Back to Journals » Infection and Drug Resistance » Volume 15
A Cross-Sectional Study to Evaluate Antimicrobial Susceptibility of Uropathogens from South Punjab, Pakistan
Authors Idrees MM ![]() , Rasool MF
, Rasool MF ![]() , Imran I, Khalid A, Saeed A, Ahmad T, Alqahtani F
, Imran I, Khalid A, Saeed A, Ahmad T, Alqahtani F ![]()
Received 28 January 2022
Accepted for publication 7 April 2022
Published 15 April 2022 Volume 2022:15 Pages 1845—1855
DOI https://doi.org/10.2147/IDR.S356489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Muhammad Mubashar Idrees,1,2 Muhammad Fawad Rasool,3 Imran Imran,4 Ayesha Khalid,2 Ali Saeed,1 Tanveer Ahmad,5 Faleh Alqahtani6
1Institute of Molecular Biology and Biotechnology, Bahauddin Zakariya University, Multan, 60800, Pakistan; 2Multan Institute of Kidney Diseases (MIKD), Multan, Pakistan; 3Department of Pharmacy Practice, Faculty of Pharmacy, Bahauddin Zakariya University, Multan, 60800, Pakistan; 4Department of Pharmacology, Faculty of Pharmacy, Bahauddin Zakariya University, Multan, 60800, Pakistan; 5Institute for Advanced Biosciences (IAB), CNRS UMR5309, INSERM U1209, Grenoble Alpes University, La Tronche, 38700, France; 6Department of Pharmacology and Toxicology, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Ali Saeed; Faleh Alqahtani, Email [email protected]; [email protected]
Background: Urinary tract infections (UTIs) are a common infection caused by uropathogenic bacteria. Drug resistance against common antibiotics is a leading cause of treatment failure in UTIs.
Objective: This study was conducted to check the prevalence of antimicrobial susceptibility against uropathogens and identify the best treatment option against UTIs.
Methods: In this cross-sectional study, urine samples (n = 1000) were collected and cultured for pure bacterial growth by using cysteine–lactose–electrolyte-deficient (CLED) media. After physical and biochemical characterization, antibacterial susceptibility was performed by the Kirby–Bauer disk diffusion method.
Results: Uropathogenic bacteria were successfully isolated in 57% (n = 572) of total tested samples (n = 1000). Escherichia coli 51.2% (n = 293/572), Klebsiella species 15.4% (n = 88/572), Enterococcus species 15.4% (n = 88/572), Pseudomonas species 9.4% (n = 54/572), Staphylococcus aureus 3.2% (n = 18/572), coagulase-negative Staphylococci (CoNS) 3.0% (n = 17/572) and Proteus species 2.4% (n = 14/572) were the most prevalent organism in UTIs. Prevalence of Gram-negative rods (GNRs) was 78.5% (n = 449/572) among UTI patients as compared to Gram-positive cocci (GPCs) 21.5% (n = 123/572). Escherichia coli 65.3% (n = 293/449), Klebsiella species 19.6% (n = 88/449), Pseudomonas species 12.0% (54/449) and Proteus species 3.1% (n = 14/449) were the most prevalent GNRs in UTIs, while Enterococcus species 71.5% (n = 88/123), Staphylococcus aureus 14.6% (n = 18/123) and coagulase-negative Staphylococci (CoNS) 13.8% (17/123) were the most prevalent GPCs in UTIs. The majority of isolated uropathogens showed resistance against routinely used antibiotics. However, teicoplanin and linezolid were the most effective drugs against GPCs and piperacillin/tazobactam, meropenem and imipenem were the most effective drugs against GNRs. Nitrofurantoin and fosfomycin were shown to be most effective against both GNRs and GPCs.
Conclusion: In conclusion, Escherichia coli (GNRs) and Enterococcus species (GPCs) are the most prevalent organisms among UTIs patients, which are shown to be antibiotic-resistant to the most commonly used antibiotics. However, nitrofurantoin and fosfomycin are the most effective drugs against uropathogens in UTIs.
Keywords: uropathogens, UTIs, biochemical analysis, antibacterial drugs
Introduction
Urinary tract infections (UTIs) are the most common community or hospital-acquired infection caused by bacteria, which affects 150 million people worldwide every year.1,2 Normally, all ages and populations can be affected by UTIs. However, certain factors including age, gender, genetic factor, race, and sexual activity are risk factors for UTIs.3 Females are more at risk for UTIs due to their anatomical positions of the urethra, so almost 35% of females suffer from symptomatic UTIs in their lifespan.4,5 In addition, vaginal normal flora, pregnancy, sexual intercourse, and obstruction of the urethra may increase the risk for UTIs in females.6 UTIs can be either symptomatic or asymptomatic. However, symptomatic UTIs have a high threshold for bacteriuria (100,000 CFU/mL urine) and sites of infections characterized UTIs into pyelonephritis, cystitis, urethritis, or prostatitis.7,8 UTIs are mainly caused by enteric microflora, for example, Escherichia coli (E. coli) is the most prevalent cause of UTIs (75–85%).7,9 Enterobacteriaceae, Pseudomonas species, Enterococcus species, Staphylococcus aureus (S. aureus), and Coagulase Negative Staphylococci (CoNS) are also associated with UTIs.10 Mostly, a single bacterial species is responsible for UTI rather than more bacterial strains or species.11 Excessive use of antibiotics, false diagnosis, deficiency of productive research, lack of awareness, and self-medication may cause bacterial resistance due to the development of new genetic variants, resulting from treatment failure either in developed or under developing countries and leading to increased morbidity.12,13 In uropathogenic bacteria, the abundance of virulence genes is coding to different virulence factors, eg FimH: adherence factor produced by uropathogenic Escherichia coli (UPEC)14 and associated underlying mechanisms making it difficult to treat these infectious diseases.15,16 Bacteria-harboring genetic variants, eg hlyA, Utah, cnf1, ibeA and cdtB in UPEC leading to antibiotic resistance have been increased remarkably and globally become a serious challenge for medical treatment.17,18 Extended-spectrum β-lactamases (ESBLs), Klebsiella pneumoniae carbapenemase (KPC)19 and Metallo-β-lactamases are produced by corresponding genes present in the uropathogenic bacterial chromosome that contribute to antibiotic resistance.20 It usually occurs in a normal health care setting in which antibiotics are administered without antibiotic susceptibility testing. In Pakistan, this is a leading risk factor in the development of multidrug-resistant bacteria in UTIs.
It is an alarming condition for health care to overcome multidrug resistance bacteria associated with bacterial infections including UTIs.21 It has become important to get information about the antibacterial resistance and sensitivity to overcome this challenge.22 However, overall epidemiological information on the incidence of UTIs and antibiotics susceptibility against these pathogens was lacking in South Punjab, a province of 5 million people. Six hundred patients out of thousand patients enrolled in 4 months at MIKD with chronic kidney disease (CKD) were also suffering from UTIs, indicating a very high incidence and prevalence of UTIs likely due to multidrug-resistant bacteria and lack of availability of effective drugs.
Continuous surveillance is required on the use of antibiotics, drug resistance, and susceptibility in UTIs to control the antibiotic resistance and to find the most susceptible drugs against uropathogens.21 We should also need to identify the mutant variants leading to antibiotic resistance by using molecular techniques.23 In the most recent study conducted in Pakistan in a far province, Escherichia coli was found to be the most prevalent isolates, and fosfomycin and imipenem were the most susceptible drugs against uropathogens.24 Although multiple studies have also been conducted on antibiotic resistance and sensitivity in South Punjab, the remarkable last study conducted in this region to find multidrug resistance and sensitivity survey in uropathogens was six years ago.25 However, this study has shown very limited epidemiological information on multidrug resistance and susceptibility in UTIs in this region. In South Punjab, medical practitioners do not have a piece of good information over the prevalence of antibiotic resistance and susceptibility in uropathogenic associated with UTIs. Recommendations of antibiotics without antibiotic sensitivity testing are likely to further aggravate the situation. Thus, an urgent study was needed and designed for the epidemiological surveillance of uropathogens associated with UTIs along with the information of antibiotics sensitivity or resistance in this region. Another perspective of this study is to find out the most susceptible drugs against different uropathogens causing UTIs, which will help to reduce the economic burden to treat infectious diseases.
Materials and Methods
Study Design and Ethical Approvals
A cross-sectional study was designed and conducted at Multan Institute of Kidney Diseases (MIKD) Hospital, Multan, Pakistan and Institute of Molecular Biology and Biotechnology (IMBB), Bahauddin Zakariya University (BZU), Multan, Pakistan, from September 2020 to December 2020. All ethical approvals were duly obtained from the Institutional Review Board (IRB) of IMBB with approval number 334/A. Informed consent was obtained from all the participants, and the study was performed as per the Declaration of Helsinki.
Sample Collection
MIKD hospital is a dedicated hospital for kidney diseases. One thousand urine samples (n = 1000) were collected from the patients with urinary tract dysfunction without any age limit, gender, or other discrimination. UTis patients were characterized by physical urine examination, i.e putrid or foul odor, smoky or milky color and microscopic urine examination, ie bacteriuria, hematuria, pyuria in this study. All UTI patients with bacteriuria and pyuria26 visited “MIKD” Hospital, and urine samples were taken in sterile urine culture and sensitivity (c/s) container having boric acid.27 Samples were transported immediately to the laboratory on ice and processed within two hours for further analysis.
Inoculation
Samples were inoculated onto Cysteine Lactose Electrolyte Deficient (CLED, Oxoid, Basingstoke Hampshire, United Kingdom) media, selective and differential media.28 A sterile wire loop with 0.01 µL was used for the midstream urine sample and 0.1 µL for the percutaneous nephrolithotomy (PCNL) urine sample. After inoculation, media plates were incubated into an incubator at 37°C.29 After 24 hours of incubation, pure growth was considered for further gram staining and biochemical analysis with antimicrobial susceptibility testing.
Gram Staining
A commercially prepared gram stain (Oxoid, Basingstoke Hampshire, United Kingdom) was used to differentiate between gram-positive and negative bacteria, either rods or cocci, as previously described.30–32 After confirming the bacterial nature, the biochemical tests were performed for identification and characterization of isolates along with antimicrobial testing.
Biochemical Identification
Biochemical analysis was performed to distinguish the bacterial strains. Different types of biochemical analysis including triple sugar iron, motility, indole, sulfide, urease, citrate, and oxidase assays were used for gram-negative rods (GNRs), while catalase, coagulase, and bile esculin assays were used for the gram-positive cocci (GPCs) bacteria.29
Antimicrobial Susceptibility
Pure colonies were used to make inoculum (0.5 McFarland for gram-negative and 1.0 McFarland for gram-positive bacteria). Samples were further cultured on Muller Hinton agar (MHA, Oxoid, Basingstoke Hampshire, United Kingdom) with a cotton swab. Different antibiotics were dispensed on MHA after lawning. Antibacterial activity of the below-mentioned antibiotic disks (Oxoid, Basingstoke Hampshire, United Kingdom) was done by the Kirby–Bauer disk diffusion technique.29,33 Antibiotics resistant (R) and sensitive (S) isolates were identified according to the guidelines of Clinical and Laboratory Standards Institute (CLSI)34 and the European Committee on Antimicrobial Susceptibility Testing (EUCAST).35 According to CLSI and EUCAST, each bacterial strain has its specific antibiotics recommendations. Antibiotics recommended to use against Enterobacteriaceae include ampicillin (AMP), augmentin (AMC), piperacillin/tazobactam (TZP), cefotaxime (CTX), ceftazidime (CAZ), meropenem (MEM), imipenem (IPM), gentamicin (G), amikacin (AK), nalidixic acid (NA), norfloxacin (NOR), ciprofloxacin (CIP), co-trimoxazole (SXT), nitrofurantoin (F), sulbactam/cefoperazone (SCF) and fosfomycin (FOS). Antibiotics are recommended for Pseudomonas species include piperacillin/tazobactam (TZP), ceftazidime (CAZ), cefepime (FEP), colistin (CT), meropenem (MEM), imipenem (IPM), gentamicin (G), amikacin (AK), norfloxacin (NOR), ciprofloxacin (CIP) and sulzone (SCF). Antibiotics are recommended for Staphylococcus aureus (S. aureus) and Enterococcus species include penicillin (P), ampicillin (AMP), augmentin (AMC), linezolid (LZD), teicoplanin (TEC), gentamicin (G), amikacin (AK), ciprofloxacin (CIP), levofloxacin (LFX), nitrofurantoin (F) and fosfomycin (FOS). Antibiotics are recommended for S. aureus, not against Enterococcus species, including fusidic acid (FD), tetracycline (TE), co-trimoxazole (SXT) and cefoxitin (FOX).34,35
Quality Control
American Type Culture Collection (ATCC) strains (Manassas, Virginia, near Washington DC, USA) of Escherichia coli (ATCC 25922), Pseudomonas aeruginosa (ATCC 8427) and Staphylococcus aureus (ATCC 25923) were used as a control to check the growth-supporting ability of prepared media (CLED and MHA agar) throughout the study.35 Escherichia coli (ATCC 25922) and Staphylococcus aureus (ATCC 25923) were used as quality control along with samples during gram staining. Biochemical tests were performed including catalase test, coagulase test, indole test, triple sugar iron test, citrate test, urease test and oxidase test. Accuracy and reproducibility of biochemical test results were confirmed by using ATCC strains (Staphylococcus aureus (ATCC 25923), Streptococcus pyogenes (ATCC 19615), Staphylococcus epidermidis (ATCC 12228), Escherichia coli (ATCC 25922), Pseudomonas aeruginosa (ATCC 27853) and Proteus mirabilis (ATCC 35659)) as positive and negative quality control. Different antibiotics were used against different ATCC strains to check the accuracy and reproducibility of antimicrobial sensitivity technique and the results were interpreted according to CLSI guidelines.36
Statistics
A chi-square test was performed to analyze the data using GraphPad Prism 9 (GraphPad Software, San Diego, CA, USA). p-value ≤0.05 was considered to be significant statistically.
Results
Prevalence and Distribution of Bacterial Isolates
In this study, one thousand (n = 1000) urine samples were collected and analyzed from the patients with suspected urinary tract infections (UTIs). All of these samples were inoculated onto CLED plates, and only six hundred (n = 600) patients were positive for bacterial infection. Twenty-eight out of the six hundred (n = 28) samples were rejected due to contamination of skin normal microflora (Staphylococcus epidermidis). Uropathogens were detected and successfully isolated from the remaining 57% (n = 572) samples and further analyzed for identification and characterization. Escherichia coli 51.2% (n = 293/572), Klebsiella species 15.4% (n = 88/572), Enterococcus species 15.4% (88/572), Pseudomonas species 9.4% (n = 54/572), Staphylococcus aureus 3.2% (n = 18/572), Coagulase Negative Staphylococci (CoNS) 3.0% (n = 17/572) and Proteus species 2.5% (n = 14/572) were most prevalent uropathogens in analyzed samples (Figure 1).
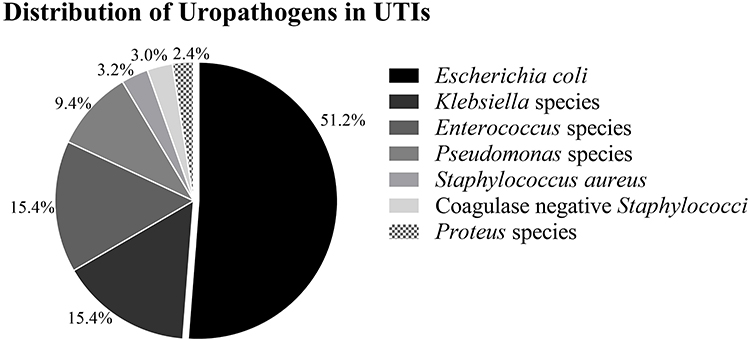 |
Figure 1 Distribution and prevalence of bacterial isolates in UTIs. Distribution of most prevalent (%) uropathogenic bacteria among the total number of isolates (n=572) from UTIs. Escherichia coli were the most prevalent (51.2%) among the UTIs pathogens followed by Klebsiella species (15.4%), Enterococcus species (15.4%), Pseudomonas species (9.4%), Staphylococcus aureus (3.2%), Coagulase-negative Staphylococci (CoNS) (3.0%) and Proteus species (2.4%) Bacterial isolates presented were significantly associated with UTI (p-value was < 0.000). |
Prevalence of Gram-Negative Rods (GNRs) and Gram-Positive Cocci (GPCs)
Gram-negative rods (GNRs) were more prevalent in UTIs patients. Prevalence of Gram-negative rods (GNRs) was 78.5% (n = 449) in UTIs patients as compared to Gram-positive cocci (GPCs) bacteria 21.5% (n = 123). Escherichia coli, Klebsiella species, Pseudomonas species, and Proteus species were the most prevalent uropathogens among GNRs, while Enterococcus species, S. aureus, and Coagulase Negative Staphylococci (CoNS) were the most prevalent uropathogens among GPCs.
The prevalence of the Escherichia coli, Klebsiella species, Pseudomonas species, and Proteus species was 65.3% (n = 293/449), 19.6% (n = 88/449), 12.0% (n = 54/449), and 3.1% (n = 14/449), respectively, among GNRs, while the prevalence of Enterococcus species, Staphylococcus aureus, and Coagulase Negative Staphylococci (CoNS) was 71.5% (n=88/123), 14.6% (n=18/123), and 13.8% (n=17/123), respectively, among GPCs (Table 1). The GNRs and GPCs bacteria were significantly associated with UTIs (p-value <0.000).
 |
Table 1 Prevalence of Gram-Negative Rods (GNRs) and Gram-Positive Cocci (GPCs) in UTIs |
Effectiveness of Antibiotics Against Enterobacteriaceae
In this study, the majority of bacteria isolated from urine samples of the patients positive for UTIs belong to the family Enterobacteriaceae, including Escherichia coli, Klebsiella species, and Proteus species. These isolates have been shown to be resistant to the most commonly used antibiotics against UTIs. Antibiotics were shown resistance from higher to lower level include AMP > NA > AMC > CTX > NOR > CAZ > SXT >CIP, while certain antibiotics were also shown to have a great susceptibility against Enterobacteriaceae which included FOS > F > IPM > MEM > AK > TZP > SCF > G (Figure 2).
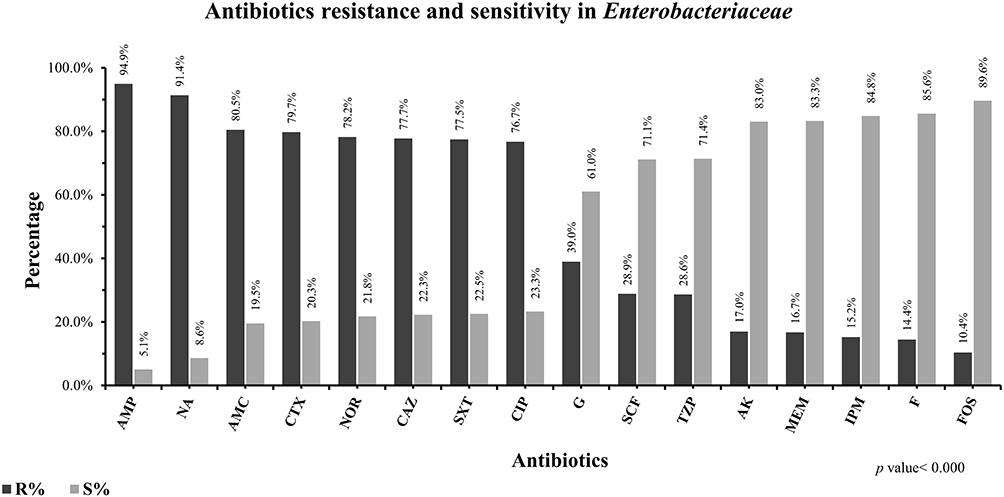 |
Figure 2 The pattern of antibiotics resistance and susceptibility against Enterobacteriaceae. Frequency of antimicrobial resistance and susceptibility of antibiotics including ampicillin (AMP), nalidixic acid (NA), augmentin (AMC), cefotaxime (CTX), norfloxacin (NOR), ceftazidime (CAZ), co-trimoxazole (SXT), ciprofloxacin (CIP), gentamicin (G), sulbactam/cefoperazone (SCF), piperacillin/tazobactam (TZP), meropenem (MEM), imipenem (IPM), amikacin (AK), nitrofurantoin (F), fosfomycin (FOS) were presented in percentages against Enterobacteriaceae. Resistance (black bars) and susceptibility (grey bars) of all antibiotics mentioned in this graph were significantly associated with UTIs caused by bacterial isolates belonging to Enterobacteriaceae such as Escherichia coli, Klebsiella species, and Proteus species (p-value was < 0.000). |
Effectiveness of Antibiotics Against Pseudomonas Species
Pseudomonas species (n = 54) were the second most important organism after Enterobacteriaceae among GNRs. Different antibiotics were tested against Pseudomonas species to check their effectiveness. CT was the most sensitive drug followed by TZP > AK > MEM > IPM > SCF, respectively, that can be used as a choice of treatment if UTIs occurred by Pseudomonas species. NOR was the most resistant drug followed by G > CIP > CAZ > FEP that was ineffective in treating UTIs (Figure 3).
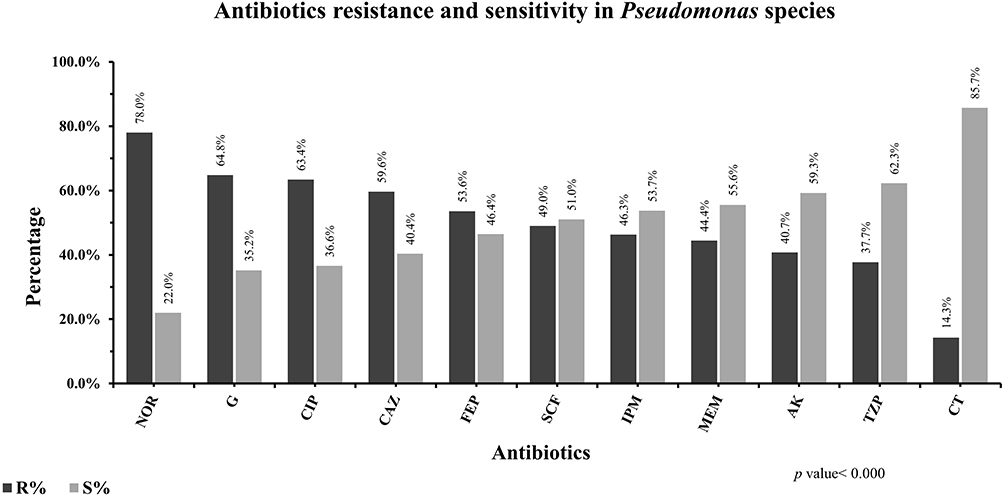 |
Figure 3 The pattern of antibiotics effectiveness against Pseudomonas species in UTIs. Frequency of antimicrobial resistance and susceptibility of antibiotics including norfloxacin (NOR), gentamicin (G), ciprofloxacin (CIP), ceftazidime (CAZ), cefepime (FEP), sulbactam/cefoperazone (SCF), imipenem (IPM), meropenem (MEM), amikacin (AK), piperacillin/tazobactam (TZP), colistin (CT) were presented in percentage against Pseudomonas species. Resistance (black bars) and susceptibility (grey bars) of these antibiotics mentioned in this graph were significantly associated with UTIs associated caused by Pseudomonas species (p-value was < 0.000). |
Effectiveness of Antibiotics Against Enterococcus Species
Enterococcus species (n = 88) was the most prevalent organism among GPCs bacteria isolated from UTIs patients followed by Staphylococcus aureus and CoNS. The commonly recommended antibiotics against these bacteria were shown to have a great resistance (AK > CIP > G), while LZD was the most sensitive drug followed by TEC > F > SCF > FOS > AMP > AMC, which can be used in UTIs caused by Enterococcus species (Figure 4).
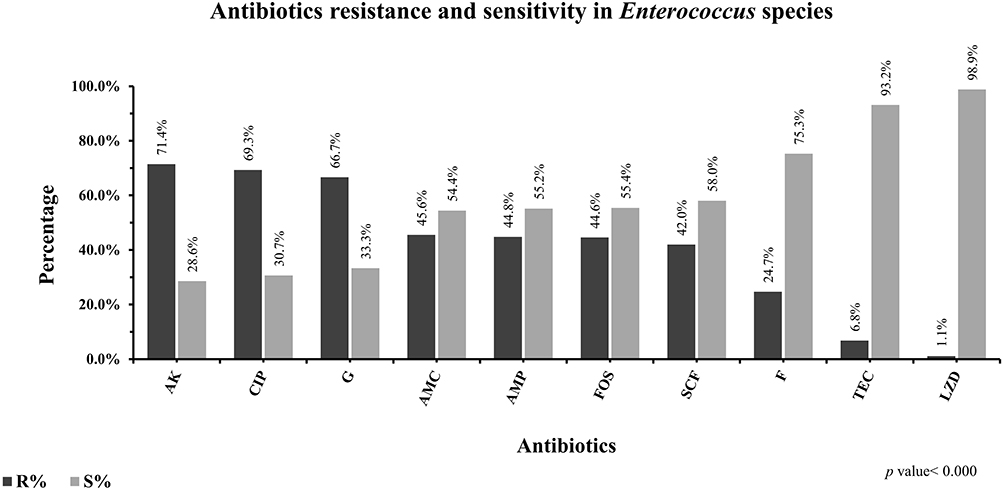 |
Figure 4 The pattern of antibiotics effectiveness against Enterococcus species in UTIs. Frequency of antimicrobial resistance and susceptibility of antibiotics including amikacin (AK), ciprofloxacin (CIP), gentamicin (G), augmentin (AMC), ampicillin (AMP), fosfomycin (FOS), sulbactam/cefoperazone (SCF), nitrofurantoin (F), teicoplanin (TEC), linezolid (LZD) were presented in percentage against Enterococcus species. Resistance (black bars) and susceptibility (grey bars) of all antibiotics mentioned in this graph were significantly associated with UTIs caused by Enterococcus species (p-value was < 0.000). |
Effectiveness of Antibiotics Against Staphylococcus Species
Staphylococcus species were also identified to cause UTIs in our population with less frequency as compared to others. Different antibiotics were tested to check their effectiveness against these pathogens to cure the UTIs. CIP was the most resistant drug in the case of Staphylococci species, followed by LFX > P > TE > AMC > FOX, respectively. TEC and LZD were shown to have a great susceptibility followed to F > AK > FD > SXT > G (Figure 5).
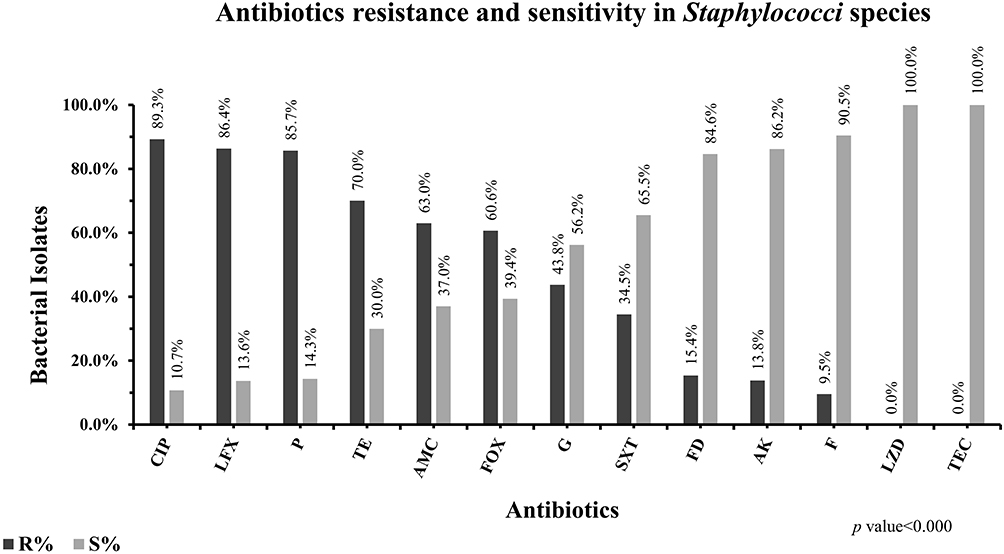 |
Figure 5 The pattern of antibiotics effectiveness against Staphylococci species in UTIs. Frequency of antimicrobial susceptibility of antibiotics including ciprofloxacin (CIP), levofloxacin (LFX), penicillin (P), tetracycline (TE), augmentin (AMC), fosfomycin (FOS), gentamicin (G), co-trimoxazole (SXT), fusidic acid (FD), amikacin (AK), nitrofurantoin (F), linezolid (LZD), teicoplanin (TEC) was presented in percentage against Staphylococci species. Resistance (black bars) and susceptibility (grey bars) of all antibiotics mentioned in this graph were significantly associated with UTIs caused by Staphylococci species (p-value was < 0.000). |
Discussion
Urinary tract infections (UTIs) are common infections in both Indoor Patients (IPD) and Outdoor Patients (OPD) settings throughout the world. Here, we studied UTIs in both IPD and OPD settings and further antibiotic sensitivity was analyzed. Escherichia coli (65.3%) were the predominant isolates among the gram-negative bacteria, while Enterococcus species (71.5%) were the predominant isolates among the gram-positive bacteria. Klebsiella species, Proteus species, Pseudomonas species, and S. aureus were other uropathogens that can cause UTIs. Previously, Gupta et al 2002,37 and Haque et al 20157 also reported similar uropathogens associated with UTIs. Similar to the previous study,5,38 Escherichia coli was the most prevalent uropathogen in this study associated with UTIs in the South Punjab region of Pakistan.
Drug resistance patterns among uropathogens have been increased and become a major challenge in clinical practices to treat UTIs. AMP, AMC, CTX, CAZ, CIP, LFX, NA, and SXT are commonly used drugs to overcome the UTIs caused by gram-positive and negative bacteria in developing countries like Pakistan.39 Unfortunately, all these antibiotics were identified as ineffective against uropathogens in our setting. It is an alarming condition for physicians to use antibiotics as an effective therapeutic option to control UTIs.40
In this study, Enterobacteriaceae found highly resistant to AMP (94.9%), NA (91.4%), AMC (80.5%), CTX (79.7%), NOR (78.2%), SXT (77.5%), CAZ (77.7%) and CIP (76.7%) and less resistant to G (39.0%), SCF (28.9%), TZP (28.6%), AK (17%), MEM (16.7%), IMP (15.2%), F (14.4%) and FOS (10.4%). Falagas et al, 201041 also reported high resistance of TZP, CTX, CAZ, IMP, G, CIP, SXT, while Woldemariam et al, 201942 reported less resistance of AMP, AMC. CTX, CAZ, G, AK, CIP, F against Enterobacteriaceae, both studies showed a different pattern of antibiotic resistance. The difference in drug resistance patterns in similar bacteria in different populations is likely due to different prevention and treatment strategies against UTIs in different geographic regions. However, certain antibiotics also showed similar resistance patterns in different geographic regions indicating the involvement of common mechanisms involved in drug resistance. For example, in our study, FOS and SXT showed 10.4% and 77.5% resistance, respectively, against Enterobacteriaceae, in a previous study conducted in Greece, a similar resistance pattern of these drugs, FOS (2%) and SXT (87) in UTIs, has been also reported,41 which indicates the involvement of common mechanisms involved in drug resistance in these uropathogens. However, some studies conducted in our region39 reported different drug resistance patterns including CTX, CAZ, MEM, IMP, G, AK, NOR, F, FOS against Enterobacteriaceae, which were also indicating the different treatment strategies of UTIs in the same regions or misuse of drugs and self-medication by the population; however, this study also reported antibiotic resistance pattern of AMC, CIP, and NA similar to our study.
Mehrishi et al, 201943 reported less resistance of AMP, TZP, CTX, CAZ, IMP and NOR, while MEM, CIP, SXT showed more resistance against Enterobacteriaceae. This difference likely came from the frequency of use of certain antibiotics. However, the antibiotic resistance pattern of F, AK, G in this population was similar to our study. Similar to our data, other researchers reported ceftazidime resistance up to 100% in India,44 while in other countries, Malaysia and China ceftazidime resistance has been reported at 11% and 28%, respectively.45,46 Variation in findings with different studies conducted by different authors in different countries is due to epidemiological variation, various treatment strategies against UTIs, samples numbers, and awareness about the misuse of antibiotics among the population.
Pseudomonas species is an important bacterium that contributes to hospital-acquired UTIs and other infections. Similar to the previous report,39 we found TZP, CT, MEM, IPM, AK, SCF sensitive, while CAZ, FEP, G, NOR, CIP were resistant against Pseudomonas species Similarly, another study47 also reported some resistance patterns (MEM, IPM, TZP, G) in Pseudomonas species; however, the sample size in this study was very low.
Among gram-positive bacteria, Enterococcus species were the most prevalent organism associated with UTIs in our population. We found G, AK, CIP resistant, while AMP, AMC, LZD, TEC, F, SCF, FOS were the most sensitive drugs against Enterococcus species. Similarly, Woldemariam et al, 201942 also reported that F was the most sensitive drug against Enterococcus species in Ethiopian UTI patients, most likely due to having the same treatment strategy and similar mechanism to develop antibiotics resistance in Enterococcus species. On the other hand, Muhammad et al, 202039 reported resistance of VA, CIP, FOS in Enterococcus species along with AMC and LZD in our populations likely due to different antibiotics strategies in a different province of our country. Pouladfar et al, 201747 reported antibiotic resistance patterns including AMP, AMC, CIP, and F in Enterococcus species in the Iranian population, while LZD and VA were the most sensitive drugs against Enterococcus species in this study.
In this study, we reported that Staphylococcus species were shown to have a high level of resistance to P, AMC, FOX, TE, CIP and LFX antibiotics that cannot be used to treat this infection, while FD, LZD, TEC, G, AK, SXT and F were reported to be more sensitive drugs against Staphylococcus species. These findings were also confirmed in different studies in different geographic regions including Ethiopia, Pakistan, and Iran,39,42,47 respectively, which confirmed the P, AMC, FOX, TE, CIP, LFX more resistant and G, SXT, F more sensitive drugs against Staphylococcus species in UTIs.
Ciprofloxacin was considered the most effective drug against uropathogens; however, it lost effectiveness in the past few years likely due to irrational use or self-medication, which leads to the development of resistance against CIP along with other drugs including 1st, 2nd, and 3rd generations of cephalosporins.48,49 Our study demonstrated that nitrofurantoin and fosfomycin were the most effective drugs against both gram-negative and positive bacteria. Other studies also supported our finding that nitrofurantoin and fosfomycin were good alternative treatment options for UTIs.41–43,50 Similar to previous studies,51,52 we also reported that F, FOS, TEC, and LZD were the most effective drugs against gram-positive bacteria, while F, FOS, TZP, MEM, and IPM were the most effective drugs against gram-negative bacteria. Fosfomycin was identified as an effective drug against Enterobacteriaceae and Enterococcus species causing UTIs.
In conclusion, drug resistance against uropathogens is an evolving process that is increasing gradually. Ampicillin, augmentin, cefotaxime, ceftazidime, ciprofloxacin, levofloxacin, nalidixic acid and co-trimoxazole are used as a choice of drugs to overcome the UTIs caused by gram-positive and negative bacteria in developing countries like Pakistan. Unfortunately, most of the antibiotics used to treat UTIs showed a high level of antibiotic resistance in our setting due to overuse and/or misuse of these antibiotics, prolonged stay in the hospital, no proper monitoring, lack of testing and awareness in the population, which is an alarming situation to treat UTIs. Our study advocates that nitrofurantoin and fosfomycin were the most effective drugs against both gram-negative and positive bacteria that can be a better option against UTIs. In addition to nitrofurantoin and fosfomycin, teicoplanin and linezolid were identified as effective drugs against gram-positive bacteria and piperacillin/tazobactam, meropenem, and imipenem against gram-negative bacteria. Thus, continuous investigation and monitoring are required to identify the drug effectiveness and resistance against uropathogens to treat UTIs. However, authorities should take actions to prevent the overuse or self-medication of these highly susceptible drugs in UTIs to avoid the development of resistance.
Acknowledgments
The authors extended their appreciation to the Distinguished Scientist Fellowship program at King Saud University, Riyadh, Saudi Arabia, for funding this work through Research Supporting Project Number (RSP-2021/131). The authors further appreciate the support provided by ORIC, Bahauddin Zakariya University, Multan, Pakistan, through Project No. ORIC/2021/143.
Disclosure
No potential conflict of interest in this work was reported by the authors.
References
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–284. doi:10.1038/nrmicro3432
2. McLellan LK, Hunstad DA. Urinary tract infection: pathogenesis and outlook. Trends Mol Med. 2016;22(11):946–957. doi:10.1016/j.molmed.2016.09.003
3. Heffner VA, Gorelick MH. Pediatric urinary tract infection. Clin Pediatr Emerg Med. 2008;9(4):233–237. doi:10.1016/j.cpem.2008.09.009
4. Schaeffer A, Rajan N, Cao Q, et al. Host pathogenesis in urinary tract infections. Int J Antimicrob Agents. 2001;17(4):245–251. doi:10.1016/S0924-8579(01)00302-8
5. Behzadi P, Behzadi E. The microbial agents of urinary tract infections at central laboratory of Dr. Shariati Hospital, Tehran, Iran. Turk Klin Tip Bilim. 2008;28(4):445.
6. Stamm WE. Urinary tract infections and pyelonephritis. In: Harrison's Principles of Internal Medicine. Vol. 16, 2005:1715.
7. Haque R, Akter ML, Salam MA. Prevalence and susceptibility of uropathogens: a recent report from a teaching hospital in Bangladesh. BMC Res Notes. 2015;8(1):1–5. doi:10.1186/s13104-015-1408-1
8. Idrees MM, Saeed A. Genetic and molecular mechanisms of multidrug-resistance in uropathogens and novel therapeutic combat. In: Biochemistry of Drug Resistance. Springer; 2021:505–538.
9. Rampure R, Gangane R, Oli AK, Chandrakanth K. Prevalence of MDR-ESBL producing Klebsiella pneumoniae isolated from clinical samples. J Microbiol Biotech Res. 2013;3(1):32–39.
10. Issakhanian L, Behzadi P. Antimicrobial agents and urinary tract infections. Curr Pharm Des. 2019;25(12):1409–1423. doi:10.2174/1381612825999190619130216
11. Ahmed S, Rashid H. Urinary tract infection in adults. Bangladesh Renal J. 1996;15:23–31.
12. Gold HS, Moellering RC Jr. Antimicrobial-drug resistance. N Engl J Med. 1996;335(19):1445–1453. doi:10.1056/NEJM199611073351907
13. Khanum H, Munir F, Shafiullah A, Muznebin F. Prevalence and comparative likelihood of urinary tract infection (UTI) among female out patients in BSMMU. Bangladesh J Zool. 2012;40(2):231–239. doi:10.3329/bjz.v40i2.14317
14. Sarshar M, Behzadi P, Ambrosi C, Zagaglia C, Palamara AT, Scribano D. FimH and anti-adhesive therapeutics: a disarming strategy against uropathogens. Antibiotics. 2020;9(7):397. doi:10.3390/antibiotics9070397
15. Behzadi P. Classical chaperone-usher (CU) adhesive fimbriome: uropathogenic Escherichia coli (UPEC) and urinary tract infections (UTIs). Folia Microbiol (Praha). 2020;65(1):45–65. doi:10.1007/s12223-019-00719-x
16. Khonsari MS, Behzadi P, Foroohi F. The prevalence of type 3 fimbriae in Uropathogenic Escherichia coli isolated from clinical urine samples. Meta Gene. 2021;28:100881. doi:10.1016/j.mgene.2021.100881
17. Septiana L, Harahap U, Ginting F. Identification of gyrA gene resistance on bacteria Escherichia coli and Klebsiella pneumoniae in urinary tract infection patients in Haji Adam Malik Center Hospital, Medan, Indonesia. Asian J Pharm Res. 2020;8(4):27–29.
18. Hozzari A, Behzadi P, Kerishchi Khiabani P, Sholeh M, Sabokroo N. Clinical cases, drug resistance, and virulence genes profiling in Uropathogenic Escherichia coli. J Appl Genet. 2020;61(2):265–273. doi:10.1007/s13353-020-00542-y
19. Ahmadi M, Ranjbar R, Behzadi P, Mohammadian T. Virulence factors, antibiotic resistance patterns, and molecular types of clinical isolates of Klebsiella Pneumoniae. Expert Rev Anti Infect Ther. 2021:1–10. doi:10.1080/14787210.2022.1990040
20. Behzadi P, García-Perdomo HA, Karpiński TM, Issakhanian L. Metallo-ß-lactamases: a review. Mol Biol Rep. 2020;47(8):6281–6294. doi:10.1007/s11033-020-05651-9
21. Behzadi P, Urbán E, Matuz M, Benkő R, Gajdács M. The role of gram-negative bacteria in urinary tract infections: current concepts and therapeutic options. Adv Microbiol Infect Dis Public Health. 2020:35–69. doi:10.1007/5584_2020_566
22. Farrell D, Morrissey I, De Rubeis D, Robbins M, Felmingham D. A UK multicentre study of the antimicrobial susceptibility of bacterial pathogens causing urinary tract infection. J Infect. 2003;46(2):94–100. doi:10.1053/jinf.2002.1091
23. Behzadi P, Behzadi E. Uropathogenic Escherichia coli: an ideal resource for DNA microarray probe designing.
24. Malik J, Javed N, Malik F, Ishaq U, Ahmed Z. Microbial Resistance in Urinary Tract Infections. Cureus. 2020;12(5). doi:10.7759/cureus.8110
25. Sohail M, Khurshid M, Saleem HGM, Javed H, Khan AA. Characteristics and antibiotic resistance of urinary tract pathogens isolated from Punjab, Pakistan. Jundishapur J Microbiol. 2015;8(7). doi:10.5812/jjm.19272v2
26. Stamm WE. Measurement of pyuria and its relation to bacteriuria. Am J Med. 1983;75(1):53–58. doi:10.1016/0002-9343(83)90073-6
27. Lum K, Meers P. Boric acid converts urine into an effective bacteriostatic transport medium. J Infect. 1989;18(1):51–58. doi:10.1016/S0163-4453(89)93667-0
28. Phuong NT, Lee BJ, Choi JK, Kang JS, Kwon KI. Enantioselective pharmacokinetics of carvedilol in human volunteers. Arch Pharm Res. 2004;27(9):973–977. doi:10.1007/BF02975853
29. Cheesbrough M. District Laboratory Practice in Tropical Countries, Part 2. Cambridge university press; 2005.
30. Ali Raza J, Movahed A. Use of cardiovascular medications in the elderly. Int J Cardiol. 2002;85(2–3):203–215. doi:10.1016/S0167-5273(02)00193-6
31. Johnson TN. The problems in scaling adult drug doses to children. Arch Dis Child. 2008;93(3):207–211. doi:10.1136/adc.2006.114835
32. Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA. Manual of Clinical Microbiology.
33. Sahil A. Manual of Laboratory Medicine.
34. Humphries R, Bobenchik AM, Hindler JA, Schuetz AN. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100. J Clin Microbiol. 2021;59(12):e00213–00221. doi:10.1128/JCM.00213-21
35. Testing ECoAS. EUCAST: clinical breakpoints and dosing of antibiotics; 2019.
36. Weinstein MP, Lewis JS. The clinical and laboratory standards institute subcommittee on antimicrobial susceptibility testing: background, organization, functions, and processes. J Clin Microbiol. 2020;58(3):e01864–01819. doi:10.1128/JCM.01864-19
37. Palewar M, Mudshingkar S, Dohe V, Bharadwaj R. Spectrum and antimicrobial susceptibility pattern of uropathogens: indoor versus outdoor isolates. Int J Trop Dis Health. 2017;27(1):1–7. doi:10.9734/IJTDH/2017/36611
38. Akhtar SMH, Sattar A, Rizwan W, Cheema NA, Anwar A. Microbes and antibiotic susceptibility patterns of urinary tract infections in toilet-trained children at a Tertiary Care Hospital of Sialkot, Pakistan. Prof Med J. 2021;28(01):22–26. doi:10.29309/TPMJ/2021.28.01.4657
39. Muhammad A, Khan S, Ali N, Rehman M, Ali I. Prevalence and antibiotic susceptibility pattern of uropathogens in outpatients at a tertiary care hospital. New Microbes New Infect. 2020;36:100716. doi:10.1016/j.nmni.2020.100716
40. Mohammed MA, Alnour TM, Shakurfo OM, Aburass MM. Prevalence and antimicrobial resistance pattern of bacterial strains isolated from patients with urinary tract infection in Messalata Central Hospital, Libya. Asian Pac J Trop Med. 2016;9(8):771–776. doi:10.1016/j.apjtm.2016.06.011
41. Falagas ME, Maraki S, Karageorgopoulos DE, Kastoris AC, Mavromanolakis E, Samonis G. Antimicrobial susceptibility of multidrug-resistant (MDR) and extensively drug-resistant (XDR) Enterobacteriaceae isolates to fosfomycin. Int J Antimicrob Agents. 2010;35(3):240–243. doi:10.1016/j.ijantimicag.2009.10.019
42. Woldemariam HK, Geleta DA, Tulu KD, et al. Common uropathogens and their antibiotic susceptibility pattern among diabetic patients. BMC Infect Dis. 2019;19(1):1–10.
43. Mehrishi P, Faujdar SS, Kumar S, Solanki S, Sharma A. Antibiotic susceptibility profile of uropathogens in rural population of Himachal Pradesh, India: where We are heading? Biomed Biotech Res J. 2019;3(3):171.
44. Jena J, Sahoo RK, Debata NK, Subudhi E. Prevalence of TEM, SHV, and CTX-M genes of extended-spectrum β-lactamase-producing Escherichia coli strains isolated from urinary tract infections in adults. 3 Biotech. 2017;7(4):1–7. doi:10.1007/s13205-017-0879-2
45. Lim K-T, Yasin R, Yeo -C-C, Puthucheary S, Thong K-L. Characterization of multidrug resistant ESBL-producing Escherichia coli isolates from hospitals in Malaysia. J Biomed Biotechnol. 2009;2009:1–10. doi:10.1155/2009/165637
46. Xue Y, Chen J, Hua Y. Resistance of strains producing extended-spectrum [beta]-lactamases and genotype distribution among Escherichia coli in China. Pak J Zool. 2012;44(2):53–57.
47. Pouladfar G, Basiratnia M, Anvarinejad M, Abbasi P, Amirmoezi F, Zare S. The antibiotic susceptibility patterns of uropathogens among children with urinary tract infection in Shiraz. Medicine. 2017;96(37):e7834. doi:10.1097/MD.0000000000007834
48. Lu P-L, Liu Y-C, Toh H-S, et al. Epidemiology and antimicrobial susceptibility profiles of Gram-negative bacteria causing urinary tract infections in the Asia-Pacific region: 2009–2010 results from the Study for Monitoring Antimicrobial Resistance Trends (SMART). Int J Antimicrob Agents. 2012;40:S37–S43. doi:10.1016/S0924-8579(12)70008-0
49. Falup-Pecurariu O, Leibovitz E, Bucur M, Lixandru R, Bleotu L, Falup-Pecurariu C. High resistance rates to 2 nd and 3 rd generation cephalosporins, ciprofloxacin and gentamicin of the uropathogens isolated in young infants hospitalized with first urinary tract infection. Biomed Res. 2017;28(20):8675–8680.
50. Prasad B, Arora P. Antibiotic susceptibility profiling of bacterial biodiversity associated with urinary tract infections. World Sci News. 2021;155:129–139.
51. Sharifian M, Karimi A, Tabatabaei SR, Anvaripour N. Microbial sensitivity pattern in urinary tract infections in children: a single center experience of 1177 urine cultures. Jpn J Infect Dis. 2006;59(6):380.
52. Sharmin S, Alamgir F, Fahmida M, Saleh AA. Antimicrobial sensitivity pattern of uropathogens in children. Bangladesh J Med Microbiol. 2009;3(2):18–22. doi:10.3329/bjmm.v3i2.5322
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.