Back to Journals » Infection and Drug Resistance » Volume 15
A Comprehensive Evaluation of a Loop-Mediated Isothermal Amplification Assay for the Diagnosis of Pulmonary Tuberculosis in Children Using Bronchoalveolar Lavage Fluid
Authors Fan L, Guan B, Cheng M, Liu C, Tian Y, Li R, Chen Y
Received 17 December 2021
Accepted for publication 3 March 2022
Published 10 March 2022 Volume 2022:15 Pages 975—987
DOI https://doi.org/10.2147/IDR.S354660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lichao Fan,1,* Bo Guan,2,* Moxin Cheng,1,* Chang Liu,3 Yao Tian,1 Ran Li,1 Yu Chen1
1Department of Tuberculosis, Shenyang Tenth People’s Hospital, Shenyang Chest Hospital, Shenyang, Liaoning Province, 110044, People’s Republic of China; 2Geriatric Cardiology Department of the Second Medical Center & National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Department of Thoracic Surgery, Shenyang Tenth People’s Hospital, Shenyang Chest Hospital, Shenyang, 110044, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Chen, Email [email protected]
Objective: Using TB-LAMP for diagnosing pediatric PTB, however, still requires systematic evaluation. Here, we evaluated TB-LAMP performance alone and in combination with conventional assays for diagnosing PTB in Chinese children, using mycobacterial culture or CCRS (the composite clinical reference standard) as references.
Design or Methods: BALF samples were collected at Shenyang Tenth People’s Hospital from 251 children susceptible to TB infection with indications for fiberoptic bronchoscopy.
Results: When mycobacterial culture was the reference, TB-LAMP used alongside smear microscopy doubled sensitivity for detecting pediatric PTB compared with smear microscopy alone (82.5% vs 40.0%). When CCRS was the reference, AFB microscopy, MTB culture, and TB-LAMP had sensitivities of 16.5%, 30.1%, and 51.1%, respectively, and specificities of 98.2%, 100.0%, and 99.1%. Combining MTB culture with TB-LAMP gave a sensitivity of 61.1% and specificity of 96.6%. TB-LAMP identified 39.3% and 43.2% of cases with negative MTB culture or AFB microscopy results.
Conclusion: TB-LAMP using BALF samples provided faster results, allowing early and accurate PTB diagnosis. Our findings provide insights for optimizing diagnostic algorithms for pediatric PTB.
Keywords: child, pulmonary tuberculosis, diagnosis, loop-mediated isothermal amplification assay, bronchoalveolar lavage fluid
Introduction
Children with tuberculosis (TB) account for almost 12% of global tuberculosis cases and account for 14% of the total deaths.1 In China and other countries with a heavy TB-burden, however, there is a huge gap between the total incidence reported and cases estimated in the real world, mainly due to underdiagnosis and underreporting of TB cases. Timely and accurate diagnosis of pediatric TB cases, therefore, would greatly help to minimize the TB infection rate. Effective management of pediatric TB is held back by difficulties in microbiological confirmation as sample collection and low bacterial load remain two formidable clinical challenges. Clinical diagnosis of TB in children generally depends on their contact history, signs and symptoms, and radiography results, as microscopy and TB culture can only provide limited auxiliary information.2 Acid-fast bacilli (AFB) microscopy and mycobacterial culture have been regarded as the gold standard for TB diagnosis in recent decades.3 However, due to their low positive rates and delayed results,4,5 molecular assays have attracted increasing clinical attention. Significant improvements have been made in the diagnosis of TB since the WHO updated its recommendation to use the rapid test based on nucleic acid amplification test (NAAT) for TB not only in adults but also children.6 More comparative research is required to validate NAAT in detecting pediatric pulmonary tuberculosis from pertinent samples. The loop-mediated isothermal amplification (LAMP) assay has been developed as a novel technique for nucleic acid amplification.7 LAMP can amplify DNA with high specificity and efficiency under isothermal conditions using six sets of primers that recognize eight distinct regions in the target sequence, and diagnostic kits for TB using the LAMP method (TB-LAMP) are commercially available.8 TB-LAMP results can be interpreted with the naked eyes, making it more suitable for application in developing countries where TB is epidemic. Based on a worldwide multicenter study from 2012–2016, the World Health Organization (WHO) issued policy guidance in July 2016, recommending TB-LAMP as an alternative to smear tests for diagnosing TB in adults or for follow-up in smear-negative adults.9 According to the WHO report, when using culture-based standards as a reference, the pooled sensitivity and specificity of TB-LAMP ranges from 74.1% to 78.0% and 98.2% to 98.9%, respectively. A recent evaluation of the performance of TB-LAMP in pediatric pulmonary tuberculosis (PTB) patients using sputum/gastric aspirate as the test specimen gave a sensitivity of 94.9% (95% CI, 85.9–98.9%), suggesting that TB-LAMP may also be suitable for diagnosis of PTB in the pediatric population.10
Occasionally, when producing enough sputum for TB examination is difficult for children, alternative samples such as bronchoalveolar lavage fluid (BALF), gastric aspirate (GA) and laryngeal swabs are warranted.11,12 Of these, BALF samples tend to show a higher detection rate,13 but to date, there are no systemic evaluations of the performance of TB-LAMP using BALF as the test specimen for detecting PTB in children. Fiberoptic bronchoscopy is strongly indicated for diagnosing space-occupying lesions such as caseous necrosis or regional swollen lymph nodes. Here, we recruited children who needed fiberoptic bronchoscopy and collected BALF to test the performance of TB-LAMP either as a substitute for smear microscopy or in combination with conventional tests, against mycobacterial culture as a reference. In addition, we also evaluated our results against the composite clinical reference standard (CCRS) as a reference to provide a more comprehensive evaluation of the test.
Methods
Study Setting and Study Population
This retrospective study was performed at Shenyang Tenth People’s Hospital and Shenyang Chest Hospital from May 2020 to May 2021. Patients aged 18 years or younger were enrolled in the study if (1) they had symptoms of suspected tuberculosis, including a cough for more than 2 weeks or gasping; (2) a chest X-ray consistent with pulmonary TB; (3) they had indications to undergo fiberoptic bronchoscopy, such as dyspnea, obstructive pneumonia, localized emphysema, or ambiguous imaging changes warranting further microbiologic confirmation; (4) informed consent for fiberoptic bronchoscopy had been given. Children were excluded if they tested HIV positive or were taking anti-TB medications, or informed consent had not been obtained.
We applied two standards as references (mycobacterial culture and CCRS) to evaluate the performance of all the tests. Mycobacterial culture is the conventional gold standard for detecting M. tuberculosis and was applied in our study to check the performance of TB-LAMP, smear microscopy or their combination. The CCRS involves the following 2 items: (1) bacteriologically confirmed tuberculosis (positive for culture of MTB), (2) clinically diagnosed tuberculosis (clinical symptoms indicating PTB), radiographic evidence consistent with tuberculosis, and at least 1 of the following: positive tuberculin skin test or interferon release assay results, clinical and radiologic improvement seen after antituberculosis chemotherapy, or confirmed TB exposure.14 Our study design is presented in Figure 1.
 |
Figure 1 Selection of the study population. Abbreviations: BALF, bronchoalveolar lavage fluid; S-M, smear-microscopy; TB-LAMP, Loop-mediated Isothermal Amplification Assay; CCRS, the composite clinical reference standard. |
The study was approved (KYXM-2020-002-02) by the Medical Ethics Committee of Shenyang Chest Hospital. Hand-written informed consent was obtained from the guardians of all patients included in the study and this study was conducted in accordance with the Declaration of Helsinki.
Justification of Choosing BALF Over Expectorated Sputum for Evaluation of TB-LAMP
Our study compared the results of smear microscopy, liquid mycobacterial culture and TB-LAMP from expectorated sputum and BALF, however, only 65 of the 243 patients included in the study were able to produce sputum, and so BALF was collected from all 243 patients. A comparison was made between the two specimens for diagnosing PTB using all three methods.
Bronchoscopy Procedure, Specimen Collection and Handling
Bronchoscopy was performed on all patients by experienced infectious disease pediatricians in dedicated suites to collect BALF. Children were fasted and deprived of water for 4–6 hours before bronchoalveolar lavage. All children were anesthetized by local anesthesia, nebulized lidocaine was given for 30 minutes before bronchoscopy, and midazolam 0.3 mg/kg (maximum dose 10 mg) was given to the children during bronchoscopy. After successful induction of anesthesia, the bronchoscope was operated by the method of entering the bronchoscope while anesthesia. Flexible bronchoscopes with a 2.8 mm diameter (model XP-260F, Olympus Medical, Tokyo, Japan) or a 4.0 mm diameter (model BF-P260F, Olympus Medical, Tokyo, Japan) were used. After inspecting all visible segmental or bronchial trees, samples were collected from the lung segment or subsegment that showed abnormal lesions suggestive of active pulmonary TB on chest CT. For BALF collection, 5–10 mL of sterile saline was instilled and aspirated from the lung segments involved. Each specimen was quickly transported to the lab, where it was divided evenly into two portions for further detection. One portion was used for smear microscopy and mycobacterial culture, and the other for TB-LAMP.
TB-LAMP Assay
The TB-LAMP assay was performed stringently according to the protocol proposed by WHO9 using Loop amp PURE DNA extraction and Loop amp MTBC Detection kits (Eiken, Japan) according to the manufacturer’s instructions. 60 μL BALF samples were added to heating tubes and incubated at 90°C for 5 min, after which samples were mixed with absorbent powder by physical shaking until thoroughly mixed. 30 μL DNA solution was added to the reaction tube from the Loop amp MTBC detection kit and reaction tubes were then placed into a turbidimeter at 67°C for at least 30 min. Results were then observed with the help of ultraviolet fluorescence.
Smear Microscopy
0.05–0.1 mL sputum or BALF samples were collected for auramine O staining, after which light-emitting diode (LED) microscopy was applied for bacterial inspection. Results are presented according to the guidelines.15
Mycobacterial Culture
In all, 2 mL of the sputum or BALF sample, together with 1–2 times the volume of 2% N-acetyl-L-cysteine NaOH-Na citrate, was vortexed for 20 seconds before it was incubated for 15 minutes (room temperature). Phosphate-buffered saline (PBS) buffer (pH = 6.8) was then added to a final volume of 45 mL and centrifuged at 3000 × g for 15 minutes at 4 °C. Afterward, the supernatant was discarded, and the pellet was resuspended with 1.5 mL of PBS. Then, 0.5 mL of the final product was placed into MGIT 960 liquid culture tubes for incubation. After the instrument automatically reported a positive culture, the culture was smeared for microscopy, and 0.1 mL of the Auramine O dye was added for Ziehl–Neelsen staining, followed by fluorescence microscopy. If AFB were detected, the result was considered true positive. If no AFB were found, the result was as negative. If the tube remained negative for 42 days, this result was also defined as negative. All procedures were performed according to the instructions in the MGIT 960 manual.16
Statistical Analysis
The values of test sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), and their 95% confidence intervals, were preliminarily calculated for smear microscopy, TB-LAMP or smear microscopy accompanied by TB-LAMP using the Wilson score binomial method, taking bacterial culture as a reference standard.17 The abovementioned parameters were then calculated a second time, taking clinical diagnosis as a reference. Differences between two assays or their combination were assessed using one-way analysis of variance (ANOVA). A P value (two-tailed) less than 0.05 was assumed to be statistically significant. All statistical analyses were performed using SPSS 20.0 software and Excel 2010 software.
Results
Demographical Information on the Study Population
A total of 425 patients with symptoms potentially associated with PTB visited Shenyang Tenth People’s Hospital and Shenyang Chest Hospital during the study period. Of these, 251 were children and fulfilled the criteria for enrollment, but 8 children did not complete the TB-LAMP assay and were excluded from our study. Of the remaining 243 children, 133 (55.6%) had active PTB, and 110 (44.4%) did not (97 pneumonia, 3 nontuberculous mycobacterium lung disease, 1 lung cancer, 9 other lung conditions). For 235 children (96.7%), this was the first time they were suspected to have PTB, while 8 children (3.3%) had previously been treated for TB. Forty of the 133 children with active TB were culture-confirmed cases. Of the 243 children included, 121 (49.8%) subjects were under 14 [sub-groups: aged < 5 (n=8), 5–9 (n=27) and 10–14 years old (n=86)], and 122 (50.2%) were 15–18 years of age. The average age of participants was 13.52±3.80 years, and ranged from 3 months to 18 years old. All 243 patients had received the Bacillus Calmette–Guérin (BCG) vaccine. Demographics and clinical characteristics for the study population are shown in Table 1.
 |
Table 1 Clinical Characteristics of the Study Population (n=243) |
Recommendations on BALF Over Expectorated Sputum for TB-LAMP
Sputum specimens could only be obtained from 65 of the 243 patients in the larger study. Of the 65 patients recruited, 34 were clinically diagnosed with PTB. BALF was chosen as the final specimen to complete the comparison between TB-LAMP and conventional methods for diagnosing PTB as a there was a lower chance of detection M. tuberculosis infection in expectorated sputum regardless of which detection tool was employed (Table 2).
 |
Table 2 Comparison of BALF and Expectorated Sputum for Detecting Mycobacterium tuberculosis in Pediatric Patients Using the Composite Clinical Reference Standard (CCRS) as a Reference |
Performance of TB-LAMP and Smear Microscopy Using Culture as a Reference
The performance of TB-LAMP and smear microscopy for detecting M. tuberculosis infection in the 243 recruited patients (40 culture-positive and 203 culture-negative patients) when mycobacterial culture was used as a reference is presented in Table 3. TB-LAMP had significantly higher sensitivity (77.5 vs 40.0%, P<0.05) but lower specificity than smear microscopy (81.8 vs 96.1%, P<0.05). When smear microscopy and LAMP were performed serially, the overall sensitivity increased to 82.5% (33/40) against culture. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve for smear microscopy, TB-LAMP and the two tests performed in parallel was 0.680, 0.794, and 0.814, respectively (Figure 2). As 93 cases (69.9%) clinically diagnosed with TB were culture-negative, using culture results as the sole reference may lack power for assessing the performance of TB-LAMP. Therefore, we also used a clinical diagnostic framework to evaluate TB-LAMP performance.
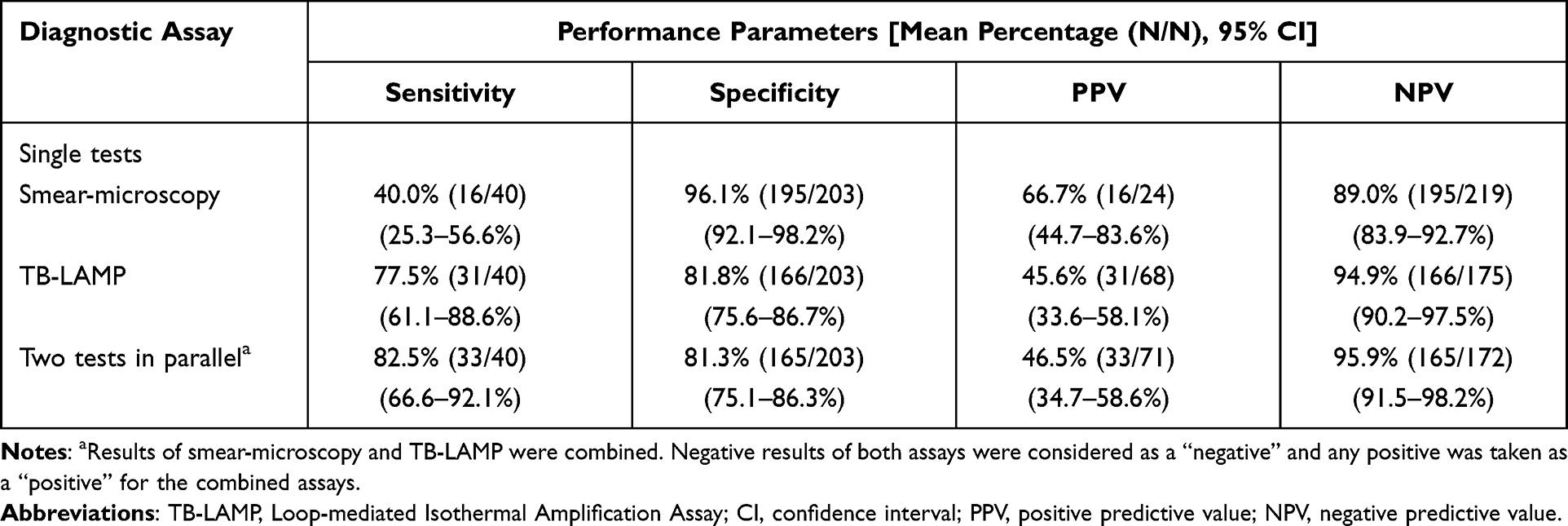 |
Table 3 Performance of Smear-Microscopy, TB-LAMP and Their Combination for Detecting M. tuberculosis Using Culture as a Reference |
 |
Figure 2 Receiver operating characteristic (ROC) curves for determining the sensitivity and specificity of smear-microscopy, TB-LAMP and the two tests in parallel using culture as a reference. Abbreviation: TB-LAMP, Loop-mediated Isothermal Amplification Assay. |
Performance of TB-LAMP and Conventional Methods Using Clinical Diagnosis as a Reference
Based on CCRS criteria, 133 of the 243 patients enrolled in the study had a positive PTB diagnosis and 110 a negative PTB diagnosis, with 40, 24 and 69 cases of PTB being identified by mycobacterial culture, smear microscopy and TB-LAMP, respectively (Figure 3). Results from our assessment of the performance of TB-LAMP, mycobacterial culture and smear microscopy alone or in combination for diagnosing PTB using clinical diagnosis as a reference are shown in Table 4. TB-LAMP showed higher sensitivity (51.1%; 68/133) and specificity (99.1%; 109/110) as an independent test than smear microscopy (sensitivity: 16.5%; 22/133 and specificity: 98.2%; 108/110) using CCRS as the reference standard. When smear microscopy and LAMP were performed in parallel, the overall sensitivity and specificity were 53.4% (71/133) and 99.1% (109/110) respectively. Simultaneous combination of TB-LAMP with smear microscopy improved sensitivities by 36.9% and 2.3% compared to smear microscopy or TB-LAMP alone. The AUC of the ROC curve for smear microscopy, TB-LAMP and the two tests in parallel was 0.574, 0.751 and 0.753, respectively (Figure 4). When culture and TB-LAMP were performed in parallel, the overall sensitivity and specificity were 57.9% (77/133) and 99.1% (109/110), respectively. Simultaneous combination of TB-LAMP and culture improved sensitivities by 27.8% and 6.8% compared to culture or TB-LAMP alone. The AUC of the ROC curve for culture, TB-LAMP and the two tests in parallel was 0.650, 0.751 and 0.785, respectively (Figure 5). Simultaneous combination of TB-LAMP, culture and smear microscopy increased assay sensitivities by 42.1%, 28.5% and 7.5%, respectively, compared with culture, smear microscopy or TB-LAMP alone. TB-LAMP detected 43.2% (48/11) and 39.8% (37/93) of the cases determined to be positive using CCRS criteria that were smear-negative or mycobacterial culture-negative (Table 4).
 |
Table 4 Performance of TB-LAMP, Culture and Smear-Microscopy as Single Tests and Combined Tests for the Diagnosis of Pulmonary TB Using the Composite Clinical Reference Standard (CCRS) as a Reference Standard |
 |
Figure 3 Venn diagram showing results of different diagnostic tests on bronchoalveolar lavage fluid samples from children with suspected pulmonary tuberculosis (N = 243). Abbreviation: TB-LAMP, Loop-mediated Isothermal Amplification Assay. |
 |
Figure 4 Receiver operating characteristic (ROC) curves for determining the sensitivity and specificity of smear-microscopy, TB-LAMP and the two tests in parallel using CCRS as a reference. Abbreviations: TB-LAMP, Loop-mediated Isothermal Amplification Assay; CCRS, the composite clinical reference standard. |
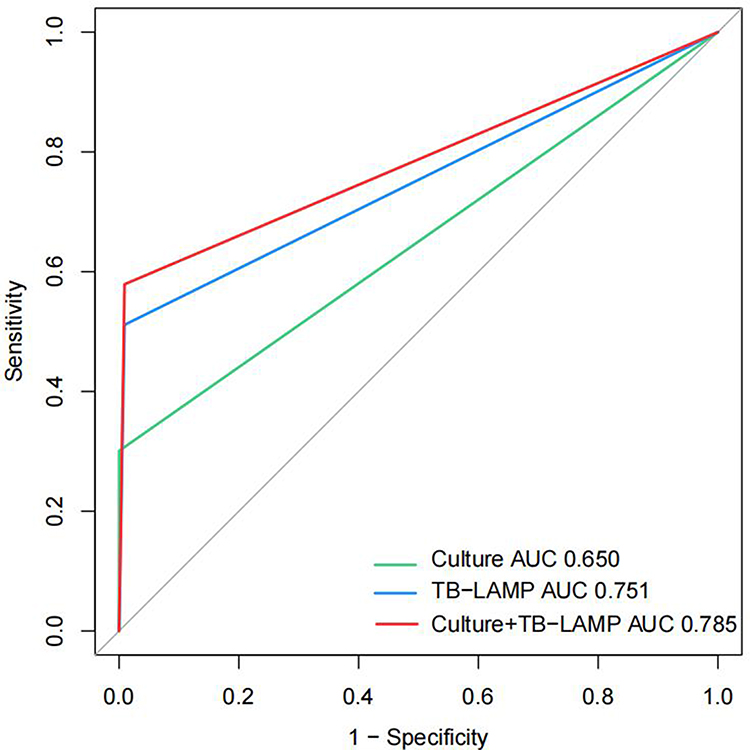 |
Figure 5 Receiver operating characteristic (ROC) curves for determining the sensitivity and specificity of culture, TB-LAMP and the two tests in parallel using CCRS as a reference. Abbreviations: TB-LAMP, Loop-mediated Isothermal Amplification Assay; CCRS, the composite clinical reference standard. |
Discussion
In this study, we conducted TB-LAMP and conventional laboratory tests on BALF specimens for diagnosing PTB in Chinese children, and evaluated the performance of the tests in a rigorous and standardized manner, applying two different reference standards to provide a more comprehensive evaluation. Findings indicated that BALF was better than expectorated sputum for PTB detection in the context of our hospital and that TB-LAMP conducted using BALF was the best single assay for PTB diagnosis due to its accuracy and simplicity. Combining TB-LAMP with smear-microscopy provides an accurate early diagnostic tool for confirming PTB in children, and combining TB-LAMP with culture is the best choice for clinical diagnosis. TB-LAMP was also a useful tool for diagnosing PTB in smear-negative or culture-negative pediatric cases.
Though invasive, the diagnostic value of fiberoptic bronchoscopy is irreplaceable in children with dyspnea, obstructive pneumonia, and complicated pulmonary diseases.18 In our hospital, fiberoptic bronchoscopy is routinely scheduled for children with suspicious PTB chest images. BALF specimens tend to have a high yield for isolating Mycobacterium tuberculosis in children with severe airway obstruction.19 Although several types of samples, such as sputum, gastric juice, urine, stool and BALF,20–22 can be used as TB test specimens, BALF is considered to be a reliable alternative to sputum specimens, especially in sputum-free or sputum-scarce children.23 Here, 34 out of the 65 patients expectorated sputum were diagnosed with pulmonary TB, we made a direct comparison between BALF and expectorated sputum in 34 pediatric TB patients. We found BALF gave positive rates of 29.4%, 38.2%, and 70.6% using smear microscopy, mycobacterial culture, and TB-LAMP, respectively, and BALF was therefore considered a better choice for diagnosing PTB than expectorated sputum.
In our retrospective study, 133 and 110 children with or without active TB children were enrolled, respectively. The sensitivity of TB-LAMP for detecting PTB in bacteriologically confirmed TB and clinically diagnosed TB cases was 77.5% (31/40) and 51.1% (68/133), respectively. The specificity of TB-LAMP was high (99.1%, 109/110). Similar findings have been reported by Sreedeep et al24 in a recently published cross-sectional analytical study using respiratory specimens (sputum, gastric lavage, bronchoalveolar lavage and/or endotracheal aspirates) in children with pulmonary tuberculosis. TB-LAMP conducted using BALF samples can provide faster results, allowing an early and accurate TB diagnosis in both bacteriologically confirmed and clinically diagnosed TB children. Results from our research are also in accordance with reports on the use of TB-LAMP on sputum samples from adults in countries with a high TB burden,25 with sensitivities of 77.7% and specificities of 98.1%.
It is noteworthy that there may be discrepancies in TB-LAMP results between regions with different TB burdens. However, according to the WHO expert committee report on the use of TB-LAMP, the sensitivity of TB-LAMP in heavily afflicted countries such as India, South Africa and Peru (89.1%, 84.4 and 77.7%, respectively) is not much different to that in countries with a lower TB burden such as Japan (87.9%).26,27 The TB-LAMP test, then should be suitable for application in different TB endemic regions.
The sensitivity of TB-LAMP in our study was 77.5% (31/40), significantly exceeding that of smear microscopy, which is currently regarded as a frontline diagnostic test in China.28 Our study also showed that when used in combination with smear microscopy, the sensitivity of TB-LAMP increased to 82.5% and had an AUC value of 0.814 in reference to mycobacterial culture, making this combination superior to all other single tests evaluated here in terms of diagnostic accuracy. Since MGIT 960 culture takes more than 2 to 3 weeks, finding a method for diagnosing patients rapidly is of great clinical importance. The combination of TB-LAMP and smear microscopy may fill this gap and allow early and adequate anti-TB treatment of potential patients.
Because of low sensitivity of MTB culture in pediatric PTB, we also assessed the diagnostic performance against CCRS. Our results showed that when using CCRS as a reference, the sensitivity of TB-LAMP reached 51.0%, somewhat higher than the 37.8% previously reported by Govindan et al.29 When CCRS was used as the reference, the sensitivity of TB-LAMP was significantly higher than that of culture and smear-microscopy. The TB-LAMP assay can detect 21.0% more PTB patients than MTB culture and 34.6% more PTB patients than AFB microscopy. Our results are in agreement with a study by Wang et al who found that multiplex LAMP-LFB (82.0%, 82/100) showed higher sensitivity than culture (47.0%, 47/100, P < 0.001) and detected an additional 28 probable TB cases, increasing the percentage of definite TB cases from 62.0% (62/100) to 90.0% (90/100).30 Yadav et al also found a higher overall sensitivity of the TB-LAMP assay than smear tests (82% vs 64%).31 In another study,32 the sensitivity of TB-LAMP was reported as 84.5%, and was significantly higher than that of AFB microscopy (67.9%) and culture (75.7%). Taken together, our findings, together with previous studies, suggest that the TB-LAMP assay may be a promising test for the diagnosis of pediatric PTB.
The WHO have highlighted that existing tests included in diagnostic algorithms for active PTB can be tailored for each country’s settings and resources. In our study, simultaneous combination of culture with TB-LAMP showed that TB-LAMP is a power tool for detecting M. tuberculosis infection in children with PTB, presenting a sensitivity of 57.9%, NPV of 66.1%, a specificity of 99.1%, and PPV of 98.7% when CCRS is used as a reference. The performance of culture and TB-LAMP in parallel was significantly better than that of other single tests for TB, as evidenced by the respective ROC curves and AUC values (culture and TB-LAMP in parallel: AUC of 0.785; culture alone: AUC of 0.650; TB-LAMP alone, AUC: 0.751). As these results were similar to simultaneously combining smear-microscopy, culture and TB-LAMP, we concluded that combining these two assays to be a rational diagnostic algorithm for PTB confirmation in Chinese children. However, mycobacterial culture should remain the gold standard for confirming PTB, especially when smear microscopy misguides clinical judgment, and its role in detecting clinical NTM is also irreplaceable. In our study, the 65 (out of 133) false-negative TB-LAMP results may have been caused by a low mycobacterial burden.33 Several cases also had false positive results, likely due to dead M. tuberculosis cells still being present after effective treatment; established PTB status prior to testing can cloud the judgment of all nucleic acid amplification technique-based assays.34 In our study, one patient diagnosed with previous PTB presented with obstructive pneumonia and had a positive TB-LAMP result. After removal of sputum in the airway and 2 weeks of antibacterial treatment, the lower specificity of TB-LAMP was further confirmed through a 6-month chest image recheck.
TB-LAMP also holds strong potential for setting definitive diagnosis in culture-negative and smear-negative samples; 43.2% (48/111) and 39.8% (37/93) of smear-negative and culture-negative cases tested positive in our study using TB-LAMP. Our data provide insight into the added value of TB-LAMP for clinical diagnosis of PTB in children in China, a country with a high burden of tuberculosis. BALF showed a superior diagnostic yield in children with bacteriology-negative or sputum-scarce PTB. The overall performance of TB-LAMP was superior to smear microscopy and culture in this study. It is less affected by electricity and temperature.9 While most NAATs require a separate DNA extraction step, the TB-LAMP system only requires use of a solution for DNA extraction (Loopamp PURE DNA extraction kit). In addition, amplification can be detected by visual inspection under UV light instead of using a turbidimeter.
Our hospital is a well-equipped medical institution with full capacity for conducting TB confirmatory tests, and we can routinely perform both mycobacterial culture and TB-LAMP on BALF samples. Hospitals with limited medical resources, however, rarely perform TB culture on site because of the lack of necessary equipment and facilities. As mycobacterial culture is not readily available in many less-developed regions, TB-LAMP could be a good substitute as its routine operation requires minimal training, and it is also very useful in cases when children with PTB show negative etiological results. Since all BALF samples in this study were tested immediately, one of the limitations of our study is whether DNA degradation will occur in BALF samples after long-term storage and transportation. Therefore, and further experiments should be performed to analyze the effect of storage and transportation on the accuracy of TB-LAMP. Secondly, limited by the retrospective design of our study, we only analyzed one-sample test and thus may underestimate the diagnostic value of all methods. Moore et al showed that detection of Mtb is enhanced by submitting many samples on separate days in the diagnosis of pulmonary tuberculosis in young children.35 So we think, a prospective study may provide more accurate information on the yield of molecular or bacteriological tests on repeated BALF samples from children. A third limitation of our study is that our results might be difficult to extrapolate as only children with indications for fiberoptic bronchoscopy were included, and obtaining BALF specimens during fiberoptic bronchoscopy must be performed by experienced physicians. Fourth, considering the small number of culture-confirmed pulmonary tuberculosis cases and very young children or infants in our study, larger studies are required to determine the benefit of TB-LAMP testing in pediatric TB clinical settings.
Conclusion
TB-LAMP assays using BALF were superior to conventional tests for the rapid diagnosis of childhood PTB. TB-LAMP is a promising alternative test that has much higher sensitivity and a shorter detection interval than smear microscopy and mycobacterial culture. Combining TB-LAMP with smear microscopy greatly improved accuracy in diagnosing bacteriologically-confirmed PTB in children. A combination of MTB culture and TB-LAMP provides a rational diagnostic algorithm for pediatric PTB in China.
Ethical Approval Statement
The study was approved (KYXM-2020-002-02) by the Medical Ethics Committee of Shenyang Chest Hospital. Hand-written informed consent was obtained from the guardians of all patients included in the study.
Acknowledgments
These authors contributed equally to this work and share first authorship: Lichao Fan, Bo Guan, and Moxin Cheng.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. World Health Organization. Global Tuberculosis Report 2020. Geneva: World Health Organization; 2020.
2. Lamb GS, Starke JR. Tuberculosis in infants and children. Microbiol Spectr. 2017;5:541–569. doi:10.1128/microbiolspec.TNMI7-0037-2016
3. Gupte S. Short textbook of medical microbiology. In: Mycobacteria.
4. Cruz AT, Starke JR. Clinical manifestations of tuberculosis in children. Paediatr Respir Rev. 2007;8:8107–8117.
5. Moore DP, Klugman KP, Madhi SA. Role of Streptococcus pneumoniae in hospitalization for acute community-acquired pneumonia associated with culture-confirmed Mycobacterium tuberculosis in children: a pneumococcal conjugate vaccine probe study. Pediatr Infect Dis J. 2010;29:1099–1104. doi:10.1097/INF.0b013e3181eaefff
6. World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. World Health Organization; 2013.
7. Itani W, Matsuyama S, Azhar EI. Development of fluorescent reverse transcription loop-mediated isothermal amplification (RT-LAMP) using quenching probes for the detection of the Middle East respiratory syndrome coronavirus. J Virol Methods. 2018;258:41–48. doi:10.1016/j.jviromet.2018.05.006
8. Bojang AL, Mendy FS, Tientcheu LD, et al. Comparison of TB-LAMP, GeneXpert MTB/RIF and culture for diagnosis of pulmonary tuberculosis in The Gambia. J Infect. 2016;72:332–337. doi:10.1016/j.jinf.2015.11.011
9. World Health Organization. The Use of Loop-Mediated Isothermal Amplification (TB-LAMP) for the Diagnosis of Pulmonary Tuberculosis: Policy Guidance. Geneva: World Health Organization; 2016.
10. Dayal R, Yadav A, Agarwal D, et al. Comparison of diagnostic yield of tuberculosis loop-mediated isothermal amplification assay with cartridge-based nucleic acid amplification test, acid-fast bacilli microscopy, and mycobacteria growth indicator tube culture in children with pulmonary tuberculosis. J Pediatric Infect Dis Soc. 2021;10:83–87. doi:10.1093/jpids/piaa019
11. Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med. 2015;3:451–461. doi:10.1016/S2213-2600(15)00095-8
12. Nicol MP, Spiers K, Workman L, et al. Xpert MTB/RIF testing of stool samples for the diagnosis of pulmonary tuberculosis in children. Clin Infect Dis. 2013;57:e18–e21. doi:10.1093/cid/cit230
13. Petrović S. Diagnostic value of certain methods for isolation of Mycobacterium tuberculosis in children with suspected pulmonary tuberculosis. Med Pregl. 2005;58:231–235. doi:10.2298/MPNS0506231P
14. Graham SM, Ahmed T, Amanullah F, et al. Evaluation of tuberculosis diagnostics in children: 1. Proposed clinical case definitions for classification of intrathoracic tuberculosis disease. Consensus from an expert panel. J Infect Dis. 2012;205(Suppl2):S199–208. doi:10.1093/infdis/jis008
15. Akhtar M. Technical Guide: Sputum Examination for Tuberculosis by Direct Microscopy in Low Income Countries.
16. Siddiqi SH, Rüsch-Gerdes S. MGIT Procedure Manual. Geneva: FIND; 2006.
17. Luetkemeyer AF, Firnhaber C, Kendall MA, et al. Evaluation of Xpert MTB/RIF versus AFB smear and culture to identify pulmonary tuberculosis in patients with suspected tuberculosis from low and higher prevalence settings. Clin Infect Dis. 2016;62:1081–1088. doi:10.1093/cid/ciw035
18. Abadco DL, Steiner P. Gastric lavage is better than bronchoalveolar lavage for isolation of Mycobacterium tuberculosis in childhood pulmonary tuberculosis. Pediatr Infect Dis J. 1992;11:735–738. doi:10.1097/00006454-199209000-00013
19. Goussard P, Gie RP, Kling S, et al. Bronchoscopic assessment of airway involvement in children presenting with clinically significant airway obstruction due to tuberculosis. Pediatr Pulmonol. 2013;48:1000–1007. doi:10.1002/ppul.22747
20. Liu XH, Xia L, Song B, et al. Stool-based Xpert MTB/RIF Ultra assay as a tool for detecting pulmonary tuberculosis in children with abnormal chest imaging: a prospective cohort study. J Infect. 2021;82:84–89. doi:10.1016/j.jinf.2020.10.036
21. Yin QQ, Jiao WW, Han R, et al. Rapid diagnosis of childhood pulmonary tuberculosis by Xpert MTB/RIF assay using bronchoalveolar lavage fluid. Biomed Res Int. 2014;2014:310194. doi:10.1155/2014/310194
22. Sun L, Zhu Y, Fang M, et al. Evaluation of Xpert MTB/RIF ultra assay for diagnosis of childhood tuberculosis: a multicenter accuracy study. J Clin Microbiol. 2020;58:e00702–20. doi:10.1128/JCM.00702-20
23. Çakır E, Özdemir A, Daşkaya H, Umutoğlu T, Yüksel M. The value of nasopharyngeal aspirate, gastric aspirate and bronchoalveolar lavage fluid in the diagnosis of childhood tuberculosis. Turk J Pediatr. 2018;60:10–13. doi:10.24953/turkjped.2018.01.002
24. Sreedeep KS, Sethi S, Yadav R, et al. Loop-mediated isothermal amplification (LAMP) in the respiratory specimens for the diagnosis of pediatric pulmonary tuberculosis: a pilot study. J Infect Chemother. 2020;26:823–830. doi:10.1016/j.jiac.2020.03.019
25. Shete PB, Farr K, Strnad L, Gray CM, Cattamanchi A. Diagnostic accuracy of TB-LAMP for pulmonary tuberculosis: a systematic review and meta-analysis. BMC Infect Dis. 2019;19:268. doi:10.1186/s12879-019-3881-y
26. WHOFIND: WHO Expert Group Meeting Report Geneva. The use of a commercial loop-mediated isothermal amplification assay (TB-LAMP) for the detection of tuberculosis. WHO/HTM/TB/2013.5. 2013.
27. Mitarai S, Okumura M, Toyota E. Evaluation of a simple loop-mediated isothermal amplification test kit for the diagnosis of tuberculosis. Int J Tuberc Lung Dis. 2011;15:1211–1217. doi:10.5588/ijtld.10.0629
28. Gelaw B, Shiferaw Y, Alemayehu M, Bashaw AA. Comparison of loop-mediated isothermal amplification assay and smear microscopy with culture for the diagnostic accuracy of tuberculosis. BMC Infect Dis. 2017;17:79. doi:10.1186/s12879-016-2140-8
29. Govindan SA, Yadav R, Vaidya PC, et al. Comparison of performances of loop-mediated isothermal amplification, XPERT MTB/RIF and BACTEC MGIT in the diagnosis of childhood tuberculosis. J Paediatr Child Health. 2021;57:847–853. doi:10.1111/jpc.15334
30. Wang X, Wang G, Wang Y, et al. Development and preliminary application of multiplex loop-mediated isothermal amplification coupled with lateral flow biosensor for detection of mycobacterium tuberculosis complex. Front Cell Infect Microbiol. 2021;11:666492. doi:10.3389/fcimb.2021.666492
31. Yadav R, Daroch P, Gupta P, Agarwal P, Aggarwal AN, Sethi S. Diagnostic accuracy of TB-LAMP assay in patients with pulmonary tuberculosis-A case-control study in northern India. Pulmonology. 2020;
32. Sethi S, Singh S, Dhatwalia SK, et al. Evaluation of in-house loop-mediated isothermal amplification (LAMP) assay for rapid diagnosis of M. tuberculosis in pulmonary specimens. J Clin Lab Anal. 2013;27:272–276. doi:10.1002/jcla.21596
33. Notomi T, Mori Y, Tomita N, Kanda H. Loop-mediated isothermal amplification (LAMP): principle, features, and future prospects. J Microbiol. 2015;53:1–5. doi:10.1007/s12275-015-4656-9
34. Dorman SE, Schumacher SG, Alland D, et al. Xpert MTB/RIF ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study. Lancet Infect Dis. 2018;18:76–84. doi:10.1016/S1473-3099(17)30691-6
35. Moore DP, Higdon MM, Hammitt LL, et al. The incremental value of repeated induced sputum and gastric aspirate samples for the diagnosis of pulmonary tuberculosis in young children with acute community-acquired pneumonia. Clin Infect Dis. 2017;64(suppl_3):S309–S316. doi:10.1093/cid/cix099
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.