")
Back to Journals » Patient Preference and Adherence » Volume 14
A Comparison of the Effects of Teach-Back and Motivational Interviewing on the Adherence to Medical Regimen in Patients with Hypertension
Authors Zabolypour S, Alishapour M, Behnammoghadam M, Abbasi Larki R , Zoladl M
Received 23 September 2019
Accepted for publication 22 January 2020
Published 26 February 2020 Volume 2020:14 Pages 401—410
DOI https://doi.org/10.2147/PPA.S231716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Soheila Zabolypour,1 Maryam Alishapour,2 Mohammad Behnammoghadam,3 Rozina Abbasi Larki,4 Mohammad Zoladl5
1Medical Surgical Nursing Department, Yasuj University of Medical Sciences, Yasuj, Iran; 2Student Research Committee, Yasuj University of Medical Sciences, Yasuj, Iran; 3Critical Department, Nursing School, Yasuj University of Medical Sciences, Yasuj, Iran; 4Urology Department, Medicine Faculty, Yasuj University of Medical Sciences, Yasuj, Iran; 5Social Determinants of Health Research Center, Yasuj University of Medical Sciences, Yasuj, Iran
Correspondence: Maryam Alishapour
Student Research Committee, Yasuj University of Medical Sciences, Yasuj, Iran
Tel/Fax +98 74 33235141
Email [email protected]
Background and Objective: Arterial hypertension is considered a chronic medical problem and also a challenging condition. The present study aimed to compare the effects of motivational interviewing and teach-back on people with hypertension.
Materials and Methods: In this clinical trial conducted in Yasuj in 2018 a total of 81 patients with essential hypertension were selected in terms of the inclusion criteria. Then, they were randomly divided into three groups: teach-back (Group 1), motivational interviewing (Group 2), and control (Group 3). Three teach-back sessions were held for the teach-back group, five sessions of motivational interviewing for the motivational interviewing group, and the routine care was provided for the control group. In addition, data were collected by the demographic form and scale of Adherence to Systemic Hypertension Treatment, which were completed by participants of all three groups at baseline and also two months from the intervention. Data were analyzed using SPSS 21 by applying descriptive statistics, one-way ANOVA, chi-squared test, Fisher’s exact test, and Bonferroni test.
Findings: Two months from the interventions, in Group 1, the score of adherence to the hypertension treatment regimen significantly increased by 816.38 points compared to the control group, in Group 2 by 1228.9 points compared to the control group, and in Group 2 by 412.6 points compared to Group 1 (p > 0.05).
Conclusion: Both teach-back and motivational interviewing increased the adherence to the hypertension treatment regimen; however, motivational interviewing was more effective compared to teach-back in boosting adherence to the hypertension treatment regimen.
Keywords: teach-back, motivational interview, hypertension, adherence
Introduction
Hypertension is a major risk factor for cardiovascular diseases, accounting for an all-cause mortality of over nine million people worldwide.1 By 2025, the prevalence of hypertension is expected to increase by 60%, affecting 1.56 billion people.2 According to the studies conducted in different provinces of Iran, the incidence rate of hypertension was estimated to be between 7% and 25% among adults, expected to be more frequent in men compared to women.3–5 The American Heart Association defined normal blood pressure as a reading of less than 120/80 mmHg, and accordingly, subjects who were in this range, are considered to be prone to hypertension or have prehypertension. In fact, arterial hypertension is a prognostic sign, which indicates that the person will be at a high risk of developing cardiovascular diseases in the future.6
In most cases, the exact etiology of hypertension is still unidentified; however in general, factors such as diseases and lifestyle including physical inactivity, bad nutrition,7 inheritance, obesity, stress, high salt intake, alcohol consumption, smoking, sleep apnea, taking herbal, and chemical medications contribute to hypertension.8
Inappropriate strategies for controlling the hypertension may increase the risk of irreversible damage to the heart, kidneys, brain, and eyes, as well as threatening the patients’ health. In some cases, if not treated, hypertension can also lead to disability and death, and also impose huge costs to the community.9
In addition, scientific evidence suggests that hypertension is controllable,10 and is largely controlled by patients.11 Nonadherence, which can be defined as a lack of concordance among patients’ behaviors and medical prescriptions, is a major issue in the care of chronic diseases.12
It was estimated that between 30% and 60% of patients with hypertension fail to adhere their treatment.13 Adherence to treatment regimen covers a wide range of individual behaviors that are in accordance with the recommendations of health care providers to follow the prescribed regimen. Adherence to regimen in hypertension implies several issues such as diet and drug regimen, sodium and fluid intake restrictions, exercise, and lifestyle changes.14
A systematic synthesis of qualitative studies showed that treatment adherence depends on four major factors as follows: structural factors, the social context, health service factors, and personal factors.15 Nowadays, training and counseling programs are important parts in managing the disease in people with chronic illnesses, to gain and maintain self-care, support, self-efficacy, and compliance skills.16 Traditional and old approaches are ineffective in promoting adherence to therapeutic interventions.17 In addition, using motivational interviewing is a good choice throughout the world, due to the high rate of early cessation of treatment, lack of adherence to treatment regimen, lack of patient participation, lack of readiness to change, recurrence of the disorder, lack of regular attendance at the medical sessions, low motivation, high levels of doubt and ambiguity, resistance, and the fear of treatment in routine procedures. Patients with certain diseases will require counselling in addition to the use of common interventions.18 Motivational interviewing is one of the most effective psychotherapies, which is a promising intervention for positive behavioral change in medicine, health, and psychiatry.19
Based on an idea that motivation comes from within the clients, we should not seek to motivate them. However, we provide conditions for them to discover their intrinsic motives, and also inform them about the difference between what is present now and what they should achieve, as well as the impact of their behaviors on the goals.20 Research evidence supports the impact of motivational interviewing in chronic patients. In the same vein, a systematic study by Knight et al indicated that motivational interviewing can have a positive effect on controlling blood pressure, diabetes, asthma, blood lipids, and cardiovascular diseases.21 In addition, Honarvar et al showed that motivational interviewing could improve the commitment to implement therapeutic interventions and blood pressure control among people with hypertension.22 According to Jackson et al, motivational interviewing can improve the physical activity in patients with type 2 diabetes.23
Studies have shown that 40–80% of patients forget their medical information immediately after they receive it and nearly half of them misunderstand the given information.24,25 Therefore, it is essential to ensure that the patients with chronic illnesses understand and remember the information including complex regimens, self-management, drug plans, and clinical status.26 Nowadays, the effectiveness of traditional and old teaching and learning methods has declined. Therefore, the teachers should use new practices and techniques to transfer their knowledge, and enhance the level of learning.27 Teach-back is an effective direct training method that can be performed individually, face-to-face, with eye contact, by the use of body language,28 and repetition of the taught materials, in order to ensure full understanding of the patient.25 Behavior can be improved in this method using mutual discussions.29 In fact, this training method is an evidence-based patient-training approach model introduced by health-care organizations as an effective way to ensure understanding and remembrance of health information.29
This training method has been used in many studies, which indicate its positive results regarding transmission of information to patients.30,31 In this regard, Dinh et alshowed that, the teach-back method generally has positive effects on a wide range of health care outcomes; however, these were not always significant.32 In addition, Salavati et al and Ghanbari et al showed that teach-back can improve the quality of life in patients with myocardial infarction, and can lead to compliance with regimen in hemodialysis patients.33,34
Given the high incidence of hypertension and its complications and major impacts on health and well-being of societies, as well as regarding previous studies that showed high rates of noncompliance of hypertensive patients with therapeutic regimen, taking different measures to prevent, control, and treat the hypertension seems to be important; and hence, it is necessary to find more effective educational methods for that. According to the conducted studies, there is no survey performed on the effect of teach-back on the adherence to treatment regimen of patients with hypertension, and also no study compared this method with motivational interviewing in Iran. Therefore, the present study aimed to compare the effects of teach-back and motivational interviewing on adherence to treatment regimen of hypertensive patients in Yasuj in 2018.
Methodology
This clinical trial included all patients with essential hypertension who were referred to Yasuj health-care centers in 2018. Totally, 81 patients were selected through convenience sampling method and were randomly divided into three equal groups of teach-back, motivational interviewing, and control (the details are presented in Figure 1). Inclusion criteria included reading and writing skills; essential hypertension according to diagnosis; not attending training programs on blood pressure in the last six months; no history of chronic diseases such as cancer, lupus, advanced heart disease, kidney disease, diabetes, stroke, kidney disease, and endocrine diseases including pheochromocytoma and Cushing’s syndrome; no contraceptive pills six months before the intervention and during the study; passing at least six months from the diagnosis of hypertension; (acquire an undesirable score (less than 50 percent from two of three scales including diet, exercise and medicines) following the questionnaires from people diet that they afflicts with hypertension Exclusion criteria);35 auditory and verbal ability; consent to participate in the study; aged between 35 and 60 years old, and the lack of psychological treatment simultaneously with the above interventions. Exclusion criteria included incompletion of a training session in both teach-back and motivational interviewing groups due to any reason; pregnancy during the study; development of known psychiatric disorders during the study; development of known progressive diseases such as cancer, lupus, advanced heart failure, kidney disease, diabetes, and stroke; drug and alcohol addiction during the study; unwillingness to continue participation in the study; hospitalization in a health facility due to illness; immigration; and death. Before the intervention and after fully explaining the study objective, the written informed consent was obtained from all participants. In addition, confidentiality of collected data as well as full autonomy of the participants to participate in or leave the study at each stage was emphasized. This study was registered at the Research Ethics Committee of the Research and Technology Deputy of Yasuj University of Medical Sciences with the code IR.YUMS.REC.1397.075 as well as in the Iranian Registry of Clinical Trials website with the code IRCT20180711040430N1.
 |
Figure 1 Consort flow diagram. |
In addition to the demographic form, the scale of Adherence to Systemic Hypertension Treatment was used to collect information. This inventory included three subscales of adherence to medication, adherence to diet, and adherence to the exercise program. The diet subscale had 34 items on the patient’s food basket, fat and salt intake, and also the consumption frequency and the amount of 30 main foods. This table was scored from 0 to 100, according to the food types (five-point Likert scale). The second subscale included 10 items about the adherence to medication in the form of a two-part six-point Likert table (the first and second parts included four and six items, respectively). This subscale was scored from 0 to 100, according to the types of the items. The third subscale included items about the exercise program such as items about time, interval, duration, and type of exercise. In the second part, in order to check adherence to the exercise program, 14 five-point Likert items were asked in the mentioned fields. Similar to two previous subscales, this subscale was scored from 0 to 100 based on the item types. Regarding the rate of adherence to treatment regimen, scores of <50%, 50–75%, and >75% were considered as unfavorable, relatively favorable, and favorable adherence, respectively. Validity and reliability of the questionnaire were investigated by Sanaie et al.36 Based on the test-retest model, the reliability of this tool was estimated as R=0.83, and the scientific validity was determined through the content validity method. It is worth noting that in the present study, the Cronbach’s alpha coefficient of the scale of Adherence to Systemic Hypertension Treatment was 0.8. Regarding the intervention method, patients in the teach-back group received face-to-face training and an educational pamphlet about hypertension. Each patient received three individual sessions of 40–45 min, which sometimes took 60 min according to the patients’ desire or to their learning level33 (Table 1).
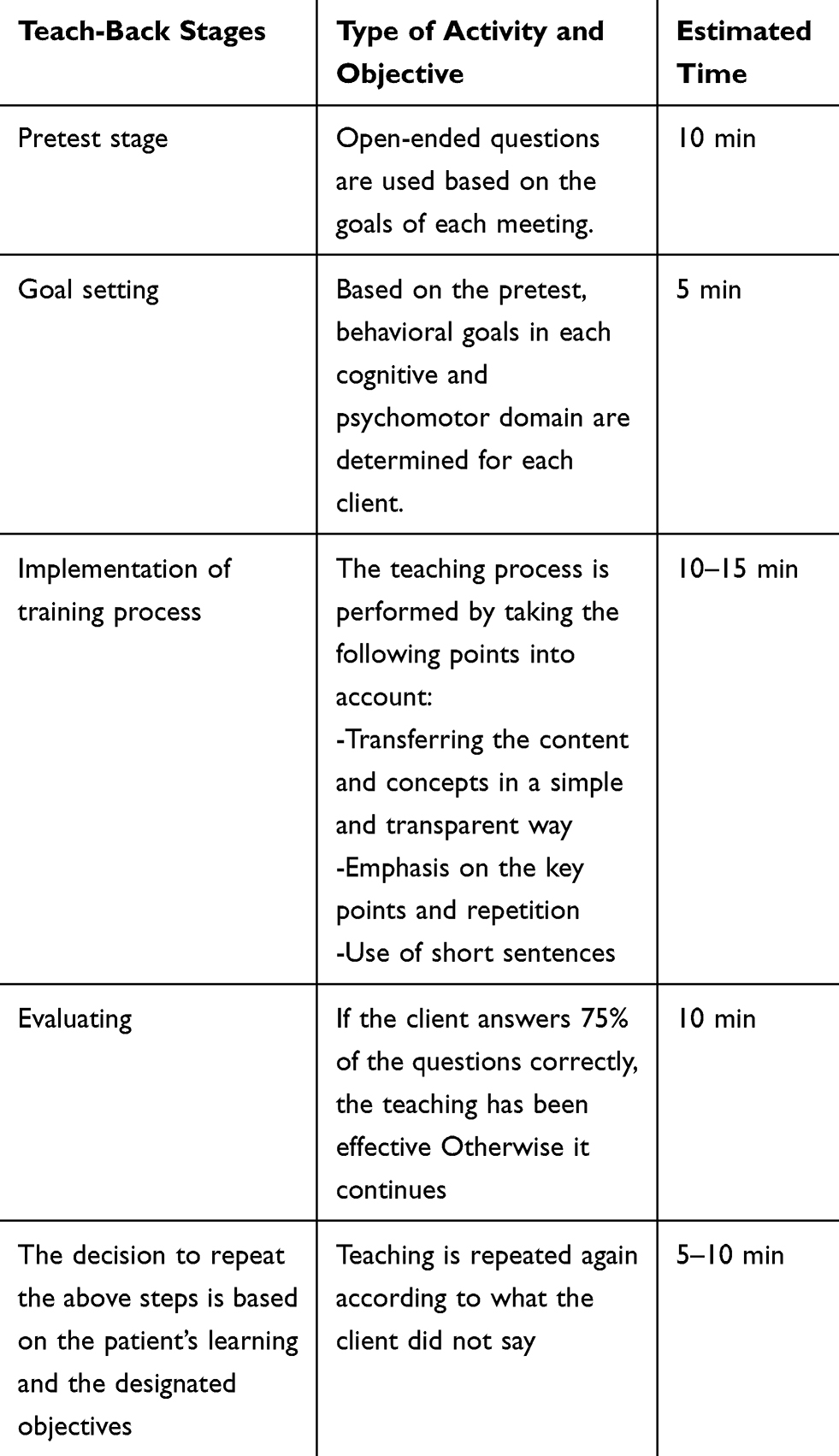 |
Table 1 The Teach-Back Training Group Intervention Protocol (in each Session) |
Hypertension, its symptoms, risk factors, and complications, and the importance of preventing and controlling them were discussed in the first session; also, nutritional skills, exercise, and its effect on blood pressure in the second session, and drugs, drug regimen, their limitations, and breaking inappropriate habits were discussed in the third session. In order to persuade the patients to observe the mentioned issues, they were called at a certain time within a month after the intervention and their questions were answered.37 In the motivational interviewing group, the structure of the motivational interviewing sessions was extracted from the work book of the five-session motivational interviewing group intervention structure, in terms of the Miller and Rollnick principles18 (Table 2).
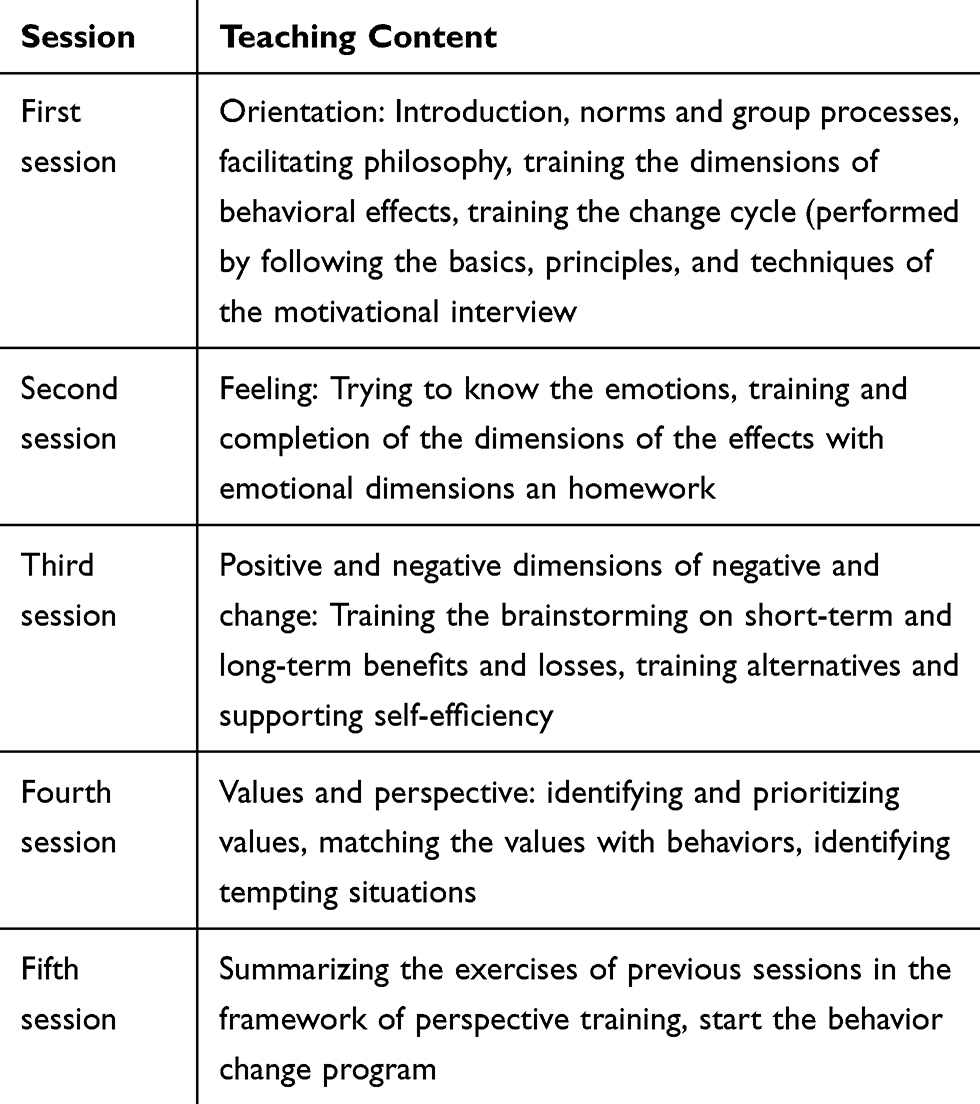 |
Table 2 The Structure of Motivational Interviewing Sessions |
Participants were enrolled in motivational interviewing by a researcher in groups of 8–12 patients for five sessions of 60 to 90 min (two sessions per week; a psychologist was attended in all sessions to assess sessions, and reduce and eliminate errors). The content of the training sessions included healthy eating habits, regular physical activity, smoking cessation, timely drug use, and stress relief.38
In the control group, patients received routine care for hypertension including training for proper drug use, diet, and exercise, as well as blood pressure checking.
Two months from the intervention, as described earlier, the scale of Adherence to Systemic Hypertension Treatment was completed by all participants as a post-test. Data were analyzed using SPSS 21 with a significance level of p>0.05 by applying one-way ANOVA, chi-squared test, Fisher’s exact test, Bonferroni post hoc test, and paired t-test.
Results
In the present study, 81 patients with hypertension were enrolled, including 25 males (30.9%) and 56 females (69.1%) with an average age of 47.4±7.4 years old. There was no significant difference among the study groups at baseline, in terms of qualitative variables such as gender, marital status, education, living conditions, employment, supportive coverage, smoking, and food preparing person (P >0/05) (Table 3).
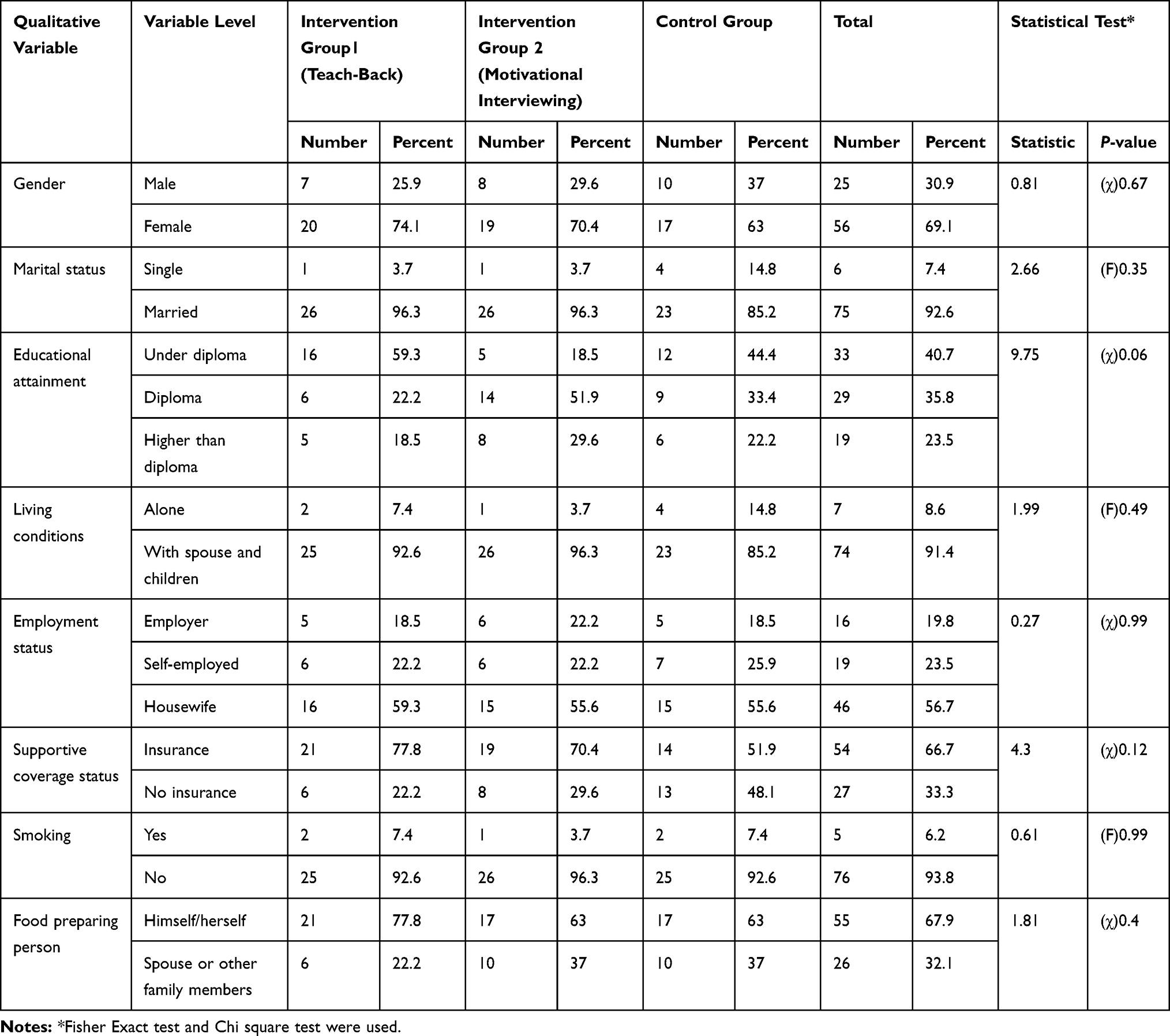 |
Table 3 Frequency Distribution and Comparison of Qualitative Demographic Variables Among Patients with Hypertension in Intervention Group 1 (Teach-Back), Group 2 (Motivational Interviewing), and Control Group at Baseline |
In addition, the score of adherence to treatment regimen and its subscales including adherence to medication, diet, and exercise program before the intervention were 2805.5±409.29, 1917.73±193.13, 530.4±125.9, and 357.4±318.66, respectively. The results of statistical descriptive statistics and one-way ANOVA showed that, at the beginning, there was no significant difference among Group 1 (teach-back), Group 2 (motivational interviewing), and control group in the mean score of adherence to treatment regimen in hypertensive patients. However, a statistically significant difference was observed between the groups two months from the intervention in the mean score of adherence to treatment regimen and its subscales (Tables 4, 5, 6).
 |
Table 4 Comparison of the Groups Adherence to Regimen and its Subscales in Patients with Hypertension at the Beginning |
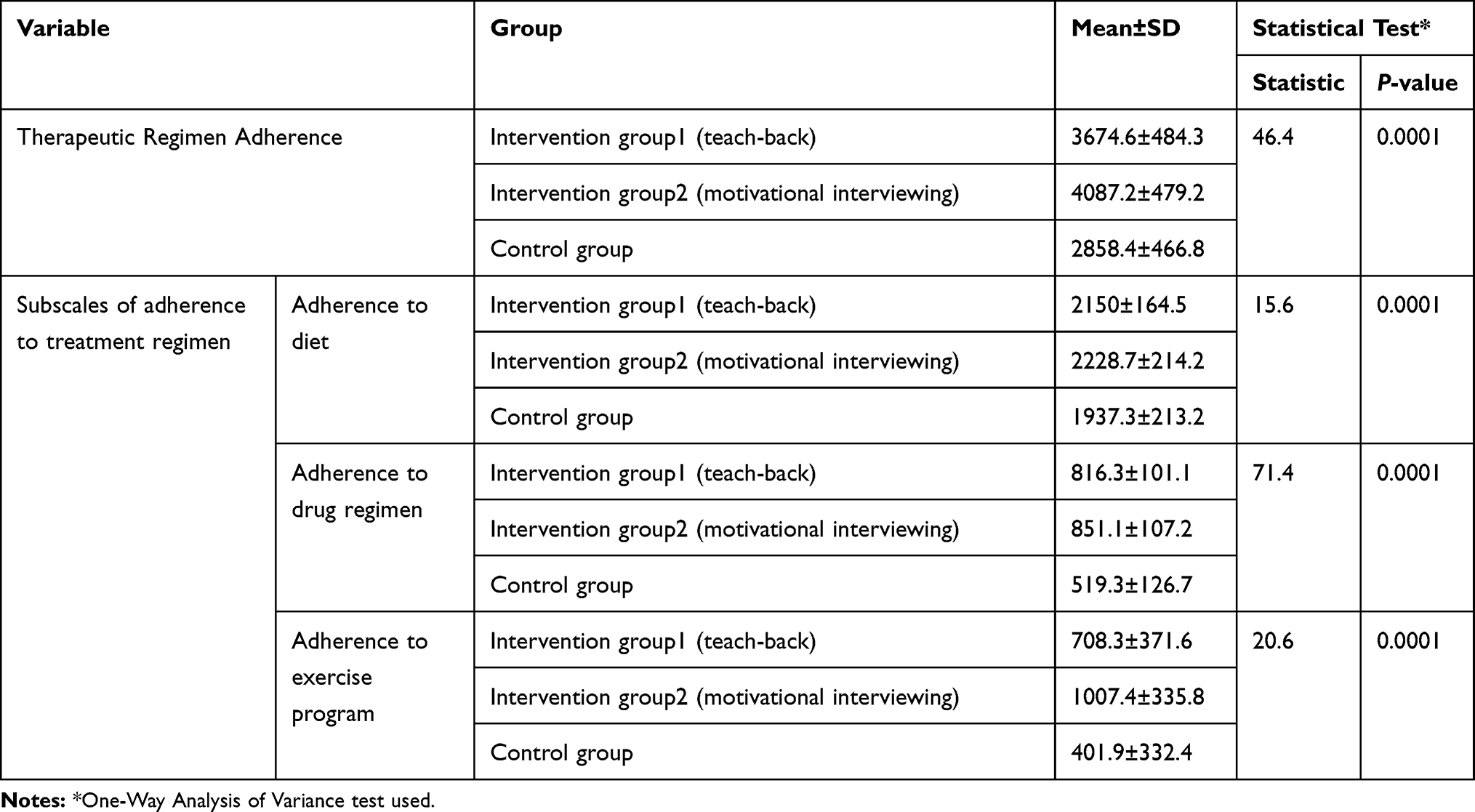 |
Table 5 Comparing the Groups Adherence to Regimen and its Subscales in Patients with Hypertension Two Months After Intervention |
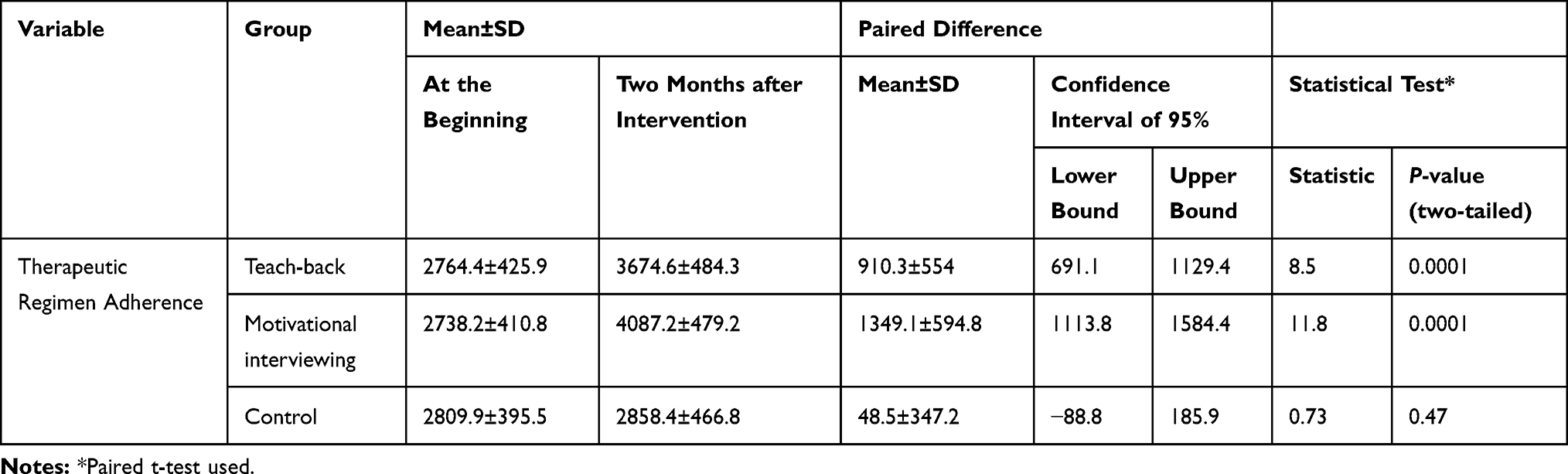 |
Table 6 Within-group Comparison of Adherence to Regimen in Patients with Hypertension in Intervention Group Teach-Back, Intervention Group Motivational Interviewing, and Control Group at the Beginning and Two Months After Intervention |
In addition, the overall mean score of adherence to treatment regimen in the motivational interviewing group was higher by 412.66, compared to the teach-back group. In addition, the intragroup comparison was performed for overall score of adherence to treatment regimen and its subscales. The results of the Bonferroni test indicated a significant increase in the mean score of adherence to treatment regimen after the intervention by 910.35±554 in Group 1 (teach-back) and 1349.1±594.8 in Group 2 (motivational interviewing). There no significant difference in the overall score of adherence to treatment regimen and its subscales between baseline and after intervention in the control group.
Discussion
The findings of this study showed that the overall mean score of adherence to treatment regimen scale was significantly higher in both experimental groups after the intervention compared to before it; however, there was no significant difference observed in the control group. Despite methodological differences such as the duration of intervention, time, and sample size; the results of this study were consistent with that of studies published on teach-back and motivational interviewing among hypertensive and nonhypertensive patients. For example, the present research was consistent with the studies by Honarvar et al,22 Ogedegbe et al39 and Ma et al17 which can be attributed to the use of similar techniques in motivational interviewing such as creating suspicion and emphasis on values. In addition to the standard structure of motivational interviewing (as in the present study), Ma et al used other educational methods such as lecture, practical demonstration, role playing, and discussion that were not performed in the present study. Moreover, Ma et al reevaluated the participants six months from the intervention; whereas, in the present study, reevaluation was performed two months after the intervention due to lack of time. Stenman et al investigated the effect of one session motivational interview on improvement of adherence to periodontal infection control, and reported that no significant difference was observed between the intervention and control groups in terms of gingivitis and platelet count; however, gingival bleeding was lower in the intervention group.40 This difference can be attributed to one session motivational interview in the study by Stenman et al.
A comparison of the present research with previous studies indicated that providing nonintensive and face-to-face motivational interviewing could change health behaviors. Motivational interviewing increases the effect and success rate of treatment programs through increasing the individual’s internal incentive and ability of changing, adhering to the treatment plan, strengthening positive behaviors, increasing concern about pressure and persuasion of unhealthy behavior, participating in work planning, reviewing the profit and loss of change, determining the core values of life, increasing the conflict between values and problematic behaviors, providing information, evaluating, and strengthening the confidence for change, and supporting the self-efficacy.41 Regarding the use of teach-back in this study, it should be noted that, given the novelty of this training method and the limited number of studies conducted on the effect of this training method on adherence to treatment regimen, we cited some studies investigating the impact of teach-back on other problems. Ghanbari et al studied the effect of teach-back on adherence to treatment regimen of dialysis patients with end-stage renal failure, and showed that teach-back can lead to adherence to treatment regimen in four domains of hemodialysis, drug regimen, fluid intake restriction, and diet in hemodialysis patients,34 which are in line with the present study. Dastoma et al reviewed the effect of group teach-back on the quality of life and re-hospitalization of the patients with heart failure, and also showed that this method, as a training strategy, can improve the quality of life and reduce re-hospitalization of the patients,42 which is consistent with the present study. Teach-back is a direct training method that can be applied as face-to-face teaching. Mahmoudi Rad et al examined the effect of teach-back on foot care in patients with type 2 diabetes. Their results showed that one and three months from intervention, the mean foot care score was significantly higher in the teach-back group compared to the control group,43 which is consistent with the present study. Ashwandi et al studied the effect of teach-back on self-care behaviors in patients with type 2 diabetes, and demonstrated that self-care training through teach-back can increase patient participation in self-care, as well as adherence to it that can increase knowledge and self-care performance of patients in terms of nutritional needs, physical activity, foot care, drug use, blood glucose control, and smoking cessation in patients with type 2 diabetes one month after intervention;44 this is in line with the present study. The advantage of this type of training is that one can discuss with patients and encourage them to change their behavior. In face-to-face training, behavior can be improved due to mutual discussions, but the difficulty is that it is time-consuming and requires human resources.45 In addition, the trainer provides patients with simple and understandable language, without using medical terms, and after completing the training, they are requested to repeat the understood subject in their own language, and if they do not understand the subject well enough, the trainer repeats the subject until full comprehension is achieved.46 Another finding of this study, although both methods of teach-back and motivational interviewing increased adherence to treatment regimen, it was higher in the motivational interviewing group.
The findings of this study indicated an increase in adherence of the patients with hypertension to the treatment regimen. Accordingly, using group motivational interviewing, which increased its effectiveness, was an advantage of this study. In addition, the present study was a complementary research for previous studies on motivational interviewing. The lack of sample attrition during intervention, stability of the intervention space, and implementation of a relatively long structure (five sessions) were other advantages of this study. However, the present research had some undeniable limitations such as errors in using the self-report questionnaire, the effect of patients’ mental and emotional conditions during completion of the questionnaire, and the impact of other communications such as media, which should be considered for the generalization of the results. Similar studies conducted on the adherence to treatment regimen of other chronic patients are recommended, as well as a study on this subject with longer follow-up periods (six months and one year).
Conclusion
Regarding the findings of this study, both teach-back and motivational interviewing may improve the adherence to treatment regimen in hypertensive patients. As treatment regimen adherence is the main goal for controlling hypertension, the use of these training methods can increase patient compliance and improve the relationship between patients and health-care providers.
Data Sharing Statement
All available data can be obtained by contacting the corresponding author. All data requests should be submitted to the corresponding author for consideration. Access to anonymized data may be granted following a review.
Acknowledgment
This paper was extracted from a Master’s thesis, and the authors express their gratitude to all patients and their families and also Yasuj Health Center staff for their help in this study, as well as the Deputy of the Research Center of Yasuj University of Medical Sciences for financial and spiritual support.
Disclosure
The authors declare no conflict of interest. The study was carried out in accordance with the principles of the Declaration of Helsinki.
References
1. Joffres M, Falaschetti E, Gillespie C, et al. Hypertension prevalence, awareness, treatment and control in national surveys from England, the USA and Canada, and correlation with stroke and ischaemic heart disease mortality: a cross-sectional study. BMJ Open. 2013;3(8):e003423. doi:10.1136/bmjopen-2013-003423
2. Jabalameli S, Moulavi H. Efficacy of cognitive-behavioral stress management intervention on quality of life and blood pressure in female patients with hypertension. Sci J Kurdistan Univ Med Sci. 2010;15(2):88–97.
3. Esteghamati A, Abbasi M, Alikhani S, et al. Prevalence, awareness, treatment, and risk factors associated with hypertension in the Iranian population: the national survey of risk factors for noncommunicable diseases of Iran. Am J Hypertens. 2008;21(6):620–626. doi:10.1038/ajh.2008.154
4. Kazemi T, Hajihosseini M, Mashreghimoghadam H, Azdaki N, Ziaee M. Prevalence and determinants of hypertension among Iranian adults, Birjand, Iran. Int J Prev Med. 2017;8.
5. Eghbali M, Khosravi A, Feizi A, Mansouri A, Mahaki B, Sarrafzadegan N. Prevalence, awareness, treatment, control, and risk factors of hypertension among adults: a cross-sectional study in Iran. Epidemiol Health. 2018;40.
6. Fuster V, Association AH. The AHA Guidelines and Scientific Statements Handbook. Wiley Online Library; 2009.
7. Ghembaza M, Senoussaoui Y, Kendouci Tani M, Meguenni K. Impact of patient knowledge of hypertension complications on adherence to antihypertensive therapy. Curr Hypertens Rev. 2014;10(1):41–48. doi:10.2174/157340211001141111160653
8. Andreoli TE, Fitz JG, Benjamin I, Griggs RC, Wing EJ. Andreoli and Carpenter’s Cecil Essentials of Medicine E-Book. Elsevier Health Sciences; 2010.
9. Lackland DT, Weber MA. Global burden of cardiovascular disease and stroke: hypertension at the core. Can J Cardiol. 2015;31(5):569–571. doi:10.1016/j.cjca.2015.01.009
10. Chiong JR. Controlling hypertension from a public health perspective. Int J Cardiol. 2008;127(2):151–156. doi:10.1016/j.ijcard.2007.10.039
11. Kamran A, Sharifirad G, Mohebi S. Psychometric assessment of nutritional knowledge, illness perceptions and dietary adherence in hypertensive patients—Ardabil. Health Syst Res. 2013;1774–1785.
12. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; 2003.
13. Baggarly SA, Kemp RJ, Wang X, Magoun AD. Factors associated with medication adherence and persistence of treatment for hypertension in a Medicaid population. Res Social Adm Pharm. 2014;10(6):e99–e112. doi:10.1016/j.sapharm.2014.02.002
14. Sotodeh Asl N, Neshat Dost H, Kalantery M, Talebi H, Khosravi A. Comparison of the effectiveness of cognitive behavioral therapy and medication on the quality of life in the patients with essential hypertension. Koomesh. 2010;11(4):294–301.
15. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238. doi:10.1371/journal.pmed.0040238
16. Desnous B, Bourel-Ponchel E, Raffo E, Milh M, Auvin S. Assessment of education needs of adolescents and parents of children with epilepsy. Rev Neurol (Paris). 2013;169(1):67–75. doi:10.1016/j.neurol.2012.03.011
17. Ma C, Zhou Y, Zhou W, Huang C. Evaluation of the effect of motivational interviewing counselling on hypertension care. Patient Educ Couns. 2014;95(2):231–237. doi:10.1016/j.pec.2014.01.011
18. Navidiyan A, Pour Sharifi H. Practical guide to Motivational Interviewing. Zahedan: Sokhan Gostar Pub. 2012:98–166.
19. Cummings SM, Cooper RL, Cassie KM. Motivational interviewing to affect behavioral change in older adults. Res Soc Work Pract. 2009;19(2):195–204. doi:10.1177/1049731508320216
20. Bricker J, Tollison S. Comparison of motivational interviewing with acceptance and commitment therapy: a conceptual and clinical review. Behav Cogn Psychother. 2011;39(5):541–559. doi:10.1017/S1352465810000901
21. Knight K, McGowan L, Dickens C, Bundy C. A systematic review of motivational interviewing in physical health care settings. Br J Health Psychol. 2006;11(2):319–332. doi:10.1348/135910705X52516
22. Honarvar M, Ariaie M, Bordi R, Kamran A. Effect of motivational interviewing on adherence to treatment in patients with hypertension. Horiz Med Sci. 2015;21(3):213–220. doi:10.18869/acadpub.hms.21.3.213
23. Jackson R, Asimakopoulou K, Scammell A. Assessment of the transtheoretical model as used by dietitians in promoting physical activity in people with type 2 diabetes. J Hum Nutr Diet. 2007;20(1):27–36. doi:10.1111/jhn.2007.20.issue-1
24. Wilson FL, Baker LM, Nordstrom CK, Legwand C. Using the teach-back and orem’s self-care deficit nursing theory to increase childhood immunization communication among low-income mothers. Issues Compr Pediatr Nurs. 2008;31(1):7–22. doi:10.1080/01460860701877142
25. Sudore RL, Schillinger D. Interventions to improve care for patients with limited health literacy. J Clin Outcomes Manag. 2009;16(1):20.
26. White M, Garbez R, Carroll M, Brinker E, Howie-Esquivel J. Is “teach-back” associated with knowledge retention and hospital readmission in hospitalized heart failure patients? J Cardiovasc Nurs. 2013;28(2):137–146. doi:10.1097/JCN.0b013e31824987bd
27. Naghibi A, Alizadeh M, Faghrzadeh H, et al. Efficacy of the two educational methods: traditional and electronic techniques in training of nutritional aspect to healthy life style in elderly. Iran J Diabetes Metab. 2013;13(1):9–20.
28. Hasanzadeh F, Shamsoddini S, Moonaghi HK, Ebrahimzadeh S. A comparison of face to face and video-based education on attitude related to diet and fluids adherence in hemodialysis patients. Horiz Med Sci. 2011;17(3):34–43.
29. Kripalani S, Bengtzen R, Henderson LE, Jacobson TA. Clinical research in low-literacy populations: using teach-back to assess comprehension of informed consent and privacy information. IRB Ethics Hum Res. 2008;30(2):13–19.
30. Nasiri A. Effect of an educational plan based on Teach-Back method on hemodialysis patients’ Self-care deficits. Mod Care J. 2012;9(4):344–354.
31. Howie-Esquivel J, White M, Carroll M, Brinker E. Teach-back is an effective strategy for educating older heart failure patients. J Card Fail. 2011;17(8):S103. doi:10.1016/j.cardfail.2011.06.345
32. Dinh TTH, Bonner A, Clark R, Ramsbotham J, Hines S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: a systematic review. JBI Database Syst Rev Implement Rep. 2016;14(1):210–247. doi:10.11124/jbisrir-2016-2296
33. Salavati M, Khatiban M, Moghadari KB, Soltanian A. Evaluating the effect of teach back education on self-care behaviours and quality of life in patients with myocardial infarction in 2015: A randomised controlled trial. Sci J Hamadan Nurs Midwifery Fac. 2017;25(1):1–8. doi:10.21859/nmj-25011
34. Ghanbari A, Tabrizi KN, Dalvandi A, Kavari SH, Noroozi M. Effect of an educational program based on the teach-back method on adherence to treatment regimen in dialysis patients with end stage renal disease referred to sina hospital during 2015–2016. Urmia Nurs Midwifery Fac. 2017;15(9):688–695.
35. Sookhak F. The effect of cognitive-behavioral intervention on adherence to therapeutic regimen and remove of related barriers in hemodialysis patients. Tehran Univ Med Sci. 2013.
36. Sanaie N, Nejati S, Zolfaghari M, Alhani F, Kazemnezhad A. The effects of family-based empowerment on family cooperation in following patient treatment regime after coroner arteries bypass surgery. Mod Care J. 2014;11(1):19–27.
37. Ataee E, Haghjoo M, Dalvandi A, Bakhshandeh H. Effect of self-care education on quality of life among patients with permanent pacemaker. Iran J Cardiovasc Nurs. 2013;1(4):40–47.
38. Ossman SS. Motivational interviewing: a process to encourage behavioral change. Nephrol Nurs J. 2004;31(3):346.
39. Ogedegbe G, Chaplin W, Schoenthaler A, et al. A practice-based trial of motivational interviewing and adherence in hypertensive African Americans. Am J Hypertens. 2008;21(10):1137–1143. doi:10.1038/ajh.2008.240
40. Stenman J, Lundgren J, Wennström JL, Ericsson JS, Abrahamsson KH. A single session of motivational interviewing as an additive means to improve adherence in periodontal infection control: a randomized controlled trial. J Clin Periodontol. 2012;39(10):947–954. doi:10.1111/j.1600-051X.2012.01926.x
41. Navidian A, Abedi M, Baghban I, Fatehizadeh M, Poursharifi H. Effect of motivational interviewing on blood pressure of referents suffering from hypertension. Trauma Mon. 2010;2010(2, Summer):115–121.
42. Dastoom M, Elahi N, Baraz S, Latifi SM. The effects of group education with the teach-back method on hospital readmission rates of heart failure patients. JJCDC. 2016;5:1. doi:10.5812/jjcdc.
43. Mahmoudirad G, Hoseini MS, Madarshahian F. The effect of teach-back education on foot self-care among npatients with type ii diabetes mellitus. Patient Educ Couns. 2015;98(8):977–983. doi:10.1016/j.pec.2015.03.008
44. Oshvandi K, Jokar M, Khatiban M, Keyani J, Yousefzadeh MR, Sultanian AR. The effect of self care education based on teach back method on promotion of self care behaviors in type ii diabetic patients: a clinical trial study. Iran J Diabetes Metab. 2014;13(2):131–143.
45. Burkhart JA. Training nurses to be teachers. J Contin Educ Nurs. 2008;39(11):503–510. doi:10.3928/00220124-20081101-02
46. Mahramus T, Penoyer DA, Frewin S, Chamberlain L, Wilson D, Sole ML. Assessment of an educational intervention on nurses’ knowledge and retention of heart failure self-care principles and the Teach Back method. Heart Lung. 2014;43(3):204–212. doi:10.1016/j.hrtlng.2013.11.012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.