvement in patients’ clinical outcomes and reduce their mortality and morbidity.11
Up-to-date availability and utilisation of HNS in Saudi Arabia are currently unknown and needs to be investigated. The Ministry of health (MOH) sector in Saudi Arabia, which currently operates 287 hospitals, is the largest health sector in Saudi Arabia.12 Most of the home healthcare services in Saudi Arabia are publicly funded. However, there is a variation between these hospitals in terms of the delivered services. Therefore, the purpose of this study is to assess the availability of HNS in Saudi hospitals and to explore factors associated with the presence of HNS in different healthcare facilities in Saudi Arabia.
Methods
Study Design and Participants
A cross-sectional study was conducted using an online questionnaire between August 2020 and February 2021. Dietitians, clinical pharmacists, and doctors with regular involvement in nutrition support (ie, gastroenterologists, surgeons, and critical care intensivists) who worked in hospitals in Saudi Arabia were eligible to participated in the study. All other healthcare professionals were excluded. We included participants who worked in both sectors governmental and private hospitals. Medical cities, Military hospitals, Ministry of Health (MOH) hospitals, National guard hospitals, Security Forces Hospital, Specialized hospitals, University teaching hospitals, are considered governmental hospitals. However, the variation between them is related to the source of budget and funding provided to operate the hospital. Participants who worked in private hospitals were also recruited in this study.
Eligible participants in this study were recruited via a chain referral sampling. Members of national societies, like the Saudi Gastroenterology Association (SGA), the Saudi Society for Clinical Nutrition (SSCN), the Saudi Society of Clinical Pharmacy (SSCP), the Saudi Oncology Association, and the Saudi General Surgery Society (SGSS), were invited to participate in the study via e-mail containing a link directing them to the questionnaire. We also used convenient sampling to achieve adequate number of participants via social media platforms (ie, Twitter and WhatsApp). The overall response rate was not calculated, as recruitment for the study was online and open.
Ethical Approval
The current study was approved by the Unit of the Biomedical Ethics Research Committee at King Abdulaziz University in Jeddah, Saudi Arabia (HA-02-J-008). Consent for participation was obtained from all the study participants by answering a mandatory question to indicate that they agree to participate. The first page of the questionnaire contained assurances of confidentiality and anonymity. Data was securely stored, and access was only granted to the main study researchers to ensure proper data management.
Survey Development
The questionnaire comprised two main sections covering 15 items. It started with a brief introduction stating the study aims, contact information of the researcher, and the consent form. The included questions in the survey were developed by the study investigators after reviewing previous international questionnaires concerning nutrition support practice in clinical setting;13–15 however, other questions were designed by the researchers. The questionnaire was then pilot tested on one dietitian, two PhD holders in clinical nutrition, and two pharmacists and was adjusted based on the provided feedback. The first section of the questionnaire covered the demographic data of the participants. The second part included multiple choice questions to assess the availability and practices of HNS, including the type of HNS provided in the facility, the healthcare professionals responsible for patient training and education, monitoring methods, and the most encountered complications of HNS. The questionnaire was in English language and electronically developed Google Forms.
Statistical Analysis
Data were downloaded and analysed using the Statistical Package for Social Sciences software version 23 (SPSS Inc.). The Shapiro–Wilk test was used to assess the normality of continuous variables. Frequencies and percentages were presented to describe the data.
Fisher’s exact test was used to determine the association between the availability of HNS services and geographical distribution of the participants and the type and capacity of the healthcare facility in which they worked. A follow-up post-hoc test was then performed to identify the source of the significant results of Fisher’s exact test.
Logistic regression analysis was performed to identify the factors that influenced the availability of HNS services in healthcare facilities in Saudi Arabia. The availability of HNS as a categorial variable was used as the outcome in the regression models. The independent variables used in the models were region (Western coded as 1, Central coded as 2, other regions coded as 3), type of healthcare facility (Ministry of Health [MOH] hospital coded as 1, military hospital coded as 2, university teaching hospital coded as 3, specialised hospital coded as 4, National Guard hospital coded as 5, medical city coded as 6, and private hospital coded as 7), and the capacity of the healthcare facility (<100 beds coded as 1, 100–250 beds coded as 2, 251–500 coded as 3, >500 beds coded as 4). All the tests were two-tailed, with a significance level of 95%.
Results
We received a total of 114 responses from healthcare providers involved in nutrition support across Saudi Arabia, including 38 physicians, 62 dietitians, and 14 pharmacists. Of the respondents, 55 (48.2%) indicated that they have nutrition support services at their facility and 59 participants indicated that either they do not provide HNS services at their facility or they are not aware of such services. Most of the responses were from the Western region. The characteristics of the study participants are presented in Table 1.
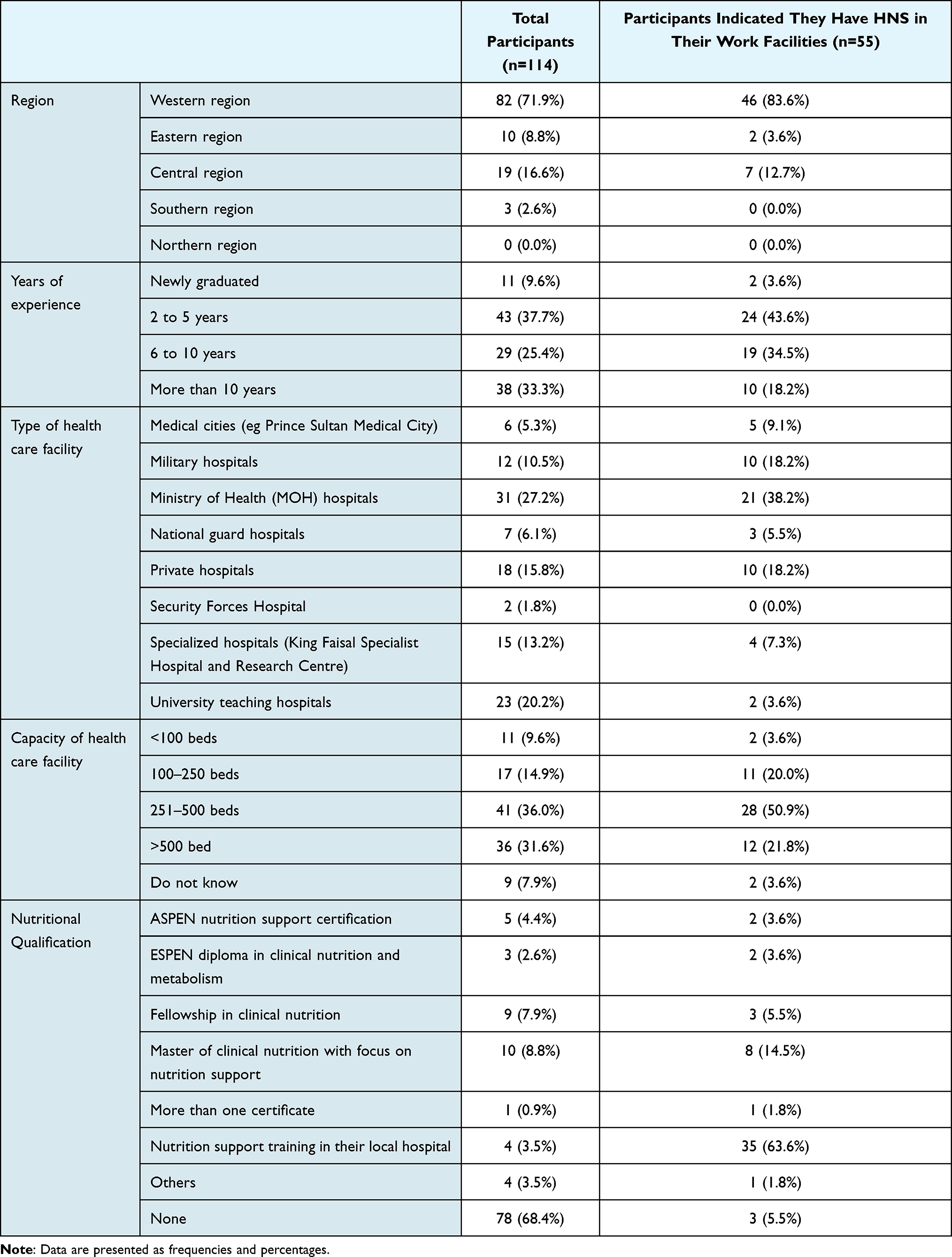 |
Table 1 General Characteristics of the Study Participants |
Of the 55 participants who indicated that they had HNS in their facility, 44 (80%) participants reported that they provided home enteral nutrition (HEN) services in their facility, 10 (18%) participants reported that they provided both home EN and home parenteral nutrition (PN) services, and only 1 (1.8%) participant indicated that their facility provided only home PN services. It was reported by 47 (89%) participants that dietitians were involved in training patients and family members on HNS, 33 (60%) participants reported that physicians were involved, and 30 (55%) participants reported that nurses were also involved in this task. Regarding the monitoring process of HNS, 37 (67%) participants reported that the dietitians were involved in the monitoring process, 30 (55%) participants reported that physicians were involved, and 24 (44%) participants reported that nurses were also involved in this task. However, no other allied healthcare professions were reported by the study participants to be involved in the training and monitoring of HNS. The most common complication of HNS reported by the participants was infection reported by 33 (60%) participants followed by mechanical complications reported by 32 (58%) participants (Table 2).
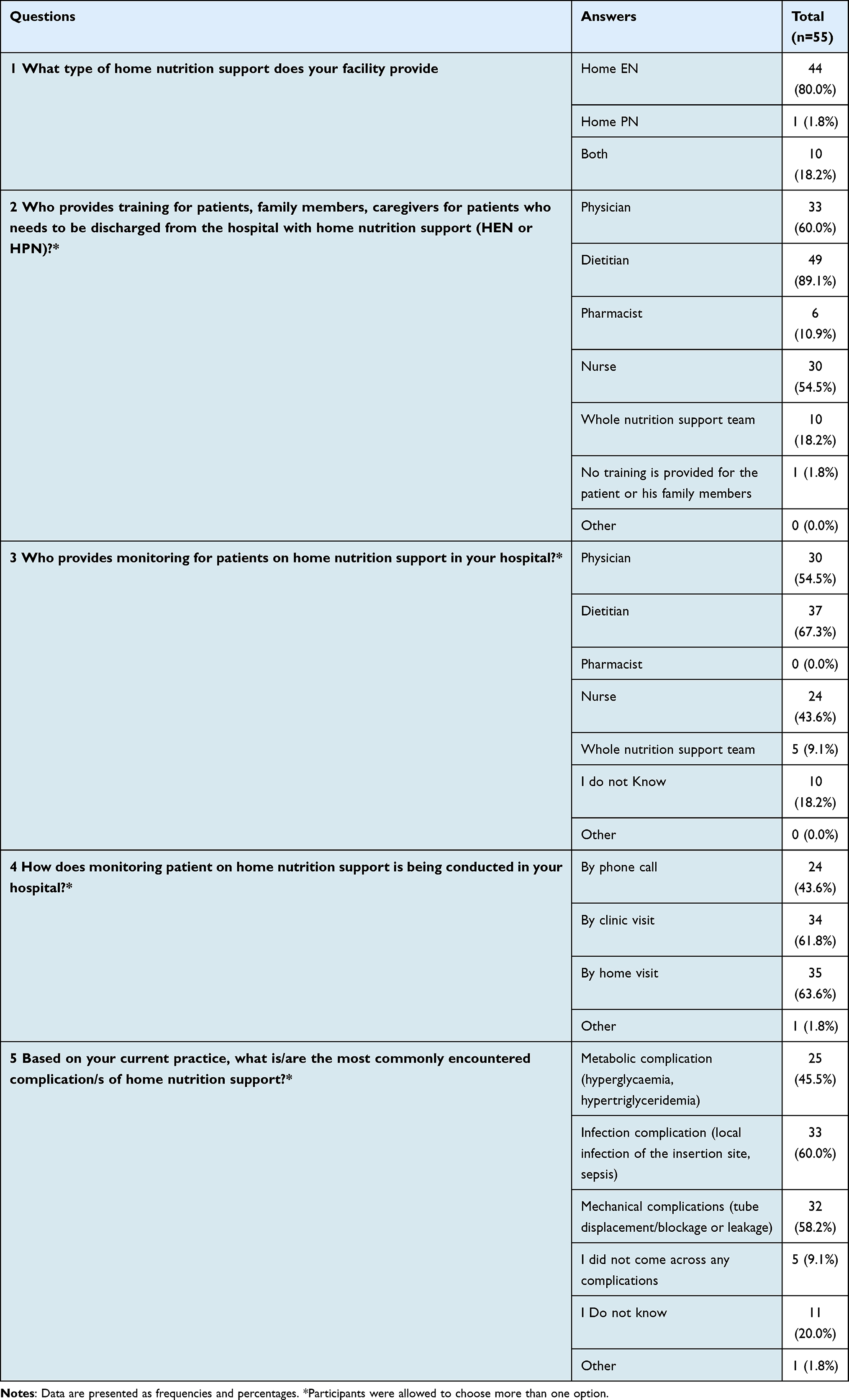 |
Table 2 Home Nutrition Support (HNS) Services in Saudi Arabia |
Fisher’s exact test showed a statistical association between the availability of HNS services and the geographical distribution of the participants and the type and capacity of the healthcare facility in which they worked (p<0.05) (Table 3). Post-hoc analysis showed a significantly higher rate of HNS utilisation in the Western regions compared with other regions (p=0.0067). In addition, post-hoc analysis revealed that MOH hospitals had higher rates of HNS utilisation compared with other types of healthcare facilities (p<0.001), and university hospitals had statistically lower rates of HNS utilisation compared with other hospitals (p<0.001). Furthermore, hospitals with a capacity of 251–500 beds had statistically higher rates of HNS utilisation compared with smaller hospitals (p=0.00).
 |
Table 3 Assessing the Association Between the Geographical Distribution of the Participants, the Type and Capacity of the Healthcare Facility in Which They Worked, and the Availability of HNS Services |
Data obtained from the logistic regression analysis showed that other regions in Saudi Arabia had lower odds of having HNS compared with the Western region (OR=0.01; 95% CI=0.01 −0.69). The regression model showed that university hospitals and specialised hospitals had statistically lower odds of having HNS compared with MOH hospitals (OR=0.11; 95% CI=0.02 −0.71, OR=0.11; 95% CI=0.02 −0.56, respectively). In contrast, hospitals with a capacity of 100–250 beds and 251–500 had higher odds of having HNS than smaller hospitals (OR=13.17; 95% CI=1.09–159.5, OR=3.11; 95% CI=2.04 −248.77, respectively) (Table 4).
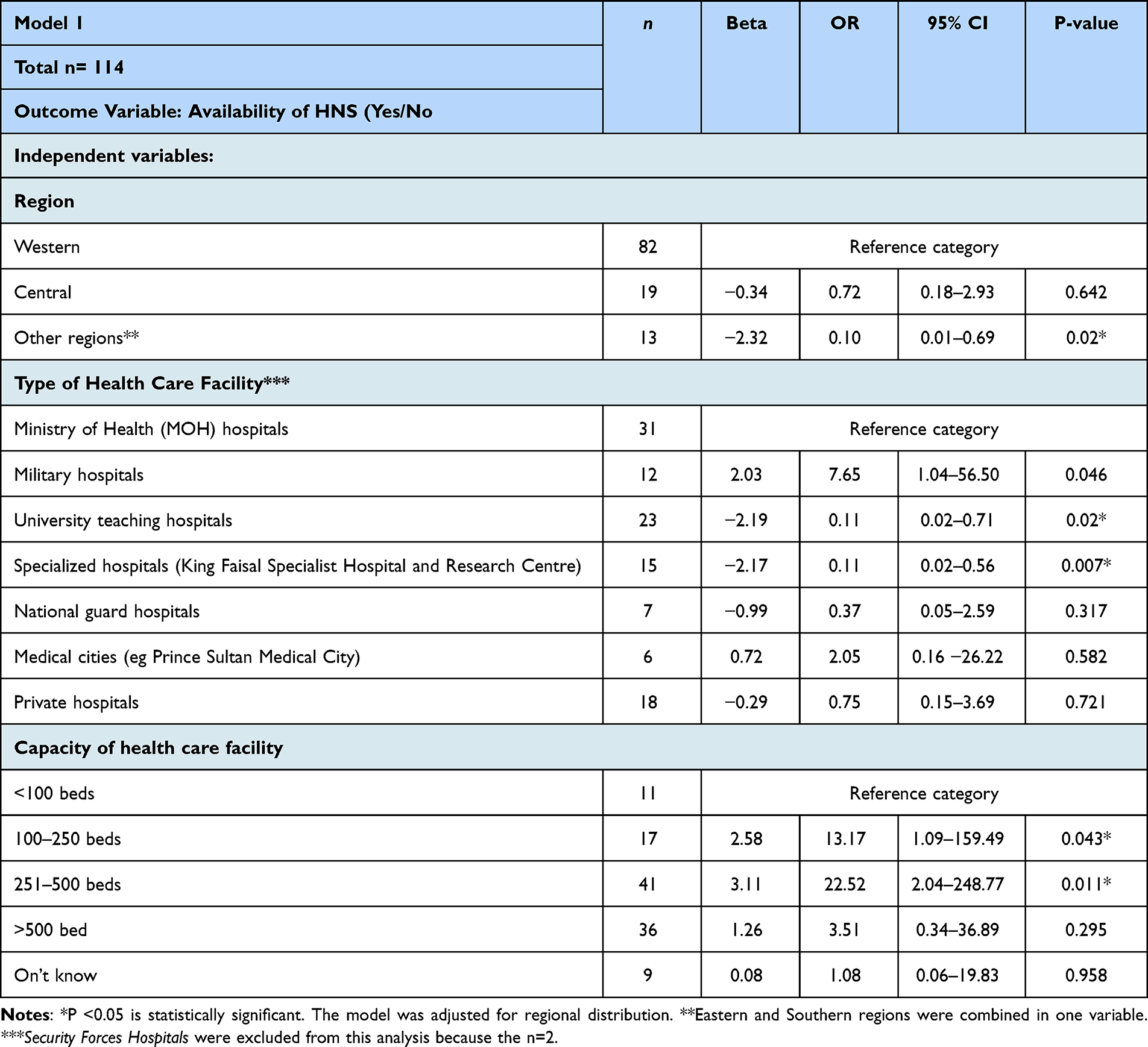 |
Table 4 Logistic Regression Analysis of HNS Services, the Geographical Distribution of the Participants, and the Type and Capacity of Healthcare Facility in Which They Worked |
Discussion
Globally, the prevalence of HNS services is rising in parallel with the rise in scientific data supporting the beneficial outcomes of nutrition support.16 However, the availability of a focused HNS service with medical professionals differs between countries and hospitals. In Saudi Arabia, the availability and practices of HNS services have yet to be investigated. Overall, this study revealed that nearly one-half of healthcare professionals had HNS services at their facility, while the main type of service provided was HEN. The role of participants in the process of patient training and monitoring varied across professions. The most reported complication of HNS was infection. Factors related to geographical region, hospital type, and capacity were identified as possible predictors for the availability of HNS.
We found that many nutrition support professionals provided HEN. As a life-sustaining intervention, many types of patients are continuously dependent on HEN. In contrast, HPN provision was less reported by the study participants. Safe delivery of HPN is challenging and necessitates the implementation of an interdisciplinary nutrition support team (NST).17 Although the number of home healthcare programmes that provides HNS in Saudi Arabia is unknown, according to recently published national data from the MOH, 236 hospitals currently provide home healthcare, of which some incorporate HEN, HPN, or both services.12 HPN programmes are considered new in Saudi Arabia, and the first programme in the region was established in 2004 in a governmental tertiary care hospital.18 Our study confirmed that HPN is underutilized. Thus, the underutilization of HPN services needs to be addressed by the country’s healthcare workforce. Unfortunately, regional data concerning HPN-associated challenges and outcomes are lacking. However, a previous international study performed in Europe by an expert group found a significant correlation between HPN duration and quality of life19. Therefore, future research in the region needs to focus on describing the level of HPN expertise for nutrition support clinicians, clinical challenges, and outcomes associated with HPN in order to implement an effective HPN program in different healthcare facilities in Saudi Arabia. Such program requires a multidisciplinary nutrition support team with adequate funding, clinical expertise, and proper nutritional education as reported by a previous report developed by the American Society of Parenteral and Enteral Nutrition (ASPEN)20.
Study participants reported variation in the involvement of healthcare professionals in HNS practices. Most participants reported that dietitians were frequently involved in the education and training of patients receiving HNS, followed by doctors and nurses. Adequate training and delivery of instructions to patients and caregivers was found to be associated with better adherence and fewer complications.21 According to recent European society for Clinical Nutrition and Metabolism (ESPEN) guidelines, hospitals with patients receiving HNS should have at least one specialised nutrition support dietitian or nurse and ideally an established multidisciplinary team.9 In this study, few participants reported that the whole NST was involved in the training process.
Due to the complexity of HNS therapies and their risk of complications (ie, aspiration pneumonia, infections, mechanical complications, GI issues, venous thrombosis, and metabolic complications), close and regular monitoring by a specialised nutrition support clinician is highly recommended.22 In this study, the most reported complications were infections followed by mechanical complications. HPN is frequently associated with complications, namely catheter infections, which result in a higher rate of hospital readmission.8 In contrast, HEN is considered safe, and its associated complications can easily be prevented and treated with simple measures.8 Implementing an NST with various allied healthcare experts in addition to doctors, dietitians, and nurses is strongly recommended for a better management approach.9 In this study, participants reported that only dietitians, physicians, and nurses were involved in the monitoring process. However, no other allied healthcare professions were reported by the study participants to be involved in the training and monitoring process of HNS.
Multivariate regression analysis showed that the Western region of the country had a significant influence on the use of HNS. A possible interpretation of this finding is that many clinicians in this study were based in the Western region. According to previous studies, healthcare accessibility in some regions of Saudi Arabia (ie, Northern, Southern, and areas with a small population sizes) is generally far from equal.23,24 Good access to HNS services across all regions will result in better population health outcomes. Another factor that influenced the provision of HNS by the healthcare professionals in this study was the type of hospital. A significantly higher rate of HNS utilisation was reported in MOH hospitals. The MOH sector, which currently operates 287 hospitals, is the largest health sector in Saudi Arabia.12 Most of the home healthcare services in Saudi Arabia are publicly funded, and the first programme under the MOH was initiated in 2008.25 Nonetheless, due to the unavailability of data describing how HNS programmes are being implemented in Saudi Arabia as a part of home healthcare services, it is challenging to assess the current regional situation of HNS programmes.
In addition, we found that hospitals with capacities of 100–250 beds and 251–500 had higher odds of providing HNS compared with smaller hospitals. Patients receiving HNS are usually discharged from hospitals with acute care services or rehabilitation care facilities (eg, intestinal failure rehabilitation centres).8 Important components to maximising HNS treatment are structural facilities and trained manpower. The recent ESPEN guidelines for HPN state that HPN facilities must be able to provide offices for outpatient visits and beds for patients who require hospital admission.22
To our knowledge, this study is the first to assess the provision and utilisation of HNS services in Saudi Arabia. The current study provides directions for future national studies focusing on HNS patients, caregivers, and healthcare providers. Moreover, the sample for this study was not limited to a single profession; it included doctors, dietitians, and pharmacists, which broadened the scope of the findings. A possible limitation of this study is the high proportion of healthcare professionals residing in the Western region, which limits the generalisability of the findings across the country. Another limitation of this study might be the sampling method, which might be associated with selection bias. However, this study was conducted to initially explore the current situation of HNS in Saudi Arabia, future research concerning HNS should be conducted in a larger scale.
Conclusion
In Saudi Arabia, published reports from hospitals with implemented HNS are lacking. Therefore, it is difficult to assess the current situation of HNS programmes. However, there is a rising international trend in the number of patients depending on HNS therapies. Therefore, home healthcare services should support the development of more HNS programmes across all regions of Saudi Arabia, with standardised monitoring and patient training protocols.
Acknowledgments
We would like to thank all the healthcare professionals who kindly agreed to participate in the study. We would also like to thank the expert panel for their effort and time in revising the questionnaire and for providing helpful feedback. We would like to thank Dr. Hani Jawa and Dr. Rania Malatani for their help in the data collection.
Author Contributions
The authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Montoro-Huguet MA, Belloc B, Domínguez-Cajal M. Small and large intestine (I): malabsorption of nutrients. Nutrients. 2021;13:1254. doi:10.3390/nu13041254
2. El-Salhy M. Nutritional management of gastrointestinal diseases and disorders. Nutrients. 2019;11:3013. doi:10.3390/nu11123013
3. Krasaelap A, Kovacic K, Goday PS. Nutrition management in pediatric gastrointestinal motility disorders. Nutr Clin Pract. 2020;35:265–272. doi:10.1002/ncp.10319
4. Liu J, Ge X, Ouyang C, et al. Prevalence of malnutrition, its risk factors, and the use of nutrition support in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2022;28:S59–S66. doi:10.1093/ibd/izab345
5. Bielawska B, Allard JP. Parenteral nutrition and intestinal failure. Nutrients. 2017;9:466. doi:10.3390/nu9050466
6. Dibb M, Teubner A, Theis V, Shaffer J, Lal S. Review article: the management of long-term parenteral nutrition. Aliment Pharmacol Ther. 2013;37:587–603. doi:10.1111/apt.12209
7. Puntis JW. Nutritional support at home and in the community. Arch Dis Child. 2001;84:295–298. doi:10.1136/adc.84.4.295
8. Konrad D, Mitchell R, Hendrickson E, et al. Home nutrition support. In: The ASPEN Adult Nutrition Support Core Curriculum.
9. Bischoff SC, Arends J, Bozzetti F, et al. ESPEN guideline on home enteral nutrition. Clin Nutr. 2020;39:5–22. doi:10.1016/j.clnu.2019.04.022
10. Koenen B, Benjamin R, Panciu A. Navigating the Challenges of Home Parenteral Nutrition. Nutr Clin Pract. 2019;34:204–209. doi:10.1002/ncp.10264
11. Shafiekhani M, Nikoupour H, Mirjalili M. The experience and outcomes of multidisciplinary clinical pharmacist-led parenteral nutrition service for individuals with intestinal failure in a center without home parenteral nutrition. Eur J Clin Nutr. 2022;76:841–847. doi:10.1038/s41430-021-01048-4
12. Ministry of Health statistical Yearbook. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-2021.pdf.
13. Behara AS, Peterson SJ, Chen Y, et al. Nutrition support in the critically ill: a physician survey. JPEN J Parenter Enteral Nutr. 2008;32:113–119. doi:10.1177/0148607108314763
14. Cahill NE, Narasimhan S, Dhaliwal R, Heyland DK. Attitudes and beliefs related to the Canadian critical care nutrition practice guidelines: an international survey of critical care physicians and dietitians. JPEN J Parenter Enteral Nutr. 2010;34:685–696. doi:10.1177/0148607110361908
15. Singh H, Duerksen DR. Survey of clinical nutrition practices of Canadian gastroenterologists. Can J Gastroenterol. 2006;20:527–530. doi:10.1155/2006/835462
16. Mundi MS, Pattinson A, McMahon MT, Davidson J, Hurt RT. Prevalence of home parenteral and enteral nutrition in the United States. Nutr Clin Pract. 2017;32:799–805. doi:10.1177/0884533617718472
17. Winkler M, Guenter P. Long-term home parenteral nutrition: it takes an interdisciplinary approach. J Infus Nurs. 2014;37:389–395. doi:10.1097/NAN.0000000000000068
18. Al-Tawil ES, Almuhareb AM, Amin HM. Catheter-related blood stream infection in patients receiving long-term home parenteral nutrition: tertiary care hospital experience in Saudi Arabia. Saudi J Gastroenterol. 2016;22:304–308. doi:10.4103/1319-3767.187604
19. Baxter JP, Fayers PM, Bozzetti F, et al. An international study of the quality of life of adult patients treated with home parenteral nutrition. Clin Nutr. 2019;38:1788–1796. doi:10.1016/j.clnu.2018.07.024
20. Mundi MS, Mechanick JI, Mohamed Elfadil O, et al. Optimizing the nutrition support care model: analysis of survey data. JPEN J Parenter Enteral Nutr. 2022;46:1709–1724. doi:10.1002/jpen.2326
21. Metzger LC. Education materials for home nutrition support consumers. Nutr Clin Pract. 2010;25:451–470. doi:10.1177/0884533610379608
22. Pironi L, Boeykens K, Bozzetti F, et al. ESPEN Guideline ESPEN guideline on home parenteral nutrition. Clinical Nutrition. 2020;39(6):1645–1666. doi:10.1016/j.clnu.2020.03.005
23. Al-Ahmadi K, Al-Zahrani A, Al-Ahmadi S. Spatial accessibility to cancer care facilities in Saudi Arabia; 2014.
24. Baazeem M, Tennant M, Kruger E. Determining variations in access to public hospitals in Makkah, Kingdom of Saudi Arabia: a GIS-based approach. Saudi J Med Med Sci. 2021;1:26–32. doi:10.1159/000513632
25. Al-Surimi K, Al-Harbi I, El-Metwally A, Badri M. Quality of life among home healthcare patients in Saudi Arabia: household-based survey. Health Qual Life Outcomes. 2019;17:21. doi:10.1186/s12955-019-1095-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.