Back to Journals » Journal of Pain Research » Volume 19
A Comprehensive Mendelian Randomization Study of Bidirectional Causal Relationships Between Pain and Mental Disorders
Received 17 August 2025
Accepted for publication 17 January 2026
Published 21 February 2026 Volume 2026:19 561284
DOI https://doi.org/10.2147/JPR.S561284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Xiao Liang,1 Yuchao Fan2
1Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Department of Anesthesiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, Affiliated Cancer Hospital of University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China
Correspondence: Yuchao Fan, Department of Anesthesiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, Affiliated Cancer Hospital of University of Electronic Science and Technology of China, No. 55, Section 4, Renmin South Road, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]
Background: Pain and mental disorders frequently co-occur, yet the direction and specificity of their relationship remain uncertain due to limitations of observational studies. Mendelian randomization (MR) provides an opportunity to clarify causal links between distinct pain phenotypes and psychiatric outcomes.
Methods: We performed a comprehensive bidirectional MR analysis to investigate causal relationships between multiple pain conditions and mental and personality disorders. Multivariable MR was applied to assess the independence of these associations while accounting for common comorbidities. Robustness was evaluated using complementary sensitivity analyses.
Results: Forward analyses showed that several pain phenotypes - including back pain, headaches, neck or shoulder pain, stomach or abdominal pain, migraine, and trigeminal neuralgia—were associated with increased risk of specific mental disorders. Reverse analyses indicated that mental disorders also predispose individuals to certain pain conditions. Most associations remained robust after multivariable adjustment, although some were attenuated by obesity or substance use.
Conclusion: These findings demonstrate structured, pain - type - specific bidirectional relationships between pain and mental disorders. Clinically, they support phenotype-informed screening and management strategies, including targeted assessment of depression and anxiety in patients with high-risk pain conditions and proactive evaluation of pain symptoms in patients with mental disorders, to facilitate earlier risk stratification and integrated care.
Keywords: pain, mental disorders, bidirectional mendelian randomization, multivariate mendelian randomization, causal effect
A Letter to the Editor has been published for this article.
Introduction
Pain and mental disorders, recognized as significant public health challenges imposing substantial clinical and economic burdens on individuals and society, have been extensively studied and found to exhibit a profound comorbidity foundation.1–4 Pain, defined as an “unpleasant sensory and emotional experience typically caused by, or resembling that caused by, actual or potential tissue injury,” has been acknowledged for its adverse impact on functioning, social engagement, and psychological well-being.4–6 This subjective, multidimensional discomfort encompasses sensory, emotional, and cognitive dimensions and is frequently accompanied by emotional and cognitive impairments such as anxiety, depression, sleep disturbances, and cognitive deficits.7,8
Pain not only triggers extensive and profound functional and morphological reorganization in the brain but also leads to widespread disruption in the brain’s topological structure.9–12 This disruption can induce disarray in information sharing, consequently affecting advanced brain functions.11–16 In the experience of pain, abnormalities in gray matter density,17,18 white matter connectivity,11,18,19 and neurotransmitters like glutamate, opioids, and dopamine play crucial roles.11,16,20–23 These mechanisms are closely intertwined with emotional states, mental disorders, and even personality disorders.6,11,24–26 Additionally, pain is often reported as a somatic symptom by patients with mental disorders.22,27 These pieces of evidence strongly support the potential bidirectional relationship between pain and mental disorders. Clarifying this relationship not only aids in developing novel therapeutic approaches for pain management but also holds promise for early interventions to prevent patients from falling victim to the co-occurrence of emotional and mental disorders.7
Nevertheless, current research in this field is predominantly confined to preclinical and observational studies, facing challenges such as interspecies differences between animals and humans, inadequate research designs, and intricate confounding factors.27–29 Moreover, existing studies have predominantly concentrated on assessing the relationship between pain and depression or anxiety, overlooking a broader spectrum of psychiatric diagnoses.24 This limited focus may lead to neglecting the circumstances of patients with other mental disorders. Hence, there is an urgent need for the adoption of innovative research methodologies to comprehensively explore and elucidate the causal relationship between pain, mental disorders, and personality disorders.
In recent years, there has been a significant focus on harnessing genetic prediction methods to uncover the intricate causal associations between intricate risk factors and diseases in the realm of epidemiological research.30–32 One such influential technique is Mendelian randomization (MR), which employs genetic variations as instrumental variables (IVs) to explore the causal associations between various exposures and their corresponding outcomes. By ensuring the haphazard allocation of genetic material, MR establishes the independence of these IVs from confounding factors. This process effectively eradicates the influence of both identified and unidentified confounding elements that could interfere with the relationship between pain and mental or personality disorders.33,34 This method adeptly resolves the vexing challenge of confounding variables that often plague observational studies.35
Furthermore, in MR analysis, single nucleotide polymorphisms (SNPs) serve as key factors for investigating causal associations with outcomes. These SNPs follow strictly Mendelian genetic principles, distributing randomly into gametes during the formation of germ cells. This random allocation ensures a level of comparability akin to that achieved in randomized controlled trials, enhancing the robustness of the analysis.31–33,36 Additionally, MR successfully sidesteps the potential ethical and practical dilemmas that can arise in the context of randomized controlled trials.34 Consequently, MR stands out as an exceptionally viable and sophisticated approach for delving into the intricate causal relationships between pain and mental or personality disorders. Its rigorous methodology and ability to address confounding factors make it a valuable tool in advancing our understanding of these complex interactions.
Therefore, MR offers several advantages over traditional research methods.32,37,38 Firstly, it reduces confounding effects. MR utilizes genetic variation as a natural randomization control, reducing the impact of environmental and behavioral factors on study outcomes.31,39 This helps to assess the influence of genes on specific traits or diseases more clearly, avoiding common issues with confounding factors in conventional research. Secondly, it handles comorbid conditions effectively.40,41 MR allows for an independent evaluation of the relationship between genes and diseases, unaffected by the presence of comorbid conditions (multiple diseases existing together). This enables researchers to more accurately determine causal relationships between genes and specific diseases. Thirdly, it is closer to randomized controlled trials.40,41 MR is akin to a randomized controlled trial, providing evidence that is closer to experimental design, aiding in inferring causal relationships rather than mere associations. Lastly, it reduces bias in observational studies.39–41 Traditional observational studies are susceptible to individual reporting biases and uncontrollable confounding factors, whereas MR reduces these biases by leveraging the randomness of genetic variation.
This study employed bidirectional Univariable MR (UVMR) and Multivariate MR (MVMR) approach,42–44 aiming to delve deeply into the intricate causal relationships between pain and mental or personality disorders. UVMR, a foundational MR method focusing on one exposure and one outcome. It uses genetic variants (as instrumental variables) strongly associated with the target exposure to infer the causal relationship between this single exposure and the outcome, minimizing confounding and reverse causation.42 MVMR, an extended MR approach incorporating ≥2 exposures (or confounders/mediators). It applies independent genetic variant sets linked to each variable to disentangle their independent causal effects on the outcome, enabling precise inference in complex multi-factor scenarios (eg, coexisting pain subtypes and mental disorders).43,44 The aim of this study is to comprehensively evaluate bidirectional causal relationships between multiple regional pain phenotypes and a broad spectrum of mental and personality disorders using UVMR and MVMR approaches. We hypothesise that genetic liability to specific pain phenotypes and to particular psychiatric disorders exhibit bidirectional causal associations — some of which remain after accounting for correlated risk factors such as obesity, insomnia, and substance use — thereby providing clinically actionable information for early identification and intervention.
Methods
Study Design
This study utilized bidirectional two-sample UVMR and MVMR,42–44 employing genome-wide association study (GWAS) summary statistics, to investigate the potential causal relationship between pain and Mental or Personality disorders, as illustrated in Figure 1. This study was initiated on September 13, 2023.
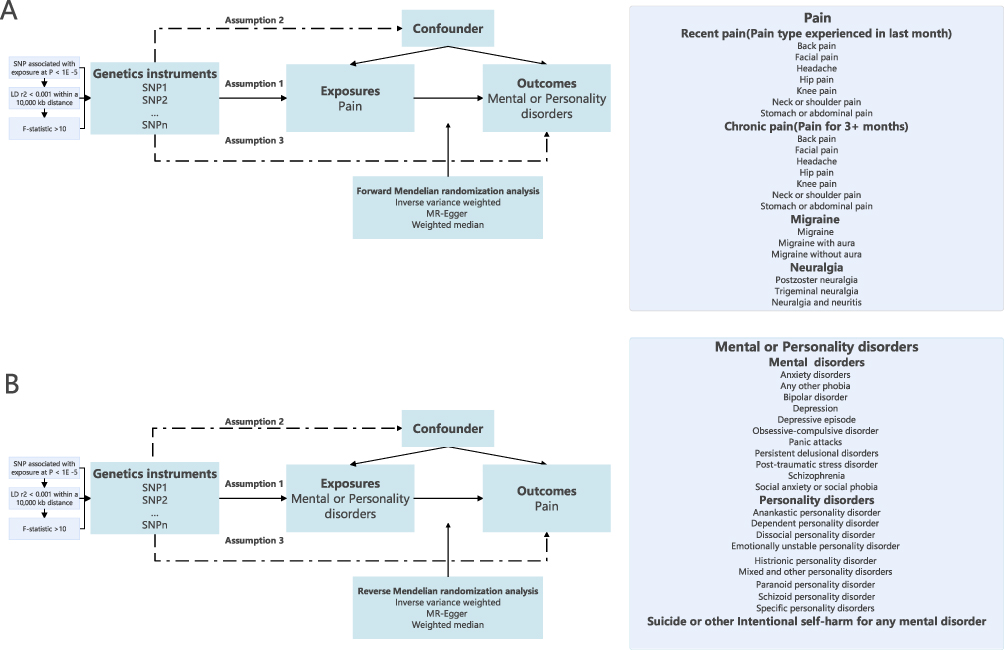 |
Figure 1 Design Overview and Instrumental Variable Assumptions in this Mendelian Randomization (MR) Study Using genetic variants as instrumental variables, this MR study explores causal associations between Pain and Mental or Personality disorders. (A) In the forward MR analysis, Pain serves as the exposure, while Mental or Personality disorders serve as the outcomes. (B) In a reverse MR analysis, Mental or Personality disorders serve as the exposures, with Pain as the outcome.Subsequently, insomnia, obesity, and substance use were included as risk factors in the multivariable Mendelian randomization analysis to assess the independent effects of pain on mental disorders and vice versa. The genetic variant employed as an Instrumental Variable in the analysis needs to satisfy three criteria: Assumption 1: The genetic variant must manifest a substantial association with the Exposure. Assumption 2: The genetic variant should exhibit no discernible correlation with confounding factors capable of affecting the association between the Exposure and the Outcomes. Assumption 3: The genetic variant must refrain from exerting a direct influence on the Outcomes, except through its well-established correlation with the Exposure. Abbreviations: MR, Mendelian randomization; LD, Linkage disequilibrium; SNP, single nucleotide polymorphisms. |
The general process of the study involves first collecting relevant datasets, then selecting SNPs as IVs based on predefined thresholds and assumptions. Next, MR analysis is conducted to explore causal relationships between exposure and outcome. Finally, sensitivity analysis is performed to assess the presence of heterogeneity, horizontal pleiotropy, and the robustness of MR results.
In the forward MR analysis, pain was posited as the exposure, while Mental or Personality disorders were considered as the outcome. Conversely, in the reverse MR analysis, Mental or Personality disorders were treated as the exposure variable, with pain as the outcome of interest. Subsequently, obesity, insomnia, and substance use will be included as additional factors in a multivariable model for a MVMR analysis.
The assessment of the causal effect was predicated on genetic variation, which served as IVs. The IV assumptions necessary for the validity of our genetic instruments in this research are as follows:31,32 Assumption 1: The genetic variant must manifest a substantial association with the Exposure. Assumption 2: The genetic variant should exhibit no discernible correlation with confounding factors capable of affecting the association between the Exposure and the Outcomes. Assumption 3: The genetic variant must refrain from exerting a direct influence on the Outcomes, except through its well-established correlation with the Exposure.
Data Source
The genetic dataset utilized in this study was derived from the IEU open GWAS project (https://gwas.mrcieu.ac.uk/), an encompassing compilation of data from multiple reputable origins. Notable contributors include the UK Biobank (https://biobank.ctsu.ox.ac.uk/), FinnGen (https://risteys.finregistry.fi/), Neale Lab (https://nealelab.ucdavis.edu/), the Medical Research Council Integrative Epidemiology Unit (MRC-IEU) (https://www.bristol.ac.uk/integrative-epidemiology/), and the Psychiatric Genomics Consortium (PGC).45 To minimize the impact of potential confounding factors, this study strategically leveraged genetic associations drawn from separate GWAS datasets, all originating from the same ancestral population (European descent). These datasets uniformly employed a binary classification system, encompassing both males and females. A comprehensive summary of the datasets utilized in this investigation is available in Supplemental Table 1.
Trait Related to Pain
The datasets pertaining to pain encompass two primary categories: “Recent pain” (representing pain types experienced within the last month, including Back pain (Cases = 118471, Controls = 343,386), Facial pain (Cases = 8595, Controls = 453,262), Headache (Cases =93308, Controls = 368,549), Hip pain (Cases = 52087, Controls = 409,770), Knee pain (Cases = 98704, Controls = 363,153), Neck or shoulder pain (Cases = 106521, Controls = 355,336), and Stomach or abdominal pain (Cases = 39646, Controls = 422,211)) and “Chronic pain” (indicating pain persisting for three or more months, including Back pain (Cases = 80588, Controls = 36,816), Facial pain (Cases =3107, Controls = 3403), Headache (Cases = 41719, Controls = 49,550), Hip pain (Cases = 40152, Controls = 11,364), Knee pain (Cases = 76910, Controls = 20,979), Neck or shoulder pain (Cases = 72887, Controls = 32,509), and Stomach or abdominal pain (Cases = 21711, Controls = 17,200)). These data were collected through the ACE system, which gathers information on health and medical history, including details related to pain, using screenshots of touchscreen questionnaires administered in the UK Biobank Assessment Centres for the collection of self-reported medical conditions. Participants were queried regarding their experiences, specifically inquiring, “In the last month, have you experienced any of the following pain that interfered with your usual activities?” and “Have you had specific pains for more than three months?”
In addition, we expanded our analysis to include data on “Migraine” (comprising Migraine (Cases = 8547, Controls = 176107, ICD-10 (G43), Mean age at first event (years) was 40.27), Migraine with aura (Cases = 3541, Controls =176107, ICD-10 (G43.1), Mean age at first event (years) was 42.96), and Migraine without aura (Cases = 3215, Controls = 176107, ICD-10 (G43.0), Mean age at first event (years) was 388.23),) and “Neuralgia” (encompassing Postzoster neuralgia (Cases = 144, Controls = 195047, ICD-10 (G53.0*G53.0*B02.20, G53.0*B02.2), Mean age at first event (years) was 66.61), Trigeminal neuralgia (Cases = 800, Controls = 195047, ICD-10 (G50.0), Mean age at first event (years) was 54.23), and Neuralgia and neuritis (Cases = 800, Controls = 167641, ICD-10 (G79.2.0), Mean age at first event (years) was 53.10)) as representative pain categories. These Supplemental datasets were sourced from the FinnGen database.
Trait Related to Mental and Personality Disorders
The datasets related to mental and personality disorders cover a wide range of conditions. Specifically, the datasets for Any Other Phobia (Cases = 1591, Controls = 116,119), Depression (Cases = 25087, Controls = 92,695), Panic Attacks (Cases = 6518, Controls = 111,204), and Social Anxiety or Social Phobia (Cases = 1474, Controls = 116242) are sourced from the Neale Lab. Participants were asked during the diagnostic assessment: “Have you been diagnosed with one or more of the following mental health problems by a professional, even if you don’t currently have it?” By “professional”, we mean any doctor, nurse, or individual with specialized training (such as a psychologist or therapist).
The dataset for depressive episode (Cases = 5842, Controls = 457168) is sourced from MRC-IEU and is included in the Biobank’s “Source of the Outcome First Reported in Health-related Outcomes” catalog. The diagnosis criteria for this condition are based on ICD-10 (F32) standards.
The datasets for bipolar disorder (Cases = 20352, Controls = 31358) and schizophrenia (Cases = 76755, Controls = 243649) are from the PGC. The GWAS data for bipolar disorder are derived from the study by Stahl et al (2019),46 with cases meeting international consensus criteria (DSM-IV or ICD-10). Lifetime diagnosis of bipolar disorder was confirmed using structured diagnostic tools administered by trained interviewers, clinical assessment by physicians, or review of medical records.
The GWAS data for schizophrenia is from the study by Trubetskoy et al (2022).45 This dataset consists of schizophrenia cases recruited from eight collections within the UK10K sequencing project. These cases were compared with matched population controls including non-psychiatric individuals from the UK10K project, healthy blood donors from the INTERVAL project, and participants from five Finnish population studies. The UK10K dataset was merged and analyzed with published data from a Swedish case-control study on schizophrenia.
The datasets for the remaining mental and personality disorders are all sourced from FinnGen, including Anxiety disorders (Cases = 20992, Controls = 166584, ICD-10 (F40-F48), Mean age at first event (years) was 38.75), Obsessive-compulsive disorder (Cases = 1059, Controls = 198110, ICD-10 (F42), Mean age at first event (years) was 32.63), Post-traumatic stress disorder (Cases = 1103, Controls = 198110, ICD-10 (F43.1), Mean age at first event (years) was 35.73), Persistent delusional disorder (Cases = 1665, Controls = 208674, ICD-10 (F22), Mean age at first event (years) was 49.05), Anankastic personality disorder (Cases = 476, Controls = 212179, ICD-10 (F60.5), Mean age at first event (years) was 42.98), Anxious personality disorder (Cases = 280, Controls = 212179, ICD-10 (F60.6), Mean age at first event (years) was 36.72), Dependent personality disorder (Cases = 411, Controls = 212179, ICD-10 (F60.7), Mean age at first event (years) was 41.48), Dissocial personality disorder (Cases = 340, Controls = 212179, ICD-10 (F60.2), Mean age at first event (years) was 31.19), Emotionally unstable personality disorder (Cases = 2637, Controls = 212179, ICD-10 (F60.3), Mean age at first event (years) was 32.50), Histrionic personality disorder (Cases = 96, Controls = 212179, ICD-10 (F60.4), Mean age at first event (years) was 34.41), Mixed and other personality disorders (Cases = 1666, Controls = 212179, ICD-10 (F61), Mean age at first event (years) was 38.50), Paranoid personality disorder (Cases = 354, Controls = 212179, ICD-10 (F60.0), Mean age at first event (years) was 39.20), Schizoid personality disorder (Cases = 424, Controls = 212179, ICD-10 (F60.1), Mean age at first event (years) was 33.32), and Specific personality disorders (Cases = 5409, Controls = 212179, ICD-10 (F60), Mean age at first event (years) was 34.93).
Furthermore, we included an analysis of Suicide or other Intentional self-harm for any mental disorder (SOIH−MD) (Cases = 55208, Controls = 166584, ICD-10 (X60-X84), Mean age at first event (years) was 37.39) as a severe adverse event related to mental disorders.
Trait Related to MVMR Factors
Data of Obesity (Cases = 8908, Controls = 209827, ICD-10 (E66), Mean age at first event (years) was 48.86), Insomnia (Cases = 1691, Controls = 216164, ICD-10 (F51.0, G47.0), Mean age at first event (years) was 49.42), Substance abuse (Cases = 12819, Controls = 166549, ICD-10 (F10-F19), Mean age at first event (years) was 45.24) were obtained from FinnGen.
Selection of Instrumental Variables
The study followed strict criteria when selecting IVs to ensure the reliability and validity of the chosen parameters. These IVs were carefully chosen based on several important factors. First, they had strong and significant associations with the exposure variable at a genome-wide level (with a significance threshold of P < 5e-6). Secondly, they needed to have an allele frequency above 0.01 within the group related to the outcome. Lastly, a crucial criterion was that these IVs had low linkage disequilibrium (LD), with an r2 value of less than 0.001 within a 10,000 kb radius (Figure 1).
To evaluate the strength of the IVs, we calculated the F-statistic for each individual SNP. IVs with a low F-statistic value below the threshold of 10 were considered weak. It was crucial to classify IVs in this way because weak IVs have the potential to introduce bias into the study outcomes.
The derivation of the F-statistic followed a prescribed mathematical formulation, denoted as  In order to quantify the proportion of variance elucidated by each SNP, the ensuing mathematical expression, denoted as
In order to quantify the proportion of variance elucidated by each SNP, the ensuing mathematical expression, denoted as  , was employed. Within this context, the symbol β conveys the effect size pertaining to the specific SNP under consideration. SE2 represented the square of the standard error associated with the effect size estimation. EAF, in turn, denotes the minor allele frequency inherent to the SNP. Notably, the variable N signifies the total count of individuals actively participating in the GWAS.
, was employed. Within this context, the symbol β conveys the effect size pertaining to the specific SNP under consideration. SE2 represented the square of the standard error associated with the effect size estimation. EAF, in turn, denotes the minor allele frequency inherent to the SNP. Notably, the variable N signifies the total count of individuals actively participating in the GWAS.
The confirmation of the correct direction for the instrumental SNPs is conducted using the Steiger test.47 SNPs that do not pass the Steiger screening will be excluded from the MR analysis. In this test, a p-value less than 0.05 signifies the validity of the causal direction.
MR Analysis
In the context of UVMR, the main analysis used in this study focused on using the Inverse Variance Weighting (IVW). This method is known for its ability to provide precise estimates of causation when all genetic variants are assumed to be valid IVs.48 It served as the foundation of our analysis.
In cases where there was heterogeneity, we used a random-effects IVW approach. However, if there was no heterogeneity, we employed a fixed-effects model to ensure the accuracy of our statistical analysis.
To manage the challenges of multiple hypothesis testing effectively, we utilized the Bonferroni method as a correction technique. This statistical approach helped us address the issue of inflated Type I error rates that can occur when testing many hypotheses simultaneously.49
The thresholds utilized for Bonferroni correction, denoting statistical significance, were as follows: For Recent pain (pain types experienced in the last month) or Chronic pain (pain persisting for 3+ months), the threshold was set at 0.007143 (0.05 divided by 7). In the case of Migraine, Neuralgia, Mental disorders, and Personality disorders, the thresholds were determined as 0.0167 (0.05 divided by 3), 0.0167 (0.05 divided by 3), 0.004545 (0.05 divided by 11), and 0.005 (0.05 divided by 10), respectively. These thresholds were applied to assess statistical significance in our analysis, ensuring a stringent control for multiple hypothesis testing across the various categories of pain and disorders.
Since some of the exposures and outcomes in our analysis may come from the same dataset, there is a possibility of sample overlap and weak IVs. MRlap was employed to identify potential sample overlap and assess its impact on result bias.50 If the difference between the observed effect and the adjusted effect is not significant (p > 0.05), the IVW-MR estimates can be considered reliable. Conversely, if a significant difference is found (p < 0.05), the adjusted effect should be prioritized.
MVMR Analysis
All pairs of exposures and outcomes that show significant causal effects in the UVMR analyses will undergo subsequent MVMR analysis. Obesity, insomnia, and substance abuse will each be included as adjustment factors in constructing separate multivariable models with the exposures.
Sensitivity Analyses
To enhance the robustness of IVW findings, we employed two complementary methodologies: MR-Egger regression and the weighted median (MR-WM) approach. MR-Egger was employed to address issues related to horizontal pleiotropy, albeit with a slight reduction in precision.51 We considered MR-Egger as supportive when the effect estimate aligned with MR-IVW, and the MR-Egger intercept exhibited a non-significant value (P > 0.05). Additionally, we adopted the MR-WM approach, an additional technique that yields a reliable causal estimate, provided that at least half of the weight in the analysis is derived from valid IVs.52
The assessment of heterogeneity was carried out using Cochran’s Q statistic derived from the MR-Egger method,51,53 with heterogeneity indicated by p-values below the threshold of 0.05. We performed a “leave-one-out” analysis to gauge the individual SNP’s impact on the causality between exposure and outcome. To assess IV pleiotropy, we utilized both the MR-Egger intercept and MR-PRESSO,54 with p-values exceeding 0.05 indicating the absence of pleiotropy. MR-PRESSO was instrumental in identifying SNP outliers, and post-outlier removal, it yielded results akin to IVW.54
It’s important to note that substantial result significance was contingent upon the alignment of directional outcomes among MR-Egger, MR-WM, and IVW. Otherwise, significance would be deemed nominal.
In MVMR analysis. The IVW method was used as the primary analytical tool for MVMR. Additionally, we included MR-WM as a Supplemental approach. The horizontal pleiotropy of IVs was assessed using MR-Egger, which ruled out horizontal pleiotropy when the p-value was greater than 0.05.
To detect heterogeneity, we utilized the IVW heterogeneity Q test. A p-value below 0.05 in this test indicated the presence of heterogeneity. In such cases, we relied on the MR-WM results to ensure accurate causality estimation, provided that at least 50% of the analysis’s weight came from valid IVs.52
Effect estimates, represented as odds ratios (ORs), along with their corresponding 95% confidence intervals (CIs), were presented as part of our analysis.
Significant results will undergo Z-score normalization of the beta values of SNPs in the exposure dataset. The mRnd online analysis tool, available at https://shiny.cnsgenomics.com/mRnd/, was utilized to evaluate the statistical power of our MR estimates. An excellent value was defined as achieving a statistical power greater than 80%.55 The MR analyses were conducted using R software (version 4.2.2) and the packages “TwoSampleMR,” “MendelianRandomization,” “MVMR,” “MRlap,” and “MRPRESSO.” Heatmaps and forest plots visualizing the causal effects were generated using “ggplot2 [3.3.6].” This study adheres to the guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR).
Results
In accordance with our defined criteria, each exposure-outcome paired IVs’ number has been determined, as detailed in Table 1. The details of SNPs used as IVs in both forward and reverse MR analyses are provided in Supplemental Tables 2 and 3. After the Steiger test, some SNPs were deleted (Supplemental Table 4). It is noteworthy that all IVs exhibited F-values exceeding 10, thereby eliminating the possibility of weak instrument bias.
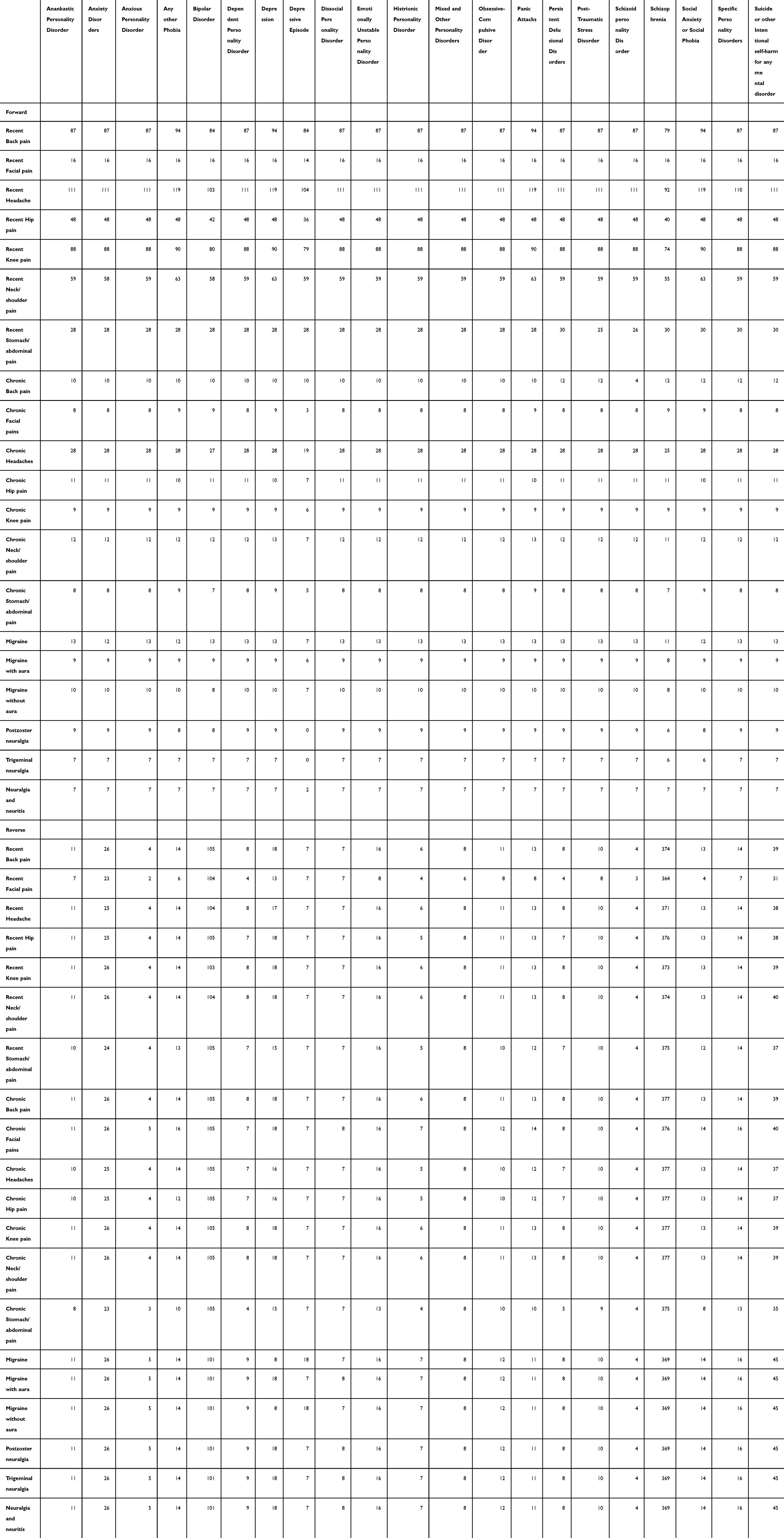 |
Table 1 Summary of SNP’s Number for Mendelian Randomization Analysis |
UVMR Analyses
Forward Analysis
Forward UVMR analyses identified multiple pain phenotypes that genetically increased the risk of mental and personality disorders (Figures 2–3; Supplemental Figures 1A–C and Supplemental Tables 5–7).
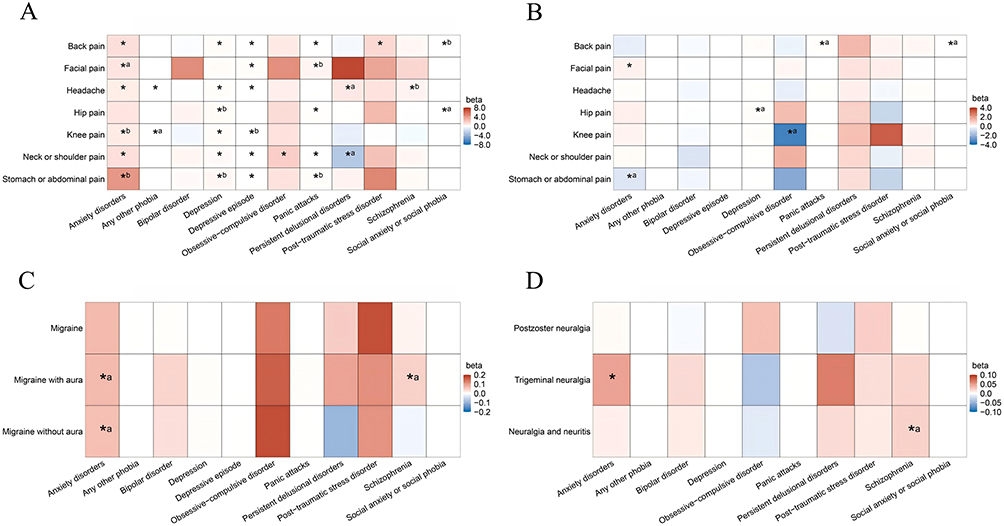 |
Figure 2 Forward Mendelian Randomization analysis the causal effect of Pain on Mental disorders. (A) Recent pain (Pain type experienced in last month) on Mental disorders; (B) Chronic pain (Pain for 3+ months) on Mental disorders; (C) Migraine on Mental disorders; (D) Neuralgia on Mental disorders. A positive beta value is indicated in red, while a negative beta value is indicated in blue, with the color intensity increasing as the absolute value of beta becomes larger. “*” represents a significance level of P < 0.05 (inverse variance weighted) “a” denotes a p-value less than 0.05 (inverse variance weighted) but not lower than Bonferroni thresholds. “b” indicates that the results from the inverse variance weighted method differ in direction from MR-Egger or weighted median methods, suggesting a nominal rather than substantial association. |
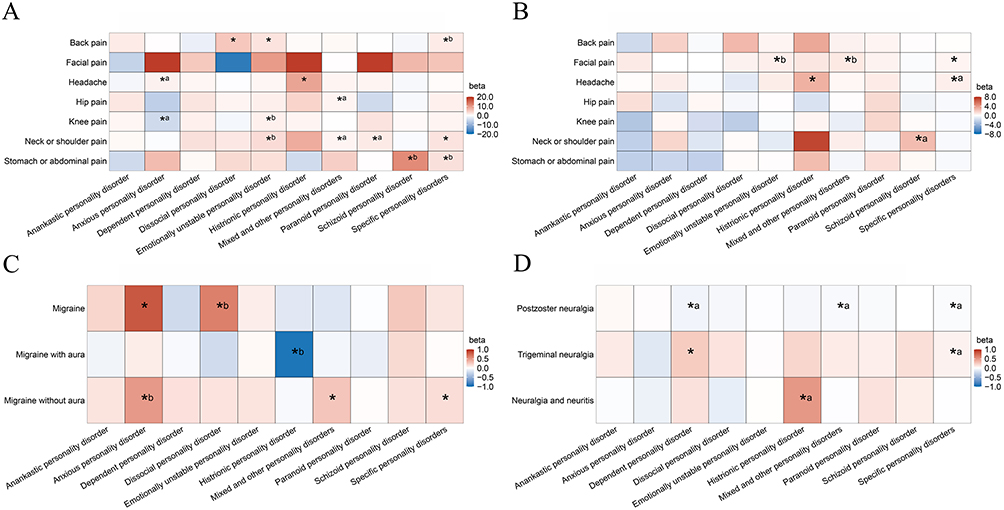 |
Figure 3 Forward Mendelian Randomization analysis the causal effect of Pain on Personality disorders. (A) Recent pain (Pain type experienced in last month) on Personality disorders; (B) Chronic pain (Pain for 3+ months) on Personality disorders; (C) Migraine on Personality disorders; (D) Neuralgia on Personality disorders. A positive beta value is indicated in red, while a negative beta value is indicated in blue, with the color intensity increasing as the absolute value of beta becomes larger. “*” represents a significance level of P < 0.05 (inverse variance weighted) “a” denotes a p-value less than 0.05 (inverse variance weighted) but not lower than Bonferroni thresholds. “b” indicates that the results from the inverse variance weighted method differ in direction from MR-Egger or weighted median methods, suggesting a nominal rather than substantial association. |
Among recent pain conditions, back pain showed consistent associations with anxiety disorders, depression-related phenotypes, post-traumatic stress disorder, and panic attacks. Headache was linked to anxiety disorders, depression, depressive episodes, and phobic disorders. Neck or shoulder pain demonstrated broad associations across anxiety, depression-related phenotypes, obsessive–compulsive disorder, and panic attacks. More specific associations were observed for facial pain and stomach or abdominal pain with depressive episodes, and for knee pain with depression.
For chronic pain (≥3 months), fewer but more selective associations were detected. Chronic facial pain and trigeminal neuralgia were associated with anxiety disorders.
Regarding personality disorders, recent back pain was associated with dissocial and emotionally unstable personality disorders, while headache showed strong links with histrionic personality disorder. Neck or shoulder pain was associated with specific personality disorders. In chronic pain analyses, facial pain and headache remained associated with specific and histrionic personality disorders, respectively. Migraine and migraine without aura were linked to anxious, mixed, and specific personality disorders, whereas trigeminal neuralgia was associated with dependent personality disorder (Figure 3 and Supplemental Table 7).
Reverse MR Analysis
Reverse MR analyses suggested that several mental disorders predispose individuals to pain phenotypes (Supplemental Figures 1D and Figures 4 and 5 and Supplemental Tables 8–10).
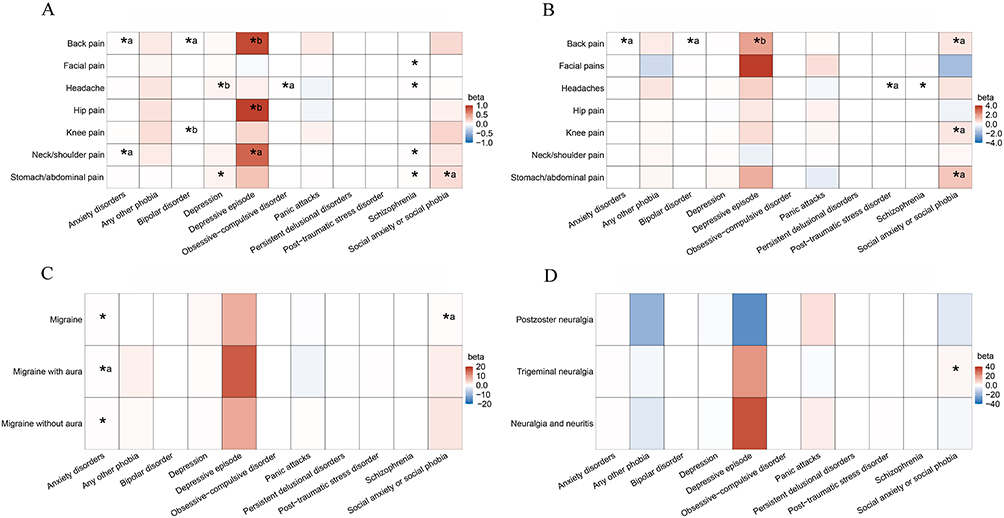 |
Figure 4 Reversed Mendelian Randomization analysis the causal effect of Pain on Mental disorders. (A) Recent pain (Pain type experienced in last month) on Mental disorders; (B) Chronic pain (Pain for 3+ months) on Mental disorders; (C) Migraine on Mental disorders; (D) Neuralgia on Mental disorders. A positive beta value is indicated in red, while a negative beta value is indicated in blue, with the color intensity increasing as the absolute value of beta becomes larger. “*” represents a significance level of P < 0.05 (inverse variance weighted) “a” denotes a p-value less than 0.05 (inverse variance weighted) but not lower than Bonferroni thresholds. “b” indicates that the results from the inverse variance weighted method differ in direction from MR-Egger or weighted median methods, suggesting a nominal rather than substantial association. |
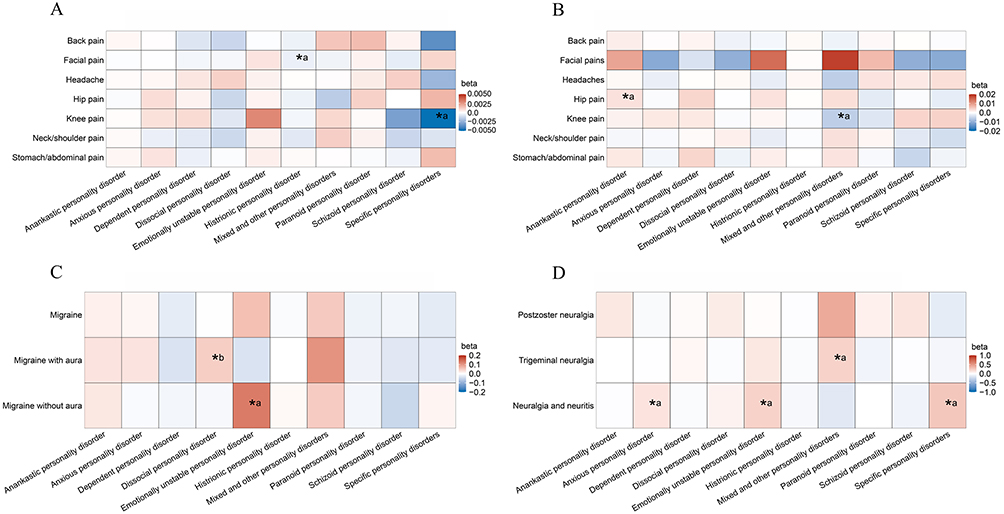 |
Figure 5 Reversed Mendelian Randomization analysis the causal effect of Pain on Personality disorders. (A) Recent pain (Pain type experienced in last month) on Personality disorders; (B) Chronic pain (Pain for 3+ months) on Personality disorders; (C) Migraine on Personality disorders; (D) Neuralgia on Personality disorders. A positive beta value is indicated in red, while a negative beta value is indicated in blue, with the color intensity increasing as the absolute value of beta becomes larger. “*” represents a significance level of P < 0.05 (inverse variance weighted) “a” denotes a p-value less than 0.05 (inverse variance weighted) but not lower than Bonferroni thresholds. “b” indicates that the results from the inverse variance weighted method differ in direction from MR-Egger or weighted median methods, suggesting a nominal rather than substantial association. |
Anxiety disorders were associated with migraine and migraine without aura. Depression was associated with recent stomach or abdominal pain. Schizophrenia showed associations with multiple pain phenotypes, including facial pain, neck or shoulder pain, stomach or abdominal pain, and headache, with differing patterns between recent and chronic headache. Anxiety or social phobia was associated with trigeminal neuralgia. No evidence was found for effects of personality disorders on pain outcomes.
Associations with suicide or intentional self-harm with mental disorders (SOIH-MD).
Several pain conditions—including migraine, trigeminal neuralgia, recent knee pain, neck or shoulder pain, and stomach or abdominal pain—were associated with an increased risk of SOIH-MD. Conversely, SOIH-MD showed a modest association with recent stomach or abdominal pain (Figure 6 and Supplemental Table 11).
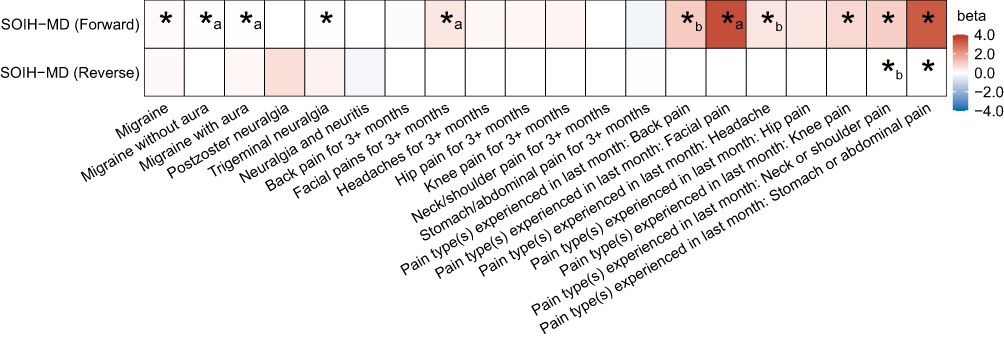 |
Figure 6 Forward and Reversed Mendelian Randomization analysis the causal effect of Pain on Suicide or other Intentional self-harm for any mental disorder (SOIH−MD) A positive beta value is indicated in red, while a negative beta value is indicated in blue, with the color intensity increasing as the absolute value of beta becomes larger. “*” represents a significance level of P < 0.05 (inverse variance weighted) “a” denotes a p-value less than 0.05 (inverse variance weighted) but not lower than Bonferroni thresholds. “b” indicates that the results from the inverse variance weighted method differ in direction from MR-Egger or weighted median methods, suggesting a nominal rather than substantial association. |
Sensitivity Analyses
Heterogeneity was observed in several analyses and was addressed using random-effects IVW models. Outlier variants identified by MR-PRESSO did not materially influence the results, and MR-Egger intercepts provided no strong evidence for directional pleiotropy (Supplemental Table 12). Leave-one-out analyses confirmed the robustness of the findings (Supplemental Figures 2–5).
MRlap analyses indicated that sample overlap affected some estimates; therefore, corrected results were adopted where appropriate and were largely consistent with the primary analyses (Supplemental Tables 6–13). Power was adequate for most associations, although limited for some rare pain–disorder pairs, warranting cautious interpretation (Figure 7).
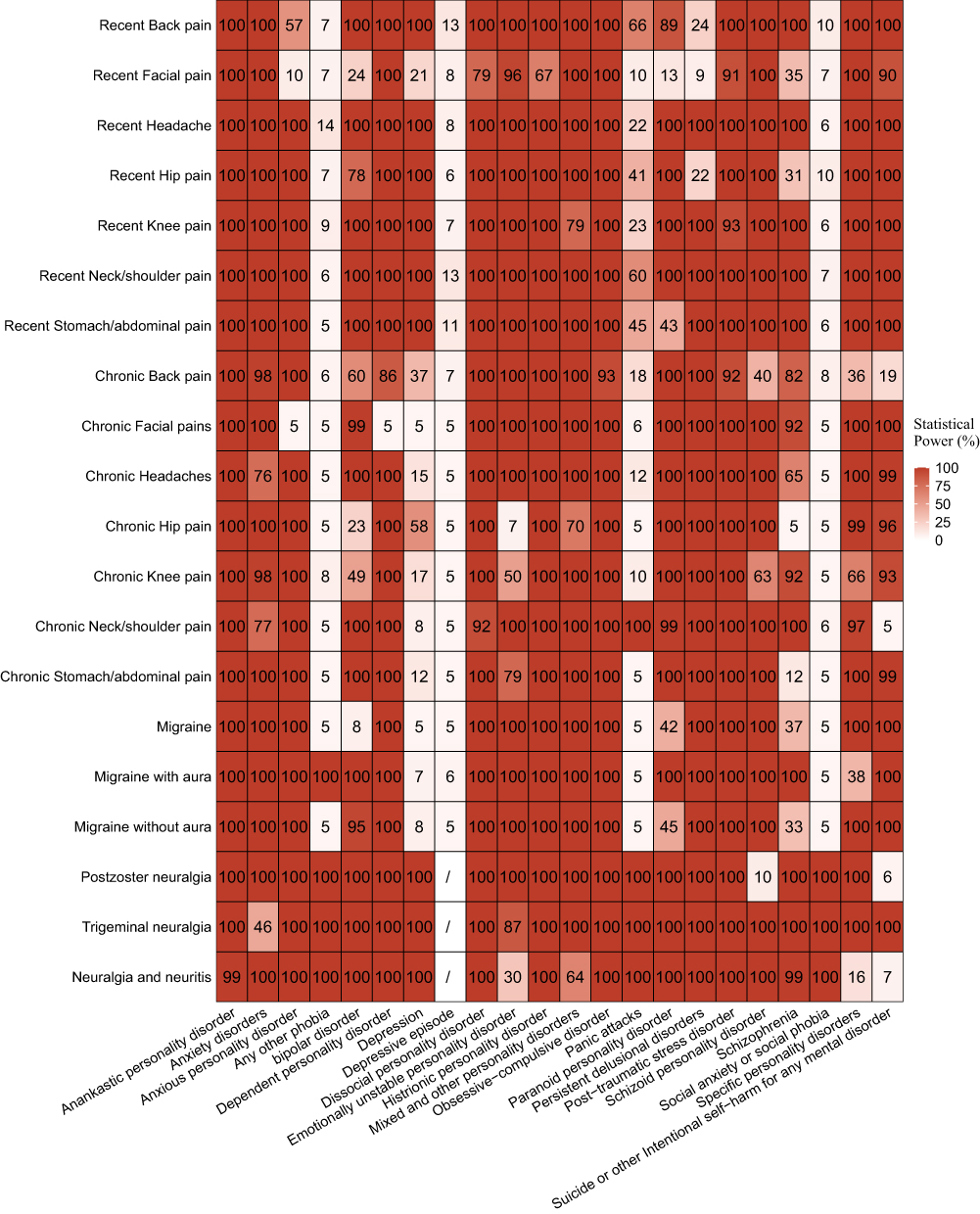 |
Figure 7 Heatmap of the statistical power for the Mendelian randomization (MR) analysis.The intensity of red color indicates the level of statistical power, with darker shades representing higher power. |
In MVMR analyses, most associations remained stable after adjustment for insomnia, obesity, and substance abuse. However, obesity and substance abuse attenuated several associations involving migraine, trigeminal neuralgia, and SOIH-MD, suggesting potential mediating or confounding effects (Table 2).
 |
Table 2 Results of Multivariate Mendelian randomization |
MVMR Analyses
All exposure–outcome pairs showing significant associations in both forward and reverse UVMR analyses were further evaluated using MVMR, with insomnia, obesity, and substance abuse included as potential confounders (Table 2).
Overall, most associations remained robust after multivariable adjustment, indicating that the observed effects were largely independent of these common comorbid conditions. However, several associations were attenuated after adjustment. Specifically, substance abuse diminished the association between recent neck or shoulder pain and SOIH-MD. Adjustment for obesity abolished the associations of migraine and trigeminal neuralgia with anxious personality disorder and SOIH-MD. In addition, substance abuse attenuated the association between trigeminal neuralgia and SOIH-MD.
Due to evidence of pleiotropy in the MR-Egger test, the multivariable estimate for schizophrenia and recent neck or shoulder pain should be interpreted with caution (Supplemental Table 14).
Discussion
The interaction between physical pain and psychological health has long attracted sustained interest from both researchers and clinicians. Nevertheless, much of the existing evidence has been derived from preclinical or observational studies, which are inherently limited by interspecies differences, suboptimal study design, and residual confounding. Prior work has focused predominantly on common psychiatric conditions such as depression and anxiety,56,57 with relatively little attention paid to broader diagnostic spectra, including personality disorders. The application of MR offers an opportunity to move beyond correlation by leveraging genetic liability as a proxy for lifelong exposure. Using this framework, the present study provides genetic evidence linking multiple recent and chronic pain phenotypes with a wide range of psychiatric and personality disorders, while MVMR further clarifies the extent to which these relationships are independent of major comorbid risk factors.
Compared with previous investigations,56–63 our study is distinguished by its breadth and granularity. We examined both recent and chronic pain, capturing different temporal dimensions of pain experience, and extended the analysis to specific pain phenotypes such as migraine and neuropathic pain. These distinctions are clinically relevant, as different pain types may engage partially distinct biological and psychological mechanisms. Consistent with prior literature,64–66 headache-related phenotypes showed robust associations with several psychiatric outcomes. Notably, migraine liability was linked to anxiety-related and personality disorder traits, in line with reports of elevated emotional and behavioral problems among individuals with migraine,64,67. In contrast, we did not observe strong evidence linking migraine with depression, which may reflect limited statistical power in available migraine GWAS data or the complex confounding structures present in epidemiological studies of migraine and mood disorders.
The psychiatric datasets used in this study were derived from large, well-characterized sources, with diagnoses based on professional assessment or strict ICD criteria. This enhances the reliability and generalizability of our findings within populations of European ancestry. Although some exposure–outcome pairs were derived from overlapping samples, correction using MRlap indicated that most forward associations were robust to sample overlap. Where overlap substantially influenced estimates, corrected results suggested that conventional inverse-variance–weighted estimates tended to underestimate effect sizes, underscoring the importance of addressing this issue in future MR research.
While depression and anxiety remain the most commonly studied psychiatric correlates of pain,56,57,68–70 our analyses extended to a broader spectrum of mental disorders and their subtypes. Anxiety disorders, for example, encompass clinically and biologically heterogeneous conditions, including generalized anxiety disorder, panic disorder, social anxiety disorder, and PTSD.68,71 By examining these categories separately where data permitted, our study provides a more nuanced view of how distinct pain phenotypes relate to different psychiatric profiles. Nevertheless, limited sample sizes for certain subtypes constrained precision, and heterogeneity within diagnostic categories cannot be excluded.
We also explored links between pain phenotypes and self-harm or suicide-related outcomes. Genetic liability to migraine, knee pain, neck–shoulder pain, and abdominal pain was associated with increased risk of self-harm or suicidal tendencies. In certain individuals, cognitive disruptions seem to lead to a preference for experiencing acute physical pain rather than constructing emotional pain memories,72,73 potentially contributing to self-harming or even suicidal behaviors.74–76
Our study extends existing MR research by examining the relationship between pain and personality disorders, an area that has received relatively limited causal investigation to date. Personality disorders are known to adversely affect clinical course and treatment outcomes and have been associated with increased risks of premature mortality and suicide.77–79 Previous observational studies have reported a higher prevalence of personality disorders among individuals with pain compared with the general population.78,80,81 By evaluating genetic liability across multiple pain phenotypes and personality disorder categories, our analyses provide additional evidence supporting a non-random co-occurrence between these conditions. Rather than implying direct clinical translation, these findings highlight the potential for shared biological or behavioral pathways linking pain and personality traits, and underscore the need for further mechanistic and longitudinal studies to clarify directionality, specificity, and clinical relevance.
The observed reciprocal patterns between pain and psychiatric traits align with epidemiological evidence demonstrating frequent co-occurrence of these conditions. A representative annual survey of self-reported health status and treatment utilization in the United States showed that approximately 12 million American adults concurrently suffer from chronic pain and anxiety/depressive symptoms.11 Furthermore, a study with a sample size of 2,358 participants demonstrated that major depression is also prospectively associated with back pain at follow-up.82 Another study covering 48,007 individuals revealed that participants diagnosed with spinal pain were 1.41 times more likely to be diagnosed with new-onset depression than age- and sex-matched non-diagnosed individuals, while those newly diagnosed with depression were 1.28 times more likely to develop spinal pain compared to their age- and sex-matched counterparts without the diagnosis.83 Multiple studies have reported increased rates of anxiety disorders among patients with abdominal pain, migraines, pelvic pain, and arthritis.11,84–86 Individuals with migraines were more likely to be diagnosed with anxiety disorders than those without migraines, and conversely, individuals with anxiety were likely to experience migraines compared to those without anxiety.87–89
These research findings partially align with our own study results, supporting the idea of shared neurobiological mechanisms between pain and mental disorders. These mechanisms may involve factors such as corticotropin-releasing factor, endorphins, the hypothalamic-pituitary-adrenal axis, increased activation of the noradrenergic stress pathway, heightened amygdala reactivity, and the involvement of gut microbiota.90–93 Moreover, neuroimaging studies also support the bidirectional relationship between pain and mental disorders. Functional imaging studies indicate that pain and depression or anxiety can activate overlapping brain regions associated with higher cognitive functions and emotional regulation, including the anterior cingulate cortex and prefrontal cortex.94–100 Finally, pain and mental disorders may also be mediated by shared genetic factors.92,101,102 Bahrami et al used a binary causality mixture model to evaluate and identify specific genetic loci shared among headaches, depression, and schizophrenia.103
Furthermore, our research findings suggest that the association between pain and mental or personality disorders may not only be influenced by genetic factors but also mediated by other non-genetic factors. For instance, our study results indicate that even for pain occurring in the same body region, recent pain is causally linked to a wider range of mental and personality disorders, unlike the common comorbidity between chronic pain and mental disorders.104,105 This difference is likely a result of the combined influence of various factors. The datasets we incorporated for recent pain may represent a more immediate and unadulterated experience of pain as it describes recent experiences of pain within the past month, as opposed to the description of pain persisting for three months in the case of chronic pain. Therefore, though genetic predictions suggest causal associations between recent pain and multiple mental and personality disorders, this relationship is more likely to be primarily mediated by other factors in the case of chronic pain. Pain experiences encompass multiple dimensions, including emotions, sensations, and cognition,105,106 and, as a result, pain is not merely a physiological response to external stimuli but is influenced by the complex interplay of biological, psychological, and social factors.107,108
Another important consideration is the heterogeneity within broad psychiatric categories. For example, “anxiety disorders” encompass clinically and biologically distinct conditions—including generalized anxiety disorder, social anxiety disorder, panic disorder, and specific phobias—that differ in their genetic architectures and underlying neurobiological mechanisms.109 Recent large-scale genetic studies have demonstrated that these subtypes do not share a uniform genetic background and may exhibit subtype-specific associations with other psychiatric traits. Evidence from multi-ancestry GWAS, epigenetic aging analyses, and subtype-focused studies further supports meaningful divergence among anxiety-related phenotypes.110 Although we included several subtypes where GWAS data were available, limited sample sizes reduced estimation precision and prevented robust characterization of subtype-specific causal effects. Therefore, heterogeneity in causal effects across different subtypes within the same diagnostic category cannot be excluded. Future MR studies based on larger, better-phenotyped, and subtype-specific GWAS datasets will be essential to disentangle these potentially distinct causal pathways.
A challenge in conducting MR studies in the field of mental disorders is the issue of pleiotropy in IVs.111 However, sensitivity analyses robust to pleiotropy,112 MVMR,113 and Steiger test47 can help exclude alternative explanations. In addition to sensitivity analyses and Steiger filtering, our study performed MVMR to estimate the direct effects of pain independent of other risk factors for mental disorders. The results showed that, in most cases, the effects of pain on mental disorders were independent of obesity, insomnia, and substance abuse, indicating that these findings are robust. However, in some instances, the causal effects of pain on mental disorders were influenced by obesity or substance abuse. This suggests that, for certain pain patients, such as those with migraines, allocating resources to treat obesity could mitigate the causal effects of migraines on increasing the risk of anxious personality disorder and SOIH-MD.
Likewise, the study results also reveal that according to the positive MR analyses, back pain, headaches, and neck-shoulder pain are causally associated with a broader range of mental and personality disorders relative to other types of pain. This finding implies that these mental or personality disorders may share a close association with back pain, headaches, and neck-shoulder pain at biological or psychological levels, possibly sharing certain neural mechanisms or risk factors.68 Simultaneously, it suggests that non-genetic factors may mediate the comorbidity of other specific types of pain and mental or personality disorders.56,114 This aligns with the findings of previous genetic studies quantifying the genetic correlation between depression and pain, revealing a significant common genetic structure between depression and headaches, neck-shoulder pain, and back pain, while being unrelated to facial, hip, or knee pain.115
Future research can build upon current discoveries by investigating the biological and neural mechanisms linking back pain, headaches, and neck-shoulder pain with mental or personality disorders. This includes studying shared neurotransmitter systems, inflammatory responses, and genetic regulation factors. It’s also important to consider the influence of psychosocial factors on these relationships and conduct long-term tracking and intervention studies to confirm the effectiveness of specific interventions in improving pain and mental well-being. By taking into account individual differences and environmental factors, fostering interdisciplinary collaboration among experts in biomedical sciences, psychology, neuroscience, and epidemiology will lead to a comprehensive understanding of the complex relationship between pain and mental health. Ultimately, this will contribute to the development of more effective intervention strategies and treatment approaches in clinical practice and precision medicine.
Additionally, it is noteworthy that, due to our strict adherence to multiple testing correction, some MR results showing associations between pain and psychiatric or personality disorders had p-values less than 0.05 but did not reach the Bonferroni correction threshold. Examples include the association between migraines and anxiety, chronic hip pain and depression, and chronic back pain and panic attacks. However, prior studies have already reported significant associations between these pains and corresponding mental disorders.116–118 This discrepancy may arise because while multiple testing corrections reduce Type I errors (the probability of incorrectly rejecting true effects), they might also increase Type II errors (the probability of failing to detect true effects).49,119,120 This also indicates that multiple testing corrections might not be universally applicable in certain exploratory studies,49,119,121 as these studies often lack specific hypotheses and aim to discover new associations or effects. Therefore, further research is needed to draw more definitive conclusions for the exposure-outcome pairs in our study where the p-values were less than 0.05 but did not meet the Bonferroni correction threshold.
Our findings also have important implications for clinical practice. The bidirectional causal associations identified between several pain phenotypes and specific mental disorders suggest that clinicians should adopt a more integrated approach when evaluating and managing patients presenting with either condition. For example, the robust causal link observed between headache and depressive or anxiety-related traits supports more proactive mental health screening in this population, as early recognition and timely psychological or pharmacological interventions may help prevent progression to more severe comorbid states. Conversely, given the causal effects of certain mental disorders on pain susceptibility, clinicians treating patients with mood or anxiety disorders may benefit from systematic assessment of pain symptoms, which may otherwise remain underrecognized. These results also highlight the potential value of multidisciplinary care models that incorporate both pain management and mental health services. In addition, the subtype-specific associations observed in our analysis indicate that future research should explore tailored intervention strategies targeting the shared neurobiological pathways linking distinct pain types with specific psychiatric conditions. Collectively, these insights may guide more precise risk stratification, inform preventive strategies, and stimulate the development of personalized therapeutic approaches.
This study presents certain limitations that require careful consideration. Firstly, the study datasets comprised individuals of European ancestry. Therefore, caution must be exercised when extrapolating the results to other ancestral backgrounds, and future analyses based on more diverse or locally derived GWAS datasets will be essential to validate the transferability of these causal estimates. Additionally, the issue of sample overlap arises when the exposure and outcome datasets originate from the same database. To address this, we employed the MRlap method to correct for estimation bias due to sample overlap. The results indicated that sample overlap did not affect the robustness of most forward MR findings. Secondly, although we performed multiple pleiotropy-robust sensitivity analyses— including MR-Egger, weighted-median estimators, MR-PRESSO, Steiger filtering, leave-one-out tests, and MVMR—there remains the possibility of residual or unmeasured horizontal pleiotropy. Such complex genetic pathways cannot be fully excluded by current methods, and some causal estimates may therefore still be influenced by biological mechanisms not captured by our instruments. Thirdly, the datasets utilized binary variables and lacked stratified analyses by pain intensity or the severity of mental and personality disorders. This limitation may materially influence causal effect estimates and increase the risk of false-negative findings, as pain intensity and psychiatric severity are likely to exert dose-dependent effects on both pain perception and psychiatric vulnerability.105,122,123 Finally, some of the datasets we included have relatively small sample sizes, which may have led to lower statistical power in the analysis of the exposure–outcome MR relationships, such as between chronic headache and depression or depressive episodes. This could also explain why certain pain conditions reportedly associated with mental disorders in previous studies did not demonstrate significant causal relationships in our research. Additionally, not all nominally significant findings were supported by adequate statistical power. Several exposure–outcome pairs, including those involving depressive episodes in relation to recent back pain, facial pain, headache, neck or shoulder pain, and stomach or abdominal pain, had statistical power below 80%. Moreover, the associations between recent headache and any other phobia (power = 14%) and between trigeminal neuralgia and anxiety disorders (power = 46%) were particularly underpowered. These estimates are therefore less reliable and should be interpreted cautiously as hypothesis-generating signals rather than definitive causal effects.
Conclusion
This study aimed to clarify the bidirectional causal relationships between multiple pain phenotypes and a broad spectrum of mental disorders. We hypothesized that genetic liability to pain would increase the risk of specific psychiatric disorders, and that certain mental disorders might also exert causal effects on pain susceptibility. Using bidirectional and multivariable Mendelian randomization, our findings largely corroborate these hypotheses, demonstrating robust and pain-type–specific effects of pain on mental disorders, alongside more limited, phenotype-dependent reverse effects that were partly independent of obesity, insomnia, and substance-use pathways.
By explicitly establishing the directionality and relative independence of these associations, this study fulfills its research aim and extends existing observational evidence. Importantly, the results have clear clinical implications: patients presenting with specific pain phenotypes may benefit from targeted screening for psychiatric symptoms, while systematic assessment of pain should be considered in patients with mental disorders. Furthermore, the heterogeneity observed across pain types and psychiatric outcomes supports the development of more personalized and mechanism-based prevention and treatment strategies, enabling earlier risk stratification and more integrated management of pain–psychiatric comorbidity.
Abbreviations
MR, Mendelian randomization; IVW, Inverse-variance weighted; SNP, Single nucleotide polymorphism; IV, Instrumental variables; GWAS, Genome-wide association study; MRC-IEU, Council Integrative Epidemiology Unit; PGC, Psychiatric Genomics Consortium; SOIH−MD, suicide or other Intentional self-harm for any mental disorder; LD, Linkage disequilibrium; OR, Odds ratio; CIs, Confidence intervals; ICD, International Classification of Diseases;
PTSD, post-traumatic stress disorder.
Data Sharing Statement
All data were available in IEU open GWAS project (https://gwas.mrcieu.ac.uk/). The process of registration and login is not necessary.
Ethics Approval and Consent to Participate
This study was conducted using summary-level genetic association data obtained from publicly available genome-wide association studies (GWAS). No individual-level data were accessed, and all data were fully anonymized. According to the Measures for the Ethical Review of Life Science and Medical Research Involving Human Subjects issued by the National Health Commission of the People’s Republic of China on February 18, 2023, this study meets the criteria for exemption from ethical review under Article 32, Items (1) and (2), which stipulate that ethical approval may be waived for research that (1) uses legally obtained public data or data generated through observation of public behavior without interference, and (2) uses anonymized information data.
Therefore, this study was exempt from review by an Institutional Review Board or local ethics committee, and informed consent was not required for this secondary analysis of publicly available, anonymized data.
Acknowledgments
We appreciate the work of UK Biobank, FinnGen, Neale Lab, Medical Research Council Integrative Epidemiology Unit (MRC-IEU), and Psychiatric Genomics Consortium (PGC).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Vos T, Lim SS, Abbafati C, et.al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–26. doi:10.1016/S0140-6736(20)30925-9
2. Mackey S, Kao MC. Managing twin crises in chronic pain and prescription opioids. BMJ. 2019;364:l917. doi:10.1136/bmj.l917
3. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
4. Rometsch C, Martin A, Junne F, Cosci F. Chronic pain in European adult populations: a systematic review of prevalence and associated clinical features. Pain. 2025;166(4):719–731. doi:10.1097/j.pain.0000000000003406
5. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
6. Aaron RV, Ravyts SG, Carnahan ND, et al. Prevalence of depression and anxiety among adults with chronic pain: a systematic review and meta-analysis. JAMA Netw Open. 2025;8(3):e250268. doi:10.1001/jamanetworkopen.2025.0268
7. Navratilova E, Porreca F. Reward and motivation in pain and pain relief. Nat Neurosci. 2014;17(10):1304–1312. doi:10.1038/nn.3811
8. Phelps CE, Navratilova E, Porreca F. Cognition in the chronic pain experience: preclinical insights. Trends Cognit Sci. 2021;25(5):365–376. doi:10.1016/j.tics.2021.01.001
9. Farmer MA, Baliki MN, Apkarian AV. A dynamic network perspective of chronic pain. Neurosci Lett. 2012;520(2):197–203. doi:10.1016/j.neulet.2012.05.001
10. Cauda F, Palermo S, Costa T, et al. Gray matter alterations in chronic pain: a network-oriented meta-analytic approach. Neuroimage Clin. 2014;4:676–686. doi:10.1016/j.nicl.2014.04.007
11. JS DLR, Brady BR, Ibrahim MM, et al. Co-occurrence of chronic pain and anxiety/depression symptoms in U.S. adults: prevalence, functional impacts, and opportunities. Pain. 2024;165(3):666–673. doi:10.1097/j.pain.0000000000003056
12. Kan R, Padberg F, Giron CG, et al. Effects of repetitive transcranial magnetic stimulation of the left dorsolateral prefrontal cortex on symptom domains in neuropsychiatric disorders: a systematic review and cross-diagnostic meta-analysis. Lancet Psychiatry. 2023;10(4):252–259. doi:10.1016/S2215-0366(23)00026-3
13. Fornito A, Zalesky A, Bullmore ET. Network scaling effects in graph analytic studies of human resting-state FMRI data. Front Syst Neurosci. 2010;4:22. doi:10.3389/fnsys.2010.00022
14. Bullmore E, Sporns O. Complex brain networks: graph theoretical analysis of structural and functional systems. Nat Rev Neurosci. 2009;10(3):186–198. doi:10.1038/nrn2575
15. Vachon-Presseau E, Centeno MV, Ren W, et al. The emotional brain as a predictor and amplifier of chronic pain. J Dent Res. 2016;95(6):605–612. doi:10.1177/0022034516638027
16. Yarns BC, Cassidy JT, Jimenez AM. At the intersection of anger, chronic pain, and the brain: a mini-review. Neurosci Biobehav Rev. 2022;135:104558. doi:10.1016/j.neubiorev.2022.104558
17. Geha PY, Baliki MN, Harden RN, Bauer WR, Parrish TB, Apkarian AV. The brain in chronic CRPS pain: abnormal gray-white matter interactions in emotional and autonomic regions. Neuron. 2008;60(4):570–581. doi:10.1016/j.neuron.2008.08.022
18. May A. Chronic pain may change the structure of the brain. Pain. 2008;137(1):7–15. doi:10.1016/j.pain.2008.02.034
19. Zhang W, Cheng Z, Fu F, Zhan Z. Prevalence and clinical characteristics of white matter hyperintensities in Migraine: a meta-analysis. Neuroimage Clin. 2023;37:103312. doi:10.1016/j.nicl.2023.103312
20. Harris RE, Clauw DJ, Scott DJ, McLean SA, Gracely RH, Zubieta JK. Decreased central mu-opioid receptor availability in fibromyalgia. J Neurosci. 2007;27(37):10000–10006. doi:10.1523/JNEUROSCI.2849-07.2007
21. Wood PB, Patterson JC 2nd, Sunderland JJ, Tainter KH, Glabus MF, Lilien DL. Reduced presynaptic dopamine activity in fibromyalgia syndrome demonstrated with positron emission tomography: a pilot study. J Pain. 2007;8(1):51–58. doi:10.1016/j.jpain.2006.05.014
22. Kuner R, Kuner T. Cellular circuits in the brain and their modulation in acute and chronic pain. Physiol Rev. 2021;101(1):213–258. doi:10.1152/physrev.00040.2019
23. Labrakakis C. The role of the insular cortex in pain. Int J Mol Sci. 2023;24(6):5736. doi:10.3390/ijms24065736
24. van Rijswijk SM, van Beek M, Schoof GM, et al. Iatrogenic opioid use disorder, chronic pain and psychiatric comorbidity: a systematic review. Gen Hosp Psychiatry. 2019;59:37–50. doi:10.1016/j.genhosppsych.2019.04.008
25. Proctor SL, Estroff TW, Empting LD, Shearer-Williams S, Hoffmann NG. Prevalence of substance use and psychiatric disorders in a highly select chronic pain population. J Addict Med. 2013;7(1):17–24. doi:10.1097/ADM.0b013e3182738655
26. Wilsey BL, Fishman SM, Tsodikov A, Ogden C, Symreng I, Ernst A. Psychological comorbidities predicting prescription opioid abuse among patients in chronic pain presenting to the emergency department. Pain Med. 2008;9(8):1107–1117. doi:10.1111/j.1526-4637.2007.00401.x
27. Bravo L, Llorca-Torralba M, Suárez-Pereira I, Berrocoso E. Pain in neuropsychiatry: insights from animal models. Neurosci Biobehav Rev. 2020;115:96–115. doi:10.1016/j.neubiorev.2020.04.029
28. Moore A, Fisher E, Eccleston C. Flawed, futile, and fabricated-features that limit confidence in clinical research in pain and anaesthesia: a narrative review. Br J Anaesth. 2023;130(3):287–295. doi:10.1016/j.bja.2022.09.030
29. Barroso J, Branco P, Apkarian AV. Brain mechanisms of chronic pain: critical role of translational approach. Transl Res. 2021;238:76–89. doi:10.1016/j.trsl.2021.06.004
30. Kachuri L, Saarela O, Bojesen SE, et al. Mendelian Randomization and mediation analysis of leukocyte telomere length and risk of lung and head and neck cancers. Int J Epidemiol. 2019;48(3):751–766. doi:10.1093/ije/dyy140
31. Sanderson E, Glymour MM, Holmes MV, et al. Mendelian randomization. Nat Rev Meth Primers. 2022:2. doi:10.1038/s43586-021-00092-5.
32. Birney E. Mendelian randomization. Cold Spring Harb Perspect Med. 2022;12(4). doi:10.1101/cshperspect.a041302
33. Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318:1925–1926. doi:10.1001/jama.2017.17219
34. Richmond RC, Davey Smith G. Mendelian randomization: concepts and scope. Cold Spring Harb Perspect Med. 2022;12:a040501. doi:10.1101/cshperspect.a040501
35. Skrivankova VW, Richmond RC, Woolf B, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
36. Davey Smith G, Hemani G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum Mol Genet. 2014;23:R89–98. doi:10.1093/hmg/ddu328
37. Larsson SC, Butterworth AS, Burgess S. Mendelian randomization for cardiovascular diseases: principles and applications. Eur Heart J. 2023;44:4913–4924. doi:10.1093/eurheartj/ehad736
38. Mukamal KJ, Stampfer MJ, Rimm EB. Genetic instrumental variable analysis: time to call mendelian randomization what it is. The example of alcohol and cardiovascular disease. Eur J Epidemiol. 2020;35:93–97. doi:10.1007/s10654-019-00578-3
39. Chen LG, Tubbs JD, Liu Z, Thach TQ, Sham PC. Mendelian randomization: causal inference leveraging genetic data. Psychol Med. 2024;54(8):1461–1474. doi:10.1017/S0033291724000321
40. Zhang H. Pros and cons of Mendelian randomization. Fertil Steril. 2023;119(6):913–916. doi:10.1016/j.fertnstert.2023.03.029
41. Nguyen K, Mitchell BD. A guide to understanding mendelian randomization studies. Arthritis Care Res. 2024;76(11):1451–1460. doi:10.1002/acr.25400
42. Wang Y, Qian W, Sun H, Zhao J, Mu M, Yang Z. Identify key environmental factors and neglected genetic SNPs associated with obsessive-compulsive disorder by two-sample multivariate Mendelian randomization analysis. J Affect Disord. 2026;392:120181. doi:10.1016/j.jad.2025.120181
43. Xu X, Yu H, Yang M, et al. Unraveling the relationship between obstructive sleep apnea and osteoarthritis: a multivariate mendelian randomization highlighting the role of BMI as a confounding factor. Exp Gerontol. 2025;199:112657. doi:10.1016/j.exger.2024.112657
44. Yu N, Wang J, Liu Y, Guo Y. Multivariate Mendelian randomization provides no evidence for causal associations among both psoriasis and psoriatic arthritis, and skin cancer. Front Immunol. 2023;14:1252720. doi:10.3389/fimmu.2023.1252720
45. Trubetskoy V, Pardiñas AF, Qi T, et al. Mapping genomic loci implicates genes and synaptic biology in schizophrenia. Nature. 2022;604:502–508. doi:10.1038/s41586-022-04434-5
46. Stahl EA, Breen G, Forstner AJ, et al. Genome-wide association study identifies 30 loci associated with bipolar disorder. Nat Genet. 2019;51:793–803. doi:10.1038/s41588-019-0397-8
47. Carter AR, Sanderson E, Hammerton G, et al. Mendelian randomisation for mediation analysis: current methods and challenges for implementation. Eur J Epidemiol. 2021;36(5):465–478. doi:10.1007/s10654-021-00757-1
48. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
49. Keselman HJ, Cribbie R, Holland B. Controlling the rate of Type I error over a large set of statistical tests. Br J Math Stat Psychol. 2002;55(Pt 1):27–39. doi:10.1348/000711002159680
50. Mounier N, Kutalik Z. Bias correction for inverse variance weighting Mendelian randomization. Genet Epidemiol. 2023;47:314–331. doi:10.1002/gepi.22522
51. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32:377–389. doi:10.1007/s10654-017-0255-x
52. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
53. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44:512–525. doi:10.1093/ije/dyv080
54. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50:693–698. doi:10.1038/s41588-018-0099-7
55. Brion MJ, Shakhbazov K, Visscher PM. Calculating statistical power in Mendelian randomization studies. Int J Epidemiol. 2013;42:1497–1501. doi:10.1093/ije/dyt179
56. Tang B, Meng W, Hägg S, Burgess S, Jiang X. Reciprocal interaction between depression and pain: results from a comprehensive bidirectional Mendelian randomization study and functional annotation analysis. Pain. 2022;163(1):e40–e48. doi:10.1097/j.pain.0000000000002305
57. Yao C, Zhang Y, Lu P, et al. Exploring the bidirectional relationship between pain and mental disorders: a comprehensive Mendelian randomization study. J Headache Pain. 2023;24(1):82. doi:10.1186/s10194-023-01612-2
58. Xiang Y, Song J, Liang Y, Sun J, Zheng Z. Causal relationship between psychiatric traits and temporomandibular disorders: a bidirectional two-sample Mendelian randomization study. Clin Oral Investig. 2023;27(12):7513–7521. doi:10.1007/s00784-023-05339-x
59. Li WW, Zhang JX, Wang J, Chen YQ, Lai S, Qiu ZK. Bidirectional two-sample Mendelian randomization analysis identifies causal associations between migraine and five psychiatric disorders. Front Neurol. 2024;15:1432966. doi:10.3389/fneur.2024.1432966
60. Zhao SS, Holmes MV, Alam U. Disentangling the relationship between depression and chronic widespread pain: a Mendelian randomisation study. Semin Arthritis Rheum. 2023;60:152188. doi:10.1016/j.semarthrit.2023.152188
61. Meng J, Cai Y, Yao J, Yan H. Bidirectional causal relationship between psychiatric disorders and osteoarthritis: a univariate and multivariate Mendelian randomization study. Brain Behav. 2024;14(2):e3429. doi:10.1002/brb3.3429
62. Liu R, Liu Q, Xu S, Mei R. Mood instability and low back pain: a mendelian randomization study. Front Neurol. 2023;14:1252329. doi:10.3389/fneur.2023.1252329
63. Lv X, Xu B, Tang X, et al. The relationship between major depression and migraine: a bidirectional two-sample Mendelian randomization study. Front Neurol. 2023;14:1143060. doi:10.3389/fneur.2023.1143060
64. Hommer R, Lateef T, He JP, Merikangas K. Headache and mental disorders in a nationally representative sample of American youth. Eur Child Adolesc Psychiatry. 2022;31(1):39–49. doi:10.1007/s00787-020-01599-0
65. Klan T, Bräscher AK, Klein S, et al. Assessing attack-related fear in headache disorders-structure and psychometric properties of the fear of attacks in migraine inventory. Headache. 2022;62(3):294–305. doi:10.1111/head.14272
66. Saunders K, Merikangas K, Low NC, Von Korff M, Kessler RC. Impact of comorbidity on headache-related disability. Neurology. 2008;70(7):538–547. doi:10.1212/01.wnl.0000297192.84581.21
67. Lateef T, He JP, Nelson K, Calkins ME, Gur R, Merikangas KR. Physical-mental comorbidity of pediatric migraine in the philadelphia neurodevelopmental cohort. J Pediatr. 2019;205:210–217. doi:10.1016/j.jpeds.2018.09.033
68. Hooten WM. Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. 2016;91(7):955–970. doi:10.1016/j.mayocp.2016.04.029
69. Cato B. Shared pain. Nature. 2021. doi:10.1038/d41586-021-02432-7
70. Velly AM, Mohit S. Epidemiology of pain and relation to psychiatric disorders. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):159–167. doi:10.1016/j.pnpbp.2017.05.012
71. Leichsenring F, Heim N, Steinert C. A review of anxiety disorders. JAMA. 2023;329(15):1315–1316. doi:10.1001/jama.2023.2428
72. Yamin JB, Meints SM, Pester BD, et al. Childhood abuse and health outcomes in patients with fibromyalgia: a cross-sectional exploratory study of the moderating effects of pain catastrophizing and mindfulness. BMC Musculoskelet Disord. 2025;26(1):195. doi:10.1186/s12891-025-08449-7
73. Sieberg CB, Lebel A, Silliman E, Holmes S, Borsook D, Elman I. Left to themselves: time to target chronic pain in childhood rare diseases. Neurosci Biobehav Rev. 2021;126:276–288. doi:10.1016/j.neubiorev.2021.03.008
74. Kirtley OJ, Rodham K, Crane C. Understanding suicidal ideation and behaviour in individuals with chronic pain: a review of the role of novel transdiagnostic psychological factors. Lancet Psychiatry. 2020;7(3):282–290. doi:10.1016/S2215-0366(19)30288-3
75. Pakniyat-Jahromi S, Korenis P, Sher L. Pain and suicide: what should we tell our trainees. Acta Neuropsychiatr. 2022;34(3):127–131. doi:10.1017/neu.2021.46
76. Themelis K, Gillett JL, Karadag P, et al. Mental defeat and suicidality in chronic pain: a prospective analysis. J Pain. 2023;24(11):2079–2092. doi:10.1016/j.jpain.2023.06.017
77. Tyrer P, Reed GM, Crawford MJ. Classification, assessment, prevalence, and effect of personality disorder. Lancet. 2015;385(9969):717–726. doi:10.1016/S0140-6736(14)61995-4
78. Bax OK, Chartonas D, Parker J, Symniakou S, Lee T. Personality disorder. BMJ. 2023;382:e050290. doi:10.1136/bmj-2019-050290
79. Newton-Howes G, Austin S, Foulds J. The prevalence of personality disorder in mental state disorder. Curr Opin Psychiatry. 2022;35(1):45–52. doi:10.1097/YCO.0000000000000761
80. Stein AG, Johnson BN, Kelly AG, Cheavens JS, McKernan LC. Negative affect and pain catastrophizing link borderline personality disorder to pain: replicating and extending the borderline personality disorder-pain association. Personal Disord. 2026;16(2):173–183. doi:10.1037/per0000704
81. Boni M, Ciaramella A. Role of personality and psychiatric disorders in the perception of pain. Psychiatr Q. 2023;94(2):297–310. doi:10.1007/s11126-023-10026-x
82. Yang H, Hurwitz EL, Li J, et al. Bidirectional comorbid associations between back pain and major depression in US adults. Int J Environ Res Public Health. 2023;20(5):4217. doi:10.3390/ijerph20054217
83. Thériault FL, Momoli F, Hawes RA, Garber BG, Gardner W, Colman I. Spinal pain and major depression in a military cohort: bias analysis of dependent misclassification in electronic medical records. Soc Psychiatry Psychiatr Epidemiol. 2022;57(3):575–581. doi:10.1007/s00127-021-02160-3
84. Ploutarchou G, Savva C, Karagiannis C, Pavlou K, O’Sullivan K, Korakakis V. The effectiveness of cognitive behavioural therapy in chronic neck pain: a systematic review with meta-analysis. Cogn Behav Ther. 2023;52(5):523–563. doi:10.1080/16506073.2023.2236296
85. He YY, Ding KR, Tan WY, et al. The role of depression and anxiety in the relationship between arthritis and cognitive impairment in Chinese older adults. Am J Geriatr Psychiatry. 2024;32(7):856–866. doi:10.1016/j.jagp.2024.01.228
86. Vargas-Costales JA, Rosero C, Mazin SC, et al. Prevalence of chronic pelvic pain and associated factors among indigenous women of reproductive age in Ecuador. BMC Womens Health. 2024;24(1):388. doi:10.1186/s12905-024-03189-7
87. Onofri A, Pensato U, Rosignoli C, et al. Primary headache epidemiology in children and adolescents: a systematic review and meta-analysis. J Headache Pain. 2023;24(1):8. doi:10.1186/s10194-023-01541-0
88. Stovner LJ, Hagen K, Linde M, Steiner TJ. The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J Headache Pain. 2022;23(1):34. doi:10.1186/s10194-022-01402-2
89. Zhao Y, Yi Y, Zhou H, Pang Q, Wang J. The burden of migraine and tension-type headache in Asia from 1990 to 2021. J Headache Pain. 2025;26(1):49. doi:10.1186/s10194-025-01990-9
90. Michaelsen MM, Esch T. Motivation and reward mechanisms in health behavior change processes. Brain Res. 2021;1757:147309. doi:10.1016/j.brainres.2021.147309
91. Kim DJ, Jassar H, Lim M, Nascimento TD, DaSilva AF. Dopaminergic regulation of reward system connectivity underpins pain and emotional suffering in migraine. J Pain Res. 2021;14:631–643. doi:10.2147/JPR.S296540
92. Vieira WF, Coelho D, Litwiler ST, et al. Neuropathic pain, mood, and stress-related disorders: a literature review of comorbidity and co-pathogenesis. Neurosci Biobehav Rev. 2024;161:105673. doi:10.1016/j.neubiorev.2024.105673
93. Zhang Y, Ma H, Bai Y, et al. Chronic neuropathic pain and comorbid depression syndrome: from neural circuit mechanisms to treatment. ACS Chem Neurosci. 2024;15(13):2432–2444. doi:10.1021/acschemneuro.4c00125
94. Luo J, Zhu HQ, Gou B, Wang XQ. Neuroimaging assessment of pain. Neurotherapeutics. 2022;19(5):1467–1488. doi:10.1007/s13311-022-01274-z
95. Davidson RJ, Abercrombie H, Nitschke JB, Putnam K. Regional brain function, emotion and disorders of emotion. Curr Opin Neurobiol. 1999;9(2):228–234. doi:10.1016/S0959-4388(99)80032-4
96. Rosen SD, Paulesu E, Frith CD, et al. Central nervous pathways mediating angina pectoris. Lancet. 1994;344(8916):147–150. doi:10.1016/S0140-6736(94)92755-3
97. Hsieh JC, Hannerz J, Ingvar M. Right-lateralised central processing for pain of nitroglycerin-induced cluster headache. Pain. 1996;67(1):59–68. doi:10.1016/0304-3959(96)03066-7
98. Hashmi JA, Baliki MN, Huang L, et al. Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain. 2013;136(Pt 9):2751–2768. doi:10.1093/brain/awt211
99. Berman SM, Naliboff BD, Suyenobu B, et al. Reduced brainstem inhibition during anticipated pelvic visceral pain correlates with enhanced brain response to the visceral stimulus in women with irritable bowel syndrome. J Neurosci. 2008;28(2):349–359. doi:10.1523/JNEUROSCI.2500-07.2008
100. Baliki MN, Chialvo DR, Geha PY, et al. Chronic pain and the emotional brain: specific brain activity associated with spontaneous fluctuations of intensity of chronic back pain. J Neurosci. 2006;26(47):12165–12173. doi:10.1523/JNEUROSCI.3576-06.2006
101. Cruz-Almeida Y, Tamargo J, Strath LJ. Epigenetic Aging: a socio-biological link to chronic pain. J Pain. 2024;25(2):572–573. doi:10.1016/j.jpain.2023.11.007
102. Krause S, Torok D, Bagdy G, Juhasz G, Gonda X. Genome-wide by trait interaction analyses with neuroticism reveal chronic pain-associated depression as a distinct genetic subtype. Transl Psychiatry. 2025;15(1):108. doi:10.1038/s41398-025-03331-5
103. Bahrami S, Hindley G, Winsvold BS, et al. Dissecting the shared genetic basis of migraine and mental disorders using novel statistical tools. Brain. 2022;145(1):142–153. doi:10.1093/brain/awab267
104. Goesling J, Lin LA, Clauw DJ. Psychiatry and pain management: at the intersection of chronic pain and mental health. Curr Psychiatry Rep. 2018;20(2):12. doi:10.1007/s11920-018-0872-4
105. Bhatt K, Palomares AC, Jutila L, Rohde I, Forget P. Societal Impact of Pain Platform (SIP). The pain and mental health comorbidity. Epidemiol Psychiatr Sci. 2024;33e46. doi:10.1017/S204579602400057X
106. Porreca F, Navratilova E. Reward, motivation, and emotion of pain and its relief. Pain. 2017;158(Suppl 1):S43–S49. doi:10.1097/j.pain.0000000000000798
107. Gilam G, Gross JJ, Wager TD, Keefe FJ, Mackey SC. What is the relationship between pain and emotion? bridging constructs and communities. Neuron. 2020;107(1):17–21. doi:10.1016/j.neuron.2020.05.024
108. Yuan Y, Schreiber K, Flowers KM, et al. The relationship between emotion regulation and pain catastrophizing in patients with chronic pain. Pain Med. 2024;25(7):468–477. doi:10.1093/pm/pnae009
109. Ohi K, Fujikane D, Takai K, et al. Clinical features and genetic mechanisms of anxiety, fear, and avoidance: a comprehensive review of five anxiety disorders. Mol Psychiatry. 2025;30(10):4928–4936. doi:10.1038/s41380-025-03155-1
110. Friligkou E, Løkhammer S, Cabrera-Mendoza B, et al. Gene discovery and biological insights into anxiety disorders from a large-scale multi-ancestry genome-wide association study. Nat Genet. 2024;56(10):2036–2045. doi:10.1038/s41588-024-01908-2
111. Wootton RE, Jones HJ, Sallis HM. Mendelian randomisation for psychiatry: how does it work, and what can it tell us. Mol Psychiatry. 2022;27(1):53–57. doi:10.1038/s41380-021-01173-3
112. Minelli C, F DGM, van der Plaat DA, Bowden J, Sheehan NA, Thompson J. The use of two-sample methods for Mendelian randomization analyses on single large datasets. Int J Epidemiol. 2021;50(5):1651–1659. doi:10.1093/ije/dyab084
113. Sanderson E. Multivariable mendelian randomization and mediation. Cold Spring Harb Perspect Med. 2021;11(2):a038984. doi:10.1101/cshperspect.a038984
114. Jochimsen KN, Noehren B, Mattacola CG, Di Stasi S, Duncan ST, Jacobs C. Preoperative psychosocial factors and short-term pain and functional recovery after hip arthroscopy for femoroacetabular impingement syndrome. J Athl Train. 2021;56(10):1064–1071. doi:10.4085/1062-6050-139-20
115. Meng W, Adams MJ, Reel P, et al. Genetic correlations between pain phenotypes and depression and neuroticism. Eur J Hum Genet. 2020;28(3):358–366. doi:10.1038/s41431-019-0530-2
116. Singh JA, Lewallen D. Age, gender, obesity, and depression are associated with patient-related pain and function outcome after revision total Hip arthroplasty. Clin Rheumatol. 2009;28(12):1419–1430. doi:10.1007/s10067-009-1267-z
117. Norris RJ, Oancea SC, Nucci LB. Self-reported chronic back pain and current depression in brazil: a national level study. Int J Environ Res Public Health. 2023;20(8):5501. doi:10.3390/ijerph20085501
118. Lee W, Shin HJ, Min IK, et al. Shared comorbidity of depression, migraine, insomnia, and fibromyalgia in a population-based sample. J Affect Disord. 2024;354:619–626. doi:10.1016/j.jad.2024.03.077
119. Curtin F, Schulz P. Multiple correlations and Bonferroni’s correction. Biol Psychiatry. 1998;44(8):775–777. doi:10.1016/S0006-3223(98)00043-2
120. Lu Y, Lu D, Zhang H, et al. Causality between Ankylosing Spondylitis and osteoarthritis in European ancestry: a bidirectional Mendelian randomization study. Front Immunol. 2024;15:1297454. doi:10.3389/fimmu.2024.1297454
121. Menyhart O, Weltz B, Győrffy B. MultipleTesting.com: a tool for life science researchers for multiple hypothesis testing correction. PLoS One. 2021;16(6):e0245824. doi:10.1371/journal.pone.0245824
122. Sturgeon JA, Cooley C, Minhas D. Practical approaches for clinicians in chronic pain management: strategies and solutions. Best Pract Res Clin Rheumatol. 2024;38(1):101934. doi:10.1016/j.berh.2024.101934
123. Hebert SV, Green MA, Mashaw SA, et al. assessing risk factors and comorbidities in the treatment of chronic pain: a narrative review. Curr Pain Headache Rep. 2024;28(6):525–534. doi:10.1007/s11916-024-01249-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.