Back to Journals » Lung Cancer: Targets and Therapy » Volume 16
A Concise Review of the Approved MET TKIs (Savolitinib, Gumarontinib, Vebreltinib, Tepotinib, Capmatinib) in China for MET Exon 14 Splice Site Mutated (METex14+) NSCLC Circa 2025
Received 14 June 2025
Accepted for publication 26 August 2025
Published 31 October 2025 Volume 2025:16 Pages 147—159
DOI https://doi.org/10.2147/LCTT.S547090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fengying Wu
Yanyan Hu,1 Sai-Hong Ignatius Ou2,3
1Department of Oncology, The Fifth Medical Center of Chinese PLA General Hospital, Beijing, 100039, People’s Republic of China; 2University of California Irvine School of Medicine, Orange, CA, 92868, USA; 3Chao Family Comprehensive Cancer Center, Orange, CA, 92868, USA
Correspondence: Sai-Hong Ignatius Ou, Email [email protected]
Abstract: Splice site mutations around or within exon 14 of MET (METex14+) are rare, but are one of the common actionable driver mutations in elderly patients with non-small cell lung cancer (NSCLC). Globally, only two MET tyrosine kinase inhibitors (TKIs), both Type Ib (capmatinib and tepotinib), have been approved in a single Phase 2 trial. In China, three additional Type Ib MET TKIs (savolitinib, gumarontinib, and vebreltinib), in addition to capmatinib, and tepotinib, have been approved. Here, we report the timeline for MET TKIs approval in China. We summarized the Chinese METex14+ NSCLC demographic and molecular characteristics and reviewed pivotal phase 2 data (clinical efficacy and adverse events). All five MET TKIs seem to have similar efficacy and adverse events with vebreltinib reported numerically the highest BIRC-ORR. Notably, the gumarontinib (GLORY) trial conducted in both China and Japan also led to the approval of gumarontinib in Japan for METex14+ NSCLC. On June 30, 2025, vebreltinib has been approved for NSCLC with MET amplification while combination of savoltinib and osimertinib has been approved for EGFR+ post EGFR TKINSCLC with MET amplification post EGFR TKI based on the SACHI trial (NCT05015608). We discuss the current unmet clinical need (need to develop Type II MET TKI to overcome acquired resistance MET mutations at D1228 and Y1230) and future optimal treatment approaches.
Keywords: Type Ib MET TKI, Type II MET TKI, MET exon 14 mutation, savolitinib, gumarontinib, vebreltinib, tepotinib, capmatinib, amivantamab
Introduction
Establishment of MET Exon 14 Splice Site Mutations (Metex14+) as an Actionable Driver Mutation in Non-Small Cell Lung Cancer (NSCLC)
The receptor tyrosine kinase (RTK) Mesenchymal Epithelial Transition (MET) is one of the 58 human RTKs.1 Splice site mutations (donor, acceptor) around exon 14 of MET (METex14+) are rare but are validated as actionable driver mutations in non-small cell lung cancer (NSCLC) with approved targeted therapy. METex14+ mutations are heterogeneous (base institutions, insertions, deletions); however, the phenotype of these diverse METex14+ mutations is the non-incorporation of exon 14 into mature MET messenger RNA.2,3 MET exon 14 encodes the juxtamembrane domain and contains a CBL E3-ubiquitin ligase-binding site, allowing the attachment of ubiquitin and designating MET for degradation.4 It took decades for the discovery of MET exon 14 splice site mutations to realize the underlying phenotype that underpins the pathogenesis to the first report of multi-targeted kinase inhibitors, crizotinib and cabozantinib, demonstrating a response in METex14+ NSCLC patients and proof of principle of METex14+ mutations.5 A case series by Drs. Paul Paik and Alex Drilon of four patients who responded to MET tyrosine kinase inhibitors (TKIs) jump-started the rapid development of MET TKIs against METex14+ NSCLC.5
MET TKIs
MET can be classified into several types. Type I inhibitors are direct competitive inhibitors that bind to the kinase domains of inactive MET proteins. Type I inhibitors are further divided into Type Ia, a multi-targeted MET TKI, of which crizotinib is the only member, and Type Ib, a more selective MET TKI. Type II inhibitors are competitive inhibitors that bind to both the kinase domain and surrounding domains of inactive MET proteins. Type III inhibitors are competitive allosteric inhibitors that bind to domains outside of the kinase domain. Most clinically active MET TKIs are Type Ib or Type II inhibitors (i.e. cabozantinib).6 It is important to distinguish between Type I and II inhibitors as Type II inhibitors can overcome the most common on-target resistance mutations at amino acid residues 1228 and 1230 to Type I inhibitors.7,8
Two type Ib MET TKIs, capmatinib (卡马替尼) and tepotinib (特泊替尼), have been approved globally based on efficacy from two globally conducted phase 2 trial.9,10 Capmatinib received accelerated approval in the US on May 6, 2021, based on the GEOMETRY mono-1 trial, while tepotinib received accelerated US approval on February 3, 2021, based on the VISION trial results and full approval on February 15, 2024, with a longer follow-up of VISION.11 Although the updated data of GEOMETRY mono-1 have been published,12 capmatinib is still under accelerated approval in the US. To date, no other compounds are being developed in the US to target METex14+ NSCLC. Current no randomized trials comparing MET TKI versus chemotherapy with or without immunotherapy in the first-line setting in locally advanced and metastatic METex14+ NSCLC. Recently, a real world retrospective case-control comparison study indicated MET TKI may be more effective than immunotherapy +/- chemotherapy in METex14+ NSCLC with PD-L1 ≤ 50%, while immunotherapy +/- chemotherapy is more effective than MET TKI in METex14+ NSCLC with PD-L1 ≥ 80%.13
Crizotinib, a multi-targeted ALK/ROS1/MET TKI, was the first MET TKI to prospectively demonstrate METex14+ NSCLC is actionable, with a reported overall response rate (ORR) of 32% (95% confidence interval [CI]: 21–45), median duration of response (DOR) of 9.1 months (95% CI: 6.4–12.7), and a median progression-free survival (PFS) of 7.3 months (95% CI: among 65 evaluable METex14+ NSCLC patients.14 METex14+ NSCLC patients are the third molecular subset of NSCLC from the initial Phase 1 crizotinib trial, which led to the approval of crizotinib for ALK+ NSCLC15 and ROS1+ NSCLC.16 Despite the large number of METex14+ NSCLC patients enrolled, the relatively lower ORR, the lack of development of a companion diagnostic test (CDx) for METex14 mutation by the sponsor of crizotinib,and two contemporaneous phase 2 trials (capmatinib and tepotinib) in METex14+ NSCLC resulted in crizotinib not seeking regulatory approval in the US.
Capmatinib and tepotinib have been approved in China based on global GEOMETRY mono-019 and VISION10,11,17 trials, respectively. Three additional Type I MET TKIs (savolitinib赛沃替尼, gumarontinib谷美替尼, vebreltinib伯瑞替尼) have been approved in China all based on phase 2 studies with savolitinib being the first MET TKI approved for previously treated patients in 2021 (Figure 1).17–21 It is important for oncologists to be familiar with all approved MET, as patients are mobile and travel between countries. Here, we summarize the pivotal study data underpinning all approved indications in China in Table 1 and Figure 1. In addition, with many more patient characteristics, clinical efficacy, and safety data from six different MET TKI trials, we gained further insight into the clinical and genomic characteristics of METex14+ NSCLC, especially in Chinese patients, and the class effects of MET inhibition with Type I MET TKIs.
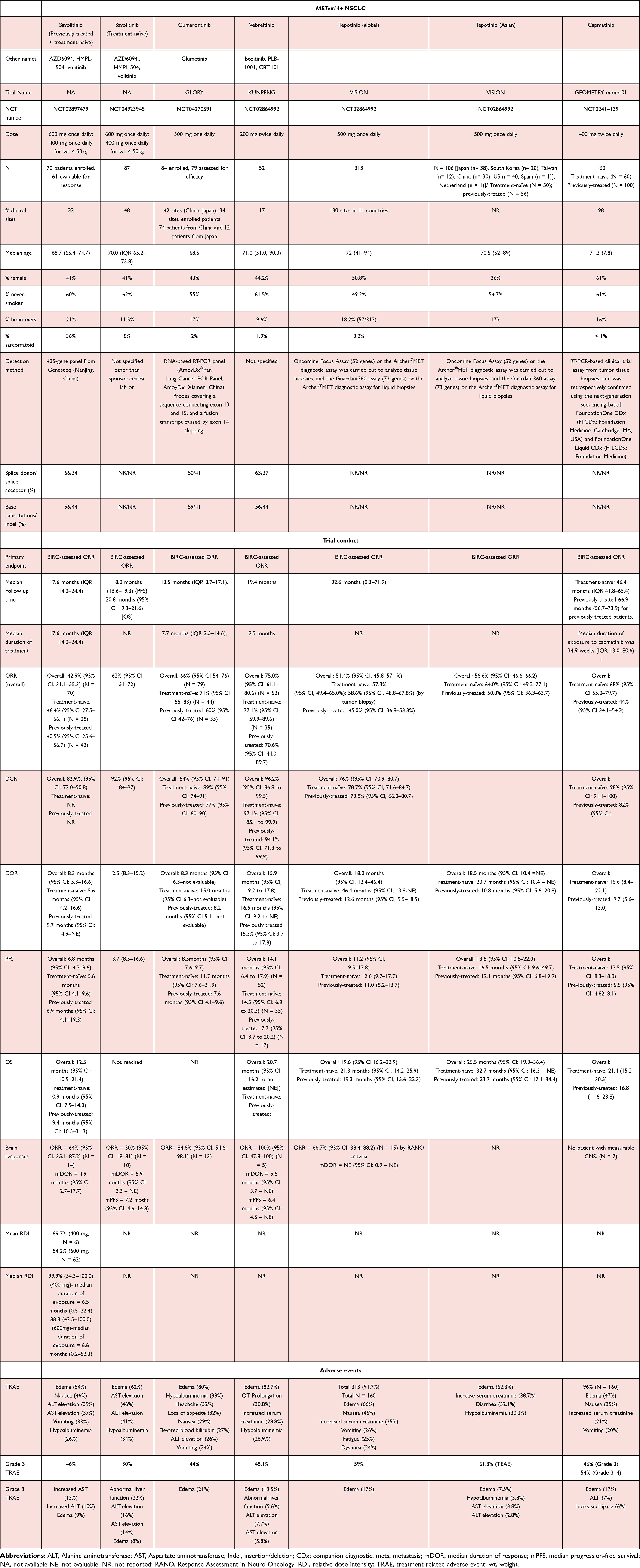 |
Table 1 List of Approved MET TKIs in China with Indications for Treatment of MET Exon 14 Splicing Mutation Positive NSCLC |
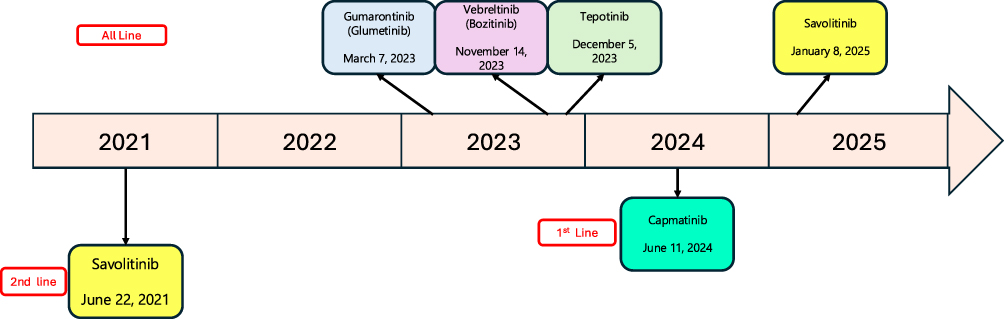 |
Figure 1 Timeline of approval of MET TKIs in China with the line of therapy indications. |
Characteristics of Chinese METex14+ NSCLC Patients
Chinese METex14+ NSCLC are diagnosed at a relatively old age, with a median age of 70 years, which is similar to the global METex14+ NSCLC patient population.3,9,10 As such, the tolerability of the treatment will be as paramount as the efficacy for this group of elderly patients will have to be equally considered. Most Chinese METex14+ NSCLC patients are never-smokers, indicating that screening for METex14 mutations is still paramount among elderly Chinese never-smokers. Overall, the percentage of patients with brain metastasis is generally less than 20%, which is slightly below the percentage of patients with actionable driver mutations with a predilection for the central nervous system.22 Furthermore, in clinical trials that broke out the percentage of the categories of METex14 alterations, splice donor site mutations were more common than splice acceptor site mutations, and base substitutions were more common than insertions/deletions (Table 1).
During the earlier days of characterization of METex14+ NSCLC, it was reported that METex14 is enriched may be enriched sarcomatoid histology.23,24 Hence, in the first trial of savolitinib, sarcomatoid histology was used to enrich for METex14 mutations and constituted approximately 36% of METex14+ NSCLC patients.17 Subsequent patient clinicopathologic characteristics indicated the vast majority of METe14+ NSCLC patients had adenocarcinoma histlogy becauseadenocarcinoma is much more common than sarcomatoid histology in NSCLC.
Summary of Clinical Data for MET TKIs
The primary endpoint of all the trials’ overall response rate (ORR) by blinded independent central review (BICR)-assessed ORR and other important clinical efficacies (duration of response and median progression-free survival) of both treatment-naïve and previously treated patients are summarized in Table 1 and graphically depicted in Figure 2A–C (treatment-naïve) and D–F (previously treated), respectively. The VISION trial also analyzed the efficacy of the Asian subgroup separately25 while the global capmatinib trial (GEOMETRY mono-1) did not.
Figure 2 Continued. Figure 2 (A) Bar-chart plot of blinded independent review committee assessed overall response rate (ORR) achieved by the 5 MET TKIs among treatment-naïve METex14+ NSCLC patients. (B) Bar-chart plot of median duration of response (mDOR) achieved by the 5 MET TKIs among treatment-naïve METex14+ NSCLC patients. (C) Bar-chart plot of median progression-free survival (mPFS) achieved by the 5 MET TKIs among treatment-naïve METex14+ NSCLC patients. (D) Bar-chart plot of blinded independent review committee assessed overall response rate (ORR) achieved by the 5 MET TKIs among previously treated METex14+ NSCLC patients. (E) Bar-chart plot of median duration of response (mDOR) achieved by the 5 MET TKIs among previously treated METex14+ NSCLC patients. (F) Bar-chart plot of median progression-free survival (mPFS) achieved by the 5 MET TKIs among previously treated METex14+ NSCLC patients.
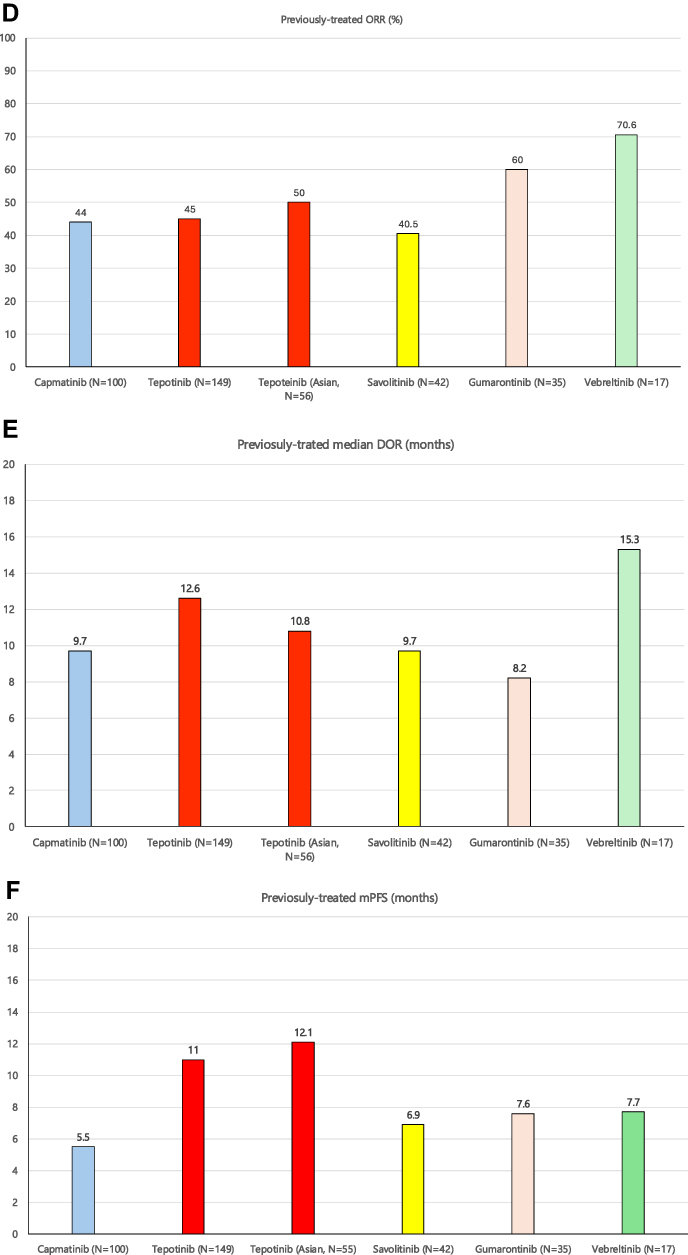
Overall, the efficacy results were comparable among the five approved MET TKIs, with vebreltinib reporting the highest numerically blinded independent central review (BICR)-assessed ORR (both treatment-naïve and previously treated patients with NSCLC). However, with different patient compositions, very small numbers of patients, and different follow-up durations, cross-trial comparisons are fraught with errors. It is important to have follow-up reports with longer follow-up periods. Suffice to say with a limited number of patients analyzed, the ORR among patients with splice donor or acceptor sites were similar, as was the comparison between base substitutions and indels.17,18,20,21 Additionally, there was no difference in the efficacy of savolitinib between patients with sarcomatoid and adenocarcinoma histologies.18 Intracranial-ORR was reported for all compounds, except capmatinib, for which no patient had measurable brain metastases. Again, with a very limited number of patients, savolitinib, gumarontinib, vebreltinib, and tepotinib all reported robust intra-cranial responses.11,17–20
In terms of adverse events, peripheral edema is a significant adverse event and a class effect of Type I MET TKIs and is the most common treatment-related adverse event (TRAE) and grade 3 TRAEs (Table 1). Elevated liver enzyme levels are also common among the five MET used in the treatment of Chinese METex14+ NSCLC. Vebreltinib reported a mean relative dose intensity (RDI) of 98.6%21 while savolitinib reported a mean RDI of 84.2% for 600 mg of savolitinib17 (Table 1). It is important for sponsors of these MET TKI trials to report the mean RDI so that readers can have a more granular understanding of dosage adjustments for this class of treatment among elderly patients with a high incidence of peripheral edema.
Importantly, a phase 2 trial of gumarontinib was conducted in both China and Japan, and 12 Japanese patients were enrolled from four clinical sites, which was approved by the Japan Pharmaceuticals and Medical Devices Agency (PMDA) approval of the use of gumarontinib in METex14+ NSCLC patients.26 Furthermore, on June 30, 2025 vebreltinib has been approved in China for locally advanced and metastatic NSCLC with de novo MET amplification.27 Additionally on the same day, June 30, 2025, savolitinib in combination with osimertinib has been approved as second-line treamtment of EGFR+ NSCLC post EGFR TKI with MET amplification based on the randomzied phase 3 SACHI trial.28
Unmet Need with Current Approved MET TKIs
On-Target Resistance Mutations (D1228N/H/Y/E and Y1230C/H/N/S) (Class Effect) to Current Approved Type I MET TKIs
Acquired D1228 and Y1230 are two of the most common acquired resistance mutations that confer resistance to Type I MET TKIs.29,30 Once these mutations develop, they render all currently approved Type Ib MET TKIs ineffective. Type II multi-targeted MET TKIs, especially cabozantinib, have demonstrated both pre-clinical7,31 and clinical activity29 against acquired MET resistance mutations and CNS activity against METex14+ NSCLC.32 An ongoing trial in Japan is investigating the efficacy of carbozantinib against these two principal acquired MET mutations.33 Meanwhile, without a formally approved indication for METex14+ NSCLC, cabozantinib is not available to many patients because of its cost without reimbursement. ANS014004, a Type II multi-targeted MET TKI, is currently under clinical development (NCT06307795 [in the US], NCT06328439 [in China]). In pre-clinical studies, ANS014004 demonstrated superior inhibitory activity against acquired D1228 and Y1230 resistance mutations when compared with other Type II TKIs, such as cabozantinib and merestinib.34 Achieving an indication against D1228 and Y1230 resistance mutations will be another step forward in the treatment of METex14+ NSCLC.
Inability to Inhibit the Active MET Protein When Potential Lack of Negative Feedback on Hepatocyte Growth Factor, the Major Ligand to MET Protein, Switch the Equilibrium to Active MET Protein
It is likely that with the inhibition of inactive MET protein, there is loss of negative feedback upon hepatocyte growth factor (HGF), the ligand to MET, leading to its increased expression and shifting most of the MET protein to the active state,4 where current Type Ib inhibitors cannot bind. In addition to the necessity to develop a TKI that can inhibit the active MET protein,35 the development of a monoclonal antibody against the HGF ligand is necessary to complement MET TKIs although there is no current development.36 Blocking the entire MET signaling axis (MET TKI + anti-MET monoclonal antibodies + anti-HGF monoclonal antibodies) may need to be developed to ensure the optimal control of METex14+ NSCLC.37 The approved bi-specific EGFR/MET antibody amivantamab has reported modest activity against METex14+ NSCLC patients (ORR = 50% in treatment-naïve participants [N = 16]; ORR = 46% in participants without prior MET therapies [N = 28]; ORR = 19% in participants with prior MET therapies [N = 53]) has been reported. The median PFS was 5.3 months (95% CI, 4.3–7.0).38 Peripheral edema occurred in 40% of patients, with 4% having grade ≥ 3.38 Thus, minimizing peripheral edema in any future combination treatment is paramount given the elderly age of these patients.
Lack of Randomized Trials
The time to conduct randomized trials in METex14+ NSCLC to demonstrate the superiority of MET TKIs over chemotherapy may have largely been passed, given the robust efficacy of the five MET TKIs and their proven CNS activities. However, given the differential efficacy of MET TKI and immunotherapy based on PS-L1 expression from a recent real-world retrospective case-control study, a randomized trial may still be desired.13 Going forward, next-generation MET TKI (even Type Ib inhibitors) may need to complete a randomized trial against currently approved MET TKIs (or chemotherapy +/- immunotherapy) likely deters future global development of MET TKI beyond tepotinib and capmatinib. A pathway to the accelerated approval of a novel MET TKI would be a Type II MET TKI that can demonstrate activity against acquired MET mutations at D1228 and Y1230. This will require sponsors to also develop a CDx to detect acquired MET mutations and may limit the approved indications of the Type Ib inhibitor but may bypass the need for a randomized phase 3 trial that is not guaranteed for success.
Indications for Tumors Other Than METex14+ NSCLC
On April 17, 2024, vebreltinib was approved for adult patients with IDH-mutant astrocytoma (WHO Grade 4) or glioblastoma with a history of low-grade glioma harboring the PTPRZ1-MET fusion gene who had failed prior therapies in China based on the results of the FUGEN study (NCT06105619).39 The median OS in the vebreltinib group (N=42) and chemotherapy group (N=39) was 6.31 months (95% CI, 4.44–8.77) and 3.38 months (95% CI, 2.37–4.27), respectively. The HR for OS was significant at 0.52 (90% CI, 0.32–0.85; P = 0.009), which was the primary endpoint of the trial.39 Furthermore, vebreltinib has demonstrated activity (partial response) against MET fusions in other tumor types, including lung adenocarcinoma, pancreatic adenocarcinoma, intrahepatic cholangiocarcinoma, and salivary gland carcinoma.40
Summary
We have provided a concise regulatory timeline and indications for the five approved Type Ib MET TKIs (all have first-line or previously-treated indications) in China for METex14+ NSCLC. We further summarized the patient characteristics, clinical efficacy, and adverse events that underpinned the five MET-TKIs approved in China. All five MET TKIs had similar clinical efficacy and incidence of adverse events, with peripheral edema being the most common class effect of MET protein inhibition. Similar to the decision on which MET TKI to use outside China (either capmatinib or tepotinib), the decision on which MET TKI to use depends on physicians’ familiarity with a particular TKI, perceived efficacy versus toxicities, and potential cost to patients. However, resistance to one MET TKI is likely to result in resistance to all other approved MET TKIs as they are all Type Ib inhibitors. The development of Type II MET TKIs for formal regulatory approval to overcome acquried resistance MET mutations to current Type Ib MET TKIs, and combination therapies to completely block the HGF-MET signaling axis is the future goal and aspiration in the treatment of METex14+ NSCLC patients.
Disclosure
Dr Sai-Hong Ou reports stock ownership from BlossomHill Therapeutics, MBrace Therapeutics, Nuvalent, Lilly, and Nuvation Bio; also personal fees from Pfizer, Astra Zeneca, BMS, and Bayer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Blume-Jensen P, Hunter T. Oncogenic kinase signalling. Nature. 2001;411(6835):355–365. doi:10.1038/35077225
2. Frampton GM, Ali SM, Rosenzweig M, et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 2015;5(8):850–859. doi:10.1158/2159-8290.CD-15-0285
3. Schrock AB, Frampton GM, Suh J, et al. Characterization of 298 patients with lung cancer Harboring MET Exon 14 skipping alterations. J Thorac Oncol. 2016;11(9):1493–1502. doi:10.1016/j.jtho.2016.06.004
4. Reungwetwattana T, Liang Y, Zhu V, Ou SI. The race to target MET exon 14 skipping alterations in non-small cell lung cancer: the why, the how, the who, the unknown, and the inevitable. Lung Cancer. 2017;103:27–37. doi:10.1016/j.lungcan.2016.11.011
5. Paik PK, Drilon A, Fan PD, et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping. Cancer Discov. 2015;5:842–849. doi:10.1158/2159-8290.CD-14-1467
6. Cui JJ. Targeting receptor tyrosine kinase MET in cancer: small molecule inhibitors and clinical progress. J Med Chem. 2014;57:4427–4453. doi:10.1021/jm401427c
7. Fujino T, Kobayashi Y, Suda K, et al. Sensitivity and resistance of MET Exon 14 mutations in lung cancer to eight MET tyrosine kinase inhibitors in vitro. J Thorac Oncol. 2019;14:1753–1765. doi:10.1016/j.jtho.2019.06.023
8. Pruis MA, Paats MS, Geurts WRR, et al. Overcoming acquired resistance mutation MET D1228N to crizotinib with cabozantinib in NSCLC with MET Exon 14 skipping mutation. JCO Precis Oncol. 2021;5:849–853. doi:10.1200/PO.21.00076
9. Wolf J, Seto T, Han JY, et al. Capmatinib in MET Exon 14-mutated or MET-amplified non-small-cell lung cancer. N Engl J Med. 2020;383(10):944–957. doi:10.1056/NEJMoa2002787
10. Paik PK, Felip E, Veillon R, et al. Tepotinib in Non-Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. N Engl J Med. 2020;383(10):931–943. doi:10.1056/NEJMoa2004407
11. Mazieres J, Paik PK, Garassino MC, et al. Tepotinib treatment in patients with MET Exon 14-skipping non-small cell lung cancer: long-term follow-up of the VISION Phase 2 nonrandomized clinical trial. JAMA Oncol. 2023;9(9):1260–1266. doi:10.1001/jamaoncol.2023.1962
12. Wolf J, Hochmair M, Han JY, et al. Capmatinib in MET exon 14-mutated non-small-cell lung cancer: final results from the open-label, phase 2 GEOMETRY mono-1 trial. Lancet Oncol. 2024;25(10):1357–1370. doi:10.1016/S1470-2045(24)00441-8
13. Pecci F, Li H, Di Federico A, et al. First-line MET tyrosine kinase inhibitors versus immunotherapy ± chemotherapy for patients with MET exon 14 skipping mutant metastatic NSCLC. Clin Cancer Res. 2025. doi:10.1158/1078-0432.CCR-25-1735
14. Drilon A, Clark JW, Weiss J, et al. Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration. Nat Med. 2020;26(1):47–51. doi:10.1038/s41591-019-0716-8
15. Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363(18):1693–1703. doi:10.1056/NEJMoa1006448
16. Shaw AT, Ou SH, Bang YJ, et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2014;371(21):1963–1971. doi:10.1056/NEJMoa1406766
17. Lu S, Fang J, Li X, et al. Once-daily savolitinib in Chinese patients with pulmonary sarcomatoid carcinomas and other non-small-cell lung cancers harbouring MET exon 14 skipping alterations: a multicentre, single-arm, open-label, phase 2 study. Lancet Respir Med. 2021;9(10):1154–1164. doi:10.1016/S2213-2600(21)00084-9
18. Lu S, Fang J, Li X, et al. Long-term efficacy, safety, and subgroup analysis of Savolitinib in Chinese patients with NSCLCs harboring MET Exon 14 skipping alterations. JTO Clin Res Rep. 2022;3(10):100407. doi:10.1016/j.jtocrr.2022.100407
19. Yu Y, Guo Q, Zhang Y, et al. Savolitinib in patients in China with locally advanced or metastatic treatment-naive non-small-cell lung cancer harbouring MET exon 14 skipping mutations: results from a single-arm, multicohort, multicentre, open-label, phase 3b confirmatory study. Lancet Respir Med. 2024;12(12):958–966. doi:10.1016/S2213-2600(24)00211-X
20. Yu Y, Zhou J, Li X, et al. Gumarontinib in patients with non-small-cell lung cancer harbouring MET exon 14 skipping mutations: a multicentre, single-arm, open-label, phase 1b/2 trial. EClinicalMedicine. 2023;59:101952. doi:10.1016/j.eclinm.2023.101952
21. Yang JJ, Zhang Y, Wu L, et al. Vebreltinib for advanced non-small cell lung cancer Harboring c-Met Exon 14 skipping mutation: a multicenter, single-arm, Phase II KUNPENG Study. J Clin Oncol. 2024;42(31):3680–3691. doi:10.1200/JCO.23.02363
22. Drilon A, Lin JJ, Filleron T, et al. Frequency of brain metastases and multikinase inhibitor outcomes in patients with RET-rearranged lung cancers. J Thorac Oncol. 2018;13(10):1595–1601. doi:10.1016/j.jtho.2018.07.004
23. Liu X, Jia Y, Stoopler MB, et al. Next-generation sequencing of pulmonary sarcomatoid carcinoma reveals high frequency of actionable MET gene mutations. J Clin Oncol. 2016;34(8):794–802. doi:10.1200/JCO.2015.62.0674
24. Schrock AB, Li SD, Frampton GM, et al. Pulmonary sarcomatoid carcinomas commonly harbor either potentially targetable genomic alterations or high tumor mutational burden as observed by comprehensive genomic profiling. J Thorac Oncol. 2017;12(6):932–942. doi:10.1016/j.jtho.2017.03.005
25. Kato T, Yang JC, Ahn MJ, et al. Efficacy and safety of tepotinib in Asian patients with advanced NSCLC with MET exon 14 skipping enrolled in VISION. Br J Cancer. 2024;130(10):1679–1686. doi:10.1038/s41416-024-02615-9
26. Matsumura N, Mandai M. PMDA regulatory update on approval and revision of the precautions for use of anticancer drugs: approval selpercatinib for solid tumor with RET fusion, gumarontinib for non-small cell lung cancer with MET gene exon 14 skipping mutation, momelotinib for myelofibrosis, bexarotene for adult T-cell leukemia/lymphoma, valemetostat for peripheral T-cell lymphoma, and pirtobrutinib for mantle cell lymphoma in Japan. Int J Clin Oncol. 2024;29(9):1207–1208. doi:10.1007/s10147-024-02579-z
27. Awad MM, Devarakonda S, Yang JL, et al. PP01.104 vebreltinib efficacy in METex14 mutant NSCLC with or without concurrent MET amplification, MET GCN status distributions compared with public databases. j Thorac Oncol. 2024;19(7):e45–e46. doi:10.1016/j.jtho.2024.05.331
28. Lu S, Wang J, Yang N, et al. Savolitinib combined with osimertinib versus chemotherapy in EGFR-mutant and MET-amplified advanced NSCLC after disease progression on EGFR TKI: results from a randomized phase 3 SACHI study. j Clin Oncol. 2025;43(17_suppl):LBA8505. doi:10.1200/JCO.2025.43.17_suppl.LBA8505
29. Cai B, Li X, Huang X, et al. Case report: sequential combination targeted therapy with Type I and II MET inhibitors in a metastatic EGFR-Mutated, MET-Amplified NSCLC patient with acquired MET Y1230H mutation. Front Oncol. 2021;11:738832. doi:10.3389/fonc.2021.738832
30. Yao Y, Yang H, Zhu B, et al. Mutations in the MET tyrosine kinase domain and resistance to tyrosine kinase inhibitors in non-small-cell lung cancer. Respir Res. 2023;24(1):28. doi:10.1186/s12931-023-02329-1
31. Fujino T, Suda K, Koga T, et al. Foretinib can overcome common on-target resistance mutations after capmatinib/tepotinib treatment in NSCLCs with MET exon 14 skipping mutation. J Hematol Oncol. 2022;15(1):79. doi:10.1186/s13045-022-01299-z
32. Klempner SJ, Borghei A, Hakimian B, Ali SM, Ou SI. Intracranial activity of cabozantinib in MET Exon 14-Positive NSCLC with brain metastases. J Thorac Oncol. 2017;12(1):152–156. doi:10.1016/j.jtho.2016.09.127
33. Takeda M, Ota M, Iwama E, et al. A Phase II, open label, single-arm study on the efficacy of cabozantinib in patients with advanced/metastatic nonsmall cell lung cancer harboring MET Exon 14 alterations who developed acquired resistance to tepotinib or capmatinib (CAPTURE Trial). Clin Lung Cancer. 2025;26(3):e232–e235. doi:10.1016/j.cllc.2024.12.004
34. Li G, Shi HP, Zhang P, et al. ANS014004, a novel small-molecule type II c-Met inhibitor effectively overcomes clinical-resistance MET mutations and exhibits antitumor activity in preclinical models of MET-amplified non-small cell lung cancer (NSCLC) and gastric cancer [abstract]. Mol Cancer Ther. 2023;22(12 Suppl):AbstractnrC145. doi:10.1158/1535-7163.TARG-23-C145
35. Shin JS, Hong SW, Moon JH, et al. NPS-1034, a novel MET inhibitor, inhibits the activated MET receptor and its constitutively active mutants. Invest New Drugs. 2014;32(3):389–399. doi:10.1007/s10637-013-0039-4
36. Okamoto W, Okamoto I, Tanaka K, et al. TAK-701, a humanized monoclonal antibody to hepatocyte growth factor, reverses gefitinib resistance induced by tumor-derived HGF in non-small cell lung cancer with an EGFR mutation. Mol Cancer Ther. 2010;9(10):2785–2792. doi:10.1158/1535-7163.MCT-10-0481
37. Reungwetwattana T, Ou S-HI. MET exon 14 deletion (METex14): finally, a frequent-enough actionable oncogenic driver mutation in non-small cell lung cancer to lead MET inhibitors out of “40 years of wilderness” and into a clear path of regulatory approval. Transl Lung Cancer Res. 2015;4(6):820–824. doi:10.3978/j.issn.2218-6751.2015.12.03
38. Krebs MG, Cho BC, Hiret S, et al. Amivantamab in participants with advanced Non-small Cell Lung Cancer (NSCLC) and MET Exon 14 skipping mutations: final results from the CHRYSALIS Study. J Thorac Oncol. 2025. [in press]. doi:10.1016/j.jtho.2025.05.012
39. Jiang T, Bao Z, Yang FD, et al. Efficacy and safety of the vebreltinib in patients with previously treated, secondary glioblastoma/IDH mutant glioblastoma with PTPRZ1-METFUsion GENe (FUGEN): a randomised, multicentre, open-label, phase II/III trial. J Clin Oncol. 2024;42:2003. doi:10.1200/JCO.2024.42.16_suppl.2003
40. Nakazawa S, Pecci F, Odintsov I, et al. Antitumor activity of vebreltinib and characterization of clinicogenomic features in solid tumors with MET rearrangements. Cancer Discov. 2025;15:1129–1140. [in press]. doi:10.1158/2159-8290.CD-24-1726
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.