Back to Journals » Clinical Interventions in Aging » Volume 18
A Comparison of Dynamic SPECT Coronary Flow Reserve with TIMI Frame Count in the Treatment of Non-Obstructive Epicardial Coronary Patients
Authors He M, Han W, Shi C, Wang M ![]() , Li J, He W, Xu X, Gan Q, Guan S, Zhang L, Chen Y, Chang X, Li T, Qu X
, Li J, He W, Xu X, Gan Q, Guan S, Zhang L, Chen Y, Chang X, Li T, Qu X
Received 7 July 2023
Accepted for publication 24 October 2023
Published 2 November 2023 Volume 2023:18 Pages 1831—1839
DOI https://doi.org/10.2147/CIA.S429450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Mingping He,1,* Wenzheng Han,1,* Chuan Shi,1 Ming Wang,1 Junheng Li,2 Wei He,2 Xinxin Xu,3 Qian Gan,1 Shaofeng Guan,1 Liang Zhang,1 Yang Chen,1 Xifeng Chang,1 Tianqi Li,1 Xinkai Qu1
1Department of Cardiology, Huadong Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China; 2Department of Nuclear Medicine, Huadong Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China; 3Clinical Research Center for Geriatric Medicine, Huadong Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenzheng Han; Xinkai Qu, Department of Cardiology, Huadong Hospital Affiliated to Fudan University, No. 221, Yan’an Road (W), Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Background: Microvascular dysfunction in patients with non-obstructive epicardial coronary may aggravate patient’s symptoms or lead to various clinical events.
Objective: To investigate the correlation between dynamic single photon emission computed tomography (D-SPECT) derived coronary flow reserve (CFR) and TIMI frame count (TFC) in patients with non-obstructive epicardial coronary patients.
Methods: Patients with suspected or known stable CAD who were recommended to undergo invasive coronary angiography were prospectively enrolled in this study. Those who had non-obstructive coronary received TIMI frame count (TFC) and D-SPECT. A cut-off value of > 40 was defined as slow flow referred to TFC.
Results: A total of 47 patients diagnosed with non-obstructive coronary were enrolled. The mean age of patients was 66.09 ± 8.36 years, and 46.8% were male. Dynamic SPECT derived coronary flow reserve (CFR) was significantly correlated with TIMI frame count in 3 epicardial coronary (LAD: r=− 0.506, P = 0.0003; LCX: r= − 0.532, P = 0.0001; RCA: r= − 0.657, P < 0.0001). The sensitivity and specificity of CFR in identifying abnormal TIMI frame count < 40 was 100.0% and 57.6% in LAD, 62.5% and 87.0% in LCX, 83.9% and 75.0% in RCA, respectively. The optimal CFR cut-off values were 2.02, 2.47, and 1.96 among the three vessels.
Conclusion: In patients with non-obstructive coronary, CFR derived from D-SPECT was strongly correlated with TFC. This study demonstrates that that CFR may be an alternative non-invasive method for identifying slow flow in non-obstructive coronary.
Keywords: dynamic single photon emission computed tomography, thrombolysis in myocardial infarction frame count, slow flow, non-obstructive coronary, coronary flow reserve
Introduction
Coronary artery disease (CAD) is the main cause of death worldwide. In most CAD patients, invasive angiography shows significant obstruction (≥70%) in the epicardial coronary system.1 In recent years, studies have shown that coronary microvascular disease is the major cause of CAD with non-obstructive epicardial coronary or normal coronary artery as determined by angiography.2–4 Although coronary microvascular dysfunction has significant clinical and prognostic implications, there is no effective diagnostic tool.5,6
In the past decades, thrombolysis in myocardial infarction (TIMI) flow grade system has been widely applied in assessment of blood flow within the epicardial coronary system.7–9 Generally, TIMI1-2 flow indicates microvascular resistance from the side where the epicardial coronary artery has not narrowed significantly. However, TIMI flow grade system (TFG) only provides semi-quantitative or categorical variables rather than continuous ones, which limits its statistical power in clinical trials. In contrast, TIMI Frame Count (TFC) allows quantitative assessment of the number of cine-frames required for contrast to reach standardized distal landmarks.10 The ideal cut off value of TFC in defining TIMI 3 flow was found to be 40. It therefore allows physicians to diagnose a microvascular dysfunction in epicardial coronary by TFC under angiography.11–13
Positron emission tomography (PET) has been considered the gold standard non-invasive imaging examination tool for myocardial perfusion imaging (MPI).14 However, it is not widely available in many centers due to the high costs of the tracer. In contrast to PET, single-photon emission computed tomography (SPECT) is less expensive and readily available. In recent years, cardiac SPECT systems equipped with stationary solid-state cadmium-zinc-telluride (CZT) detectors with improved sensitivity, spatial and energy resolution have been developed for myocardial flow determination.6,15,16 Myocardial blood flow (MBF) and myocardial flow reserve (MFR) provides more accurate assessment of microvascular disease than visual assessment or semi-quantitative perfusion evaluation. However, CFR derived from D-SPECT and CFR derived from fractional flow reserve (FFR) were found to be correlated in multivessel coronary disease.17,18 The performance of D-SPECT and other clinical diagnostic methods in functional assessment of non-obstructive coronary disease is currently not well understood.19
In this study, we aimed to investigate the relationship between CFR quantification by D-SPECT and TFC based on angiography in non-obstructive coronary disease. Moreover, we investigated the diagnostic cut off value by D-SPECT in the visual assessment of blood flow in different epicardial coronary systems.
Materials and Methods
Study Design and Objectives
A total 236 patients with suspected coronary disease who underwent invasive coronary angiography (CAG) were prospectively screened between April 2021 and November 2022. Among them, 147 patients underwent percutaneous intervention after CAG. In addition, 47 of the 89 remaining patients without obstructive stenosis (angiography stenosis < 30%) in any epicardial coronary vessel were enrolled (Figure 1). TIMI frame count (TFC) and 99mTcsestamibi (MIBI) SPECT imaging were performed within 3 days before or after invasive CAG. The exclusion criteria were as follows: (1) ≥50% stenosis in any coronary artery at invasive CAG, (2) patients who could not afford D-SPECT examination, (3) had a history of myocardial infarction, (4) nonischemic cardiomyopathy, (5) PCI or coronary artery bypass grafting (CABG), and (6) left ventricular ejection fraction < 35%.
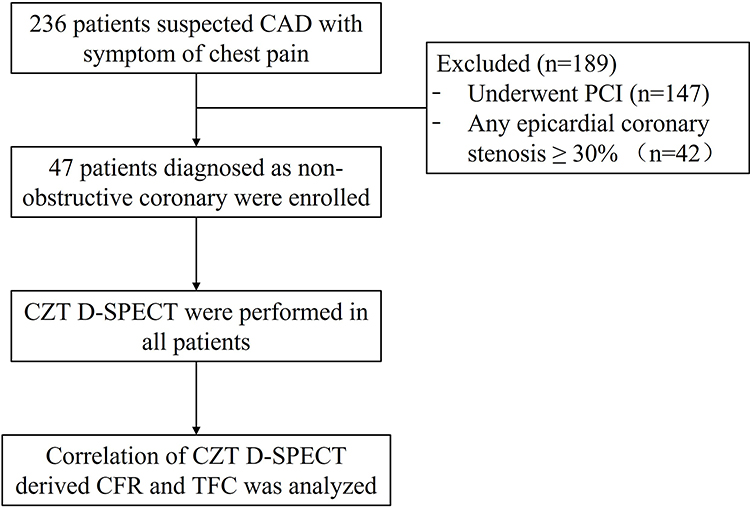 |
Figure 1 Flowchart of the study population. |
Data Collection
TIMI Frame Count
TIMI frame count was performed within 3 days after CAG. Clinically, the first frame in the TIMI frame count is defined by a column of contrast extending across >70% of the arterial lumen with antegrade motion. The last frame counted is that in which the contrast enters (but not necessarily fills) a distal landmark. These main landmarks are as follows: the first branch of posterolateral artery in the right coronary artery; the distal branch of the lateral left ventricular wall artery farthest from the coronary ostium in the circumflex system; and the distal bifurcation known as the “whale’s tail” in the left anterior descending artery.9
In this study, TFC for the left anterior descending (LAD) was evaluated in the right anterior oblique projection with cranial angulation (RAO cranial view). The TFC for the circumflex (LCX) arteries was examined in the right anterior oblique projection with caudal angulation (RAO caudal view) and the TFC for the right coronary artery (RCA) in a left anterior oblique projection with cranial angulation (LAO cranial view). In addition, conversion factors of 3.0 and 2.0 were used to convert the frame rate values when filmed at 10 f/s and 15 f/s, respectively, to adjust for the 30 f/s acquisition speed. The cut-off value of TFC in determining coronary slow flow was >40 (Figure 2).9
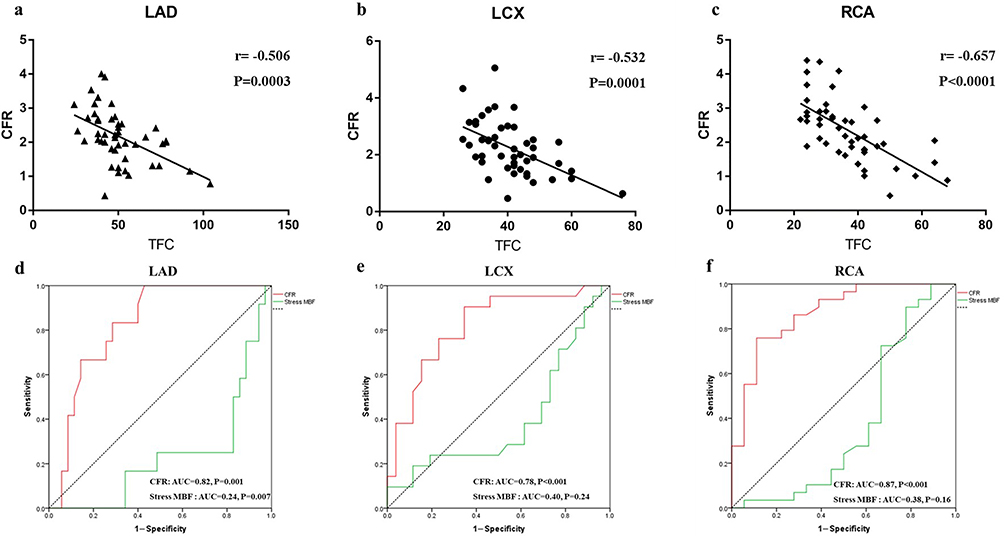 |
Figure 2 Correlation between regional CFR and TFC in different coronary artery. (a–c) Correlation between CFR and TFC in LAD (r=−0.506, P=0.0003), LCX (r=−0.532, P=0.0001) and RCA (r=−0.657, P<0.0001). (d–f) AUC of sensitivity and specificity in LAD, LCX and RCA. Data showed that regional CFR was significantly negatively correlated with TFC in all 3 epicardial coronary arteries. |
Dynamic Perfusion SPECT Imaging and Analysis
SPECT imaging was performed using a previously published protocol. All image acquisitions were performed using a D-SPECT cardiac scanner (Spectrum Dynamics, Caesarea, Israel) equipped with nine individual Cadmium-zinc-telluride (CZT) detector columns. A one-day protocol was adopted to assess MBF and coronary flow reserve (CFR). According to the guideline published by Chinese expert in 2022, pre-scanning was performed after administration of an initial dose of approximately 1 mCi MIBI to enable positioning of the heart in the center of the field of view and establishment of the scanning region of interest (ROI). Full scanning was started immediately after injection of the remaining dose of approximately 15 mCi MIBI, and dynamic images were acquired in the list mode for over 6 minutes. After the rest dynamic scanning, rest perfusion scanning was performed. To conduct stress imaging, pharmacological stress was induced through an intravenous infusion of adenosine triphosphate (ATP) disodium at a rate of 140μg*kg−1*min−1 for 5 minutes, and 25 mCi MIBI was injected 3 minutes later from the start of ATP injection. Dynamic image acquisition was then performed for more than 6 minutes. Finally, stress perfusion scanning was carried out (Figure 2).20,21
Images were analyzed using the Corridor 4DM software (INVIA, Ann Arbor, MI, USA). MBF was extrapolated from the uptake rate K1 using the Renkin–Crone equation for MIBI reported previously. CFR was then calculated as the ratio of stress MBF to the rest MBF.
Statistical Analysis
Continuous variables were expressed as the mean plus SD or median and interquartile range. Categorical variables were expressed as rates with percentages (%). Pearson correlation analysis was conducted to determine the relationship between CFR derived from D-SPECT and TFC. A receiver operating characteristic (ROC) curve analysis was constructed to evaluate the accuracy of CFR in detecting coronary slow flow based on TFC. A 2-tailed P<0.05 was considered statistically significant. All statistical analyses were performed using the IBM SPSS version 22.0 (IBM Statistics, Armonk, NY).
Results
Patients Characteristics
A total of 47 patients with non-obstructive stenosis under CAG were enrolled. The baseline clinical data of the patients are summarized in Table 1. The mean age of the patients was 66.09 ± 8.36 years old, 22 (46.8%) were male, and the mean body mass index was 24.61 ± 2.97 kg*m−2. In terms of risk factors of coronary disease, 32 patients (68.1%) had hypertension, 5 (10.6%) had dyslipidemia, 10 (21.3%) had diabetes mellitus, and 10 (21.3%) were current smokers. Left ventricular ejection fraction (LVEF) was 63.89 ± 2.39 and 45 patients (95.7%) had right coronary dominance (Table 1).
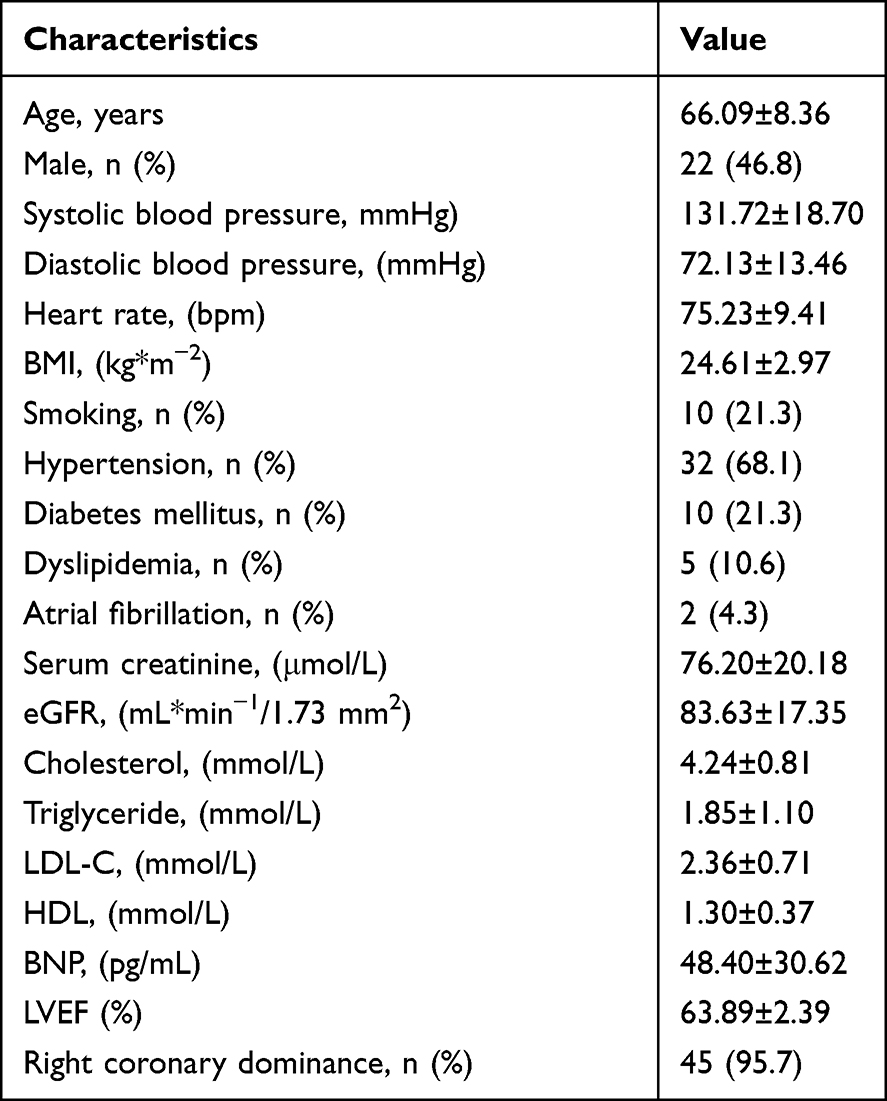 |
Table 1 Baseline Characteristics of Patients |
D-SPECT and TFC Data
None of the patients developed complications after ATP or contrast infusion or during the procedure. Table 2 displays the description of MBF, CFR and TFC by different epicardial coronary vessels (LAD, LCX and RCA). The results showed that regional CFR in all 3 different vessels was significantly lower in slow flow vessels based on TFC (LAD: 1.98 ± 0.78 vs 2.72 ± 0.49, P = 0.003; LCX: 1.80 ± 0.74 vs 2.78 ± 0.91, P < 0.001; RCA: 1.64 ± 0.65 vs 2.79 ± 0.78, P < 0.001).
 |
Table 2 D-SPECT and TFC Data in Epicardial Coronary |
Correlation of CFR with TFC in Different Epicardial Coronary Artery
The results of the correlation analysis between CFR and TFC are shown in Figure 2. Data showed that regional CFR was significantly negatively correlated with TFC in all 3 epicardial coronary arteries (LAD: r = −0.506, P = 0.0003; LCX: r = −0.532, P = 0.0001; RCA: r = −0.657, P < 0.0001). The sensitivity and specificity for CFR were 100.0% and 57.0% in LAD with a ROC-optimized cutoff value of 2.04, 90.5% and 65.4% in LCX with a ROC-optimized cutoff value of 1.92, 76.0% and 89.0% in RCA with a ROC-optimized cutoff value of 2.17, respectively. The area under the ROC curve of CFR in all 3 vessels was larger than that of stress MBF in the diagnosis of slow flow (Figure 3).
 |
Figure 3 TIMI frame count and D-SPECT image. Arrow: Distal landmark. The area under the ROC curve of CFR in all 3 vessels was larger than that of stress MBF in the diagnosis of slow flow. |
Discussion
In this study, we performed a prospective trial to evaluate the diagnostic performance of CFR derived from D-SPECT in comparison with that of TFC in patients with non-obstructive coronary. The main findings of our study are as follows: 1) CFR derived from D-SPECT was moderately correlated with TFC derived from angiography, demonstrating that CFR derived from D-SPECT is a good non-invasive method for assessing blood flow in non-obstructive coronary patients. 2) The cut off value of CFR derived from D-SPECT varied across different coronary vessels. These results may provide valuable data to improve the diagnosis of blood flow in different regions of the heart. Moreover, CFR showed better performance compared to stress MBF in the diagnosis of slow flow in the three coronary regions suggesting regional microvascular dysfunction.
PET with 15O-water and 13N-ammonia and 82Rb are the gold standard tools for MBF and MFR assessment.22 However, the widespread application of PET is limited by its high costs. In contrast to PET, SPECT is less expensive and readily available. Agostini et al reported that MBF and MFR derived from CZT D-SPECT with motion correction and optimal placement of the arterial input function showed good agreement with 15O-water PET.23 In previous studies, a negative correlation was reported between MFR and global indexes of atherosclerotic burden such as the Syntax (r = 0.360, P = 0.006) and Gensini (r = - 0.345, P = 0.037) score in multi-vessel disease.18,24 Current data shows that CZT D-SPECT provides accurate assessment of MBF and MFR compared with semi-quantitative MPI. However, the diagnostic value of quantitative indexes differs among non-obstructive CAD patients.19 Che et al reported that 33.2% of non-obstructive patients had abnormal D-SPECT MPI, but had a poor prognosis similar to patients with obstructive condition.25 The TFC method was introduced in the early 1990s for assessing coronary artery blood flow. In patients undergoing primary PCI, TFC is considered an important predictive indicator of regional left ventricular function. Moreover, TFC can be utilized to evaluate microvascular dysfunction in patients with microvascular angina.26 Sun et al showed that TFC was significantly increased in patients with microvascular spasm. This study demonstrates that TFC is a simple technique suitable for the diagnosis of microvascular spasm.10 Elsewhere, TFC was found to be strongly correlated with IMR derived from FFR in patients with coronary microvascular disease.27 Kayapinar et al reported that coronary slow flow (CSF) may have a poorer prognosis compared with Cardiac syndrome X (CSX) in non-obstructive patients. They also found that the level of myocardial ischemia on SPECT-MPI was correlated with TFC and the number of affected coronary vessels in patients with CSF.28 In the present study, CZT D-SPECT was used to evaluate MBF in patients with non-obstructive coronary. CFR is equal to the ratio of regional stress to rest MBF. Further analysis revealed a negative correlation between regional CFR and TFC in different coronaries. These data proved that CFR derived from CZT D-SPECT may be a more effective noninvasive method for evaluating blood flow in the coronary artery compared with TFC.
TIMI grade flow indicates the blood flow in the coronary vessels, especially after primary PCI in patients with acute myocardial infarction. A lower TIMI grade score suggests a poor prognosis.8 In non-obstructive coronary patients, TIMI grade flow <3 (TFC > 40) indicated slow blood flow. Studies have shown that improved TIMI grade flow may be independently associated with a better prognosis in PCI patients.11,13 However, the relationship between TIMI grade flow and prognosis in non-obstructive coronary patients has only been demonstrated in few studies. A TIMI grade <3 was considered an indicator of microvascular dysfunction. In this study, we found that CFR derived from CZT D-SPECT had a good sensitivity and specificity in distinguishing slow blood flow based on the cut off value 40 of TFC. Moreover, we also found that CFR had a significantly better performance in diagnosing slow flow compared with stressed MFR in patients with non-obstructive coronary disease. This was consistent to findings from the study by Li which assessed the value of CFR derived from CZT D-SPECT in single vessel disease.29 The normal value of CFR highly depends on the technique used for quantification, but most publications consider CFR<2.0 to be sufficiently abnormal to cause ischemia.30–32 In our study, different cut off values were obtained in three different epicardial coronary regions. Therefore, in non-obstructive coronary patients, regional CFR derived from CZT D-SPECT may provide a more precise diagnosis.
Limitation
There are several limitations in this study should be considered when interpreting our results. Firstly, this is a single center small sample study. Therefore, the sample size may cause some bias although CFR derived from CZT D-SPECT was found to be significantly correlated with TFC. Moreover, subgroup analysis was not performed due to the small sample size. Secondly, we did not assess CFR derived from FFR or CMR in these patients. Although two physicians conducted the TFC analysis, there may be some level of bias compared with the use of gold standard CFR derived from FFR and CMR. Finally, the prognostic value was not tested in this study. Further studies with larger samples and including gold standard analyses and long-term follow up are needed.
Conclusion
In summary, CFR derived from CZT D-SPECT may provide a more accurate correlation with TFC in non-obstructive coronary patients. It can therefore be used an optimal non-invasive method for evaluating the microvascular function in patients with non-obstructive coronary disease.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethics approval Ethics Committee approval was granted by the local institutional ethics review board of Huadong Hospital Affiliated to Fudan University. All patients provided informed consent. All procedures performed in the present study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grant from Clinical medical research of Geriatric Coronary Disease Center (No. LCXZ2205), Project of Huadong Hospital clinical research (HDLC2022014), Clinical Research Plan of Shanghai Health and Family Planning Commission (No. 202040298) and Shanghai Municipal Key Clinical Specialty (No. shslczdzk02801).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Timmis A, Townsend N, Gale CP, et al. European society of cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2020;41(1):12–85. doi:10.1093/eurheartj/ehz859
2. Verna E, Ghiringhelli S, Provasoli S, et al. Epicardial and microvascular coronary vasomotor dysfunction and its relation to myocardial ischemic burden in patients with non-obstructive coronary artery disease. J Nucl Cardiol. 2017;25(5):1760–1769. doi:10.1007/s12350-017-0871-6
3. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237–269. doi:10.1093/eurheartj/ehy462
4. Vancheri F, Longo G, Vancheri S, et al. Coronary microvascular dysfunction. J Clin Med. 2020;9(9):2880. doi:10.3390/jcm9092880
5. Bekkers SC, Yazdani SK, Virmani R, et al. Microvascular obstruction: underlying pathophysiology and clinical diagnosis. J Am Coll Cardiol. 2010;55(16):1649–1660. doi:10.1016/j.jacc.2009.12.037
6. Feher A, Sinusas AJ. Quantitative assessment of coronary microvascular function: dynamic single-photon emission computed tomography, positron emission tomography, ultrasound, computed tomography, and magnetic resonance imaging. Circ Cardiovasc Imaging. 2017;10(8). doi:10.1161/CIRCIMAGING.117.006427
7. Kunadian V, Harrigan C, Zorkun C, et al. Use of the TIMI frame count in the assessment of coronary artery blood flow and microvascular function over the past 15 years. J Thromb Thrombolysis. 2009;27(3):316–328. doi:10.1007/s11239-008-0220-3
8. Gibson CM, Cannon CP, Murphy SA, et al. Relationship of the TIMI myocardial perfusion grades, flow grades, frame count, and percutaneous coronary intervention to long-term outcomes after thrombolytic administration in acute myocardial infarction. Circulation. 2002;105(16):1909–1913. doi:10.1161/01.CIR.0000014683.52177.B5
9. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93(5):879–888. doi:10.1161/01.CIR.93.5.879
10. Sun H, Fukumoto Y, Ito A, et al. Coronary microvascular dysfunction in patients with microvascular angina analysis by TIMI frame count. J Cardiovasc Pharmacol. 2005;46:622–626. doi:10.1097/01.fjc.0000181291.96086.ae
11. Gibson CM, Ryan KA, Kelley M, et al. Methodologic drift in the assessment of TIMI grade 3 flow and its implications with respect to the reporting of angiographic trial results. Am Heart J. 1999;137(6):1179–1184. doi:10.1016/S0002-8703(99)70380-7
12. Gibson.C.M EA, Murphy SA, Rizzo MJ. Relationship between TIMI frame count and clinical outcomes after thrombolytic administration. Circulation. 1999;99:1945–1950. doi:10.1161/01.CIR.99.15.1945
13. Hamada S, Nishiue T, Nakamura S, et al. TIMI frame count immediately after primary coronary angioplasty as a predictor of functional recovery in patients with TIMI 3 reperfused acute myocardial infarction. J Am Coll Cardiol. 2001;38(3):666–671. doi:10.1016/S0735-1097(01)01424-3
14. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
15. Zavadovsky KV, Varlamova JV, Nikitin NA, et al. The current status of CZT SPECT myocardial blood flow and reserve assessment: tips and tricks. J Nucl Cardiol. 2021;29:2220–2231. doi:10.1007/s12350-021-02658-y
16. Krakovich A, Zaretsky U, Moalem I, et al. A new cardiac phantom for dynamic SPECT. J Nucl Cardiol. 2021;28(5):2299–2309. doi:10.1007/s12350-020-02028-0
17. Ben Bouallegue F, Roubille F, Lattuca B, et al. SPECT myocardial perfusion reserve in patients with multivessel coronary disease: correlation with angiographic findings and invasive fractional flow reserve measurements. J Nucl Med. 2015;56(11):1712–1717. doi:10.2967/jnumed.114.143164
18. Miyagawa M, Nishiyama Y, Uetani T, et al. Estimation of myocardial flow reserve utilizing an ultrafast cardiac SPECT: comparison with coronary angiography, fractional flow reserve, and the SYNTAX score. Int J Cardiol. 2017;244:347–353. doi:10.1016/j.ijcard.2017.06.012
19. Panjer M, Dobrolinska M, Wagenaar NRL, et al. Diagnostic accuracy of dynamic CZT-SPECT in coronary artery disease. A systematic review and meta-analysis. J Nucl Cardiol. 2022;29(4):1686–1697. doi:10.1007/s12350-021-02721-8
20. Yu HJ. Procedural guideline for quantification of myocardial blood flow with D-SPECT: expert consensus. Chin J Clin Med. 2022;29(4):379–386.
21. Johnson RD, Bath NK, Rinker J, et al. Introduction to the D-SPECT for technologists: workflow using a dedicated digital cardiac camera. J Nucl Med Technol. 2020;48(4):297–303. doi:10.2967/jnmt.120.254870
22. Yoshinaga K, Katoh C, Manabe O, et al. Incremental diagnostic value of regional myocardial blood flow quantification over relative perfusion imaging with generator-produced rubidium-82 PET. Circ J. 2011;75(11):2628–2634. doi:10.1253/circj.CJ-11-0502
23. Agostini D, Marie P-Y, Ben-Haim S, et al. Performance of cardiac cadmium-zinc-telluride gamma camera imaging in coronary artery disease: a review from the cardiovascular committee of the European Association of Nuclear Medicine (EANM). Eur J Nucl Med Mol Imaging. 2016;43(13):2423–2432. doi:10.1007/s00259-016-3467-5
24. Iguchi N, Utanohara Y, Suzuki Y, et al. Myocardial flow reserve derived by dynamic perfusion single-photon emission computed tomography reflects the severity of coronary atherosclerosis. Int J Cardiovasc Imaging. 2018;34(9):1493–1501. doi:10.1007/s10554-018-1358-5
25. Liu L, Abdu FA, Yin G, et al. Prognostic value of myocardial perfusion imaging with D-SPECT camera in patients with ischemia and no obstructive coronary artery disease (INOCA). J Nucl Cardiol. 2021;28(6):3025–3037. doi:10.1007/s12350-020-02252-8
26. Yazici M, Demircan S, Durna K, et al. The role of adrenergic activity in slow coronary flow and its relationship to TIMI frame count. Angiology. 2007;58(4):393–400. doi:10.1177/0003319707305118
27. Xu X, Zhou J, Zhang Y, et al. Evaluate the correlation between the TIMI frame count, IMR, and CFR in coronary microvascular disease. J Interv Cardiol. 2022;2022:6361398. doi:10.1155/2022/6361398
28. Ozde C, Aktüre G, Aytekin S, et al. Assessment of the relationship between coronary flow rates and myocardial perfusion abnormality in patients with nonobstructive coronary artery disease: an observational study in cardiac syndrome X and coronary slow flow. Nucl Med Commun. 2019;40(11):1122–1129. doi:10.1097/MNM.0000000000001080
29. Li C, Xu R, Yao K, et al. Functional significance of intermediate coronary stenosis in patients with single-vessel coronary artery disease: a comparison of dynamic SPECT coronary flow reserve with intracoronary pressure-derived fractional flow reserve (FFR). J Nucl Cardiol. 2022;29(2):622–629. doi:10.1007/s12350-020-02293-z
30. Pepine CJ, Anderson RD, Sharaf BL, et al. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the national heart, lung and blood institute WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55(25):2825–2832. doi:10.1016/j.jacc.2010.01.054
31. Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356(8):830–840. doi:10.1056/NEJMra061889
32. Murthy VL, Naya M, Foster CR, et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation. 2011;124(20):2215–2224. doi:10.1161/CIRCULATIONAHA.111.050427
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.