Back to Journals » Patient Preference and Adherence » Volume 17
A Cross-Sectional Analysis into the Willingness and Hesitancy to Test and Vaccinate Against COVID-19 Among the Elderly Population in the Kingdom of Saudi Arabia
Authors AlOmar RS ![]() , AlShamlan NA
, AlShamlan NA ![]() , Shafey MM
, Shafey MM ![]() , AlAbdulKader AM
, AlAbdulKader AM ![]() , AlHarkan KS
, AlHarkan KS ![]() , Al-Johani WM
, Al-Johani WM ![]() , Motabgani S, Alkaltham NK, Alharbi AA
, Motabgani S, Alkaltham NK, Alharbi AA ![]()
Received 21 September 2023
Accepted for publication 25 November 2023
Published 5 December 2023 Volume 2023:17 Pages 3173—3184
DOI https://doi.org/10.2147/PPA.S440821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Reem S AlOmar,1 Nouf A AlShamlan,1 Marwa Mahmoud Shafey,1 Assim M AlAbdulKader,1 Khalid S AlHarkan,1 Wejdan M Al-Johani,1 Sameerah Motabgani,1 Nourah K Alkaltham,1 Abdullah A Alharbi2
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Family and Community Medicine Department, Faculty of Medicine, Jazan University, Jazan City, Jazan, Saudi Arabia
Correspondence: Reem S AlOmar, Email [email protected]
Introduction: COVID-19 remains a public health concern. Vaccinations, testing and tracing have been proven to provide strong protection against severe illness and death. Older adults are amongst the groups with an increased risk of severe illness. This study aimed to explore the willingness and hesitancy of the elderly population in the Kingdom of Saudi Arabia to test and vaccinate against COVID-19.
Methods: This cross-sectional study targeted participants aged 65 years and above. The questionnaire included both sociodemographic variables, and variables related to willingness and hesitancy to vaccinate and test for COVID-19 that were mainly based on existing literature. Bivariate analyses were performed to test for associations. Significance was set at the 0.05 level.
Results: The total sample of respondents was 502. The results show that 52.4% were not aware of a previous infection. Participants aged above 70 years and females were found to be more aware of a previous infection (51.6% and 53.1% respectively) (P < 0.05). Also, 54.7% felt it necessary to test against COVID-19, and among those, 70.8% believed that testing would contain and control the spread. The results also show that 3.2% were not vaccinated to date, compared to 95.41% who had the complete dose as well as the recommended booster dose for elderlies. Age, sex and level of education were significantly associated with vaccine uptake, where participants aged between 65 and 70 years, males and high levels of education were associated with a complete vaccine uptake.
Discussion: The current findings add to the epidemiological evidence and show that the social network theory within the context of health may have played a role in self-awareness of previous infections. Also, social factors should be incorporated in public health interventions and public health campaigns targeting the elderly are still needed especially with the continued discovery of variants of interests.
Keywords: COVID-19, public health, health promotion, prevention, elderly
Introduction
Since the coronavirus disease 2019 (COVID-19) epidemic was announced in March of 2020, there has been over 770,085,713 confirmed cases and 6,956,173 deaths worldwide as of the end of August 2023.1,2 The pandemic spread is mostly due to its high rate of contagion and mutation, resistance to climatic variations, and simple mode of transmission. Several worrisome variants for COVID-19 have been identified, which include Delta and Omicron. As recently as the 9th of August, the EG.5 - a descendant sublineage of Omicron – has been assigned as a variant of interest due to its high ability to spread globally and contribute to a surge in hospitalisations.3
Worldwide, several measures were taken to control the spread and subsequent detrimental consequences of infection as recommended by international guidelines. These included lockdowns, curfews, and travel restrictions. In the Kingdom of Saudi Arabia (KSA), the Ministry of Health (MoH) in cooperation with other governmental agencies, took several measures to contain and control the spread of infection. These included mass lockdowns, suspension of international flights and rapid deployments of testing protocols.4 Furthermore, the MoH always maintained direct communication with its citizens via campaigns that promote personal protective measures, vaccinations and testing through several channels that included text messages, daily news reports and through official social media accounts.5 The Saudi Data and Artificial Intelligence Authority had also launched the Tawakkalna mobile application which was and still is successfully able to support government efforts through the issuance of movement permits during curfew periods as well as showing the users’ health immune status.6
Evidence has shown that the elderly population are considered among the most vulnerable in the face of COVID-19. Although, this has not been yet fully understood on a molecular level, it is clear that age alone is a significant risk factor for death due to the disease.7,8 Also, severity of COVID-19 is significantly associated with the presence of comorbidities, such as cardiovascular diseases, hypertension, diabetes and respiratory disease which are more prevalent in this age group.8 Therefore, since the arrival of vaccines to the KSA on December 2020, the priority was to vaccinate the most vulnerable groups which included patients with comorbidities, immunocompromised patients, all first line responders and naturally those aged 65 years of age and above.9
Despite COVID-19 restrictions, such as proof of vaccinations and mask mandates were lifted in March 2023, the importance of abiding by national and international guidelines is crucial in this age group. Although several studies have been published that explored the attitudes towards COVID-19 vaccinations, none have targeted this specific vulnerable age group. The only study that looked at adults and included 116 adults aged above 60 years, has found that the vaccination acceptance rate was low, and that this was mainly due to concerns regarding its safety and potential side effects.10 Therefore, this study aimed to explore the willingness and hesitancy of the elderly aged 65 years and above regarding the uptake of both the COVID-19 tests and vaccines and explore the reasons of both.
Materials and Methods
Study Design and Participants
This cross-sectional study recruited elderly patients within the Eastern region of the KSA. The eligibility criteria were being aged 65 years or older. Patients who were diagnosed with neurocognitive disorders, such as dementia and Parkinson’s disease were excluded from the study.
Ethical Considerations
The study was approved by the Imam Abdulrahman Bin Faisal University’s Institutional Review Board (IRB-2023-01-302). Participation in this study was voluntary and anonymous. To comply with ethical considerations of the research, consent to participate was obtained from all participants. The study complied with the principles of the Declaration of Helsinki.
Sample Size and Sampling Technique
The minimum required sample size was 378. This was based on a prevalence of 43.85% for the willingness to vaccinate among adults in the KSA.10 The precision of 5% and alpha level of 0.05 were used in the calculation of the sample size. The sample size calculation was performed in Epi info 7.0. Due to the sensitive and delicate nature of our target population, the subjects were enrolled via a non-probability sampling technique from community health centres where visits were usually for physical examinations. People were approached and invited to voluntarily participate in the study by responding to face-to-face interviews between the 1st and 31st of August 2023.
Data Collection Tool and Processes
The questionnaire used in this study was developed based on an extensive review of the literature,11–13 as well as after discussion between the research team. The tool had two main parts, the first was based on sociodemographic variables which included variables on age, sex, level of education (below high school, high school graduate, university or postgraduate), whether the participant was a healthcare professional (yes/no), presence of chronic conditions (yes/no), living circumstances (alone/with family), perceived financial status (poor/good), had been familiar with a person who had been infected with COVID-19 (yes/no) and had been familiar with someone who had died from COVID-19 (yes/no).
The second part of the tool consisted of questions on attitudes of acceptance and hesitancy towards testing against COVID-19 as well as questions on attitudes of acceptance and hesitancy towards the COVID-19 vaccine. Two experts reviewed the questionnaire and approved the final version, the first a geriatric consultant and the second was a preventive medicine consultant to enhance content validity and ensure that all questions were within the Saudi context. A pilot study was performed on 20 elderly participants, and their responses were excluded from the final analysis. After the pilot study, no modifications on the tool were made.
Statistical Analysis
All variables were coded and analysed using the Statistical Package for Social Sciences (SPSS) version 26.0.14 For vaccine uptake, the outcome was categorised into three categories, the first was none for respondents who had no vaccines, partial for those who had only one dose of the vaccine, and complete for respondents with two, three and four vaccines. For descriptive statistics, frequencies and percentages were used for all categorical variables, and means ± standard deviations for continuous variables. Cross tabulations using Chi-squared tests, and where applicable Fisher’s Exact tests were performed to compute the p-value. The level of significance was set at 0.05.
Results
The total number of elderly participants included in this study was 502. The mean age was 70.34 ± 5.85. The range of age of participants was 65 to 95 years. Males and females were similarly distributed.
Sociodemographic and Health Characteristics in Relation to Self-Awareness of a Previous COVID-19 Infection
Table 1 shows the distribution of sociodemographic and health-related characteristics according to self-awareness of a previous COVID-19 infection. Among the total participants, 47.6% were aware of having previously acquired COVID-19. Statistically significant differences were observed with age, sex and level of education where a higher proportion of self-awareness of a previous COVID-19 infection was reported among those aged above 70 years (51.6%), females (53.1%) and high-school graduates (54.3%). Furthermore, elderly participants who were familiar with other people who had been previously infected with the virus or had died from infection with the virus reported significantly higher proportions of self-awareness of personal previous infection (53.0% and 61.9% respectively). Among those who were aware of being infected, the majority had undergone a test confirmation (84.1%) compared to 15.9% who did not.
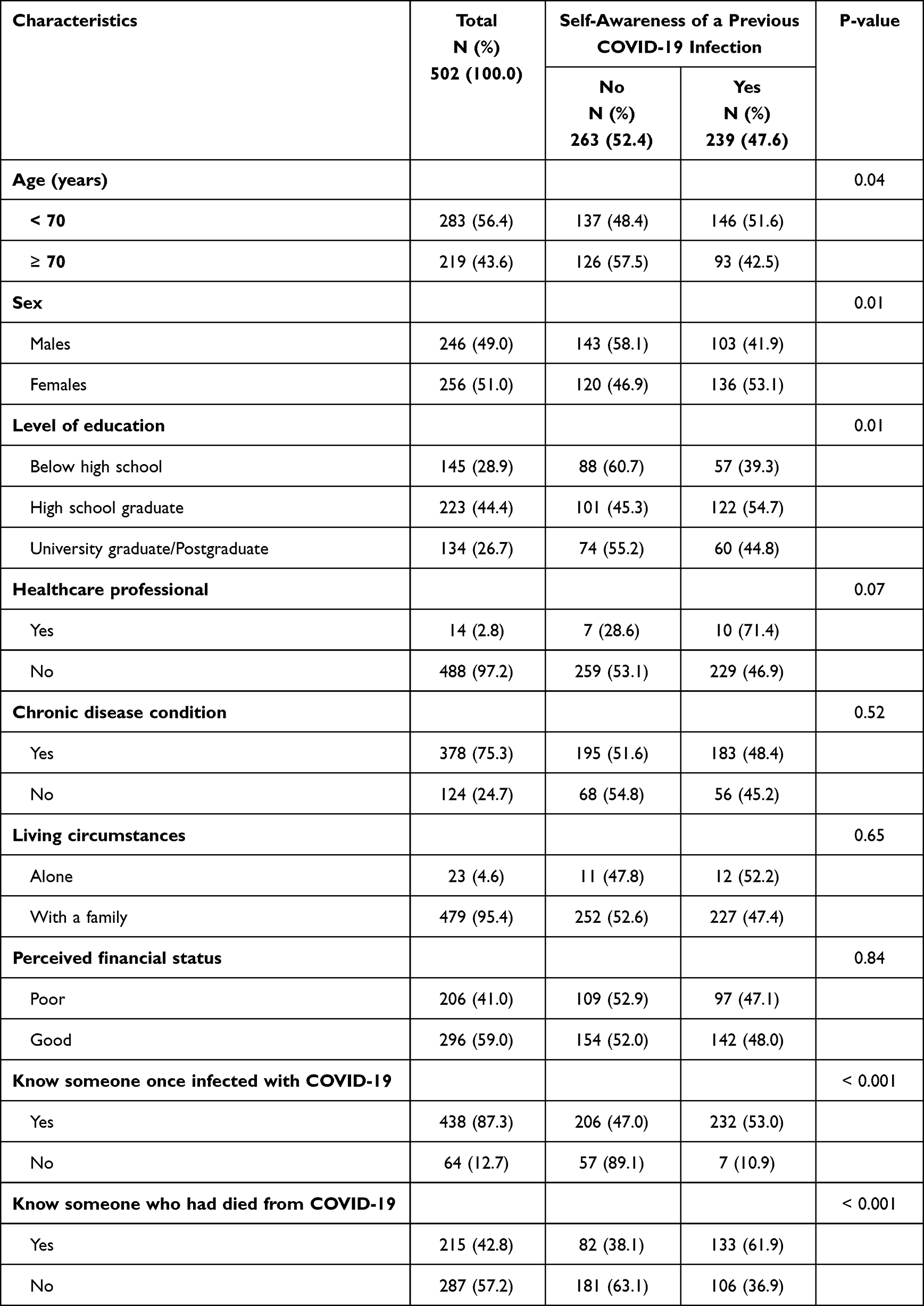 |
Table 1 Sociodemographic and Health Related Characteristics of the Elderly Participants in Relation to Their History of a COVID-19 Infection |
Acceptance and Hesitancy to Undergo a COVID-19 Test Among the Elderly Participants
Figure 1 shows that more than half the participants (54.6%) would get tested for COVID-19 if they knew they had been in contact with a person(s) positive even if no symptoms are present. The highest reported reason for this response was the belief that testing may help to control the spread of the disease and protect others (70.8%). Other reasons included awareness of own responsibility as a citizen (62.8%), the willingness to receive appropriate care in case of a positive result (61.3%) and to oblige to the expectation of family and friends in taking the test (12.8%). The least reported reason for testing was fear of penalties in only 3.3% of the total participants.
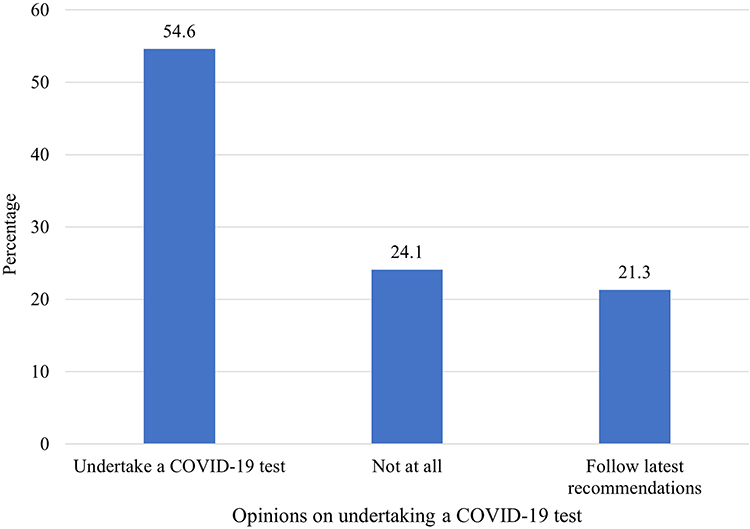 |
Figure 1 Distribution of elderly participants opinions on undertaking a COVID-19 test. |
Among the 24.1% participants not willing to undertake the test despite knowing that they had been in contact with other individuals who had been positive for COVID-19, the most reported reasons were feeling that the test was unnecessary if no symptoms are present (24.1%), believing there is nothing to do even if the result is positive (26.4%) and that the test is time consuming (24.8%) (Table 2).
 |
Table 2 Acceptance and Hesitancy of Elderly Participants to Take a COVID-19 Test |
Acceptance and Hesitancy to Be Vaccinated Against COVID-19 Among the Elderly
Regarding the participants attitude towards the COVID-19 vaccine, the mean attitude score was 31.93 ± 5.51 (Median 32, range = 18–54). Participants who had a negative attitude for the vaccine represented 58.6% of the total samples, whereas 41.4% had a positive attitude towards the vaccine.
Figure 2 shows that only 3.18% of the total participants did not receive the COVID-19 vaccine, whereas 1.39% had received one dose, 14.3% had received two doses, 75.7% had received the completed three doses and 5.4% had the recommended fourth vaccine.
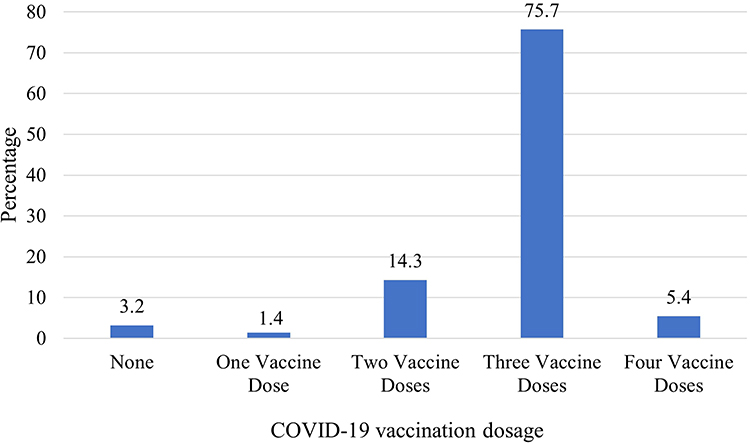 |
Figure 2 Distribution of elderly participants in relation to COVID-19 vaccine uptake. |
Table 3 presents the associations between sociodemographic and health-related characteristics of participants and vaccine uptake. Statistically significant associations were observed for age, sex and educational status only where higher proportions of complete doses of the vaccines were observed for participants aged less than 70 (97.5%), and similarly for males (97.2%) and for high-school graduates (97.3%). No statistically significant differences were observed with other characteristics.
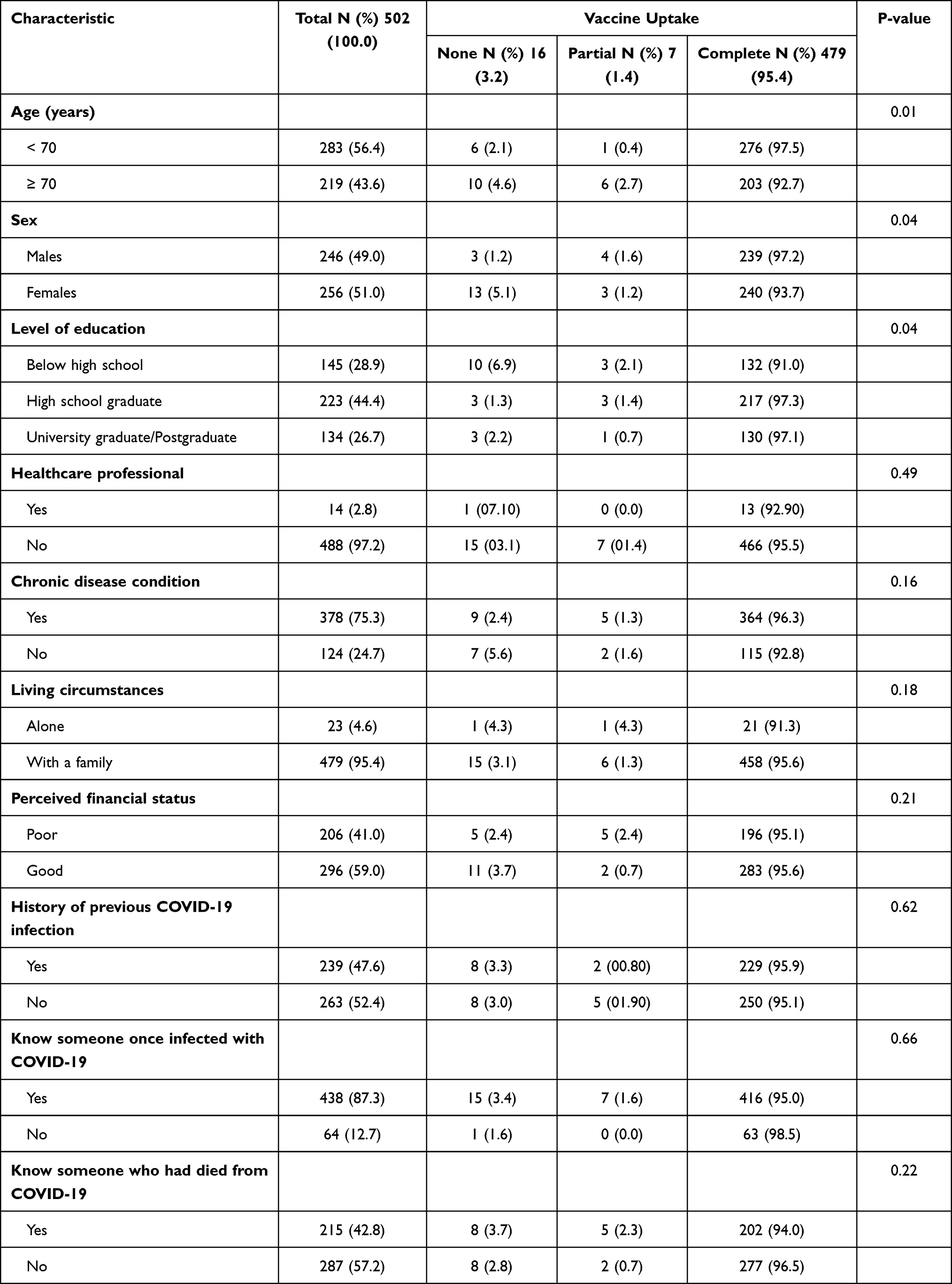 |
Table 3 Sociodemographic and Health Related Characteristics of Elderly Participants in Relation to Vaccine Uptake |
Table 4 presents each question regarding the attitude towards the vaccine on a five-point Likert’s scale. The highest proportion of participants strongly agreed that the vaccine can help control the spread of infection (43.0%), and around one-third strongly disagreed with the statement that had they known they were going to be infected, they would not get the vaccine even if it were available (33.7%). Also, 36.6% strongly disagreed with the statement that if everyone else is vaccinated against COVID-19, they would have to be vaccinated themselves. The results also show that the highest proportion of participants strongly agreed that their decision to take the vaccine depends mainly upon recommendations from the MoH (43.8%), that the high vaccination uptake would lift the restrictions on movement (41.0%), and to allow clearance of immune status on the Tawakkalna application (37.7%).
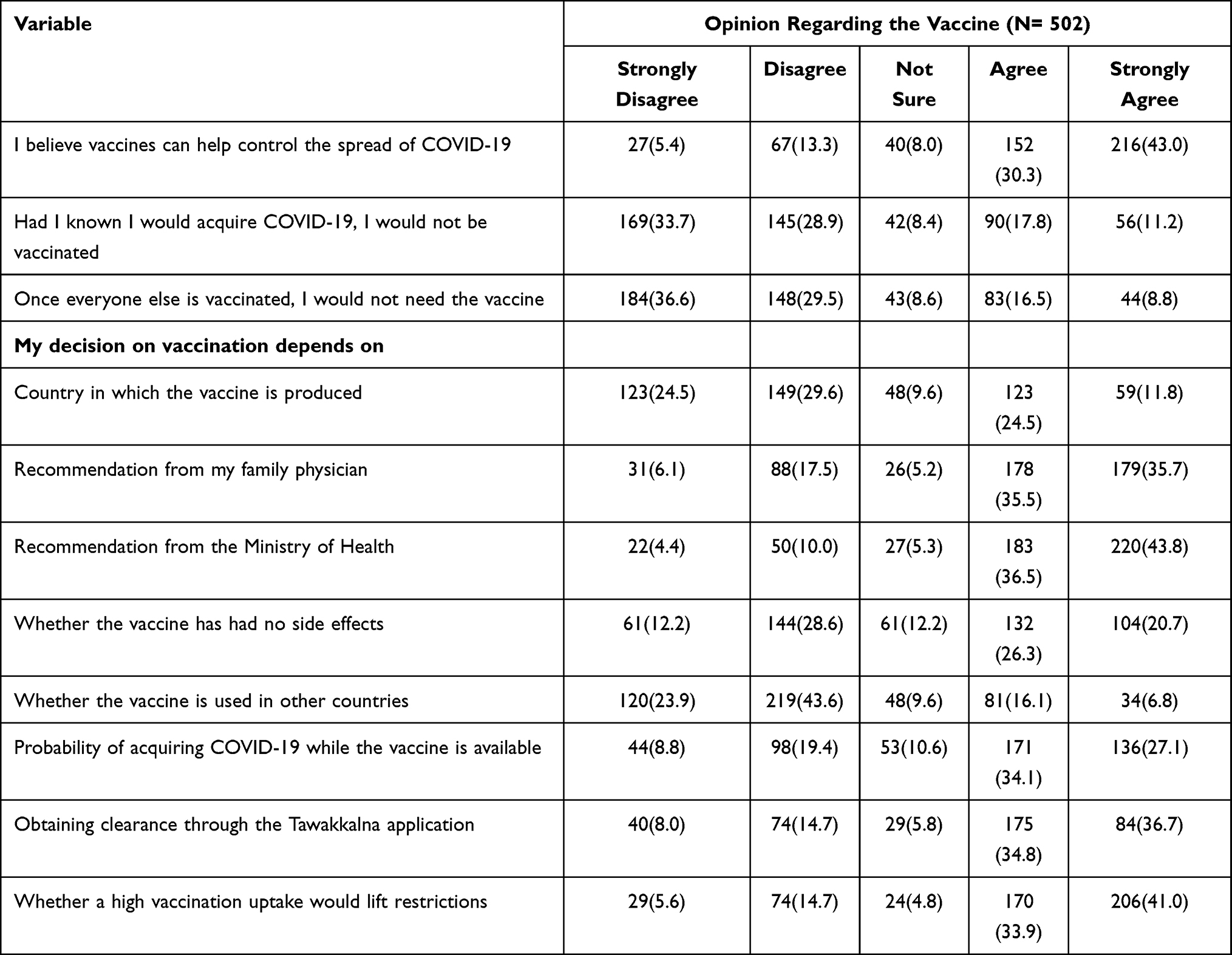 |
Table 4 Attitudes of Elderly Participants Regarding the Uptake of the COVID-19 Vaccine |
Discussion
During the COVID-19 pandemic era, implementing preventive measures including testing and vaccination to control the spread of the highly contagious virus requires the population’s willingness to adopt this behaviour.15 This study was able to assess the willingness and hesitancy of the elderly population in the KSA towards COVID-19 testing and vaccinations. Although few studies have had similar objectives, none have targeted this vulnerable age group. Several important findings have emerged from the current analyses which give rise to policy recommendations during the next phase of planning towards the prevention of infection in this age group.
Associations with Self-Awareness of a Previous COVID-19 Infection
Over half the participants were not aware of a previous COVID-19 infection, this finding is consistent with other research demonstrating that a significant proportion of COVID-19 infections are asymptomatic or minimally symptomatic and thus may go unnoticed.16 These asymptomatic infections can still result in long-term health effects and contribute to the spread of the virus, and their share could be as high as 20% and possibly more among older adults.17,18
Furthermore, we found a statistically significant correlation between self-awareness of a previous COVID-19 infection and various sociodemographic characteristics. For instance, participants aged below 70 years reported a higher percentage of self-awareness compared to those aged 70 and older. Similarly, one hundred and thirty-six women reported being aware of their COVID-19 infection than men. Interestingly, the level of education also appeared to be a factor, with high-school graduates showing a higher percentage of self-awareness. This aligns with previous research suggesting that age, sex, and educational level can influence the perception and awareness of health-related issues, including infectious diseases.19,20 The findings emphasize the importance of targeted public health strategies to increase awareness and understanding of COVID-19 across all demographic groups, particularly those who may be less likely to recognize or report infection.21
Personal experiences and connections can significantly shape an individual’s perception and awareness of a disease. In our study, we observed associations between the self-awareness of a previous COVID-19 infection and having prior knowledge of someone who had suffered from the disease or knowing someone who had died from it. This finding aligns with existing literature where for example, a study found that direct or indirect exposure to a disease could enhance the perceived severity and susceptibility, thereby influencing individuals’ health behaviours and responses.22,23 With respect to the older population, this finding is particularly relevant. Older adults are at a higher risk of severe outcomes from COVID-19; thus, their awareness and understanding of the disease could have significant implications for their health outcomes.24 Additionally, these findings echo the social network theory in health contexts, which posits that individuals’ health behaviours and attitudes are influenced by their social connections.25 In this case, the social connection manifests as knowing someone infected or has died from COVID-19, which increases the individual’s self-awareness of their infection. This concept may explain that, among those aware of being infected, the majority had undergone a COVID-19 test confirmation (84.1%). These findings underscore the importance of social factors in disease awareness and highlights the need for targeted public health interventions that consider these factors.
Acceptance and Hesitancy to Undergo a COVID-19 Test Among the Elderly Participants
Our study’s findings shed light on the attitudes of elderlies towards COVID-19 testing. Notably, none of the participants expressed fear of fines or penalties for violating any official COVID-19 related restrictions should they choose not to get tested. This may suggest a high level of compliance with public health measures among this group, consistent with prior research indicating that older adults are generally more likely to adhere to public health guidelines.26 Interestingly, a significant proportion of our sample perceived COVID-19 testing as unnecessary in the absence of symptoms. This belief is contrary to the widespread consensus in the medical community, which emphasizes that asymptomatic individuals can still transmit the virus.27 Lastly, the fear of being stigmatized or blamed by others if they tested positive also emerged as a contributing factor for test hesitancy. This finding aligns with previous studies that have highlighted stigma as a barrier to disease testing and disclosure in several contexts, including HIV and COVID-19.28,29 These insights underscore the need for targeted communication strategies to address misinformation and stigma associated with COVID-19 testing, particularly among older adults.
Acceptance and Hesitancy to Be Vaccinated Against COVID-19 Among the Elderly
With regard to vaccinations, age sex and educational level were significantly related to vaccine uptake. We found that full vaccine uptake was less among those aged above 70 years old compared to those aged between 65 and 70. The literature in this matter differs between geographical areas. For example, similar results to ours were present in China, however in Australia older adults tended to vaccinate in comparison to their younger counterparts.30,31 It is likely that cultural and social factors have played a role in these differences. Furthermore, we found that vaccinations were less among females in comparison to males. In a systematic review of over sixty studies to identify gender differences in the intention to vaccinate, they found that males had a higher intention to vaccinate against COVID-19.32 Since females play a central role in ensuring the health of their families and children, this difference between sexes should be an additional point of focus in future health campaigns. As for educational level, our results are consistent with those elsewhere in which we found that a lower educational level of was associated with a lower uptake of vaccinations.33 In fact, 10 of the 16 elderlies in our study had a lower education level.
Reluctance to receive the COVID-19 vaccine either due to conspiracy beliefs or a lack of awareness are major obstacles facing health authorities. Confidence in vaccines is considered by the World Health Organisation as one of the significant factors that affect people’s opinion towards taking the vaccine.34 Similar to our results, studies exploring the attitudes and beliefs of the elderlies towards COVID-19 have found that beliefs in vaccine efficacy were the main factor driving peoples’ intention towards receiving those vaccines.35 Our findings, in line with international studies, reflect a good level of confidence among Saudi participants in vaccine efficacy. Consequently, more than half of the study participants disagreed and strongly disagreed with the fact that their intention to take the vaccine will be reduced by knowing their previous infection status or the number of people receiving the vaccine. In contrast, a study conducted among Saudi young adults found that most of the participants were willing to take the vaccine only if it was taken by many people or if it was made mandatory.36 However that study only targeted young adults who were not considered at a high risk of COVID-19 complications compared to the elderly which might make them feel less motivated to take the vaccine. Moreover, it was published during the early pandemic when the vaccine was just released to the public, which could justify the reluctance towards taking the novel vaccine. Furthermore, the high willingness in this study could also be explained by the availability of free vaccines to all Saudi residents provided by the government, which eliminates the cost barrier.
Additionally, almost two-thirds of the study participants agreed and strongly agreed that their decision to take the vaccine depends mainly on recommendations from their family physician and the MoH. Similarly, 66.2% of the elderly population in the US stated that their decision to take the vaccine is based on health care providers’ recommendations.37 This indicates confidence and trust in healthcare providers and public health campaigns.
Most of our respondents did not consider the country of vaccine production or whether the vaccine has been used in other countries as factors that would impact their decision towards vaccine uptake. In contrast to previous studies in the US and Jordan which found that people trust the safety of vaccines produced in the US and Europe.2,37 Given the fact that the MoH launched the vaccination campaign through means accessible to all citizens, such as the use of the Sehhaty mobile application which facilitates registration to all vaccination centres around the country, is reassuring for the public. Thus, it was reported in a previous study that confidence in the decisions of the government was the strongest factor influencing participants positively toward vaccination.
Furthermore, most participants agreed and strongly agreed to the fact that the convenience of utilising public services and lifting gathering restrictions are positively influencing factors towards vaccine uptake. It is well known that the pandemic and the applied precautionary measures have negatively affected people’s lives, and their careers, and consequently impacted their physical health and mental well-being.38 Therefore, it is not surprising that the perceived benefits of vaccination, including less anxiety, less likelihood of getting infected with COVID-19, and easing of the preventative efforts were encouraging factors.
Limitations of the Study
Although this study is the first to analytically explore the willingness and hesitancy of the elderly population in the KSA, there are a few limitations that may limit generalisations. The sampling technique employed was a non-probability sampling technique which inherently limits generalisation efforts to the general elderly population. However, this technique was chosen due to the nature of our target population. The elderly is a sensitive group of people who would not normally tolerate questioning, especially with regard to their own attitudes and opinions. Also, the tool consists of questions on attitudes and opinions, which are entirely subjective.
Conclusion
This study explored the willingness and hesitancy of the elderly in the KSA towards COVID-19 testing and vaccination and has been able to add to the epidemiological literature on this matter. We found that over half the participants were not aware of a previous COVID-19 infection, and that this self-awareness of a previous infection was related to age, sex, level of education, and being familiar with someone who had been previously infected with COVID-19 and someone who had died due to this infection. Additionally, we were able to conclude that there is a high degree of compliance with regulations on COVID-19 testing. Also, willingness to vaccinate against COVID-19 were significantly associated with age, sex and level of education.
Abbreviations
COVID-19, coronavirus disease 2019; KSA, Kingdom of Saudi Arabia; MoH, Ministry of Health; SPSS, Statistical Package for Social Sciences.
Data Sharing Statement
The dataset used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Imam Abdulrahman Bin Faisal University’s institution review board (IRB-2023-01-302). All respondents were informed about the purpose of the study, and all participants consented voluntarily. Informed consent was obtained from all study participants.
Author Contributions
All authors have made a significant contribution to the work reported here, whether it be in the conceptualisation, design of the study, acquisition of the data, analyses and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO COVID-19 Dashboard. World Health Organization; 2023.
2. Elhadi M, Alsoufi A, Alhadi A, et al. Knowledge, attitude, and acceptance of healthcare workers and the public regarding the COVID-19 vaccine: a cross-sectional study. BMC Public Health. 2021;21(1):955. doi:10.1186/s12889-021-10987-3
3. World Health Organization. EG.5 Initial Risk Evaluation, 9 August 2023. World Health Organization; 2023.
4. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. 2020;13(6):834–838. doi:10.1016/j.jiph.2020.04.016
5. Alhassan FM, AlDossary SA. The Saudi ministry of health’s twitter communication strategies and public engagement during the COVID-19 pandemic: Content Analysis Study. Original Paper. JMIR Public Health Surveill. 2021;7(7):e27942. doi:10.2196/27942
6. SDAIA. About tawakkalna. Saudi data and artificial intelligence authority; 2023. Available from: https://ta.sdaia.gov.sa/en/index.
7. Collaborative O, Williamson E, Walker AJ, et al. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. MedRxiv. 2020;2020:1.
8. Amber ML, Maeva MS, David SA. Why does COVID-19 disproportionately affect older people? Aging. 2020;12(10):9959.
9. Assiri A, Al-Tawfiq JA, Alkhalifa M, et al. Launching COVID-19 vaccination in Saudi Arabia: lessons learned, and the way forward. Travel Med Infectious Dis. 2021;43:102119. doi:10.1016/j.tmaid.2021.102119
10. Al-Hanawi MK, Alshareef N, El-Sokkary RH. Willingness to receive COVID-19 vaccination among older adults in Saudi Arabia: a community-based survey. Vaccines. 2021;9(11):1257. doi:10.3390/vaccines9111257
11. Alkhaldi G, Aljuraiban GS, Alhurishi S, et al. Perceptions towards COVID-19 and adoption of preventive measures among the public in Saudi Arabia: a cross sectional study. BMC Public Health. 2021;21(1):1251. doi:10.1186/s12889-021-11223-8
12. World Health Organization. Report of the SAGE working group on vaccine hesitancy; 2014. Available from: https://cdn.who.int/media/docs/default-source/immunization/sage/2014/october/sage-working-group-revised-report-vaccine-hesitancy.pdf?sfvrsn=240a7c1c_4.
13. El-Elimat T, AbuAlSamen MM, Almomani BA, Al-Sawalha NA, Alali FQ, Di Gennaro F. Acceptance and attitudes toward COVID-19 vaccines: a cross-sectional study from Jordan. PLoS One. 2021;16(4):e0250555. doi:10.1371/journal.pone.0250555
14. IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. IBM Corp; 2019.
15. Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis. 2020;26(7):1470. doi:10.3201/eid2607.200282
16. Zhang X, Lin D, Pforsich H, Lin VW. Physician workforce in the United States of America: forecasting nationwide shortages. Hum Resour Health. 2020;18(1):1–9. doi:10.1186/s12960-020-0448-3
17. Buitrago-Garcia D, Egli-Gany D, Counotte MJ, et al. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis. PLOS Medicine. 2020;17(9):e1003346. doi:10.1371/journal.pmed.1003346
18. Rivett L, Sridhar S, Sparkes D, et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife. 2020;9:e58728. doi:10.7554/eLife.58728
19. Al-Matary A, Almatari F, Al-Matary M, et al. Clinical outcomes of maternal and neonate with COVID-19 infection - multicenter study in Saudi Arabia. J Infect Public Health. 2021;14(6):702–708. doi:10.1016/j.jiph.2021.03.013
20. So WK, Chan SS, Lee AC, Tiwari AF. The knowledge level and precautionary measures taken by older adults during the SARS outbreak in Hong Kong. Int J Nurs Stud. 2004;41(8):901–909. doi:10.1016/j.ijnurstu.2004.04.004
21. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a Cross-Sectional Study. Front Public Health. 2020;8:217. doi:10.3389/fpubh.2020.00217
22. Rubin GJ, Smith LE, Melendez-Torres G, Yardley L. Improving adherence to ‘test, trace and isolate’. J R Soc Med. 2020;113(9):335–338. doi:10.1177/0141076820956824
23. Brewer NT, Chapman GB, Rothman AJ, Leask J, Kempe A. Increasing vaccination: putting psychological science into action. Psychol Sci. 2017;18(3):149–207. doi:10.1177/1529100618760521
24. Lloyd-Sherlock P, Ebrahim S, Geffen L, McKee M. Bearing the brunt of covid-19: older people in low and middle income countries. BMJ. 2020;368:m1052. doi:10.1136/bmj.m1052
25. Centola D. An experimental study of homophily in the adoption of health behavior. Science. 2011;334(6060):1269–12725. doi:10.1126/science.1207055
26. Seale H, Heywood AE, Leask J, et al. COVID-19 is rapidly changing: examining public perceptions and behaviors in response to this evolving pandemic. PLoS One. 2020;15(6):e0235112. doi:10.1371/journal.pone.0235112
27. Oran DP, Topol EJ. The proportion of SARS-CoV-2 infections that are asymptomatic: a systematic review. Ann Intern Med. 2021;174(5):655–662. doi:10.7326/m20-6976
28. Logie CH, Turan JM. How do we balance tensions between COVID-19 public health responses and stigma mitigation? Learning from HIV research. AIDS Behav. 2020;24(7):2003–2006. doi:10.1007/s10461-020-02856-8
29. Earnshaw VA, Eaton LA, Kalichman SC, Brousseau NM, Hill EC, Fox AB. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl Behav Med. 2020;10(4):850–856. doi:10.1093/tbm/ibaa090
30. You Y, Li X, Chen B, Zou X, Liu G, Han X. Knowledge, attitude, and practice towards influenza vaccination among older adults in Southern China during the COVID-19 pandemic. Vaccines. 2023;11(7):1197. doi:10.3390/vaccines11071197
31. Bullivant B, Bolsewicz KT, King C, Steffens MS. COVID-19 vaccination acceptance among older adults: a qualitative study in New South Wales, Australia. Public Health Pract. 2023;5:100349. doi:10.1016/j.puhip.2022.100349
32. Zintel S, Flock C, Arbogast AL, Forster A, von Wagner C, Sieverding M. Gender differences in the intention to get vaccinated against COVID-19: a systematic review and meta-analysis. Zeitschrift für Gesundheitswissenschaften. 2022;1–25. doi:10.1007/s10389-021-01677-w
33. Guay M, Maquiling A, Chen R, et al. Measuring inequalities in COVID-19 vaccination uptake and intent: results from the Canadian Community Health Survey 2021. BMC Public Health. 2022;22(1):1708. doi:10.1186/s12889-022-14090-z
34. Babatope T, Ilyenkova V, Marais D. COVID-19 vaccine hesitancy: a systematic review of barriers to the uptake of COVID-19 vaccine among adults in Nigeria. Bull Natl Res Cent. 2023;47(1):45. doi:10.1186/s42269-023-01017-w
35. Malesza M, Wittmann E. Acceptance and intake of COVID-19 vaccines among older Germans. J Clin Med. 2021;10(7):1388. doi:10.3390/jcm10071388
36. Almaghaslah D, Alsayari A, Kandasamy G, Vasudevan R. COVID-19 vaccine hesitancy among young adults in Saudi Arabia: a Cross-Sectional Web-Based Study. Vaccines. 2021;9(4):330. doi:10.3390/vaccines9040330
37. Malik AA, McFadden SM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495. doi:10.1016/j.eclinm.2020.100495
38. Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;102:152192. doi:10.1016/j.comppsych.2020.152192
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of the COVID-19 Lockdown on Physical Therapy Undergraduates and Their Families. A Qualitative Study from the United Arab Emirates
Alanazi FS, Mysore SB, Farghaly AA
International Journal of General Medicine 2022, 15:6373-6380
Published Date: 1 August 2022
Building the Culture of Public Health as a Positive Reflection from the COVID-19 Crisis
Alsaqqa HH
Risk Management and Healthcare Policy 2022, 15:1683-1693
Published Date: 6 September 2022
Health Risks During Ukrainian Humanitarian Crisis
Cojocaru E, Cojocaru C, Cojocaru E, Oancea CI
Risk Management and Healthcare Policy 2022, 15:1775-1781
Published Date: 22 September 2022
Initial Psychometric Development of the Fear and Anxiety to COVID-19 Scale in Nursing Professionals: An Occupational Health Assessment Tool
Morgado-Toscano C, Allande-Cussó R, Fagundo-Rivera J, García-Iglesias JJ, Climent-Rodríguez JA, Navarro-Abal Y, Gómez-Salgado J
Risk Management and Healthcare Policy 2022, 15:1947-1957
Published Date: 14 October 2022
Enhancing Literature Review and Understanding Under Global Pandemic
Qiao G, Song H, Hou S, Xu J
Risk Management and Healthcare Policy 2023, 16:143-158
Published Date: 3 February 2023