Back to Journals » Patient Preference and Adherence » Volume 17
A Comparative Piloting of Determinants of Self-Medication Among University Students in the MENA Region; UAE and Jordan as an Example
Authors Alzoubi A ![]() , Nasor EM
, Nasor EM ![]() , Suliman EM, AlQaderi N, AbbasTanira SH, Abdi SAH, Mustafa S, Kheirallah K
, Suliman EM, AlQaderi N, AbbasTanira SH, Abdi SAH, Mustafa S, Kheirallah K ![]()
Received 18 January 2023
Accepted for publication 9 March 2023
Published 16 March 2023 Volume 2023:17 Pages 699—709
DOI https://doi.org/10.2147/PPA.S405279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Qizhi (Cathy) Yao
Abdallah Alzoubi,1,2 Eiman M Nasor,1 Elaf MO Suliman,1 Nour AlQaderi,1 Shahd HI AbbasTanira,1 Syed Ali Hussein Abdi,1 Shadi Mustafa,3 Khalid Kheirallah3
1Department of Pathological Sciences, College of Medicine, Ajman University, Ajman, United Arab Emirates; 2Department of Pharmacology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Public Health and Community Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Abdallah Alzoubi, Department of Pathological Sciences, College of Medicine, Ajman University, P.O. Box 346, Ajman, United Arab Emirates, Tel +971 6 705 5340, Fax +971 6 743 8888, Email [email protected]
Purpose: Unsupervised self-medication (SM) is a global public health concern. University students are particularly vulnerable due to misperceptions of improved academic performance and thus are at risk of dependence, addiction, and drug overdose. Past studies have shown an alarming prevalence of SM among university students in the Middle East and North Africa (MENA) region. However, there is a scarcity of reports from the region dissecting determinants of SM. Therefore, this study aimed to determine the prevalence and epidemiological correlates of SM among university students and its perceived impact on their academic performance.
Methods: Two countries in the MENA region were surveyed in a cross-sectional design; UAE and Jordan. Through a stratified sampling technique, undergraduate students in both healthcare and non-healthcare majors of study were recruited to participate. A structured, self-administered questionnaire developed for the purpose of this study was distributed to consented participants via the university’s official email. Statistical analyses were performed using SPSS. Descriptive and inferential statistics were used to analyze data. A p-value < 0.05 was considered statistically significant.
Results: A total of 362 students participated in the study (74% were females, 60% were from the UAE, and 59% were in healthcare majors). Significantly higher prevalence rates and adjusted odds of SM were found among females, students from Jordan, and those in healthcare majors, particularly for paracetamol (90.2% of females [p=0.001], 88.3% from Jordan [p=0.03], 92.5% in healthcare majors [p=0.001]) and antibacterial drugs (48.9% of females [p=0.01], 60.7% from Jordan [p=0.001], 53.3% in healthcare majors [p=0.001]). Majoring in healthcare fields was the most consistent determinant of such practice, while social influences of family and friends represented the chief source of recommendation. Only 21% of respondents assumed SM boosts their academic performance.
Conclusion: Our pilot study underlines the predominant determinants of SM among university students in the MENA region, namely female gender, students from Jordan, and those in healthcare majors. Informed data-driven awareness campaigns to mitigate such practice should be designed to focus on these susceptible populations.
Keywords: self-medication, university, pilot, UAE, Jordan, MENA
Introduction
Self-medication (SM) is the practice of using drugs according to self-diagnosis without referring to physicians, or continuing the use of a physician-prescribed drug beyond its specified time.1,2 A recent surge in SM rates has been reported worldwide, reaching endemic proportions among populations in developing countries.3 University students in general,4 and those in the Middle East and North Africa (MENA) region in particular,5 have embarked heavily on such practice warranting public health attention. Past studies have shown a prevalence of SM among university students reaching up to 98.7% in Saudi Arabia,6 98.4% in Jordan,7 98% in Palestine,8 97.8% in Kuwait,9 92.4% in Iraq,10 86.7% in Iran,11 86% in the UAE,12 79.5% in Sudan,13 and 62.9% in Egypt.14 These alarmingly high prevalence rates encompassed mainly students who were influenced by TV commercials, online advertisements, and purchasing through mass media. Unfortunately, university students, as educated individuals, tend to share their experiences and recommend SM to their family and friends.15
The informed and responsible self-use of medicines has the potential to save time and cost on the patient, as well as reducing the load on the different constituents of the national healthcare system, including the emergency departments, outpatient and private clinics, primary healthcare facilities, governmental agencies, and insurance companies.16 This has been particularly elucidated during times of crises such as that during the most recent coronavirus pandemic (COVID-19).17 However, the unsupervised reliance on the practice of SM carries detrimental consequences, including missed/delayed diagnosis, development of drug resistance, addiction and dependence, and drug overdose and death, warranting immediate interventions to tone down these long-term effects.
A considerable number of papers has been produced in recent years to tackle the epidemiology of SM among university students in the MENA region (Table 1). Based on the sociodemographic factors of investigated student populations, the university major has been frequently underscored for playing a pivotal role in SM habits, with medical and pharmacy students being the most prone.3,18–22 Furthermore, over-the-counter analgesics and non-steroidal anti-inflammatory drugs (NSAIDs), as well as antibiotics, have been found to be the most widely used SM drugs worldwide.23,24 Substantively cited motives for such practices by university students included perceiving symptoms as minor and too insignificant to visit a physician, thus saving their time and money.15,25–28 SM was also sought by many students to better their academic performance.29
 |
Table 1 Summary of a Selected Number of Published Research Articles Assessing the Prevalence of Self-Medication Among University Students in the MENA Region (as Defined by the UNICEF Website in 2021) |
There is, however, a considerable variability in the reported prevalence rates of SM practices by university students in the aforementioned studies from the MENA region. This can be principally attributed to the lack of standardization of study population, design, and endpoints, limiting their comparability and the exact assessment of the scale of misuse.5 As a result, building on the generated conclusions of those studies to audit, guide, and inform drug prescription policy making efforts becomes seriously problematic. For instance, the recent adoption of the Antimicrobial Stewardship Programs (ASP) in several countries of the MENA region necessitates gauging its uptake and application, particularly amid the more educated stratum of the community; ie, university students.30,31
Based on this background, this study aimed to comparatively pilot the prevalence and epidemiological determinants of SM practice among university students, as well as correlating the habits of SM with the perceived effect on academic performance. Two countries in the MENA region were surveyed; UAE and Jordan.
Subjects and Methods
Ethical Statement
This study was approved by the Research Ethics Committee at Ajman University (#C-H-F-April 13), and in accordance with the Declaration of Helsinki.
Study Design, Population, and Settings
An analytical cross-sectional study was conducted between September 2021 to June 2022. A stratified sampling technique was used to recruit undergraduate students (ages of 18–25 years) at both Ajman University, UAE, and Jordan University of Science and Technology, Jordan. Students from healthcare-related (medicine, dentistry, pharmacy, nursing, allied health) and non-healthcare related (engineering, sciences and arts, and humanities) university majors were eligible to participate in the study. Study participants were recruited using a standardized online “recruitment message” explaining the purpose of the study and asking participants for consent. Messages were disseminated via official university websites and social media platforms (WhatsApp, Facebook, etc.). Consented respondents received an electronic version of a questionnaire specifically developed and piloted for the purpose of this study.
Study Questionnaire
A structured questionnaire was used to collect the study data. The questionnaire was adapted from several instruments used elsewhere considering the aim of the current study.7,14,18,32 Validity of the questionnaire was reviewed by an expert panel of physicians, pharmacists, students, academicians, and public health experts. The questionnaire was then piloted on a sample of 20 students from each institution to check for the time needed to finish, overall understanding of its components, particularly with students in non-healthcare-related fields of study, as well as the interpersonal and intrapersonal consistency. All needed adjustments were then made as scientifically justified. Those were not included in the final results. The overall reliability of the study tool was assessed using Cronbach alpha (0.7).
The questionnaire consisted of four major sections; sociodemographic characteristics, past medical and surgical history, SM habits and correlates, and academic performance. The sociodemographic characteristics section included questions relating to gender, age, nationality, marital status, university major, academic level, and social behavior indicators such as smoking habits. The past medical and surgical history section explored chronic diseases and surgeries in study participants. The SM habits and correlates section included directed questions about the self-use of certain drugs over the past two years, specifying the dose, frequency, and rationale behind using the drug, in addition to the source of information/recommendation about that drug. The choice of drugs surveyed in this study was based on a host of previous reports in the literature, taking into account the cultural and public contexts of the two countries, as well as the overall study objective exploring the perceived enhancers of academic performance.33,34 The medications evaluated were: peripheral analgesics (paracetamol and nonsteroidal anti-inflammatory drugs [NSAIDs]), central analgesics (eg, morphine, tramadol, pethidine), antibacterial drugs, sleeping pills, anabolic agents, propranolol, and amphetamine. The last section in the questionnaire gauged the rationale and the perceived academic benefits of SM through statements presented on a 3-point Likert scale (agree, neutral, disagree).
Statistical Analysis
The minimum sample size was calculated using the Cochran’s formula and found to be approximately 350 across the two universities, with a conservative estimate of 50% prevalence rate of SM, 95% confidence interval, and 5% margin of error, considering the combined total number of registered students at both universities (35,000). Data analysis was performed using the Statistical Package for Social Sciences (SPSS) program version 26 (IBM Inc., New York, USA). Descriptive statistics were employed for analysis. Categorical variables were presented as proportions and frequencies, while continuous variables were presented as means (±SD). Chi square test or Fisher’s exact test was used to compare proportions while independent sample T-test was used to compare means. Logistic regression analyses were used to assess the adjusted effects of gender, country, and university major on SM use. Adjusted odds ratio and 95% confidence interval were reported. A P-value of less than 0.05 was considered statistically significant.
Results
Background Characteristics of Study Respondents
The total number of consented respondents was 362. The overall mean age (±SD) was 20.36 (±1.66) years, with no statistically significant differences between students from Jordan (20.68±1.84 years) and their peers from the UAE (20.14±1.49 years; p=0.1). As shown in Table 2, 267 (73.8%) study participants were females, 217 (59.9%) were from the UAE, and 214 (59.1%) were in the healthcare-related majors. The majority of students were single (352 [97.2%]) and had no chronic illnesses (328 [90.6%]). Smoking was reported by 20% of our sample, with vapes and e-cigarettes being the most prevalent (80%).
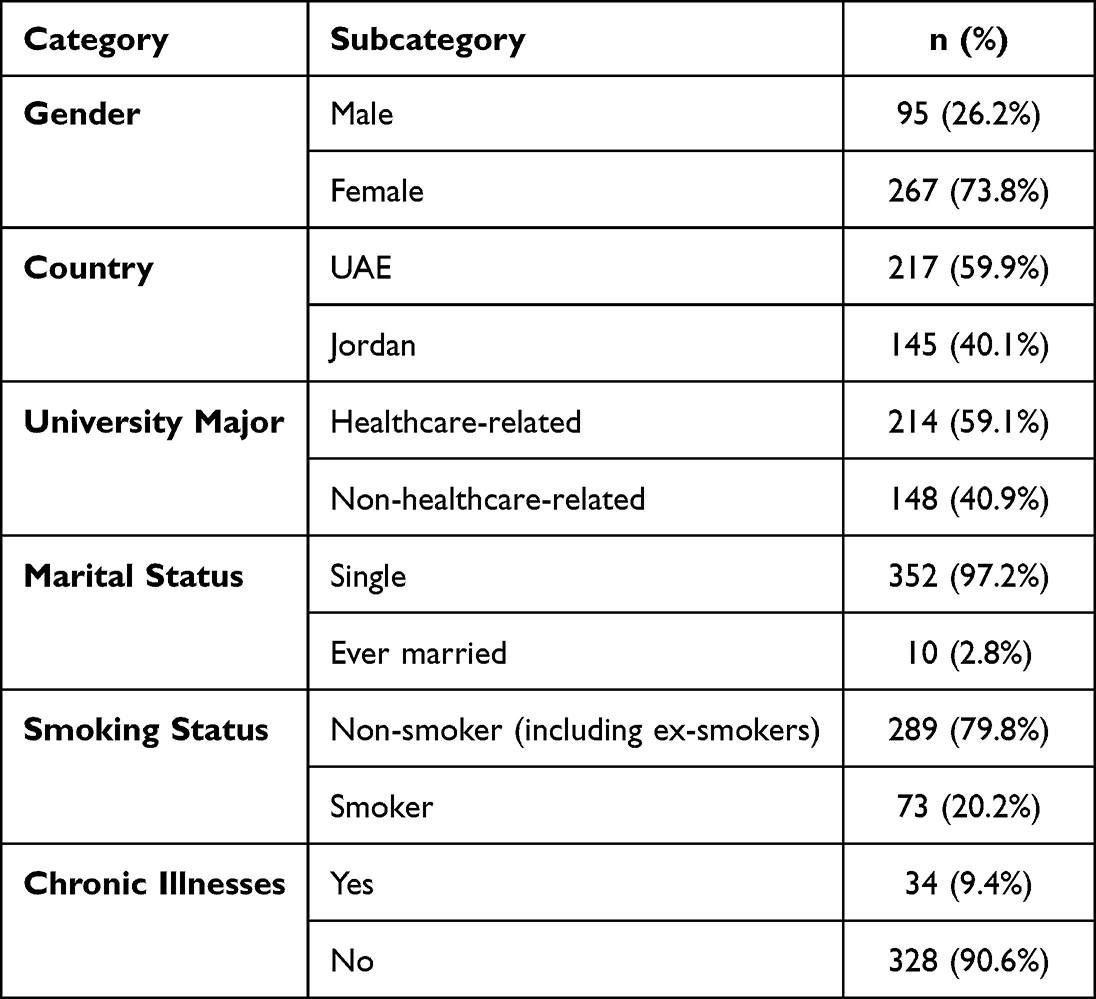 |
Table 2 Participants’ Background Characteristics (N = 362) |
Prevalence and Determinants of SM Usage
Table 3 summarizes the prevalence of SM usage of drugs/drug classes under investigation stratified by gender, country, and university major. Overall, gender differences in SM use were statistically significant only for paracetamol (p=0.001), ibuprofen (p=0.001), and antibacterial drugs (p=0.01). The use of these drugs was significantly higher among female compared to male students. Similarly, significant differences in SM by country were only detected for paracetamol and antibacterial drugs, with students from Jordan reporting a higher prevalence of use of these medications compared to students from the UAE (p=0.03 and p=0.001, respectively). Of importance, as well, is the magnitude of gap in the prevalence of antibacterial drug use between participants from Jordan (88 [60.7%]) and the UAE (74 [34.3%]). Further, the prevalence of SM was significantly higher among healthcare-related compared to non-healthcare-related majors of study for paracetamol (p=0.001), ibuprofen (p=0.001), NSAIDs (p=0.006), and antibacterial drugs (p=0.001). Importantly, the rate of inappropriate use of central analgesics, sleeping pills, amphetamine, anabolic drugs, and propranolol was limited, with no significant differences found among strata.
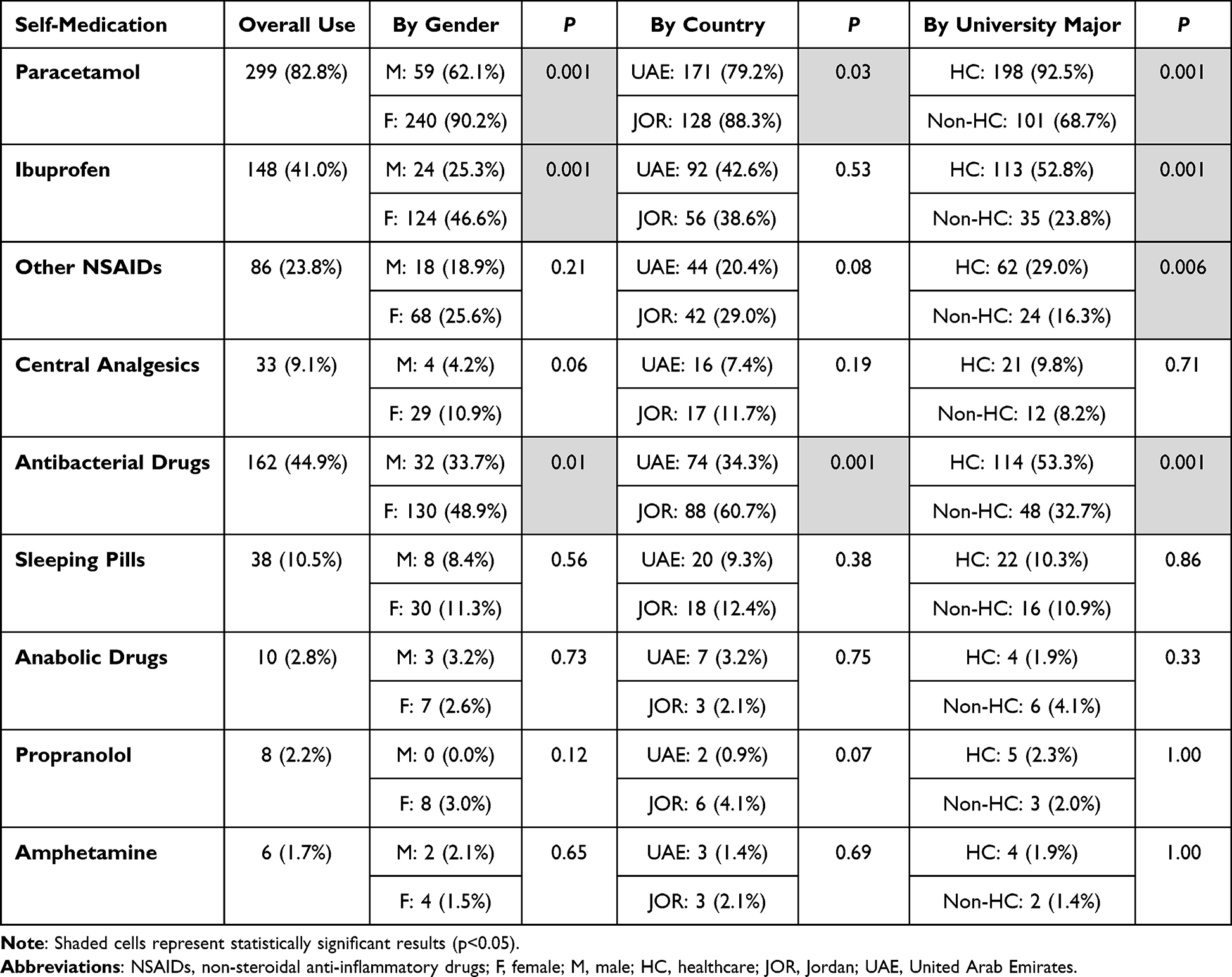 |
Table 3 Prevalence of Self-Medication Usage Stratified by Gender, Country, and University Major |
To further identify how gender, country, and university major impact the SM habits of the frequently utilized drugs in our sample, a binary logistic regression model was performed. The adjusted odds ratio (95% confidence interval) was estimated for each of these factors after controlling for potential confounders in the regression model (Table 4). Of the three investigated factors, the university major was found to be consistently significant as a determinant of the self-use of paracetamol, ibuprofen, and other NSAIDs, as well as antibacterial drugs, with the adjusted odds of using these medications invariably higher among healthcare-related majors (5.9 [95% CI: 3.06–11.38], 3.54 [95% CI: 2.20–5.68], 2.05 [95% CI: 1.21–3.49], and 2.39 [95% CI: 1.51–3.77], respectively). Female gender was significantly associated with the self-use of paracetamol (5.55 [95% CI: 2.95–10.41]) and ibuprofen (2.62 [95% CI: 1.52–4.54]) only. Of interest, the country of origin for participants was found to be a significant determinant of SM habits only for antibacterial drugs, with the odds of inappropriate use approximately three times higher among students from Jordan compared to those from the UAE (2.91 [95% CI: 1.86–4.57]).
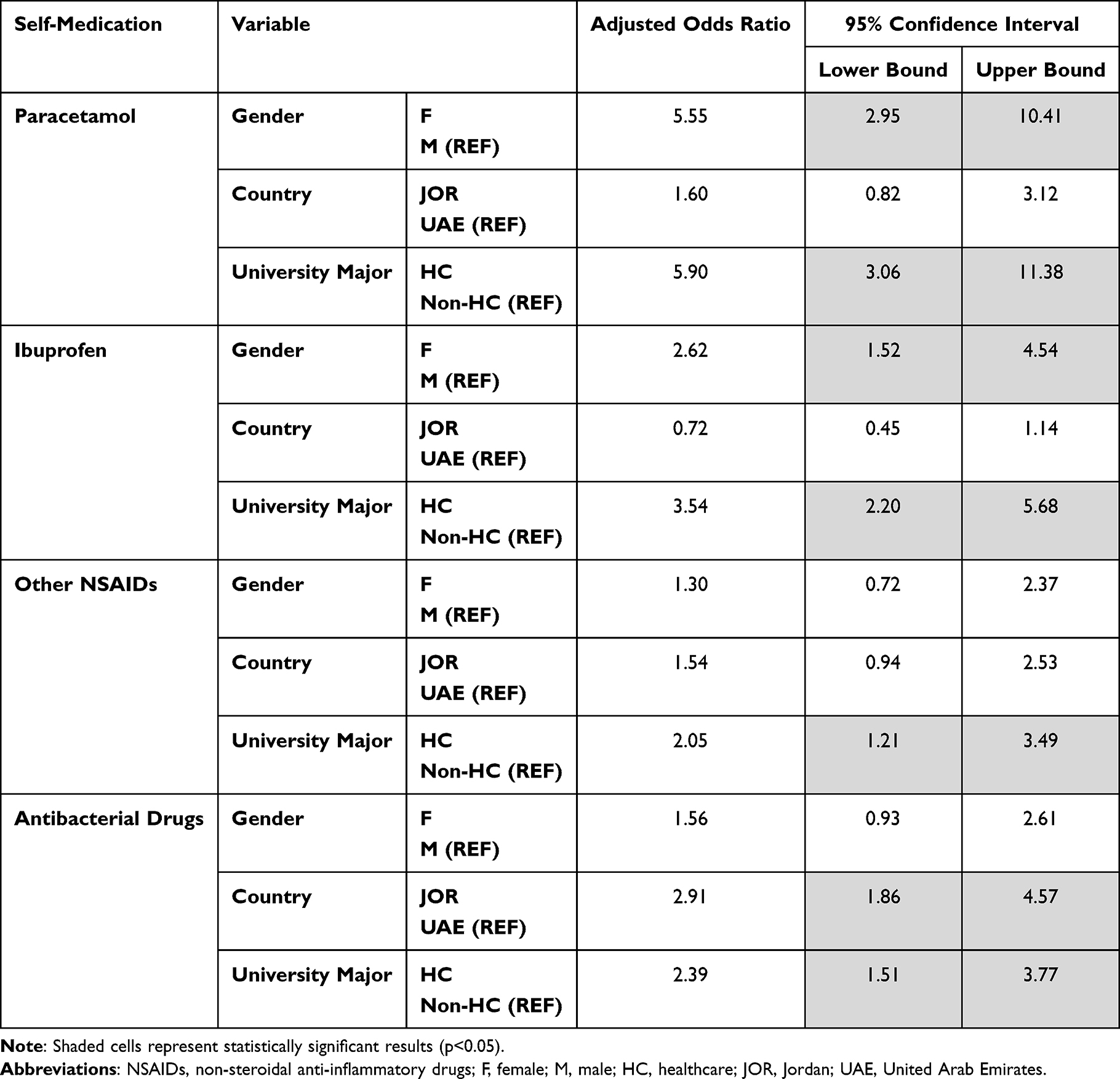 |
Table 4 Regression Analysis of Determinants of Self-Medication Usage |
Moreover, the study respondents reported that family and friends, regardless of their profession, as well as an inappropriate/extended use of a doctor prescription were by far the major sources of recommendation for SM use, as shown in Table 5. The role of pharmacists in such practices was justifiably less frequent, particularly for centrally acting drugs. On the other hand, participants’ absolute reliance on their own judgement upon embarking on SM use was least frequently reported.
 |
Table 5 Distribution of Self-Medications by the Source Recommending Its Use |
The Perceived Rationale and Academic Performance Benefits of SM Practice
We evaluated how university students justify the practice of self-medicating and whether it improves their academic performance by considering their agreement with specified open statements (Figure 1). Of the suggested motives, the majority of students assumed they self-medicate when their health issue is perceived as minor (197 [54.6%]), albeit only 125 (34.6%) of them thought that they are knowledgeable enough to do so. Further, the practice of SM was believed to save time and/or money by 148 (41.0%) and 116 (32.1%) of students, respectively. Notably, only 74 (20.5%) of the respondents agreed that the practice of self-medicating boosts their academic performance. Such perception was justified by improved concentration and focus during study (84 [23.3%]), improved performance in exams (57 [15.8%]), and relief of the stresses of exams (66 [8.0%]) and public appearances (29 [8.0%]). Of significance, we found that almost 27% of students did not agree to any of the proposed/stated benefits of SM on the academic performance, while a minor 4% of respondents agreed to all statements, particularly among those who reported using central analgesics and/or propranolol (data not shown).
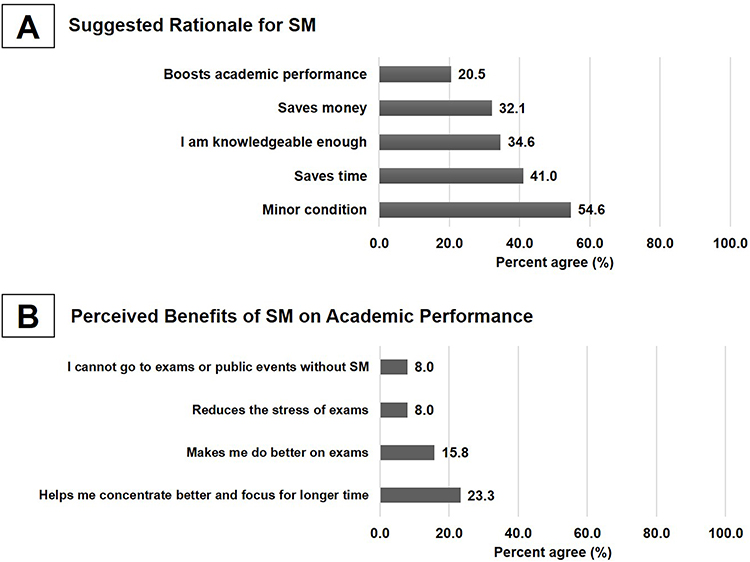 |
Figure 1 (A) Frequency distribution of study participants’ rationale for self-medication use. (B) Frequency distribution of study participants’ perceived benefits of self-medication on their academic performance. |
Discussion
This comparative pilot study shed light on the most predominant determinants of SM among university students in the MENA region using UAE and Jordan as an example. The main findings of this study are; (1) over-the-counter analgesics as well as antibacterial drugs are the most widely misused medications by university students; (2) female gender, Jordan as the country of study, and majoring in healthcare fields were the significant determinants of SM in our sample, with the latter being the most consistent factor impacting this practice; and (3) only a minority of university students believe that SM boosts their academic performance.
In agreement with a substantial body of literature, we report here that peripheral pain killers, such as paracetamol, ibuprofen and other NSAIDs, and antibacterial drugs have been most frequently self-used by university students.3,35 This finding is justifiable for peripheral analgesics as they are sold over-The-counter and represent a patient’s “best friend” in the face of conventional pain, particularly among females suffering regularly from menstrual pains and associated symptoms.36,37 For instance, Al-Kubaisi et al has reported in 2022 that approximately 60% of university students across the UAE have used over-The-counter medications in the past three months with or without a pharmacist advice.38 Similarly, a recent study by AlShahrani et al in 2019 showed an overwhelming 92% self-use of painkillers among medical students in Saudi Arabia.6 However, the prevalent unsupervised use of antibacterial drugs in our sample is quite perplexing, given that both the UAE and Jordan have recently adopted the ASP in their healthcare systems.30 Among the general population, it was recently reported that the prevalence of SM with antibiotics was almost comparable between the two countries; 31.7% in the UAE39 vs 40.4% in Jordan.40 To the contrary, we report here that the odds of misusing antibacterials have been almost three times greater for students from Jordan compared to their peers from the UAE. This serves as a proper window into the uptake and application of ASP in both countries, particularly Jordan. While most published literature alludes to the significant success of ASP strategies in the UAE and Jordan,41,42 our findings must be dissected by health policy makers to better understand the deep-rooted limitations and strategies to alleviate them. In the context of university education, for example, revolutionization of health education curricula and targeted awareness campaigns to students tackling ASP and antimicrobial resistance are urgently needed.
Consistent with our results, the university major of students has been frequently highlighted for its essential role in their SM habits. Medical students, as potential medical doctors, have a unique drive to bring their ill-perceived expertise into effect, creating serious issues regarding misdiagnosis and overdosage. Niroomand et al found in 2020 that almost 72% of medical students in Iranian universities practiced SM in their first year.25 Interestingly, Kasulkar et al revealed in 2015 that the prevalence rate of SM among medical students in India starts rising from the first year to the graduation year.19 In pharmacy majors, a study surveyed the SM habits among pharmacy and PharmD students at the University of Jordan. Within that group, approximately 87% of students reported self-medicating.43 Nonetheless, these findings are in contrast to other studies conducted in Brazil,44 Pakistan,45 and Ghana,46 which found insignificant differences in the prevalence of SM between students in health- and non-health-related majors. Whether this contrast is related to successful health education programs and policies in these countries or simply mirroring a cultural variation is not clear though.
Moreover, our results show that social influences from family, friends, and relatives played a significant role in spreading the practice of SM. This is in line with several previous studies delineating the high cultural and societal acceptance of SM in developing countries. For instance, Janatolmakan et al have recently identified cultural promotion of SM as a strong driving factor for the unsupervised use of medicines in the Iranian society.15 In Nigeria, social factors such as peer pressure played a positive role in endorsing SM behavior.47 Further, students in Saudi universities6 as well as Egyptian universities14 were found to list “relatives” knowledge of medications as the second main source of information regarding drugs. Critically, such societal attitude leads to a vicious cycle of misuse in the community as students who self-medicate tend to offer advice to family and friends. In a study among adults in Uganda, more than half (68.2%) of the participants expressed their willingness to recommend SM to sick people.48
Noteworthy, our results highlight an encouraging limited abuse of central analgesics, sleeping pills, amphetamine, and propranolol. This perhaps can be intuitively connected to the finding that only a minority of our respondents assumed that SM improves their academic performance. Studies from the US34,49 and Switzerland50 have previously shown that a significant percentage of self-medicating university students were found to engage in the nonmedical use of prescription and illicit neuroenhancers to allegedly boost their concentration and ability to sustain focus for a longer duration. Such misconception, however, has been refuted by several cross-sectional studies emphasizing that college students on such stimulants skipped more classes, had a lower cumulative grade point average (cGPA), and were involved in other forms of illicit drugs use.33 Furthermore, experimental studies have clearly shown no significant improvement of any molecular or biochemical markers of cognition in users compared with controls.51
Our study manifests several limitations. First, the sample size is not sufficient to yield more robust statistical analyses with more precise correlation statistics, which precludes generalizability of results. Second, the stratified sampling technique in our pilot study has its inherent limitations that could affect the interpretation of the results. Exact matching of respondents based on gender, university major, and country of study was indeed difficult to achieve despite efforts to extend timeframe and to employ targeted invitations to participate. Based on the reported results, however, one can focus future research to fine-tune research methods addressing more specified research questions. Third, online self-administered questionnaires surveying practices over a long duration carry the risks of recall bias, duplication, inaccuracy, and dishonesty. Nonetheless, the comparative and multicentric nature of our study targeting a critical public health gap should be viewed as major strengths that support its utilization by health policy makers.
Conclusion
Our study identifies the major determinants of SM among university students in the MENA region, namely female gender, students from Jordan, and those in healthcare majors. Results of this study should be the cornerstone for informed, data-based awareness campaigns in the future, aiming to mitigate the prevalent practice of SM among university students, with a special focus on the aforementioned susceptible populations. Further research in this area is needed to better understand the impact and determinates of SM use among this vulnerable age group.
Acknowledgments
Funding for this research was provided by the Deanship of Research and Graduate Studies at Ajman University, UAE (Grant number: 2021-IRG-MED-2).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alghanim SA. Self-medication practice among patients in a public health care system. East Mediterr Health J. 2011;17(5):409–416. doi:10.26719/2011.17.5.409
2. Bennadi D. Self-medication: a current challenge. J Basic Clin Pharm. 2013;5(1):19–23.
3. Behzadifar M, Behzadifar M, Aryankhesal A, et al. Prevalence of self-medication in university students: systematic review and meta-analysis. East Mediterr Health J. 2020;26(7):846–857.
4. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21–31.
5. Khalifeh MM, Moore ND, Salameh PR. Self-medication misuse in the Middle East: a systematic literature review. Pharmacol Res Perspect. 2017;5:4.
6. Alshahrani SM, Alavudeen SS, Alakhali KM, Al-Worafi YM, Bahamdan AK, Vigneshwaran E. Self-medication among King Khalid university students, Saudi Arabia. Risk Manag Healthc Policy. 2019;12:243–249.
7. Malak MZAA. Self-medication practices among university students in Jordan. Malaysian J Med Health Sci. 2019;15(2):112–119.
8. Sawalha AF. A descriptive study of self-medication practices among Palestinian medical and nonmedical university students. Res Social Adm Pharm. 2008;4(2):164–172.
9. Al-Hussaini M, Mustafa S, Ali S. Self-medication among undergraduate medical students in Kuwait with reference to the role of the pharmacist. J Res Pharm Pract. 2014;3(1):23–27.
10. Al-Ameri RJ, Abd Al-Badri HJ, Lafta RK. Prevalence of self-medication among university students in Baghdad: a cross-sectional study from Iraq. East Mediterr Health J. 2017;23(2):87–93. doi:10.26719/2017.23.2.87
11. Tabiei SFZ, Eizadpanah A. Self-medication with drug amongst university students of Birjand. Mod Care J. 2012;9(4):371–378.
12. Sharif SAIO. Evaluation of self-medication among pharmacy students. Am J Pharmacol Toxicol. 2012;7(4):135–140. doi:10.3844/ajptsp.2012.135.140
13. Awad AI, Eltayeb IB. Self-medication practices with antibiotics and antimalarials among Sudanese undergraduate university students. Ann Pharmacother. 2007;41(7–8):1249–1255. doi:10.1345/aph.1K068
14. Helal RM, Abou-ElWafa HS. Self-medication in university students from the city of Mansoura, Egypt. J Environ Public Health. 2017;2017:9145193. doi:10.1155/2017/9145193
15. Janatolmakan M, Abdi A, Andayeshgar B, Soroush A, Khatony A. The reasons for self-medication from the perspective of Iranian nursing students: a qualitative study. Nursing Research and Practice. 2022;2022:2960768. doi:10.1155/2022/2960768
16. Hughes CM, McElnay JC, Fleming GF. Benefits and risks of self medication. Drug Saf. 2001;24(14):1027–1037. doi:10.2165/00002018-200124140-00002
17. Shrestha AB, Aryal M, Magar JR, Shrestha S, Hossainy L, Rimti FH. The scenario of self-medication practices during the covid-19 pandemic; a systematic review. Ann Med Surg. 2022;82:104482.
18. Alshogran OY, Alzoubi KH, Khabour OF, Farah S. Patterns of self-medication among medical and nonmedical University students in Jordan. Risk Manag Healthc Policy. 2018;11:169–176.
19. Kasulkar AA, Gupta M. Self medication practices among medical students of a private institute. Indian J Pharm Sci. 2015;77(2):178–182.
20. James H, Handu SS, Al Khaja KA, Otoom S, Sequeira RP. Evaluation of the knowledge, attitude and practice of self-medication among first-year medical students. Med Princ Pract. 2006;15(4):270–275.
21. El Ezz NF, Ez-Elarab HS. Knowledge, attitude and practice of medical students towards self medication at Ain Shams University, Egypt. J Prev Med Hyg. 2011;52(4):196–200.
22. Haroun MF, Al-Kayali RS. Self‑medication among undergraduate medical students in two universities in Syria. Int J Pharm Sci Res. 2017;8(4):1881–1886.
23. Gras M, Champel V, Masmoudi K, Liabeuf S. Self-medication practices and their characteristics among French university students. Therapie. 2020;75(5):419–428.
24. AlQahtani HA, Ghiasi FS, Zahiri AN, Rahmani NI, Abdullah N, Al Kawas S. Self-medication for oral health problems among adults attending the University Dental Hospital, Sharjah. J Taibah Univ Med Sci. 2019;14(4):370–375.
25. Niroomand N, Bayati M, Seif M, Delavari S, Delavari S. Self-medication pattern and prevalence among Iranian medical sciences students. Curr Drug Saf. 2020;15(1):45–52.
26. Ahmadi SM, Jamshidi K, Sadeghi K, Abdi A, Vahid MP. The prevalence and affecting factors on self-medication among students of Kermanshah university of medical science in 2014. J Clin Diagn Res. 2016;10(5):IC01–IC04.
27. Pirzadeh A, Mostafavi F. Self-medication among students in Isfahan university of medical sciences based on health belief model. J Educ Health Promot. 2014;3:112.
28. Mannasaheb BA, Al-Yamani MJ, Alajlan SA, et al. Knowledge, attitude, practices and viewpoints of undergraduate university students towards self-medication: an institution-based study in Riyadh. Int J Environ Res Public Health. 2021;18:16.
29. Arria AM, Geisner IM, Cimini MD, et al. Perceived academic benefit is associated with nonmedical prescription stimulant use among college students. Addict Behav. 2018;76:27–33.
30. Ababneh MA, Nasser SA, Rababa’h AM. A systematic review of antimicrobial stewardship program implementation in Middle Eastern countries. Int J Infect Dis. 2021;105:746–752.
31. Ghaieth MF, Elhag SR, Hussien ME, Konozy EH. Antibiotics self-medication among medical and nonmedical students at two prominent Universities in Benghazi City, Libya. J Pharm Bioallied Sci. 2015;7(2):109–115.
32. Alkhatatbeh MJ, Alefan Q, Alqudah MA. High prevalence of self-medication practices among medical and pharmacy students: a study from Jordan. Int J Clin Pharmacol Ther. 2016;54(5):390–398.
33. Arria AM, Caldeira KM, Vincent KB, et al. Do college students improve their grades by using prescription stimulants nonmedically? Addict Behav. 2017;65:245–249.
34. Ross MM, Arria AM, Brown JP, et al. College students’ perceived benefit-to-risk tradeoffs for nonmedical use of prescription stimulants: implications for intervention designs. Addict Behav. 2018;79:45–51.
35. Al-Qahtani AM, Shaikh IA, Shaikh MAK, Mannasaheb BA, Al-Qahtani FS. Prevalence, perception, and practice, and attitudes towards self-medication among undergraduate medical students of Najran University, Saudi Arabia: a cross-sectional study. Risk Manag Healthc Policy. 2022;15:257–276.
36. Habeeb GE
37. Albasheer OBMM, Masmali BM, Ageeli RA, et al. Self-medication practice among undergraduate medical students of a Saudi tertiary institution. Trop J Pharm Res. 2016;15(10):2253–2259.
38. Al-Kubaisi KA, Hassanein MM, Abduelkarem AR. Prevalence and associated risk factors of self-medication with over-The-counter medicines among university students in the United Arab Emirates. Pharm Pract. 2022;20(3):2679.
39. Abduelkarem AR, Othman AM, Abuelkhair ZM, Ghazal MM, Alzouobi SB, El Zowalaty ME. Prevalence of self-medication with antibiotics among residents in United Arab Emirates. Infect Drug Resist. 2019;12:3445–3453.
40. Nusair MB, Al-Azzam S, Alhamad H, Momani MY. The prevalence and patterns of self-medication with antibiotics in Jordan: a community-based study. Int J Clin Pract. 2021;75(1):e13665.
41. Yusef D, Hayajneh WA, Bond SE, et al. Analysis of hospital antimicrobial consumption to identify targets for antimicrobial stewardship. Infect Control Hosp Epidemiol. 2022;43(7):943–945.
42. Hamdan S, El-Dahiyat F. Implementation and evaluation of an antimicrobial stewardship program across nine hospitals in the United Arab Emirates: a qualitative study. J Pharm Pract Res. 2020;50(2):124–131.
43. Alsous MEE, Jalil MA, Alhawmdeh E. Evaluation of self-medication practice among pharmacy students in Jordan. Jordan J Pharm Sci. 2018;11(1):15–24.
44. Correa da Silva MG, Soares MC, Muccillo-Baisch AL. Self-medication in university students from the city of Rio Grande, Brazil. BMC Public Health. 2012;12(339):1.
45. Zafar SN, Syed R, Waqar S, et al. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58(4):214–217.
46. Donkor ES, Tetteh-Quarcoo PB, Nartey P, Agyeman IO. Self-medication practices with antibiotics among tertiary level students in Accra, Ghana: a cross-sectional study. Int J Environ Res Public Health. 2012;9(10):3519–3529.
47. Ejeh V, Ojotu BN. Peer influence and self esteem as predictors of self-medication among the youth in the middle belt region of Nigeria. Int J Adv Res. 2021;9:544–550.
48. Ocan M, Bwanga F, Bbosa GS, et al. Patterns and predictors of self-medication in northern Uganda. PLoS One. 2014;9(3):e92323.
49. Dupont RL, Coleman JJ, Bucher RH, Wilford BB. Characteristics and motives of college students who engage in nonmedical use of methylphenidate. Am J Addict. 2008;17(3):167–171.
50. Maier LJ, Liechti ME, Herzig F, Schaub MP. To dope or not to dope: neuroenhancement with prescription drugs and drugs of abuse among Swiss university students. PLoS One. 2013;8(11):e77967.
51. Volkow ND, Fowler JS, Wang GJ, et al. Methylphenidate decreased the amount of glucose needed by the brain to perform a cognitive task. PLoS One. 2008;3(4):e2017.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Self-Medication Practice and Its Determinants Among Undergraduate Health Science Students of College of Medicine and Health Sciences, Bahir Dar University, North West Ethiopia: A Cross-Sectional Study
Yismaw MB, Feyisa K, Yehualaw A, Tafere C, Demsie DG, Bahiru B, Kefale B
Advances in Medical Education and Practice 2023, 14:279-288
Published Date: 27 March 2023
Assessing Anxiety and Depression Among Students Post-COVID-19: Exploring Associating Factors
Basheti IA, Assaraira TY, Obeidat NM, Al‐Abed Al‐haq F, Refai M
Psychology Research and Behavior Management 2023, 16:1797-1810
Published Date: 12 May 2023
Depression Among University Students in Jordan After the COVID-19 Pandemic: A Cross-Sectional Study
Alhemedi AJ, Qasaimeh MG, Abdo N, Elsalem L, Qaadan D, Alomari E, lssa Q, Alhadeethi M, Abdul Kareem HM, Almasri A, Elkhateeb O, Naser AY
Psychology Research and Behavior Management 2023, 16:4237-4249
Published Date: 18 October 2023