Back to Journals » Drug Design, Development and Therapy » Volume 20
A Comparison of Oliceridine versus Sufentanil for Patient-Controlled Analgesia After Total Knee Arthroplasty in Elderly Patients: A Double-Blinded Randomized Controlled Study
Authors Liu X, Wang S, Chen X, Tian Y, Sun J, Wang A, Li Q, Zhang H
Received 10 December 2025
Accepted for publication 23 March 2026
Published 31 March 2026 Volume 2026:20 587944
DOI https://doi.org/10.2147/DDDT.S587944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Xi Liu,1,* Suna Wang,2,* Xiaoxiao Chen,1,* Yuanyuan Tian,1 Junli Sun,1 Aizhong Wang,1 Qi Li,1 Hui Zhang1
1Department of Anesthesiology, Shanghai Sixth People’s Hospital Affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Clinical Research Center, Shanghai Sixth People’s Hospital Affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Zhang, Shanghai Sixth People’s Hospital Affiliated with Shanghai Jiao Tong University School of Medicine, No. 600, Yishan Road, Xuhui District, Shanghai, People’s Republic of China, Tel +86 18930173683, Email [email protected] Qi Li, Shanghai Sixth People’s Hospital Affiliated with Shanghai Jiao Tong University School of Medicine, No. 600, Yishan Road, Xuhui District, Shanghai, People’s Republic of China, Tel +86 18930173681, Email [email protected]
Purpose: Oliceridine is a G protein-biased μ-opioid receptor agonist, maintaining potent analgesic effects and simultaneously lessening disadvantageous reactions. This study is intended to compare Oliceridine and sufentanil patient-controlled analgesia (PCA) for postoperative analgesia in elderly patients suffering from knee arthroplasty.
Patients and Methods: A total of 138 patients scheduled for knee arthroplasty were randomized to receive postoperative PCA with either Oliceridine (2 μg kg− 1 mL− 1) or sufentanil (0.02 μg kg− 1 mL− 1). To preserve blinding, identical volume-based settings (mL) were used for both groups. The PCA regimen comprised a 1 mL loading dose (equivalent to 2 μg kg− 1 Oliceridine or 0.02 μg kg− 1 sufentanil), a background infusion of 2 mL h− 1, and a 2 mL bolus dose with a 10-minute lockout interval. Outcomes for systematic assessment included the sum of pain intensity difference (SPID), numeric rating scale (NRS) scores, and the incidence of postoperative nausea, vomiting and respiratory depression.
Results: Subjects in this research were 71.5 years on average, and 83% were female. Throughout 48 h postoperatively, the mean difference between Group Oliceridine and Group sufentanil was − 7.13 (95% CI: − 24.26 to 10.00); the upper bound of the 95% CI did not exceed the pre-specified non-inferiority margin of 10, thereby meeting the non-inferiority criterion. Aside from that, nausea (33.33% vs. 50.72%; P = 0.039) and vomiting (14.49% vs. 34.78%; P = 0.006) presented much lower incidence in Group Oliceridine within 48 h postoperative.
Conclusion: Oliceridine may have non-inferior analgesic efficacy to sufentanil and is associated with a lowered incidence of nausea and vomiting within 48 h.
Plain Language Summary: Many older adults need strong pain relief after knee replacement surgery. While common opioid pain medications work well, they often cause bothersome side effects like nausea and vomiting. Finding a pain control option that is both effective and easier to tolerate is an important goal. Our research team compared a newer pain medication, oliceridine (also known as TRV130), with a commonly used opioid, sufentanil. We studied 138 older patients who used a patient-controlled pump to manage their pain for two days after knee surgery. We tracked how their pain was controlled and recorded any side effects. We found that pain relief with oliceridine was non-inferior to sufentanil. The key difference was in side effects: significantly fewer patients who received oliceridine experienced nausea or vomiting. This means that for older adults recovering from knee surgery, oliceridine offers a potentially better-tolerated choice for effective pain control, with less of the stomach-related side effects that can make recovery unpleasant.
Keywords: patient-controlled analgesia, oliceridine, pain measurement, postoperative nausea and vomiting, PONV, TRV130
Introduction
Total knee arthroplasty (TKA) is the primary treatment for elderly patients with end-stage knee osteoarthritis.1 These patients normally experience moderate to severe pain after surgery, which considerably impedes recovery, compromises satisfaction, and adversely affects overall outcomes.2,3 Notwithstanding the fundamental fact that regional nerve blocks are extensively employed for postoperative pain management in our clinical daily, a multitude of patients still report moderate to severe pain within the first 24 to 48 hours (h) after surgery. At present, the mainstream clinical regimen is dependent upon sufentanil delivered via patient-controlled analgesia (PCA) pumps in conjunction with nonsteroidal anti-inflammatory drugs. Nonetheless, opioid-related adverse events (ORAEs) remain principal concerns attributable to the activation of the β-arrestin pathway.4,5 And elderly patients are particularly vulnerable to ORAEs due to factors such as declining organ function, reduced physiological reserve, increased comorbidity burden, frailty, and age-related pharmacokinetic and pharmacodynamic changes.6,7
Oliceridine serves as a G protein-biased μ-opioid receptor agonist,8,9 first reported in 2013 and approved by the U.S. Food and Drug Administration in 2020.10,11 As the first novel analgesic that selectively activates G protein signaling while limiting β-arrestin recruitment, Oliceridine not only maintains potent analgesic effects, but also substantially lowers the risk of unfavorable reactions.12–14 As indicated by preclinical and early clinical studies, Oliceridine optimizes μ-opioid receptor function through its G protein-biased mechanism, demonstrating advantages in both maintaining analgesic efficacy and improving safety profile.13–17 It is even well-tolerated in special populations such as the elderly and obese patients.18
Existing studies have commonly used the conventional opioid morphine as a control. Nonetheless, sufentanil has been universally employed in clinical practice on account of its higher therapeutic index and shorter plasma-to-central nervous system equilibrium half-life (t½ke0),19 which contribute to a superior safety profile. This phenomenon is more striking in postoperative PCA pumps. In such cases, sufentanil gains progressively extensive application scopes in contrast to morphine. Considering its prominent status as a dominant analgesic, a question arises from the public and the academic society: how is the novel agent Oliceridine comparable with sufentanil?
As a consequence, this study seeks to evaluate the efficacy and side effects of Oliceridine for postoperative analgesia of the elderly undergoing TKA in contrast to sufentanil.
Materials and Methods
Trial Design and Ethics Approval
This was a single-center, prospective, double-blinded, randomized controlled, non-inferiority study with a 1:1 allocation ratio. The study was approved by the Ethical Committee of Shanghai Sixth People’s Hospital, affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai, China (Chairperson: Prof. Weiping Jia) on September 23, 2024 (approval number: 2024–169-(1)) and registered with the Chinese Clinical Trial Registry (http://www.chictr.org.cn/index.aspx, registration number: ChiCTR2500099271; principal investigator: HZ; registration date:2025–03-20). All participants provided written informed consent before their inclusion in the study. This manuscript adheres to the principles of the Helsinki Declaration and complies with the Consolidated Standards of Reporting Trials guidelines.
Participants
Eligible patients were aged 65 years or older, had an ASA physical status of I or II, and a body mass index (BMI) ranging from 19.0 to 30.0 kg m−2 at screening. They were recruited to undergo elective knee arthroplasty. The exclusion criteria were as follows: refusal to participate; participation in other drug trials within 30 days before enrollment; contraindications to the study medications; history of opioid addiction; chronic analgesic use; severe hepatic or renal dysfunction; history of vestibular disorders or presence of dizziness, nausea, retching, or vomiting within one week prior to enrollment; history of obstructive sleep apnea syndrome; history of alcohol, drug, or medication withdrawal within the past three years; and postoperative detection of nerve injury or other serious complications. All participants were recruited from Shanghai Sixth People’s Hospital, affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai, China. The recruitment was completed from March 21, 2025, to August 6, 2025. All the participants underwent follow-up from March 21, 2025, to August 8, 2025. After the predetermined sample size was reached, the trial would be terminated accordingly.
Randomisation and Blinding
Allocation concealment was ensured by an independent researcher. This researcher generated a 1:1 computer-based randomization schedule using Microsoft Excel. The allocation sequence was then kept strictly concealed in a password-protected electronic file, accessible only to this individual. On the day of surgery, after a patient was enrolled, the same independent researcher would open this file, prepare the PCA pump with Oliceridine (2 μg kg−1 mL−1) (Nhwa Pharma. Corporation, Jiangsu, China) or sufentanil (0.02 μg kg−1 mL−1) (Humanwell Healthcare (Group). Corporation, Jiangsu, China) according to the next assignment on the concealed list, and then provide it to the attending anesthesiologist. To preserve blinding, identical volume-based pump settings (mL) were used for both groups. The PCA regimen comprised a 1 mL loading dose (equivalent to 2 μg kg−1 Oliceridine or 0.02 μg kg−1 sufentanil), a background infusion of 2 mL,−1 and a 2 mL bolus dose (equivalent to 4 μg kg−1 Oliceridine or 0.04 μg kg−1 sufentanil) with a 10-minute lockout interval. Everyone else involved, like patients, surgeons, and post-anesthesia care unit (PACU) nurses, did not know which group each participant was in.
Intervention
All participants adhered to the usual preoperative fasting rule (6 h no solids, 2 h no colored fluids) and took no premeds. Once in the operating room, regular ASA monitors were put on, and an intravenous access was started. General anesthesia was induced intravenously using dexamethasone (5 mg), propofol (2 mg kg−1), sufentanil (0.3 μg kg−1), and rocuronium (0.6 mg kg−1). Mechanical ventilation was started by using 6–8 mL kg−1 tidal volume and 10–12 breaths each minute. The anesthesia was sustained by using propofol, sufentanil, and sevoflurane, aiming for a bispectral index of 40–60. Three investigators, each with over five years’ clinical experience, handled all anesthetic tasks, while four skilled surgeons performed the surgeries.
Patients underwent monitoring in the PACU one hour subsequent to surgery. When leaving, all patients were awake and could clearly tell the investigator how much pain they felt. A prepared PCA electronic pump was subsequently initiated for postoperative pain control, and both patients and their family members were instructed on its appropriate use. Follow-up assessments were conducted at 3, 8, 24, and 48 h postoperatively. Pain intensity was assessed by employing the numeric rating scale (NRS, ranging from 0 to 10). Subjects with an NRS score > 4 received 40 mg parecoxib sodium as rescue analgesia, with additional doses administered as needed.20,21 If ineffective, 100 mg tramadol was administered. Severe nausea and vomiting were treated with 5 mg tropisetron. All interventions and observations were accurately recorded, and any other adverse reactions were promptly managed with appropriate symptomatic treatment and documented.
Outcomes and Data Collection
The primary outcome of this study was the sum of pain intensity difference (SPID) of NRS at rest state during 48 h postoperatively. Secondary outcomes included: (a) SPIDs and NRS at rest state during 3 h, 8 h, and 24 h postoperatively; (b) SPIDs and NRS at active state during 3 h, 8 h, 24 h and 48 h postoperatively; (c) the incidence of nausea and vomiting within 48 h; and (d) the incidence of respiratory depression (SPO2 <90% or respiratory rate of <8 breaths/min) within 48 h. All unfavorable events were recorded. The SPID for a given time interval (t) is calculated as follows: SPIDt =Σ(NRSti − NRSbaseline) × (ti − ti−1).
Demographic and baseline characteristics of the patients were systematically recorded, encompassing age, sex, height, weight, ASA physical status, and duration of surgery. Additionally, intraoperative sufentanil consumption and other analgesic medications administered on the ward were also documented.
Sample Size
We assumed a mean difference of −12.77 and a pooled standard deviation of 36.37 for the primary endpoint between the Oliceridine and sufentanil groups according to previous study and our pretrial.20 Subsequently, a two-sample non-inferiority t-test was carried out by using a one-sided alpha of 0.025, power of 90%, a non-inferiority margin of 10, and a 1:1 allocation ratio. The margin of Δ=10 was determined by applying a 60% retention factor to the 48-hour SPID difference between morphine and placebo (M1 = −27.7) reported in prior evidence.20 The calculation, performed with PASS software, indicated a requirement of 55 subjects per group. To account for a potential 20% dropout rate, the total sample size was increased to 138 subjects, with 69 allocated to each group.
Statistical Analysis
Baseline characteristics and all outcomes were summarised as mean (standard deviation, SD) or median (interquartile range, IQR) for continuous variables, and count (percentage) for categorical variables. With regard to primary outcome, non-inferiority was declared if the upper bound of the two-sided 95% confidence interval (CI) for the mean difference in the primary outcome did not exceed the pre-specified non-inferiority margin of 10 in the intent-to-treat set. With respect to secondary outcomes, continuous variables with a normal distribution were compared by carrying out the independent samples t-test. Those with a non-normal distribution were compared by conducting the Mann–Whitney U-test. Categorical variables, including secondary and safety outcomes, were analyzed by performing the Chi-square test or Fisher’s exact test, as appropriate. A post hoc sensitivity analysis was performed using a linear regression model to adjust for the intraoperative dose of sufentanil. Statistical significance was defined as a two-sided P value < 0.05 and all analyses were performed using R software (version 4.4.2).
Results
After screening 186 patients, 138 subjects were enrolled in this study ultimately, and then randomly assigned to Group Oliceridine (n=69) and Group sufentanil (n=69) (Figure 1). No participants were lost to follow-up. The intention-to-treat set and per-protocol set comprised the same 138 participants. The mean age of subjects was 71.5 (SD 4.8) years, and 83% were female. There were no significant differences in the baseline characteristics of patients, types of surgery and postoperative medication between these two groups. Nevertheless, Group sufentanil had a lower dose of sufentanil during the surgery period (Table 1).
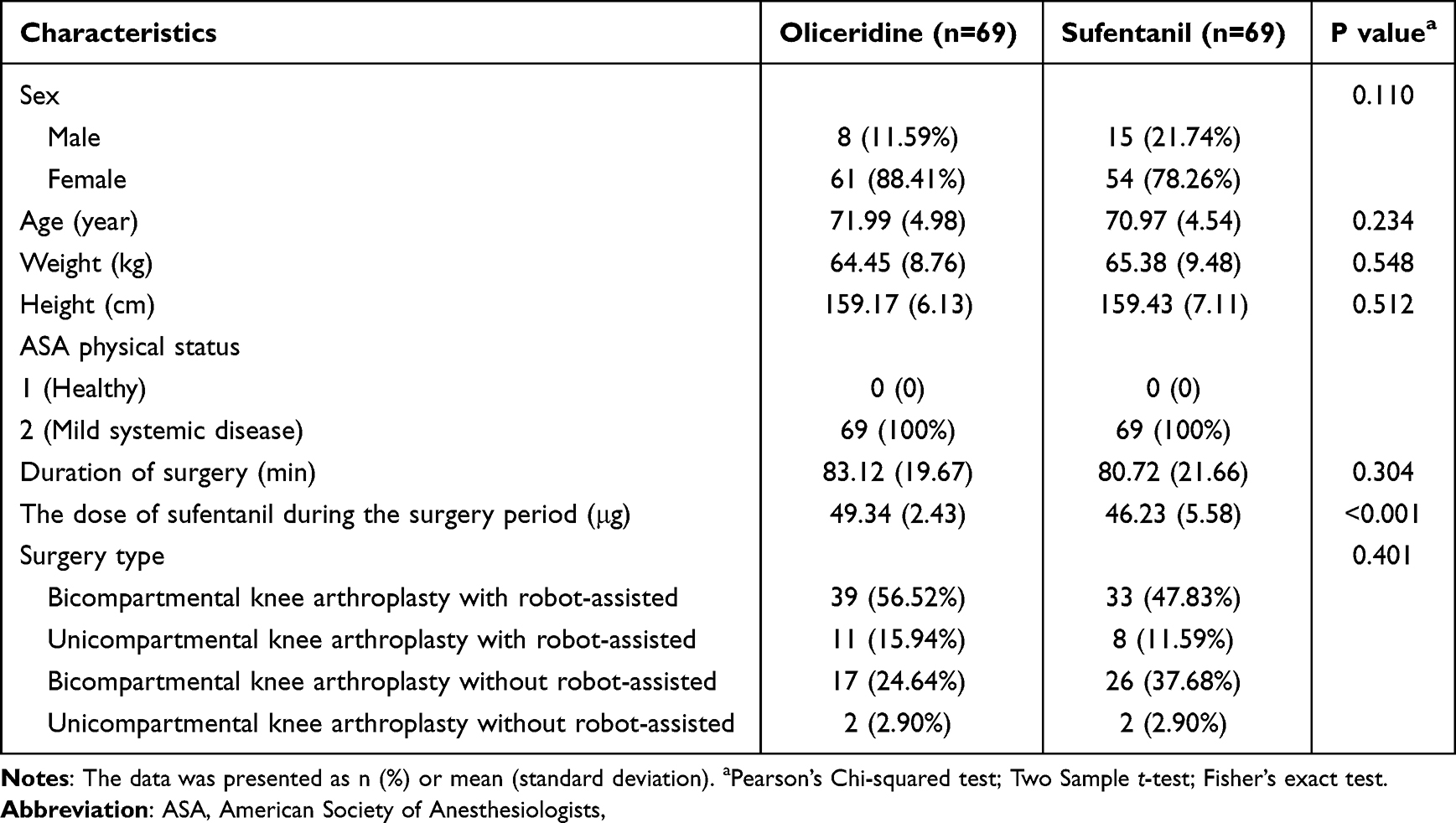 |
Table 1 Basic Characteristics |
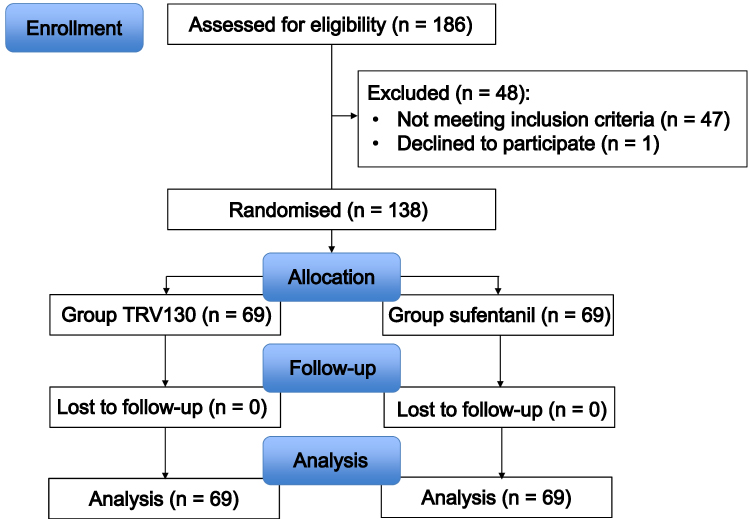 |
Figure 1 The Study flow diagram. |
For primary outcome, the rest state SPID during 48 h postoperatively (rSPID48h) was 135.36 (47.63) in Group Oliceridine versus 142.49 (53.91) in Group sufentanil (Figure 2). The mean difference between these two group was −7.13 (95% CI: −24.26 to 10.00). The upper bound of the 95% CI did not exceed the pre-specified non-inferiority margin of 10, which confirmed non-inferiority (P for non-inferiority: 0.025). The SPIDs at other time points including rest or active state displayed no conspicuous distinction between Group Oliceridine and Group sufentanil. Given the significant difference between the two groups in intraoperative sufentanil dose, a post hoc analysis adjusting for this confounder showed that the mean difference for rSPID48h failed to meet the non-inferiority criterion (mean difference, −2.45; 95% CI, −20.60 to 15.70) (Supplemental Table 1).
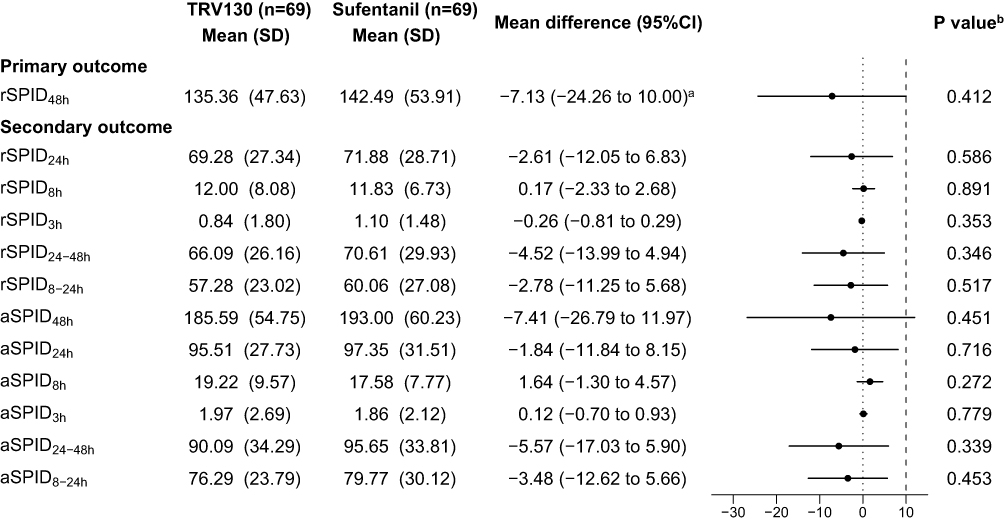 |
Figure 2 Comparison of SPIDs between treatment groups. Data are mean (SD) or mean difference (95% CI). aThe upper bound of the 95% confidence interval for rSPID48h was 9.9977, which is less than the non-inferiority margin of 10 that had been pre-specified. The P value for the non-inferiority test was 0.02498. bTwo-sided independent t-test. Abbreviations: rSPID, resting summed pain intensity difference; aSPID, active summed pain intensity difference; CI, confidence interval. |
Consistent with the SPID results, NRS scores at rest and during activity showed no significant difference between the Oliceridine and Sufentanil groups at any time point. As illustrated by our observations, while the vast majority of patients were pain-free at 1 h postoperative (The median (first quartile, third quartile)) of both groups were 0.00 (0.00, 0.00) no matter at rest or active), pain intensity increased thereafter. This trend was most pronounced during activity, with a marked rise after 8 h postoperative (aNRS8h: 4.00 (2.00, 4.00) vs. 3.00 (2.00, 4.00), aNRS24h: 5.00 (4.00, 6.00) vs. 5.00 (4.00, 6.00), aNRS48h: 4.00 (3.00, 4.00) vs. 4.00 (3.00, 5.00)) (Table 2).
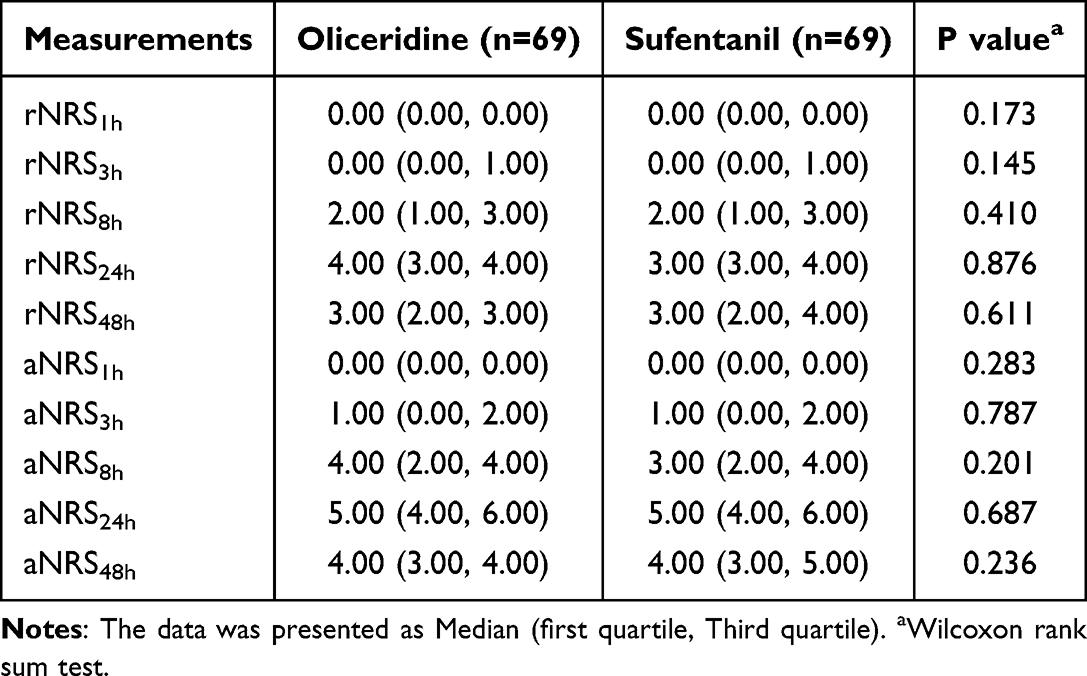 |
Table 2 The Numeric Rating Scale of Each Time-Point at Rest or Active State |
For safety outcome, nausea occurred in 23 (33.33%) participants in Group Oliceridine and 35 (50.72%) participants in Group sufentanil within 48 h postoperatively; vomiting occurred in 10 (14.49%) participants in Group Oliceridine and 24 (34.78%) participants in Group sufentanil. The incidence of nausea and vomiting within 48 hours postoperatively was much lower in the Oliceridine group than in the sufentanil group (P = 0.039 and P = 0.006, respectively). No cases of respiratory depression were observed in either group (Table 3).
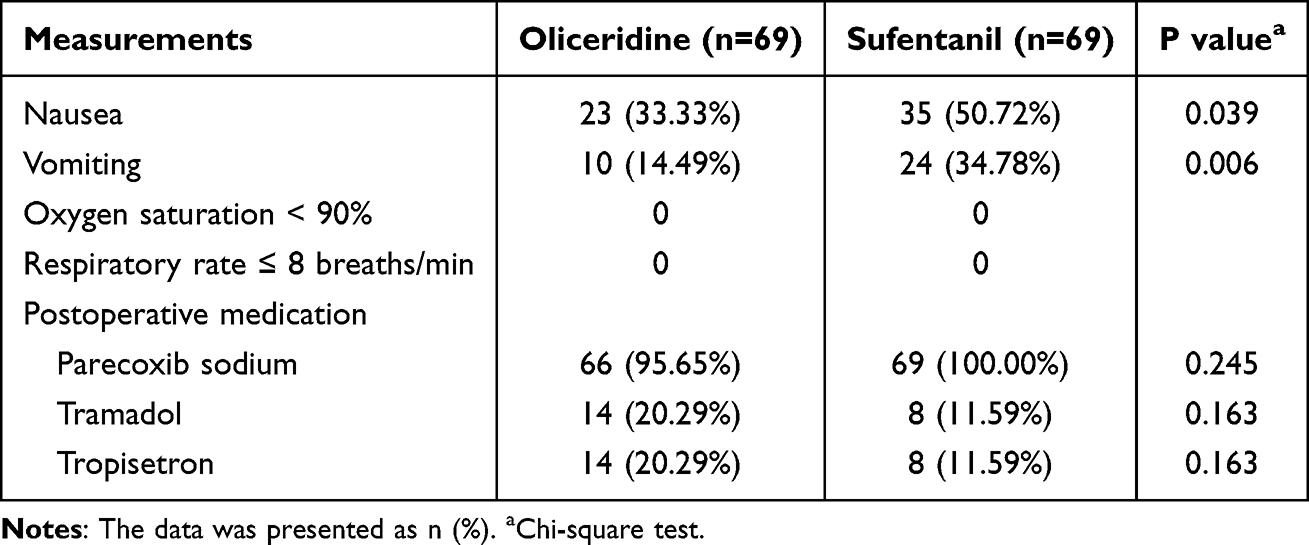 |
Table 3 The Other Secondary Outcomes |
Discussion
To our knowledge, we report the first randomized trial comparing a Oliceridine-based patient-controlled analgesia (PCA) pump with a sufentanil-based PCA pump in elderly patients. The results demonstrate that Oliceridine provides non-inferior analgesic efficacy to sufentanil while yielding a significantly lower incidence of nausea and vomiting within the first 48 hours postoperatively.
As a G protein-biased μ-opioid receptor agonist, oliceridine preferentially activates G-protein signaling and reduces β-arrestin recruitment, which was a mechanism recommended for the preservation of potent analgesia and the mitigation of undesirable effects simultaneously.22 This biased signaling profile not only differentiates it from morphine in vitro, but also underscores its ameliorated safety outcomes in animals. However, this profile gives rise to less respiratory depression and gastrointestinal dysfunction at equianalgesic doses.5,8,9,23,24 In humans, Oliceridine exhibited remarkable, dose-related drug behavior and gives strong pain relief in both healthy volunteers and post-surgery pain tests, suggesting that it is comparable to morphine but with fewer side effects.14–16 Proof also shows it’s useful in tough medical cases, like giving quick and lasting pain relief to burn patients.17,25
Our results match earlier studies showing that Oliceridine PCA works was comparable to regular opioid PCA for pain relief.26 Unlike previous studies that mainly compared Oliceridine with morphine, a classic opioid, our study is the first to test Oliceridine against sufentanil, a commonly used opioid in Chinese clinics. As one of the fentanyls, sufentanil is a synthetic μ-opioid receptor agonist, which is 50 to 100 times stronger than morphine in the body, but its effects are similar, including pain relief, drowsiness, slowed breathing, constipation, euphoria, and the risk of tolerance and addiction.27 In everyday use, sufentanil PCA works better for pain relief than morphine, with fewer side effects. However, some patients still feel sick and vomit, and doctors still worry about breathing problems, especially in older people. The Oliceridine PCA dosage was selected on the basis of our previous studies,11,28 and the lockout interval was determined in line with the Expert Consensus on Postoperative Pain Management in Adults (2017) issued by the Chinese Society of Anesthesiology. As found before, fewer patients in the Oliceridine group felt sick and vomited. In particular, the nausea rate (33.33%) stayed similar, while the vomiting rate (14.49%) rose slightly.29 This outcome might stem from more women in our group. Compared to SHR8554, another type of μ-opioid drug, our Oliceridine group had more nausea but similar vomiting rates.20 In contrast, our Oliceridine group saw fewer cases of both nausea and vomiting than in a past study.30 This phenomenon may be the result of differences in surgical type The reason is that abdominal procedures are bound up with a more striking risk of postoperative nausea and vomiting. And the application of dexamethasone used in our study also lead to a lower incidence of nausea and vomiting. Importantly, our study witnessed no breathing problems, which was dissimilar from earlier reports.28 Differences in surgery type and postoperative analgesic dosing may be the primary reason why the above phenomena occurred. Abdominal surgeries often bring about breathing issues, but our study included patients having knee replacements, which do not usually affect breathing. Moreover, using both general anesthesia and ultrasound-guided nerve block in our plan cut down opioid needs. The Oliceridine PCA regimen also had a slow basal rate, with just 0.2 mg per bolus (for a 50 kg patient). Follow-up records show not every patient needed extra doses. And, we acknowledge that several earlier studies have indicated a significant influence of intraoperative sufentanil dosage on postoperative morphine consumption, pain levels, and hyperalgesia.31–33 Therefore, to ensure the robustness of our findings, we performed a sensitivity analysis of the analgesic scores at each follow-up time point. However, after adjustment for the intraoperative dose of sufentanil, the mean difference of rSPID48h failed to meet the non-inferiority criterion, which suggested that our results are not robust. This sensitivity analysis reveals that the apparent non-inferiority in the primary analysis could be partially attributed to, or confounded by, differences in intraoperative analgesic management. These findings should be interpreted with caution and warrant further research for confirmation.
In this study, in contrast to studies using a standardized fixed-dose regimen, our protocol individualized the analgesic pump dosage based on patient body weight, thereby prioritizing inter-individual variation and delivering a truly personalized analgesic regimen. Nevertheless, we should note several limitations. First, this was a trial at one center. As a top orthopedic hospital, our study’s surgery and anesthesia methods are commonly used for quick recovery. Second, we only included patients with ASA I–II status and BMI in a set range. Thus, patients with serious health risks like severe chronic illnesses, obesity, or sleep apnoea were not included. While the utility of oliceridine in such risky groups requires dedicated proof, its mechanistic profile suggests the observed safety benefits might be particularly beneficial for, and could be extrapolated to, frail elderly patients with reduced physiologic reserve (eg., ASA ≥III), pending confirmatory studies. Third, owing to the inclusion of elderly patients and associated clinical safety concerns, a conservative, lower-dose PCA pump regimen was deliberately chosen. This approach, however, likely led to increased consumption of supplemental analgesics on the ward, which may have compromised the interpretation of the primary outcome by introducing a potential confounding variable. Nevertheless, our non-inferiority conclusion likely applies to this overall, multimodal analgesic strategy, which aligns with recommended practice for elderly patients.34,35 This showed that within such a safety-oriented protocol, an oliceridine-based regimen is not inferior to one based on sufentanil. Finally, while this study focused on analgesic efficacy and select disadvantageous effects, it did not address economic implications. As noted by Simpson et al,36 using Oliceridine instead of morphine for 1000 patients cost $96,623 more on pain drugs. Nonetheless, this cost could be balanced by fewer ORAEs: managing ORAEs with oliceridine costs $528,424, while morphine costs $852,429, saving $324,005. Moreover, using Oliceridine just for high-risk patients and morphine for others could boost savings to $363,944.37 In other words, it remains ambiguous about the cost difference between Oliceridine and sufentanil.
Nevertheless, the findings of this study indicate that with the assistance of regional nerve blocks, most patients reported satisfactory analgesia within the first 3 h postoperatively, with the majority exhibiting NRS scores below 4. Nonetheless, pain levels began to increase by the 8 h mark. These observations underline the imperative for continued exploration of analgesic strategies following total knee arthroplasty, which is a research priority that aligns with two ongoing carried out by our research group at present.
Conclusion
Our study suggests that Oliceridine may have a non-inferior analgesic to sufentanil for PCA pump subsequent to knee arthroplasty in the elderly. And the advantage of Oliceridine at the aspect of lessening nausea and vomiting in elderly patients has been confirmed. Future research is necessary to determine whether they could potentially supplement or even replace traditional opioids, particularly cost-effective options like fentanyl.
Abbreviations
TKA,Total knee arthroplasty; patient-controlled analgesia, PCA; ORAEs, opioid-related adverse events; BMI, body mass index; PACU, post-anesthesia care unit; NRS, numeric rating scale; SPID, sum of pain intensity difference; SD, standard deviation; IQR, interquartile range; CI, confidence interval.
Data Sharing Statement
Subject to the policies of the Ethics Committee, the anonymized dataset from this study can be accessed by submitting a reasonable academic request to the corresponding author, along with a research protocol approved by the applicant’s local ethics committee.
Ethics Approval and Informed Consent
All procedures performed on the patients were in accordance with the 1964 helsinki declaration and its later amendments. The study was approved by the Ethical Committee of Shanghai Sixth People’s Hospital, affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai, China (approval number: 2024-169-(1)).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Optimized Acute Pain Management programme of Wu Jieping Medical Foundation (Grant NO.: 320.6750.2024-15-97). The sponsor supervised the progress of this trial.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision Hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–10. doi:10.2106/00004623-200704000-00012
2. Andersen LØ, Husted H, Otte KS, Kristensen BB, Kehlet H. High-volume infiltration analgesia in total knee arthroplasty: a randomized, double-blind, placebo-controlled trial. Acta Anaesthesiol Scand. 2008;52(10):1331–1335. doi:10.1111/j.1399-6576.2008.01777.x
3. Andersen LØ, Gaarn-Larsen L, Kristensen BB, Husted H, Otte KS, Kehlet H. Subacute pain and function after fast-track Hip and knee arthroplasty. Anaesthesia. 2009;64(5):508–513. doi:10.1111/j.1365-2044.2008.05831.x
4. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248–273. doi:10.1097/ALN.0b013e31823c1030
5. Raehal KM, Walker JK, Bohn LM. Morphine side effects in beta-arrestin 2 knockout mice. J Pharmacol Exp Ther. 2005;314:11951201. doi:10.1124/jpet.105.087254
6. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
7. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67–76. doi:10.1080/03602530902722679
8. Ju J, Li Z, Liu J, Peng X, Gao F. Biased opioid receptor agonists: balancing analgesic efficacy and side-effect profiles. Int J Mol Sci. 2025;26(5):1862. doi:10.3390/ijms26051862
9. Song C, Huang X, Chen N, Song Q, Qiu Y. A bibliometric and visual analysis of oliceridine research (2013-2024). Drug Des Devel Ther. 2025;19:1305–1321. doi:10.2147/DDDT.S497186
10. DeWire SM, Yamashita DS, Rominger DH, et al. A G protein-biased ligand at the mu-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344:708–717. doi:10.1124/jpet.112.201616
11. Food and Drug Administration. Oliceridine briefing document: FDA advisory committee meeting 2018. Available from https://www.fda.gov/media/121230/download.
12. Violin JD, Crombie AL, Soergel DG, Lark MW. Biased ligands at G-protein-coupled receptors: promise and progress. Trends Pharmacol Sci. 2014;35(7):308–316. doi:10.1016/j.tips.2014.04.007
13. Chen XT, Pitis P, Liu G, et al. Structure activity relationships and discovery of a G protein biased mu opioid receptor ligand, [(3-methoxythiophen-2-yl)methyl]({2-[(9R)-9-(pyridin-2yl)-6-oxaspiro-[4.5]decan- 9-yl]ethyl})amine (TRV130), for the treatment of acute severe pain. J Med Chem. 2013;56:8019–8031. doi:10.1021/jm4010829
14. Soergel DG, Subach RA, Sadler B, et al. First clinical experience with TRV130: pharmacokinetics and pharmacodynamics in healthy volunteers. J Clin Pharmacol. 2014;54:351–357. doi:10.1002/jcph.207
15. Ruscheweyh R, Stumpenhorst F, Knecht S, Marziniak M. Comparison of the cold pressor test and contact thermode-delivered cold stimuli for the assessment of cold pain sensitivity. J Pain. 2010;11(8):728–736. doi:10.1016/j.jpain.2009.10.016
16. Soergel DG, Subach RA, Burnham N, et al. Biased agonism of the mu-opioid receptor by TRV130 increases analgesia and reduces on-target adverse effects versus morphine: a randomized, double-blind placebo-controlled, crossover study in healthy volunteers. Pain. 2014;155:1829–1835. doi:10.1016/j.pain.2014.06.011
17. Viscusi ER, Webster L, Kuss M, et al. A randomized, Phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157:264–272. doi:10.1097/j.pain.0000000000000363
18. Simons P, van der Schrier R, van Lemmen M, et al. Respiratory effects of biased ligand oliceridine in older volunteers: a pharmacokinetic-pharmacodynamic comparison with morphine. Anesthesiology. 2023;138:249–263. doi:10.1097/ALN.0000000000004473
19. Minkowitz HS. A review of sufentanil and the sufentanil sublingual tablet system for acute moderate to severe pain. Pain Manag. 2015;5:237–250. doi:10.2217/pmt.15.22
20. Zhao Y, Lu Z, Song X, et al. Efficacy and safety of SHR8554 on postoperative pain in subjects with moderate to severe acute pain following orthopedic surgery: a multicenter, randomized, double-blind, dose-explored, active-controlled, Phase II/III clinical trial. Pharmacol Res. 2025;212:107576. doi:10.1016/j.phrs.2025.107576
21. Gan TJ, Wase L. Oliceridine, a G protein-selective ligand at the μ-opioid receptor, for the management of moderate to severe acute pain. Drugs Today. 2020;56:269–286. doi:10.1358/dot.2020.56.4.3107707
22. Yazicioğlu D, Caparlar C, Akkaya T, Mercan U, Kulaçoğlu H. Tizanidine for the management of acute postoperative pain after inguinal hernia repair: a placebo-controlled double-blind trial. Eur J Anaesthesiol. 2016;33(3):215–222. doi:10.1097/EJA.0000000000000371
23. Bohn LM, Lefkowitz RJ, Gainetdinov RR, Peppel K, Caron MG, Lin FT. Enhanced morphine analgesia in mice lacking beta-arrestin 2. Science. 1999;286(5449):2495–2498. doi:10.1126/science.286.5449.2495
24. Liang DY, Li WW, Nwaneshiudu C, Irvine KA, Clark JD. Pharmacological characters of oliceridine, a μ-opioid receptor G-protein-biased ligand in mice. Anesth Analg. 2019;129(5):1414–1421. doi:10.1213/ANE.0000000000003662
25. Hill DM, Todor LA. A prospective, historical-controlled evaluation of oliceridine for moderate or severe pain in patients with acute burn injuries (RELIEVE). Burns. 2025;51:107343. doi:10.1016/j.burns.2024.107343
26. Huang C, Liu B, Xie S, et al. Evaluating the opioid-related adverse events of oliceridine versus conventional opioids in patient-controlled analgesia after thoracoscopic lung resection: a retrospective cohort study. Drug Des Devel Ther. 2025;19:5929–5939. doi:10.2147/DDDT.S532778
27. Ramos-Gonzalez N, Groom S, Sutcliffe KJ, et al. Carfentanil is a β-arrestin-biased agonist at the μ opioid receptor. Br J Pharmacol. 2023;180:2341–2360. doi:10.1111/bph.16084
28. Brzezinski M, Hammer GB, Candiotti KA, et al. Low incidence of opioid-induced respiratory depression observed with oliceridine regardless of age or body mass index: exploratory analysis from a phase 3 open-label trial in postsurgical pain. Pain Ther. 2021;10:457–473. doi:10.1007/s40122-020-00232-x
29. Bergese SD, Brzezinski M, Hammer GB, et al. ATHENA: a phase 3, open-label study of the safety and effectiveness of oliceridine (TRV130), A G-Protein selective agonist at the µ-opioid receptor, in patients with moderate to severe acute pain requiring parenteral opioid therapy. J Pain Res. 2019;12:3113–3126. doi:10.2147/JPR.S217563
30. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO-2: a randomized, placebo and active-controlled phase III study investigating oliceridine (TRV130), a G Protein-biased ligand at the μ-opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Pract. 2019;19:715–731. doi:10.1111/papr.12801
31. Gerlach K, Uhlig T, Hüppe M, et al. Remifentanil-propofol versus sufentanil-propofol anaesthesia for supratentorial craniotomy: a randomized trial. Eur J Anaesthesiol. 2003;20(10):813–820. doi:10.1097/00003643-200310000-00007
32. Bidgoli J, Delesalle S, De Hert SG, Reiles E, Van der Linden PJ. A randomised trial comparing sufentanil versus remifentanil for laparoscopic gastroplasty in the morbidly obese patient. Eur J Anaesthesiol. 2011;28(2):120–124. doi:10.1097/EJA.0b013e3283405048
33. Martorano PP, Aloj F, Baietta S, et al. Sufentanil-propofol vs remifentanil-propofol during total intravenous anesthesia for neurosurgery. A multicentre study. Minerva Anestesiol. 2008;74(6):233–243.
34. Chen X, Chu Q, Peng Y, et al. Clinical practice guidelines for postoperative pain management in adults (2024 edition). J Anesth Transl Med. 2025;4(3):161–185. doi:10.1016/j.jatmed.2025.09.001
35. Aubrun F, Marmion F. The elderly patient and postoperative pain treatment. Best Pract Res Clin Anaesthesiol. 2007;21(1):109–127. doi:10.1016/j.bpa.2006.12.005
36. Simpson KN, Fossler MJ, Wase L, Demitrack MA. Cost-effectiveness and cost-benefit analysis of oliceridine in the treatment of acute pain. J Comp Eff Res. 2021;10(15):1107–1119. doi:10.2217/cer-2021-0107
37. Simpson KN, Fossler MJ, Wase L, Demitrack MA, Wandstrat TL. Budget impact and pharmacy costs with targeted use of oliceridine for postsurgical pain in patients at high risk of opioid-related adverse events. Expert Rev Pharmacoecon Outcomes Res. 2022;22(4):671–681. doi:10.1080/14737167.2022.2038137
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.