Back to Journals » Medical Devices: Evidence and Research » Volume 16
A Comparison of the Preclinical Performance of the Echelon™+ Stapler with Thunderbird Reloads to Two Commercial Endoscopic Surgical Staplers
Authors Wang S, Hua Y, Liu J, Huang ZF, Clymer JW ![]() , Ricketts CD
, Ricketts CD ![]() , Hao J
, Hao J
Received 4 October 2023
Accepted for publication 21 November 2023
Published 5 December 2023 Volume 2023:16 Pages 229—236
DOI https://doi.org/10.2147/MDER.S443067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shanshan Wang, Ying Hua, Jun Liu, Zhifan F Huang, Jeffrey W Clymer, Crystal D Ricketts, Jin Hao
Ethicon, Inc, Cincinnati, OH, USA
Correspondence: Jeffrey W Clymer, Ethicon, Inc, 4545 Creek Road, Cincinnati, OH, 45242, USA, Email [email protected]
Background: Design of surgical staplers continues to advance with more consistent staple formation that can lead to higher leak pressures and lower rates of leak along the staple line. This study was performed to compare the Ethicon Echelon™+ Stapler with Thunderbird reloads to two other currently available commercial staplers, Reach Anzhi and Fulbright Lunar with corresponding reloads.
Methods: The rate of malformed staples for three staplers was determined in porcine stomach (3.0– 3.3 mm thickness) via CT scanning. Staple line air leak pressures in bronchial tissue (3.0– 3.3 mm) and fluid leak pressures in colon (1.3– 1.7 mm) were measured and compared to a standard success criterion for both tissues.
Results: The rate of malformed staples in gastric tissue for Echelon+ was more than 90% lower than for the two other commercial staplers (p < 0.001). In bronchus, Echelon+ had 56% higher air leak pressures than Reach Anzhi (p < 0.001) and was not significantly different from Fulbright Lunar. In colon, Echelon+ had over twice the fluid leak pressures of the comparators (p < 0.001).
Conclusion: The Echelon+ Stapler with Thunderbird reloads exhibited a low rate of malformed staples, and its staple lines withstood high leak pressures in both thick and thin tissues. Clinical studies are needed to confirm that these observed benefits carry over into actual practice.
Keywords: stapler, endoscopic, burst pressure, malformed staples, leaking
Introduction
In 1908, Hungarian surgeon Humer Hultl and Hungarian surgical device designer Victor Fisher developed the first internal surgical stapler.1 Since their introduction, surgical staplers have continuously evolved and are one of the most widely used surgical instruments for tissue transection, resection and creation of anastomoses. The evolution of the modern stapler facilitated the development of minimally invasive surgery, particularly in thoracic and general surgery. For instance, stapling has become part of the standard of care in video-assisted thoracic surgery (VATS) to treat lung cancer.2 Stapling also makes the method of extracorporeal/intracorporeal anastomosis in laparoscopic surgery possible for gastric cancer patients with faster recovery and less pain compared with open surgery.3
As the volume of minimally invasive surgery using staplers that grows throughout the world, it is important that medical device manufacturers continue to develop and then evaluate stapling surgery outcomes. Although today's surgical staplers are safe, efficient, and reliable, a potential risk still exists for staple-line failures, leading to complications, including leakage from staple lines, bleeding, and fistula formation.4–6 In addition to staple-line failures, other complications that have been reported as adverse events (AE) related to tissue stapling include tissue damage due to fragility, stapler rocking during stapling, stapler-tissue thickness mismatch and technical failure.7
While various designs of surgical staplers are available, most staplers bend the staples into a B configuration that aids in securing the tissue. During the stapler firing sequence, malformed staples can result if the unformed staples do not properly align with the anvil pocket. Various tissue characteristics including tissue thickness, tissue viscosity, and differing properties between layers of tissue (eg, cartilage and mucosa in bronchus) can cause malformed staples to occur due to the staple leg being dragged or deflected during firing. Selecting the appropriate cartridge for a given target firing based on tissue characteristics is also critical as a mismatch could compromise the integrity of the staple line. In addition, staple properties such as staple diameter, unformed height, bending characteristics and metal composition can affect the staple leg’s ability to overcome tissue variation.8 Malformed staples can also occur if the stapler is fired over clips or a similar obstruction or the device fails to release from tissue.9,10
The Echelon+ Stapler with Thunderbird reloads (TBGST, Figure 1) has an advanced anvil curvature as well as wide, tapered staple pockets that are designed to improve the capture and formation of staples when the stapler is fired. The powered firing of the Echelon+ TBGST stapler adapts to tissue thickness; when used on thicker tissue, the speed of stapler firing decreases ensuring compression is uniform throughout the staple line, and staple formation is optimal.11 The Gripping Surface Technology (GST) incorporated in the Thunderbird reloads, provides improved tissue manipulation while securely holding tissue during stapling to improve tissue approximation and seal strength.12–16 In addition, the TBGST reload has glass fiber technology in the sled and driver for enhanced strength which is designed to provide better staple formation.
 |
Figure 1 The Echelon+ Stapler with Thunderbird reloads. |
To simulate the challenging conditions that may occur in surgery, we present here the results of a series of comparative ex-vivo tests performed in a laboratory-based setting. Staple form quality on relatively thick porcine stomach, as well as fluid leak pressure in colon and air leak pressure in bronchus were evaluated. Staplers evaluated were the Echelon+ TBGST Stapler with Thunderbird Reloads, the Reach Anzhi stapler and the Fulbright Lunar stapler with their corresponding reloads. These three staplers represent the most prevalent China commercial devices in the category of single-use powered articulating endoscopic cutter staplers.
Methods
All tissue testing was performed on ex vivo samples sourced from a commercial food supplier, hence no internal review board was necessary. Devices evaluated were the Echelon™+ stapler with Thunderbird (TBGST) reloads (PSEE60A stapler, GCFLGB/GCFLGG reloads, Ethicon, Inc., Cincinnati, OH, USA), the Reach Anzhi stapler with reloads (IM60AM stapler with REC60BLU/REC60GRN reloads, Reach Surgical Co., Ltd, Tianjin, China), and the Fulbright Lunar stapler with reloads (FSAM60 stapler with FMCB60/FMCG60 reloads, Fulbright Medical Inc., Wuxi, Jiangsu, China). The number of firings for all staplers was similar at the left, right and straight articulation positions.
Staple Form in Stomach
Porcine stomach of thickness 3.0–3.3 mm, determined by applying an 8 g/mm2 pressure for 15 seconds prior to measurement,17 was stapled of the stapler using a green reload. The tissue was mounted on tongue depressors using cyanoacrylate glue during computed tomography (CT) scanning. The imaging system (X50 CT System, North Star Imaging, Rogers, MN) was operated at 70 kV, 170 µA, for 720 projections at an 11.9 µm focal spot size. The scanned image was reconstructed with efX-CT Computed Tomography Reconstruction and Visualization (North Star Imaging). Images were analyzed by Kinetic Vision Inc. (Cincinnati OH) to provide staple form quality (SFQ). SFQ is a 5-point grading scale (Figure 2), with a score of 1–2 considered well formed, and 3–5 considered malformed.18 Statistical comparisons were performed using Fisher’s exact test with α = 0.05.
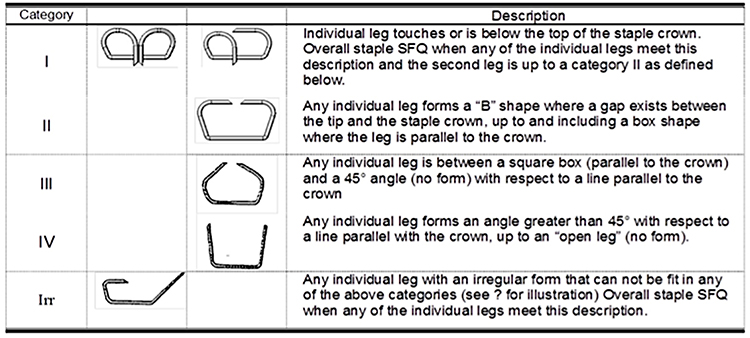 |
Figure 2 Staple Form Quality categories. Scores of 1–2 were considered well-formed, whereas 3–5 were considered malformed. |
Bronchus Leak Pressure
Porcine bronchus of thickness 3.0–3.3 mm, determined by applying an 8 g/mm2 pressure for 15 seconds prior to measurement, was stapled at one end of the stapler using a green reload. Air leak testing was performed using a custom system designed by Advint LLC (Reynoldsburg OH) based on a metering pump (Pulsatron, Pulsafeeder, Punta Gorda, Florida) to fill the anastomosis with air at a rate of pressure increase of approximately 60 mmHg per minute with incremental steps every 15 seconds. Data were censored at 250 mmHg. The leak onset pressure was recorded, and the proportion of leakers below 88 mmHg was tallied. This criterion was chosen based on 88 mmHg being the maximum exhalation pressure that the diaphragm and thoracic muscles have been observed to exert.19 Statistical comparison was performed via Student’s t-test for mean observed leak pressure and Fisher’s exact test for frequency of leak at a pressure less than 88 mmHg with α=0.05.
Colon Leak Pressure
Staple firings using blue reloads were performed longitudinally on porcine colon of a selected tissue thickness range (1.5 ± 0.2 mm). The proximal end of the staple line was attached to a barbed Luer lock fitting and securely tied with a suture. The distal end was sealed with a zip tie and any leak at the zip tie was ignored unless the leak rate affected the recorded pressure, in which case the specimen was discarded. A computer-controlled pressure ramp-up rate of 30 mmHg/minute was utilized with dyed room-temperature water. Fluid leaks were visually identified as originating from the staple line or the cut line. If a staple line leak occurred, testing was continued until there was a cut line leak. Statistical comparison was performed via Student’s t-test for mean observed leak pressure and Fisher’s exact test for frequency of leak at a pressure less than 30 mmHg with α=0.05.20
Results
In Staple Form Quality testing in 3.0–3.3 mm stomach with green loads (Table 1, Figure 3), Echelon+ TBGST produced 97% fewer malformed (Category 3 or higher) staples than Fulbright Lunar and 92% fewer malformed staples than Reach Anzhi (p < 0.001).
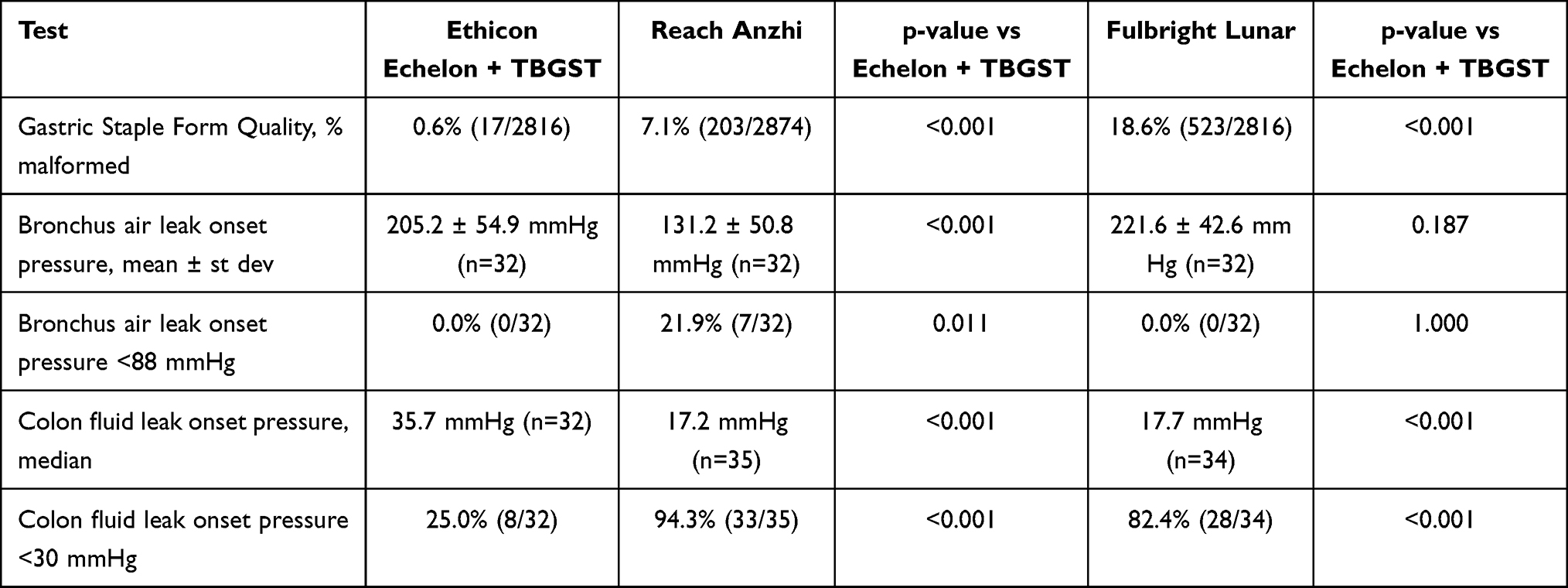 |
Table 1 Summary of Comparisons Between Staplers |
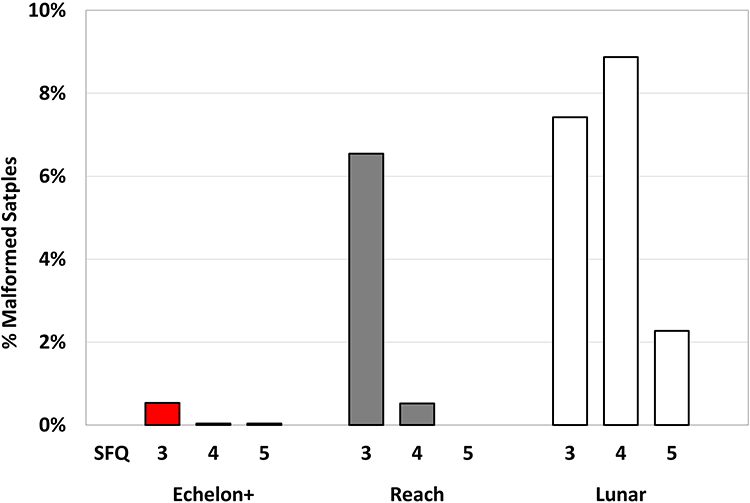 |
Figure 3 Percentage of malformed staples by SFQ (Staple Form Quality) category for Echelon+ TBGST, Reach Anzhi and Fulbright Lunar staplers in gastric tissue. |
In air leak testing in the bronchus with green reloads (Figure 4), Echelon+ TBGST had a similar mean air leak pressure to Fulbright Lunar (p = 0.187), and a 56% higher mean leak pressure than Reach Anzhi (p < 0.001). Both the Echelon+ TBGST and Fulbright Lunar had no leaking below the 88 mmHg criterion, while Reach Anzhi had a 22% rate of leaking below the criterion, significantly higher than Echelon+ TBGST (p = 0.011).
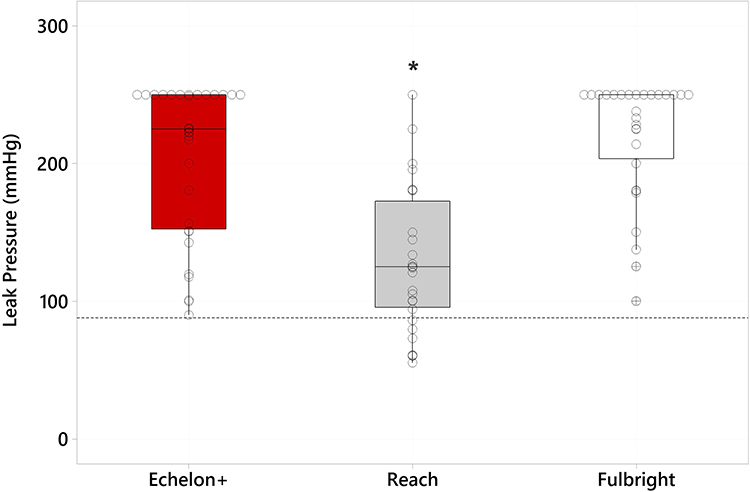 |
Figure 4 Boxplot of bronchus air leak pressures for Echelon+ TBGST, Reach Anzhi and Fulbright Lunar staplers. Dotted lines represent target minimum values of 88 mmHg. Circles represent individual points, whereas those with a cross show statistical outliers. An asterisk represents a significant difference versus Echelon+ TBGST. |
In fluid leak testing in the colon with blue reloads (Figure 5), Echelon+ TBGST had a 102% higher median leak pressure than Fulbright Lunar (p < 0.001) and 107% higher leak pressure than Reach Anzhi (p < 0.001). For the percentage of samples leaking below the 30 mmHg criterion, Echelon+ TBGST had 71% fewer leaks than Fulbright Lunar, and 76% fewer leaks than Reach Anzhi (p < 0.001).
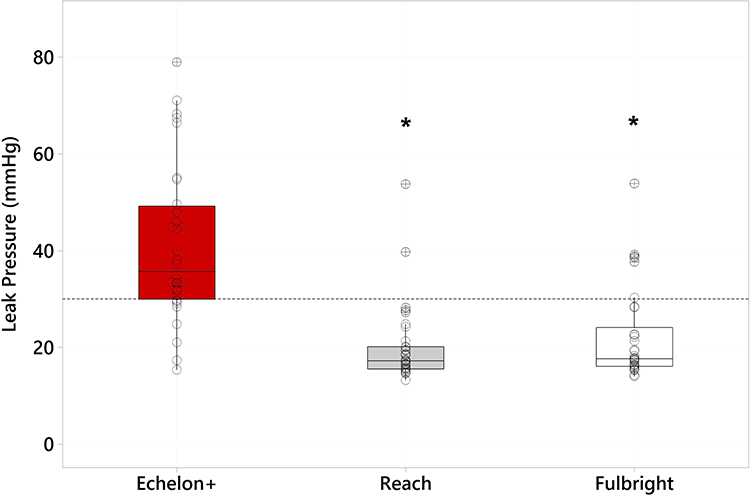 |
Figure 5 Boxplot of colon fluid leak pressures for Echelon+ TBGST, Reach Anzhi and Fulbright Lunar staplers. Dotted lines represent target minimum values of 30 mmHg. Circles represent individual points, whereas those with a cross show statistical outliers. Asterisks represent a significant difference versus Echelon+ TBGST. |
Discussion
Surgical staplers are used universally in laparoscopic procedures and are known to be reliable and convenient. Even though surgical staplers have low failure rates overall, bleeding and leakage are the leading complications that can increase the occurrence of morbidities and mortalities in surgery. Tissue thickness has been adduced as a factor in the mechanical integrity of the staple line, which may be a contributing factor to staple-line bleeding and leakage.21 In order to optimize staple formation, matching staple height to tissue thickness is the most common challenge to be overcome. Gastric tissue thickness is highly associated with difficulty in proper staple formation and serosal laceration in sleeve gastrectomy.11 Besides the gastric wall, thick tissue also is present in rectum in gastrointestinal surgery.22 The most common clinical practice scenario is transection/resection of gastrointestinal (GI) tissue and creation of anastomosis in laparoscopic procedures. GI tissues are considered biphasic with solid and liquid components, which may affect the manner in which staples are formed.23
In thoracic surgery, lung parenchyma can be thick in wedge resection depending on the cutting extension,24 and torn visceral pleura can lead to bleeding and air leakage.25,26 Bronchial stapling is another challenge in lung resection procedures, with possible post-operative complications of bronchopleural fistula formation and bleeding.7 The bronchial outer diameter is correlated with the compressed thickness, which is negatively related to the air leak pressure.27 Currently, one-third of the lung resection procedures is down-staging tumors after neoadjuvant treatment, where inflammation and fibrosis may lead to edema and adhesion, adding another factor to consider in assessing tissue and placement of stapler.28 Challenges when stapling lung tissue include slippage between the stapler surface, cartilage pieces, and mucosal tissues during firing, which may lead to malformation of staples. Increased resistance of cartilage would further lead to the possibility of penetration inconsistency of both legs and failure to align to the anvil pockets. Minor and/or major stapling failure could cause intra-operative air leak and post-operative bronchopleural fistula.7
Commonly, the staple is formed into a “B” configuration. The critical step of staple formation occurs when the anvil and sleigh are pushing staples upward and simultaneously the anvil pockets are guiding the staples into the B-shape formation. The staples are designed to be inert and are generally regarded as benign; however, slippage between the stapler surface and tissue during firing may lead to malformation of the staple. Malformed staples and their consequences have been reported in the scientific literature.29,30 Malformed staples can potentially cause detrimental adverse effects during surgery or post-operatively. Complications of malformed staples may include bleeding or the reopening of an incision if the staple line is not complete or does not hold.8
Although the thickness of gastric wall varies in patients, the thickest part is on antrum, which follows the body and fundus in a gradient manner.17 Using a pre-compression period of 15 seconds, the strength of TBGST reloads along with enhanced glass fiber technology secure tissue firmly to provide optimum B-shape staple formation. We used Staple Form Quality (SFQ), a 5-point grading scale (Figure 2), to evaluate the B-shape formation of each staple. In our study, on gastric wall with compressed thickness in range 3.0–3.3 mm, Echelon+ TBGST produced the fewest malformed staples (0.6%), compared to Reach Anzhi (7.1%, p < 0.001) and Fulbright Lunar (18.6%, p < 0.001). TBGST staple design is intended to overcome resistance of thick or rigid tissue and provide good formation with minimal chance of staple leg displacement from the pockets. Selecting the correct staple height, and an effective stapler/reload design is critical in the effort to reduce leaks31 and bleeding.15 In addition, the Echelon+ TBGST stapler is designed to decrease the firing speed when it engages thick tissues and slows down due to dynamic firing technology. The slower speed helps to improve the capture and formation of staples leading to fewer malformed staples. Better staple formation may be responsible for the higher leak pressures/lower rates of leakage observed in both bronchial and colon tissues.
The Gripping Surface Technology (GST) in TBGST reloads is designed to minimize tissue creep, while compression force is being applied. Since the GST 60 stapler was approved by the FDA in 2014 and the GST 45 stapler in 2016, GST has been added to several stapler reloads and used not only in GI tissues but also in general, thoracic, urologic and pediatric procedures on both non-vascular and vascular targeting tissues.32–35 The Echelon+ TBGST Stapler has an advanced anvil curvature as well as wide, tapered staple pockets that are designed to improve the capture and formation of staples when the stapler is fired. In addition to glass fiber technology, stapler design has continued to evolve with TBGST reloads which are designed to provide optimal staple formation even on thick tissue.
The benefit of the advanced design of the Echelon™+ stapler with Thunderbird reloads is more pronounced while stapling in thick and challenging tissues, such as stomach or bronchus. There are two key features of the new design. First, Thunderbird reloads have enhanced glass fiber technology in the sled and driver for enhanced strength which is designed to provide optimal B-shaped staple formation. Secondly, Echelon+ TBGST is designed to decrease the firing speed while engaging thick tissues. This dynamic firing helps to improve the tissue capture and optimize staple formation.
In our study, TBGST green reloads with a target stapling height of 2.0–3.3mm were applied for bronchial closure. The compressed thickness of porcine bronchus 3.0–3.3mm was up to the high limit of green reloads. TBGST green reloads showed sufficient safety and performance with 0.0% air leak at the 88 mm Hg criterion. In the comparison of onset colon fluid leak pressure, consistent with the result of SFQ testing, the fluid leak pressure for ECHELON+ stapler with TBGST reloads was significantly higher than that for Reach Anzhi and Fulbright Lunar, with significantly lower leak rates below the 30 mmHg criterion. This test mimics the methylene blue leak test to test colonic anastomotic leak intraoperatively,36 and may provide insight to clinical performance.
Limitations of the Study
Even though thick and rigid tissue, such as gastric wall, colon, and bronchus, were tested in this study, this is an ex vivo study within a controlled experimental environment. Because this is an ex vivo study, intra-operative and post-operative bleeding could not be evaluated based on the model. An in vivo study will be explored to further assess the preclinical performance of tested devices.
Conclusion
Over the last several decades significant stapler technology advancements have occurred. Recent advancements in Ethicon Echelon+ TBGST stapler and reload include gripping strength technology and enhanced tissue management during powered firing with glass fiber technology. The stapler and reload design augments the stabilization of tissue which has demonstrated a decrease in the number of staple-line interventions and resulted in fewer hemostatic complications compared to standard stapler cartridge reloads in sleeve gastrectomy procedures.12,14 The use of powered staplers has been associated with decreased hospital costs as well as improved clinical outcomes.37–39
Proper formation of each staple is the fundamental guarantee of staple-line integrity and therefore strength. The Echelon+ TBGST Stapler with Thunderbird reloads produced fewer malformed staples and had as high or higher leak pressures in bronchus and colon tissue compared to similar competitor stapling systems in benchtop analyses. Clinical studies are needed to confirm these results.
Acknowledgments
We wish to thank Alec Sun for his efforts on statistical evaluations.
Disclosure
All authors are employees of Ethicon, Inc.
References
1. Gaidry AD, Tremblay L, Nakayama D, et al. The history of surgical staplers: a combination of Hungarian, Russian, and American innovation. Am J Surg. 2019;85(6):563–566. doi:10.1177/000313481908500617
2. Saji H, Okada M, Tsuboi M, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, Phase 3, randomised, controlled, non-inferiority trial. Lancet. 2022;399(10335):1607–1617. doi:10.1016/S0140-6736(21)02333-3
3. Lee H-J, Hyung WJ, Yang HKet al. Short-Term Outcomes of a Multicenter Randomized Controlled Trial Comparing Laparoscopic Distal Gastrectomy with D2 Lymphadenectomy to Open Distal Gastrectomy for Locally Advanced Gastric Cancer (KLASS-02-RCT). LWW; 2019.s
4. Heath D, Complications arising from staple lines and anastomotes in bariatric surgery: why they happen and how to avoid them.
5. Hwa Han S, Gracia C, Mehran A, et al. Improved outcomes using a systematic and evidence-based approach to the laparoscopic roux-en-Y gastric bypass in a single academic institution. Am J Surg. 2007;73(10):955–958. doi:10.1177/000313480707301004
6. Carrasquilla C, English WJ, Esposito P, et al. Total stapled, total intra-abdominal (TSTI) laparoscopic Roux-en-Y gastric bypass: one leak in 1000 cases. Obes Surg. 2004;14(5):613–617. doi:10.1381/096089204323093372
7. Yano M, Yokoi K, Numanami H, et al. Complications of bronchial stapling in thoracic surgery. World J Surg. 2014;38(2):341–346. doi:10.1007/s00268-013-2292-2
8. Chekan E, Whelan RL. Surgical Stapling Device–Tissue Interactions: What Surgeons Need to Know to Improve Patient Outcomes. Medical Devices. Vol. 7. Auckland: NZ; 2014:305.
9. Mansour AM, El-Nashar O, El-Nahas AR, et al. pd13-11 endovascular-gia stapler device malfunction during laparoscopic nephrectomy: a comprehensive analysis of the FDA-manufacturer and user facility device experience (Maude) Database. Urol J. 2014;191(4S):e356–e356. doi:10.1016/j.juro.2014.02.996
10. Riggs MK, Bohm MR, Mountain PJ. Examining relationships between device complexity and failure modes of minimally invasive surgical staplers. In: ASME International Mechanical Engineering Congress and Exposition. American Society of Mechanical Engineers; 2016.
11. Matsuzawa F, Homma S, Yoshida T, et al. Serosal laceration during firing of powered linear stapler is a predictor of staple malformation. Surg Innov. 2017;24(6):590–597. doi:10.1177/1553350617733350
12. Fegelman E, Knippenberg S, Schwiers M, et al. Evaluation of a powered stapler system with gripping surface technology on surgical interventions required during laparoscopic sleeve gastrectomy. J Laparoendosc Adv Surg Tech. 2017;27(5):489–494. doi:10.1089/lap.2016.0513
13. Park J, Suh S-W, Kim MK, et al. Less pain and reduced risk of early postoperative ileus after clipless versus conventional laparoscopic appendectomy. surgical laparoscopy. Endosc. Percutaneous Tech. 2019;29(6):543–547. doi:10.1097/SLE.0000000000000721
14. Rawlins L, Johnson BH, Johnston SS et al. Comparative Effectiveness Assessment of Two Powered Surgical Stapling Platforms in Laparoscopic Sleeve Gastrectomy: A Retrospective Matched Study. Medical Devices. Vol. 13. Auckland: NZ; 2020:195.
15. Yeo E, Thompson J, Hanseman D, et al. Increased staple loading pressures and reduced staple heights in laparoscopic sleeve gastrectomy reduce intraoperative bleeding. Surgery. 2021;169(5):1110–1115. doi:10.1016/j.surg.2020.10.045
16. Fortin SP, Johnston SS, Chaudhuri R et al. Incidence, predictors, and economic burden of circular anastomotic complications in left-sided colorectal reconstructions involving manual circular staplers. J Med Econ. 2021;241.
17. Elariny H, González H, Wang B. Tissue thickness of human stomach measured on excised gastric specimens from obese patients. Surg Technol Int. 2005;14:119–124.
18. Henninger DD, Jones J, Clymer JW. Tighter formed staples produce stronger sealing against luminal leakage. Med Dev Diagn Eng. 2017;2:48–51.
19. Pleil JD, Ariel Geer Wallace M, Davis MD, et al. The physics of human breathing: flow, timing, volume, and pressure parameters for normal, on-demand, and ventilator respiration. J Breath Res. 2021;15(4):042002. doi:10.1088/1752-7163/ac2589
20. Rojatkar P, E henderson C, Hall S, et al. A novel powered circular stapler designed for creating secure anastomoses. Med Devices Diagn Eng. 2017;2(2):94–100. doi:10.15761/MDDE.1000123
21. Clapp B, Schrodt A, Ahmad MVet al. Stapler malfunctions in bariatric surgery: an analysis of the MAUDE database. JSLS. J Soc Laparoendosc Surg. 2022;26:1
22. Huang ZF, Vandewalle JA, Clymer JW et al. Improving performance and access to difficult-to-reach anatomy with a powered articulating stapler. Medical Devices Evidence Res. 2022;2022:329–339.
23. Baker RS, Foote J, Kemmeter P, et al. The science of stapling and leaks. Obes Surg. 2004;14(10):1290–1298. doi:10.1381/0960892042583888
24. Chekan EG, Cummings JF, Mabe I, et al. Thickness of Cadaveric Human Lung Tissue. Surg Technol Int. 2016;29:207–213.
25. Bonnet B, Tabiai I, Rakovich G, et al. Air leaks: stapling affects porcine lungs biomechanics. J Mech Behav Biomed Mater. 2022;125:104883. doi:10.1016/j.jmbbm.2021.104883
26. Takamochi K, Oh S, Miyasaka Y, et al. Prospective randomized trial comparing buttressed versus nonbuttressed stapling in patients undergoing pulmonary lobectomy. J Thorac Cardiovasc. 2014;62(08):696–704. doi:10.1055/s-0033-1363295
27. Kuroda H, Sugita Y, Nakanishi K, et al. Favorable clinical application for segmental bronchial closure based on experiment results. J Thorac Dis. 2019;11(6):2267. doi:10.21037/jtd.2019.06.18
28. Travis WD, Dacic S, Wistuba I, et al. IASLC multidisciplinary recommendations for pathologic assessment of lung cancer resection specimens after neoadjuvant therapy. J Thorac Oncol. 2020;15(5):709–740. doi:10.1016/j.jtho.2020.01.005
29. Fegelman EJ. Comment on: comparison of endostapler performance in challenging tissue applications. Surg Obes Relat Dis. 2013;9(3):421–422. doi:10.1016/j.soard.2013.01.011
30. Makanyengo SO, Thiruchelvam D. Literature review on the incidence of primary stapler malfunction. Surg Innov. 2020;27(2):229–234. doi:10.1177/1553350619889274
31. Huang R, Gagner M. A thickness calibration device is needed to determine staple height and avoid leaks in laparoscopic sleeve gastrectomy. Obes Surg. 2015;25(12):2360–2367. doi:10.1007/s11695-015-1705-8
32. Fortin SP, Petraiuolo W, Cafri G, et al. Comparison of clinical outcomes of gripping surface technology staple reloads versus standard staple reloads used with manual linear surgical staplers. Evidence Res. 2022;2022:385–399.
33. Johnston SS BH, Chakke Det al. Retrospective comparison of clinical and economic outcomes of non-donor patients undergoing radical nephrectomy using one of two different linear stapler technologies for transection of the renal vessels: fixed-height gripping surface reloads vs variable-height reloads. medical devices. Evidence Res. 2022;2022:317–328.
34. Park SY, Kim DJ, Mo Nam C, et al. Clinical and economic benefits associated with the use of powered and tissue-specific endoscopic staplers among the patients undergoing thoracoscopic lobectomy for lung cancer. J Med Econ. 2019;22(12):1274–1280. doi:10.1080/13696998.2019.1634081
35. Murakami M, Muto M, Nakagawa S, et al. Successful laparoscopy-assisted en bloc resection of bulky omental malignant lymphoma involving the ascending colon and multiple lymph node metastases: report of a technically demanding case in a pediatric patient. Asian J Endoscopic Surgery. 2022;15(4):836–840. doi:10.1111/ases.13081
36. Kryzauskas M, Degutyte A, Abeciunas V, et al. Experimental study of mechanical integrity testing in stapled large bowel: methylene blue leak test is not inferior to air leak test. Visc Med. 2021;37(3):189–197. doi:10.1159/000510660
37. Wise A, Rector J, Orr K, et al. Measuring staple line security and compression uniformity with an advanced endoscopic powered stapler. Open Access J Surg. 2021;7(2):1–5.
38. Miller DL, Roy S, Kassis ES, et al. Impact of powered and tissue-specific endoscopic stapling technology on clinical and economic outcomes of video-assisted thoracic surgery lobectomy procedures: a retrospective, observational study. Adv Ther. 2018;35(5):707–723. doi:10.1007/s12325-018-0679-z
39. Roy S, Yoo A, Yadalam S, et al. Comparison of economic and clinical outcomes between patients undergoing laparoscopic bariatric surgery with powered versus manual endoscopic surgical staplers. J Med Econ. 2017;20(4):423–433. doi:10.1080/13696998.2017.1296453
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.